Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Identifying Patterns of Turnover Intention Among Alabama Frontline Nurses in Hospital Settings During the COVID-19 Pandemic
Authors Cole A, Ali H ![]() , Ahmed A, Hamasha M
, Ahmed A, Hamasha M ![]() , Jordan S
, Jordan S
Received 13 March 2021
Accepted for publication 24 May 2021
Published 9 July 2021 Volume 2021:14 Pages 1783—1794
DOI https://doi.org/10.2147/JMDH.S308397
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 7
Editor who approved publication: Dr Scott Fraser
Astin Cole,1 Haneen Ali,2 Abdulaziz Ahmed,3 Mohammad Hamasha,4 Soren Jordan5
1Public Administration, Auburn University, Auburn, AL, USA; 2Health Services Administration Program, Auburn University, Auburn, AL, USA; 3Health Services Administration Program, University of Alabama at Birmingham, Birmingham, AL, USA; 4Department of Industrial and Systems Engineering, Hashemite University, Zarqa, Jordan; 5Department of Political Science, Auburn University, Auburn, AL, USA
Correspondence: Haneen Ali
Health Services Administration Program, Auburn University, 351 W Thach Concourse, 7080 Haley Center, Auburn, AL, 36849, USA
Email [email protected]
Introduction: Current research about frontline nurse stress and turnover intention lacks context related to rural communities’ plight in providing organizational resources during the current COVID-19 pandemic. These implications have been particularly underexamined in the United States, whose regional differences may influence how frontline nurses perceive the access and utility of organizational resources. This study investigates if anxiety and stress while working during the current COVID-19 pandemic contribute to frontline nurses’ desire to leave their current position in Alabama hospital settings.
Material and Methods: A cross-sectional survey was developed and distributed as a Qualtrics survey to frontline nurses using social media and professional contacts. A total of 111 frontline nurse respondents within May 19–June 12, 2020 were included in this study.
Results: A significant correlation was found between gender (p= 0.002), marital status (p= 0.000) and seniority (p= 0.049) on turnover intention. A nurse’s perceived anxiety and stress related to their patients’ acuity (r= 0.257, p= 0.004), their personal health as a risk factor (r= 0.507, p= 0.000), their patient assignments (r= 0.239, p= 0.01), their personal protective equipment (r= 0.412, p= 0.000), and their psychological support (r= 0.316, p= 0.001) correspond to higher turnover intention among nurses working with patients infected with COVID-19.
Conclusion: Perceived resource loss in task autonomy, PPE, and psychosocial support increased turnover intention among frontline nurses in Alabama. Research is needed to understand how intrinsic motivations and social support influence individual nurse staff’s perceptions of resource loss and job demands. Further, more research is necessary to examine the implications of rurality and place in discussing turnover intention and organizational resources across multiple health systems.
Keywords: pandemic, COVID-19, nurse stress, fear, job demand, organizational resources, turnover intention
Introduction
Due to the COVID-19 pandemic, current health systems, businesses, school systems, and public service agencies are struggling to control the spread of the infection through stricter safety regulations, social distancing requirements, and more frequent COVID-19 testing. In addition to greater professional requirements, the current public health climate provides a host of challenges like those observed in previous pandemic literature.1–3 Due to the speed and spread of the infection, it is expected that many health systems are struggling to cope with the resource scarcity and personnel demands of the current pandemic.4,5 This exponential demand in health worker personnel translates into higher stress levels and risks for frontline nurses currently working in hospital settings.4–9 For frontline nurses, this stress may increase with the number of infected patients, thereby raising their concerns about their health risks and the risk of spreading the infection to their loved ones.4,9,10 Additionally, current frontline nurses must face long working hours amid reports of personal protective equipment (PPE) and ventilator shoratges, thereby making frontline nurses feel especially vulnerable to additional job demands.9,11 In such cases, nurses perceiving a high level of stress and anxiety may feel helpless, fatigued, depressed, and burned out.4,9,10 Ultimately, these feelings might lead nurses to consider leaving their job or assessing their career choices.4,5,8,12–14 Turnover intention, then, provides the best proxy measurement of whether a frontline nurse plans to leave their current position.4,5,8,12–14
As Alabama is one of the poorest states, its capacity to respond to and treat patients infected with COVID-19 is limited compared to larger, wealthier states.9,13,15 Nurses that are willing to work with acutely infectious patients in these settings may feel that their job presents a moral imperative, thereby reducing their turnover intention.9,13,15,16 This assumption would be consistent with much of the health administration literature regarding frontline nurses during the COVID-19 pandemic, which finds that frontline nurses continue to exhibit high internal motivation while working with infectious patients.16–18 However, other studies report nurses showing the desire to leave their current positions due to heightened feelings of fear and anxiety related to working during the pandemic.10
Nurses are assumed to exhibit intrinsic motivations that compel them to work longer hours despite experiencing additional stress, such as higher patient treatment complexity, stricter safety regulations, and more significant occupational risks.10,19–22 Ali et al (2020) found that Alabama frontline nurses exhibited heightened feelings of stress and anxiety due to working with patients infected with COVID-1911 and significant concerns about the increasing number of infected patients.9 Previous research shows that higher stress and anxiety levels and feelings of burnout related to the current pandemic are contributing to higher levels of reported turnover intention in numerous hospital settings.10,19,21,23 This study will investigate if psychological anxiety resulting from perceived job demand and organizational resources contributes to increased turnover intention. This study will answer the following research questions:
- What factors related to frontline nurse job demand stress and anxiety contribute to turnover intention?
- To what extent do stress and anxiety related to shortages in organizational resources contribute to turnover intention among frontline hospital nurses?
Recent studies related to nurse stress find that many hospitals are overestimating the resilience of nurses in keeping up with the demands of patient care during the COVID-19 pandemic.4,5,8,12–14,24 Due to their professional obligations to provide patients with the best treatment possible, many nurses may feel the emotional and mental stress of watching their patient’s health quickly deteriorate due to worsening symptoms.9,14,25 As one nurse from the initial design phase stated:
The only times I think to myself ‘this job sucks’ is when I have to hear families talk to their loved one before they are put on ventilators. It is so incredibly said because everyone is so sad and scared for them, and the patient is usually weak since they are put on ventilators far too late. I just hold up an IPad or phone while they say goodbye to their loved one because they are more than likely not being taken off the ventilator once put on. Like, it makes me cry just thinking about it.
This suggests that frontline nurses during this time may feel that their health systems are struggling to treat patients and that these gaps are worsening the emotional stress felt by nurses during a routine but crucial job function.1–4 Ethically, nurses may experience moral injury, as they must balance their responsibility to safeguard patient welfare and provide patient satisfaction with their fear, anxiety, and emotional fatigue surrounding the pandemic.9,14,25
Psychological anxiety resulting from job demands during the COVID-19 may help to explain the ethical component to patient services that appear to exacerbate nurse stress.9,14,25 In this case, a frontline nurse’s inability to provide patient services, particularly in cases where the nurse perceives gaps in their training and the patient’s treatment complexity, is expected to lead to high turnover intention.4,5,8,12–14,24
Their perceived access to organizational support also influences frontline nurse stress.4,5,8,12–14,24 A reliance on organizational resources for employees in ethically salient job positions is consistent among a wide range of organizations.16,17,26–28 Organizational resources and a positive work environment help reduce turnover intention.16,17,26–28 These resources included providing promotion opportunities, compensation raises, and supervisor support.27,29–33 Organizational resources can also reduce burnout.16,17,26–28 However, it is unclear whether nurses perceive greater turnover intention from a perceived lack of organizational resources.19,20,34,35 The psychological anxiety and stressors resulting from a lack of organizational resources worsen during a pandemic, whereby nurse-patient interactions now require stricter PPE and are limited by additional COVID-19 regulations to ensure their safety and patient safety.3,9,19,36,37 Studies suggest that it is unclear the extent that nurses perceive access and benefits to psychiatric consultation.9 If nurses do not perceive access to psychosocial support, they may experience gaps in their ability to cope with the current pandemic through healthy means. Further, they may also experience resource loss due to increasing job demand due to a lack of additional (or accessible) resources. Results from a previous study found that very few, if any, nurses in Alabama were currently using psychosocial support as a coping mechanism, thereby reducing the chances that such programs have of effectively reducing turnover intention.9 As a result, additional research is needed to understand how nurses perceive stress related to a lack of psychological support.16,27,28,38
While the literature has already identified characteristics related to nursing turnover, few studies have engaged in research designed to investigate the implications of perceived shortages in organizational resources on turnover intention in health systems located in poor states.10,12–14,39,40 Additionally, more research is needed to investigate the perceived lack of organizational resources on current frontline nurse turnover intention in hospital settings. As a result, questions remain about the motives of turnover intention among individual staff and what stressors related to job demands and organizational resources correspond to turnover intention.
The Current Study
This study is a continuation of the conversation of resources theory by Hobfoll (1989; 2000; 2018).41–43 According to the theory, a significant physical and mental/emotional loss could result from continuous stress in the work environment and lead to different coping strategies. Further, the perception of resource loss and gaps in organizational support can worsen the effects of continuous stress in the work environment.41–43 This study investigates if nurses are more likely to consider quitting their job due to the psychological anxiety and stress resulting from job demand and organizational resources during the COVID-19 pandemic. According to Hobfoll (1989; 2000; 2018), people seek different coping strategies when they work under a lack of emotional, psychological, and physical environment.41–43 This study provides further context to the growing turnover intention literature by observing the state of Alabama in the United States. The state’s health system reflects many of the communities in the Southeast region, given its reliance on a handful of major health systems and largely rural population.9,15 This study investigates to what degree turnover intention is a coping strategy resulting from the stressors from the nurses’ job demand and lack of resources among nurses in Alabama.
Figure 1 provides a model that describes the occupational stress leading to turnover intention due to both internal and external effects, which increase the perceived difficulty of performing nurse tasks. Job demands measure the stress and anxiety caused by job demands that directly impact nurse tasks’ perceived difficulty. This domain includes patient acuity, task assignment, stress related to personal protective equipment (PPE), and personal health as a stress factor.17,29 Organizational resources measure the stress and anxiety caused by a perceived lack of resources in the work environment which indirectly impacts the perceived ease of nurse tasks. This domain includes PPE, psychosocial support, supervisor support, and compensation.27,29–33 Figure 1 reflects how nurses are ultimately seeking to balance the “burden of prevailing circumstances” related to personal and job external factors and the clinical status of patients.12,44,45 It suggests that increases in stress and anxiety related to job demand and the stress and anxiety related to work environments will result in a desire to quit.29,41,43,46 Further, this model hypothesizes that perceptions of resources lost may also increase turnover intention by also increasing stress.29,42,43,46
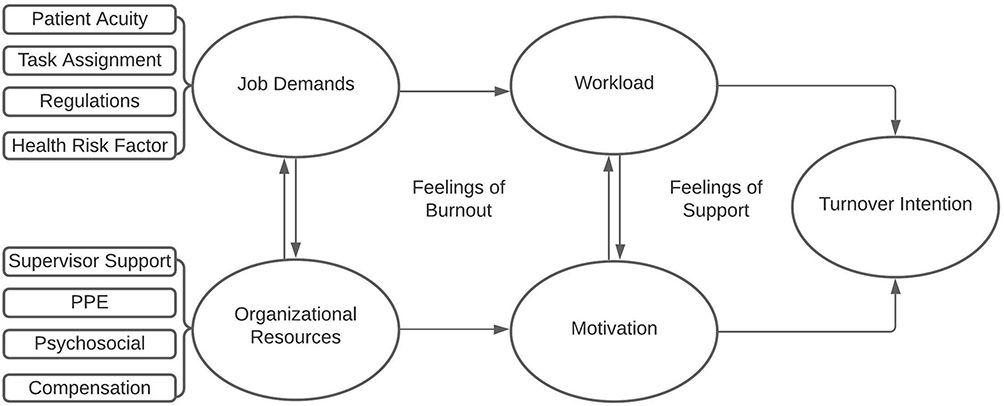 |
Figure 1 The theoretical framework of this study. Depicts turnover intention as a relationship between job demands and perceptions organizational resources. |
Materials and Methods
Research Design
Cross-sectional designs help gain insights from initial examinations of a new research area and ruling out explanations in more developed areas of inquiry.47 While the study of nurse turnover intention in the United States is not a new concept, relevant observations are sparse, with no notable update in the 21st century.12 It therefore makes sense to begin this area of inquiry with a minimal design to determine with initial evidence whether the research area of turnover intention in rural regions of the United States is worth more attention.
A cross-sectional survey was administered to frontline nurses who worked with COVID-19 infected patients in the last three months in hospital settings in Alabama. The nurses were invited to participate through social media platforms such as LinkedIn and share information about this study’s purpose. This study shared an online link to a Qualtrics survey with currently employed frontline nurses along with a consent form. The largest factor in the design choice stemmed from a lack of willing health systems to provide access to many nurses.12 Not only were health risk factors a cited issue but health systems are disincentivized from disclosing potentially sensitive information related to gaps in their organizational resources. As a result, this cross-sectional design was used as an efficient alternative to scarce researcher resources.47
This study was approved by the Auburn University Institutional Review Board (IRB reference # is: 20–238 EX 2005) per the Declaration of Helsinki. Participants were compensated for their time. This study’s inclusion criteria specified only Alabama nurses working directly with COVID-19 patients within the last three months from the collection start date. Participants were notified about the aims of the project and the risks that might be associated with the survey study. They were also notified that no identifiable information would be collected because their participation was voluntary, and by completing the survey, they agree to participate in this study. Informed consent was provided at the beginning of each survey.
Questionnaire Development
Principal items were developed based on the questionnaire designed by Lee et al (2005) that were used to investigate medical staff during the 2003 SARS epidemic. Ali et al (2020) investigated major psychological stressors resulting from COVID-19 in Alabama following Cai et al, who evaluated the COVID-19 related stress factors among the medical staff in Hubei, China.3,9,19 Lastly, Labrague (2020) provided further evidence of frontline nurse turnover intention in the Philippines.8 A preliminary list of 37 items was created for the eight constructs in the three major domains according to Figure 1 and demographic characteristics. A full list of the items is provided in Appendix 1.
The preliminary list was distributed to a group of experts in the field with research experience (two ICU nurses, one general nurse, one nursing faculty, one hospital administrator, two nurse managers). After one week, a virtual focus session was conducted with the experts to discuss the preliminary list of items. As a result of the experts’ feedback, four items were removed, and six items were revised.
The questionnaire consists of four major domains: demographic characteristics, job demands, organizational resources, and turnover intention. Job demands and organizational resources are captured using eight constructs. Perception of stress from job demands is categorized as a patient assignment, patient acuity, stress related to lack PPE, and stress caused by a lack of psychosocial support. Perceptions of organizational resources are categorized as PPE, psychosocial support, supervisor support, and compensation. The questionnaire instrument is comprised of demographic and work-related questions (eight items), stress from job demands and workload (fourteen items divided into four constructs), perceptions of organizational support and resources (thirteen items divided into four constructs), and turnover intention (two items).
The items were measured along a five-point Likert scale, from strongly disagree to strongly agree.48
Reliability and Validity
All necessary tests were performed to assess the items’ interrelatedness within each construct. Additional reliability tests included a pilot survey that was distributed to ten frontline nurses in Auburn, AL who were invited to participate through social media platforms. Reliability was assessed using Cronbach’s alpha, which reflects the interrelatedness among the items in each construct, and Cronbach’s alpha value ranged from 0.70–0.91, see Table 1. Stability test-retest overtime was not tested. Validity was reviewed by the focus group to assess the quality and clarity of the questions asked, the time it takes to complete the survey, and whether the list of questions appears comprehensive.
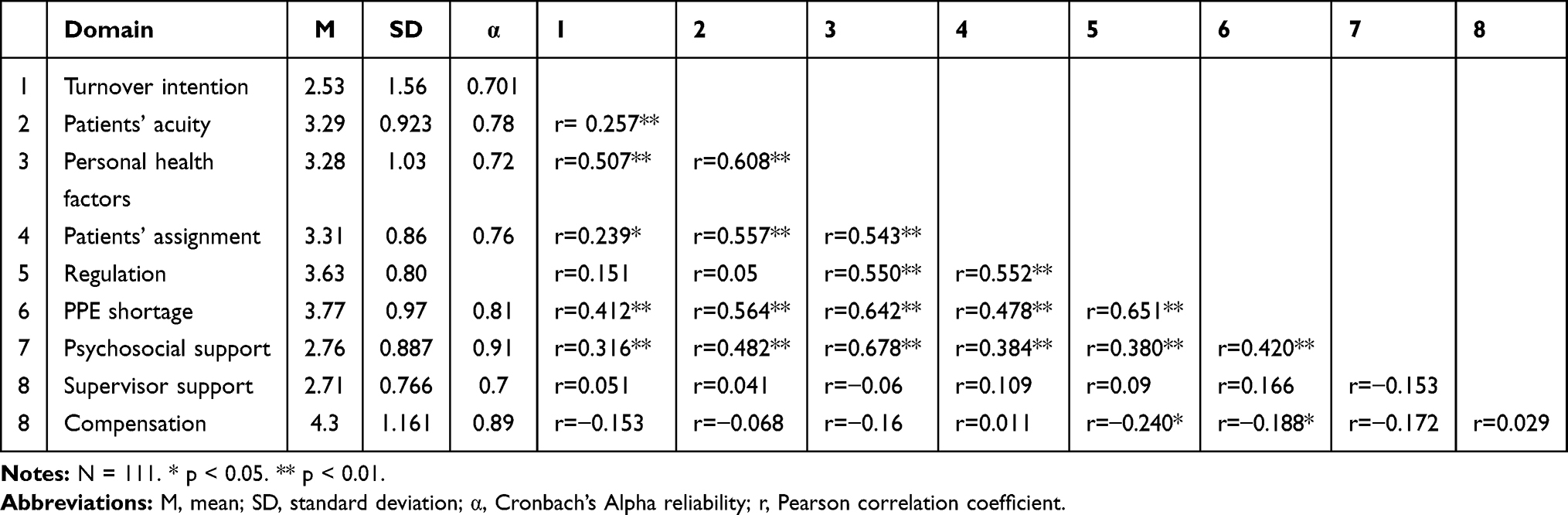 |
Table 1 Means, Standard Deviations, and Correlations |
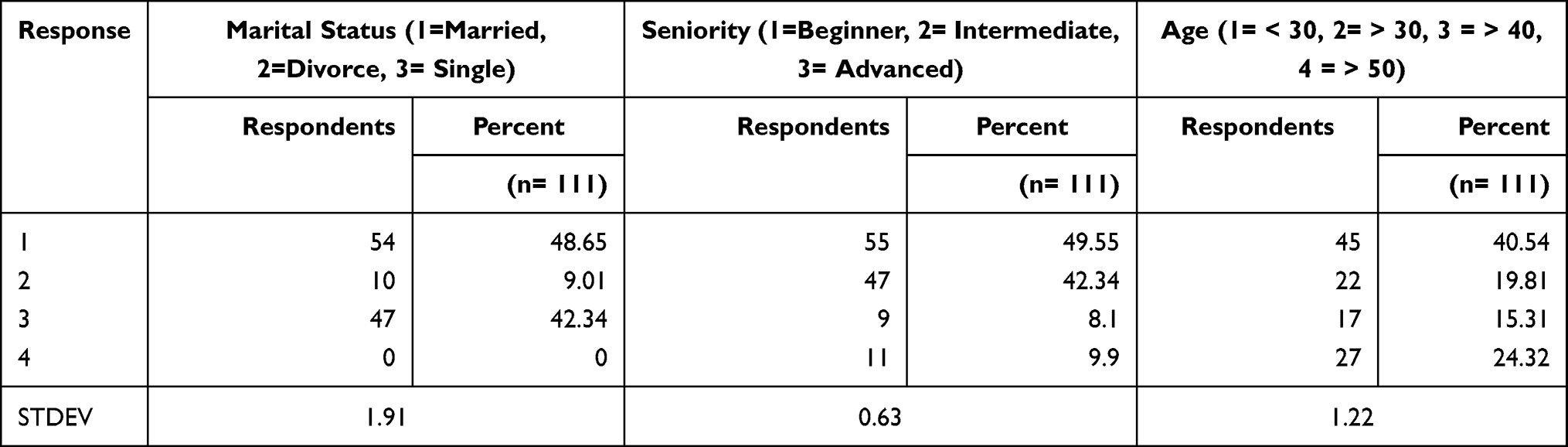 |
Table 2 Descriptive Statistics of Demographics |
Measures
Job Demand Domain
This domain refers to the perceived level of psychological anxiety and stress resulting from job demands and workload resulting from COVID-19. This was measured by four constructs.4–9,42
Patient Acuity Construct
Patient acuity refers to the perceived degree of care and attention a patient’s treatment requires. While nurses are educated to handle a wide range of patient complexity, the current pandemic brings more opportunities for them to become overwhelmed in dealing with the rapid deterioration of their patients. Nurses who report feeling overwhelmed by their patients’ complexity of treatment also report lower job satisfaction. Three items were used to capture the perceived level of anxiety and stress caused by increased intensity, effort, or complexity in completing tasks for a patient.9,21
Patient Assignment Construct
Due to the high demand for frontline nurses during a pandemic, high instances of nurses being asked, or required, to work with patients infected with COVID-19 can be expected.19 Previous studies suggest that task autonomy, or the freedom of task assignment, is associated with job satisfaction, workload, and turnover intention among experienced nurses. Studies suggest that a lack of autonomy is associated with higher instances of turnover intention among nurses.10,12,13,39 Three items used captures the perceived level of anxiety and stress caused by a lack of autonomy.
COVID-19 Regulations Construct
Healthcare workers in the United States are mandated to wear PPE, such as an N95 face mask while attending to patients.49 Additional protective equipment, such as face shields and other protective eyewear, is mandated in most high-risk areas in the United States.49 Studies have found that while this equipment reduces risks of infection, the elastic band that is used to hold these devices around faces has been linked to shortness of breath and trouble breathing,11 as well as ear pain near or around the temple, which have been linked to headaches caused by the compression of peri-cranial soft tissue.16 Five items were used to capture the perceived level of anxiety and stress caused by compliance to COVID-19 regulations.
Health as a Personal Risk Factor Construct
Nurses who feel heightened levels of stress and anxiety have been found to also experience adverse health effects such as insomnia, depression, overeating, and suicidal thoughts.50–52 A longitudinal analysis of nurse suicide in the United States found that nurses were at greater risk of suicide than the general population.50 The study cited the use of opioids and benzodiazepines as a form of pharmacologic poisoning from substance abuse or adverse events such as deaths caused by overdose.50 Ali et al (2020) also found a small percentage (5.5%) of frontline nurses reporting alcohol consumption to cope with sources of stress caused by COVID-19.9 Substance abuse, in addition to other negative coping habits, has been linked to nurses suffering from continuously high levels of stress and long work hours.51 Three items were used to captures the perceived level of anxiety and stress that impacts their health.
Organizational Resource Domain
The perceived benefit for organizational resources measures the extent that frontline nurses perceive organizational resources reducing the stress caused by job demands.4–9,42 The domain is often categorized by job-specific resources such as access to materials and supplies, occupational resources such as safety and stress management, and professional resources such as compensation and supervisor support.4–9,42 This study expects that organizational resources reduce turnover intention caused by stress due to current COVID-19 job demands. Further, this study expects that perceived resource loss increases turnover intention.
PPE and Medical Equipment (ME) Construct
PPE refers to occupational resources related to health and safety, such as latex gloves and N95 face masks.3,19,37,49 Previous studies on frontline nurse stress and nurse satisfaction in hospital settings suggest that a lack of crucial medical equipment such as ventilators is associated with higher stress and job satisfaction.9,52 Medical equipment refers to essential medical devices and technology needed to provide patient services.52 Three items were used to measure the perceived level of anxiety and stress resulting from news related to shortages in PPE and ME.
Compensation Construct
Compensation refers to the perceived level of access to resources that enable frontline nurses to socially cope with long work hours and greater risk factors associated with their occupation.9 One item was used to capture perceived benefits from additional rewards and benefits from working during the pandemic.
Psychosocial Support Construct
Psychosocial support refers to the perceived level of access to resources that enable frontline nurses to engage in healthy psychosocial activities and habits such as psychological therapy, engaging in communication with family and friends, and attending religious services.3,9,19,36,37 Five items were used to capture the perceived levels of benefits from psychosocial support to reduce the level of anxiety and stress.
Supervisor Support Construct
Supervisor support refers to the perceived level of access to resources that enables frontline nurses to engage in communication and feedback with their supervisors actively.4–9,42 Supervisor support has been found to help buffer the effects of job demands by encouraging nurses to form interpersonal connections with management staff and promote a healthier working environment through the process of work-group cohesion.3,9,19,36,37 Four items were used to capture the perceived levels of benefits from additional supervisor support.
Turnover Intention Domain
Turnover intention is defined as the nurse’s desire to leave their current position.4–9,42 Turnover intention is a proxy measure used to capture the feelings that lead to leaving the position.4–9,42 Turnover intention was captured by asking nurses if they thought about leaving due to feelings of burnout and by asking nurses if they consider leaving as the COVID-19 infection rate increases.
Statistical Analysis
Data from completed questionnaires were processed and analyzed using R Studio version 1.2.5001, a software platform that uses R computing language for statistical analysis. Descriptive statistics such as mean value, standard deviation, frequency, and mean responses were used to describe respondent characteristics and reactions to turnover intention. Analysis of Variance (ANOVA) was used to investigate the relationship between the demographic information and the turnover intention in addition to the other measured constructs. Pearson correlations were conducted to assess the strength and direction of relationships between the constructs.
Results
A total of 150 hospital nurses were invited to take the survey. 141 hospital nurses responded to the survey; however, twelve did not complete the survey, and Qualtrics verified eighteen as working outside of Alabama. As a result, 111 surveys were collected in the time between May 19 - June 12, 2020.
Descriptive Statistics
Table 2 provides the demographic characteristics of the respondents. It suggests that respondents were relatively young, with 40% (n= 45) under thirty years old. Respondents were also less experienced, with only 8% (n= 9) of the participants reported having a senior-level (over 15 years of experience) status. Lastly, the distribution of nurses along marital status was relatively even, with around 48% (n= 54) of the participants reporting they were married compared to the 42% (n= 47) reporting they were single (never married) with 35% (n= 39) reporting having children.
Regression Analysis
ANOVA was used to examine the relationship between the demographic information and the constructs.
Turnover Intention
ANOVA shows a significant correlation between gender (p= 0.002), material status (p= 0.000), seniority (p= 0.049), and turnover intention. Married and senior nurses gave a higher score for turnover intention. Nurses with children also gave a higher score, but it was not found to be significant.
Stress Resulting from Perceptions of Patients’ Acuity
More than 64% (n= 76) of nurses reported stress and anxiety related to patients’ acuity. The results from the ANOVA found that a nurse’s age, gender, and specialty were significantly correlated with stress resulting from patients’ acuity (p= 0.01, 0.02, 0.002, respectively). Female (average score= 3.5) and younger (average score= 3.7) nurses reported higher perceived stress resulting from patients’ acuity than male nurses and older nurses.
Anxiety and Stress Resulting from Personal Health Risk
Sixty-six percent (n= 73) of nurses agreed with having concerns and stress related to their health risks. More than 86% (n= 95) of nurses reported more stress and anxiety levels than before COVID-19. Gender, marital status, having children, seniority, specialty, and shifts were significant to the anxiety and stress resulting from personal risk factors (p= 0.004, 0.000, 0.001, 0.03, 0.037, respectively). Married nurses with children and younger nurses reported higher stress and anxiety levels.
Patient Assignment
More than 69% (n= 77) of nurses reported stress and anxiety resulting from patients infected with COVID-19. Around 66% (n= 70) reported concerns about having to take care of a colleague. Age, gender, marital status, and seniority were found to have a significant effect on anxiety and stress levels resulting from the patient assignment (p= 0.001, 0.000, 0.002, 0.000). Single, female, and younger nurses reported higher levels of anxiety and stress.
Regulation
More than 80% (n= 92) of nurses are stressed and anxious about continuous changes in regulations related to COVID-19. Around 70% (n= 77) of nurses are stressed and worried about wearing the face mask all the time, and 68% (n= 67) are stressed about constantly being screened for COVID-19. In general, more than 76% (85) have anxiety and stress resulting from COVID-19 related items. Gender, marital status, seniority, and specialty were found to have significant effects on regulation constructs (p < 0.004). Female, single, and younger nurses reported higher levels of anxiety and stress resulting from changing or lack of regulations. ICU and ER nurses also reported more stress and anxiety levels related to regulation constructs.
PPE & ME
More than 89% (99) experienced stress and anxiety from hearing the news about the PPE shortage. More than 76% (85) experienced stress from reports of ventilator shortages. Gender, material status, having children, seniority, and specialty all had significant relationships with PPE constructs (p < 0.05). Young, single, and childless nurses reported higher levels of anxiety and stress. ICU nurses also reported higher levels.
Psychosocial Support
Around 52% (58) reported concerns about lack of psychological support for patient care. Thirty percent (33) of nurses believe they could benefit from psychological care themselves, while 11% (13) reported needing grief counseling, 16% (18) reported needing trauma counseling, and only six nurses reported needing family counseling. Gender, seniority, specialty, and shift were found to be significant factors (p < 0.05). For example, young, female nurses working morning shifts reported higher levels of stress and anxiety related to psychological support.
Supervisor Support
More than 37% (42) of nurses reported that supervisors cared about their opinions. Forty-one percent (46) agreed that supervisors cared about their well-being, but more than 54% (61) reported that supervisors showed little concern for the nurses. Only age was significant (p= 0.018) with young nurses reporting higher stress levels resulting from supervisor support.
Compensation
Seventy-seven percent (86) of nurses thought they should be compensated for the workload and risks associated with working during COVID-19. Age and seniority were found to be significant factors (p= 0.000, 0.0049 respectively), with younger nurses expecting to be compensated for the workload resulting from COVID-19.
Correlation Analysis
Pearson correlations were checked to identify significant relationships between the constructs, as shown in Table 1 (the list of survey items and their mean scores are provided in Supplementary Table S1). Perceived psychological anxiety and stress resulting from the patients’ acuity (r= 0.257, p= 0.004), personal health factors (r= 0.507, p= 0.000), patients’ assignments (r= 0.239, p= 0.01), PPE shortage (r= 0.412, p= 0.000), and psychological support (r= 0.316, p= 0.001) were all found to be positively related to turnover intention. Patient assignments (r= 0.543, p= 0.000), regulation (r= 0.55, p= 0.000), PPE shortage (r= 0.642, p= 0.000), psychological support (r= 0.678, p= 0.000) were found to be positively related to the perceived stress and anxiety resulting from personal health factors. PPE shortage (r= 0.478, p= 0.000) and psychological support (r= 0.384, p= 0.000) were found to have a positive relation with anxiety and stress resulting from changes in regulations. Supervisor support was not found to have strong relations with any of the other constructs. Stress resulting from PPE shortage (r= 0.384, p= 0.000) was found to be positively related to perceived psychological support.
Discussion
The COVID-19 pandemic continues to be a significant threat to people’s psychological health, especially frontline workers.4–9,42 Previous studies show that nurses fear getting the virus, shortages in PPE and ventilators, and psychological anxiety resulting from COVID-19 could lead them to revisit their career options or leave their job.4–9,42 This study contributes to the literature by investigating the primary cause of psychological stressors faced by frontline nurses in Alabama and their behavioral outcomes resulting from stress due to turnover intention. This study proposed eight major construct causes of psychological anxiety and stress that nurses face as crucial predictors of turnover intention. The results presented by this study concur with the other tasks and show that job demands, and the lack of resources provided by the organization are causing anxiety and stress and forcing nurses to reassess their career choices.4–9,42 This study finds evidence that stress and anxiety caused by the current pandemic influence the perceived stress related to job demand and organizational resources of frontline nurses in Alabama. Following a discussion of notable factors of turnover intention, we provide suggestions on how these influences translate into individual and work-environment job factors that hospitals can address in future recruitment and stress management interventions.
Stress and Anxiety Related to Demographic Variables
This study found significant differences in the demographic characteristics of turnover intention between nurses. In addition, the results show that seniority and marital status were significant demographic factors for turnover intention due to fear of increasing COVID-19 infection rates.
As stated previously, age correlated strongly with seniority in the initial analysis. While studies involving nurse stress find that more experienced nurses can cope with greater patient acuity, highly experienced nurses may feel increased risks to their health.3,9,19,36,37 It makes sense that seniority was a significant indicator of turnover intention. In addition, evidence was found for the effects of fear and burnout on frontline nurses concerning their marital status, as married respondents were found to have a greater desire to leave than single (never-married) nurses. This study expected additional loved ones, such as spouses and children, to increase anxiety caused by working as a frontline nurse.
While parental status (from not having children to having children) was not found to increase turnover intention significantly, this study found that marital status (from married to being single) increased turnover intention for both fear and burnout, respectively. This suggests that nurses may perceive the virus from the perspective of less dangerous to children simply because it is more dangerous for elderly individuals.11 This corresponds with seniority, which correlated strongly with age and was significant in explaining turnover intention. Regarding marital status, this measure may capture aspects related to perceived limited access to social support in addition to a perceived increase in potential risks in spreading the virus to an intimate partner.11 These findings are consistent with studies investigating the effects of parental and marital status on the perception of workload and social support for nurses in hospital settings.9,29,32,53–55
Stress and Anxiety Related to Job Demand Factors
Perceived psychological anxiety and stress resulting from patient acuity, patient assignment, and personal health as risk factors were found to significantly contribute to turnover intention among nursing staff in the state of Alabama. Stress caused by reports of PPE and ventilators and lack of psychosocial support were the only organizational resources that were found to be related to turnover intention.
Patient acuity and personal risk factors were significant contributors to turnover intention. Patient acuity and personal risk are factors that were found to have been heightened in highly stressful environments. Both factors are also prevalent indicators to measure the perceived and output of intense workloads.9,12,19,21,40,52 These findings are consistent with the literature regarding the relationship between patient acuity and workload on stress, negative health outcomes, and feelings of burnout.12,19,21,40 Additionally, frontline nurses are not only scared of getting infected,3,9,19,36,37 but they also experience heightened fears and anxiety from the risk of becoming asymptomatic carriers and unknowingly amplify the spread of the infection.3,9,19,36,37
Patient assignment significantly affected the fear on personal health among nurses due to nurses’ work environments in hospital settings. Task autonomy related to patient assignment can vary from relative flexibility to a complete lack of autonomy.12,19,21,40 In cases where nurses must work during a pandemic, the literature suggests it is difficult to avoid working or interacting with patients infected with COVID-19.12,19,21,40 Recent studies related to nurse stress find that many hospitals may be overestimating the resilience of nurse staff in keeping up with the demands of patient-centered care during the COVID-19 pandemic.10,22,56 Due to their professional obligations to provide patients with the best treatment possible, many nurses may feel the emotional and mental stress of watching their patient’s health quickly deteriorate due to worsening symptoms9 or due to a lack of resources such as ventilators.10,20,23,57 Ethically, nurses may experience compassion fatigue or moral injury, as they must balance their perceived responsibility to safeguard patient welfare with the fear and anxiety of getting infected and amplifying the spread of the infection.25,57 These results are consistent with qualitative and empirical research that found many nurses feel they are being pushed beyond their limits.12,19,21,40 Frontline nurses during this time have limited team support due to the number of professionals allowed in the room with the patient, as well as time constraints related to the suggested time nurses can be in the rooms with patients.9 Given the unique work environment many nurses face in current hospital settings, more qualitative research is needed to better understand the extent that supervisors can provide meaningful support. It remains unclear the extent that positive communication affects nurses that lack physical interaction with colleagues and supervisors.
Ali et al (2020) found that no frontline hospital nurse staff in Alabama reported seeking psychological treatment or counseling.9 However, psychosocial support was found to reduce turnover intention significantly due to feelings of anxiety or stress. While many international studies suggest that psychosocial support is sufficiently provided to frontline nurses in hospital settings, this may not be the case in the United States.3,19,36,37 This study’s findings suggest that frontline nurses need additional psychosocial support to overcome wanting to leave their position due to feelings of burnout.
Potential Public Service Motivations and Suggestions for Intervention
Compensation was not found to be significant. However, scholars such as Knapp et al (2017) suggest that differences in intrinsic motivations related to public service motivations can help explain why some nurses may perceive stress related to their current tasks and work environment, as well as the benefit of compensation.16 Additional research is needed to understand the relationship between intrinsic motivations, compensation, and turnover intention for nurses working in hospital settings, which accounts for both temporal factors related to a decline in intrinsic motivation and changes in the perceived utility of organizational resources over time.
This study offers two suggestions related to future recruitment and stress management functions. First, this study’s findings suggest that less experienced nurses (five years or less) and senior nurses (over fifteen years) had significantly higher stress levels. Second, many hospitals are currently recruiting nurses using sign-on bonuses. While Knapp et al (2017) finds compensation to be impactful in positions of low income and high moral importance, the nursing profession was already a well-paid job that suffered from turnover before the pandemic.16 As a result, nurse recruitment may need to focus less on financial incentives and more on targeting individuals who would view the position as a “calling” rather than a career.
Ali et al (2020) found that none of the nurses who were surveyed reported using psychological counseling. The authors suggest that access to psychosocial support may be limited or non-existent in Alabama hospitals.9 This study finds that the stress and anxiety caused by a lack of perceived psychosocial support correspond to greater turnover intention. As a result, this study provides further evidence of what scholars have already known, that greater access to resources is needed to reduce the impact of nurse stress on organizational outcomes. While this design cannot test the extent to which access plays a part in the perceived stress of resource shortages, the results suggest that nurses desire greater access.
Limitations and Future Research
This cross-sectional study on hospital nurses helped to identify unique patterns related to motives for turnover intention. However, this study lacked the sample diversity and size to properly test our model on different organization-level dimensions found relevant to turnover intention such as organization-type and relational dimensions such as religiosity and public service motivation.16 This study also lacked a proper “baseline” statistic to compare nurse turnover intention in a similar environment before the COVID-19 pandemic. This study’s unique relationships and patterns provide evidence to help formulate causal models for turnover intention. These insights must be tested with a more extensive and more diverse range of nurses to test the implications properly. Ideally, this test would include comparative data for discussing differences between nurses among different levels of hospital management (nurse, head nurse, and nurse manager) within other hospital units to identify differences in specialty and within different hospital types (public, nonprofit, private). The limited data on private hospitals requires that scholarship provides alternatives to direct observational comparisons.
Conclusion
This study’s findings suggest that the variations in the turnover intention for frontline nurses in hospital settings can be explained as a relationship between resources and job demands. Additionally, this study found variations between job demand stress sources and organizational resources related to fears of increasing COVID-19 infection rates and feelings of burnout. By investigating the differences in turnover intention due to workload, this study identifies and provides insights into why turnover intention occurs during the pandemic, how stress related to job demands contributes to turnover intention, and what organizational resources help reduce motivations for turnover intention. These findings are consistent with studies that look at ways to improve work processes by investigating relationships between perceived workloads and gaps in organizational support.9,14,19,20,52,55,58
Acknowledgment
The authors would like to thank Auburn University for supporting this research project. This study was funded through Dr. Ali’s (corresponding author) start-up funds.
Disclosure
The authors have no conflicts of interest to disclose for this work.
References
1. Lowcock EC, Rosella LC, Foisy J, McGeer A, Crowcroft N. The social determinants of health and pandemic H1N1 2009 influenza severity. Am J Public Health. 2012;102(8):e51–e58. doi:10.2105/AJPH.2012.300814
2. Goulia P, Mantas C, Dimitroula D, Mantis D, Hyphantis T. General hospital staff worries, perceived sufficiency of information and associated psychological distress during the A/H1N1 influenza pandemic. BMC Infect Dis. 2010;10:1. doi:10.1186/1471-2334-10-322
3. Lee S-H, Juang -Y-Y, Su Y-J, Lee H-L, Lin Y-H, Chao -C-C. Facing SARS: psychological impacts on SARS team nurses and psychiatric services in a Taiwan general hospital. Gen Hosp Psychiatry. 2005;27(5):352–358. doi:10.1016/j.genhosppsych.2005.04.007
4. Boudrias V, Trépanier S-G, Foucreault A, Peterson C, Fernet C. Investigating the role of psychological need satisfaction as a moderator in the relationship between job demands and turnover intention among nurses. Empl Relat Int J. 2020;42(1):213–231. doi:10.1108/ER-10-2018-0277
5. Wan Q, Li Z, Zhou W, Shang S. Effects of work environment and job characteristics on the turnover intention of experienced nurses: the mediating role of work engagement. J Adv Nurs. 2018;74(6):1332–1341. doi:10.1111/jan.13528
6. Del Carmen Giménez-Espert M, Prado-Gascó V, Soto-Rubio A. Psychosocial risks, work engagement, and job satisfaction of nurses during COVID-19 pandemic. Front Public Health. 2020;8:753.
7. Muller AE, Hafstad EV, Himmels JPW, et al. The mental health impact of the covid-19 pandemic on healthcare workers, and interventions to help them: a rapid systematic review. Psychiatry Res. 2020;293:113441. doi:10.1016/j.psychres.2020.113441
8. Labrague LJ, de Los Santos JAA, Falguera CC, et al. Predictors of nurses’ turnover intention at one and five years’ time. Int Nurs Rev. 2020;67(2):191–198. doi:10.1111/inr.12581
9. Ali H, Cole A, Abdulaziz A, Hamasha S, Hamasha M. Major stressors and coping strategies of frontline nursing staff during the outbreak of Coronavirus Disease 2020 (COVID-19) in Alabama. J Multidiscip Healthc. 2020;Volume 13:2057–2068. doi:10.2147/JMDH.S285933
10. Labrague LJ, de Los Santos JAA. Fear of COVID-19, psychological distress, work satisfaction and turnover intention among frontline nurses. J Nurs Manag. 2020. doi:10.1111/jonm.13168
11. Purushothaman PK, Priyangha E, Vaidhyswaran R. Effects of prolonged use of facemask on healthcare workers in tertiary care hospital during COVID-19 pandemic. Indian J Otolaryngol Head Neck Surg. 2020. doi:10.1007/s12070-020-02124-0
12. Cavanagh SJ. Predictors of nursing staff turnover. J Adv Nurs. 1990;15(3):373–380. doi:10.1111/j.1365-2648.1990.tb01825.x
13. Shader K, Broome ME, Carroll broome FD, Ellen West M, Mary Nash R, Karen shader F. Factors influencing satisfaction and anticipated turnover for nurses in an Academic Medical Center. J Nurs Adm. 2001;31:210–216. doi:10.1097/00005110-200104000-00010
14. Mosadeghrad AM, Ferlie E, Rosenberg D. A study of relationship between job stress, quality of working life and turnover intention among hospital employees. Health Serv Manage Res. 2011;24(4):170–181. doi:10.1258/hsmr.2011.011009
15. Walsh L. Alabama health officials worry about hospital capacity as COVID-19 cases rise. 2020. Available from: https://abc3340.com/news/local/alabama-health-officials-worry-about-hospital-capacity-as-covid-19-cases-rise.
16. Knapp JR, Smith BR, Sprinkle TA. Is it the job or the support? Examining structural and relational predictors of job satisfaction and turnover intention for nonprofit employees. Nonprofit Volunt Sect Q. 2017;46(3):652–671. doi:10.1177/0899764016685859
17. Nantsupawat A, Kunaviktikul W, Nantsupawat R, Wichaikhum OA, Thienthong H, Poghosyan L. Effects of nurse work environment on job dissatisfaction, burnout, intention to leave. Int Nurs Rev. 2017;64:1. doi:10.1111/inr.12342
18. Hamid S, Malik AU, Kamran I, Ramzan M. Job satisfaction among nurses working in the private and public sectors: a qualitative study in tertiary care hospitals in Pakistan. J Multidiscip Healthc. 2014;7. doi:10.2147/JMDH.S55077
19. Cai H, Tu B, Ma J, et al. Psychological impacts and coping strategies of frontline medical staff during COVID-19 outbreak in Hunan, China. Med Sci Monit. 2020;26. doi:10.12659/MSM.924171
20. Kang L, Ma S, Chen M, et al. Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: a cross-sectional study. Brain Behav Immun. 2020;87:11–17. doi:10.1016/j.bbi.2020.03.028
21. Babore A, Lombardi L, Viceconti ML, et al. Psychological effects of the COVID-2019 pandemic: perceived stress and coping strategies among healthcare professionals. Psychiatry Res. 2020;293:113366. doi:10.1016/j.psychres.2020.113366
22. Labrague LJ, de Los Santos JAA. COVID-19 anxiety among frontline nurses: predictive role of organisational support, personal resilience and social support. J Nurs Manag. 2020. doi:10.1111/jonm.13121
23. Turale S, Meechamnan C, Kunaviktikul W. Challenging times: ethics, nursing and the COVID-19 pandemic. Int Nurs Rev. 2020;67(2):164–167. doi:10.1111/inr.12598
24. Irshad M, Khattak SA, Hassan MM, Majeed M, Bashir S. How perceived threat of Covid-19 causes turnover intention among Pakistani nurses: a moderation and mediation analysis. Int J Ment Health Nurs. 2020. doi:10.1111/inm.12775
25. Stovall M, Hansen L, van Ryn M. A critical review: moral injury in nurses in the aftermath of a patient safety incident. J Nurs Scholarsh. 2020;52(3):3. doi:10.1111/jnu.12551
26. Nantsupawat A, Nantsupawat R, Kunaviktikul W, Turale S, Poghosyan L. Nurse burnout, nurse-reported quality of care, and patient outcomes in Thai Hospitals. J Nurs Scholarsh. 2016;48(1):83–90. doi:10.1111/jnu.12187
27. Park S, Kim J, Park J, Lim DH. Work engagement in nonprofit organizations: a conceptual model. Hum Resour Dev Rev. 2018;17(1):5–33. doi:10.1177/1534484317750993
28. Selden SC, Sowa JE. Voluntary turnover in Nonprofit Human Service Organizations: the impact of high performance work practices. Hum Serv Organ Manag Leadersh Gov. 2015;39(3):182–207. doi:10.1080/23303131.2015.1031416
29. Demerouti E, Bakker AB, Nachreiner F, Schaufeli WB. Job demands-resources model of burnout. J Appl Psychol. 2001;86(3):499–512. doi:10.1037/0021-9010.86.3.499
30. Delery J, Shaw J, Ferris G. Research in Personnel and Human Resources Management. Bingley: Emerald Publishing; 2001:165–197.
31. Prapanjaroensin A, Patrician PA, Vance DE. Conservation of resources theory in nurse burnout and patient safety. J Adv Nurs. 2017;73(11):11. doi:10.1111/jan.13348
32. Huynh J-Y, Metzer JC, Winefield AH. Engaged or connected? A perspective of the motivational pathway of the job demands-resources model in volunteers working for Nonprofit Organizations. VOLUNTAS Int J Volunt Nonprofit Organ. 2012;23(4):870–898. doi:10.1007/s11266-011-9233-1
33. Juhdi N, Pa’wan F, Hansaram RMK. HR practices and turnover intention: the mediating roles of organizational commitment and organizational engagement in a selected region in Malaysia. Int J Hum Resour Management. 2013;24(15):3002–3019. doi:10.1080/09585192.2013.763841
34. Kalichman SC, Gueritault-Chalvin V, Demi A. Sources of occupational stress and coping strategies among nurses working in AIDS care. J Assoc Nurses AIDS Care. 2000;11(3):31–37. doi:10.1016/S1055-3290(06)60274-4
35. Monticone M, Ferrante S, Giorgi I, Galandra C, Rocca B, Foti C. The 27-item coping strategies questionnaire — revised: confirmatory factor analysis, reliability and validity in italian-speaking subjects with chronic pain. Pain Res Manag. 2014;19(3):956828. doi:10.1155/2014/956828
36. Shen X, Zou X, Zhong X, Yan J, Li L. Psychological stress of ICU nurses in the time of COVID-19. Crit Care. 2020;24(1):1. doi:10.1186/s13054-020-02926-2
37. Sun N, Wei L, Shi S, et al. A qualitative study on the psychological experience of caregivers of COVID-19 patients. Am J Infect Control. 2020;48(6):592–598. doi:10.1016/j.ajic.2020.03.018
38. Perry JL. Measuring public service motivation: an assessment of construct reliability and validity. J Public Adm Res Theory. 1996;6(1):5–22. doi:10.1093/oxfordjournals.jpart.a024303
39. Castle NG, Engberg J. Organizational characteristics associated with staff turnover in nursing homes. Gerontologist. 2006;46(1):62–73. doi:10.1093/geront/46.1.62
40. Parry J. Intention to leave the profession: antecedents and role in nurse turnover. J Adv Nurs. 2008;64(2):157–167. doi:10.1111/j.1365-2648.2008.04771.x
41. Hobfoll SE. Conservation of resources a new attempt at conceptualizing stress. Am Psychol. 1989;44(3):513. doi:10.1037/0003-066X.44.3.513
42. Hobfoll SE, Halbesleben J, Neveu J-P, Westman M. Conservation of resources in the organizational context: the reality of resources and their consequences. Annu Rev Organ Psychol Organ Behav. 2018;5(1):103–128. doi:10.1146/annurev-orgpsych-032117-104640
43. Hobfoll SE, Shirom A, Golembiewski R. Conservation of resources theory. In: Handbook of Organizational Behavior. New York: Marcel Dekker; 2000:57–81.
44. D’Lima DM, Murray EJ, Brett SJ. Perceptions of risk and safety in the ICU. Crit Care Med. 2018;46(1):1. doi:10.1097/CCM.0000000000002773
45. Price JL. The Study of Turnover. Ames: Iowa State University Press; 1977.
46. van Woerkom M, Bakker AB, Nishii LH. Accumulative job demands and support for strength use: fine-tuning the job demands-resources model using conservation of resources theory. J Appl Psychol. 2016;101(1):141. doi:10.1037/apl0000033
47. Spector PE. Do not cross me: optimizing the use of cross-sectional designs. J Bus Psychol. 2019;34(2):125–137. doi:10.1007/s10869-018-09613-8
48. Chyung SY, Roberts K, Swanson I, Hankinson A. Evidence‐based survey design: the use of a midpoint on the likert scale. Perform Improv. 2017;56(10):15–23. doi:10.1002/pfi.21727
49. Goh Y, Tan BYQ, Bhartendu C, Ong JJY, Sharma VK. The face mask: how a real protection becomes a psychological symbol during Covid-19? Brain Behav Immun. 2020;88:1–5. doi:10.1016/j.bbi.2020.05.060
50. Davidson JE, Proudfoot J, Lee K, Terterian G, Zisook S. A longitudinal analysis of nurse suicide in the United States (2005–2016) with recommendations for action. Worldviews Evid Based Nurs. 2020;17(1):6–15. doi:10.1111/wvn.12419
51. Rafati F, Nouhi E, Sabzevari S, Dehghan-Nayeri N. Coping strategies of nursing students for dealing with stress in clinical setting: a qualitative study. Electron Physician. 2017;9(12):12. doi:10.19082/6120
52. Ali H, Cole A, Sienkiewicz A, Ho T. Perspectives of nursing homes staff on the nature of residents-initiated call lights. SAGE Open Nurs. 2020;6:237796082090354. doi:10.1177/2377960820903546
53. Hayward D, Bungay V, Wolff AC, MacDonald V. A qualitative study of experienced nurses’ voluntary turnover: learning from their perspectives. J Clin Nurs. 2016;25(9–10):1336–1345. doi:10.1111/jocn.13210
54. Al-Dweik G, Ahmad M. Matching nursing assignment to patients’ acuity level: the road to nurses’ satisfaction. J Nurs Meas. 2019;27(1):E34–E47. doi:10.1891/1061-3749.27.1.E34
55. Leiter MP, Maslach C. Nurse turnover: the mediating role of burnout. J Nurs Manag. 2009;17(3):331–339. doi:10.1111/j.1365-2834.2009.01004.x
56. Trent SB, Allen JA. Resilience only gets you so far: volunteer incivility and burnout. Organ Manag J. 2019;16(2):69–80. doi:10.1080/15416518.2019.1604199
57. Al-Majid S, Carlson N, Kiyohara M, Faith M, Rakovski C. Assessing the degree of compassion satisfaction and compassion fatigue among critical care, oncology, and charge nurses. J Nurs Adm. 2018;48(6):310–315. doi:10.1097/NNA.0000000000000620
58. Plasse MJ. Psychosocial support for providers working high-risk exposure settings during a pandemic: a critical discussion. Nurs Inq. 2020;e12399. doi:10.1111/nin.12399
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.