Back to Journals » Patient Preference and Adherence » Volume 17
Illustrating How to Use the Validated Alsayed_v1 Tools to Improve Medical Care: A Particular Reference to the Global Initiative for Asthma 2022 Recommendations
Authors Alsayed AR ![]()
Received 2 February 2023
Accepted for publication 7 April 2023
Published 28 April 2023 Volume 2023:17 Pages 1161—1179
DOI https://doi.org/10.2147/PPA.S403239
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ahmad R Alsayed
Department of Clinical Pharmacy and Therapeutics, Faculty of Pharmacy, Applied Science Private University, Amman, 11937, Jordan
Correspondence: Ahmad R Alsayed, (PharmD, MSc, PhD in Therapeutics and Precision Medicine), Department of Clinical Pharmacy and Therapeutics, Faculty of Pharmacy, Applied Science Private University, Amman, Jordan, Tel +962786770778, Email [email protected]; [email protected]
Purpose: The current research aimed to illustrate a real case using the validated Alsayed_v1 tools as tutorial training to improve the knowledge and skills of healthcare practitioners in the clinical problem-solving process necessary to implement medical and pharmaceutical care.
Patients and Methods: The Alsayed_v1 instruments consist of principal components: data collection, assessment of treatments, the medical problem oriented plan (MPOP), as well as a care plan and patient education.
Results: This study illustrated a real case of asthma patient using the validated Alsayed_v1 tools. These validated and clinically tested tools provide a coding system for the MPOP that permits easy documentation with an open hierarchical structure where higher levels are broad and lower levels are particular, and the possibility to enter free text. The section dedicated to treatment assessments is intended to synthesize patient information to facilitate the identification of the MPOPs. Effective management requires the development of a partnership between the patient with asthma (or the patient’s caregivers) and his healthcare professional(s). This partnership aims to allow the patient to control his condition with guidance from the healthcare professional(s), discuss and agree on therapy goals, and develop a personalized, written, self-management asthma care plan.
Conclusion: By implementing Alsayed_v1 tools, the clinical practitioner can actively give the best practice for optimal patient outcomes.
Keywords: asthma, Alsayed_v1 tools, MPOP, medical care, patient outcome
Introduction
Over the years, pharmacists’ role has expanded from traditional dispensing to patient-focused pharmaceutical care practice.1,2 Pharmacists are now working collaboratively with other healthcare practitioners as a neighborhood of the healthcare team to provide optimized patient care services in hospitals and various clinical settings.3–7 As pharmacists are now required to possess closer contact with patients,8 the general public naturally expects them to handle challenges competently and in the best interests of their patients.9 Numerous studies have found that pharmacists’ participation in pharmaceutical care services improves patients’ health outcomes by recognizing and preventing treatment-related problems in various disorders10–17 and saves health care expenses.18–21
Among the primary responsibilities of clinical pharmacy and pharmaceutical care practitioners are the detection, prevention, and resolution of medical issues.7 Pharmacist interventions are pivotal in developing new pharmaceutical care services and increasing knowledge about the types and frequencies of medical problems.7 Clinical pharmacists must utilize a systematic documentation and classification system when reporting medical problems.22–26
Pharmaceutical care and clinical problem-solving have a recognized utility as a method that lowers medication errors and patient harm.27,28 Nevertheless, health care practitioners in general, including pharmacists, receive minimal formal education throughout their college years on how to gather patient data, assess this data, including drugs, establish and implement the patient’s care plan, educate the patient, and offer proper follow-up.27,28 This may be attributed to the lack of awareness and vague understanding of who is responsible for providing this service.29,30
Our recent interventional study found that the tutorial improved pharmacy students’ decision-making skills. The intervention also taught students teamwork, peer assessment, communication, and critical thinking.31 The novel Alsayed_v1 tools introduced in a recent paper were applied to actual patient cases and were validated.31 The tools received favorable feedback from users. The Alsayed_v1 tools include three main parts: the assessment of treatments, the medical problem-oriented plan (MPOP) classification system, and the care plan.31 The term MPOP was defined in our previous research9 as “an interventional plan directed to a specific medical problem or event involving patient treatment to achieve the optimum outcomes for a certain patient”.
Therefore, this study aims to illustrate a real case using the validated Alsayed_v1 tool as tutorial training to improve the knowledge and skills of healthcare practitioners and pharmacy /medical students in the clinical problem-solving process that is necessary to implement medical and pharmaceutical care. A real asthma case was selected to apply the tools with a particular reference to evidence-based medicine using the updated 2022 version of the Global Initiative for Asthma (GINA).
Materials and Methods
Data Collection and Assessment
In this study, the Alsayed_v1 tools were used.9 We provided the method in light of our recent two published studies using our related templates.9,31 The template pertaining to the assessment of therapies was thought to be crucial since it aids in analyzing patient data for the presence of medical problems and aids in providing a suitable plan.31
Regarding the data collection, seven parts were included: demographic data, current issues, medical problems, patient history, treatments, tests, and special situations.
In addition to the updated related guidelines, the following websites were utilized throughout the tutorial: Lexicomp’s Drug Information, UpToDate, accesspharmacy.mhmedical.com, https://online.epocrates.com, and www.medscape.com. Practitioners are advised to consult a minimum of two sources to gather the relevant information. Practitioners must also possess decision-making and professional communication skills.
The practitioner identified the necessary data in the appropriate sources, documented the patient’s data, evaluated the distinct components with documentation, and evaluated the coherence between the recommended and the patient’s therapeutic indications. Effectiveness was determined by comparing the patient’s therapy to the most recent evidence-based clinical practice guideline recommendations and achieving treatment objectives (treatment goals). The medication’s safety was evaluated by examining the patient’s symptoms and medical records for any indications of probable adverse reactions, contraindications, or precautionary measures. Possible medication safety issues were also evaluated by determining whether or not the patient was at risk but not receiving prophylaxis. The adequacy of the dosage regimen was determined by comparing doses to evidence-based guidelines and recommendations or by consulting drug information resources such as Lexicomp’s Drug Information. The clinical characteristics of the patient were considered when determining the dosing regimen. Utilizing the UpToDate drug interactions tool, clinically significant drug-drug interactions were identified.
The patient’s knowledge and adherence were evaluated and recorded. Poor, average, or appropriate levels of knowledge of the disease and non-pharmacological and pharmacological treatments were documented. Assessing and documenting adherence to non-pharmacological and pharmacological therapies are also necessary. Primary and secondary non-adherence to pharmacological treatment can be distinguished. Primary non-adherence occurs when a patient has been prescribed a new medicine but fails to obtain it (or a suitable alternative) within a reasonable period of time. Secondary non-adherence occurs when a patient fills a prescription but does not take the medication as prescribed. Non-adherence can also be characterized based on the patient’s intent to take treatment (intentional versus unintentional non-adherence).9 Due to the various underlying causes, each type of non-adherence must be addressed separately. It is possible to document the reasons for insufficient knowledge and non-adherence.
Cost-effectiveness was also documented, including questioning the patient about cost. Furthermore, the monitoring parameters and their costs should also be considered.
After completing this analysis step for one drug, all of the patient’s medications must be assessed prior to the synthesis step (MPOP tool).
MPOP, Care Plan, Patient Education, and Follow Up
All medical problems reported in the assessment step were pooled and then classified according to their shared components: Indication, Effectiveness, Safety, Patient, and Miscellaneous, according to the MPOP tool.9
The care plan template was created to incorporate the detected MPOP as well as a free-text field for inserting additional intervention, monitoring, and follow-up details. Each care plan table was tailored to a specific patient’s disease/condition. Appropriate systematic patient education was provided directly to the patient, with a particular follow-up schedule to evaluate the outcome of the care plan.
Case Summary
A 20-year-old male with a history of uncontrolled persistent asthma presented to his primary care physician with complaints of shortness of breath (SOB), poor exercise tolerance, nighttime awakening, and the need for frequent use of his quick-relief asthma medication. The clinical pharmacist was asked to recognize and address the possible factors contributing to this patient’s uncontrolled asthma and to develop a plan for better long-term control of his asthma symptoms using the novel validated “Alsayed_v1” tools.9,31 Changes in the patient’s pharmacotherapeutic regimen for long-term asthma control were needed.
Ethical approval was attained from a medical center in Amman, Jordan (2021-IRB-1-1). The patient’s informed consent was obtained to participate in and publish the study, including anonymized responses. This study complies with the Declaration of Helsinki.
Results
Data Collection and Assessment
1. Demographic Data
- Who is the patient? -
- Age: 20 years
- Gender: Male
- Education: Bachelor’s student
- Occupation: NA
- Phone no. NA
- Dr name: -
Day and Date: 9 October 2022
2. Current Issues
Day and Date: 9 October 2022
Time: 16.00
CC: “The dust is bothering me.”
HPI:
- Location: Lower respiratory tract
- Characteristic of symptoms: cough and SOB
- Timing (onset, duration, frequency):
He reports being awakened by a cough at night once a week during the last 4 weeks. His cough and SOB occur during at least 3 days per week in the last 4 weeks.
- Severity: needs further investigations
- Factors:
Aggravating factors:
The patient states he especially becomes short of breath when he exercises (although he admits that his SOB is not always brought on by exercise and sometimes occurs when he is not actively exercising).
The family has one cat, which may be a possible trigger of his asthma symptoms.
Alleviating factors:
Taking his medications
- Environment: Dust environment; both father and brother are smokers
- Other symptoms: NA
- Differential diagnosis: well-known asthma case
Review of Systems (ROS)
Denies fever, chills, headache, eye discharge or redness, rhinorrhea, sneezing, sputum production, chest pain, palpitations, dizziness, or confusion.
Physical Examination (PE)
Gen: Well-developed, well-nourished male
HEENT: Mild oral thrush is present on the tongue and buccal mucosa
Neck/Lymph Nodes: Supple; no lymphadenopathy or thyromegaly
Lungs/Thorax: No intercostal retractions or accessory muscle use with respirations; good air movement; mild expiratory wheezes bilaterally
CV: RRR; no MRG
Abd: Soft, NTND; (+) BS
Ext: Normal ROM; periphisal pulses 3+; no CCE
Neuro: A&O × 3. Cranial nerves II–XII are grossly intact. No focal weakness or loss of sensation.
Day and Date: 9 October 2022
3. Medical Problems
Table 1 shows the medical problems the patient has.
 |
Table 1 Medical Problems Part of Data Collection |
4. Patient History
- Surgeries: No previous intubations history
- Hospitalization: Once in the last year due to asthma exacerbation and treated with oral corticosteroids (OCS); one visit to the emergency department (ED) during the previous 6 months and treated with OCS.
- Vaccination: NA
- Allergies: No known drug allergies (NKDA)
- Family history (FH): Mother, 45 years old with hypertension (HTN) and allergic rhinitis; (nonsmoker); father, 51 years old (smoker) with HTN, type 2 diabetes mellitus, and some food allergy; brother, age 15, healthy (smoker); sister, age 6, healthy (suspected asthma).
- Social history (SH): No alcohol or tobacco use, single, not sexually active, lives at home with his parents (his father is a teacher) and one cat.
5. Treatments
Table 2 shows the medications and other treatments taken by the patient.
 |
Table 2 Treatments Part of Data Collection |
6. Tests
Day and Date: 9 October 2022
Vital signs:
BP 110/68, HR 78, RR 16, T 37°C; Wt 58 kg, Ht 170 cm
Lab tests:
Na 136 mEq/L, K 3.6 mEq/L (at risk for hypokalemia due to frequent Albuterol use), Cl 98 mEq/L, CO2 27 mEq/L, BUN 18 mg/dL, serum creatinine 0.6 mg/dL, Glu 95 mg/dL, Hgb 15 g/dL, Hct 42%, Plts 192 × 103/mm3, WBC 6.0 × 103/mm3, PMNs 56%. Bands 1%, Eosinophils, Basophils 2%, Lymphocytes 33%, Monocytes 5%.
Other tests:
His morning peak expiratory flows (PEF) have been running around 270 L/min (personal best = 400 L/min) over the last several weeks. PEF = 68% (yellow zone; caution).
7. Special Situations
- Pediatric, geriatric, pregnancy, breast-feeding, ethnicity: None
- Age 12+ according to GINA32
- Limitations (NPO, bedridden, inability to swallow): None
- Renal impairment: Normal kidney function (Table 3)
- Hepatic impairment: No
- Allergies: No known drug allergy (NKDA)
- Sensitive issues/barriers to communication: No
- Abuse: No
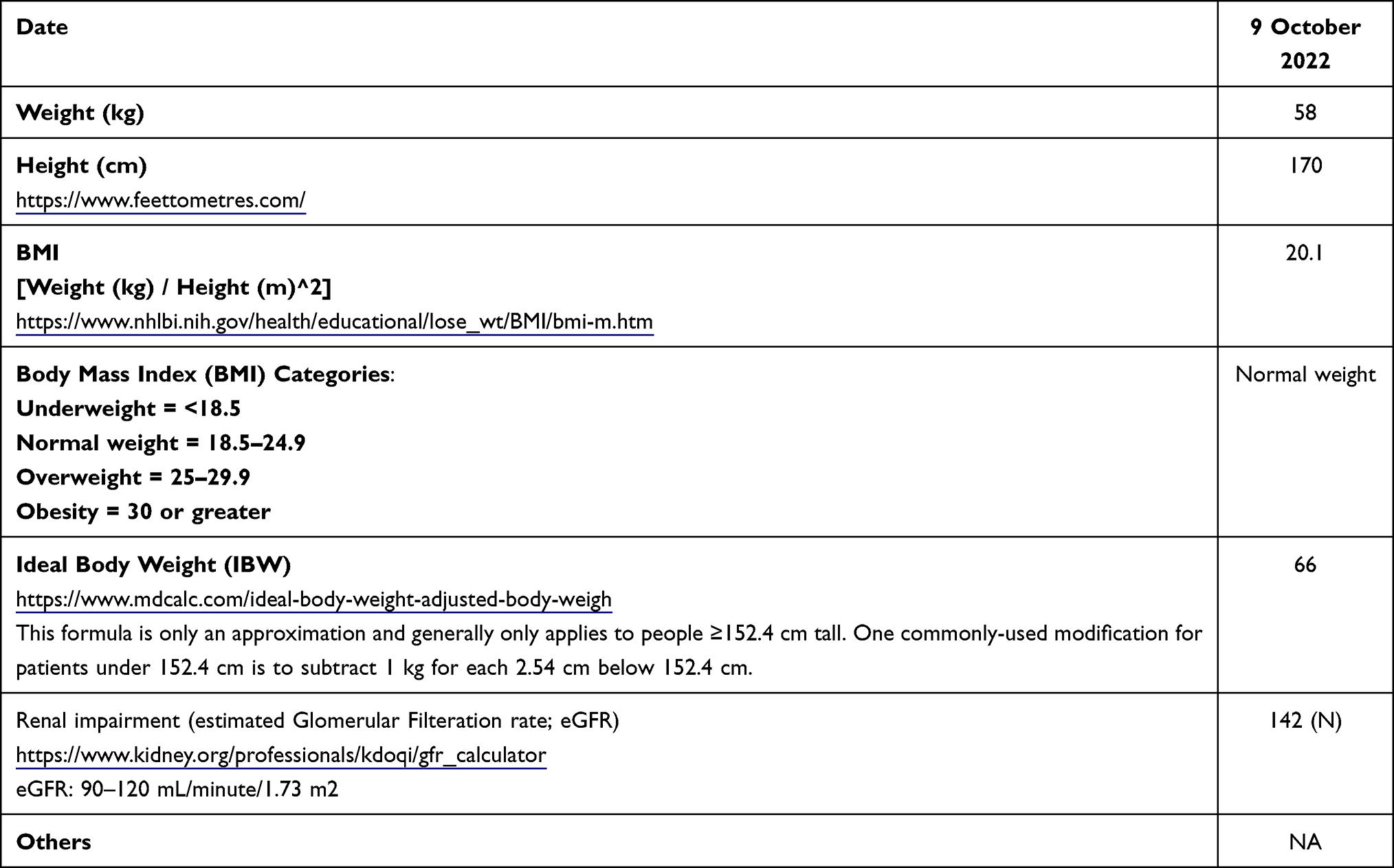 |
Table 3 Basic Calculations |
Day and Date: 9 October 2022
Basic Calculations and Assessment of Medications
Table 3 shows some basic calculations, and Table 4 and Table 5 detail the assessment of his medications.
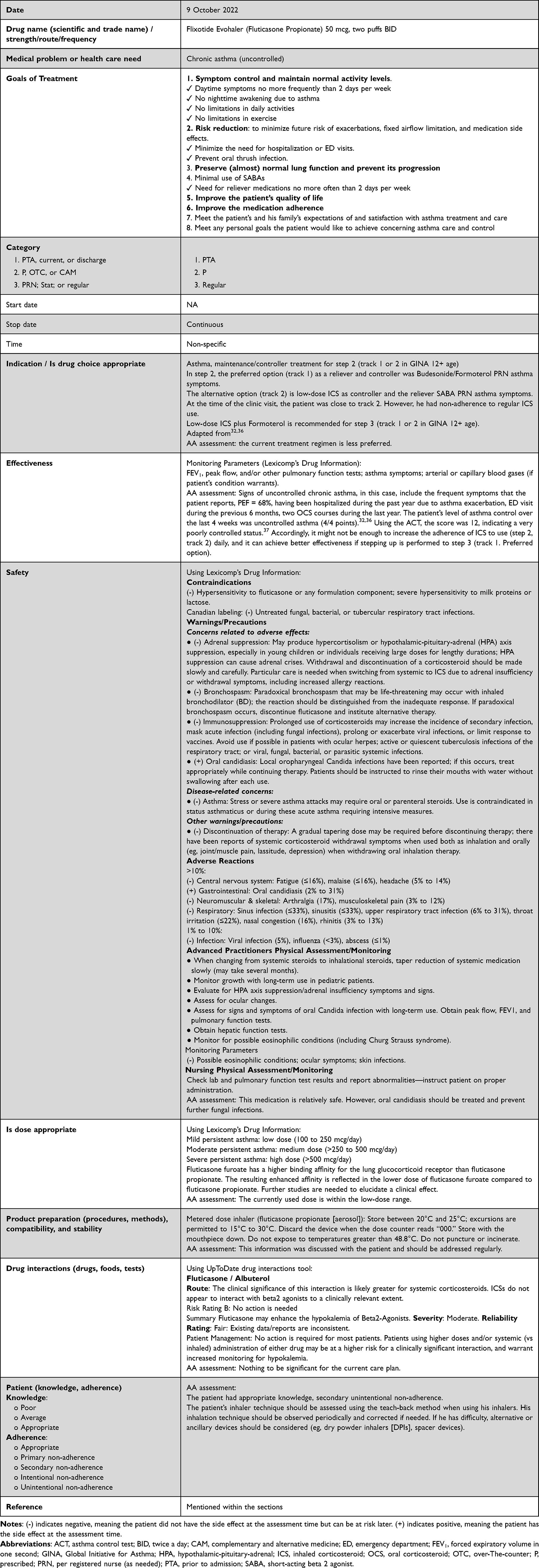 |
Table 4 Assessment for Fluticasone |
 |
Table 5 Assessment for Albuterol |
MPOP and Care Plan
Table 6 and Table 7 represent the patient’s care plans for chronic asthma and oral thrush infection, including the related MPOP.
 |
Table 6 The Care Plan for the Chronic Asthma |
 |
Table 7 The Care Plan for the Oral Thrush Infection |
Patient Education, Care Plan Implementation, and Follow Up
The care plan and patient education aim to provide the patient with a management plan at home when his peak flow readings go below the Green Zone. Following the care plan will help the patient gain control of his asthma symptoms if they worsen (Table 8). The instructions were given to the patient in Arabic, his mother language.
 |
Table 8 Patient Education for Chronic Asthma for the Included Patient |
Discussion
The current research aimed to illustrate a real case using the validated Alsayed_v1 tools as tutorial training to improve the knowledge and skills of healthcare practitioners, pharmacy, and medical students in the clinical problem-solving process necessary to implement medical and pharmaceutical care.
The created classification system (MPOP tool) was intended to be user-friendly, applicable, and valuable in many healthcare settings (general practice, medical centers, hospitals, community pharmacies, etc.), as well as for research and education. The MPOP classification system is an open hierarchical structure with five broad categories at the higher levels and increasing specificity at the lower ones. Incorporating interventions into the classification system is crucial, particularly in medical and pharmaceutical care research, where the type of advice should be documented to evaluate the service’s value and impact. It saves practitioners time in keying in the correct interventions. However, this MPOP application user can enter some information in the free text section.9
The section dedicated to treatment assessments is intended to synthesize patient information to facilitate the identification of the MPOPs. The absence of an evaluation component is a major limitation in some categorization systems.
The pharmacist’s position has changed substantially, and they will likely provide pharmaceutical care services. In most hospitals, pharmacists have not previously collected medication histories.33 This may be due to poor process knowledge, lack of awareness, unclear understanding of who is responsible for pharmaceutical care services, and shifting obligations to other healthcare professionals.34,35 Lack of expertise, skills, and awareness hindered pharmaceutical care service implementation. This study developed an innovative learning tool to help pharmacy and medical students and medical practitioners understand clinical problem-solving.
The ongoing project seeks to evaluate the implementation and user satisfaction of Alsayed_v1 tools in daily practice and analyze data obtained from hospitals, medical centers, community pharmacies, and other primary care settings. In addition, these templates are part of a larger project managed and owned by the corresponding author, including a website and a mobile application to provide medical care support (https://www.asami-draacare.com).
Effective management requires the development of a partnership between the patient with asthma (or the patient’s caregivers) and his healthcare professional(s). The goal of this partnership is to provide the patient with the ability to control his condition with guidance from the healthcare professional(s), discuss and agree on therapy goals, and develop a personalized, written, self-management asthma care plan.32
While initial diagnosis and treatment of asthma typically begin with primary care providers, there are situations when specialists should become involved in managing the asthmatic patient. Education can be conducted by PharmD, pharmacist, respiratory therapist, or nurse to ensure an understanding of the technique and to stress the importance of adherence to new respiratory devices.
Primary care providers should consider referral of the asthmatic patient to pulmonology and/or allergy/immunology practices for any of the following: poorly controlled or severe asthma despite appropriate treatment and compliance, presence of comorbidities that may affect response to treatment (eg, nasal polyps, COPD, etc), additional diagnostic tests are needed (eg, skin allergy testing, bronchoscopy, etc.), asthma diagnosis is uncertain, or occurrence of a life-threatening asthma exacerbation. Referral to appropriate specialists should also be considered when a psychiatric or psychosocial condition impacts the patient’s ability to comply with appropriate asthma treatment.
The involvement of a social worker may also be considered when a patient is routinely and unwillingly exposed to environmental triggers which negatively impact their condition, such as cigarette smoke, cockroaches, fumes, etc. A social worker can also help ensure that the patient’s family can afford the recommended medications.
Conclusion
This paper applied the validated Alsayed v1 tools to an actual patient situation. These instruments consist of principal components: data collection, assessment of treatments, the MPOP, as well as a care plan and patient education. Incorporating interventions into the classification system is crucial, particularly in pharmaceutical and medical research, where the type of recommendations must be documented to evaluate the service’s value and impact, and it saves practitioners time from manually typing the appropriate interventions. These validated, and clinically tested tools provide a coding system for the MPOP that permits easy documentation with an open hierarchical structure where higher levels are broad and lower levels are particular, and the possibility to enter free text. By implementing Alsayed_v1 tools, the clinical practitioner can actively give the best practice for optimal patient outcomes.
Disclosure
The author report no conflicts of interest in this work.
References
1. Bradley C. The future role of pharmacists in primary care. Br J General Practice. 2009;59(569):891–892. doi:10.3399/bjgp09X473105
2. Toklu HZ, Hussain AJ. The changing face of pharmacy practice and the need for a new model of pharmacy education. Journal of Young Pharmacists: JYP. 2013;5(2):38–40. doi:10.1016/j.jyp.2012.09.001
3. Roughead E, Semple SJ, Vitry AJ. Pharmaceutical care services: a systematic review of published studies, 1990 to 2003, examining effectiveness in improving patient outcomes. Int J Pharmacy Practice. 2005;13(1):53–70.
4. Hepler CD, Therapy D. Clinical pharmacy, pharmaceutical care, and the quality of drug therapy. Pharmacotherapy. 2004;24(11):1491–1498. doi:10.1592/phco.24.16.1491.50950
5. Aburuz S. The case for evidence-based pharmaceutical care. Res Social Adm Pharm. 2015;11(3):e146–7. doi:10.1016/j.sapharm.2009.06.001
6. Khader H, Hasoun LZ, Alsayed A, Abu-Samak M. Potentially inappropriate medications use and its associated factors among geriatric patients: a cross-sectional study based on 2019 Beers Criteria. Pharmacia. 2021;68(4):789–795. doi:10.3897/pharmacia.68.e73597
7. Alsayed AR, Halloush S, Hasoun L, et al. Perspectives of the community in the developing countries toward telemedicine and pharmaceutical care during the COVID-19 pandemic. Pharm Pract (Granada). 2022;20(1):2618. doi:10.18549/PharmPract.2022.1.2618
8. Kruijtbosch M, Göttgens-Jansen W, Floor-Schreudering A, van Leeuwen E, Bouvy ML. Moral dilemmas of community pharmacists: a narrative study. J Article Int J Clin Pharm. 2018;40(1):74–83. doi:10.1007/s11096-017-0561-0
9. Alsayed AR, Al-Dulaimi A, Alnatour D, Awajan D, Alshammari B. Validation of an assessment, medical problem-oriented plan, and care plan tools for demonstrating the clinical pharmacist’s activities. Saudi Pharm J. 2022;30(10):1464–1472. doi:10.1016/j.jsps.2022.07.007
10. Shao H, Chen G, Zhu C, et al. Effect of pharmaceutical care on clinical outcomes of outpatients with type 2 diabetes mellitus. Patient Preference and Adherence. 2017;11:897. doi:10.2147/PPA.S92533
11. Parajuli DR, Franzon J, McKinnon RA, Shakib S, Clark RA. Role of the pharmacist for improving self-care and outcomes in heart failure. Current Heart Failure Reports. 2017;14(2):78–86. doi:10.1007/s11897-017-0323-2
12. Shanmugam S, Varughese J, Nair MAS, et al. Pharmaceutical care for asthma patients: a Developing Country’s Experience. Journal of Research in Pharmacy Practice. 2012;1(2):66. doi:10.4103/2279-042X.108373
13. Cazarim M, de Freitas O, Penaforte TR, Achcar A, Pereira L. Impact assessment of pharmaceutical care in the management of hypertension and coronary risk factors after discharge. PLoS One. 2016;11(6):e0155204. doi:10.1371/journal.pone.0155204
14. Liekweg A, Westfeld M, Braun M, et al. Pharmaceutical care for patients with breast and ovarian cancer. Supportive Care in Cancer: Official Journal of the Multinational Association of Supportive Care in Cancer. 2012;20(11):2669–2677. doi:10.1007/s00520-012-1385-z
15. Kousar R, Murtaza G, Azhar S, Khan SA, LJRiS C, Pharmacy A. Randomized controlled trials covering pharmaceutical care and medicines management: a systematic review of literature. Research in Social & Administrative Pharmacy: RSAP. 2018;14(6):521–539. doi:10.1016/j.sapharm.2017.06.008
16. Poudel RS, Piryani RM, Shrestha S, Prajapati A. Benefit of hospital pharmacy intervention on the current status of dry powder inhaler technique in patients with asthma and COPD: a study from the Central Development Region, Nepal. Integrated Pharmacy Research & Practice. 2017;6:7. doi:10.2147/IPRP.S119202
17. Berenguer B, La Casa C, de la Matta MJ, Martín-Calero MJ. Pharmaceutical care: past, present and future. Curr Pharm Des. 2004;10(31):3931–3946. doi:10.2174/1381612043382521
18. Obreli-Neto PR, Guidoni CM, de Oliveira Baldoni A, et al. Effect of a 36-month pharmaceutical care program on pharmacotherapy adherence in elderly diabetic and hypertensive patients. International Journal of Clinical Pharmacy. 2011;33(4):642–649. doi:10.1007/s11096-011-9518-x
19. Clifford RM, Davis WA, Batty KT, Davis TM. Effect of a pharmaceutical care program on vascular risk factors in type 2 diabetes: the Fremantle Diabetes Study. Diabetes Care. 2005;28(4):771–776. doi:10.2337/diacare.28.4.771
20. Bunting BA, Cranor CW. The Asheville Project: long-term clinical, humanistic, and economic outcomes of a community-based medication therapy management program for asthma. Journal of the American Pharmacists Association: JAPhA. 2006;46(2):133–147. doi:10.1331/154434506776180658
21. Cranor CW, Bunting BA, Christensen DB. The Asheville Project: long-term clinical and economic outcomes of a community pharmacy diabetes care program. J Am Pharm Assoc. 2003;43(2):173–184. doi:10.1331/108658003321480713
22. Cipolle RJS, Morley L. P. Pharmaceutical Care Practice: The Patient-Centered Approach to Medication Management.
23. Chia HS, Ho JA, Lim BD. Pharmacist review and its impact on Singapore nursing homes. Singapore Med J. 2015;56(9):493–501. doi:10.11622/smedj.2015133
24. Hohmann C, Eickhoff C, Klotz JM, Schulz M, Radziwill R. Development of a classification system for drug-related problems in the hospital setting (APS-Doc) and assessment of the inter-rater reliability. J Clin Pharm Ther. 2012;37(3):276–281. doi:10.1111/j.1365-2710.2011.01281.x
25. AbuRuz SM, Bulatova NR, Yousef AM. Validation of a comprehensive classification tool for treatment-related problems. Pharm World Sci. 2006;28(4):222–232.
26. Hepler CD, Strand LM. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm. 1990;47(3):533–543.
27. Hammour KA, Farha RA, Basheti I. Hospital pharmacy medication reconciliation practice in Jordan: perceptions and barriers. J Eval Clin Pract. 2016;22(6):932–937. doi:10.1111/jep.12565
28. Ramjaun A, Sudarshan M, Patakfalvi L, Tamblyn R, Meguerditchian AN. Educating medical trainees on medication reconciliation: a systematic review. BMC Med Educ. 2015;15:33. doi:10.1186/s12909-015-0306-5
29. Boockvar KS, Carlson LaCorte H, Giambanco V, Fridman B, Siu A. Medication reconciliation for reducing drug-discrepancy adverse events. Am J Geriatr Pharmacother. 2006;4(3):236–243. doi:10.1016/j.amjopharm.2006.09.003
30. van Sluisveld N, Zegers M, Natsch S, Wollersheim H. Medication reconciliation at hospital admission and discharge: insufficient knowledge, unclear task reallocation and lack of collaboration as major barriers to medication safety. BMC Health Serv Res. 2012;12:170. doi:10.1186/1472-6963-12-170
31. Alsayed AR, Hasoun L, Al-Dulaimi A, et al. Evaluation of the effectiveness of educational medical informatics tutorial on improving pharmacy students’ knowledge and skills about the clinical problem-solving process. Pharm Pract (Granada). 2022;20(2):2652. doi:10.18549/PharmPract.2022.2.2652
32. GINA. Global Initiative for Asthma (GINA): strategy for asthma management and prevention. Available from: https://ginasthma.org/reports/.
33. Bond C, Raehl CL, Franke TJ, Therapy D. Clinical pharmacy services, hospital pharmacy staffing, and medication errors in United States hospitals. Pharmacotherapy. 2002;22(2):134–147. doi:10.1592/phco.22.3.134.33551
34. Boockvar KS, LaCorte HC, Giambanco V, Fridman B, Siu AJ. Medication reconciliation for reducing drug-discrepancy adverse events. The American Journal of Geriatric Pharmacotherapy. 2006;4(3):236–243. doi:10.1016/j.amjopharm.2006.09.003
35. van Sluisveld N, Zegers M, Natsch S, Wollersheim HJ. Medication reconciliation at hospital admission and discharge: insufficient knowledge, unclear task reallocation and lack of collaboration as major barriers to medication safety. Int J Pharm Practice. 2012;12(1):1–12.
36. Reddel HK, Bacharier LB, Bateman ED, et al. Global Initiative for Asthma Strategy 2021: executive Summary and Rationale for Key Changes. J Allergy Clin Immunol Pract. 2022;10(1s):S1–s18. doi:10.1016/j.jaip.2021.10.001
37. Kosinski M, Turner-Bowker D, Fortin E. Asthma Control Test [TM]: a User’s Guide. QualityMetric Incorporated. 2004;1:465.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.