Back to Journals » Cancer Management and Research » Volume 11
Image-Guided Percutaneous Microwave Ablation Versus Cryoablation For Hepatocellular Carcinoma In High-Risk Locations: Intermediate-Term Results
Authors Hu J, Chen S, Wang X, Lin N, Yang J, Wu S
Received 20 August 2019
Accepted for publication 25 October 2019
Published 18 November 2019 Volume 2019:11 Pages 9801—9811
DOI https://doi.org/10.2147/CMAR.S227961
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Jiahui Hu,1 Sheng Chen,2 Xin Wang,3 Ning Lin,2 Jianchuan Yang,2 Songsong Wu2
1Institute of Medical Information, Chinese Academy of Medical Sciences, Beijing 100020, People’s Republic of China; 2Department of Ultrasonography, Fujian Provincial Hospital, Shengli Clinical Medical College of Fujian Medical University, Fuzhou 350001, People’s Republic of China; 3Department of Oncology, Fuzhou Hospital of Traditional Chinese Medicine, Fujian University of Traditional Chinese Medicine, Fuzhou 350001, People’s Republic of China
Correspondence: Songsong Wu
Department of Ultrasonography, Fujian Provincial Hospital, Shengli Clinical Medical College of Fujian Medical University, Fuzhou 350001, People’s Republic of China
Tel +86-591-88217817
Fax +86-591-8821781
Email [email protected]
Objective: The aims of this study were to compare the clinical outcomes between image-guided percutaneous microwave ablation (MWA) and cryoablation (CRA) in patients with hepatocellular carcinoma (HCC) in high-risk locations and to identify the prognostic factors associated with the two treatment methods.
Methods: This retrospective study was institutional review board approved. A total of 120 patients (88 men and 32 women) with one hundred and thirty-four HCC lesions in high-risk locations from April 2014 to March 2018 were reviewed. Sixty-four patients underwent MWA and 56 patients underwent CRA. Survival, recurrence and complications were compared between the two groups. Effect of changes in key outcomes (i.e., overall survival (OS), recurrence-free survival (RFS) and local tumor progression (LTP)) was statistically analyzed with the log rank test. Univariate and multivariate analysis were performed on clinicopathological variables to identify factors affecting intermediate-term outcomes.
Results: The OS and RFS after MWA were comparable to those of CRA (P =0.141, and P=0.469, respectively). The LTP and major complication in MWA group was higher than those in CRA group (P=0.003, and P=0.039). Univariate analysis showed that age (P=0.007), tumor size (P=0.001), and Child-Turcotte-Pugh (CTP) grade (P=0.003) were risk factors for OS, and multivariate analysis results showed that older age (≥65 years) (P=0.002, HR:3.338, 95% CI:1.928–5.281), 3.0–5.0 cm in size (P<0.001, HR: 3.312, 95% CI: 1.872–4.489) and CTP grade B (P=0.001, HR:3.382, 95% CI: 1.882–5.902) were independently associated with poor OS.
Conclusion: CRA had comparable oncologic outcomes with MWA and could be a safe and effective treatment for HCC in high-risk locations.
Keywords: hepatocellular carcinoma, microwave ablation, cryoablation, outcome, high-risk
Introduction
Hepatocellular carcinoma (HCC) is the sixth most common cancer. With increasing morbidity and mortality, it is the third major reason for cancer-associated deaths worldwide.1–3 The Barcelona Clinic Liver Cancer (BCLC) classification has been recently used to decide the treatment for early-stage HCC; treatment mainly includes surgical resection, liver transplantation, and local ablation therapy.4–6 Nevertheless, many patients lose curative opportunities due to poor physical conditions and donor organ shortage. In terms of treatment, microwave ablation (MWA) has several advantages over radiofrequency ablation (RFA), including higher intratumoral temperatures, shorter duration of operation, and reliance on electrical conductivities.7–9 Despite its proven safety, the comprehensive and secure ablation of cancers in high-risk locations is challenging due to suboptimal conspicuity, insufficient electrode path, and the risk of thermal injury to neighboring organs. Moreover, patients may suffer from mild to moderate pain for several days after an RFA or MWA.
Percutaneous cryoablation (CRA), another local ablation technique, is commonly reported for HCC. CRA has numerous exclusive benefits over RFA, such as a more evidently visible ablative periphery, larger ablative areas, and lesser pain.10 There have been considerable advancements in CRA technology, including the development of percutaneous methodologies and a novel argon-helium cryo-equipment with tinnier probes.11 Guanghua Rong et al have documented that in HCC patients who experienced percutaneous CRA, the occurrence of main obstacles and tumor seeding was as little as 6.3% and 0.78%, respectively.12 Compared to surgical resection or RFA, CRA also revealed equivalently decent results and an even greater local tumor control during the treatment of early-stage HCC.13,14 However, to date, no studies have compared MWA and CRA therapies for HCC, especially of those in high-risk locations.
Thus, the present study aimed to compare the efficacy as well as safety of MWA and CRA for the treatment of HCCs in high-risk locations. Furthermore, the efficacy of CRA as a supplementary treatment for HCC in high-risk locations was investigated for future use in clinical practice.
Methods
Study Design And Patient Selection
In this single-center study, the medical records of all HCC patients admitted between April 2014 and March 2017 were retrospectively reviewed. Around 874 consecutive HCC patients underwent percutaneous ablation treatments, of which 412 patients with HCC in high-risk locations experienced MWA or CRA throughout the duration of the study. Patients were included in the study if: 1) they were diagnosed with HCC by a preoperative core biopsy; 2) the Child class was A or B; 3) the HCC was located in a high-risk location, i.e., less than 1 cm from the abdominal wall and neighboring organs, such as the stomach, colon, gallbladder, kidney, and diaphragm; 4) they had received no treatment before; 5) the tumor number and diameter was less than three and 5 cm, respectively; 6) vascular invasion or extrahepatic metastasis was absent; 7); 8) they had refused a liver transplantation; and 9) if they had chosen to undergo MWA or CRA over liver resection, for reasons including an insufficient postoperative remnant liver, reluctance to undergo liver resection and general anesthesia, and high risk of complications (in case of inaccessible location or old age). Patients were excluded in case of: 1) recurrent HCC; 2) serious comorbidities such as cardiopulmonary and renal insufficiency; 3) severe coagulation disturbance (prothrombin time >25 s, prothrombin activity <40%, and platelet count <50×109/L); and 4) severe infection.
Thus, as shown in Figure 3, 292 patients were excluded, because they did not meet the inclusion criteria. Consequently, 120 patients, including 88 men and 32 women (median age: 57.2 years, range: 28–75 years) with HCC in high-risk locations were incorporated in this study. Around 64 patients (18 females, 46 males; average age: 55.2±7.2 years) who underwent MWA, were categorized into the MWA group and 56 patients (14 females, 42 males; average age: 54.9±11.3 years) who underwent CRA, were categorized into the CRA group. The clinical features of the participants and tumors were recorded.
All experimental protocols conformed to the ICH guidelines for good clinical practices and with the principles of the Declaration of Helsinki. The study was approved by the Ethics Committee of the Fujian Provincial Hospital. All patients signed informed consent forms.
MWA Procedure
The MWA system comprised of a water-cooled microwave apparatus (Kangyou Institute, Nanjing, China) equipped with monopole antennae (16–18 G) that were composed of flexible coaxes; these antennae were connected to a water pump and MW generators (two for each). All patients underwent computed tomography/magnetic resonance imaging and ultrasound sonography (US) before the treatment. The biopsy was performed in 2–3 separate punctures following local anesthesia. Guided by US, the antennae were placed at specific locations on the tumors. Hydrodissection was performed in 21 patients; under US guidance, 5% glucose or 0.9% saline in water was injected through a 21-G needle attached to a 50-mL syringe via a connecting tube, in order to separate the tumor from the surrounding organs.15 In 48 patients, one antenna was inserted less than 1.7 cm into the center of the tumor, while in 16 patients, multiple antennae were inserted up to 1.7 cm (one case shown in Figure 1) or more into the tumor centers. Two antennae were used simultaneously during MWA to achieve a larger ablation zone, and a power output of 50 W for 10 mins was used routinely. The nominal power was set at 300 W/h. The higher temperatures and larger sphere volume could inadvertently burn non-target structures, especially in case of peripheral hepatic tumors abutting to the gastrointestinal tract. After the punctures were completed, propofol and ketamine were administered for anesthesia. If the resulting vapor failed to cover the entire tumor, the microwave radiation time was prolonged to achieve the required temperature. The microwave needle tract was ablated during the removal of the needles. For tumors infiltrated subcutaneously, an ice bag was required to prevent scalding during ablation.
 |
Figure 1 A 46-years old female patient with hepatocellular carcinoma (HCC) located on the second hepatic portal after US-MWA treatment. (A) MRI axial scan in arterial phase before MWA, one nodule was measured in 2.3 × 2.2 × 1.8 cm (arrow); (B) ultrasound -guided microwave ablation for the lesion (small cross); (C) MRI axial scan in delay phase after MWA, an ablation area was showed after three months (arrow), illustrating no viable tumor. |
CRA Procedure
CRA was performed using the Cryo-HitTM (Galilmedical, Israel) with argon gas as the cryogen, by a skilled interventional radiologist, as shown in (Figure 2). Following local anesthesia, cryoprobes were introduced percutaneously into specific lesions using CT assistance; a plain CT scan was first taken to confirm the puncture path and the location of the target lesion. The number of cryoablation sessions required in each patient was mainly determined by the size of the targeted area. Around 1–3 cryoprobes (probe diameter, 2.1–2.4 mm) were used based on the tumor characteristics. In 38 patients, a single probe was inserted less than 2.0 cm into the center of the tumors, while in 18 patients, multiple probes were inserted into the tumors to up to 2.0 cm or more. The cryoprobe was positioned 1 cm away from the other organs surrounding the tumor. Of all patients, about 25.0% received a direct tumor puncture, because the HCCs were present on the liver surface near the abdominal wall, while 39.3% received a non-tumor parenchyma puncture. The cryoprobe was located by a routine CT scan. A dual freeze-thaw cycle was conducted during ablation; each cycle included a freezing period (10 min) and a thawing period (8 min).
 |
Figure 2 A 52-years old male patient with hepatocellular carcinoma (HCC) located abutting the right renal underwent CT-CRA treatment. (A) CT axial scan show a low density nodule before CRA, which was measured in 3.2 × 2.4 × 2.0 cm (arrow) and the nodule located abutting the right renal (red arrow); (B) three cryosurgical needles are inserted into the tumor by CT guided; (C) an ablation area (arrow) with lower density than peripheral liver parenchyma after CRA and right renal (red arrow), which was showed in CT axial image. |
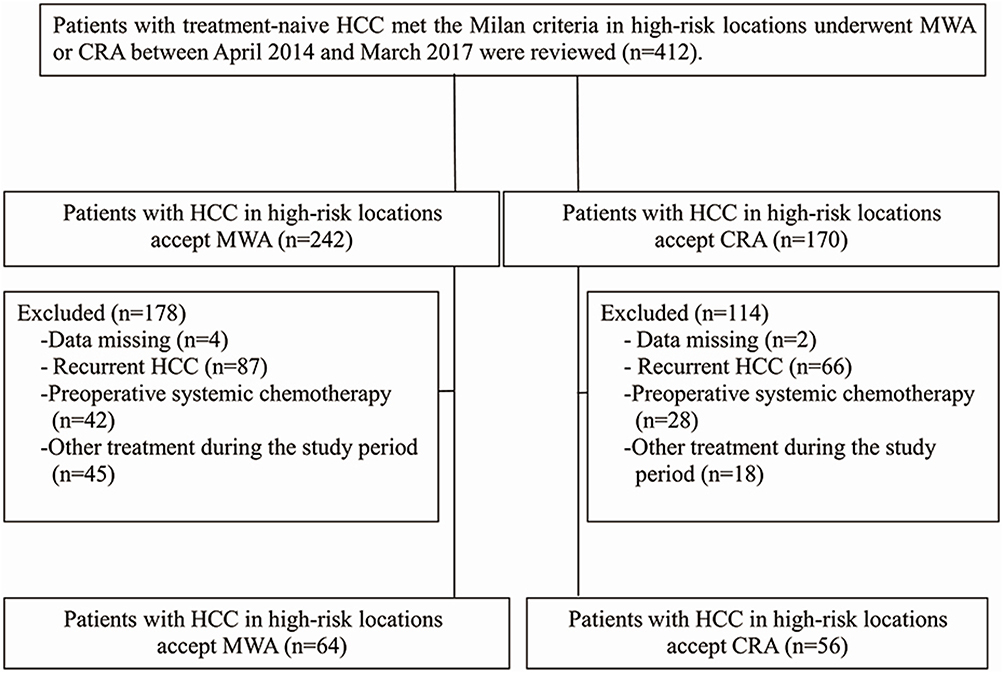 |
Figure 3 Flow diagram shows exclusion criteria in patients with hepatocellular carcinoma in high-risk location. Abbreviations: CRA, cryoablation; MWA, microwave ablation. |
Follow-Up And Endpoints
Follow-up was done at one and three months after the treatment, and thereafter, at an interval of 3–6 months. The follow-up included general physical examination, contrast-enhanced imaging, and laboratory tests for total bilirubin, serum albumin, prothrombin time, tumor marker levels, and so forth. Efficiency of methodology was described as the lack of contrast-enhancement in any part of the mass on imaging after one month from the treatment. The investigation ended with death as well as tumor reappearance [local tumor progression (LTP) and intrahepatic distant recurrence (IDR)]. LTP was determined based on the uneven enhancement patterns around the ablation area observed during imaging. IDR was defined as the occurrence of an uneven enhancement pattern (specific to an intrahepatic lesion) far from the ablation area. Once the tumor recurred, a second ablation was conducted. Overall survival (OS) was calculated as the time from the first ablation treatment to death or the final follow-up. Recurrent-free survival (RFS) was calculated as the time from the first ablation treatment to tumor recurrence or the last follow-up. Complications referred to those syndromes that resulted in high morbidity or disability and led to hospital admission, an increase in the care level, or prolonged the hospitalization time.16
Statistical Analysis
All statistical analyses were conducted using SPSS 21.0 and P<0.05 was considered as statistically significant. The Student’s t-test was used to analyze the data from the MWA and CRA groups. The Wilcoxon signed-rank test and the Pearson’s chi-squared test were used to analyze continuous and absolute variables, respectively. The Kaplan–Meier method was used to assess the OS, RFS, and LTP. A Cox regression model was adopted to inspect the impact of multiple factors on the reappearance and survival rates.
Results
Baseline Characteristics
The clinical features of the participants and tumors are reviewed in Table 1. The mean age, gender, maximum diameter, and tumor number were similar in both groups. The comorbid disorders, metastases, cirrhosis, KPS scores, HBsAg, Child–Pugh (CTP) grade, and adjacent structures were also comparable between the two groups. While serum albumin levels were similar in both groups, the total bilirubin levels and platelet counts were significantly lower in the MWA group than in the CRA group (P=0.002 and P=0.032, respectively). The LTP was significantly greater in the MWA group than in the CRA group (P= 0.039).
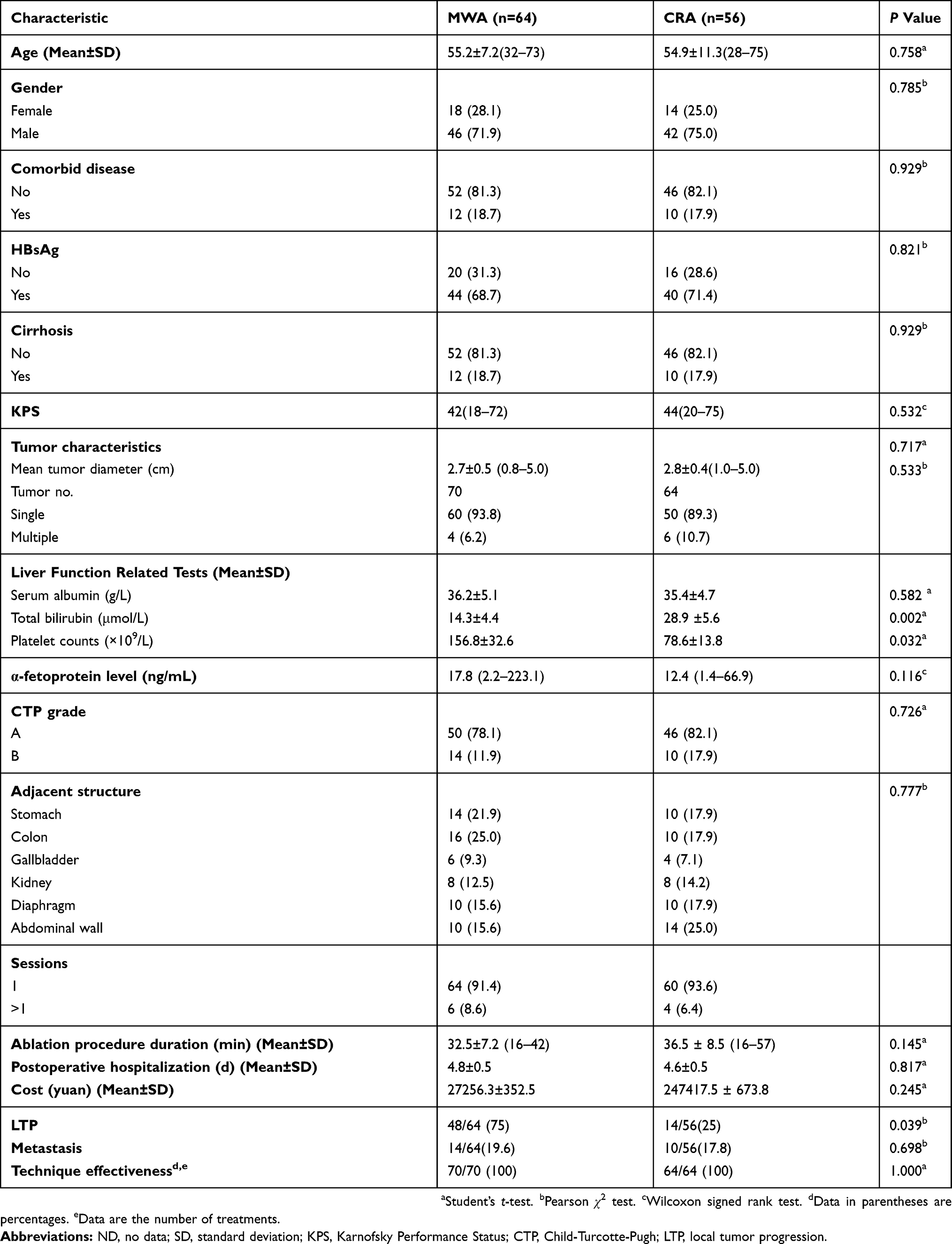 |
Table 1 Baseline Characteristics Of Patients Undergoing MWA And CRA |
Treatment Parameters
The treatment parameters are described in Table 1. Sixty-four patients with 70 tumors underwent 76 treatments sessions in the MWA group; 64 tumors were effectively treated in one MWA session and six tumors in two sessions. Fifty-six patients with 64 tumors underwent 68 treatments sessions in the CRA group; 60 tumors were effectively treated in one CRA session and four tumors in two sessions. The surgical time, anticipated blood loss, cost, and hospitalization periods were similar in both groups.
Midterm Survival And Recurrence Outcome
The average follow-up duration was 19.9 months (range: 3.3–46.2 months). In the MWA group, the mortality rate was 18.8% (12/64 patients), with tumor progression as the primary cause of casualty. In this group, 12 patients had comorbid disorders, mainly including hypertension and/or diabetes. In the CRA group, the mortality rate was 14.3% (8/56 patients), and the primary cause of fatality was local or systemic HCC development. During follow-up imaging, it was observed that a 100% method success rate was accomplished in both groups (MWA: 70 of 70 treatments; CRA: 68 of 68 treatments). Following treatment, about 75% (n=48) and 25% (n=14) of the patients in the MWA and CRA groups, respectively, developed LTP lesions. Distant metastasis was observed in 19.6% patients (n=14) following MWA and in 17.8% patients (n=10) following CRA. The key outcomes (ie, OS, RFS, and LTP) were investigated using the log rank test (Figure 4). The 1-, 3-, and 5-year OS rates were 85.8%, 63.5%, and 63.5%, respectively in the MWA group and 92.0%, 87.4%, and 74.9%, respectively in the CRA group; thus, presenting no substantial differences. The 1-, 3-, and 5-year RFS rates were 77.8%, 49.0%, and 49.0%, respectively in the MWA group and 81.4%, 58.5%, and 46.8%, respectively in the CRA group; again, no substantial differences were observed. The 3-, 6-, 9-, and 12-month LTP rates were 3.1%, 6.3%, 9.4%, and 15.9%, respectively for the MWA group and 0%, 0%, 3.7%, and 19.0%, respectively for the CRA group; significant differences were observed (P=0.039; acquired from the log rank test for complete curves).
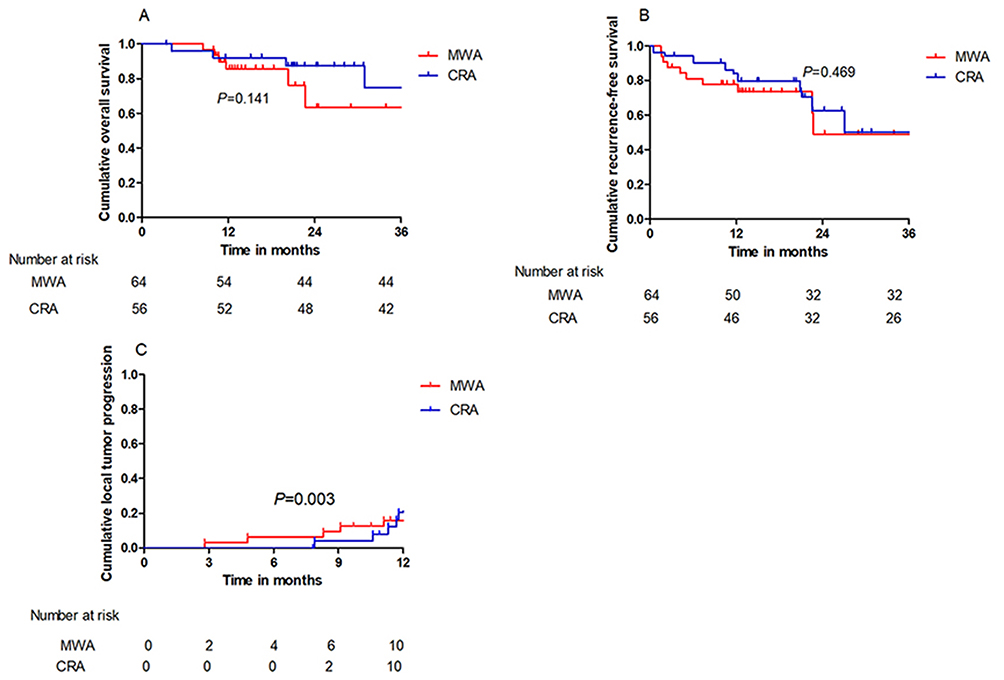 |
Figure 4 (A) The 1-, 3- and 5-year overall survival (OS) rates in the MWA group and CRA group were 85.8%,63.5% and 63.5% and 92.0%, 87.4% and 74.9%, respectively, showing no significant statistical difference (P=0.302). (B) The 1-, 3- and 5-year recurrence-free survival (RFS) rates in the MWA group and CRA group were 77.8%, 49.0% and 49.0% and 81.4%, 58.5% and 46.8%, respectively, showing no significant statistical difference (P=0.775). (C) The 3-, 6-, 9- and 12-month LTP rate of MWA group and CRA group were 3.1%, 6.3%, 9.4% and 15.9% and 0%, 0%, 3.7% and 19.0%, respectively, showing significant statistical difference (P =0.039). |
Univariate And Multivariate Evaluations
Univariate and multivariate logistic regression analyses were performed to identify the predictors affecting the intermediate-term outcomes in the patients. Univariate analysis indicated substantial differences in the OS rates, which were dependent on the age, tumor size, and the CTP grade. Multivariate analysis indicated that age (≥65 years), tumor size (3.0–5.0 cm), and the CTP grade (B) were independently associated with a poor OS (Table 2). Univariate analysis indicated significant differences in the RFS rates, which were dependent on the number of sessions and the tumor size and number. Multivariate analysis revealed that tumor size (≥3 cm), multiple tumors, and multiple sessions were independently associated with a poor RFS (Table 3).
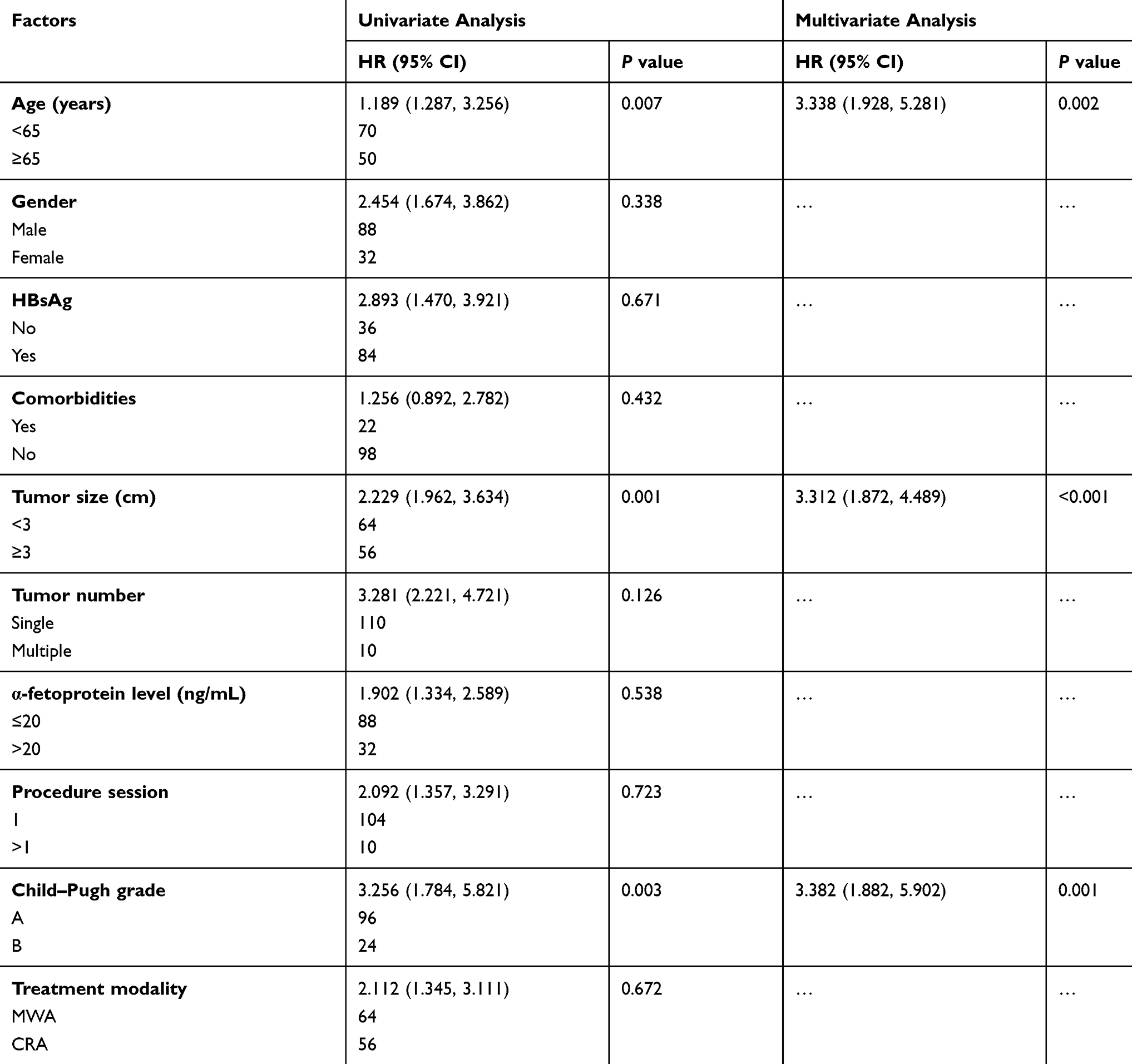 |
Table 2 Factors Associated With Overall Survival |
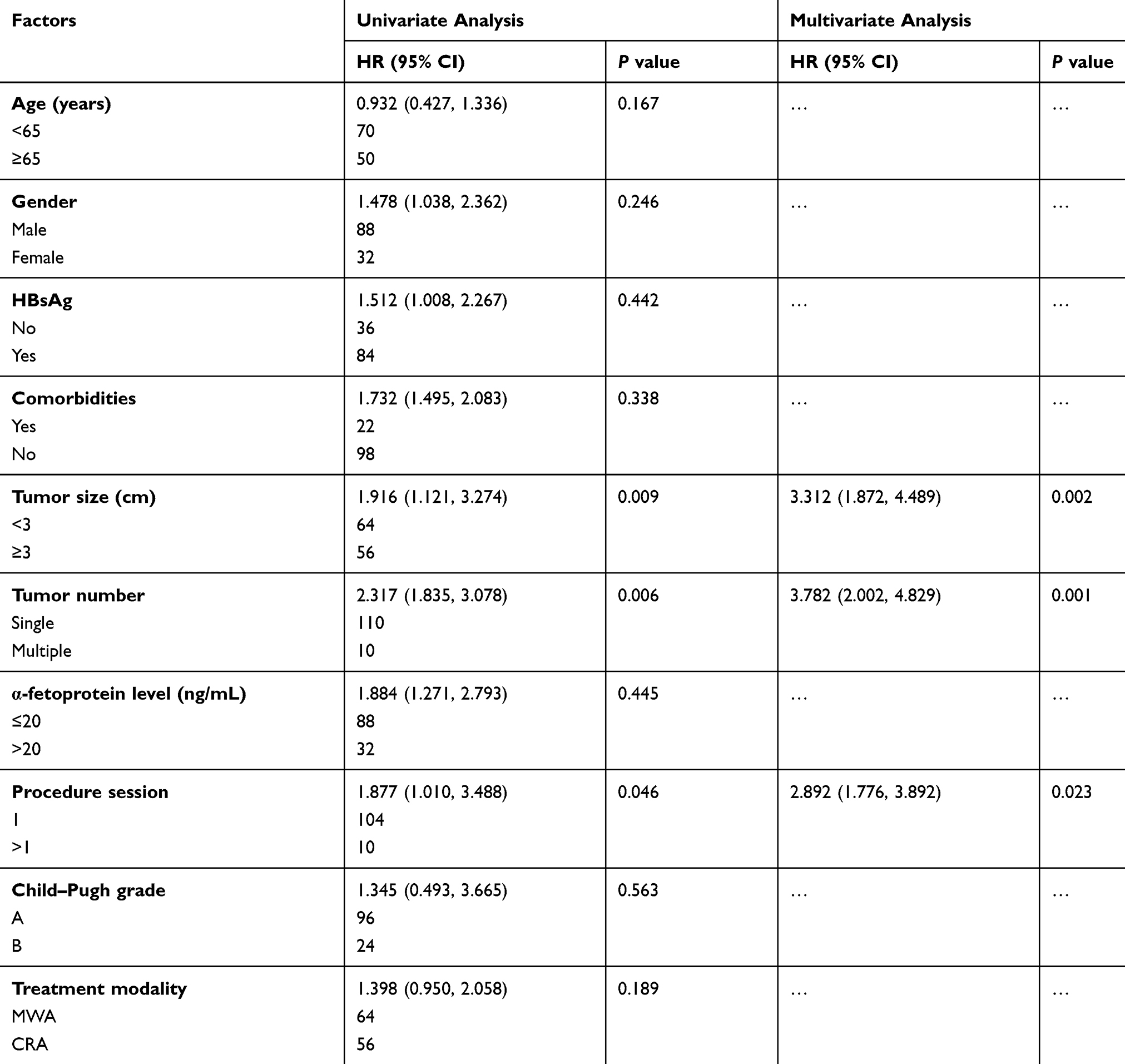 |
Table 3 Factors Associated With Tumor Recurrence |
Complications
There were no treatment-associated fatalities; the complications following ablation are summarized in Table 4. There were four major complications in the MWA group. One patient developed liver abscesses, while one developed tumor seeding. Two patients developed pleural effusion that required drainage. In the CRA group, no major complications were observed. Therefore, the major complication occurrence rate was greater in the MWA group (4 of 64; 6.3%) than in the CRA group (0 of 56; 0%) (P=0.039). The primary minor complications, including postoperative pain and fever, were higher in the MWA group than in the CRA group (P=0.001).
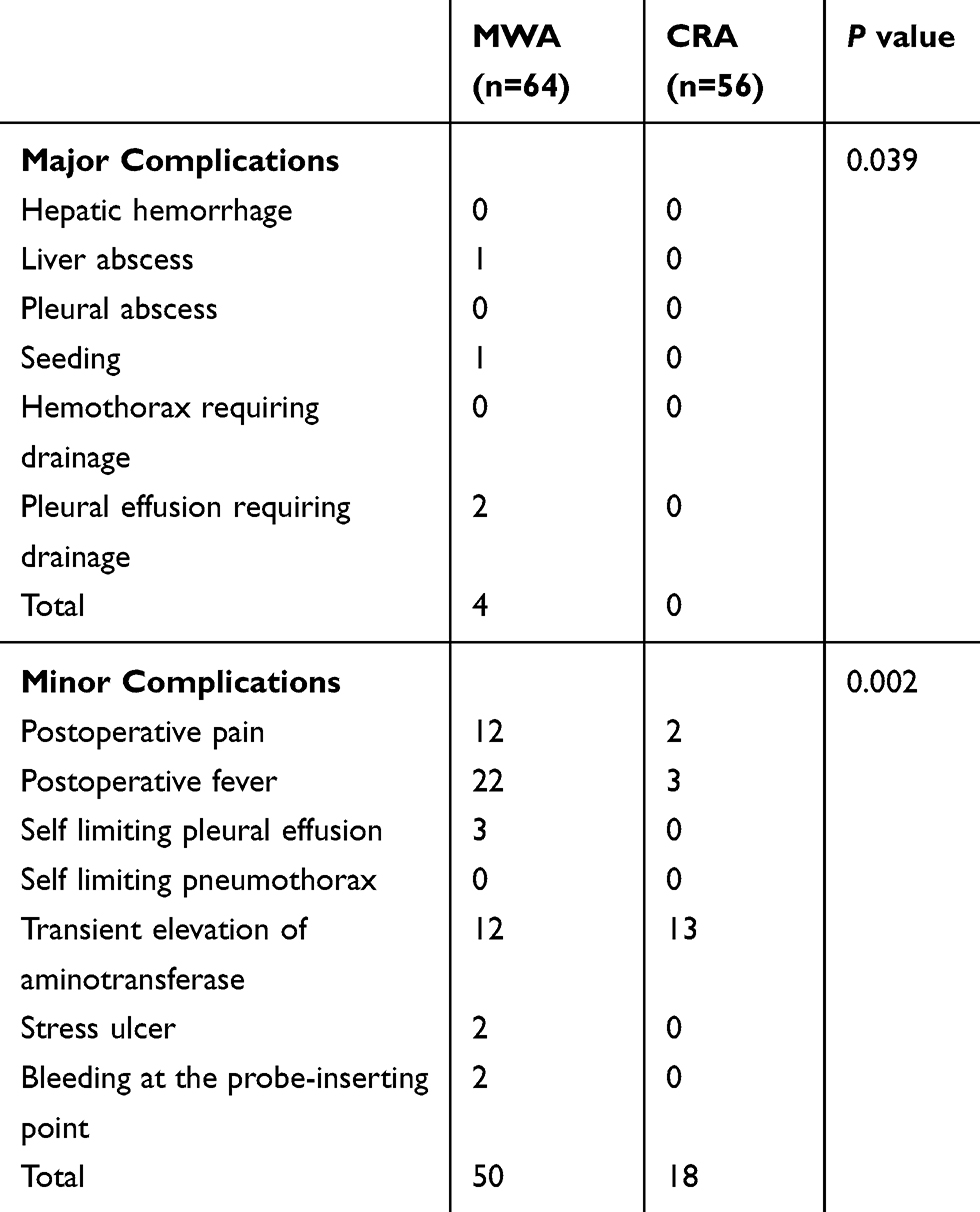 |
Table 4 Summary Of The Complications After Ablation |
Discussion
Ei S et al have reported that CRA is a safe and an effective method, which compared to RFA or MWA, provides a significantly more improved local control for the treatment of primary HCCs (>2 cm).17 Chunping Wang et al published a multicenter RCT study, comparing the outcomes between percutaneous CRA and RFA for the treatment of HCC (<4 cm in diameter);18 while the RFS and OS rates were comparable between the two groups, the LTP was greater in the MWA group than in the CRA group. CRA has greater benefits over RFA and MWA, such as lesser post-ablation pain and a clearer boundary.19,20 However, whether lesions in high-risk locations affect the complete ablation rate and oncological outcomes, and which ablation technique is more suitable for their treatment remains unclear. The objective of the present study was to compare the oncological outcomes of HCCs in high-risk locations between the MWA and CRA groups.
High-power microwave equipment, with a generator frequency of 2.45 GHz and an internal fluid cooling system, provides a larger spherical ablation zone within shorter duration.21–23 MWA mechanism involves applying high-speed molecular friction that generates a persistently high temperature; this causes protein denaturation and coagulative necrosis of the tumor cells, resulting in the in situ inactivation of the tumor. In the treatment of early-stage HCC, MWA achieves a lower LTP rate than RFA; however, using MWA in the treatment of HCCs in high-risk locations, such as those abutting the diaphragm, gastrointestinal tract, renal, and so on, is challenging,24–26 because a limited ablation volume is generated in order to avoid damage to the surrounding organs. Filippiadis et al.27 examined 26 patients with 36 HCC lesions in challenging locations, who underwent CT-guided percutaneous MWA; they found that the 2- and 5-year OS rates were 92.3% and 72.1%, respectively, with a technical efficiency rate of 100%. Smolock AR et al.24 reported that 55 peripheral hepatic tumors adjoining the diaphragm were treated by MWA supported by artificial ascites; the LTP rate and postoperative pain was lesser than that in the non-artificial ascites group. Zhang D et al assessed the sequestering influence of a thermosensitive hydrogel throughout percutaneous MWA of the liver tissue adjoining the stomach; they suggested that thermometry needles can protect the nearby stomach wall from damage during the MWA procedure.26 It is necessary to confirm the outcomes of MWA for HCC in high-risk locations.
Percutaneous cryoablation for cancer cells involves the following mechanisms: 1) intracellular ice development, 2) solute-solvent shifts that trigger cell dehydration, and 3) rupture and small-vessel destruction resulting in hypoxia. With the advent of newer technologies, including a minimally invasive percutaneous approach and a newer and safer generation of cryoablation devices, the effectiveness and safety of CRA treatment for HCC has improved.11,18,28,29 In case of CRA for lesions in high-risk locations, damage to the surrounding organs is not a concern and the ablation edges are clearly visible. Thus, percutaneous CRA is suitable for the treatment of HCCs, especially those in high-risk locations. Guanghua Rong et al reported that the cumulative 5-year LTP and OS rates of 866 HCC patients, who met the Milan criteria and underwent CRA, were 24.2% and 59.5%, respectively. Advanced age, multiple lesions, and HCC family history were found to be the independent and significantly negative predictors of the OS rates.12
In this study, the OS and RFS rates were analyzed among 120 patients experiencing CRA or MWA. The clinical effectiveness of MWA and CRA in the treatment of HCC in high-risk locations was compared. After matching the approximate liver function, CRA showed survival outcomes and reappearance rates similar to those for MWA. However, the LTP following CRA was significantly lower than that after MWA. The advantage of CRA over MWA for high-risk HCC includes a clearer ablation margin and a larger ablation sphere (accomplished with a combination of multiple probes). These results suggested that a 5–10 mm safe margin can decrease the LTP rate. The 5-year OS rate in the CRA group was 74.9%, which is higher than the rates reported for other ablation treatments.30,31 Multivariate analyses indicated that an older age (>65 years), tumor size (3.0–5.0 cm), and the CTP grade (B) were significant prognostic factors for poor OS in CRA and MWA treatments. Additionally, compared to MWA, CRA was generally well-tolerated, had manageable adverse events, and correlated with the ablative margin volume and site. It may usually be self-limited. There were no major complications in the CRA group and the post-ablation pain was lower than that in the MWA group, suggesting that HCC patients who undergo CRA have a higher quality of life following ablation. Both MWA can CRA can improve a patient’s immune system and have other beneficial treatment effects. Following the local ablation treatment, a dramatic increase in the CD4+ cells, CD4+/CD8+ ratio, and NK cells was observed in the HCC patients, while the CD8+ cell number had significantly decreased.32
Our study has several limitations. Firstly, the sample size was small, which may have decreased the statistical power in comparative evaluations; thus, several relations may have remained unidentified. Secondly, because all patients in our cohort were treated at a single medical center, referral bias could not be avoided completely. Thirdly, the accomplishment of ablation was evaluated comparing radiographic outcomes with the pathological margin-free status. Hence, in spite of intermediary follow-up, identification of ablation failures with radiographic techniques may take longer. Finally, inconsistencies in the imaging modalities in the single center may cause a difference in the ablation procedure and may change the LTP risk.
In conclusion, the clinical outcomes of CRA and MWA in the treatment of HCC were comparable. These treatments may be safe and effectual for lesions in high-risk anatomical locations. Furthermore, CRA was associated with lesser instances of postoperative fever and lesser pain, as compared to MWA.
Acknowledgment
This work has been supported by the Basic Scientific Research Fund of Chinese Academy of Medical Sciences (“Study on Semantic Annotation Method for Knowledge Discovery Based on Chinese Electronic Medical Records”, Grant No.2018PT33005). This work was supported by grants from the Young and Middle-aged Talents Training Project of Health and Family Planning Committee of Fujian Province (No. 2017-ZQN-10).
Disclosure
The authors state that there are no conflict of interests regarding the publication of this paper.
References
1. Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391(10127):1301–1314. doi:10.1016/S0140-6736(18)30010-2
2. Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64(1):9–29. doi:10.3322/caac.21208
3. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.v68.6
4. Piñero F, Poniachik J, Ridruejo E, Silva M. Hepatocellular carcinoma in Latin America: diagnosis and treatment challenges. World J Gastroenterol. 2018;24(37):4224–4229. doi:10.3748/wjg.v24.i37.4224
5. Ng KK, Cheung TT, Wong TC, et al. Long-term survival comparison between primary transplant and upfront curative treatment with salvage transplant for early stage hepatocellular carcinoma. Asian J Surg. 2019;42(2):433–442. doi:10.1016/j.asjsur.2018.08.008
6. Dimitroulis D, Damaskos C, Valsami S, et al. From diagnosis to treatment of hepatocellular carcinoma: an epidemic problem for both developed and developing world. World J Gastroenterol. 2017;23(29):5282–5294. doi:10.3748/wjg.v23.i29.5282
7. Medhat E, Abdel AA, Nabeel M, et al. Value of microwave ablation in treatment of large lesions of hepatocellular carcinoma. J Dig Dis. 2015;16(8):456–463. doi:10.1111/1751-2980.12259
8. Han Y, Shao N, Xi X, Hao X. Use of microwave ablation in the treatment of patients with multiple primary malignant tumors. Thorac Cancer. 2017;8(4):365–371. doi:10.1111/tca.2017.8.issue-4
9. Yu J, Liang P. Status and advancement of microwave ablation in China. Int J Hyperthermia. 2017;33(3):278–287.
10. Littrup PJ, Aoun HD, Adam B, Krycia M, Prus M, Shields A. Percutaneous cryoablation of hepatic tumors: long-term experience of a large U.S. series. Abdom Radiol. 2016;41(4):767–780. doi:10.1007/s00261-016-0687-x
11. Hu KQ. Advances in clinical application of cryoablation therapy for hepatocellular carcinoma and metastatic liver tumor. J Clin Gastroenterol. 2014;48(10):830–836. doi:10.1097/MCG.0000000000000201
12. Rong G, Bai W, Dong Z, et al. Long-term outcomes of percutaneous cryoablation for patients with hepatocellular carcinoma within Milan criteria. PLoS One. 2015;10(4):e0123065. doi:10.1371/journal.pone.0123065
13. Lo GH. Is cryoablation really more effective than radiofrequency ablation in hepatocellular carcinoma. Hepatology. 2016;63(6):2061. doi:10.1002/hep.28005
14. Xu J, Noda C, Erickson A, et al. Radiofrequency ablation vs. cryoablation for localized hepatocellular carcinoma: a propensity-matched population study. Anticancer Res. 2018;38(11):6381–6386. doi:10.21873/anticanres.12997
15. Liu CH, Yu CY, Chang WC, et al. Computed tomographic-guided percutaneous radiofrequency ablation with hydrodissection of hepatic malignancies in the subcapsular location: evaluation of safety and technical efficacy. J Chin Med Assoc. 2016;79(2):93–100. doi:10.1016/j.jcma.2015.07.013
16. Cardella JF, Kundu S, Miller DL, Millward SF, Sacks D. Society of interventional radiology clinical practice guidelines. J Vasc Interv Radiol. 2009;20(7 Suppl):S189–S191. doi:10.1016/j.jvir.2009.04.035
17. Ei S, Hibi T, Tanabe M, et al. Cryoablation provides superior local control of primary hepatocellular carcinomas of >2 cm compared with radiofrequency ablation and microwave coagulation therapy: an underestimated tool in the toolbox. Ann Surg Oncol. 2015;22(4):1294–1300. doi:10.1245/s10434-014-4114-7
18. Wang C, Wang H, Yang W, et al. Multicenter randomized controlled trial of percutaneous cryoablation versus radiofrequency ablation in hepatocellular carcinoma. Hepatology. 2015;61(5):1579–1590. doi:10.1002/hep.27548
19. Pusceddu C, Melis L, Ballicu N, et al. Percutaneous microwave ablation under CT guidance for hepatocellular carcinoma: a single institutional experience. J Gastrointest Cancer. 2018;49(3):295–301. doi:10.1007/s12029-017-9951-8
20. Cui W, Fan W, Huang K, et al. Large hepatocellular carcinomas: treatment with transarterial chemoembolization alone or in combination with percutaneous cryoablation. Int J Hyperthermia. 2018;35(1):239–245. doi:10.1080/02656736.2018.1493235
21. Filippiadis DK, Gkizas C, Chrysofos M, et al. Percutaneous microwave ablation of renal cell carcinoma using a high power microwave system: focus upon safety and efficacy. Int J Hyperthermia. 2018;34(7):1077–1081. doi:10.1080/02656736.2017.1408147
22. Gao Y, Wang Y, Duan Y, et al. 915MHz microwave ablation with high output power in in vivo porcine spleens. Eur J Radiol. 2010;75(1):87–90. doi:10.1016/j.ejrad.2009.03.009
23. Knavel EM, Hinshaw JL, Lubner MG, et al. High-powered gas-cooled microwave ablation: shaft cooling creates an effective stick function without altering the ablation zone. AJR Am J Roentgenol. 2012;198(3):W260–W265. doi:10.2214/AJR.11.6503
24. Smolock AR, Lubner MG, Ziemlewicz TJ, et al. Microwave ablation of hepatic tumors abutting the diaphragm is safe and effective. AJR Am J Roentgenol. 2015;204(1):197–203. doi:10.2214/AJR.14.12879
25. Zhang H, Fan W, Huang Z, Zhang L, Song Z, Qi H. [Computed tomography-guided percutaneous microwave ablation for diaphragm-abutting liver tumors: assessments of safety and short-term therapeutic efficacies]. Zhonghua Yi Xue Za Zhi. 2014;94(17):1313–1317.
26. Zhang D, Xie D, Wei X, et al. Microwave ablation of the liver abutting the stomach: insulating effect of a chitosan-based thermosensitive hydrogel. Int J Hyperthermia. 2014;30(2):126–133. doi:10.3109/02656736.2013.874048
27. Filippiadis DK, Spiliopoulos S, Konstantos C, et al. Computed tomography-guided percutaneous microwave ablation of hepatocellular carcinoma in challenging locations: safety and efficacy of high-power microwave platforms. Int J Hyperthermia. 2018;34(6):863–869. doi:10.1080/02656736.2017.1370728
28. Orlacchio A, Bazzocchi G, Pastorelli D, et al. Percutaneous cryoablation of small hepatocellular carcinoma with US guidance and CT monitoring: initial experience. Cardiovasc Intervent Radiol. 2008;31(3):587–594. doi:10.1007/s00270-008-9293-9
29. Hsieh YC, Limquiaco JL, Lin CC, Chen WT, Lin SM. Radiofrequency ablation following artificial ascites and pleural effusion creation may improve outcomes for hepatocellular carcinoma in high-risk locations. Abdom Radiol. 2019;44(3):1141–1151. doi:10.1007/s00261-018-1831-6
30. Kim GM, Won JY, Kim MD, et al. Cryoablation of hepatocellular carcinoma with high-risk for percutaneous ablation: safety and efficacy. Cardiovasc Intervent Radiol. 2016;39(10):1447–1454. doi:10.1007/s00270-016-1384-4
31. Wong SN, Lin CJ, Lin CC, Chen WT, Cua IH, Lin SM. Combined percutaneous radiofrequency ablation and ethanol injection for hepatocellular carcinoma in high-risk locations. AJR Am J Roentgenol. 2008;190(3):W187–W195. doi:10.2214/AJR.07.2537
32. Abdo J, Cornell DL, Mittal SK, et al. Immunotherapy plus cryotherapy: potential augmented abscopal effect for advanced cancers. Front Oncol. 2018;8:85–88. doi:10.3389/fonc.2018.00085
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.