Back to Journals » Patient Preference and Adherence » Volume 16
Imagine to Remember: An Episodic Future Thinking Intervention to Improve Medication Adherence in Patients with Type 2 Diabetes
Authors Epstein LH ![]() , Jimenez-Knight T, Honan AM, Paluch RA, Bickel WK
, Jimenez-Knight T, Honan AM, Paluch RA, Bickel WK ![]()
Received 9 October 2021
Accepted for publication 15 December 2021
Published 13 January 2022 Volume 2022:16 Pages 95—104
DOI https://doi.org/10.2147/PPA.S342118
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Leonard H Epstein,1 Tatiana Jimenez-Knight,1 Anna M Honan,1 Rocco A Paluch,1 Warren K Bickel2
1Department of Pediatrics, University at Buffalo Jacobs School of Medicine and Biomedical Sciences, Buffalo, NY, USA; 2Addiction Recovery Research Center, Fralin Biomedical Research Center, Virginia Tech Carilion School of Medicine, Roanoke, VA, USA
Correspondence: Leonard H Epstein
Department of Pediatrics, University at Buffalo Jacobs School of Medicine and Biomedical Sciences, G56, Farber Hall, Buffalo, NY, 14214, USA
Tel +1 716-829-3400
Email [email protected]
Purpose: Medication nonadherence is prevalent in diabetic populations, with “forgetting” a commonly cited reason. This issue of forgetfulness is due, in part, to a failure of prospective memory (PM). Episodic future thinking (EFT) has been shown to improve PM but has not been used to improve medication adherence.
Patients and Methods: The current study used a multiple baseline design (N = 4) to test the effects of EFT on medication non-adherence for four patients with a diagnosis of type 2 diabetes or prediabetes, with comorbid high blood pressure or high cholesterol. Medication adherence was objectively measured over 15 weeks using medication event monitoring systems.
Results: Results of visual analysis showed medication adherence was reliably improved, confirmed by mixed model analysis of variance (p < 0.001), with significant differences from baseline to treatment (Tau < 0.05) for 3 of 4 participants. Improvements in two measures of PM (effect size (ES) = 0.73, 0.80) and delay discounting (ES = 1.20) were observed.
Conclusion: This study provides a feasible way to improve medication adherence in patients with prediabetes or type 2 diabetes.
Keywords: episodic future thinking, prediabetes, prospective memory, medication adherence
Introduction
Many people with prediabetes1 or type 2 diabetes2 have concurrent hypertension or dyslipidemia. However, many people are not adherent to their medications, and it is estimated that as many as 50% of the patients fail to take their medications as prescribed.3 Patients who have difficulty adhering to their medication regimens frequently experience poor health outcomes and struggle to manage their disease.4,5 Nonadherence is extremely prevalent in diabetic and prediabetic populations, with “forgetting” the most commonly cited reason for nonadherence.6 Forgetfulness as a reason for medication nonadherence is due in part to problems with prospective memory (PM), or the ability to recall and engage in an action at an appropriate time in the future. Previous studies have demonstrated the relationship between poor PM and medication nonadherence.7,8 Laboratory research has shown that performance on a PM task was correlated with medication adherence in diabetic participants.9 Improving PM could be a means to enhance medication adherence within this population.
For people with prediabetes or type 2 diabetes and comorbid disease states such as hypertension or dyslipidemia, taking medication is designed to prevent future morbidity. By definition, prevention of any disease state requires engaging in behavior now for future benefits, which requires prospective thinking. Rather than focusing on immediate gratification and impulsive decision-making, prevention is associated with a focus on future benefits. One way to assess temporal decision-making is through delay discounting tasks, which assess the degree to which people prefer small immediate rewards over larger delayed rewards.10,11 High degree of discounting the future is related to poor medication adherence, poor diets and low activity levels in people with prediabetes,12 as well as poor adherence and diabetes self-care behaviors in those with type 1 or type 2 diabetes.13–15 Modifying the temporal window of a person’s decision-making by reducing delay discounting or discounting of the future may also be important to improve medication adherence and health behaviors in people with prediabetes or type 2 diabetes.12–16
One approach to improving PM is implementation intentions.8,17 Implementation intentions involve creating mental simulations of future events (such as medication taking) that take into account when, where and how to meet behavioral goals and associating these events with cues associated with the action and context of the future event using if–then statements.8,17,18 Implementation intentions have been shown to improve medication adherence across a variety of medical conditions,8 and one way in which they may work is by improving prospective memory.8
Another way to improve PM is Episodic Future Thinking (EFT),19–21 an intervention designed to mentally project oneself into vivid, highly contextual future scenarios.22–25 Prospective thinking can involve four different forms of future thinking, including simulation, prediction, intention and planning.23 While these forms can be conceptualized within EFT,23 episodic future thinking may be part of implementation intentions.22 EFT has also been shown to reduce negative health behaviors, such as smoking, drinking, and overeating,26–29 and PM in controlled laboratory studies,19–21 but has not yet been tested as a way to improve medication adherence in a clinical sample of people with prediabetes or type 2 diabetes. EFT also has the benefit of modifying a person’s temporal window of decision-making by reducing delay discounting in people with prediabetes,24,25 thus potentially targeting two factors associated with poor medication adherence, prospective memory8 and delay discounting.12–16 While no research was identified that assessed the effect of implementation intentions on delay discounting in people with poor medication adherence, research has shown that when implementation intentions are used to reduce alcohol consumption, they did not simultaneously improve delay discounting.18
The current study was an early phase translational science study designed to evaluate EFT effects on medication adherence using a single-case experimental multiple baseline design.30 Single-case experimental designs are efficient methods for testing new interventions, and for establishing a functional relationship between treatment and outcome changes across multiple dependent measures.30 In addition to measuring medication adherence, we also measured both PM as well as delay discounting to assess whether EFT could modify both potential mechanisms that may be related to poor medication adherence.
Methods
Participants
Potential participants were recruited using a local Research Match database, as well as recruiting through notices in our Clinical and Translational Research Center and notices on social media sites for people with prediabetes or type 2 diabetes who were interested in improving their medication adherence. Inclusion criteria were a diagnosis of type 2 diabetes or prediabetes, with high blood pressure or high cholesterol, and currently prescribed at least one medication for blood glucose regulation, high blood pressure, or high cholesterol, and met non-adherence criteria of less than 80% non-adherence during comprehensive baseline assessment. Exclusion criteria included unmanaged psychological disorders, neurological conditions, pregnancy, substance abuse issues, intellectual impairments or learning disabilities, not having access to the internet, and not experiencing a recent stressful major life event, which could influence prospective memory.
Multiple Baseline Design
Multiple baseline designs are part of a family of single-case experimental designs. Multiple baseline designs collect repeated measurements on a small number of participants, and implement the treatment in a staggered fashion. If the outcome variables change only after treatment is introduced, and not during extended baseline, the change can be attributed to the introduction of treatment. The more replications of this effect, the stronger the case for the treatment to have influenced the outcome. The goal in single-case experimental designs in general, and multiple baseline designs in particular, is a functional analysis of the relationship between treatment and outcome for the people that are studied.30,31
The multiple baseline design used in this study included two phases, a baseline phase and an EFT treatment phase. An important aspect of of multiple baseline designs is that the measures during each phase provide a good estimate of that behavior under those conditions, and as such the length of the phase depends on observation of relative stability, or a change in the opposite direction from treatment effects. During baseline, medication adherence was objectively measured as a screen for identifying people who were objectively nonadherent, with no indication that participants were improving as a function of repeated measurement. Participants who were not found to be nonadherent during baseline, or who improved as a function of repeated measurement without treatment were not included into treatment. After stable baselines were established for all participants, treatment is then introduced in a staggered fashion, with people randomized to when treatment began.32 This randomization removes any potential bias that may occur if people were asked when they are ready to begin, or if treatment is started based on how rapidly someone meets baseline criteria. After treatment is introduced, it should be carried out long enough to establish stability or clear trends in the direction of change. The statistical analyses to be presented are designed to assess baseline trend, the stability of baseline and EFT data, and phase changes from baseline to EFT.
Single-case experimental designs are ideally suited for early phase translational research to explore whether a basic cognitive neuroscience method, in this case EFT, can be translated into an effective intervention. If the single-case design shows a functional relationship between treatment and outcome, the next step would be a fully powered, randomized controlled study designed to compare the new treatment to established methods.
Measures
Medication Adherence
MEMS
Medication Event Monitoring Systems (MEMS) were used to assess medication adherence. Data was downloaded from the MEMS at the Assessment sessions, as well as at the intervention sessions. The MEMS provide data on how frequently the medication bottle was opened and the times at which the medication bottle was opened. The MEMS are considered the gold standard for measuring medication adherence and has been shown to correlate with pill count data.33–35
Self-Reported Medication Adherence
To determine participants’ eligibility and which medications to study, self-reported medication adherence was assessed at the Baseline/Screening session. Participants were asked, “Over the past 30 days, what percentage of the time did you take your (medication) as prescribed?” This rating was used to determine which medications to measure with the MEMS cap. Medications with the lowest rating of adherence were measured.
Prospective Memory Tasks
Virtual Week
The Virtual Week board game is a reliable and valid measure36 in non-clinical and clinical samples used to assess PM.36,37 This computerized task was completed by participants at the screening/baseline session and assessment sessions. Participants were presented with a board game paradigm, in which they simulated going through a “day” (represented by moving a token around the board). They were also instructed to complete different tasks throughout the day or when other events occurred (eg, take your antibiotics when you eat breakfast; use your asthma inhaler when the clock reads 11 am). Participants completed three “days” of this task and, in total, were asked to complete 30 tasks. In addition to being scored on their ability to complete each task, participants were also scored on completing time-based PM tasks and event-based PM tasks. Data was also collected on whether participants completed these tasks early or late. Correct in this task is defined as after the dice roll that initiated the task but before the next dice roll if the task is event based or within ten seconds if the task is time based. Early is defined as anything before the target time and anything before the dice roll of that task. Late is defined as anything after the next dice roll for that task or ten seconds after the allotted time. Additionally, during the assessment sessions, participants read through their EFT cues before beginning each “day.” As this task was administered three times throughout the study, different versions of the task were presented to eliminate practice effects. Participants’ scores are the percent of tasks correct out of 30 tasks. Higher scores indicated better prospective memory.
Event-Based PM Task
An event-based prospective memory task was also administered. This task has acceptable reliability reliability38 and extensive validation in relation to theoretically derived predictions,39 including relationships with medication adherence.40,41 In the version of the task we used, participants were asked to complete an extra task (clicking the mouse an extra time when certain words appeared) while simultaneously finding target words on a word list.40 This task was completed at the screening/baseline session, as well as the assessment sessions. Participant scores were from 0 to 8, 8 being the highest score attainable. Higher scored were indicative of better prospective memory.
Delay Discounting Task
Adjusting Amount Delay Discounting Task
All participants completed an adjusting amount delay discounting task at the baseline/screening session, and each assessment session.12 During this task, participants chose between receiving a larger amount of money at a future time point (1 week, 1 month, 3 months, 6 months, 1 year) or a smaller amount of money now (eg, “Would you rather have $50 now or $100 in 1 week?). The amount of money offered “now” adjusted based on participant’s initial response. For each participant, indifference points, or the amount of money offered now that was just as appealing to them as $100 at a future time point, were established. During the assessment sessions, participants read through their EFT cues before completing the task.
Working Memory Task
Backward Corsi Tapping Task
The Backwards Corsi Tapping Task was used to assess short-term visuospatial working memory at the screening/baseline session42,43 as diabetes can impair working memory,44 which we have shown is related to EFT.28,45 The Corsi Block Tapping Task has acceptable reliability and validity in older adults.46 This computerized task involved participants viewing a series of squares on a computer screen. The squares on the screen lit up one at a time, and participants were asked to copy the pattern that the squares lit up in the reverse order by clicking the squares with their mouse. This task began with the two squares lighting up per trial and progressively got longer as participants completed each trial. There were two trials per trial length. Following participants getting two trials of the same length wrong, the task terminated.
Procedures
Participants were randomized into one of three staggered baselines, 6, 8, or 10 weeks. Intervention for all participants continued up to week 15. The study began before the COVID-19 pandemic, and one participant had an in-person screening appointment, but all other appointments including case management were done via the video conferencing software Zoom (Zoom Video Communications, Inc., 2016). The study was approved by the IRB at the University at Buffalo, and guidelines outlined in the Declaration of Helsinki were followed. The trial was registered at NCT04157673. The study ran from February 2020 to October 2020. All participants provided informed consent. Deidentified medication, memory and delay discounting data will be available from Dr Epstein ([email protected]) upon request for at least 5 years after study publication.
Screening and Baseline
Initially, eligible participants were invited to complete a screening/baseline session. At this session, participants were shown a brief orientation, detailing the responsibilities of eligible participants, and they answered questions regarding demographics, alcohol and drug use, and their medication adherence. Additionally, participants completed prospective memory36,37,40 and delay discounting12 tasks.
Eligible participants were mailed up to 3 medication event monitoring systems (MEMS, AARDEX, Zurich, Switzerland) caps, depending on how many medications they were prescribed for blood glucose regulation, hypertension, and hyperlipidemia. Upon receiving the MEMS caps, the baseline phase of the study began. The baseline phase was conducted for at least 6 weeks for all participants to determine participants’ medication adherence and to allow for any effects of using the MEMS cap on adherence to wear off, which has been shown to last for 40 days.47 Any participant who improved adherence just due to monitoring would not be eligible for the study. Eligibility criteria were set at less than 80% adherence over the baseline period.35,48,49
Intervention
After the 6-week baseline, research staff completed a contact-free MEMS reading session, in which data from the MEMS caps were obtained. Participants whose medication adherence was below 80% per week were randomized into a 6-week baseline group, an 8-week baseline group, or a 10-week baseline group.
The EFT intervention was adapted from our EFT intervention designed to reduce delay discounting in people with prediabetes24 to focus on improving prospective memory.19,20,50,51 The intervention had participants first create their EFT cues. Cue creation involved participants creating scenarios in which they successfully took their medications at future time points. Participants were instructed to write their cues in the present tense, include specific details, such as who they are with, where they are, and how they are feeling, and focus on the positive aspects of the event. Participants created five cues in this manner and were instructed to create cues for typical weekdays, typical weekends, and unusual days (eg, when they are traveling). The cues were made bi-weekly; participants engaged with their EFT cues daily using a smartphone app52 that presented cues at set intervals, and cues could also be retrieved at the participant’s discretion.
EFT Cue Examples
1). “In about 1 week, I am taking a dance lesson. I am enjoying the dance, and I remember to take my medication. I am in the dance lesson with my teacher and other friends and enjoying the learning, and during a break, I take my medication.” 2). “In about 1 week, I am sitting in my room taking my medication. I am getting ready for work and sit on my bed to take my medication. I have a glass of water on the nightstand ready to use. I am alone as my husband has left for work. Next, I test my sugar level, get dressed, and leave for work. I am taking my medications to stay in good health.”
Participants met weekly with case managers to integrate EFT into their routine to improve medication adherence. Participants were instructed to use their cues right before taking their medications for every medication dosage. Case managers would review the participants’ medication adherence and cue usage to discuss with challenges in taking their medication and revise cues with further details to strengthen EFT. Participants also practiced and discussed how to use their cues effectively in these sessions. These sessions were recorded and were reviewed for fidelity to the protocol.
Assessment Sessions
Assessments including Backward Corsi, delay discounting, and prospective memory tasks were completed at baseline, and delay discounting and prospective memory tasks were also completed when the intervention was introduced (either at week 7, week 9, or week 11) and after the intervention was complete (week 15).
Analytic Plan
Changes in medication adherence were first analyzed across the four subjects using visual inspection of the multiple baseline graph to assess whether baseline was stable and not improving before intervention and whether improvements in medication adherence appeared to be sequentially related to the introduction of EFT. Statistical analysis to support visual inspection of each case included analysis of baseline trend, the stability of baseline and EFT data, phase changes from baseline to EFT, percent non-overlapping data from baseline to EFT, and immediacy of change from baseline to EFT.30 Changes across the three different baseline lengths across the four subjects were accomplished using a mixed model that included fixed effects of level and trend for phase A and B, and random effects level and trend in phase A.53 The p values for the multiple baseline should be interpreted as evidence for the reliable relationship between treatment and outcome for the participants that were studied, not that the results would generalize beyond the current sample. While the sample size is too small to analyze traditional pre-post changes, effect sizes were calculated for changes from baseline to the end of the study for delay discounting, virtual week, and event-based prospective memory tasks were calculated based on change/SD of change.
Results
Seven participants were recruited, six with a diagnosis of type 2 diabetes, and one with a prediabetes diagnosis. Four participants met the non-adherence criteria during baseline, were entered into the study, and randomized to one of three staggered baselines in the multiple baseline design. The participants included two females, one male and one individual identified as non-binary. Two of the participants were white, one Asian female and one American Indian or Alaskan Native. Each participant had a diagnosis of type 2 diabetes, with ages ranging from 43 to 52 years of age, and BMI ranging from 27.2 to 37.2 kg/m2. The number of medications prescribed ranged from 1 to 5. During baseline, MEMs caps were provided for multiple medications, with the medication associated with lowest adherence rates determined as the targeted medication. All participants had backward Corsi scores, a measure of short-term visuospatial memory, within the normal range (mean ± 1 SD).42,43
All participants who began the study completed the study, with 100% attendance at scheduled sessions. The objectively measured MEMs based adherence is presented in Figure 1, with 80% adherence indicated by a dotted line. Visual inspection of this data shows no upward trends for any participants during baseline and relative improvements for all participants after introducing EFT. Analysis of data for each participant, summarized in Table 1, showed significant improvement for three of the four participants, but not for participant 411. This may be because while participant 411 had overall baseline adherence results in less than 80%, they were at 100% adherence in week 2, and EFT restored them to levels achieved during baseline. The other significant effect was a significant decelerating trend during baseline for participant 403. Pre to post effect sizes for delay discounting (0.355 ± 0.295 = ES of 1.20), virtual week (0.083 ± 0.104 = ES of 0.80) and prospective memory task (2.75 ± 3.78 = ES of 0.73) were all in the large effect size range,54 suggesting that EFT training was associated with an improvement in prospective memory and delay discounting. The sample size was too small for traditional statistical testing or correlating changes in these variables with a change in medication adherence.
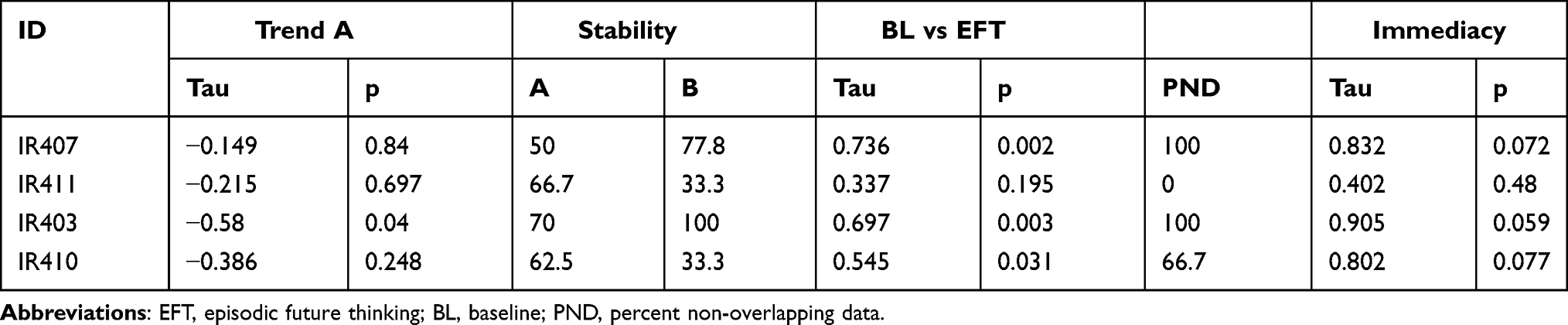 |
Table 1 Analyses Describing Changes for Individual Participants from Baseline to EFT |
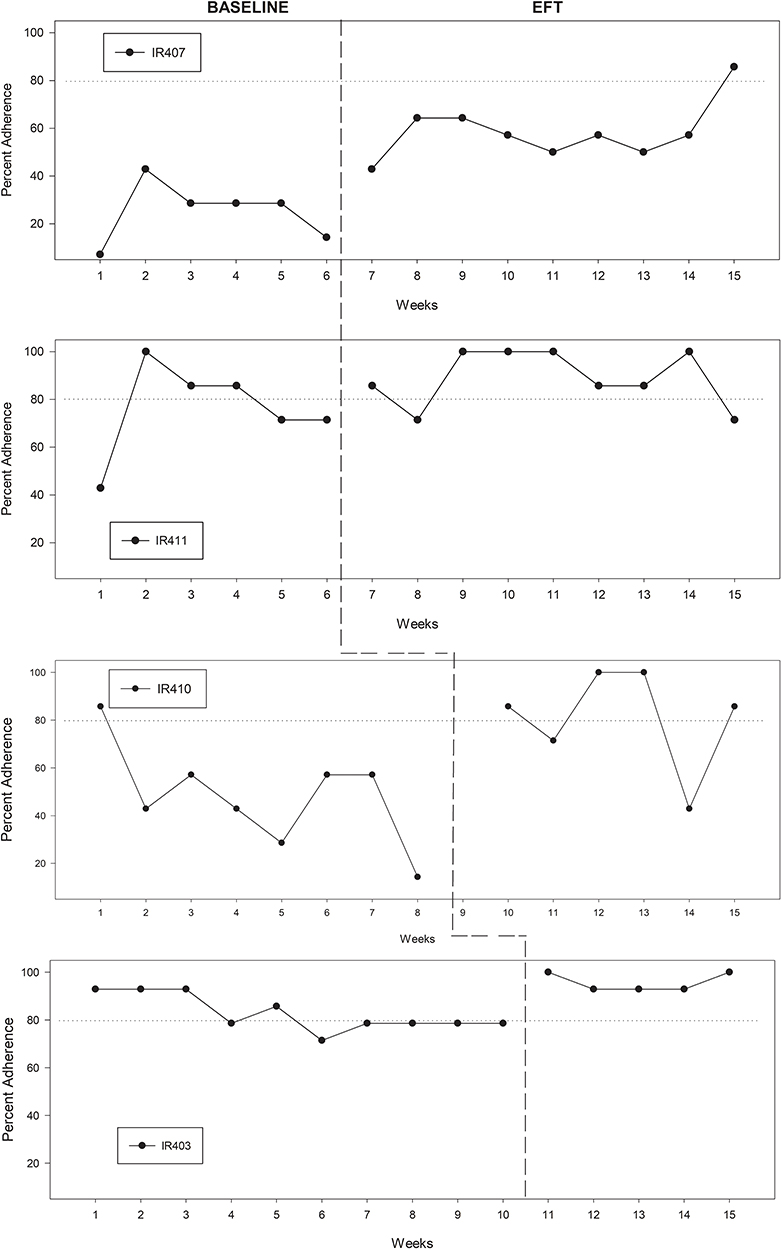 |
Figure 1 Changes in medication adherence for non-adherent participants during baseline and EFT conditions across three staggered baselines. After meeting non-adherence criteria, participants were randomized to different length baselines. The dotted line indicates 80% adherence, which was the treatment goal. Significant differences (p<0.05) between baseline and EFT influenced adherence were observed for patients 407, 403 and 410. |
Consistent with the inspection and analysis of changes for each participant, mixed model analysis showed a significant overall treatment effect, t = 4.01, p = 0.0002, autocorrelation = −0.095, with a between-case standardized mean difference (BC-SMD) of 1.62.
Discussion
These results show a functional relationship between the introduction of EFT and changes in medication adherence for the participants studied with type 2 diabetes who are taking medication to improve glucose homeostasis, blood pressure, or lipid profiles. In addition to changes in medication adherence, changes in two different measures of prospective memory that may mediate the effects of EFT on medication adherence improved were observed for the participants studied. People who are not adherent to medication often report that they forgot to take their medication,6 and while they may prompt themselves at one time of the day to take their medication, they can easily forget when the time comes to take their medication. Interestingly, participants were not chosen because they uniquely reported forgetting, suggesting generalizability of effects to a broader range of patients. In addition, EFT was associated with a reduction in delay discounting, which is independently related to poor medication adherence in people with prediabetes and diabetes.12–16 Less discounting of the future and a more prospective mindset may lead people to engage in current behaviors, such as medication taking, for their future benefits.
Previous research has shown EFT can improve prospective memory using the virtual week task.19 Still, to our knowledge, this is the first time that EFT has been used to improve medication adherence using objectively measured medication adherence. It is possible that for some diseases which can impair working memory, which would include diabetes44 and hypertension,55 EFT may have different effects, as working memory is related to episodic future thinking.28,45 Interestingly, Participant 410 had the lowest Corsi block tapping score of 18, and this person had the lowest baseline medication adherence.
A considerable body of research shows that EFT modifies delay discounting.23,26–29,56 Delay discounting represents a tendency to focus on immediate gratification and discount future events,22 and delay discounting is related to medication adherence in people with prediabetes12 or type 2 diabetes.13 This is generally conceptualized as a failure to engage in positive long-term benefits, but perhaps few immediate benefits. High delay discounting is related to the inability to engage in a wide variety of preventive health behaviors, such as flossing,57 preventive health checkups,58,59 being physically active,12,57 or wearing seatbelts,59 in addition to not taking medication to prevent worsening of prediabetes or type 2 diabetes prediabetes.12,13 Possibly, the effect of EFT on delay discounting may be part of the mechanism for positive changes in adherence observed in participants in this study, in addition to changes in prospective memory.
This study used a multiple baseline, single-case experimental design to test the effects of EFT on four patients with type 2 diabetes who were nonadherent to their medication. This represents an economical and powerful approach to early phase translational research that suggests that improvements in medication adherence were a function of the EFT intervention. Single-case experimental designs provide a strong test of the functional relationship between treatments and outcomes, and are a first step towards development of interventions for medication adherence. The next step would be to conduct a fully powered randomized controlled study to compare the effects of EFT with other interventions, which could include implementation intentions. This study would also measure potential mediators of treatment effects, which could include both prospective memory and delay discounting. This study would also measure changes in the physiological outcomes for the medication taken, which in this case would be improvements in blood pressure and lipids. This would allow generalization of the treatment to people with diabetes and medication nonadherence who met study entrance criteria. If successful, these methods may be generalizable to a wide variety of diseases where people take the medication in pill or tablet form that can be measured using an objective measure of adherence.
Study Limitations
While the results suggest EFT can be an easy to implement, scalable intervention for people with prediabetes or type 2 diabetes who are non-adherent to their medication, the study has several limitations. First, while results showed that all participants exceeded 80% adherence at least for 1 week during treatment, results did not always indicate that EFT enhanced sustained adherence beyond the 80% target used to establish non-adherence. Thus, some participants may still have been rated as relatively non-adherent, even though their adherence improved. Second, while 80% adherence is common in diabetes,48,49 greater adherence may involve further improvements in disease management, and based on the relationship between medication use and physiological changes, higher adherence may be indicated to achieve optimal control of risk factors. Third, given that this study was implemented over 15 weeks, the durability of the EFT effects over more extended periods remains unclear. Fourth, the repeated measures required for a single subject design raises the concern about improvement due to practical effects, rather than a specific effect of EFT. This concern is less for the Virtual Week task, as there are multiple versions of the task, so the person does not repeat the same task. Likewise, in previous studies with persons with prediabetes, we have not shown significant improvement for control groups who do not receive EFT,24,25,60 making this less of a concern in this study. While no decrement in EFT influenced medication-taking over time was observed, assessing longer-term changes when participants are not in weekly contact with a case manager would be worthwhile. Fifth, replicating these results in a larger number of participants is necessary to increase confidence in the findings and begin to generalize these results to other people who are not adherent to their medication intake who have type 2 diabetes. Sixth, numerous aspects of the treatment protocol besides or in addition to EFT may have influenced medication adherence. This may be a particular issue since case management itself, without EFT, may result in an improvement in medication taking. Given that corresponding changes in prospective memory and delay discounting were also observed, these effects are unlikely to be attributed to attentional effects of case management. In the future, utilizing attentional control during the baseline phase may be useful. Indeed, if this research moves to the next step of a randomized, controlled study, an attention placebo group would be necessary to control for case management. Finally, the participants were not chosen because they uniquely reported forgetting to take their medication, which may suggest generalizability of effects to a broader range of patients. Future research could focus on people who report forgetting to take their medication to better understand boundary conditions for this intervention.
Conclusion
This early phase translational study provides experimental evidence that EFT modified medication adherence for the participants studied with type 2 diabetes. In addition, the study provides suggestive evidence that these effects may be mediated by improvements in prospective memory and delay discounting. Randomized, controlled studies are needed to control for attention effects in case management, and to compare with established treatments for medication adherence on medication adherence and disease-specific outcomes, as well as potential mechanisms for change.
Acknowledgments
Appreciation is expressed to Peter Rendell for sharing and assistance with programming the Virtual Week task.
Funding
This research was funded in part by the National Institutes of Health (NIH) Science of Behavior Change Common Fund Program through an award administered by the National Institute of Diabetes and Digestive and Kidney Diseases (1UH2DK109543), awarded to Drs. Epstein and Bickel.
Disclosure
W. K. Bickel is a principal of HealthSim, LLC; BEAM Diagnostics, Inc.; and Red 5 Group, LLC. The other authors do not declare any conflicts of interest with respect to the authorship or publication of this article.
References
1. Tabak AG, Herder C, Rathmann W, Brunner EJ, Kivimaki M. Prediabetes: a high-risk state for diabetes development. Lancet. 2012;379(9833):2279–2290. doi:10.1016/S0140-6736(12)60283-9
2. Iglay K, Hannachi H, Joseph Howie P, et al. Prevalence and co-prevalence of comorbidities among patients with type 2 diabetes mellitus. Curr Med Res Opin. 2016;32(7):1243–1252. doi:10.1185/03007995.2016.1168291
3. Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. 2011;86(4):304–314. doi:10.4065/mcp.2010.0575
4. Miller NH. Compliance with treatment regimens in chronic asymptomatic diseases. Am J Med. 1997;102(2A):43–49. doi:10.1016/s0002-9343(97)00467-1
5. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. doi:10.1056/NEJMra050100
6. Walker EA, Molitch M, Kramer MK, et al. Adherence to preventive medications: predictors and outcomes in the diabetes prevention program. Diabetes Care. 2006;29(9):1997–2002. doi:10.2337/dc06-0454
7. Trawley S, Baptista S, Pouwer F, Speight J. Prospective memory slips are associated with forgetting to take glucose-lowering therapies among adults with diabetes: results from the second diabetes MILES - Australia (MILES-2) survey. Diabet Med. 2019;36(5):569–577. doi:10.1111/dme.13873
8. Zogg JB, Woods SP, Sauceda JA, Wiebe JS, Simoni JM. The role of prospective memory in medication adherence: a review of an emerging literature. J Behav Med. 2012;35(1):47–62. doi:10.1007/s10865-011-9341-9
9. Vedhara K, Wadsworth E, Norman PA, et al. Habitual prospective memory in elderly patients with type 2 diabetes: implications for medication adherence. Psychol Health Med. 2004;9(1):17–27. doi:10.1080/13548500310001637724
10. Bickel WK, Jarmolowicz DP, Mueller ET, Koffarnus MN, Gatchalian KM. Excessive discounting of delayed reinforcers as a trans-disease process contributing to addiction and other disease-related vulnerabilities: emerging evidence. Pharmacol Therapeut. 2012;134(3):287–297. doi:10.1016/j.pharmthera.2012.02.004
11. Odum AL. Delay discounting: I’m a K, you’re a K. J Exp Anal Behav. 2011;96(3):427–439. doi:10.1901/jeab.2011.96-423
12. Epstein LH, Paluch RA, Stein JS, et al. Delay discounting, glycemic regulation and health behaviors in adults with prediabetes. Behav Med. 2020:1–11. doi:10.1080/08964289.2020.1712581
13. Lebeau G, Consoli SM, Le Bouc R, et al. Delay discounting of gains and losses, glycemic control and therapeutic adherence in type 2 diabetes. Behav Processes. 2016;132:42–48. doi:10.1016/j.beproc.2016.09.006
14. Campbell JA, Williams JS, Egede LE. Examining the relationship between delay discounting, delay aversion, diabetes self-care behaviors, and diabetes outcomes in U.S. adults with type 2 diabetes. Diabetes Care. 2021;44(4):893–900. doi:10.2337/dc20-2620
15. Lansing AH, Stanger C, Crochiere R, Carracher A, Budney A. Delay discounting and parental monitoring in adolescents with poorly controlled type 1 diabetes. J Behav Med. 2017;40(6):864–874. doi:10.1007/s10865-017-9856-9
16. Epstein LH, Paluch RA, Stein JS, et al. Role of delay discounting in predicting change in HBA1c for individuals with prediabetes. J Behav Med. 2019;42:851–859. doi:10.1007/s10865-019-00026-3
17. Wieber F, Thurmer JL, Gollwitzer PM. Promoting the translation of intentions into action by implementation intentions: behavioral effects and physiological correlates. Front Hum Neurosci. 2015;9:395. doi:10.3389/fnhum.2015.00395
18. McGrath E, Elliott R, Millar T, Armitage CJ. The role of neuropsychological mechanisms in implementation intentions to reduce alcohol consumption among heavy drinkers: a randomized trial. J Behav Med. 2020;43(4):576–586. doi:10.1007/s10865-019-00078-5
19. Terrett G, Rose NS, Henry JD, et al. The relationship between prospective memory and episodic future thinking in younger and older adulthood. Q J Exp Psychol. 2016;69(2):310–323. doi:10.1080/17470218.2015.1054294
20. Neroni MA, Gamboz N, Brandimonte MA. Does episodic future thinking improve prospective remembering? Conscious Cogn. 2014;23:53–62. doi:10.1016/j.concog.2013.12.001
21. Altgassen M, Rendell PG, Bernhard A, et al. Future thinking improves prospective memory performance and plan enactment in older adults. Q J Exp Psychol. 2015;68(1):192–204. doi:10.1080/17470218.2014.956127
22. Atance CM, O’Neill DK. Episodic future thinking. Trends Cogn Sci. 2001;5(12):533–539. doi:10.1016/S1364-6613(00)01804-0
23. Schacter DL, Benoit RG, Szpunar KK. Episodic future thinking: mechanisms and functions. Curr Opin Behav Sci. 2017;17:41–50. doi:10.1016/j.cobeha.2017.06.002
24. Bickel WK, Stein JS, Paluch RA, et al. Does episodic future thinking repair immediacy bias at home and in the laboratory in patients with prediabetes? Psychosom Med. 2020;82(7):699–707. doi:10.1097/PSY.0000000000000841
25. Stein JS, Craft WH, Paluch RA, et al. Bleak present, bright future: II. Combined effects of episodic future thinking and scarcity on delay discounting in adults at risk for type 2 diabetes. J Behav Med. 2021;44(2):222–230. doi:10.1007/s10865-020-00178-7
26. Daniel TO, Stanton CM, Epstein LH. The future is now: reducing impulsivity and energy intake using episodic future thinking. Psychol Sci. 2013;24(11):2339–2342. doi:10.1177/0956797613488780
27. Daniel TO, Stanton CM, Epstein LH. The future is now: comparing the effect of episodic future thinking on impulsivity in lean and obese individuals. Appetite. 2013;71:120–125. doi:10.1016/j.appet.2013.07.010
28. Snider SE, LaConte SM, Bickel WK. Episodic future thinking: expansion of the temporal window in individuals with alcohol dependence. Alcohol Clin Exp Res. 2016;40(7):1558–1566. doi:10.1111/acer.13112
29. Stein JS, Wilson AG, Koffarnus MN, Daniel TO, Epstein LH, Bickel WK. Unstuck in time: episodic future thinking reduces delay discounting and cigarette smoking. Psychopharmacology. 2016;233(21–22):3771–3778. doi:10.1007/s00213-016-4410-y
30. Epstein LH, Bickel WK, Czajkowski SM, Paluch RA, Moeyaert M, Davidson KW. Single case designs for early phase behavioral translational research in health psychology. Health Psychol. 2021. doi:10.1037/hea0001055
31. Davidson KW, Silverstein M, Cheung K, Paluch RA, Epstein LH. Experimental designs to optimize treatments for individuals_Personalized N-of-1 trials. JAMA Pediatr. 2021;175(4):404. doi:10.1001/jamapediatrics.2020.5801
32. Kratochwill TR, Levin JR. Enhancing the scientific credibility of single-case intervention research: randomization to the rescue. Psychol Methods. 2010;15(2):124–144. doi:10.1037/a0017736
33. Cramer JA, Mattson RH, Prevey ML, Scheyer RD, Ouellette VL. How often is medication taken as prescribed? A novel assessment technique. JAMA. 1989;261(22):3273–3277. doi:10.1001/jama.1989.03420220087032
34. El Alili M, Vrijens B, Demonceau J, Evers SM, Hiligsmann M. A scoping review of studies comparing the medication event monitoring system (MEMS) with alternative methods for measuring medication adherence. Brit Clin Pharmacol. 2016;82(1):268–279. doi:10.1111/bcp.12942
35. Hartman L, Lems WF, Boers M. Outcome measures for adherence data from a medication event monitoring system: a literature review. J Clin Pharm Ther. 2019;44(1):1–5. doi:10.1111/jcpt.12757
36. Rendell PG, Henry JD. A review of virtual week for prospective memory assessment: clinical implications. Brain Impair. 2009;10:14–22. doi:10.1375/brim.10.1.14
37. Rendell PG, Craig FI. Virtual week and actual week: age related differences in prospective memory. Appl Cognitive Psych. 2000;14(7):S43–S63. doi:10.1002/acp.770
38. Kelemen WL, Weinberg WB, Alford HS, Mulvey EK, Kaeochinda KF. Improving the reliability of event-based laboratory tests of prospective memory. Psychonomic Bull Rev. 2006;13(6):1028–1032. doi:10.3758/bf03213920
39. McDaniel MA, Einstein GO. The neuropsychology of prospective memory in normal aging: a componential approach. Neuropsychologia. 2011;49(8):2147–2155. doi:10.1016/j.neuropsychologia.2010.12.029
40. Cheng H, Yang Z, Dong B, et al. Chemotherapy-induced prospective memory impairment in patients with breast cancer. Psycho-Oncology. 2013;22(10):2391–2395. doi:10.1002/pon.3291
41. Woods SP, Weinborn M, Maxwell BR, et al. Event-based prospective memory is independently associated with self-report of medication management in older adults. Aging Ment Health. 2014;18(6):745–753. doi:10.1080/13607863.2013.875126
42. Kessels RPC, van Zandvoort MJ, Postma A, Kappelle LJ, de Haan EH. The Corsi block-tapping task: standardization and normative data. Appl Neuropsychol. 2000;7(4):252–258. doi:10.1207/S15324826AN0704_8
43. Kessels RPC, van den Berg E, Ruis C, Brands AMA. The backward span of the Corsi block-tapping task and its association with the WAIS-III digit span. Assessment. 2008;15(4):426–434. doi:10.1177/1073191108315611
44. Kumari M, Brunner E, Fuhrer R. Mini review: mechanisms by which the metabolic syndrome and diabetes impair memory. J Gerontol A Biol Sci Med Sci. 2000;55(5):B228–8232. doi:10.1093/gerona/55.5.b228
45. Lin H, Epstein LH. Living in the moment: effects of time perspective and emotional valence of episodic thinking on delay discounting. Behav Neurosci. 2014;128(1):12–19. doi:10.1037/A0035705
46. Saggino A, Balsamo M, Grieco A, Cerbone MR, Raviele NN. Corsi’s block-tapping task: standardization and location in factor space with the WAIS-R for two normal samples of older adults. Percept Mot Skills. 2004;98(3):840–848. doi:10.2466/pms.98.3.840-848
47. Deschamps AE, Van Wijngaerden E, Denhaerynck K, De Geest S, Vandamme AM. Use of electronic monitoring induces a 40-day intervention effect in HIV patients. J Acquir Immune Defic Syndr. 2006;43(2):247–248. doi:10.1097/01.qai.0000246034.86135.89
48. Egede LE, Gebregziabher M, Dismuke CE, et al. Medication nonadherence in diabetes: longitudinal effects on costs and potential cost savings from improvement. Diabetes Care. 2012;35(12):2533–2539. doi:10.2337/dc12-0572
49. Williams JL, Walker RJ, Smalls BL, Campbell JA, Egede LE. Effective interventions to improve medication adherence in Type 2 diabetes: a systematic review. Diabetes Manag (Lond). 2014;4(1):29–48. doi:10.2217/dmt.13.62
50. Altgassen M, Kretschmer A, Schnitzspahn KM. Future thinking instructions improve prospective memory performance in adolescents. Child Neuropsychol. 2017;23(5):536–553. doi:10.1080/09297049.2016.1158247
51. Brewer GA, Marsh RL. On the role of episodic future simulation in encoding of prospective memories. Cogn Neurosci. 2010;1(2):81–88. doi:10.1080/17588920903373960
52. Sze YY, Daniel TO, Kilanowski CK, Collins RL, Epstein LH. Web-based and mobile delivery of an episodic future thinking intervention for overweight and obese families: a feasibility study. JMIR mHealth uHealth. 2015;16:e97. doi:10.2196/mhealth.4603
53. Valentine JC, Tanner‐Smith EE, Pustejovsky JE, et al. Between-case standardized mean difference effect size for single-case designs_A primer and tutorial using the scdhlm web application. Campbell Syst Rev. 2016;12(1):1–31.
54. Cohen J. Statistical Power Analysis for the Behavioral Sciences. Lawrence Erlbaum; 1988.
55. Obisesan TO, Obisesan OA, Martins S, et al. High blood pressure, hypertension, and high pulse pressure are associated with poorer cognitive function in persons aged 60 and older: the Third National Health and Nutrition Examination Survey. J Am Geriatr Soc. 2008;56(3):501–509. doi:10.1111/j.1532-5415.2007.01592.x
56. Rung JM, Madden GJ. Experimental reductions of delay discounting and impulsive choice: a systematic review and meta-analysis. J Exp Psychol Gen. 2018;147(9):1349–1381. doi:10.1037/xge0000462
57. Chabris CF, Laibson D, Morris CL, Schuldt JP, Taubinsky D. Individual laboratory-measured discount rates predict field behavior. J Risk Uncertainty. 2008;37(2–3):237–269. doi:10.1007/s11166-008-9053-x
58. Axon RN, Bradford WD, Egan BM. The role of individual time preferences in health behaviors among hypertensive adults: a pilot study. J Am Soc Hypertens. 2009;3(1):35–41. doi:10.1016/j.jash.2008.08.005
59. Bradford WD. The association between individual time preferences and health maintenance habits. Med Decis Making. 2010;30(1):99–112. doi:10.1177/0272989X09342276
60. Mellis AM, Snider SE, Deshpande HU, LaConte SM, Bickel WK. Practicing prospection promotes patience: repeated episodic future thinking cumulatively reduces delay discounting. Drug Alcohol Depend. 2019;204:107507. doi:10.1016/j.drugalcdep.2019.06.010
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.