Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Identifying Subjective Symptoms Associated with Psychomotor Disturbance in Melancholia: A Multiple Regression Analysis Study
Authors Tamada Y ![]() , Inoue T, Sekine A, Toda H, Takeshima M, Sasaki M, Shindome K, Morita W, Kuyama N, Ohmae S
, Inoue T, Sekine A, Toda H, Takeshima M, Sasaki M, Shindome K, Morita W, Kuyama N, Ohmae S
Received 3 January 2021
Accepted for publication 26 March 2021
Published 19 April 2021 Volume 2021:17 Pages 1105—1114
DOI https://doi.org/10.2147/NDT.S300233
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Yu Tamada,1– 3 Takeshi Inoue,2 Atsushi Sekine,4 Hiroyuki Toda,5 Minoru Takeshima,2,6 Masaaki Sasaki,3 Keisuke Shindome,5 Wataru Morita,5 Nagisa Kuyama,3 Susumu Ohmae3
1Department of Psychiatry, Toranomon Hospital Kajigaya, Kawasaki, Kanagawa, Japan; 2Department of Psychiatry, Tokyo Medical University, Tokyo, Japan; 3Department of Psychiatry, Toranomon Hospital, Tokyo, Japan; 4The Medical Foundation of Keishin-Kai, Kei Mental Clinic, Daisen, Akita, Japan; 5Department of Psychiatry, National Defense Medical College, Tokorozawa, Saitama, Japan; 6Shibata Hospital, Takaoka, Toyama, Japan
Correspondence: Yu Tamada
Department of Psychiatry, Toranomon Hospital Kajigaya, 1-3-1 Kajigaya, Takatsu-ku, Kawasaki, Kanagawa, 213-8587, Japan
Tel +81 44 877 5111
Fax +81 44 877 5333
Email [email protected]
Purpose: Melancholia has recently been re-evaluated, because patients with major depressive disorder (MDD) were found to be heterogeneous. However, the DSM-5 criteria for melancholia (DSM-MEL) have been criticized, because of the difficulty in clearly distinguishing between melancholic and non-melancholic depression using DSM-MEL. Psychomotor disturbance (PMD) is one of the most important, as well as one of the only measurable symptoms of melancholia. Parker et al developed the CORE measure, which assesses PMD as a behavioral characteristic. The aim of our study was to objectively identify the subjective symptoms of melancholia by analyzing the symptoms associated with PMD.
Patients and Methods: A total of 106 participants with MDD were examined by psychiatrists. Multiple regression analysis was performed in which the total CORE score was the dependent variable, and items of the DSM-MEL and historically suggested melancholic features were independent variables.
Results: The following five independent variables were able to predict the total CORE score: 1) feelings of having lost feeling, 2) depressive delusions, 3) perplexity, 4) indecisiveness, and 5) no aggression against others. These five variables were more strongly associated with the total CORE score than the DSM-MEL.
Limitation: The major limitation of this study was that when choosing non-DSM melancholic signs and symptoms, we did not comprehensively evaluate and select the symptoms but chose items that are clinically important.
Conclusion: We identified five subjective symptoms that were associated with PMD. These five symptoms may be clinically useful as diagnostic criteria for melancholia.
Keywords: major depressive disorder, melancholic features, CORE measure, endogenous depression, diagnosis, psychomotor retardation
Introduction
As several lines of evidence have indicated that the diagnostic criteria of major depressive disorder (MDD) in DSM-51 do not assure homogenous populations and are not sufficient for treatment decisions, melancholia has been reappraised.2–6 In modern psychiatry, melancholia refers to a subtype of depression that is assumed to have a biological basis.7 Melancholia has the therapeutic characteristics of a poor response to psychotherapy and placebo, a good response to ECT,8 and is associated with laboratory test results, such as an abnormal cortisol reaction in the dexamethasone suppression test.9 Patients with melancholia have been considered to be a more homogenous group than those with MDD.7
However, consensus diagnostic criteria for melancholia have not been established to date.10 The DSM-5 criteria for melancholia (DSM-MEL)1 were not empirically determined.11 Four of the eight items in the DSM-MEL overlap with the criteria for MDD. Therefore, it is difficult to distinguish between melancholic and non-melancholic depression using DSM–5.12–14
Traditionally, melancholic symptoms have been described as follows:10,15,16 disturbances in affect that are disproportionate to stressors, blunted emotional response, nonreactive mood, pervasive anhedonia, self-reproach, psychomotor retardation, agitation, diurnal mood variation (morning worsening), depressive delusions, weight loss, early morning awakening, and suicidal thoughts and attempts.
Classical European psychiatry, influenced greatly by Jaspers and Schneider, also pointed out various clinical features of melancholia. The term “endogenous depression” was a synonym for melancholia.7,17,18 Schneider described endogenous depression as a depressive state of “Zyklothymie” (cyclothymia).19,20 It should be noted that the “Zyklothymie” referred to here is not the same as the modern concept of cyclothymic disorder. “Zyklothymie” is synonymous with manic–depressive illness and is a concept that includes not only bipolar disorder but also recurrent unipolar depression. Schneider emphasized “vitale Traurigkeit” (vital sadness), which is the sadness physically experienced as a characteristic of melancholia.19 This symptom appears as an abnormal physical sensation in the chest, head, and extremities. Schneider19 and Jaspers21 also focused on the blunted emotional response and called it “Gefühl der Gefühllosigkeit” (the feeling of having lost feeling). Schulte called a similar condition “Nichttraurigseinkönnen” (inability to mourn), and defined it as a core symptom of melancholia.22 He pointed out the melancholic feature of being unable to shed tears.22 Jaspers described “melancholische Ratlosigkeit” (melancholic perplexity) as a condition in which the patient was confused by the inability to understand the reason for the appearance of inhibition and delusions.21 In Japan, a premorbid personality, including characteristics of orderliness, consideration for others, and a strong sense of responsibility, has been considered as an important feature of a mild form of melancholia, which has been influenced by Tellenbach’s theory of melancholia.23–25
Among these characteristics, psychomotor disturbance (PMD), comprising retardation and agitation, is one of the only objectively measurable melancholic symptoms.26 Moreover, many empirical studies have shown that PMD is a core feature of melancholia.7,10,16 Parker et al have argued that melancholia can be distinguished from non-melancholic depression by evaluating PMD as an objective behavioral feature rather than by evaluating a patient’s subjective complaints.7 Parker et al developed the CORE measure to assess PMD as a behavioral feature.7 A higher total CORE score has been demonstrated to be associated with a better response to ECT.12,27 Furthermore, they argued that most patients with melancholia who are diagnosed by the existing diagnostic criteria, such as DSM-III-R28 or the Newcastle Index,29 can be diagnosed solely by the CORE score.30 Their findings suggest that PMD was associated with other cardinal features of melancholia, including subjective symptoms.31
From the above, we considered that behaviorally observed PMD is closely associated with subjective melancholic symptoms. Sobin and Sackeim pointed out that few studies have objectively measured the minor symptoms of melancholia, and that PMD might be a reasonable starting point for such an endeavor.26 We hypothesized that the clinical symptoms associated with behavioral PMD are the subjective symptoms of melancholia. However, to the best of our knowledge, no study to date has analyzed the subjective symptoms associated with behaviorally observed PMD by multivariate analysis. Parker et al showed that the total CORE score is associated with six symptoms of melancholia (ie, weight loss, anhedonia, terminal insomnia, loss of interest, non-reactive mood, and constipation) by univariate analysis.30 However, there was a limitation to these conclusions because they did not exclude confounding factors when performing multiple regression analysis.
Therefore, the purpose of the present study was to objectively identify the subjective symptoms of melancholia by analyzing the symptoms associated with PMD. We performed multiple regression analysis using total CORE score as the dependent variable, and historically suggested melancholic symptoms as independent variables in patients with MDD, to identify symptoms associated with behavioral PMD.
Methods
Subjects
The subjects were a total of 106 patients with MDD who were treated at either Toranomon Hospital in Tokyo (general hospital), Toranomon Hospital Kajigaya in Kawasaki (general hospital), the National Defense Medical College Hospital in Saitama (university hospital), Kei Mental Clinic in Akita (psychiatric clinic), and J Clinic in Kanazawa (psychiatric clinic). All of these institutions usually provide primary general psychiatric care. The patients were recruited from January 2018 to March 2019. A total of 106 patients who visited one of the five institutions as new patients, and were diagnosed with major depressive disorder on DSM-5 were consecutively included in the study. Both outpatients and inpatients were included. The inclusion criteria were 1) meeting the criteria for MDD in DSM-5,1 2) being 20–69 years old, and 3) having the ability to consent to this study. The exclusion criteria were 1) having severe physical diseases, 2) having organic brain diseases, and 3) having severe suicidal ideation. Patients were clinically determined as to whether they had a severe physical illness or severe organic brain disease, and operational criteria were not set. In addition, patients with severe suicidal ideation were excluded from the study, because it is not ethically appropriate to burden such patients.
The following demographic and psychosocial characteristics were analyzed for each patient: age, sex, years of education, employment status, marital status, living alone or not, number of offspring, comorbid physical disease, psychiatric comorbidities, treatment setting, melancholic features and psychotic features based on DSM-5, family history of a first-degree relative with a mood disorder, age at the first episode, illness duration from the first depressive episode, number of previous depressive episodes, previous suicide attempts, and having treatment-resistant depression or not. Treatment-resistant patients were considered to be those with apparent depressive symptoms that persisted without improvement even after adequate treatment with two or more antidepressants from different pharmacological classes.32 Evaluators assessed patients at their nadir using the CORE measure and the melancholia symptom list described below. All evaluators were psychiatric specialists with more than 5 years of clinical experience. In addition, the Patient Health Questionnaire-9 (PHQ-9)33 was self-completed by the subjects in the written form at baseline.
Written informed consent was obtained from all subjects. Patients with an inability to consent were excluded. This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Toranomon Hospital (study approval no. 1516-H).
Assessment Measures
Patient Health Questionnaire-9 (PHQ-9)
The Japanese version of the PHQ-9 was self-completed by the subjects in the written form.33 In this study, the summary score of the PHQ-9 was used for assessing the severity of depressive symptoms.
CORE Measure
The CORE measure is a clinician-rated scale that measures PMD in a depressive disorder.7 The CORE measure consists of 18 items and is divided into the three subscales of retardation, agitation, and non-interactiveness. Scores are based on objective behavioral observations by the evaluator but not on the patient’s statements. Parker et al proposed a cutoff value for the diagnosis of melancholia of a total CORE score of 8 or more, and stated that the total CORE score could be used as a continuous variable.7
Melancholia Symptom List
A 26-item melancholia symptom list was created from a literature review of melancholia and interviews with experts (Table 3). This list is used by clinicians for rating the patients, and includes items from the DSM-5 criteria for melancholia. The following symptoms that were historically considered to be characteristic of melancholia or endogenous depression were included: the feeling of having lost feeling;19,21 vital sadness;19 perplexity;21 indecisiveness;20 self-reproach;19,21 repeated anxiety about excretion, such as constipation;34 and depressive delusions.19 The following items that are considered to be characteristic of non-melancholic depression were also included: binge eating; abuse of alcohol or drugs; poor treatment compliance; shedding tears during an interview;35 depressive symptoms varying from day to day;36 and aggression against others.37 These items were selected based on the diagnostic criteria for a dysthymic disorder of DSM-III,35 features of neurotic/reactive depression,36 hostile depression,37 and opinions of experts. Moreover, autonomic symptoms, such as hyperventilation, headache, nausea, and palpitations seen in general depressive states were added.38
Data Analysis
First, the associations between demographic and clinical characteristics and total CORE score were analyzed using Pearson correlation coefficient analysis and the two-sample t-test. The clinical characteristics of inpatients and outpatients were also analyzed using the two-sample t-test and Fisher’s exact test. Second, the effect of each item in the melancholic symptom list on total CORE score was analyzed by the two-sample t-test. A p-value of less than 0.05 was considered to indicate a statistically significant difference between groups on univariate analysis. Third, forced entry multiple regression analysis was performed using items in the melancholic symptom list that had a significant effect as the independent variables, and total CORE score as the dependent variable. The number of dependent variables was set to a maximum of 10 owing to the limit in sample size. Symptoms that were considered to be significantly associated with total CORE score by multiple regression analysis were referred to as psychomotor disturbance-associated subjective symptoms (PMD-SS). Fourth, the number of PMD-SS items with the largest effect size on the total CORE score were determined. The effect sizes of the PMD-SS and the DSM-MEL were also compared to determine which was more strongly associated with total CORE score. Finally, receiver operating characteristic (ROC) curves were created to analyze the optimal cutoff value for the diagnosis of melancholia by a number of PMD-SS items. As an external standard, the CORE score of 8 or more reported by Parker et al7 and the DSM-MEL were used. The optimum cutoff value was set as the value when the Youden’s index (sensitivity + specificity– 1) was the maximum.
Statistical analyses were conducted using SPSS 25 (IBM, Armonk, NY, USA). A p-value of less than 0.05 was considered to indicate a statistically significant difference between groups.
Results
Demographic and Clinical Characteristics and CORE Scores of the Subjects
The demographic and clinical characteristics and the CORE scores of the 106 MDD subjects are presented in Table 1. Being unemployed, being an inpatient, DSM-5 melancholic features, DSM-5 psychotic features, and having previous suicidal attempts were associated with a higher total CORE score by the t-test. No other demographic or clinical feature was associated with the total CORE score. There was no significant difference between inpatients and outpatients in PHQ-9 score, the number of patients with DSM-defined melancholia, and the number of patients with a CORE score of 8 or more (Table 2).
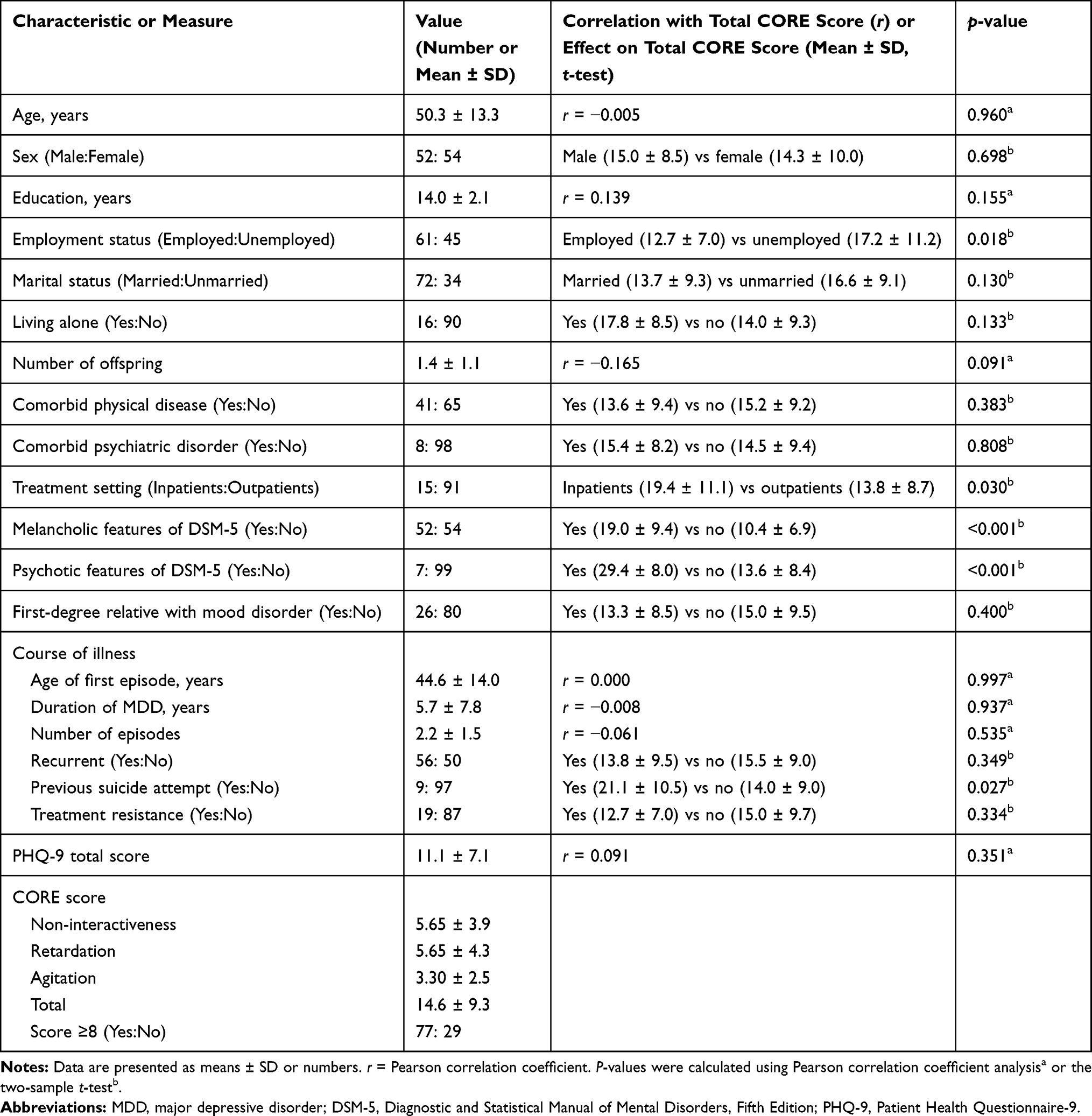 |
Table 1 Demographic and Clinical Characteristics and CORE Scores of 106 Patients with MDD |
 |
Table 2 Clinical Characteristics of the Outpatients and Inpatients |
Items in the Melancholia Symptom List and Total CORE Score
Table 3 shows the effects of the items in the melancholia symptom list on the total CORE score, analyzed by the two-sample t-test. A higher total CORE score was significantly associated with the following items: loss of pleasure, lack of reactivity, distinct quality of depressed mood, marked psychomotor agitation or retardation, significant anorexia or weight loss, excessive or inappropriate guilt, indecisiveness, perplexity, self-reproach, the feeling of having lost feeling, and depressive delusions. A lower CORE score was significantly associated with aggression against others.
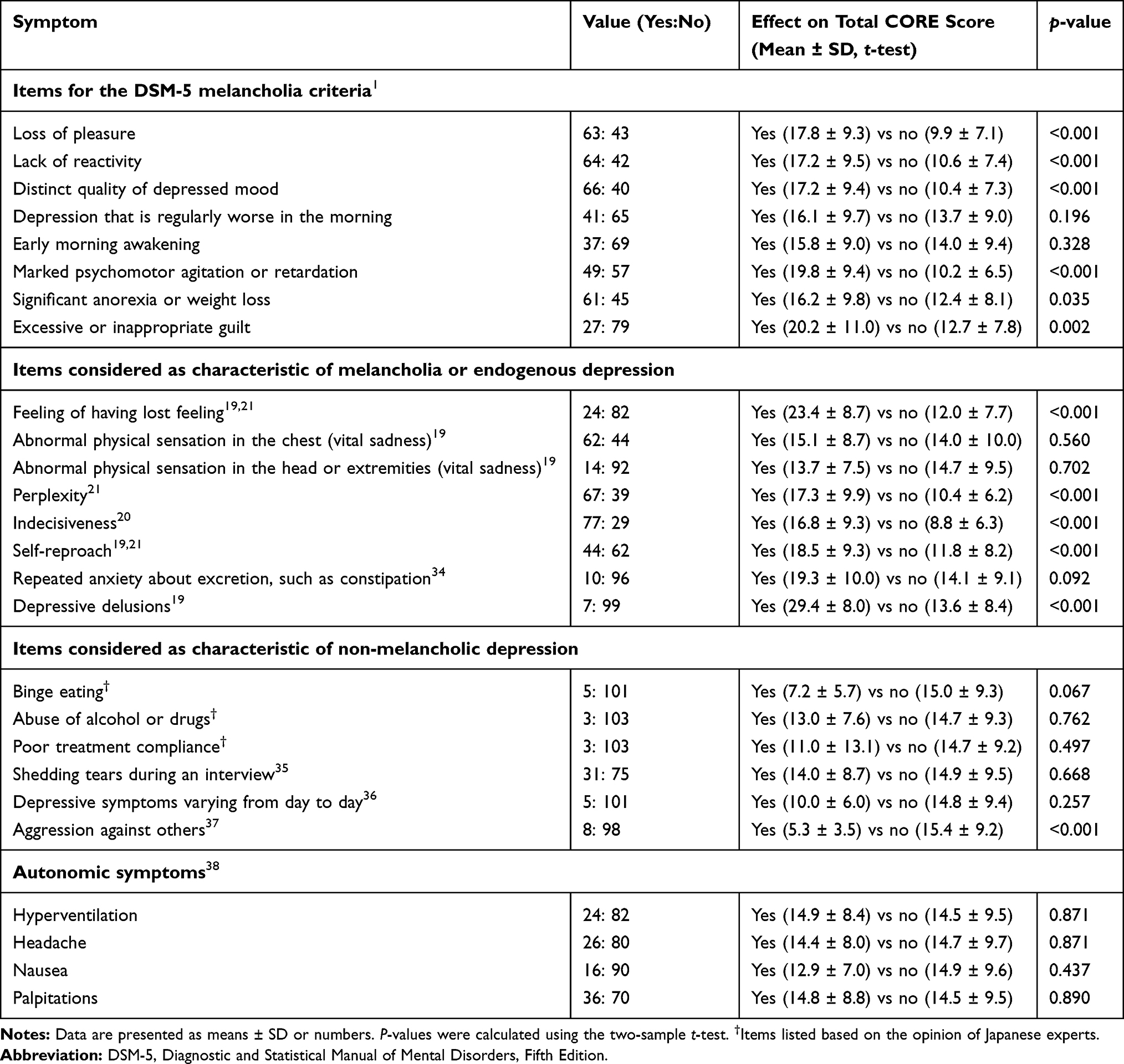 |
Table 3 The 26-Item Melancholia Symptom List and Total CORE Scores |
In performing the next multiple regression analysis, we excluded two items, namely, “lack of reactivity” and “marked psychomotor agitation or retardation,” which overlapped with the CORE measure.
Forced Entry Multiple Regression Analysis of Melancholic Symptoms on Total CORE Score
We performed multiple regression analysis by the forced entry method, using the total CORE score as the dependent variable and 10 items of the melancholic symptom list that significantly correlated with the total CORE score shown in the previous section as the independent variables. We found that the significance probability of the coefficient was p ≥ 0.05 for the following five variables: loss of pleasure (p = 0.09); distinct quality of depressed mood (p = 0.54); significant anorexia or weight loss (p = 0.13); excessive or inappropriate guilt (p = 0.27); and self-reproach (p = 0.13). We excluded these five variables and conducted multiple regression analysis by the forced entry method using the remaining five variables. The results are shown in Table 4. The item “aggression against others” had a negative beta value, so it was considered that “no aggression against others” positively correlated with the total CORE score. Therefore, the following five independent variables were identified to predict the total CORE score: 1) feelings of having lost feeling, 2) depressive delusions, 3) perplexity, 4) indecisiveness, and 5) no aggression against others (adjusted R2 = 0.499, F = 21.950, p < 0.001). Multicollinearity was negative. These five variables were hence considered to be PMD-SS.
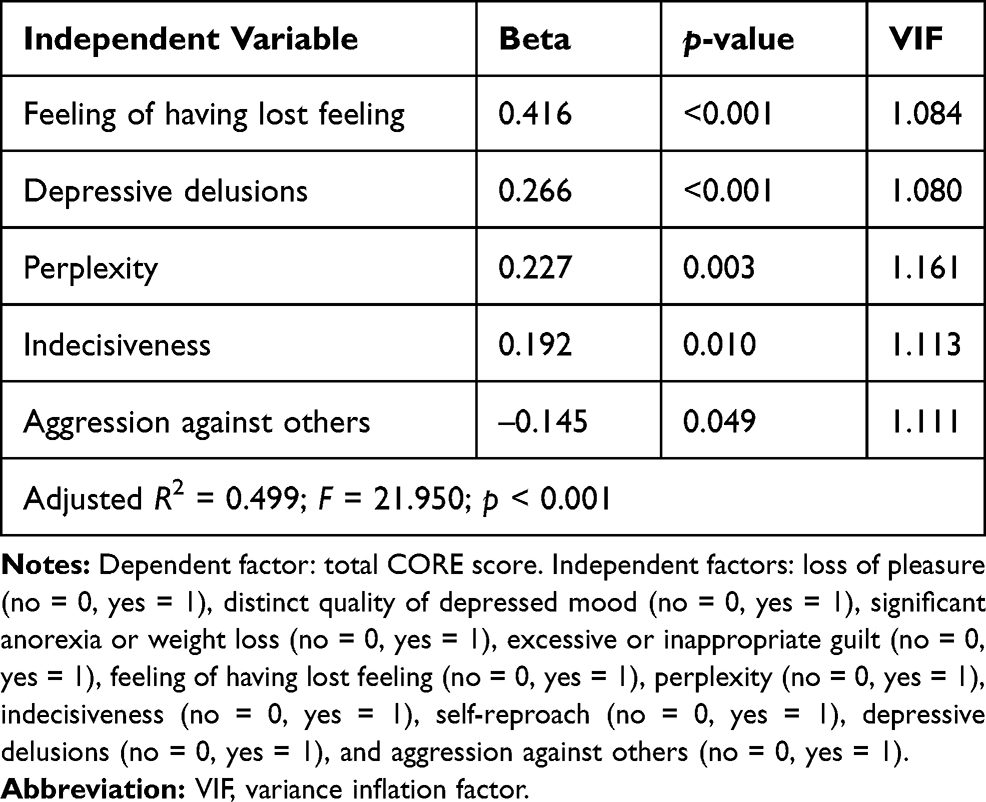 |
Table 4 Results of Multiple Regression Analysis of the Total CORE Score |
Effect Size for Total CORE Score of PMD-SS and DSM-MEL
We next investigated the effect sizes, to identify which of the PMD-SS and DSM-MEL had a strong association with the total CORE score (Table 5). As a result, when the number of PMD-SS items was set to 3 or 4, the effect size for the total CORE score was the maximum (r = 0.56). This effect size was slightly higher than that of the DSM-MEL (r = 0.47).
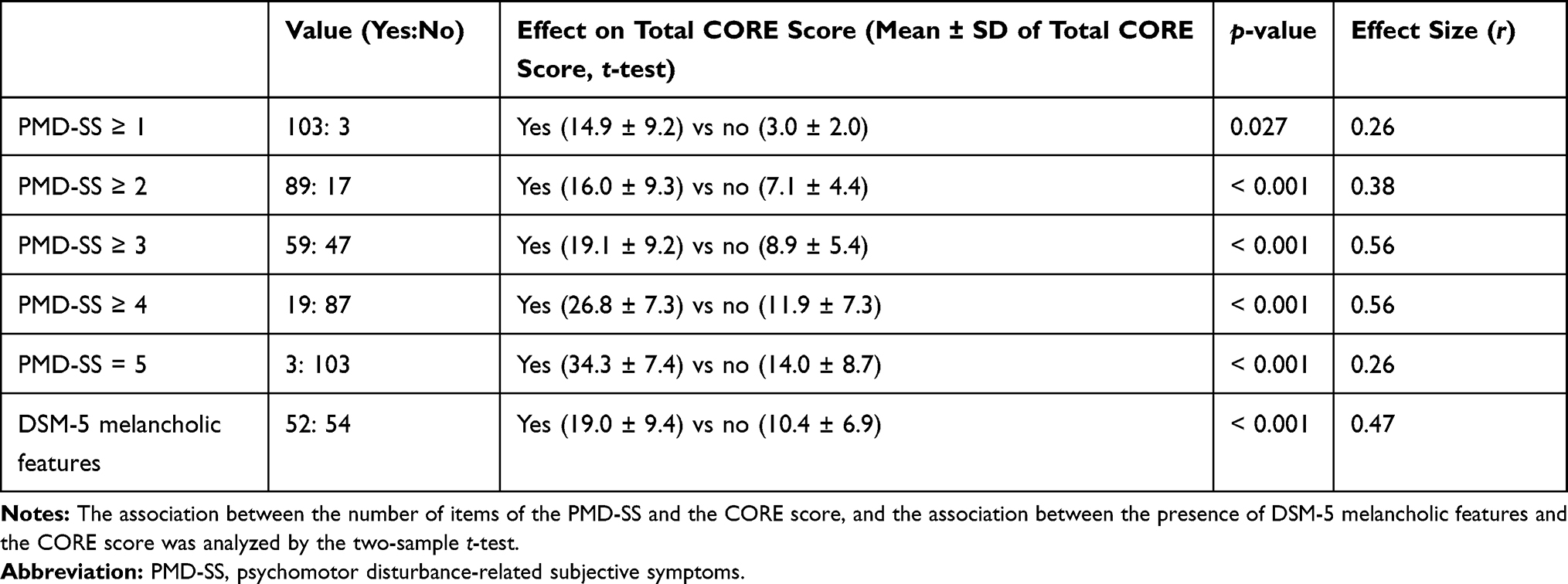 |
Table 5 Effect Sizes for the Total CORE Scores of PMD-SS and DSM-MEL |
Optimal Cutoff Value of PMD-SS
To analyze the cutoff value of PMD-SS for the diagnosis of melancholia, we set the ROC curve with “CORE score of 8 or more” or “DSM-5 melancholia” as the external standard for melancholia. We also analyzed the area under the curve (Figure 1). We concluded that PMD-SS had an optimal cutoff value of 3 or more. The diagnostic sensitivity and specificity based on this cutoff value were 68.8% and 79.3%, respectively, when the “CORE score of 8 or more” was used as an external standard, and 75.0% and 63.0%, respectively, when “DSM-5 melancholia” was used as an external standard.
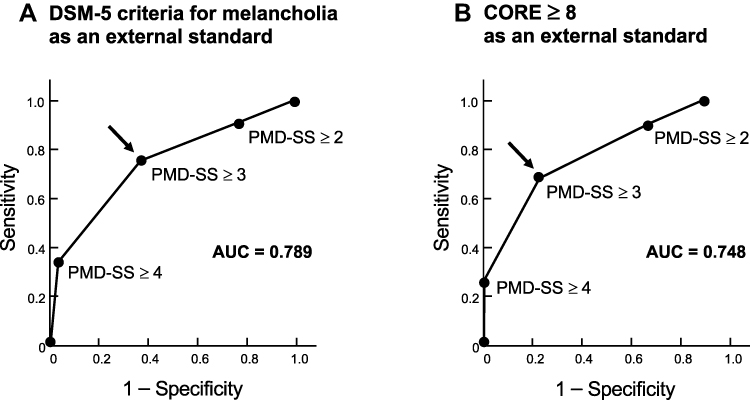 |
Figure 1 ROC curves for the diagnosis of melancholia according to the number of items of PMD-SS. ROC curves in which (A) DSM-5 criteria for melancholia, and (B) CORE score of 8 or more were used as an external standard are shown. The arrows represent optimal cutoff points. Abbreviations: PMD-SS, psychomotor disturbance-associated subjective symptoms; AUC, area under the curve. |
Discussion
In this study, we investigated the clinical symptoms of depression that are associated with behavioral PMD, to identify the subjective symptoms of melancholia. Using multiple regression analysis, we found the following five subjective symptoms to be associated with the total CORE score: 1) feelings of having lost feeling, 2) depressive delusions, 3) perplexity, 4) indecisiveness, and 5) no aggression against others. These five symptoms (PMD–SS) have been historically regarded as features of melancholia.19–21,23 PMD-SS were more strongly associated with the total CORE score than the DSM-MEL.
To our knowledge, no study to date has verified the subjective symptoms associated with behavioral PMD by multivariate analysis. Parker et al investigated the association between CORE score and melancholic features common to DSM-III-R and the Newcastle Index using univariate analysis.30 They found that six clinical symptoms (ie, appetite and/or weight loss, anticipatory and/or consummatory anhedonia, terminal insomnia, loss of interest, nonreactive mood, and constipation) were associated with the total CORE score. However, Parker et al did not perform multiple regression analysis using total CORE score as the dependent variable. They stated that the association between clinical symptoms and PMD was not straightforward. Four of the six items presented by Parker et al30 are also included in the DSM-MEL.
In the present study, we also found that “anorexia or weight loss”, “loss of pleasure (ie, anhedonia)”, and “lack of reactivity” showed a positive association with total CORE score on univariate analysis (Table 3). Nevertheless, multiple regression analysis was unable to demonstrate an association between these three items and total CORE score. This result suggests that the association reported by Parker et al30 may not actually be significant.
There are three possible reasons why PMD-SS were more strongly associated with total CORE score than the DSM-MEL. First, “feelings of having lost feeling” and “indecisiveness” of PMD-SS reflect inhibition in the areas of feeling and will, respectively. Subjective inhibition may lead to behavioral PMD. Second, psychotic depression is known to be associated with PMD,26 resulting in a higher CORE score.7 Therefore, “depressive delusions” is a feature that results in a high CORE score. Third, Jaspers pointed out that “perplexity” is a patient’s attitude toward an inability to understand the emergence of subjective inhibition and depressive delusions.21 Therefore, we considered “perplexity” to be associated with PMD. The characteristic of “no aggression against others” has been emphasized in Japan as a premorbid personality of mild melancholia,23,24 but the reason it is associated with PMD remains unknown.
Considering these findings, when PMD is taken as the core feature of melancholia, PMD-SS may reflect more core features of melancholia than DSM-5. Whereas the DSM-MEL have been criticized for not being determined empirically,11 the PMD-SS are melancholic symptoms that were determined empirically. The DSM-MEL overlap with MDD in four items, whereas PMD-SS and MDD overlap in only one item (ie, indecisiveness). Among the MDD criteria, indecisiveness is a factor that may reflect the characteristics of melancholia. Therefore, when PMD-SS are used as diagnostic criteria for melancholia, it may be easier to distinguish between melancholic and non-melancholic depression.
In recent years, it has been demonstrated that a higher total CORE score is associated with a more favorable response to ECT.12,27 Therefore, we expected that PMD-SS may be an index that can easily predict the effects of ECT, but further verification is required.
Limitations
The major limitation of the present study was that in choosing the non-DSM melancholic signs and symptoms, we did not comprehensively evaluate and select melancholia symptoms but selected the items that were important clinically. In addition, a large proportion of the subjects were outpatients with relatively mild symptoms, and symptom patterns may change when targeting hospitalized patients. Furthermore, as all subjects were being treated with medications, the effects of these medications on their symptoms cannot be excluded. Therefore, there are limitations in generalizing the results of this study.
Conclusion
In the present study, we identified five subjective symptoms associated with PMD (PMD-SS) from 26 potential depressive symptoms. PMD-SS may hence be useful criteria for the diagnosis of melancholia.
Acknowledgments
We thank Dr Katsufumi Matsunami (assistant director of Kanto Central Hospital) for his helpful advice in creating the melancholia symptom list, and Dr Helena Popiel of the Department of International Medical Communications, Tokyo Medical University, for editorial review of the manuscript.
Author Contributions
All authors made substantial contributions to the conception and design of the study, acquisition of the data, or analysis and interpretation of the data; took part in drafting the article or revising it critically for important intellectual content; agreed to its submission to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
This work was supported by a Grant-in-Aid for Early-Career Scientists from the Japan Society for the Promotion of Science (JSPS KAKENHI grant no.: JP19K14435); and grants from the Okinaka Memorial Institute for Medical Research. The funding sources had no role.
Disclosure
Takeshi Inoue has received personal fees from Mochida Pharmaceutical, Takeda Pharmaceutical, Eli Lilly, Janssen Pharmaceutical, MSD, Taisho Toyama Pharmaceutical, Yoshitomiyakuhin, and Daiichi Sankyo; grants from Shionogi, Astellas, Tsumura, and Eisai; and grants and personal fees from Otsuka Pharmaceutical, Dainippon Sumitomo Pharma, Mitsubishi Tanabe Pharma, Kyowa Pharmaceutical Industry, Pfizer, Novartis Pharma, and Meiji Seika Pharma; and is a member of the advisory boards of Pfizer, Novartis Pharma, and Mitsubishi Tanabe Pharma.
Atsushi Sekine has received lecture fees from Eli Lilly, Meiji Seika Pharma, Mochida Pharmaceutical, Yoshitomiyakuhin, and Otsuka Pharmaceutical.
Minoru Takeshima has received lecture fees from Kyowa Pharmaceutical Industry, Dainippon Sumitomo Pharma, and Yoshitomiyakuhin.
We presented a subset of our findings at the 185th General Meeting of Tokyo Medical University in Tokyo in July 2020.
All other authors declare that they have no conflicts of interest associated with this study.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
2. Frances A. Saving Normal: An Insider’s Revolt Against Out-Of-Control Psychiatric Diagnosis, DSM-5, Big Pharma, and the Medicalization of Ordinary Life. New York: Morrow; 2013.
3. Horwitz AV, Wakefield JC. The Loss of Sadness: How Psychiatry Transformed Normal Sorrow into Depressive Disorder. Oxford: Oxford University Press; 2007.
4. Fink M, Bolwig TG, Parker G, et al. Melancholia: restoration in psychiatric classification recommended. Acta Psychiatr Scand. 2007;115(2):89–92. doi:10.1111/j.1600-0447.2006.00943.x
5. Fink M, Taylor MA. Resurrecting melancholia. Acta Psychiatr Scand. 2007;115(Suppl 433):14–20. doi:10.1111/j.1600-0447.2007.00958.x
6. Valerio MP, Szmulewicz AG, Martino DJ. A quantitative review on outcome-to-antidepressants in melancholic unipolar depression. Psychiatry Res. 2018;265:100–110. doi:10.1016/j.psychres.2018.03.088
7. Parker G, Hadzi-Pavlovic D, Eyers K. Melancholia: A Disorder of Movement and Mood: A Phenomenological and Neurobiological Review. Cambridge: Cambridge University Press; 1996.
8. Brown WA. Treatment response in melancholia. Acta Psychiatr Scand. 2007;115(Suppl 433):125–129. doi:10.1111/j.1600-0447.2007.00970.x
9. Carroll BJ, Cassidy F, Naftolowitz D, et al. Pathophysiology of hypercortisolism in depression. Acta Psychiatr Scand. 2007;115(Suppl 433):90–103. doi:10.1111/j.1600-0447.2007.00967.x
10. Rush AJ, Weissenburger JE. Melancholic symptom features and DSM-IV. Am J Psychiatry. 1994;151(4):489–498.
11. Martino DJ, Szmulewicz AG, Valerio MP, Parker G. Melancholia: an attempt at definition based on a review of empirical data. J Nerv Ment Dis. 2019;207(9):792–798. doi:10.1097/NMD.0000000000001090
12. Parker G, McCraw S. The properties and utility of the CORE measure of melancholia. J Affect Disord. 2017;207:128–135. doi:10.1016/j.jad.2016.09.029
13. Tondo L, Vázquez GH, Baldessarini RJ. Melancholic versus nonmelancholic major depression compared. J Affect Disord. 2020;266:760–765. doi:10.1016/j.jad.2020.01.139
14. Sani G, Tondo L, Undurraga J, et al. Melancholia: does this ancient concept have contemporary utility? Int Rev Psychiatry. 2020;32(5–6):466–470. doi:10.1080/09540261.2019.1708708
15. Parker G, Fink M, Shorter E, et al. Issues for DSM-5: whither melancholia? The case for its classification as a distinct mood disorder. Am J Psychiatry. 2010;167(7):745–747. doi:10.1176/appi.ajp.2010.09101525
16. Nelson JC, Charney DS. The symptoms of major depressive illness. Am J Psychiatry. 1981;138(1):1–13.
17. Shorter E. The doctrine of the two depressions in historical perspective. Acta Psychiatr Scand. 2007;115(Suppl 433):5–13. doi:10.1111/j.1600-0447.2007.00957.x
18. Sadock BJ, Sadock VA. Kaplan & Sadock’s Synopsis of Psychiatry: Behavioral Sciences, Clinical Psychiatry.
19. Schneider K. Klinische Psychopathologie. [Clinical Psychopathology].
20. Huber G. Psychiatrie: Lehrbuch Für Studium Und Weiterbildung. [Psychiatry: A Textbook for Study and Training].
21. Jaspers K. Allgemeine Psychopathologie: Ein Leitfaden fur Studierende, Arzte und Psychologen. [General Psychopathology]. Berlin: Springer; 1913. German.
22. Schulte W. Studien Zur Heutigen Paychotherapie. [Studies on Today’s Psychotherapy]. Heidelberg: Quelle & Meyer; 1964. German.
23. Kasahara Y. Utsubyou no Byouzen Seikaku ni Tsuite. [On premorbid personality of depression]. In: Kasahara Y, editor. Souutsubyou No Seishin Byouri I [Psychopathology of Depression I]. Tokyo: Koubundou; 1976:1–29. Japanese.
24. Ohmae S. Rethinking the theory of melancholia (Tellenbach): its construction process and theoretical significance. Seishin Shinkeigaku Zasshi. 2013;115(7):711–728. Japanese.
25. Tellenbach H. Melancholie: Problemgeschichte, Endogenität, Typologie, Pathogenese, Klinik; Mit Einem Exkurs in Die Manisch‒melancholische Region. [Melancholy: History of the Problem, Endogeneity, Typology Pathogenesis, Clinical Considerations].
26. Sobin C, Sackeim HA. Psychomotor symptoms of depression. Am J Psychiatry. 1997;154(1):4–17.
27. van Diermen L, Vanmarcke S, Walther S, et al. Can psychomotor disturbance predict ECT outcome in depression? J Psychiatr Res. 2019;117:122–128. doi:10.1016/j.jpsychires.2019.07.009
28. American Psychiatric Association. Diagnostic and Statistical Manual for Mental Disorders.
29. Carney MW, Roth M, Garside RF. The diagnosis of depressive syndromes and the prediction of E.C.T. response. Br J Psychiatry. 1965;111:659–674. doi:10.1192/bjp.111.477.659
30. Parker G, Hadzi-Pavlovic D, Austin MP, et al. Sub-typing depression, I. Is psychomotor disturbance necessary and sufficient to the definition of melancholia? Psychol Med. 1995;25(4):815–823. doi:10.1017/S0033291700035066
31. Goodwin FK, Jamison KR. Manic-Depressive Illness: Bipolar Disorders and Reccurrent Depression.
32. Thase ME, Rush AJ. Treatment-resistant depression. In: Bloom FE, Kupfer DJ, editors. Psychopharmacology: The Fourth Generation of Progress. New York: Raven Press; 1995:1081–1097.
33. Muramatsu K, Miyaoka H, Kamijima K, et al. The patient health questionnaire, Japanese version: validity according to the mini-international neuropsychiatric interview-plus. Psychol Rep. 2007;101:952–960. doi:10.2466/pr0.101.3.952-960
34. Mayer-Gross W. The diagnosis of depression. Br Med J. 1954;2(4894):948–950. doi:10.1136/bmj.2.4894.948
35. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
36. Kendell RE. The classification of depressions: a review of contemporary confusion. Br J Psychiatry. 1976;129(1):15–28. doi:10.1192/bjp.129.1.15
37. Paykel ES. Classification of depressed patients: a cluster analysis derived grouping. Br J Psychiatry. 1971;118(544):275–288. doi:10.1192/bjp.118.544.275
38. Campbell JD. Mild manic-depressive psychosis, depressive type: psychiatric and clinical significance. J Nerv Ment Dis. 1950;112(3):206–236. doi:10.1097/00005053-195007000-00013
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.