Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Identification of Risk Factors for 30-Day and Frequent One-Year Readmissions in Chronic Obstructive Pulmonary Disease Patients Following Acute Exacerbation
Authors Ran C, Lian M, Dilixiati N, Lin R, Song J, Yang J, Wang J
Received 23 June 2025
Accepted for publication 8 January 2026
Published 15 January 2026 Volume 2026:21 549054
DOI https://doi.org/10.2147/COPD.S549054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Chunxue Ran,* Mengyu Lian,* Nafeisa Dilixiati, Ruiyan Lin, Jie Song, Jingjing Yang, Jinxiang Wang
Department of Pulmonary and Critical Care Medicine, Beijing Luhe Hospital, Capital Medical University, Beijing, 101100, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinxiang Wang, Email [email protected]
Objective: Acute exacerbations of chronic obstructive pulmonary disease (COPD) are a major cause of hospitalization and readmission, severely impacting patients’ quality of life and long-term prognosis. This study aimed to identify risk factors for both 30-day and frequent readmissions within one year following hospitalization for an acute exacerbation of COPD.
Methods: We conducted a retrospective analysis of 1,208 patients hospitalized for acute COPD exacerbations. Patients were categorized based on readmission within 30 days or multiple readmissions in the subsequent year. Univariate and multivariate logistic regression analyses were employed to identify independent risk factors. A predictive nomogram model was developed and internally validated using bootstrapping techniques.
Results: For 30-day readmissions, age was identified as an independent risk factor (OR=1.044, 95% CI: 1.008– 1.081). For frequent one-year readmissions, multivariate analysis revealed age (OR=1.025, 95% CI: 1.008– 1.042) and Anthonisen classification Type I/II (OR=1.556, 95% CI: 1.021– 2.369) as independent risk factors, while creatine kinase (CK) acted as a protective factor (OR=0.998, 95% CI: 0.996– 1.000). The nomogram demonstrated good predictive performance, with a C-index of 0.730 and an AUC of 0.730 upon internal validation.
Conclusion: This study identifies age and Anthonisen classification as key risk factors, and CK as a protective factor for readmissions in COPD patients following acute exacerbation. The validated nomogram provides a practical clinical tool for predicting readmission risks, enabling early identification of high-risk patients during hospitalization or at discharge. This risk stratification approach can facilitate implementation of personalized management strategies, such as intensified follow-up or targeted interventions, to reduce readmission rates and improve patient outcomes.
Keywords: chronic obstructive pulmonary disease, acute exacerbation, readmission, risk factors, nomogram model
Introduction
Chronic obstructive pulmonary disease (COPD) is a major global health burden, ranking as the third leading cause of death worldwide with nearly 4 million annual deaths.1 Its prevalence continues to rise, particularly in low- and middle-income countries due to factors such as pollution and limited healthcare access.2,3 Acute exacerbations of COPD (AECOPD) are critical events that drive hospitalizations, accelerate disease progression, and increase mortality.4,5 These exacerbations also lead to high rates of readmission,6,7 which further strain healthcare systems and impair patients’ quality of life.8 Despite the clinical significance of readmissions, risk factors for short-term and frequent long-term readmissions remain inadequately characterized.9,10 This study aims to identify key risk factors for 30-day and one-year readmissions in COPD patients following AECOPD, addressing a crucial gap in optimizing post-discharge management and reducing readmission rates.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) report identifies acute exacerbations of COPD (AECOPD) as the leading cause of hospitalization in COPD patients, with readmission rates serving as a critical prognostic indicator.11 Elevated readmission rates not only adversely affect patient health but also impose significant economic burdens on families and society, highlighting a major challenge for healthcare systems worldwide, particularly in resource-constrained settings.12,13 Previous studies have identified various factors associated with COPD readmissions, including exacerbation severity, comorbid conditions, patient lifestyle, and treatment adherence.14,15 For instance, reported effect sizes include hazard ratios (HRs) of 1.2–2.5 for comorbidities such as cardiovascular disease and odds ratios (ORs) of 1.1–1.7 for inadequate therapy compliance. However, these studies often exhibit limitations, such as heterogeneous methodologies, small sample sizes, or insufficient adjustment for confounders, leading to inconsistent findings and gaps in generalizability. This underscores the need for robust, large-scale analyses to validate and extend prior work. With the aging population and escalating environmental pollution, COPD incidence and readmission rates have surged, posing substantial clinical and health system challenges.16,17 Frequent readmissions within 30 days and 1 year are of particular concern, with rates reaching 20%–30% within 30 days and approximately one-third of patients readmitted within a year due to recurrent exacerbations.16,17 These high rates reflect deficiencies in disease management and are associated with poorer patient outcomes, including functional decline, reduced quality of life, and increased mortality risk. The clinical and health system implications of frequent readmissions are profound. From a clinical perspective, readmissions often signal disease deterioration and worse long-term prognosis, necessitating targeted interventions. For health systems, they contribute to rising costs and resource allocation inefficiencies. Although the use of 30-day readmission as a universal indicator has been debated—criticized for potential biases related to patient demographics or healthcare access—it remains a valuable metric for evaluating care quality and prognostic outcomes in COPD management, given its ability to capture early post-discharge vulnerabilities. Therefore, a comprehensive understanding of the risk factors for 30-day and one-year readmissions following AECOPD is essential to develop effective strategies for reducing readmission rates, improving patient outcomes, and optimizing healthcare resource allocation. This study aims to address limitations of prior research by identifying and validating these risk factors through a large, multicenter cohort, thereby advancing the field and informing clinical practice.
A growing body of research has identified several risk factors that influence readmission rates following acute exacerbations of COPD. First, the burden of comorbidities plays a significant role in determining the prognosis after an acute exacerbation. Chronic conditions, particularly cardiovascular diseases, diabetes, and hypertension, have consistently been identified as independent risk factors for readmission in COPD patients.18,19 Moreover, the degree of lung function impairment is a critical predictor of readmission risk. Specifically, a lower forced expiratory volume in one second to forced vital capacity (FEV1/FVC) ratio is strongly associated with higher readmission rates.20 In addition, the etiology and management of acute exacerbations have a direct impact on hospitalization and readmission risks. Infectious agents, particularly bacterial and viral infections of the lower respiratory tract, are common triggers of exacerbations in COPD.21 Patients experiencing infectious exacerbations, especially those requiring mechanical ventilation, face a significantly increased risk of both short-term and long-term readmissions.
While numerous clinical studies have highlighted the heightened risk of readmission in COPD patients, specific strategies for effectively predicting and preventing readmissions after AECOPD remain underdeveloped. In clinical practice, factors such as age, gender, smoking history, comorbid conditions, and lung function are commonly considered to correlate with readmission risk. However, the complex interactions among these factors and their precise influence on readmission risk in COPD patients have not been fully elucidated. Therefore, this study seeks to explore the underlying mechanisms and risk factors contributing to readmissions after AECOPD, identify more nuanced predictive indicators, and develop enhanced predictive tools and intervention strategies to improve clinical management and patient outcomes.
Methods and Materials
Study Population
This retrospective cohort study included 1,208 patients hospitalized for acute exacerbations of chronic obstructive pulmonary disease (AECOPD) between January 2018 and December 2022. The study was conducted in accordance with the Declaration of Helsinki. The initial admission was defined as the first hospitalization for AECOPD during the study period. Patients with previous COPD-related hospitalizations were excluded.
Participants met the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria for COPD and were diagnosed with AECOPD upon hospitalization 1,2. The study population was stratified into two cohorts: those with readmission within 30 days post-discharge (n=52, 4.3%) and those with frequent readmissions (≥2) within one year.
The study received approval from the Ethics Committee of Beijing Luhe Hospital, Capital Medical University (Approval No: 2020-LHKY-014-03). Informed consent was waived due to the retrospective nature of the study using anonymized data.
Inclusion Criteria
First hospitalization for AECOPD
Complete clinical and laboratory data
Exclusion Criteria
Planned readmissions (eg, for cancer care, rehabilitation, psychiatric conditions, or obstetric procedures)
Severe mental disorders or cognitive impairments
Hospital stay <24 hours
Missing data
Data Collection
Clinical data were extracted from electronic medical records, including:
Demographics (gender, age)
Medical history (COPD duration, comorbidities)
Laboratory tests (first values within 24 hours of admission): total protein, albumin, ALT, CK, GLU, pH
Imaging findings (chest CT)
Echocardiography (right ventricular enlargement)
Readmission Definitions:
30-day readmission: unplanned readmission within 30 days post-discharge
Frequent readmission: ≥2 unplanned readmissions within one year
Continuous laboratory variables were transformed into clinically meaningful categories based on reference ranges 3,4.
Statistical Analysis
Statistical analyses were performed using SPSS 26.0 and R 4.2.0. Continuous variables were expressed as mean ± SD or median (IQR), and compared using t-tests or Mann–Whitney U-tests. Categorical variables were expressed as frequencies (%) and compared using chi-square or Fisher’s exact tests.
To address class imbalance in 30-day readmissions, we performed both standard logistic regression and sensitivity analysis with SMOTE oversampling 5. Multivariate logistic regression identified independent risk factors. All tests were two-tailed with p<0.05 considered significant.
Risk Prediction Model Development
Based on the results of multivariate logistic regression analysis, a nomogram risk model was constructed to predict the likelihood of 30-day and frequent readmissions in COPD patients following acute exacerbations. Independent risk factors (eg, age, COPD duration, total protein, albumin, Anthonisen classification, CK levels) were assigned point values according to their respective regression coefficients. The total score for each patient was then calculated, and the readmission risk was predicted accordingly. The predictive performance of the model was assessed using receiver operating characteristic (ROC) curve analysis, Harrell’s C-index, Hosmer-Lemeshow goodness-of-fit test, and internal validation via bootstrap resampling.
Bootstrapping Validation: To assess the stability and accuracy of the model, internal validation was performed using 1,000 iterations of bootstrap resampling. Model performance was evaluated by calculating Harrell’s C-index and the area under the ROC curve (AUC).
Model Calibration and Validation: The goodness-of-fit of the model was further assessed using the Hosmer-Lemeshow test and chi-square statistics. Additionally, decision curve analysis (DCA) was employed to evaluate the clinical applicability of the prediction model.
Results
Univariate Analysis of 30-Day Readmission in Patients with Acute Exacerbation of COPD
Among 1208 patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD), the cohort was stratified into two groups based on the occurrence of 30-day readmission: the readmission group and the non-readmission group. No significant differences were observed between the groups with respect to gender, CT evidence of pneumonia, CT classification, or right ventricular enlargement (P > 0.05). However, notable differences were observed in age, total protein, and albumin levels (P < 0.05). Specifically, the readmission group was significantly older than the non-readmission group (P < 0.05), and had lower total protein and albumin levels (P < 0.05), as detailed in Table 1.
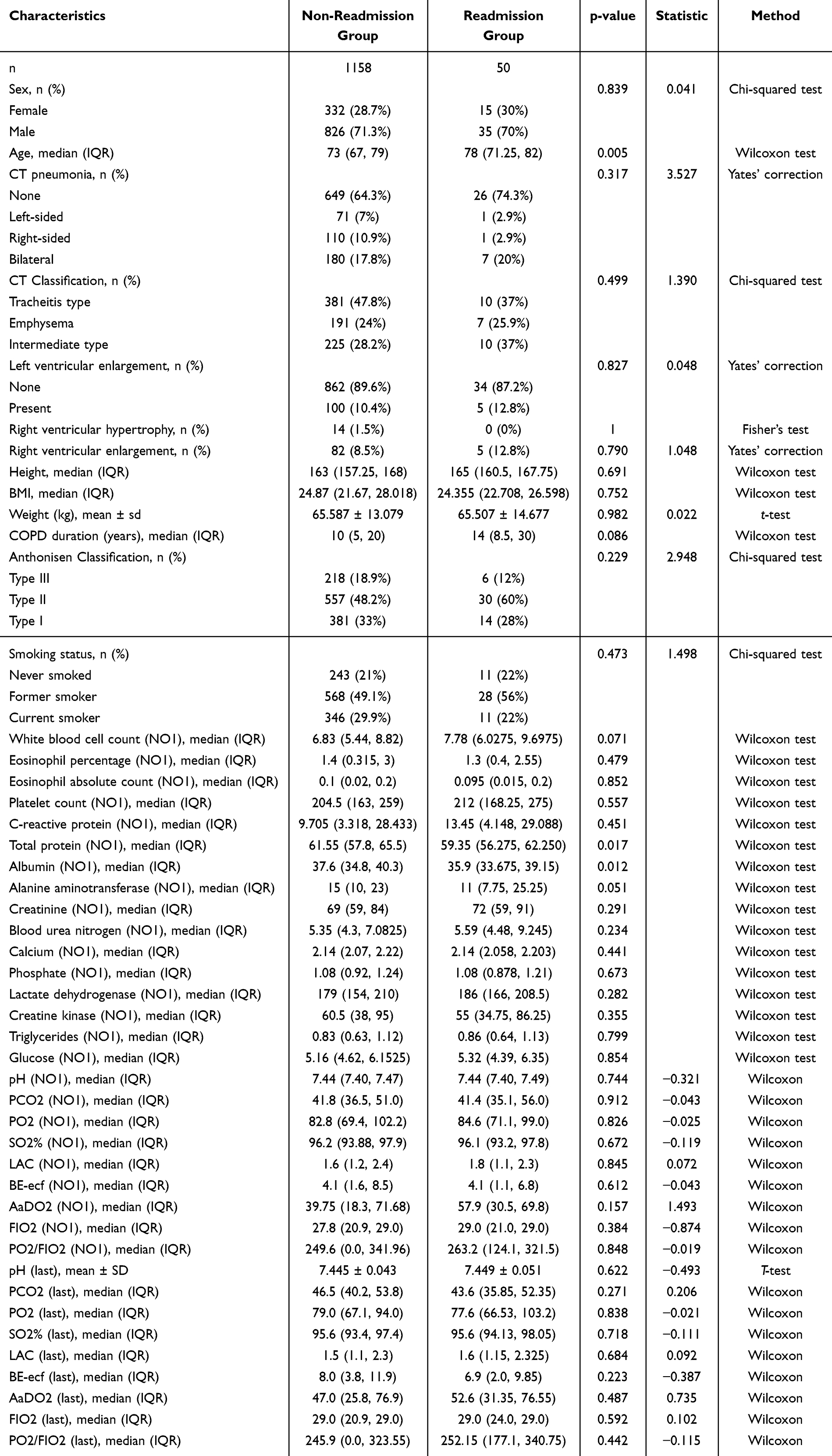 |
Table 1 Univariate Analysis of Factors Associated with 30-Day Rehospitalization Following Acute Exacerbation of Chronic Obstructive Pulmonary Disease (COPD) |
Multivariate Logistic Regression Analysis of 30-Day Readmission in Patients with Acute Exacerbation of COPD
In a multivariate logistic regression model, 30-day readmission was treated as the dependent variable, with factors identified in the univariate analysis—age, total protein, and albumin—serving as independent variables. The analysis revealed that age was an independent risk factor for 30-day readmission (P < 0.05), as presented in Table 2.
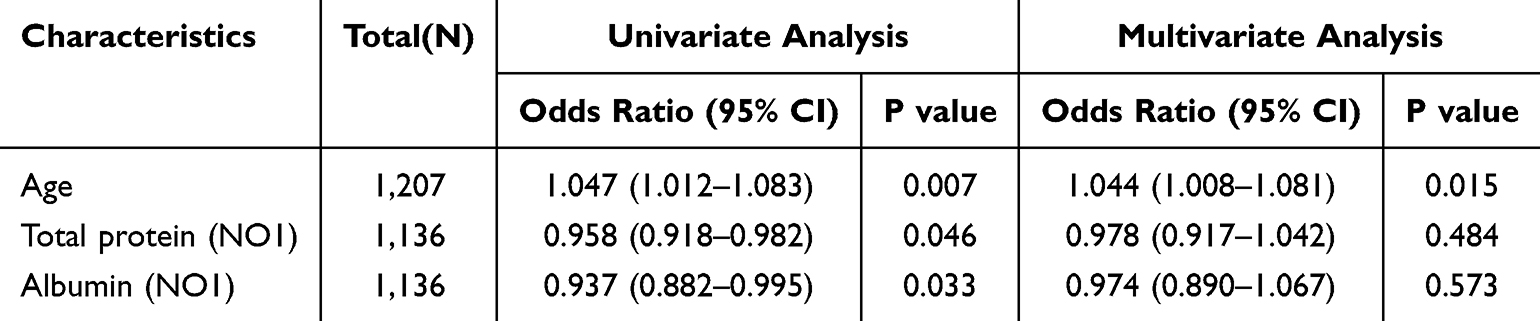 |
Table 2 Univariate and Multivariate Logistic Regression Analysis of Factors Associated with 30-Day Rehospitalization Following Acute Exacerbation of Chronic Obstructive Pulmonary Disease (COPD) |
Univariate Analysis of Frequent Readmission in the Following Year in Patients with Acute Exacerbation of COPD
Among the 1208 patients with AECOPD, the cohort was divided based on the frequency of readmissions in the following year into two groups: the frequent readmission group and the non-frequent readmission group. No significant differences were noted between the groups regarding gender, CT evidence of pneumonia, CT classification, right ventricular enlargement, or other variables (P > 0.05). However, significant differences were found in age, COPD duration, Anthonisen classification, alanine aminotransferase (ALT), creatine kinase (CK), glucose (GLU), and pH levels (P < 0.05). Specifically, the frequent readmission group was older, had a longer COPD duration, and exhibited a higher proportion of Anthonisen Type 1 and Type 2 classifications compared to the non-frequent readmission group (P < 0.05). Conversely, the frequent readmission group had lower ALT, CK, GLU, and pH levels compared to the non-frequent readmission group (P < 0.05), as shown in Table 3.
 |
Table 3 Univariate Analysis of Factors Associated with Frequent Rehospitalization Within One Year Following Acute Exacerbation of Chronic Obstructive Pulmonary Disease (COPD) |
Univariate and Multivariate Logistic Regression Analysis of Frequent Readmission in the Following Year in Patients with Acute Exacerbation of COPD
To identify factors associated with frequent readmission in the following year, both univariate and multivariate logistic regression analyses were conducted, using age, COPD duration, Anthonisen classification, ALT, CK, GLU, and pH as independent variables. The multivariate analysis revealed that both age and Anthonisen classification (Types 1 and 2) were independent risk factors for frequent readmission (P < 0.05). Conversely, CK levels were found to be an independent protective factor (P < 0.05), as detailed in Table 4.
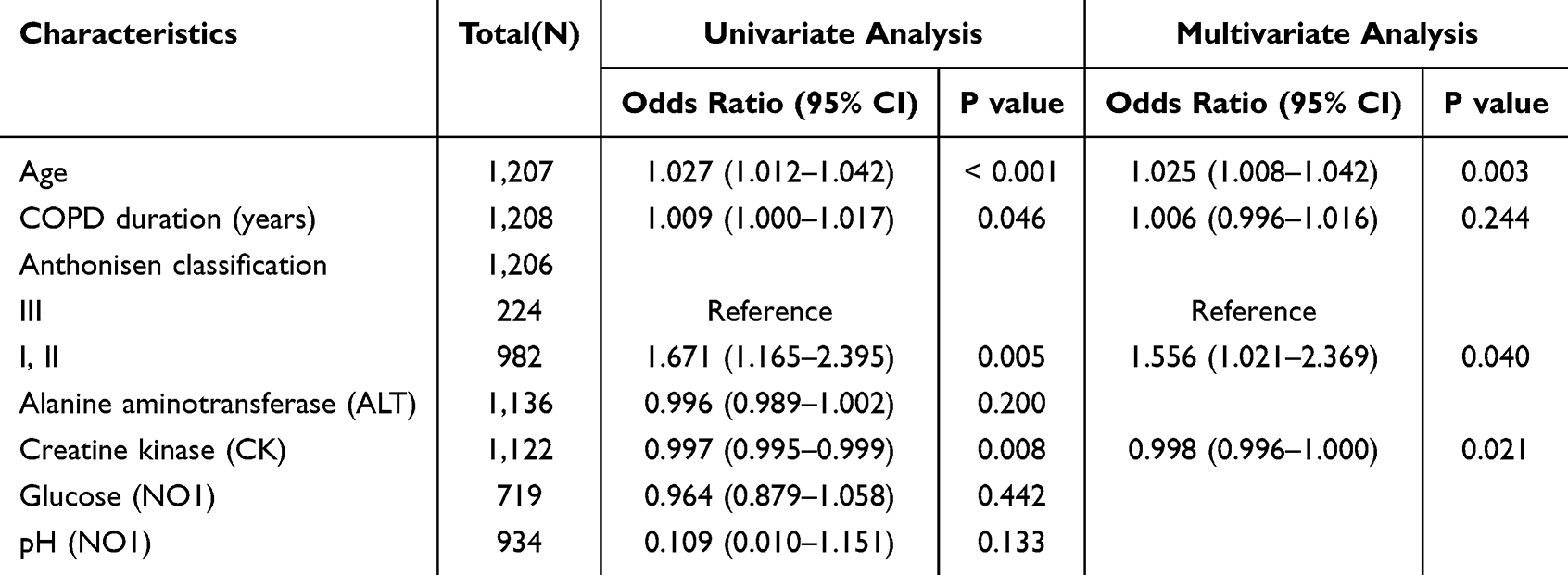 |
Table 4 Univariate and Multivariate Logistic Regression Analysis of Factors Associated with Frequent Rehospitalization Within One Year Following Acute Exacerbation of Chronic Obstructive Pulmonary Disease (COPD) |
Development of a Nomogram Risk Model for Predicting Frequent Readmission in the Following Year in Patients with Acute Exacerbation of COPD
Building on the results of the multivariate logistic regression analysis, a nomogram was developed to predict the likelihood of frequent readmission in the subsequent year among patients with acute exacerbation of COPD. The model integrates three independent risk factors, with each factor assigned a score ranging from 0 to 100. These scores are summed to derive a total score, which is then used to calculate the individual probability of frequent readmission (Figure 1).
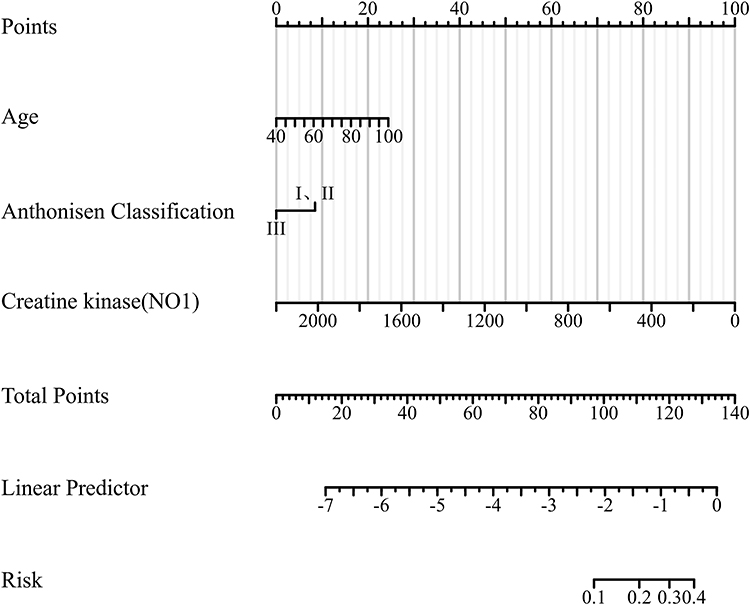 |
Figure 1 Nomogram Model for Predicting Frequent Rehospitalization Within One Year Following Acute Exacerbation of Chronic Obstructive Pulmonary Disease (COPD), Based on Multivariable Logistic Regression Analysis. |
Validation of the Nomogram Model
To assess the reliability of the nomogram, internal validation was performed using bootstrapping with 1000 resamples. The results yielded a Harrell C-index of 0.730, suggesting robust calibration. Additionally, the Hosmer-Lemeshow test produced a chi-square value of 3.905 with a P-value of 0.865, further supporting the model’s predictive accuracy (Figure 2). Receiver operating characteristic (ROC) curve analysis showed an area under the curve (AUC) of 0.730 (95% CI: 0.698–0.762), indicating strong discriminatory power (Figure 3). Furthermore, decision curve analysis (DCA) confirmed that the model holds substantial clinical utility (Figure 4).
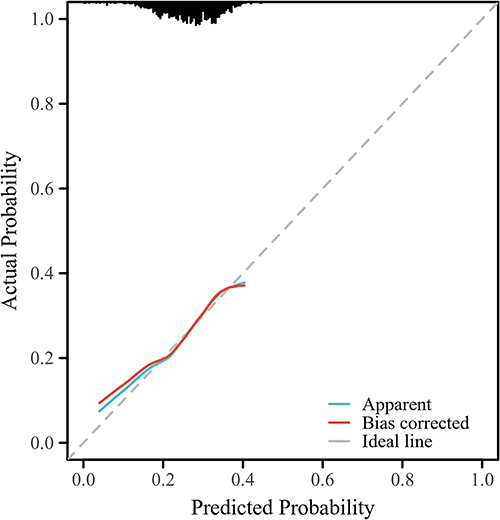 |
Figure 2 Calibration Curve for the Nomogram Model. |
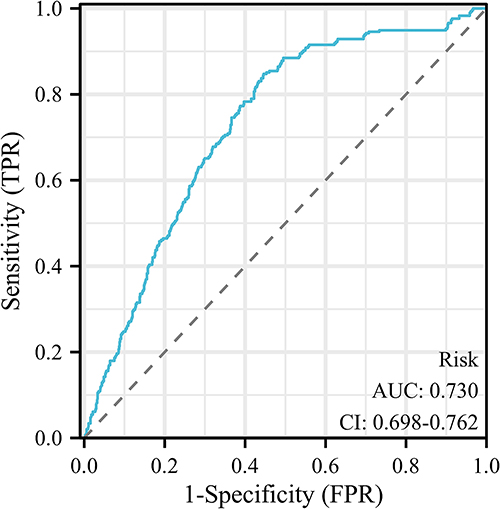 |
Figure 3 Receiver Operating Characteristic (ROC) Curve for the Nomogram Model. |
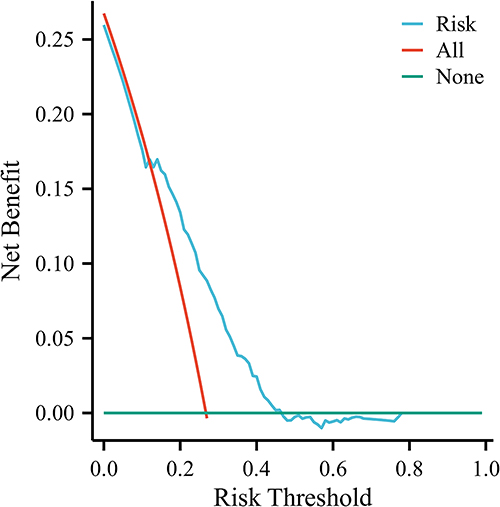 |
Figure 4 Decision Curve Analysis for the Nomogram Model. |
Discussion
COPD is a globally prevalent and progressive respiratory condition, characterized by persistent airway obstruction that significantly impairs pulmonary function.22,23 The incidence and mortality rates of COPD have been steadily increasing, leading to a substantial deterioration in patients’ quality of life and placing a considerable burden on healthcare systems worldwide.24 While current therapeutic strategies, including bronchodilators and inhaled corticosteroids, provide symptomatic relief, they are limited in their capacity to halt disease progression, improve long-term outcomes, or reduce the frequency of acute exacerbations. Thus, a deeper understanding of the underlying mechanisms driving COPD exacerbations, and the associated risk of rehospitalization, is critical for refining management strategies. Our study addresses this gap by identifying specific risk factors, such as age and Anthonisen classification, which independently predict readmissions. These findings not only align with existing knowledge on COPD heterogeneity but also provide novel insights into the role of biomarkers like creatine kinase in modulating readmission risks. Furthermore, the developed nomogram model offers a practical tool for stratifying high-risk patients, thereby facilitating targeted interventions to reduce healthcare burdens and improve long-term outcomes.
This study focuses on COPD patients who experienced acute exacerbations and assesses their subsequent risk of rehospitalization. We analyzed clinical data from 1,208 patients collected between 2018 and 2022. Our analysis revealed no significant differences between patients readmitted within 30 days and those who were not, with regard to gender, CT findings of pneumonia, CT phenotyping, or right ventricular enlargement. This finding aligns with prior literature, suggesting that traditional imaging and anatomical features may not serve as reliable predictors of early rehospitalization.25,26 However, notable differences were observed in age, total protein, and albumin levels between the two groups. Multivariable logistic regression identified age as an independent risk factor for rehospitalization within 30 days. The link between age and rehospitalization risk has been well-documented in previous studies, with older patients often presenting with comorbidities, impaired immune function, and a diminished capacity to recover from acute exacerbations, all of which elevate their risk of early readmission.27,28 Our data confirm that patients readmitted within 30 days were significantly older, a result consistent with clinical experience. Furthermore, low levels of total protein and albumin were associated with an increased risk of rehospitalization, supporting findings from existing research. These markers are crucial indicators of nutritional status and systemic inflammation, and their reduction is frequently associated with malnutrition, ongoing inflammation, or disease progression.29,30 Hypoalbuminemia, in particular, is a common consequence following acute COPD exacerbations and is strongly linked to poor prognosis.31,32 Consequently, monitoring these biochemical markers could provide valuable insights into the development of early intervention strategies.
When assessing risk factors for frequent rehospitalization over the following year, our study identified significant differences in variables including age, disease duration, Anthonisen phenotyping, and levels of ALT, CK, glucose (GLU), and pH. Through multivariable logistic regression, age, disease duration, and Anthonisen phenotyping (Type 1/2) were confirmed as independent risk factors for frequent rehospitalization, while elevated creatine kinase (CK) levels emerged as a protective factor. In contrast, variables such as ALT, GLU, and pH, which showed significance in univariate analyses, should be interpreted as correlated factors rather than independent predictors due to potential confounding effects. The relationship between age and frequent rehospitalization was further substantiated in our analysis, with each additional year of age associated with an approximate 2.5% increase in risk. This finding aligns with prior studies reporting a 3.5% annual increase in readmission risk, though the slight discrepancy may be attributed to differences in population demographics, ethnic backgrounds, or healthcare access.31,32 Elderly COPD patients often experience multiple comorbidities, diminished lung function, and a higher mortality rate, making age a critical determinant of rehospitalization risk following acute exacerbations. Similarly, disease duration emerged as a significant independent factor,33 with longer durations correlating with more severe lung function impairment and reduced tolerance to acute exacerbations, thereby increasing rehospitalization likelihood.33 In our cohort, patients with frequent rehospitalizations had a longer disease duration, indicating that a protracted disease course likely confers higher disease burden and poorer control. The Anthonisen classification, which categorizes acute COPD exacerbations into three types, was also predictive of rehospitalization risk.33 Our results showed that the frequent rehospitalization group had a higher proportion of Types 1 and 2 exacerbations, suggesting these types may be associated with more complex clinical courses and worse outcomes. This is consistent with previous research highlighting the role of exacerbation severity in driving readmissions, though variations in effect sizes across studies may reflect differences in patient populations or healthcare settings. Biochemical markers such as ALT, CK, GLU, and pH levels were significantly correlated with frequent rehospitalization in univariate analyses. Low ALT and CK levels may indicate liver and muscle dysfunction, respectively, while decreased glucose and pH levels suggest metabolic derangements, which could contribute to increased exacerbation risk.34,35 For instance, reduced CK levels might reflect muscle wasting, a known prognostic factor in COPD, whereas alterations in glucose and pH could signal systemic inflammation or acid-base imbalances. Although these biomarkers showed predictive value, their independent contribution requires further validation in multivariate settings with adjustment for confounders such as comorbidities and nutritional status. Using multivariable logistic regression, we developed a nomogram-based predictive model incorporating age, Anthonisen classification, and CK levels to assess the likelihood of frequent rehospitalization in the year following an acute COPD exacerbation. The model demonstrated good internal validation performance (C-index = 0.730, AUC = 0.730). For clinical application, healthcare providers can input individual patient characteristics (eg, age, exacerbation type, CK level) into the nomogram to generate a personalized risk score, facilitating early intervention and resource allocation for high-risk subgroups. However, further external validation is necessary before widespread implementation. It is important to note that current therapeutic strategies, including bronchodilators and inhaled corticosteroids, remain central to COPD management by providing symptomatic relief and reducing exacerbation frequency in certain populations 36. Our study does not seek to diminish their role but rather to complement existing approaches by identifying novel risk factors for targeted prevention.
This study is subject to several limitations. The retrospective design, while offering a large sample size, does not account for potential confounders that may have influenced the results, which could affect the accuracy and generalizability of the findings. Additionally, the lack of multicenter validation restricts the broader applicability of our conclusions. Variability within the dataset may have also impacted the precision of the analyses. Lastly, the absence of wet-lab data for certain biomarkers may have constrained the depth of our understanding of patient outcomes. Future research should focus on prospective, multicenter studies to further validate and expand upon the findings of this investigation.
Conclusions
In conclusion, this study provides a systematic evaluation of risk factors for rehospitalization within 30 days and frequent rehospitalization within the subsequent year following acute exacerbations of COPD. Age, total protein, albumin, disease duration, and Anthonisen classification were identified as key predictors of rehospitalization risk. By developing a nomogram-based predictive model, we offer a potentially useful tool for clinicians to identify high-risk patients, enabling more efficient resource allocation and the possibility of reducing rehospitalization rates. Nevertheless, this study’s limitations underscore the need for further multicenter validation and the exploration of personalized intervention strategies. Future by incorporating genetic and biomarker data, investigating the impact of early interventions on long-term outcomes, and assessing the effectiveness of tailored treatments for different patient subgroups. Further validation through multicenter trials will enhance the generalizability of the findings and contribute to the development of personalized care protocols for COPD patients.
Abbreviations
COPD, chronic obstructive pulmonary disease; ALT, alanine aminotransferase; CK, creatine kinase; GLU, glucose; WHO, World Health Organization; AECOPD, Acute exacerbations of COPD; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ROC, receiver operating characteristic; AUC, area under the ROC curve; DCA, decision curve analysis.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study received approval from the Ethics Committee of Beijing Luhe Hospital, Capital Medical University (Approval No: 2020-LHKY-014-03). Given the retrospective and observational nature of the study, which utilized anonymized data, the Ethics Committee granted an exemption from informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jarhyan P, Hutchinson A, Khaw D, Prabhakaran D, Mohan S. Prevalence of chronic obstructive pulmonary disease and chronic bronchitis in eight countries: a systematic review and meta-analysis. Bull World Health Organ. 2022;100(3):216–13. doi:10.2471/BLT.21.286870
2. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/S0140-6736(22)00470-6
3. Varmaghani M, Dehghani M, Heidari E, Sharifi F, Moghaddam SS, Farzadfar F. Global prevalence of chronic obstructive pulmonary disease: systematic review and meta-analysis. East Mediterr Health J. 2019;25(1):47–57. doi:10.26719/emhj.18.014
4. Vogelmeier CF, Román-Rodríguez M, Singh D, Han MK, Rodríguez-Roisin R, Ferguson GT. Goals of COPD treatment: focus on symptoms and exacerbations. Respir Med. 2020;166:105938. doi:10.1016/j.rmed.2020.105938
5. Ko FW, Chan KP, Hui DS, et al. Acute exacerbation of COPD. Respirology. 2016;21(7):1152–1165. doi:10.1111/resp.12780
6. Mantero M, Rogliani P, Di Pasquale M, et al. Acute exacerbations of COPD: risk factors for failure and relapse. Int J Chron Obstruct Pulmon Dis. 2017;12:2687–2693. doi:10.2147/COPD.S145253
7. Mathioudakis AG, Janssens W, Sivapalan P, et al. Acute exacerbations of chronic obstructive pulmonary disease: in search of diagnostic biomarkers and treatable traits. Thorax. 2020;75(6):520–527. doi:10.1136/thoraxjnl-2019-214484
8. Zhou A, Zhou Z, Zhao Y, Chen P. The recent advances of phenotypes in acute exacerbations of COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:1009–1018. doi:10.2147/COPD.S128604
9. MacLeod M, Papi A, Contoli M, et al. Chronic obstructive pulmonary disease exacerbation fundamentals: diagnosis, treatment, prevention and disease impact. Respirology. 2021;26(6):532–551. doi:10.1111/resp.14041
10. Duffy SP, Criner GJ. Chronic obstructive pulmonary disease: evaluation and management. Med Clin North Am. 2019;103(3):453–461. doi:10.1016/j.mcna.2018.12.005
11. Gerald LB, Bailey WC. Global initiative for chronic obstructive lung disease. J Cardiopulm Rehabil. 2002;22(4):234–244. doi:10.1097/00008483-200207000-00004
12. Wedzicha JA, Singh R, Mackay AJ. Acute COPD exacerbations. Clin Chest Med. 2014;35(1):157–163. doi:10.1016/j.ccm.2013.11.001
13. Basler S, Sievi NA, Schmidt F, et al. Molecular breath profile of acute COPD exacerbations. J Breath Res. 2024;19(1). doi:10.1088/1752-7163/ad9ac4
14. Meeraus WH, DeBarmore BM, Mullerova H, Fahy WA, Benson VS. Terms and definitions used to describe recurrence, treatment failure and recovery of acute exacerbations of COPD: a systematic review of observational studies. Int J Chron Obstruct Pulmon Dis. 2021;16:3487–3502. doi:10.2147/COPD.S335742
15. Sadatsafavi M, McCormack J, Petkau J, Lynd LD, Lee TY, Sin DD. Should the number of acute exacerbations in the previous year be used to guide treatments in COPD? Eur Respir J. 2021;57(2):2002122. doi:10.1183/13993003.02122-2020
16. Gloeckl R, Schneeberger T, Jarosch I, Kenn K. Pulmonary rehabilitation and exercise training in chronic obstructive pulmonary disease. Dtsch Arztebl Int. 2018;115(8):117–123. doi:10.3238/arztebl.2018.0117
17. Wu YK, Lan CC, Tzeng IS, Wu CW. The COPD-readmission (CORE) score: a novel prediction model for one-year chronic obstructive pulmonary disease readmissions. J Formos Med Assoc. 2021;120(3):1005–1013. doi:10.1016/j.jfma.2020.08.043
18. Chow R, So OW, JHB I, et al. Predictors of readmission, for patients with chronic obstructive pulmonary disease (COPD) - A systematic review. Int J Chron Obstruct Pulmon Dis. 2023;18:2581–2617. doi:10.2147/COPD.S418295
19. Halpin DM, Miravitlles M, Metzdorf N, Celli B. Impact and prevention of severe exacerbations of COPD: a review of the evidence. Int J Chron Obstruct Pulmon Dis. 2017;12:2891–2908. doi:10.2147/COPD.S139470
20. Wu YK, Su WL, Yang MC, Chen SY, Wu CW, Lan CC. Characterization associated with the frequent severe exacerbator phenotype in COPD patients. Int J Chron Obstruct Pulmon Dis. 2021;16:2475–2485. doi:10.2147/COPD.S317177
21. Huerta A, Soler N, Esperatti M, et al. Importance of aspergillus spp. isolation in acute exacerbations of severe COPD: prevalence, factors and follow-up: the FUNGI-COPD study. Respir Res. 2014;15(1):17. doi:10.1186/1465-9921-15-17
22. Kahnert K, Jörres RA, Behr J, Welte T. The diagnosis and treatment of COPD and its comorbidities. Dtsch Arztebl Int. 2023;120(25):434–444. doi:10.3238/arztebl.m2023.027
23. Sandelowsky H, Weinreich UM, Aarli BB, et al. COPD - do the right thing. BMC Fam Pract. 2021;22(1):244. doi:10.1186/s12875-021-01583-w
24. Hobman A, Levack WMM, Jones B, et al. Prevention of re-hospitalization for acute exacerbations: perspectives of people with chronic obstructive pulmonary disease: a qualitative study. Int J Chron Obstruct Pulmon Dis. 2023;18:207–218. doi:10.2147/COPD.S393645
25. Zhou Y, Thanathi Mohamed Ameen MNA, Li W, et al. Main pulmonary artery enlargement predicts 90-day readmissions in Chinese COPD patients. J Thorac Dis. 2021;13(10):5731–5740. doi:10.21037/jtd-21-344
26. Zhi J, Shan Q, Liang L, Liu H, Huang H. Low skeletal muscle area as a prognostic marker for chronic obstructive pulmonary disease in elderly patients admitted to ICU. Sci Rep. 2019;9(1):19117. doi:10.1038/s41598-019-55737-z
27. Hogea SP, Tudorache E, Fildan AP, Fira-Mladinescu O, Marc M, Oancea C. Risk factors of chronic obstructive pulmonary disease exacerbations. Clin Respir J. 2020;14(3):183–197. doi:10.1111/crj.13129
28. Zhu D, Dai H, Zhu H, et al. Identification of frequent acute exacerbations phenotype in COPD patients based on imaging and clinical characteristics. Respir Med. 2023;209:107150. doi:10.1016/j.rmed.2023.107150
29. Ramya PA, Mohapatra MM, Saka VK, Kar R, Chakkalakkoombil SV, Vemuri MB. Haematological and inflammatory biomarkers among stable COPD and acute exacerbations of COPD patients. Sultan Qaboos Univ Med J. 2023;23(2):239–244. doi:10.18295/squmj.12.2022.062
30. Han H, Hu S, Du J. Predictive value of the hemoglobin-albumin-lymphocyte-platelet (HALP) index for ICU mortality in patients with acute exacerbations of chronic obstructive pulmonary disease (AECOPD). Intern Emerg Med. 2023;18(1):85–96. doi:10.1007/s11739-022-03132-4
31. Zeng Z, Ke X, Gong S, et al. Blood urea nitrogen to serum albumin ratio: a good predictor of in-hospital and 90-day all-cause mortality in patients with acute exacerbations of chronic obstructive pulmonary disease. BMC Pulm Med. 2022;22(1):476. doi:10.1186/s12890-022-02258-7
32. Gallego M, Pomares X, Capilla S, et al. C-reactive protein in outpatients with acute exacerbation of COPD: its relationship with microbial etiology and severity. Int J Chron Obstruct Pulmon Dis. 2016;11:2633–2640. doi:10.2147/COPD.S117129
33. Machado A, Matos Silva P, Afreixo V, Caneiras C, Burtin C, Marques A. Design of pulmonary rehabilitation programmes during acute exacerbations of COPD: a systematic review and network meta-analysis. Eur Respir Rev. 2020;29(158):200039. doi:10.1183/16000617.0039-2020
34. Lasman N, Shalom M, Turpashvili N, et al. Baseline low ALT activity is associated with increased long-term mortality after COPD exacerbations. BMC Pulm Med. 2020;20(1):133. doi:10.1186/s12890-020-1169-z
35. Karimi L, Lahousse L, Ghanbari M, et al. β(2)-adrenergic receptor (ADRB2) gene polymorphisms and risk of COPD exacerbations: the rotterdam study. J Clin Med. 2019;8(11):1835. doi:10.3390/jcm8111835
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.