Back to Journals » Patient Preference and Adherence » Volume 19
Identifying Causes of Subcutaneous Immunotherapy Non-Adherence in Patients with Allergic Rhinitis: A Cross-Sectional Study
Received 18 June 2025
Accepted for publication 19 September 2025
Published 30 September 2025 Volume 2025:19 Pages 3049—3056
DOI https://doi.org/10.2147/PPA.S544333
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Cheng-Zhi Huang, Zhi-Yuan Tang
Department of Otorhinolaryngology, Shenzhen University General Hospital, Shenzhen, Guangdong, People’s Republic of China
Correspondence: Zhi-Yuan Tang, Department of Otorhinolaryngology, Shenzhen University General Hospital, 1098 Xueyuan Road, Shenzhen, Guangdong, 518055, People’s Republic of China, Email [email protected]
Purpose: To investigate the reasons for discontinuation of subcutaneous immunotherapy (SCIT) in patients with allergic rhinitis (AR) and to inform strategies for improving treatment adherence.
Materials and Methods: In this single-center retrospective cross-sectional study, 794 AR patients (age 1– 60 years) who initiated standardized SCIT with house dust mite extracts at Shenzhen University General Hospital between December 2019 and July 2023 were included. SCIT followed a structured dose-escalation and maintenance protocol: weeks 1– 4, 0.1– 0.8 mL (50 TU/mL); weeks 5– 8, 0.1– 0.8 mL (500 TU/mL); weeks 9– 14, 0.1– 1.0 mL (5000 TU/mL); weeks 14– 152, monthly 1.0 mL (5000 TU/mL). Symptom severity was assessed using a visual analogue scale (VAS) at baseline and at 6 months, 1, 2, and 3 years; < 20% VAS reduction and/or patient-reported insufficient improvement after ≥ 12 months defined “unsatisfactory efficacy”. Structured telephone follow-up was used, with caregivers interviewed for pediatric patients. All patients provided detailed contact information; no loss to follow-up occurred.
Results: Fifty-eight patients (7.30%) discontinued SCIT (27 males, 31 females; mean age 14.71 ± 10.76 years). Leading reasons were relocation for education, work, or travel (53.45%), perceived lack of efficacy (17.24%), limited time (8.62%), and pregnancy/gynecological conditions (6.90%). Females were more likely to discontinue due to relocation, males due to unsatisfactory efficacy; age and comorbidities were not significantly associated with dropout.
Conclusion: SCIT discontinuation was mainly driven by relocation, treatment expectations, and logistical factors, with gender-specific patterns. Tailored pre-treatment counseling, assessment of lifestyle and reproductive plans, and strategies to maintain continuity of care may reduce dropout and improve long-term adherence.
Keywords: urban lifestyle factors, long-term treatment challenges, patient follow-up
Introduction
Allergic rhinitis (AR) is a chronic, non-infectious inflammatory condition of the nasal mucosa, predominantly mediated by immunoglobulin E (IgE) in response to allergen exposure in atopic individuals.1 Its global prevalence has been rising steadily, now affecting approximately 10% to 40% of the population, significantly impacting patients’ quality of life and healthcare systems.2
Subcutaneous immunotherapy (SCIT) with house dust mite allergens is a well-established, disease-modifying treatment that can alter the natural course of allergic diseases by inducing long-term immunological tolerance.3 Despite its proven efficacy, the clinical effectiveness of SCIT is often undermined by poor patient adherence, primarily due to the prolonged treatment duration, delayed onset of clinical benefit, and logistical burdens associated with regular injections.4
In highly mobile urban populations, such as in Shenzhen, challenges related to continuity of care and treatment access further contribute to SCIT discontinuation. Understanding the factors that influence dropout is essential for improving patient compliance and optimizing treatment outcomes. This study aims to analyze the reasons for SCIT dropout among patients with AR at an allergy center. By identifying the key barriers to treatment completion, we seek to inform future strategies for patient education, clinical follow-up, and individualized treatment planning to enhance SCIT adherence.
Materials and Methods
Study Population and Eligibility Criteria
This single-center retrospective cross-sectional study included 794 patients diagnosed with AR, with or without comorbid allergic diseases such as bronchial asthma, allergic conjunctivitis, or atopic dermatitis. All patients initiated standardized SCIT with house dust mite extracts (Allergopharma, Germany) at the Allergy Center of the Department of Otorhinolaryngology–Head and Neck Surgery, Shenzhen University General Hospital, between December 2019 and July 2023. The sampling frame consisted of all patients who initiated SCIT at this center during the study period. A consecutive sampling method was used, including all eligible patients who met the inclusion criteria. Because of the retrospective design, no a priori sample size calculation was performed; instead, all 794 patients who initiated SCIT during the study period were consecutively included, providing sufficient power to describe patient demographics, treatment characteristics, adherence patterns, and to perform descriptive analyses of SCIT discontinuation and associated factors. Diagnosis was confirmed by clinical evaluation and allergen testing.
Patients were eligible if they had a confirmed diagnosis of AR, initiated SCIT within the study period, and had complete baseline demographic and clinical data. For pediatric patients, participation was confirmed through their primary caregivers. Exclusion criteria included treatment duration of less than three months, or incomplete medical records, and loss to follow-up after three unsuccessful contact attempts. Informed consent was obtained from all participants (or their legal guardians for minors) prior to data collection.
SCIT Protocol
Patients received standardized SCIT using house dust mite allergen extracts (Allergopharma, Germany), administered via subcutaneous injection. The allergen vaccines were supplied in three concentration vials (Bottle No. 1: 50 TU/mL; No. 2: 500 TU/mL; No. 3: 5000 TU/mL; TU = Therapeutic Units).
The treatment regimen comprised two phases: a dose-escalation phase and a maintenance phase. During the dose-escalation phase, injections were administered weekly with the following schedule: weeks 1–4: 0.1 mL, 0.2 mL, 0.4 mL, 0.8 mL (50 TU/mL); weeks 5–8: 0.1 mL, 0.2 mL, 0.4 mL, 0.8 mL (500 TU/mL); weeks 9–14: 0.1 mL, 0.2 mL, 0.4 mL, 0.8 mL, 1.0 mL (5000 TU/mL). The maintenance phase involved monthly injections of 1.0 mL (5000 TU/mL) from week 14 up to week 152. Dose or interval adjustments were allowed based on clinical response or adverse events.
Emergency medications and equipment for anaphylaxis management were prepared prior to each injection. Patients were observed for 30 minutes post-injection to monitor adverse reactions, including urticaria or bronchospasm. Clinicians managed adverse events as appropriate. Symptom evaluation and treatment efficacy were assessed every six months. The recommended duration of SCIT was three years.
Follow-up and Data Collection
A standardized telephone follow-up was conducted to assess patients’ SCIT status and identify reasons for discontinuation. The follow-up script was developed by the research team based on literature review and clinical expertise. It consisted of structured questions on treatment status, reasons for discontinuation (predefined categories with allowance for open-ended responses), adverse events, and patient perceptions of treatment efficacy and burden. For pediatric patients, the primary caregiver was interviewed. Each patient was contacted up to three times before being classified as lost to follow-up. In our department, patients undergoing SCIT are required to provide detailed contact information and addresses; at the time of this study no cases of loss to follow-up were identified. Although not previously validated, the script was pilot-tested on a small sample to ensure clarity and comprehensiveness. The complete script is provided in Supplementary Material 1.
Symptom severity was evaluated using a visual analogue scale (VAS) at baseline and at 6 months, 1 year, 2 years, and 3 years after SCIT initiation. Patients rated nasal congestion, nasal itching, sneezing, rhinorrhea, ocular itching, headache, and sleep disturbance from 0 (no bother) to 10 (severe bother), with 0–3 considered mild, 3–7 moderate, and 7–10 severe. Scores for all items were summed to obtain a total VAS score. A reduction of ≥50% from baseline was classified as markedly effective, 20–50% as effective, and <20% as ineffective. “Unsatisfactory treatment efficacy” was defined as <20% reduction in total VAS score and/or patient-reported perception of insufficient symptom relief relative to treatment expectations after ≥3 months of SCIT.
Follow-ups were conducted for each patient from the initiation of SCIT until treatment completion, discontinuation, or August 2023, whichever occurred first. Assessments were performed every six months during treatment and additionally within 4–6 weeks after treatment discontinuation. SCIT dropout was defined as permanent discontinuation within three years of initiation. Data were obtained through review of medical records and telephone follow-up. Baseline demographic and treatment information—including sex, age, date of SCIT initiation, and duration—was recorded during the up-dosing phase. Follow-up interviews were performed by two trained staff members, who received standardized training on the script and interview procedures. To ensure consistency, both staff conducted pilot interviews on a small sample of patients under supervision before initiating the full study. All subsequent interviews were conducted independently using the standardized script to minimize recall bias.
Statistical Analysis
Data were analyzed using GraphPad Prism 8.0.2 (GraphPad Software, San Diego, CA, USA). Categorical variables, such as dropout reasons by sex or by presence of comorbid allergic diseases, were compared using the chi-square (χ²) test. Continuous variables, specifically age, were compared between two dropout reason groups using independent-samples t-tests. A p-value < 0.05 was considered statistically significant. Results are presented as mean ± standard deviation (SD) for continuous variables and as counts and percentages for categorical variables.
Results
Patient Characteristics
A total of 794 patients were included in the study, all residing in Shenzhen, Guangdong Province, China, with an age range of 1 to 60 years (mean ± SD: 14.71 ± 10.76 years). Among them, 503 (63.35%) were male and 291 (36.65%) were female. All patients had moderate-to-severe allergic rhinitis sensitized to house dust mite and/or domestic dust mite. Concomitant allergic conditions included allergic conjunctivitis in 149 patients, atopic dermatitis/eczema/atopic dermatitis in 116 patients, bronchial asthma in 63 patients, and chronic urticaria in 10 patients. A total of 58 patients discontinued SCIT before completing the recommended treatment duration, resulting in an overall dropout rate of 7.30% (Table 1). The dropout group comprised 27 (46.55%) males and 31 (53.45%) females. The remaining patients either completed the standard 3–5 years of SCIT or were still undergoing treatment at the time of data collection.
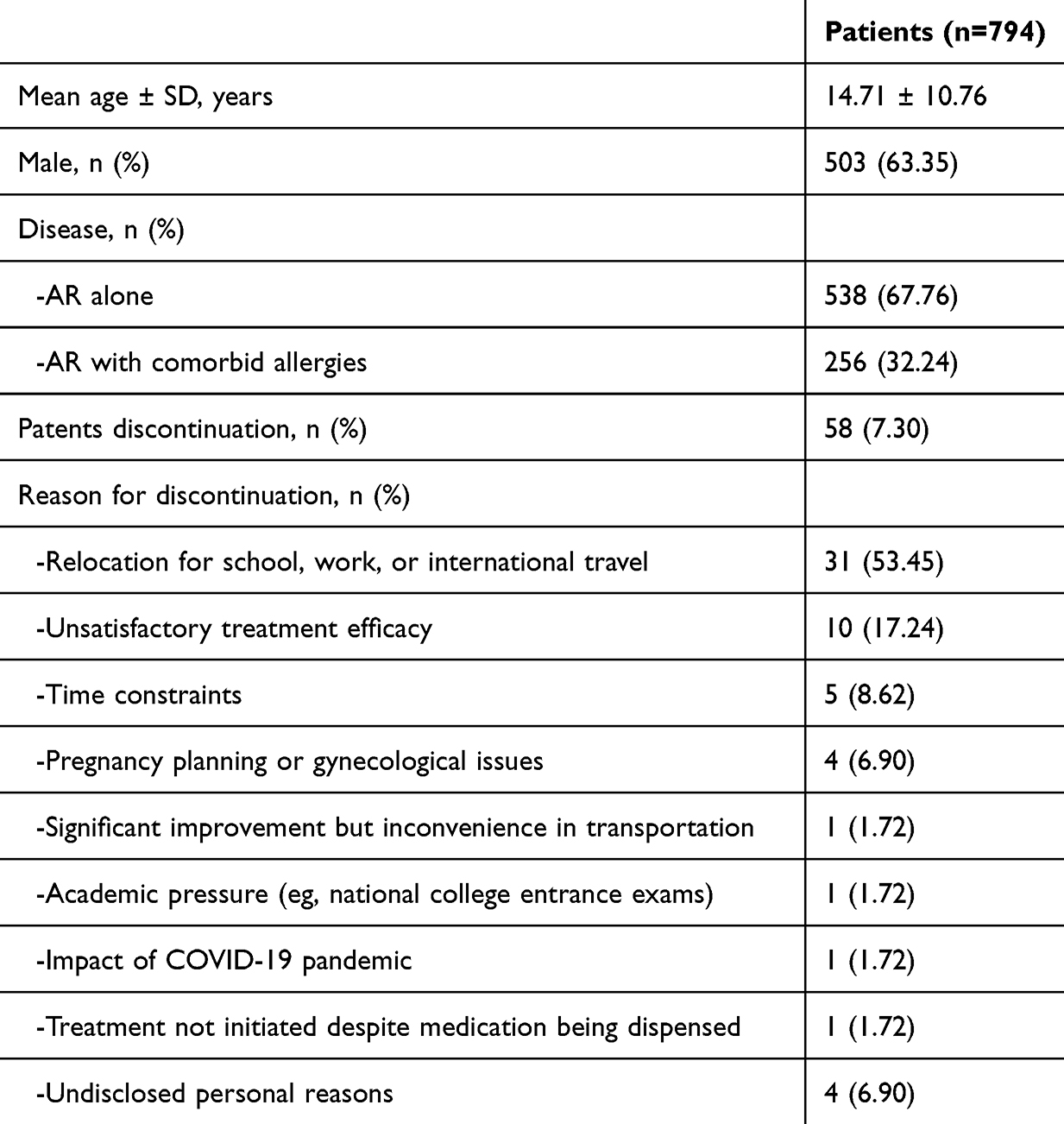 |
Table 1 Patient Characteristics and Dropout Reasons |
Clinical Diagnoses
Among the 794 patients included in the study, 538 (67.76%) were diagnosed with AR alone, while 256 (32.24%) had AR in combination with bronchial asthma or other allergic conditions (Table 1). Among the 58 patients who discontinued SCIT, 38 (65.52%) had AR alone and 20 (34.48%) had comorbid allergic conditions.
Reasons for Treatment Discontinuation
The primary reasons for SCIT discontinuation are summarized in Table 1. The most frequently cited reason was relocation due to academic, occupational, or international travel commitments, accounting for 31 patients (53.45%). The remaining reasons included: Perceived lack of treatment efficacy: 10 patients (17.24%); Limited time availability: 5 patients (8.62%); Pregnancy planning, active pregnancy, or gynecological conditions: 4 patients (6.90%); Marked symptom improvement but inconvenience in transportation: 1 patient (1.72%); Academic stress due to college entrance examinations: 1 patient (1.72%); Inability to continue treatment due to COVID-19–related restrictions: 1 patient (1.72%); Medication dispensed but SCIT never initiated: 1 patient (1.72%); Undisclosed personal reasons: 4 patients (6.90%).
Associations Between Patient Characteristics and Dropout Reasons
Chi-square analysis showed a statistically significant association between sex and dropout reasons (χ² = 19.52, p = 0.012), with females more likely to discontinue due to relocation and males more likely to discontinue due to unsatisfactory efficacy (Table 2). Age was compared between the relocation and unsatisfactory efficacy groups only, as other dropout categories had too few cases for meaningful analysis. No significant difference in mean age was observed between the relocation and unsatisfactory efficacy groups (Figure 1). The distribution of dropout reasons by the presence or absence of comorbid allergic diseases showed no statistically significant differences (Table 3).
 |
Table 2 Analysis of Dropout Reasons by Gender |
 |
Table 3 Analysis of Dropout Reasons by Comorbid Allergic Disease Status |
 |
Figure 1 Analysis of dropout reasons by age. |
Discussion
Subcutaneous immunotherapy remains the only treatment currently available that can alter the natural course of AR, providing potential long-term remission. Despite its demonstrated efficacy, adherence to SCIT remains a major clinical challenge due to the lengthy treatment duration, delayed symptom relief, and logistical demands of regular injections. These challenges are particularly pronounced in rapidly developing urban areas such as Shenzhen, where high population mobility and time constraints are common.
In this study, the SCIT dropout rate was 7.30%, which is comparatively low in the context of real-world data. This may reflect the effectiveness of structured patient education and diligent follow-up conducted at our center. Most patients were residents of central Shenzhen with relatively high socioeconomic and educational levels—factors that have been previously linked to greater treatment adherence.
The leading cause of SCIT discontinuation was relocation for educational, occupational, or international purposes. Females were significantly more likely than males to discontinue due to relocation, whereas no significant age difference was observed between patients discontinuing for relocation versus unsatisfactory efficacy, and the presence of comorbid allergic conditions did not significantly influence dropout reasons. The higher relocation-related dropout among females may reflect greater logistical or family-related constraints that interrupt treatment. Notably, more than half of the patients who relocated continued therapy at other institutions, indicating that discontinuation was primarily driven by external factors rather than dissatisfaction with SCIT itself. These findings underscore the importance of tailored adherence strategies: for female patients, facilitating continuity of care across locations and flexible scheduling may mitigate relocation-related dropout.
Another key reason for the dropout was the perception of unsatisfactory treatment efficacy. This finding emphasizes the critical role of expectation management. Unrealistic expectations, whether excessively optimistic or pessimistic, can erode patient confidence and lead to premature termination of treatment. Among patients who dropped out due to failed expectation management, aside from individual pessimism, most had anticipated greater benefits from immunotherapy compared to conventional pharmacological treatment.5 According to the present study, males may have higher sensitivity to perceived efficacy, reflecting differences in expectation management and tolerance for delayed therapeutic benefit. For male patients, early counseling regarding treatment timelines, expected benefits, and monitoring of progress may help reduce efficacy-related discontinuation. Prior studies suggest that patients with more severe or persistent symptoms, such as those with concurrent asthma, are more motivated to overcome logistical barriers due to a stronger perceived need for treatment.6 Another study has demonstrated that patients who remain adherent during the first year of SCIT are significantly more likely to complete the full therapeutic course.7 Thus, the provision of clear, written information outlining the treatment timeline, expected outcomes, risks, and limitations is essential to fostering realistic expectations and long-term adherence.8 Therefore, providing a clear and concise written summary outlining the characteristics of AR and the SCIT treatment process may help reduce dropout caused by poor expectation management. Notably, dropout rates tend to decline significantly after the first year of treatment adherence.
Inconvenience related to treatment scheduling and transportation was another important factor contributing to dropout. A retrospective study conducted in the Netherlands found that patients receiving SCIT through general practitioners demonstrated better adherence, likely due to improved convenience and closer proximity to care facilities.9 Such findings suggest that minimizing the logistical burden of treatment may enhance patient compliance, particularly in urban settings where time constraints frequently interfere with long-term care. Accordingly, strategies such as flexible appointment scheduling, decentralization of care (eg, administering SCIT in primary care settings), and reducing visit frequency—when clinically feasible—may help mitigate these barriers.
Pregnancy and gynecological concerns were also identified as factors contributing to SCIT discontinuation. Previous studies have reported pregnancy as a common reason for dropout among female patients undergoing SCIT.10,11 In our cohort, several female patients paused or discontinued treatment due to pregnancy planning, confirmed pregnancy, or gynecological conditions. Therefore, it is crucial to assess reproductive intentions before initiating SCIT in women of childbearing age. Notably, patients with allergic diseases may have increased motivation to maintain immunotherapy during pregnancy, especially given that approximately 20% of women with asthma experience symptom exacerbation during this period.12 Although SCIT has traditionally been approached with caution during pregnancy, accumulating evidence indicates that continuing immunotherapy is generally safe and does not increase the risk of adverse maternal or fetal outcomes.13–15 Consequently, individualized counseling regarding fertility plans should be an integral component of pre-treatment evaluation for female patients.
Finally, psychological conditions and systemic comorbidities such as autoimmune diseases and malignancies may also influence adherence. While active autoimmune disorders and cancers are typically contraindications for SCIT and patients with anxiety disorders should be enrolled with caution,16,17 some studies suggest that patients with post-traumatic stress disorder may exhibit higher adherence, possibly due to more frequent healthcare interactions.18,19
This study has several limitations. As a retrospective, single-center analysis, it is subject to inherent biases and limited generalizability. Data collection relied partly on telephone follow-up, which may introduce recall and selection bias; although all patients provided detailed contact information and no cases of loss to follow-up were observed, the potential for selection bias cannot be entirely excluded. Outcome assessment of “unsatisfactory treatment efficacy” was based on patient-reported symptom relief and treatment expectations, which is inherently subjective. Follow-up data regarding relocated patients and adverse reactions were limited, and information classified as “undisclosed personal reasons” reflects patient privacy constraints. Moreover, the study population mainly consisted of patients with higher educational and socioeconomic status, which may not represent the broader population. Future multicenter studies with larger and more diverse cohorts, along with more objective measures of efficacy and comprehensive tracking of relocation and adverse events, are needed to confirm these findings.
Conclusion
Discontinuation of SCIT in patients with allergic rhinitis was mainly related to relocation, perceived efficacy, and logistical challenges. Females were more likely to discontinue due to relocation, whereas males more often cited unsatisfactory efficacy. Tailored strategies, including expectation management, assessment of reproductive plans, and support for continuity of care across locations, may help reduce dropout. Strengthening patient education, offering flexible follow-up, and minimizing treatment burden are essential to improve long-term adherence.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available due to institutional restrictions and patient privacy protection, but they are available from the corresponding author upon reasonable request and with permission from Shenzhen University General Hospital.
Ethics Approval and Consent to Participate
This retrospective study used de-identified medical records from Shenzhen University General Hospital, including pediatric patients. In accordance with the Institutional Review Board/Ethics Committee of Shenzhen University General Hospital, retrospective studies based on anonymized data that pose no risk to participants do not require ethics approval. All data were analyzed anonymously, and the study complied with the Declaration of Helsinki.
Acknowledgments
The authors would like to express their sincere thanks to the participants.
Funding
This study was funded by Shenzhen Science and Technology Program, No: JCYJ20200109114244249.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Subspecialty Group of Rhinology, Editorial Board of Chinese Journal of Otorhinolaryngology Head and Neck Surgery, Subspecialty Group of Rhinology, Society of Otorhinolaryngology Head and Neck Surgery, Chinese Medical Association. [Chinese guideline for diagnosis and treatment of allergic rhinitis (2022 revision)]. Chin J Otorhinolaryngol Head Neck Surg. 2022;57(2):106–129.
2. Li H, Chen S, Cheng L, et al. Chinese guideline on sublingual immunotherapy for allergic rhinitis and asthma. J Thorac Dis. 2019;11(12):4936–4950. doi:10.21037/jtd.2019.12.37
3. Tang RB. House dust mite-specific immunotherapy alters the natural course of atopic march. J Chin Med Assoc. 2020;83(2):109–112. doi:10.1097/JCMA.0000000000000231
4. Park MJ, Kapoor S, Yi J, Hura N, Lin SY. Systematic review of real-world persistence and adherence in subcutaneous allergen immunotherapy. Int Forum Allergy Rhinol. 2023;13(3):255–264. doi:10.1002/alr.23078
5. Musa F, Al-Ahmad M, Arifhodzic N, et al. Compliance with allergen immunotherapy and factors affecting compliance among patients with respiratory allergies. Hum Vaccin Immunother. 2017;13(3):514–517. doi:10.1080/21645515.2016.1243632
6. Lee JH, Lee SH, Ban GY, et al. Factors associated with adherence to allergen-specific subcutaneous immunotherapy. Yonsei Med J. 2019;60(6):570–577. doi:10.3349/ymj.2019.60.6.570
7. Lemberg ML, Berk T, Shah-Hosseini K, Kasche EM, Mösges R. Sublingual versus subcutaneous immunotherapy: patient adherence at a large German allergy center. Patient Prefer Adherence. 2017;11:63–70. doi:10.2147/PPA.S122948
8. Incorvaia C, Rapetti A, Scurati S, et al. Importance of patient education in favoring compliance with sublingual immunotherapy. Allergy. 2010;65(11):1341–1342. doi:10.1111/j.1398-9995.2010.02347.x
9. Kiel MA, Röder E, Gerth van Wijk R, et al. Real-life compliance and persistence among users of subcutaneous and sublingual allergen immunotherapy. J Allergy Clin Immunol. 2013;132(2):353–360. doi:10.1016/j.jaci.2013.03.013
10. Yang Y, Wang Y, Yang L, et al. Risk factors and strategies in nonadherence with subcutaneous immunotherapy: a real-life study. Int Forum Allergy Rhinol. 2018;8(11):1267–1273. doi:10.1002/alr.22190
11. Tat TS. Adherence to subcutaneous allergen immunotherapy in Southeast Turkey: a real-life study. Med Sci Monit. 2018;24:8977–8983. doi:10.12659/MSM.910860
12. Murphy VE, Clifton VL, Gibson PG. Asthma exacerbations during pregnancy: incidence and association with adverse pregnancy outcomes. Thorax. 2006;61(2):169–176. doi:10.1136/thx.2005.049718
13. Mitselou N, Stephansson O, Melén E, et al. Exposure to allergen-specific immunotherapy in pregnancy and risk of congenital malformations and other adverse pregnancy outcomes. J Allergy Clin Immunol Pract. 2022;10(6):1635–1641.e2. doi:10.1016/j.jaip.2022.03.005
14. Shaikh WA. A retrospective study on the safety of immunotherapy in pregnancy. Clin Exp Allergy. 1993;23(10):857–860. doi:10.1111/j.1365-2222.1993.tb00264.x
15. Shaikh WA, Shaikh SW. A prospective study on the safety of sublingual immunotherapy in pregnancy. Allergy. 2012;67(6):741–743. doi:10.1111/j.1398-9995.2012.02815.x
16. Calderon MA, Demoly P, Gerth van Wijk R, et al. EAACI: a European declaration on immunotherapy—designing the future of allergen-specific immunotherapy. Clin Transl Allergy. 2012;2:20. doi:10.1186/2045-7022-2-20
17. Rhodes BJ. Patient dropouts before completion of optimal dose, multiple allergen immunotherapy. Ann Allergy Asthma Immunol. 1999;82(3):281–286. doi:10.1016/S1081-1206(10)62609-9
18. Guenechea-Sola M, Hariri SR, Galoosian A, et al. A retrospective review of veterans’ adherence to allergen immunotherapy over 10 years. Ann Allergy Asthma Immunol. 2014;112(1):79–81. doi:10.1016/j.anai.2013.10.018
19. Ellenburg JT, Lieberman JA, Pattanaik D. Adherence and systemic reaction rates to allergy immunotherapy among veterans. Allergy Rhinol. 2016;7(3):127–130. doi:10.2500/ar.2016.7.0170
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.