Back to Journals » Patient Preference and Adherence » Volume 17
Illness Perceptions, Cognitions, and Beliefs on COPD Patients’ Adherence to Treatment – A Systematic Review
Authors Poletti V, Pagnini F ![]() , Banfi P
, Banfi P ![]() , Volpato E
, Volpato E ![]()
Received 5 April 2023
Accepted for publication 7 June 2023
Published 28 July 2023 Volume 2023:17 Pages 1845—1866
DOI https://doi.org/10.2147/PPA.S412136
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Video abstract of "IP, cognitions, beliefs and adherence in COPD treatment" [ID 412136].
Views: 67
Valentina Poletti,1 Francesco Pagnini,1 Paolo Banfi,2 Eleonora Volpato1,2
1Department of Psychology, Università Cattolica Del Sacro Cuore, Milan, Italy; 2IRCCS Fondazione Don Gnocchi, Milan, Italy
Correspondence: Valentina Poletti, Department of Psychology, Università Cattolica del Sacro Cuore, Milan, Italy, Email [email protected]
Background: Chronic Obstructive Pulmonary Disease (COPD) is a chronic inflammatory lung disease characterized by persistent respiratory symptoms and airflow limitation. Besides its irreversibility, COPD is a treatable condition, and patients would strongly benefit from being adherent to their treatments. However, almost half of them are non-adherent, and, according to several recent studies, the way the patient perceives the disease might influence this variable.
Aim: This systematic review provided a synthesis of studies about the relationships between illness perceptions (IP), cognitions, beliefs, and adherence in COPD.
Methods: English language publications were searched in PubMed, Medline, Scopus, ResearchGate, PsycINFO, and Cochrane Library databases from November 2022 to February 2023, following PRISMA guidelines. The reference lists of eligible studies were also searched. Data extraction and critical appraisal were undertaken by two reviewers working independently.
Results: A total of 14 studies were included. Adherence to treatment in COPD is confirmed to be low, using both self-report questionnaires and objective assessment systems. Most studies concluded that COPD is perceived as a moderate threat destined to last forever, even if many participants referred to little disease knowledge. This perception did not change between adherent and non-adherent groups. Those who considered more necessary to take their medicines and had a caregiver were more adherent and less concerned about their future. On the other side, forgetfulness, lack of trust in medications, and difficulties in understanding how to take them were perceived as the main causes of non-adherence. Other predictors of non-adherence, like depression, low self-efficacy, and severity of disease were confirmed.
Conclusion: The systematic review highlights the variability of the relationship between IP, cognitions and beliefs, and COPD treatment adherence. A new level of awareness of the relationship between patients’ subjective point of view and treatment adherence may inform future treatment options and promote a more personalized intervention.
Keywords: illness perception, COPD, adherence to treatment, illness cognition, illness belief
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is an irreversible but treatable condition characterized by chronic bronchitis, airway thickening, and emphysema.1
Worldwide, COPD is considered the most frequent chronic respiratory disease and a leading cause of chronic morbidity and mortality, affecting above 391.9 million people aged between 30 and 79 years, with a higher prevalence among tobacco smokers.1
In addition to tobacco smoking, several risk factors have been studied to improve COPD management, such as indoor and outdoor air pollution, occupational hazards, and infections.2 For this reason, a crucial part of COPD treatment consists of lifestyle changes: like quitting smoking, avoiding triggers like dust and pollution, eating a healthy diet, and avoiding respiratory infection.2
Typical treatments for COPD include medications: bronchodilators, corticosteroids, antibiotics, and mucolytics, commonly used to open the airways, reduce inflammation, and clear mucus;3 oxygen therapy, used to help patients who have low oxygen levels;4 non-invasive ventilation (NIV), a form of respiratory support that uses a mask to deliver air or oxygen without the need for an invasive procedure (like intubation);5 pulmonary rehabilitation, a program of exercise and education that helps to improve breathing and muscle strength6 and surgery, which may be recommended to remove damaged parts of the lungs or to repair a collapsed lung.7
However, if on the one hand, medicine continues to introduce many treatments which can improve patient’s quality of life and disease acceptance, on the other hand, what makes a difference is their adherence rate, that is the extent to which a person’s proactive behavior coincides with medical or health advice8 which is generally low in patients with COPD.9
Studies have reported that the percentage of COPD patients who adhere to their treatment regimens ranges from as low as 30% to as high as 80%9–11 and these differences are often due to two main reasons.
First, there is no consistency in the method by which adherence is assessed in studies on COPD and, consequently, the use of different methods of assessing adherence provides different results.12 Second, inhaled drugs carry different implications for the evaluation of adherence than oral medications.13
However, as a multifactorial variable, several predictors had been studied to understand the mechanism behind these discouraging percentages. Researchers discovered that age,14 higher levels of education,15 and having a regular healthcare provider16 are associated with better adherence rates; on the contrary, factors like the use of multiple medications or having complex treatment regimens14 are associated with lower adherence.
In addition to this, considering the symptom burden in COPD patients (which may include cough, sputum production, wheeze, chest tightness, fatigue) and its impact on patient’s psychological well-being,17 more recent research led to a better understanding of some psychological aspects of it (such as psychiatric morbidity and cognitive impairment).18
Volpato et al,19 for example, described the relationship between some psychopathological conditions, ie, anxiety and depression, and their impact on adherence to treatment.
Other researchers explored the role of perceived self-efficacy20 and alexithymia21 on COPD treatment, suggesting their consideration during the implementation of a personalized treatment plan.
Only in more recent times has literature begun to show interest in patients’ perceptions of their condition.22 This research has focused on the theoretical construct of Illness Perception (IP), which, according to the Self-Regulation Model (SRM),23 consists of the patient’s set of cognitive representations including beliefs about the cause, the duration, the impact, and the controllability of the illness.24
Following this line of research, Kaptein et al demonstrated that IP is a determinant of patient’s quality of life, number of hospitalization, and medication use, even after controlling for the duration and objective severity of COPD,22 reinforcing the thesis that an inaccurate perception of one’s clinical condition might be associated to poorer treatment outcome.25
Moreover, other similar and related constructs are nowadays research objects, such as Illness Cognitions, and Beliefs.
Unlike IP, which refers to an individual’s understanding and interpretation of his/her illness, cognition refers to mental processes such as thinking and memory and it defines how an individual learns something;26 while belief refers to a conviction or acceptance that something that an individual knows is true, often without evidence.27
Considering the importance of actively involving the patient in his/her disease management, knowing the meaning patient attributes to the condition might be a first step to achieve a more detailed understanding of the relationship between patients’ subjective point of view of their illness condition and treatment adherence. This relationship, moreover, may inform future treatment options in COPD and promote a more personalized clinical intervention.
Aim
The aim of the present systematic review is providing an essential summary of the expanding literature characterizing the relation between IP, beliefs, and cognitions on treatment adherence in patients with COPD.
Materials and Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was followed in conducting this systematic review.28 The protocol was registered with PROSPERO international prospective register of systematic reviews (# CRD42022373141).
Search Strategy, Eligibility Criteria, and Information Sources
Systematic searches were conducted from November 2022 to February 2023 following PRISMA guidelines.28 The PubMed, Medline, Scopus, ResearchGate, PsycINFO, and Cochrane Library databases were consulted to capture free full-text, open-access human studies, from inception to the first of February 2023, that specified a relationship between illness perceptions/beliefs/cognition and adherence to treatment in COPD patients.
Considering that this is a Systematic Review of literature the ethics approval has been obtained by the original authors.
Inclusion and exclusion criteria, as well as comprehensive search terms, are presented below in Table 1 and 2
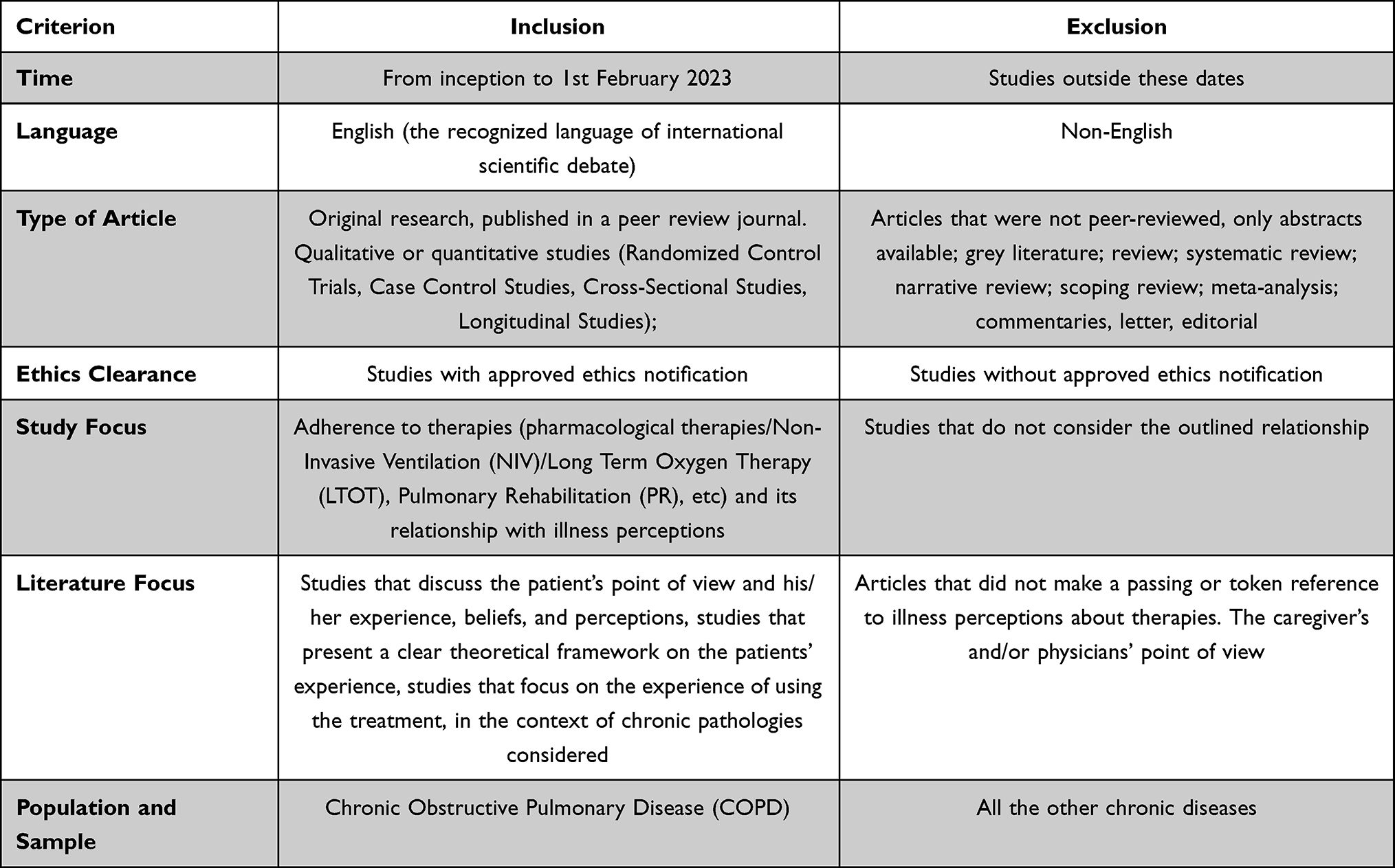 |
Table 1 Illness Inclusion and Exclusion Criteria |
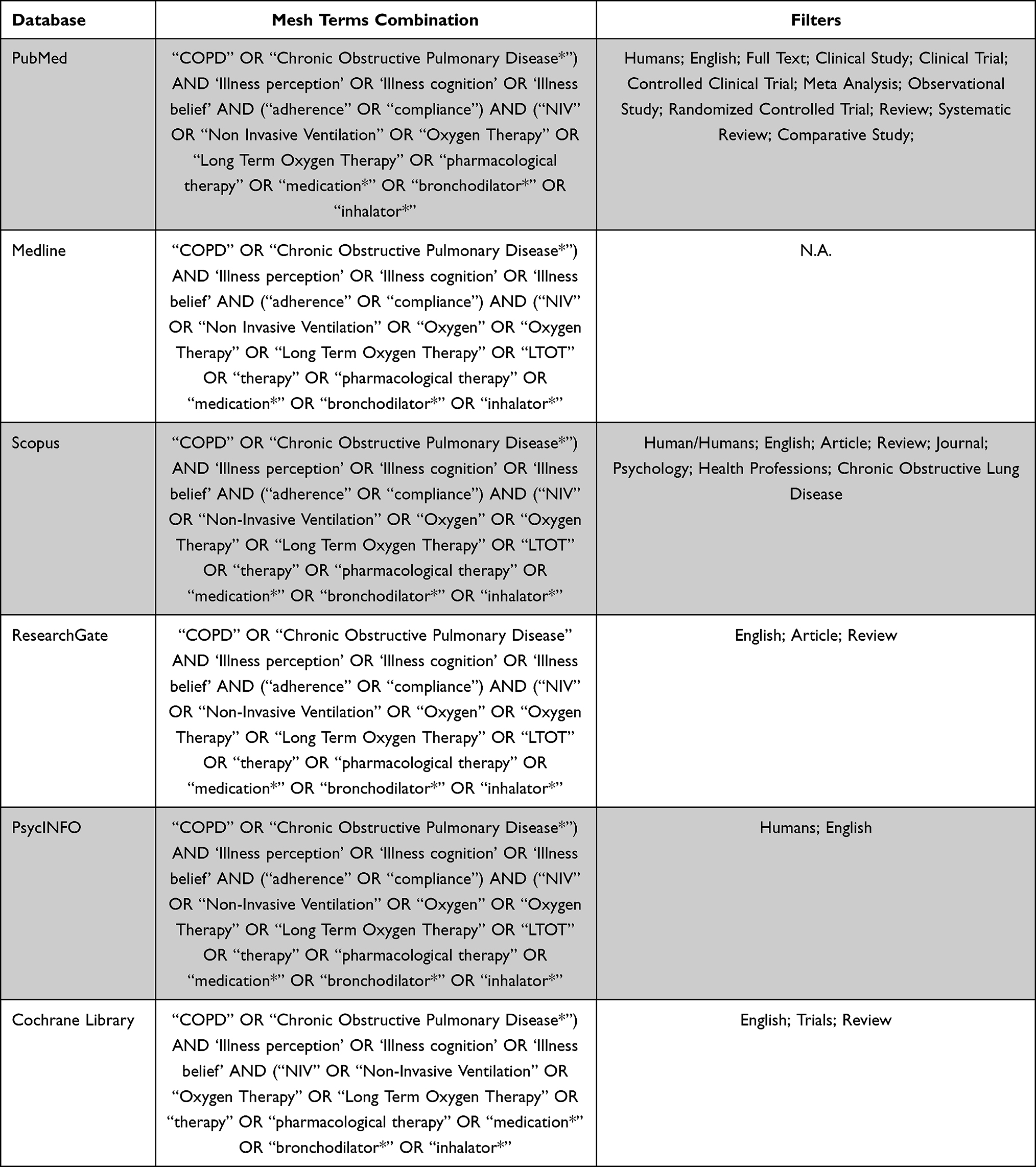 |
Table 2 Detailed Search Strategy |
Studies with populations with other illnesses besides COPD (eg, asthma) were included only if the results for the COPD group were highlighted and separated from other groups, considered the patient’s point of view, not the physicians’ or caregivers’.
Study Selection
Titles, abstracts, and keywords were independently reviewed by two authors (VP; EV) excluding those that did not meet the eligibility criteria. A third author (FP) was consulted to resolve inconsistencies in screening decisions. Other articles were excluded because they were not available or not published.
Full-text articles assessed for eligibility were read by the researchers and assessed following inclusion/exclusion criteria. To identify additional relevant literature, a manual search was conducted.
Data Extraction and Analysis
Data were extracted by two independent researchers (VP, EV) and confirmed by a third one (FP). Information gathered from each study considered the following data: title, authors, publication year, country, journal, keywords, kind of study, demographic description of participants (gender, mean age), objectives of the study, outcomes, setting, follow-up, drop-out rate, inclusion and exclusion criteria, analysis, instruments, explored themes and conclusions. Data from the final data extraction forms were tabulated and discussed in this review in a purely descriptive fashion.
Considering the heterogeneity of the data and the diversity of the clinical trial designs, no additional sub-analyses or meta-analyses were planned or performed.
Quality Assessment of Studies
Methodological quality assessment of the included studies was completed with the NIH quality assessment tool, a general guidance, composed of 14 questions, for determining the overall quality rating of observational cohort and cross-sectional studies (see https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools).
Assessment of quality was evaluated according to these published checklists by two independent authors (VP; EV), and doubts were clarified with the help of a third one (FP).
No studies were excluded based on quality. Details about quality assessment are reported in Figure 1.
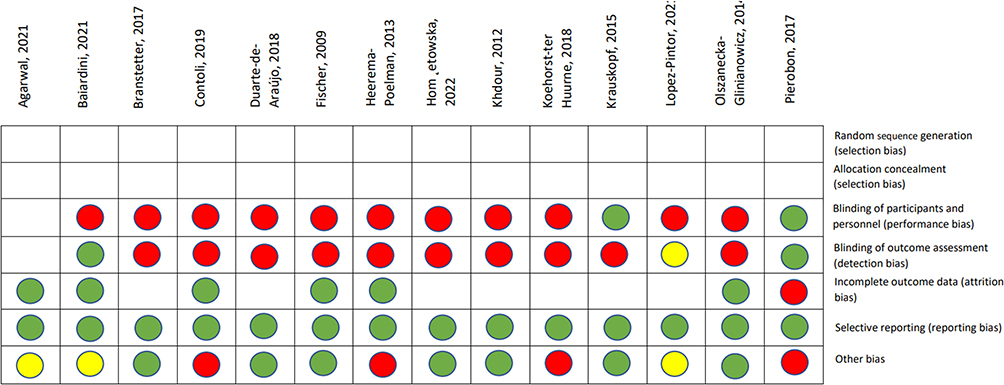 |
Figure 1 Risk of bias. |
Results
Study Selection
The search strategy allowed the identification of 209 potentially relevant records: 116 articles were retrieved from MedLine, 32 from PubMed, 11 from Cochrane Library, 15 from Scopus, 17 from PsycInfo, and 18 from Web of Science (Figure 2).
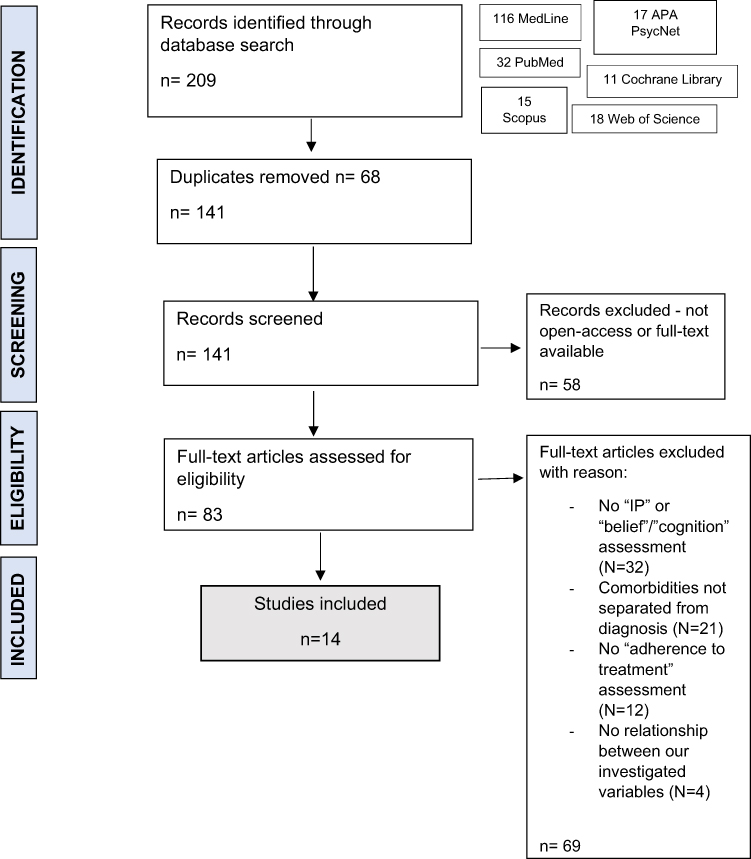 |
Figure 2 Study selection process – eligibility graph. |
After removing 68 duplicates, a total of 141 records’ titles and abstracts were screened, and from these, other 58 articles were removed because they were not open-access or full-text available.
Eighty-three full-text articles were assessed for eligibility, and 69 of them were excluded for different reasons: the most common reasons for exclusion were no mention of illness perception, cognition or belief, or adherence or no reference to the relationship between these variables and no distinction between COPD patients and other chronic disease patients (in particular, asthmatics) in the data analysis.
Finally, 14 studies were included in this review (MedLine: 55.5%, PubMed: 15.3%, Web of Science: 8.6%, APA: 8.1%, Scopus: 7.2%, Cochrane Library: 5.3%).
Samples Characteristics
The 14 included studies represent 8 different countries, including 3 from the Netherlands,29–31 3 from Italy,32–34 2 from Poland,35,36 2 from the USA,37,38 and 4 from other countries.13,15,39,40
Most of the studies were conducted in university settings or pulmonary rehabilitation and communities.
Almost all the studies (n = 10) are cross-sectional designs, only 2 are longitudinal studies,29,30 1 is a multicenter, noninterventional (observational) cohort study33 and 1 is an observational study.35
The mean age is above 66.23 years old, with a range from 52 to 80 years. On average, males outnumber women (n/males: 3519 vs n/females: 2397).
The main characteristics of the included studies are shown in Table 3.
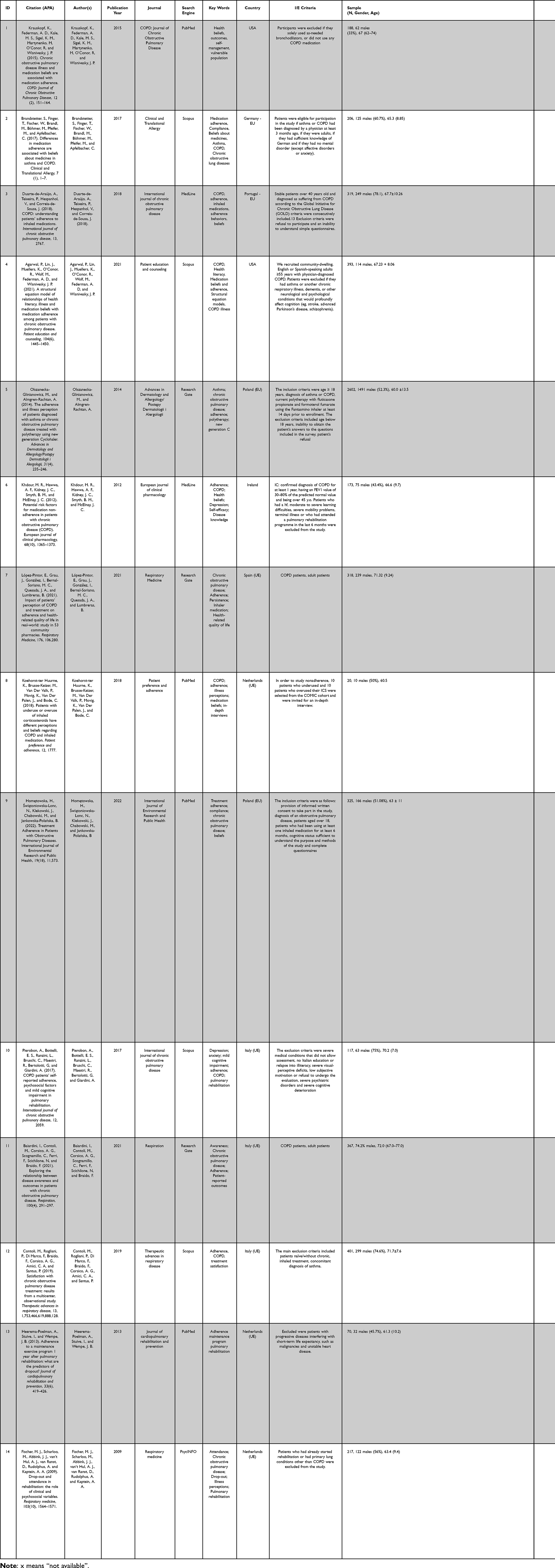 |
Table 3 Study Characteristics |
Measurements and Definition of Adherence
Adherence was assessed in many ways (see Table 4). For this reason, we decided to distinguish adherence to medication therapy from physiotherapy program, making explicit the scores and the tools used by each research group.
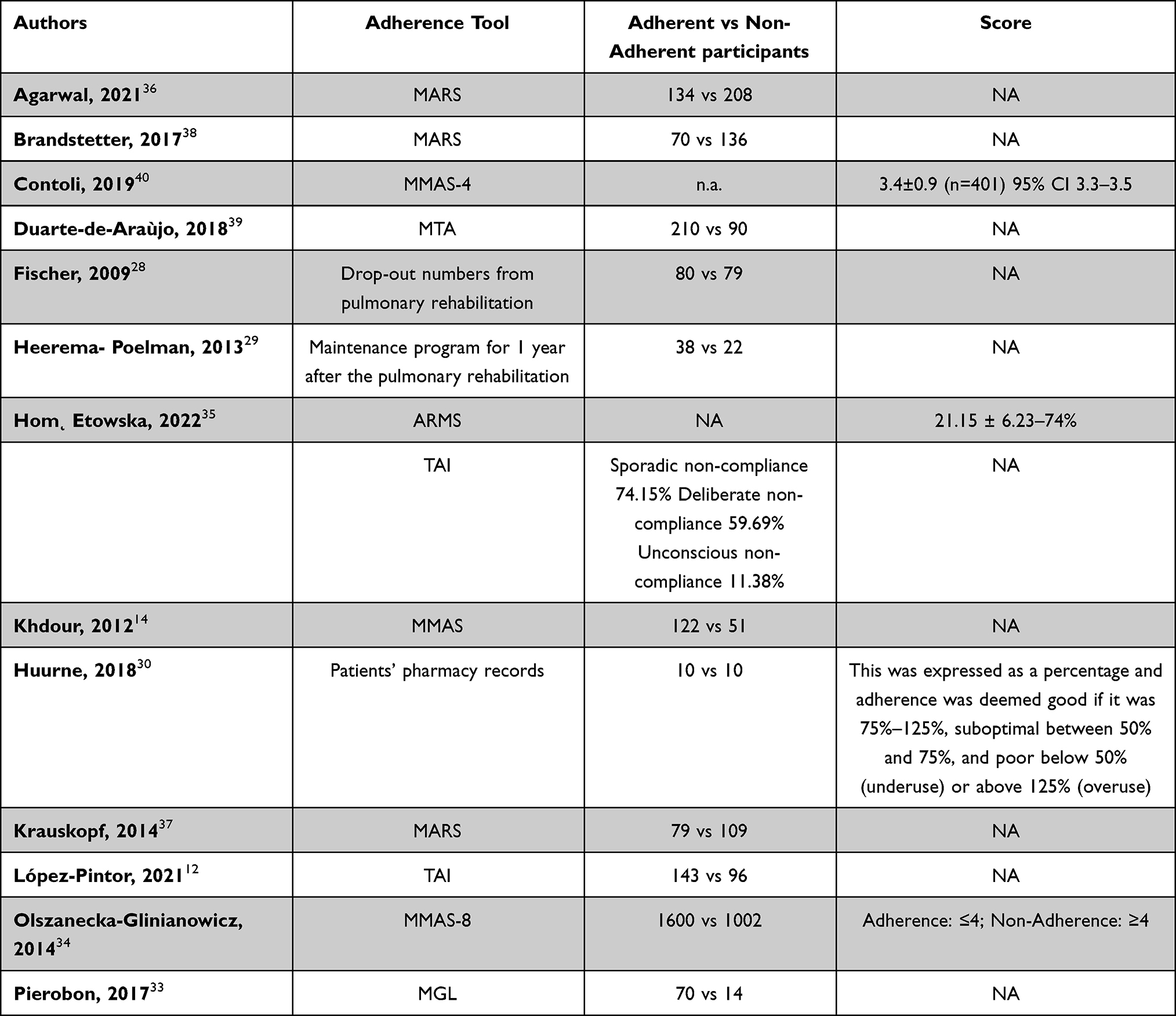 |
Table 4 List of Included Studies That Discussed Different Kinds of Adherence |
Adherence to Medication Treatment
Three studies37–39 administered the Medication Adherence Report Scale (MARS)41 and results confirmed that more patients do not adhere to treatment than those who adhere (149 vs 245 non-adherent groups).
Three authors15,32,35 administered the Morisky Medication Adherence Scale,42 in its both versions, 4 and 8 items. Khdour et al15 reported that “forgetfulness” as the main cause of non-adherence and results reported a little difference between adherence and non-adherence rate (1722 vs 1053 non-adherent groups).
Two research groups13,36 used the Test of Adherence to Inhalers’ (TAI),43 a 12-item questionnaire, designed to assess the adherence to inhalers, and results reported a similar rate of adherence and non-adherence between the two samples (228 vs 236 non-adherent groups).
One author40 used the Measure of Treatment Adherence (MTA), a psychometric tool derived from Morisky Medication Adherence Scale and found that 50 participants were non-adherent (vs 250); Pierobon et al34 used the Morisky, Green, and Levine Adherence Scale (MGL Adherence Scale)42 and the majority of the samples were adherent to treatment (70 vs 14 non-adherent groups).
Finally, Koehorst and collaborators31 recorded therapy adherence with ICS from patients’ pharmacy records: adherence was deemed good if it was 75%–125%, suboptimal between 50% and 75%, and poor below 50% (underuse) or above 125% (overuse).
Adherence to Physiotherapy Program
Heerema-Poelman30 assessed adherence as attending the maintenance program for 1 year after the Pulmonary Rehabilitation Program. [Dropouts at 6 months received the self-reported questionnaire, in which they were asked to describe the reasons for nonadherence, such as experiencing exacerbations, lack of motivation, financial burden, or distance problems, and exacerbations were the main cause] (38 vs 22 non-adherent groups).
Fischer et al29 decided to focus on drop-out numbers from pulmonary rehabilitation to evaluate adherence to the rehabilitation program. Lack of motivation and hope of improvement were important barriers to adherence.
Illness Perception in COPD Patients
Illness perception was generally assessed through The Illness Perception Questionnaire (IPQ)44 and its different versions. The IPQ is a self-report tool which was specifically constructed to assess the five components of illness representation described in Leventhal’s self-regulation model, which means beliefs about the cause, the duration, the impact, and the controllability of the illness.24
Five authors32,33,35,37,38 assessed IP through the Brief Illness Perception Questionnaire (Brief-IPQ),45 a nine-item version of the original self-report tool.44
Two authors29,30 used The Illness Perception-Revised (IPQ-R),46 a revised version which includes some additional subscales, like cyclical timeline perceptions, illness coherence, and emotional representations.
Finally, Huurne31 decided to use a semi-structured interview inspired by the 5-factor model structure of the Illness Perception Questionnaire.
The mean score of The Brief Illness Perception Questionnaire was 46.67 ± 9, which, considering the cut-off (<42 indicates low threat, 42–49 indicates moderate threat, and ≥50 indicates high threat), represents a perception of illness as a moderate threat. In particular, according to Agarwal,37 the highest scores were observed talking about the continuity of symptoms over time (M = 10; (9, 10)) and the feeling of worry for the illness (M = 10; (7, 10)).
Regarding the IPQ-R, we could not report an average score, because Fischer provided scores for the adherent group separately from the non-adherent group,29 while Heerema-Poelman only reported the Personal Control (20.7 ± 2.7 vs 20.4 ± 4.4) and the Treatment Control Scores (15.6 ± 2.2 vs 16.2 ± 3), dividing the adherent group scores from the non-adherent one,30 results explained that both adherent and non-adherent subjects perceived the same level of personal control on their illness condition, while beliefs about the possibility of being cured and able to control their illness through treatment is slightly higher in non-adherent people.
Huurne’s findings were a general belief that COPD symptoms could not be cured, associated to a feeling of worry for the future; a general perception of limitation of participants’ quality of life and daily routine activities; most of the participants reported that smoking and heredity were the main causes of their condition; and a general low acceptance of the disease.31
Illness and Medication Beliefs and Cognitions in COPD Patients
Considering beliefs and cognition in COPD patients, we mainly observed the use of the following tools (See Table 5 for more details about the scores):
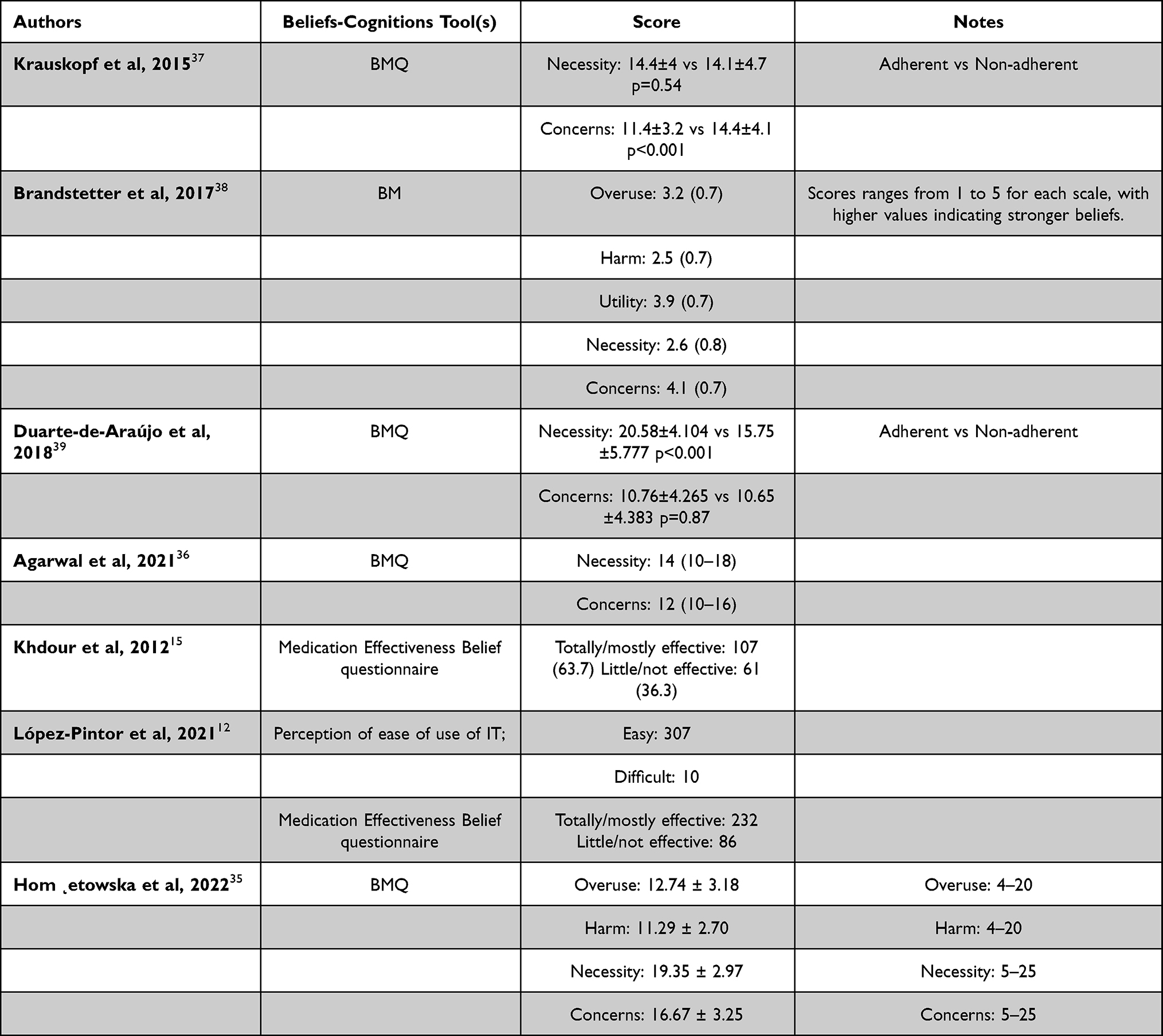 |
Table 5 List of Included Studies That Discussed Different Kinds of Illness Beliefs and Cognition Tools |
- The Belief about Medicines Questionnaire (BMQ),47 is a 10 items self-report tool for evaluating people’s beliefs about medicines, through a 5 points Likert scale. Items are divided into two subscales: “Medication Necessity score” and “Concerns about medication score”; scores range from 5 to 25: higher score indicates greater belief that COPD medications are necessary and greater worry about COPD medications.
- The Health Belief Model (HBM) Questionnaire, a 5-point Likert scale self-report tool, is widely used as a conceptual framework to explain and predict health behaviors by focusing on the beliefs and attitudes of individuals. It includes four primary variables: perceived susceptibility (eg, belief of vulnerability to disease relapse as a result of not taking the medication when not experiencing symptoms directly), perceived severity (or seriousness of the health threat), perceived benefits (eg, individual’s belief in the efficacy of the prescribed medication in reducing disease severity or susceptibility) and perceived barriers (eg, stigma of taking medication or denial of having serious illness).48
- The Medication Effectiveness Belief questionnaire,15 a ad hoc questionnaire in which patients were asked to rate their perceived medication effectiveness and their faith in their prescribed medication as totally effective, mostly effective, partially effective or totally not effective.
- An ad hoc questionnaire about the perception of ease of use of the inhaler medications.13
The Relationship Between IPs, Cognitions and Beliefs and Adherence to Treatment in COPD Patients
Below, in Table 6, we reported all the relationships (with the used statistical analysis techniques) we found, between adherence to treatment and illness perceptions, beliefs, and cognitions.
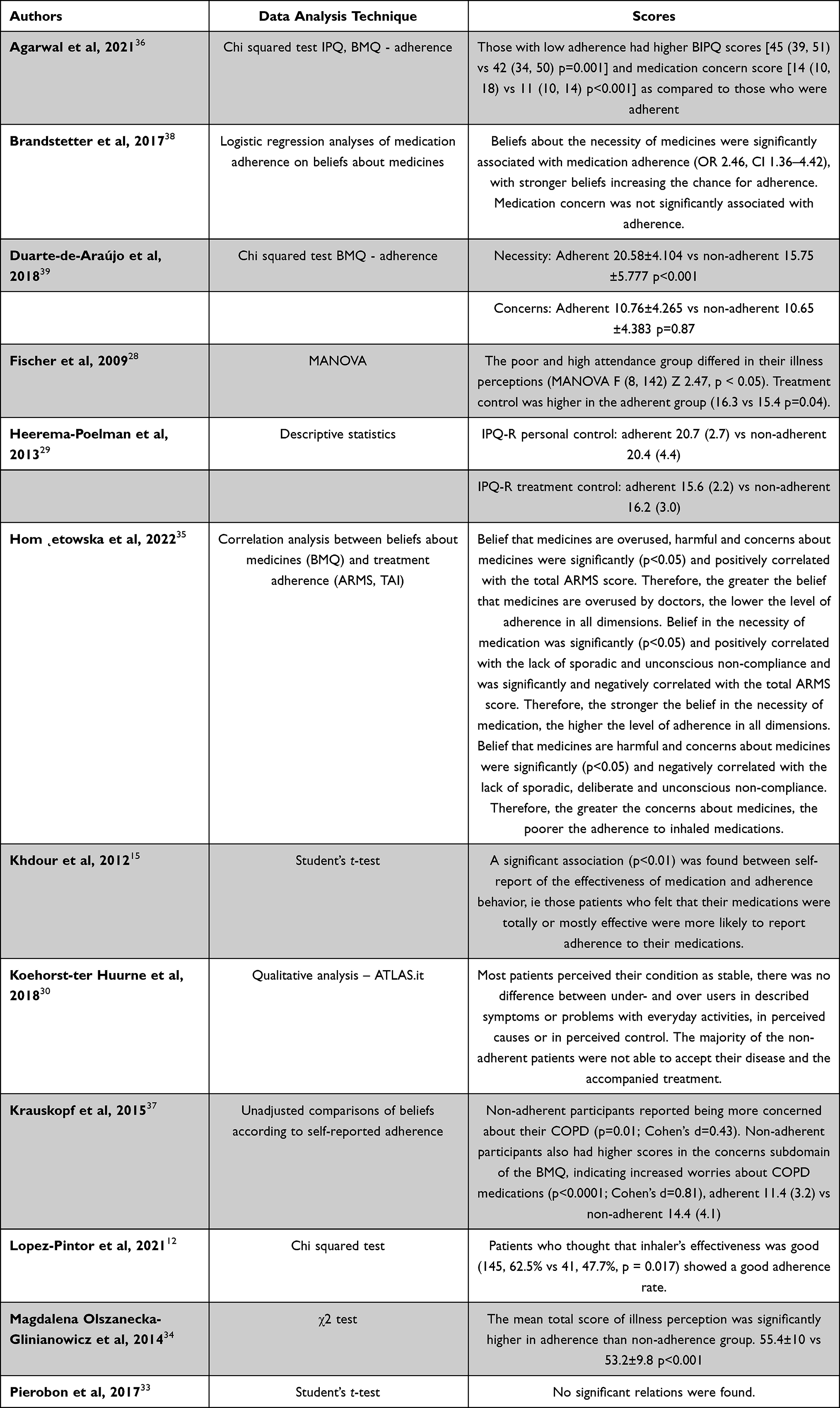 |
Table 6 Relationship Between IP, Beliefs, and Cognitions and Adherence to Treatment in COPD Patients |
Other Considered Variables and Their Relationship with Adherence to Treatment
Considering that adherence to treatment is a multifactorial variable, we decided to make explicit those predictors that have been most cited by the authors, such as some physical conditions (disease severity,38 smoking status,36 body mass index29) or some psychological variables like self-efficacy or health-related quality of life.39 Below, in Table 7, we reported all the cited predictors of adherence to treatment in COPD patients we found in our selected studies.
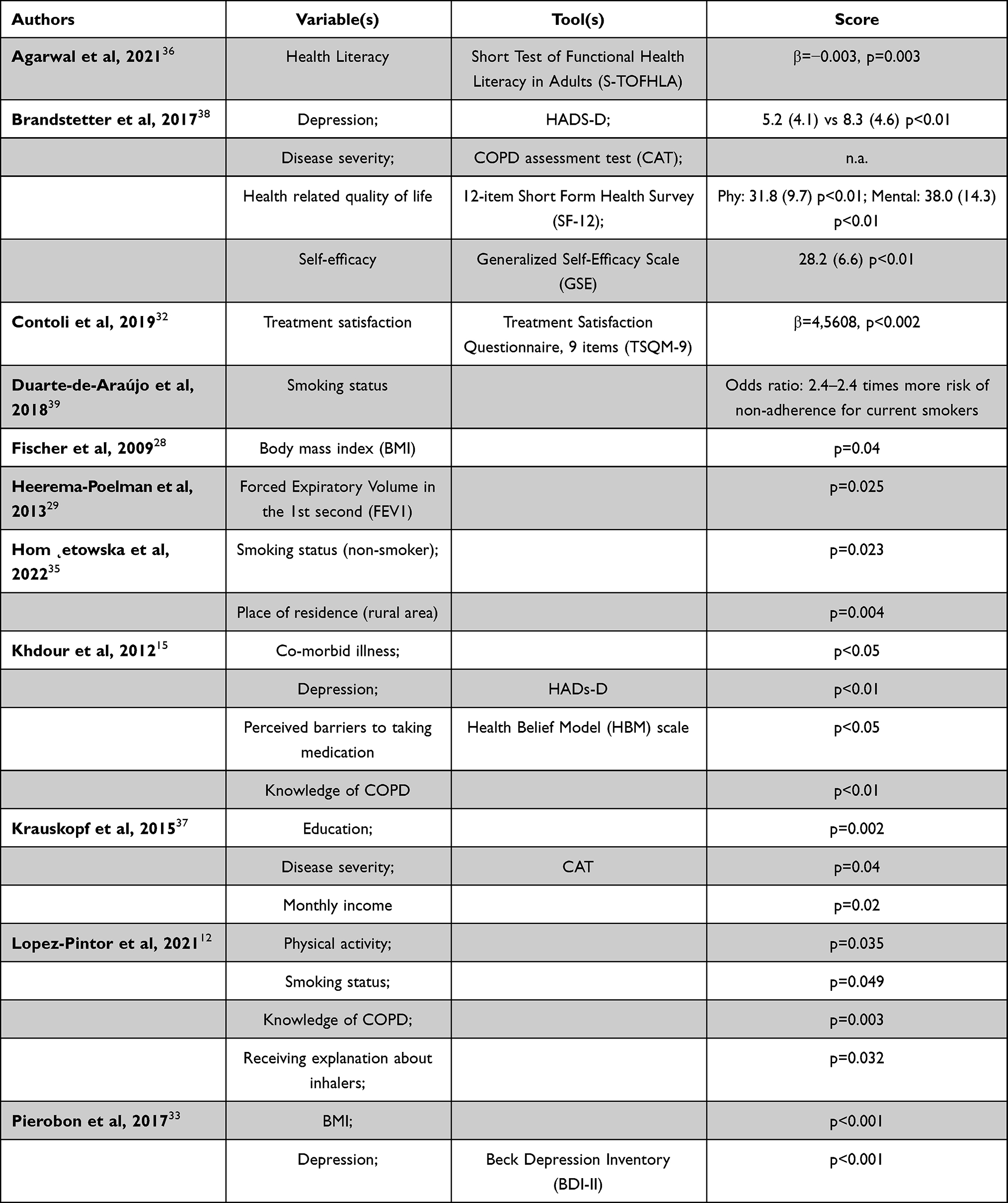 |
Table 7 Predictors of Adherence to Treatment in COPD Patients |
Discussion
Finding a definition of “adherence” continues to be a complex matter.
In 2001, the WHO defined it as
the extent to which a person’s behavior taking medication, following a diet, and/or executing lifestyle changes corresponds with agreed recommendations from a health care provider49
Giving patients a passive role, which, considering the importance of patients’ point of view about his/her illness condition, does not correspond to reality.
However, as Hughes specified, adherence is not just a dichotomous variable (ie, adherent/non-adherent), but a really more complex concept: for this reason, a common situation might be a COPD patient who may choose to stop taking some medications for no apparent reason.50
In this sense, adherence to treatment is also determined by patients’ choices of following medical directions, considering that, during a clinical experience, patient could build personal theories about it.
This latter aspect involves a real active position of the patient, whose theory about adherence, for example, might depend on whether patients are outcome-oriented, for example, “feeling better”, or process-oriented, like being more regular with the medication use.11
Therefore, by changing our perspective and assuming that the patient, in all respects, plays an active role in his/her treatment, it is easier to understand the importance of being aware of his/her point of view, through the knowledge of perceptions, cognitions, and beliefs about pathology.
To fill this research gap, we decided to focus our attention on adherence to treatment, which is considered, according to COPD guidelines,51 one of the most important aspects of COPD self-management. However, as previous studies confirmed,9 low rates of treatment adherence are common in COPD and they are also typically associated with several adverse health outcomes and a general patient’s quality of life reduction.16
Looking at our selected studies we could confirm a generally low rate of adherence, with only one exception,33 who reported a suboptimal level.
In any other case, no matter which assessment tool was chosen, no relevant differences had been found between results, reporting a general low rate of adherence, even using different ranges and cut-off. Moreover, on the contrary, two studies38,39 even found that their sample consisted of a majority of people who did not adhere to their treatment at all.
Poor adherence rates were also found when considering adherence to physiotherapy program, especially after one year;30 whereas perceived physiotherapy treatment effectiveness demonstrated to be a strong predictor of patients’ adherence behavior in rehabilitation, offering a first demonstration of the importance of considering patient’s perceptions.29
In light of this finding, factors that can improve the level of adherence should be considered during the treatment selection process and be part of a self-management program focusing on the patient’s role.
Starting from these considerations, we investigated patients’ perceptions and beliefs about their condition and their treatment, as well.
As Pierobon et al34 explained, being aware of one’s condition is essential for consciousness and long-term management of chronic diseases, such as COPD. Many patients, in fact, deny their diagnosis or prognosis, to protect themselves.52 At the same time, awareness is also considered a crucial competency for healthcare providers and public health practitioners.37 This makes it easier for them to understand why one patient may be more adherent than another and enables them to provide appropriate support to at-risk patients.37
Brandstetter et al,39 for example, discovered that COPD patients’ beliefs about medication overuse by doctors and the harm of medicines reduced adherence rates to about 40%, while patients with stronger beliefs about the necessity of their medicines were three times as likely to be completely adherent. Similar results were also collected by Khdour et al,15 Olszanecka-Glinianowicz et al35 and Duarte-de-Araùjo et al,40 who also asked their participants to provide some justifications of their (non)-adherent behavior. According to COPD patients, for example, having a caregiver and easy access to medications were predictors of adherent behavior, while a lack of trust in medication (and its effectiveness) was a risk factor.40 Regarding this, Lòpez-Pintor et al13 found that receiving information about medication from clinicians before starting treatment might improve patients’ level of adherence. This aspect was also described by Olszanecka-Glinianowicz35 who reported “Poor understanding of instructions from the doctor” and “The method of taking the drug is complicated” (p. 240) as frequent affirmations of non-adherent group.
According to Krauskopf et al38 and Koehorst-ter Huurne,31 even negative emotions (like depression, “Half of our nonadherent patients also reported depressed mood” p. 178231) and concerns about COPD and its impact on life were predictive of a low adherence rate. In line with the above point, Koehorst-ter Huurne et al31 discovered that illness acceptance is a crucial variable to take into account talking about adherence to treatment, reporting that those patients who had a greater understanding about their illness were those with a greater level of acceptance and an increased adherence level.
Considering illness perceptions according to Leventhal’s model,23 we discussed each dimension, case-by-case.
In general, COPD is perceived as a moderate threat.
Focusing on “Identity” – How a person views his/her illness,23 many participants13,15,31,37 could not give a clear definition of it; in particular, some of them even talked about a general airway obstruction.31 However, considering adherent and non-adherent groups separately, a higher rate was found in the non-adherent participants, which means that non-adherent people perceived their symptoms more than adherent participants.38
Talking about “Timeline” – How the patient believes the illness will develop over time23 - several studies,35,37 found that concerns about the future were very common, even between adherent people.31
From “Illness consequences” dimension – How the patient believes that the severity of illness will impact on physical, social, and psychological functioning23 - emerged that both adherent and non-adherent patients had many problems in daily activities;31–34,37,38 however, Khdour et al31 specified that those with a good level of COPD self-efficacy perceived less negative consequences on their life than other participants and were more likely to be classified as adherent to treatment. On the other side, most reported “causes” were smoking, genetics, and environmental factors like pollution.15,31,37,39
Finally, we explored “Control”, which is divided in “Treatment control” - How a person perceived that medication could control his/her condition - and “Personal control” - How a person perceived to be able to control his/her condition.23
Contrary to expectations, Heerema-Poelman et al,30 who specifically focused on “control” dimension and its relationship with adherence to treatment, discovered that adherent people perceived to have more treatment control than others, but no difference was reported between groups when asking about personal control. This finding, however, might be explained by the “timeline” perception of a “forever” lasting condition,35 which persists even in the adherent group.29
Limitations
As for limitations, it is useful to note that the considered sample was quite small (n = 14) and this was also since we decided to consider only open-access articles, so the external validity of our results can be threatened. In addition, only two of the studies have longitudinal design, so it would be interesting if future research will investigate whether and how these constructs change over time.
Conclusions
Adherence to treatment remains a challenge to the health and quality of life of COPD patients, as, both using objective and self-report tools, rates are low. In the light of the findings regarding the perceived threat of non-adherence and the consideration of patients’ subjective views, future interventions should try to consider the extent of the perception of disease and the beliefs that patients have about their treatment so that the level of awareness and adhesion can be improved.
However, having ascertained the interest and the novelty of this fertile research area, future research should choose to use both types of tools for the assessment of adherence to treatment, to obtain a more complete overview of the situation; moreover, and focus more on the impact these constructs have in clinical practice, for example, through the validation of new specific tools.
Abbreviations
BDI, Beck Depression Inventory; B-IPQ, Brief Illness Perception Questionnaire; BMI, Body mass index; BMQ, Beliefs about medicines questionnaire; CAT, COPD assessment test; COPD, Chronic obstructive pulmonary disease; FEV1, Forced Expiratory Volume in the 1st second; GSE, Generalized Self-Efficacy Scale; HADS, Hospital Anxiety Depression Questionnaire; HBM, Health Belief Model; IP, Illness Perception; IPQ, Illness Perception Questionnaire; IPQ-R, Illness Perception Questionnaire Revised; LTOT, Long-Term Oxygen Therapy; MARS, Medication Adherence Report Scale; MMAS, Morisky Medication Adherence Scale; MTA, Measure of Treatment Adherence; NA, Not available; NIV, Non-Invasive Ventilation; PR, Pulmonary Rehabilitation; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; SRM, Self-Regulation Model; S-TOFHLA, Short Test of Functional Health Literacy in Adults; TAI, Test of the adherence to inhalers; TSQ-9, Treatment Satisfaction Questionnaire, 9 items; WHO, World Health Organization.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was not supported by any funder.
Disclosure
The authors declare no conflicts of interest for this work.
References
1. Adeloye D, Song P, Zhu Y, Campbell H, Sheikh A, Rudan I. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med. 2022;10(5):447–458. doi:10.1016/S2213-2600(21)00511-7
2. Thys van der Molen C, van der Molen T, Maguire T, Goyal P, Altman P. Optimizing identification and management of COPD patients–reviewing the role of the community pharmacist. Br J Clin Pharmacol. 2016;83(1):192–201. doi:10.1111/bcp.13087
3. Cazzola M, Page C, Rogliani P, Calzetta L, Matera MG. Multifaceted beneficial effects of erdosteine: more than a mucolytic agent. Drugs. 2020;80(17):1799–1809. doi:10.1007/S40265-020-01412-X
4. Khor YH, Renzoni EA, Visca D, McDonald CF, Goh NSL. Oxygen therapy in COPD and interstitial lung disease: navigating the knowns and unknowns. ERJ Open Res. 2019;5(3):1–8. doi:10.1183/23120541.00118-2019
5. Ambrosino N, Vagheggini G. Non-invasive ventilation in exacerbations of COPD. Int J Chron Obstruct Pulmon Dis. 2007;2(4):471–476.
6. Wouters EFM, Posthuma R, Koopman M, et al. An update on pulmonary rehabilitation techniques for patients with chronic obstructive pulmonary disease. Expert Rev Respir Med. 2020;14:149–161. doi:10.1080/17476348.2020.1700796
7. Marchetti N, Criner GJ. Surgical approaches to treating emphysema: lung volume reduction surgery, bullectomy, and lung transplantation. Semin Respir Crit Care Med. 2015;36(4):592–608. doi:10.1055/S-0035-1556064
8. Horwitz R. Adherence to treatment and health outcomes. Arch Intern Med. 1993;153(16):1863–1868. doi:10.1001/archinte.1993.00410160017001
9. Bhattarai B, Walpola R, Mey A, Anoopkumar-Dukie S, Khan S. Barriers and Strategies for Improving Medication Adherence Among People Living With COPD: a Systematic Review. Respir Care. 2020;65:1738–1750. doi:10.4187/respcare.07355
10. Humenberger M, Horner A, Labek A, et al. Adherence to inhaled therapy and its impact on chronic obstructive pulmonary disease (COPD) 11 medical and health sciences 1102 cardiorespiratory medicine and haematology. BMC Pulm Med. 2018;18(1). doi:10.1186/S12890-018-0724-3
11. Bourbeau J, Thorax SB. Patient adherence in COPD. Thorax. 2008;63:831–838. doi:10.1136/thx.2007.086041
12. Rogliani P, Ora J, Puxeddu E, Matera MG, Cazzola M. Adherence to COPD treatment: myth and reality. Respir Med. 2017;129:117–123. doi:10.1016/J.RMED.2017.06.007
13. López-Pintor E, Grau J, González I, Bernal-Soriano MC, Quesada JA, Lumbreras B. Impact of patients’ perception of COPD and treatment on adherence and health-related quality of life in real-world: study in 53 community pharmacies. Respir Med. 2021;176:106280. doi:10.1016/j.rmed.2020.106280
14. Vetrano DL, Bianchini E, Onder G, et al. Poor adherence to chronic obstructive pulmonary disease medications in primary care: role of age, disease burden and polypharmacy. Geriatr Gerontol Int. 2017;17(12):2500–2506. doi:10.1111/ggi.13115
15. Khdour MR, Hawwa AF, Kidney JC, Smyth BM, McElnay JC. Potential risk factors for medication non-adherence in patients with chronic obstructive pulmonary disease (COPD). Eur J Clin Pharmacol. 2012;68(10):1365–1373. doi:10.1007/S00228-012-1279-5/METRICS
16. George M, Bender B. New insights to improve treatment adherence in asthma and COPD. Patient Prefer Adherence. 2019;13:1325. doi:10.2147/PPA.S209532
17. Miravitlles M, Ribera A. Understanding the impact of symptoms on the burden of COPD. Respir Res. 2017;18(1). doi:10.1186/S12931-017-0548-3
18. Hynninen KMJ, Breitve MH, Wiborg AB, Pallesen S, Nordhus IH. Psychological characteristics of patients with chronic obstructive pulmonary disease: a review. J Psychosom Res. 2005;59(6):429–443. doi:10.1016/j.jpsychores.2005.04.007
19. Volpato E, Toniolo S, Pagnini F, Banfi P. The relationship between anxiety, depression and treatment adherence in chronic obstructive pulmonary disease: a systematic review. Int J Chron Obstruct Pulmon Dis. 2021;Volume 16:2001–2021. doi:10.2147/COPD.S313841
20. Kohler CL, Fish L, Greene PG. The relationship of perceived self-efficacy to quality of life in chronic obstructive pulmonary disease. Heal Psychol. 2002;21(6):610–614. doi:10.1037/0278-6133.21.6.610
21. Milenkovic B, Latas M, Cvejic J, Jankovic J. Alexithymia in COPD patients. Eur Respir J. 2015;46(suppl 59):OA2909. doi:10.1183/13993003.CONGRESS-2015.OA2909
22. Scharloo M, Kaptein A. Illness perceptions and quality of life in patients with chronic obstructive pulmonary disease. J Asthma. 2008;45(8):625–629. doi:10.1080/02770900802127048
23. Leventhal H, Nerenz DR, Steele DJ. Illness representations and coping with health threats. Handb Psychol Heal Vol IV Soc Psychol Asp Heal. 2020;219–252. doi:10.4324/9781003044307-9/ILLNESS-REPRESENTATIONS-COPING-HEALTH-THREATS-HOWARD-LEVENTHAL-DAVID-NERENZ-DAVID-STEELE
24. Cameron LD, Leventhal H. The self-regulation of health and illness behaviour. Self Regulation Heal Illn Behav. 2012;1–346. doi:10.4324/9780203553220
25. von Leupoldt A, Dahme B. Psychological aspects in the perception of dyspnea in obstructive pulmonary diseases. Respir Med. 2007;101(3):411–422. doi:10.1016/j.rmed.2006.06.011
26. Brewer N, Chapman G, Brownlee S, Leventhal EA. Cholesterol control, medication adherence and illness cognition. Br J Health Psychol. 2002;7(4):433–447. doi:10.1348/135910702320645408
27. Årestedt L, Benzein E, Persson C. Families living with chronic illness: beliefs about illness, family, and health care. J Fam Nurs. 2015;21(2):206–231. doi:10.1177/1074840715576794
28. Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/JOURNAL.PMED.1000097
29. Fischer MJ, Scharloo M, Abbink JJ, et al. Drop-out and attendance in pulmonary rehabilitation: the role of clinical and psychosocial variables. Respir Med. 2009;103(10):1564–1571. doi:10.1016/J.RMED.2008.11.020
30. Heerema-Poelman A, Stuive I, Wempe JB. Adherence to a maintenance exercise program 1 year after pulmonary rehabilitation: what are the predictors of dropout? J Cardiopulm Rehabil Prev. 2013;33(6):419–426. doi:10.1097/HCR.0b013e3182a5274a
31. Ter HKK, Brusse-Keizer M, van der Valk P, Movig K, van der Palen J, Bode C. Patients with underuse or overuse of inhaled corticosteroids have different perceptions and beliefs regarding COPD and inhaled medication. Patient Prefer Adherence. 2018;12:1777. doi:10.2147/PPA.S167002
32. Baiardini I, Contoli M, Corsico AG, et al. Exploring the relationship between disease awareness and outcomes in patients with chronic obstructive pulmonary disease. Respiration. 2021;100(4):291–297. doi:10.1159/000513953
33. Contoli M, Rogliani P. Satisfaction with chronic obstructive pulmonary disease treatment: results from a multicenter, observational study. Ther Adv Respir Dis. 2019;2019:13. doi:10.1177/1753466619888128
34. Pierobon A, Bottelli ES, Ranzini L, et al. COPD patients’ self-reported adherence, psychosocial factors and mild cognitive impairment in pulmonary rehabilitation. Int J COPD. 2017;12:2059–2067. doi:10.2147/COPD.S133586
35. Dermatologii Alergologii P, Olszanecka-Glinianowicz M, Almgren-Rachtan A. Original paper<br>The adherence and illness perception of patients diagnosed with asthma or chronic obstructive pulmonary disease treated with polytherapy using new generation cyclohaler. Adv Dermatology Allergol. 2014;31(4):235–246. doi:10.5114/PDIA.2014.45070
36. Hom˛ Etowska H, Swi N, Klekowski J, Chabowski M, Jankowska-Polá Nska B. Treatment adherence in patients with obstructive pulmonary diseases. Int J Environ Res Public Health. 2022;19. doi:10.3390/ijerph191811573
37. Agarwal P, Lin J, Muellers K, O’Conor R. A structural equation model of relationships of health literacy, illness and medication beliefs with medication adherence among patients with chronic obstructive. Patient Educ Couns. 2021;104(6):1445–1450. doi:10.1016/j.pec.2020.11.024
38. Krauskopf K, Federman AD, Kale MS, et al. Chronic obstructive pulmonary disease illness and medication beliefs are associated with medication adherence. COPD. 2014;12(2):151–164. doi:10.3109/15412555.2014.922067
39. Brandstetter S, Finger T, Fischer W, et al. Differences in medication adherence are associated with beliefs about medicines in asthma and COPD. Clin Transl Allergy. 2017;7(1):1–7. doi:10.1186/S13601-017-0175-6/TABLES/3
40. Duarte-de-Araújo A, Teixeira P, Hespanhol V, Correia-de-Sousa J. COPD: understanding patients’ adherence to inhaled medications. Int J Chron Obstruct Pulmon Dis. 2018;Volume 13:2767–2773. doi:10.2147/COPD.S160982
41. Chan AHY, Horne R, Hankins M, Chisari C. The medication adherence report scale: a measurement tool for eliciting patients’ reports of nonadherence. Br J Clin Pharmacol. 2020;86(7):1281–1288. doi:10.1111/BCP.14193
42. Morisky D, Green L. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 2022;2022:1.
43. Plaza V, Fernández-Rodríguez C, Melero C, et al. Validation of the “Test of the Adherence to Inhalers” (TAI) for asthma and COPD patients. J Aerosol Med Pulm Drug Deliv. 2016;29(2):142–152. doi:10.1089/JAMP.2015.1212/ASSET/IMAGES/LARGE/FIGURE3.JPEG
44. Weinman J, Petrie K, Moss-morris R, Horne R. The illness perception questionnaire: a new method for assessing the cognitive representation of illness. Psychol Health. 1996;11(3):431–445. doi:10.1080/08870449608400270
45. Broadbent E, Petrie K, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–637. doi:10.1016/j.jpsychores.2005.10.020
46. Moss-Morris R, Weinman J, Petrie K, Horne R, Cameron L, Buick D. The Revised Illness Perception Questionnaire (IPQ-R). Psychol Heal. 2002;17(1):1–16. doi:10.1080/08870440290001494
47. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 2007;14(1):1–24. doi:10.1080/08870449908407311
48. Rosenstock IM. The health belief model and preventive health behavior. Heal Educ Behav. 1977;2(4):354–386. doi:10.1177/109019817400200405
49. Sabaté E, Sabaté E Adherence to long-term therapies: evidence for action; 2003. Available from: https://books.google.com/books?hl=it&lr=&id=kcYUTH8rPiwC&oi=fnd&pg=PR5&dq=Sabate+E.+Adherence+to+long-term+therapies:+evidence+for+action.+Geneva:+World+Health+Organization%3B+2003&ots=tC0Qer5fq_&sig=z_oP25oWkxsKzUnNsPJc-OEEB8g.
50. Hughes CM. Medication non-adherence in the elderly: how big is the problem? Drugs Aging. 2004;21(12):793–811. doi:10.2165/00002512-200421120-00004
51. Mirza S, Clay RD, Koslow MA, Scanlon PD. COPD guidelines: a review of the 2018 GOLD report. Mayo Clin Proc. 2018;93(10):1488–1502. doi:10.1016/J.MAYOCP.2018.05.026
52. Gerretsen P, Mallar Chakravarty M, Mamo D, et al. Illness awareness in cancer patients: a conceptual framework and a preliminary classification hypothesis. Psycho Oncol. 2013;34(5):1035–1043. doi:10.1002/hbm.21490
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.