Back to Journals » ImmunoTargets and Therapy » Volume 15
Identification of Comprehensive Landscape of Peripheral Immunity and Chemokine-Related Genes in Amyotrophic Lateral Sclerosis
Authors Yang X, Huang S, Wang Y, Yuan J, Yao X ![]()
Received 11 September 2025
Accepted for publication 31 December 2025
Published 9 January 2026 Volume 2026:15 566733
DOI https://doi.org/10.2147/ITT.S566733
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah Wheeler
Xinyu Yang,1– 3,* Sen Huang,1– 3,* Yuxin Wang,1– 3 Jing Yuan,1– 3 Xiaoli Yao1– 3
1Department of Neurology, The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 2Guangdong Provincial Key Laboratory of Diagnosis and Treatment of Major Neurological Diseases, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China; 3National Key Clinical Department and Key Discipline of Neurology, The First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoli Yao, Department of Neurology, The First Affiliated Hospital, Sun Yat-Sen University, No. 58 Zhongshan Road 2, Guangzhou, 510080, People’s Republic of China, Email [email protected]
Purpose: Amyotrophic lateral sclerosis (ALS) is a fatal neurodegenerative disease. Progressive loss of motor neuron function and disruption of the blood-brain barrier are key features of ALS. Under the influence of chemokines, peripheral immune cells migrate into the central nervous system, thereby affecting the neuronal microenvironment. The aim of this study is to classify ALS based on the immune characteristics of peripheral blood in patients with the disease, and to construct prognostic models.
Patients and Methods: A total of 397 ALS patients and 645 healthy controls (GSE112676 and GSE112680) were included. ALS chemotactic subtypes were constructed based on differentially expressed genes of chemokine and chemokine receptors (CCRs). The Cibersort algorithm was used to investigate the abundance of immune cells in peripheral blood. Univariate Cox regression analysis was performed to screen for CCRs genes, clinical characteristics, and immune cells associated with prognosis. Prognostic models were constructed based on these variables. Finally, external validation was conducted using samples from ALS patients diagnosed at the First Affiliated Hospital of Sun Yat-sen University.
Results: There were significant differences in the abundance of peripheral immune cells between ALS patients and healthy controls. 17 CCRs genes were identified as differentially expressed. CCL23, CCR8, CXCR4, site of onset, age of onset, and “CD4 naive T cells” were demonstrated to be significantly correlated with survival time. Two chemotactic subtypes were established. Eight prognostic models could distinguish between high-risk and low-risk ALS patients. At year five, the areas under the receiver operating characteristic curves for the PlsRcox, Coxboost, and Xgboost algorithms were 0.747, 0.733, and 0.728, respectively. External test sets successfully validated these results.
Conclusion: ALS patients exhibit peripheral immune abnormalities. Peripheral immune status could be used to distinguish ALS subtypes and construct prognostic models. Understanding peripheral immune changes in ALS patients may inform potential immunotherapies.
Keywords: amyotrophic lateral sclerosis, peripheral immunity, chemokine, chemokine receptor
Introduction
Amyotrophic lateral sclerosis (ALS) is a rare and fatal neurodegenerative disease. According to 2016 data, the reported incidence of ALS in China was approximately 1.65 per 100,000, with a higher incidence in men than in women, and the incidence gradually increase with age.1 ALS has heterogeneous clinical manifestations, primarily characterized by damage to upper and lower motor neurons, resulting in progressive, painless muscle weakness and atrophy in the medulla oblongata and limbs. Symptoms include dysarthria, dysphagia, choking when drinking water, and decreased muscle strength in the limbs.2 ALS can be classified as familial or sporadic types. Familial ALS is primarily associated with genetic mutations, particularly in genes such as superoxide dismutase 1, TAR DNA-binding protein 43 and fused in sarcoma. In contrast, the pathogenesis of sporadic ALS remains unclear.3
Peripheral blood testing is a promising approach for diagnosing and treating ALS due to its cost-effectiveness and minimal invasiveness.4 Recently, it has been demonstrated that the peripheral immune response participates in the pathological progression of ALS by producing inflammatory factors and undergoing changes in the number of immune cells.5 For instance, elevated levels of Th2 cells and regulatory T cells (Tregs) in the early stages of ALS have been associated with longer survival.6 These cells are thought to have neuroprotective effects through their interaction with microglia via the secretion of anti-inflammatory cytokines from the peripheral immune system, such as interleukin 4 and interleukin 10.7,8 As the disease progresses, there is a shift towards neurotoxic, pro-inflammatory Th1 and Th17 cells, accompanied by a reduction in Th2 and Treg cells. An increase in Th17 cells has been linked to greater functional disability and is mediated by the secretion of pro-inflammatory cytokines, such as interleukin 17 and interleukin 23.9 In addition, CD8+ T cells mediated neurotoxicity through the Fas/FasL and granzyme/perforin pathways following infiltration into the spinal cord.10 Furthermore, natural killer cells and neutrophils in the peripheral blood of ALS patients can infiltrate the spinal cord, carrying a poor prognosis.11,12 Therefore, exploring the immune status of peripheral blood may help to elucidate the mechanisms of ALS progression and subtype classification and predict survival.
In this study, whole blood transcriptome data from the Gene Expression Omnibus (GEO) to reveal differences in the immune microenvironment and abnormally activated pathways in the peripheral blood of patients with sporadic ALS. Meanwhile, data from the First Affiliated Hospital of Sun Yat-sen University were used to validate the above results. We hope that our study may contribute to the accurate diagnosis and treatment of ALS.
Material and Methods
Datasets and Quality Control
Whole blood human ALS microarray datasets (GSE112676 and GSE112680) were retrieved from the GEO database. These datasets comprise 397 ALS samples and 645 healthy control samples. The “sva” package was used to remove batch effects from the two datasets (Supplementary Figure 1). The study flow chart is shown in Figure 1.
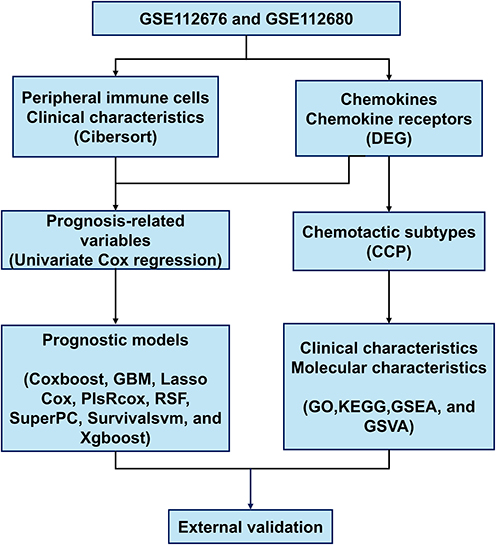 |
Figure 1 Study flow chart. |
Evaluation of Immune Cells in Peripheral Blood
The Cibersort algorithm was used to calculate the relative abundance of 22 immune cells in different groups (https://cibersortx.stanford.edu/).
Differentially Expressed Genes Analysis and Consensus Clustering Analysis
The “Limma” package was used for the analysis of differentially expressed genes (DEGs), with the “adjust-p ≤ 0.05” criterion set. The “ConsensusClusterPlus (CCP)” and “Limma” packages were used for consensus clustering analysis.
Construction of the Prognostic Model
Univariate Cox regression analysis was performed on the clinical characteristics, immune cell abundance, and DEGs of chemokines or chemokine receptors to identify variables with significant differences (p ≤ 0.05). The ALS prognostic models were constructed using eight algorithms, including Coxboost, Gradient Boosting Machine (GBM), Lasso Cox, PlsRcox, Random Survival Forests (RSF), SuperPC, Survivalsvm, and Xgboost. The time-dependent receiver operating characteristic (ROC) analysis was performed to assess patient survival at 1, 3, and 5 years. The area under the curve (AUC) was used to evaluate their performance.
Enrichment Analysis
The “ClusterProfiler” package and DEGs (|log2FC| ≥ 1, adjust-p ≤ 0.05) of subgroups were used to analysis gene ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG). Gene set enrichment analysis (GSEA) incorporated the ranking and weighting of log2FC values into its analysis. Given the large sample size, gene set variation analysis (GSVA) was also applicable to this study. The “Limma” and “GSVA” packages were used for GSVA.
External Test Set
The external test set comprises transcriptome sequencing data from the whole blood samples of 32 ALS patients. These patients were diagnosed at the First Affiliated Hospital of Sun Yat-sen University between July and December 2021. Clinical information and whole blood samples of patients were collected at the time of diagnosis. The follow-up period ends in March 2025. RNA was extracted from samples using TRIzol. Oligo dT-coated magnetic beads were used for enriching mRNA from the total RNA. Quality analysis was performed using an Agilent 2100 Bioanalyzer. Libraries were sequenced on an Illumina platform. This study complied with the Declaration of Helsinki and was approved by Ethic Committee for clinical research and animal trials of the First Affiliated Hospital, Sun Yat-sen University ([2021]260).
Results
The Immune Cells of Peripheral Blood in ALS Patients and Healthy Controls
The immune cells of peripheral blood in 397 ALS patients and 645 healthy controls were analyzed using the CIBERSORT algorithm (Figure 2A). The results revealed significant differences in immune cell composition between ALS patients and healthy controls (Figure 2B). The relative amounts of “T cells CD4 memory resting”, “Monocytes”, and “Neutrophils” in the patient group were significantly higher than that in the healthy group. In contrast, the healthy group had more “T cells regulatory”, “NK cells resting”, and “Dendritic cells activated” than the patient group. The effects of gender, site of onset, and age of onset on peripheral blood immune cells in ALS patients were further evaluated. Male patients had higher “T cells CD4 memory activated”, “NK cells resting”, “Monocytes”, “Mast cells resting” (Figure 2C and D). Patients with bulbar-onset had higher levels of “B cells CD4 memory”, “T cells CD4 memory activated”, “T cells regulatory”, and “Dendritic cells activated”, while patients with spina-onset had higher levels of “monocytes” (Figure 2E and F). For patients of different ages, “T cells CD4 naive”, “T cells CD4 memory resting” and “T cells regulatory” were higher in the lower-age group and “Monocytes” were higher in the higher-age group (Figure 2G and H). In summary, the proportion of peripheral blood immune cells in ALS patients was abnormal, with a high degree of heterogeneity among individuals.
Figure 2 Continued. Figure 2 Abundance of peripheral blood immune cells. (A) Abundance of peripheral blood immune cells in ALS patients and healthy controls. (B) Differences in peripheral blood immune cells between ALS patients and healthy controls. (C) Abundance of peripheral blood immune cells in male and female ALS patients. (D) Differences in peripheral blood immune cells between male and female ALS patients. (E) Abundance of peripheral blood immune cells in bulbar-onset and spinal-onset ALS patients. (F) Differences in peripheral blood immune cells between bulbar-onset and spinal-onset ALS patients. (G) Abundance of peripheral blood immune cells in high-age and lower-age ALS patients. (H) Differences in peripheral blood immune cells between high-age and lower-age ALS patients. *P < 0.05, **P < 0.01, ***P < 0.001.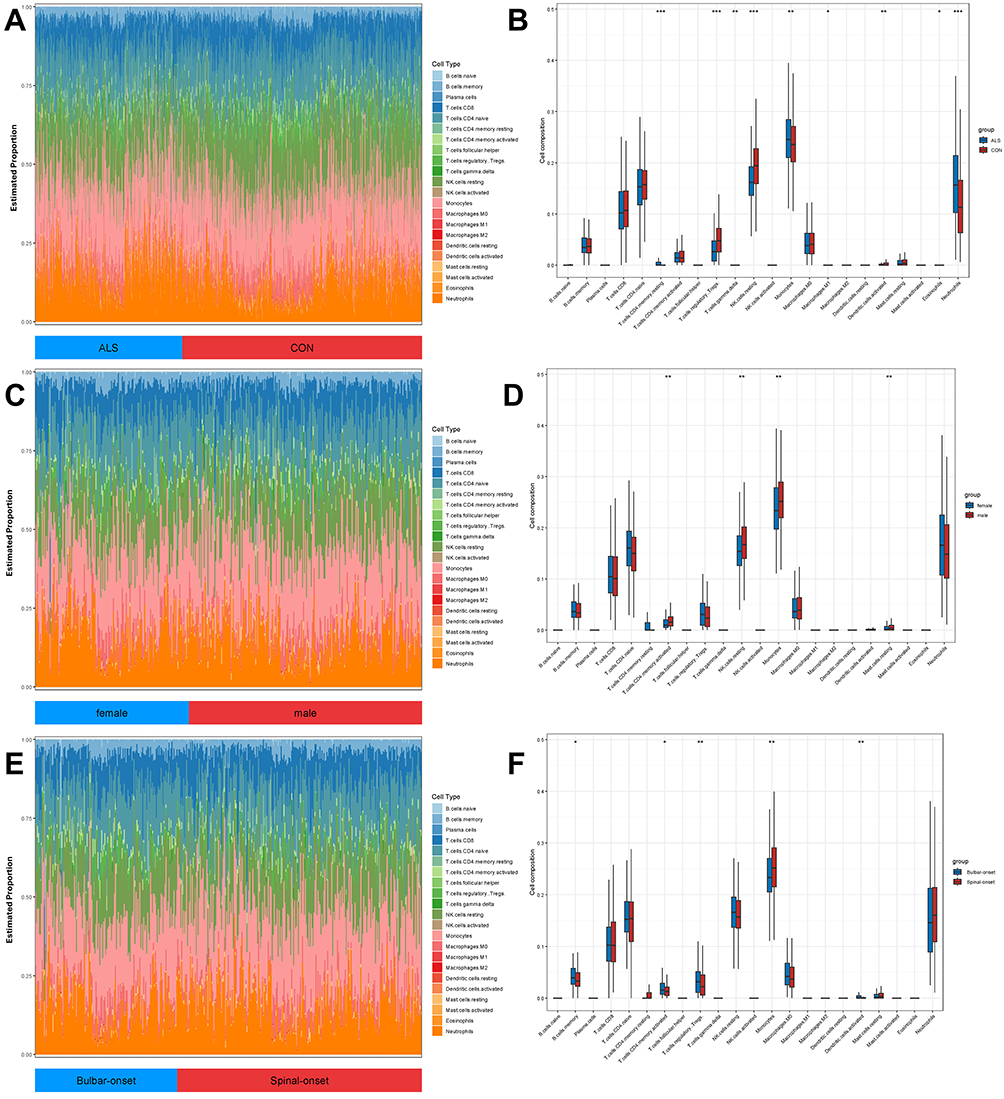
Classification of ALS Subtypes Based on Chemokine and Their Receptors
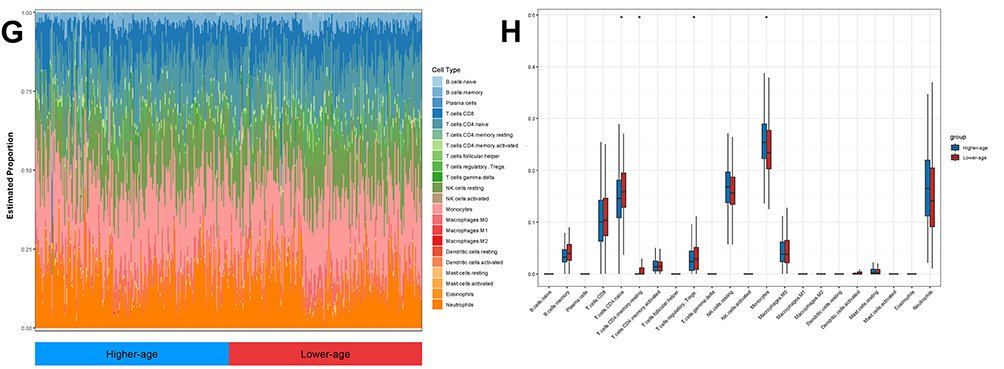
The infiltration of peripheral blood immune cells into the central nervous system is largely depends on chemokines and their receptors. DEG analysis of peripheral blood from ALS patients and healthy controls identified 8,213 differentially expressed genes (Supplementary Figure 2A). Compared with a collection of 64 chemokines and their receptors,13 17 differentially expressed genes were selected for ALS subtype classification (Supplementary Figure 2B). Based on these 17 genes of chemokines and their receptors, the CCP algorithm was used to classify ALS patients into subtypes. The results showed significant differences between groups when ALS patients were divided into two (group A) or three (group B) groups (Figure 3A and B). These ALS subtypes were defined as chemotactic subtypes.
 |
Figure 3 Clinical characteristics of chemotactic subtypes. (A) Consensus matrices of A groups in chemotactic subtypes. (B) Consensus matrices of B groups in chemotactic subtypes. (C) Differences in age of onset between group A1 and group A2. (D) Differences in gender between group A1 and group A2. (E) Differences in site of onset between group A1 and group A2. (F) Differences in age of onset among groups B1, B2, and B3. (G) Differences in gender among groups B1, B2, and B3. (H) Differences in site of onset among groups B1, B2, and B3. (I) Differences in peripheral blood immune cells between group A1 and group A2. (J) Differences in peripheral blood immune cells among groups B1, B2, and B3. *P < 0.05, ***P < 0.001. Abbreviation: NS, no significance. |
Clinical Characteristics of Chemotactic Subtypes
When ALS patients were divided into two groups, each group was named group A1 and group A2. The age of onset was later in group A1 than in group A2 (Figure 3C). Furthermore, the majority of patients in group A1 were spinal-onset (Figure 3D). However, there were no significant gender differences between the two groups (Figure 3E). Moreover, monocytes and neutrophils were higher in group A1 than in group A2, suggesting a higher inflammatory state of peripheral blood in group A1. Memory B cells, naive CD4+ T cells, and Tregs were higher in group A2 than in group A1, suggesting a stronger immune regulatory capacity in group A2 (Figure 3F). When ALS patients were divided into three groups, they were named group B1, B2 and B3. The age of onset in group B3 was significantly younger than that in groups B1 and B2 (Figure 3G). In addition, the proportion of males in group B2 was significantly higher than that in groups B1 and B3 (Figure 3H). However, there was no significant difference in the location of onset among the three patient groups (Figure 3I). The classification of the three groups also revealed significant differences in peripheral blood immune cells in each group, including “T cells CD8”, “T cells CD4 naive”, “T cells regulatory”, “Monocytes”, and “Neutrophils” (Figure 3J). In summary, ALS patients in different groups exhibit differences in clinical characteristics and peripheral immunity based on the classification of chemotactic subtypes.
Gene Ontology Features of Chemotactic Subtypes
To further distinguish differences among ALS subtypes, GO database, GSEA and GSVA were used to characterize the features of different subgroups. Groups A1 and A2 were found to differ in terms of protein synthesis, transport, metabolism, and immune regulation (Figure 4A, B). Further GSVA analysis revealed that group A1 exhibited stronger protein synthesis, transport, and metabolic capabilities, while group A2 demonstrated superior immune regulatory capacity (Figure 4C). When ALS patients were divided into three groups, group B1 exhibited strong protein synthesis, transport, and metabolic capabilities, but relatively weak glucose metabolism (Figure 4D–F). Group B2 was highly correlated with immune regulation (Figure 4G–I). Group B3 exhibited strong nucleotide metabolism but reduced protein modification capacity (Figure 4J–L). In summary, there are distinct differences exist among chemotactic subgroups in terms of biological processes, cellular components, and molecular functions.
Figure 4 Continued. Figure 4 Gene ontology features of chemotactic subtypes. (A) GO of group A1 and group A2. (B) GSEA of group A1 and group in GO A2. (C) GSVA of group A1 and group A2 in GO. (D) GO of group B1. (E) GSEA of group B1 in GO. (F) GSVA of group B1 in GO. (G) GO of group B2. (H) GSEA of group B2 in GO. (I) GSVA of group B2 in GO. (J) GO of group B3. (K) GSEA of group B3 in GO. (L) GSVA of group B3 in GO.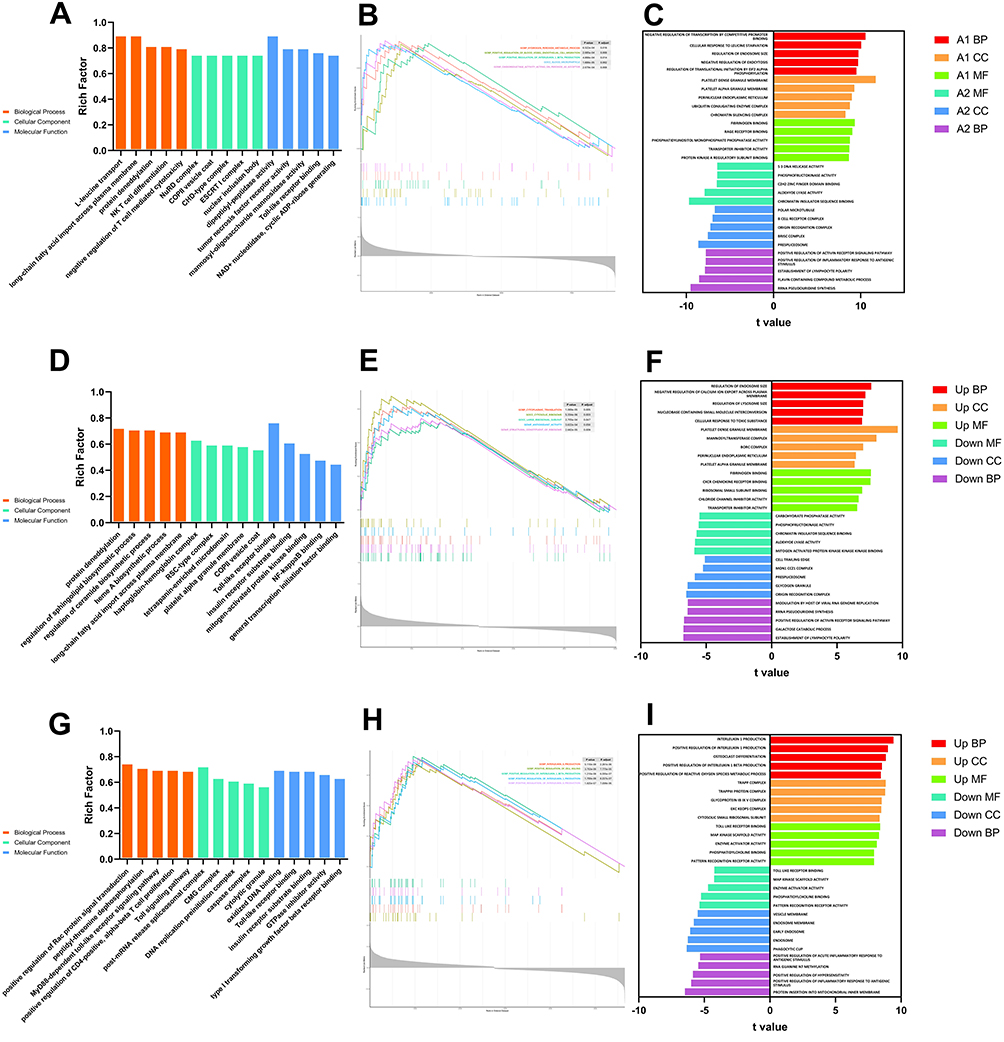
Molecular Pathways of Chemotactic Subtypes
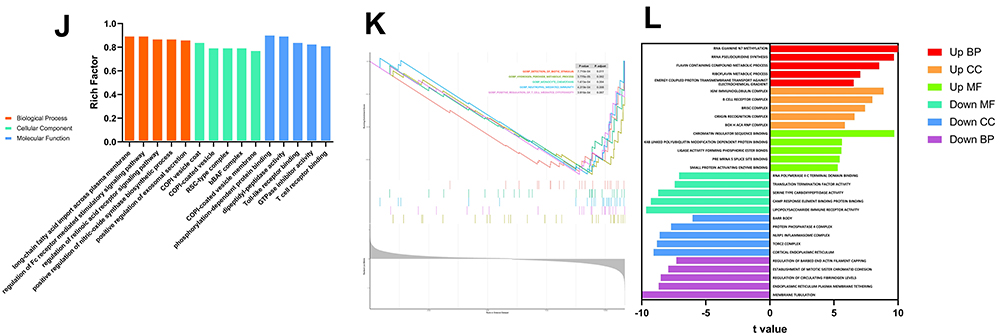
The KEGG database, GSEA, and GSVA were used to distinguish molecular pathways among chemotactic subgroups. Group A1 may be associated with GTPase regulation (Rho signaling pathways), whereas group A2 lacks specific pathways (Figure 5A and B). Similar to group A1, group B1 may also be associated with GTPase regulation and mitophagy, including the Rho and Parkin signaling pathways (Figure 5C–E). In addition, the activating transcription factor 5 (ATF5) signaling pathway was up-regulated and the Wnt signaling pathway was down-regulated in group B1 (Figure 5E). Group B2 exhibits upregulation of the inflammasome and Ras signaling pathways, suggesting its immune activation status (Figure 5F and G). In contrast to group B1, group B3 exhibited upregulation of the Wnt signaling pathway and downregulation of the Rho signaling pathway (Figure 5H and I). In summary, the changes in signaling pathways among the chemotactic subgroups are distinct.
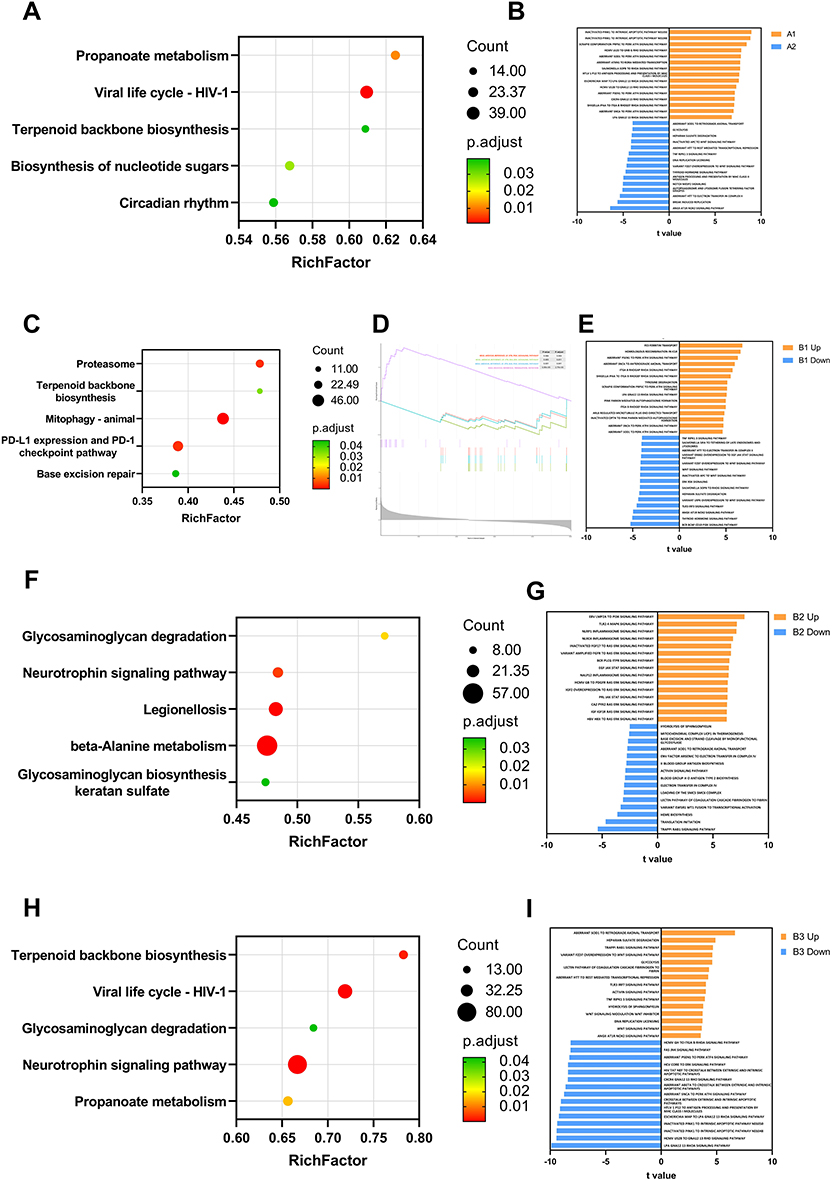 |
Figure 5 Molecular pathways of chemotactic subtypes. (A) KEGG of group A1 and group A2. (B) GSVA of group A1 and group A2 in KEGG. (C) KEGG of group B1. (D) GSEA of group B1 in KEGG. (E) GSVA of group B1 in KEGG. (F) KEGG of group B2. (G) GSVA of group B2 in KEGG. (H) KEGG of group B3. (I) GSVA of group B3 in KEGG. |
Construction and Validation of Prognostic Models
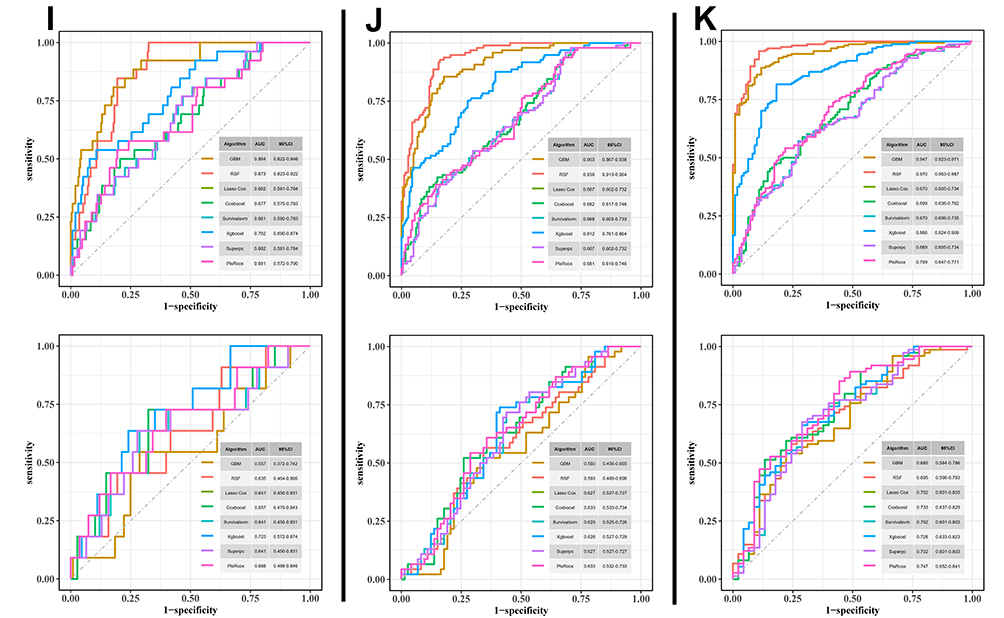
A total of 397 ALS patients were randomly assigned to a train set and a test set in a 3:1 ratio. Univariate Cox regression analysis was employed to identify variables in the train set that were significantly associated with survival time in ALS patients. Three chemokines or chemokine receptors (CCL23, CCR8, and CXCR4), site of onset, age of onset, and “T cells CD4 naive” abundance were demonstrated to be significantly correlated with survival time in ALS patients (Supplementary Table 1). Simultaneously, the multicollinearity analysis of the six variables revealed no evidence of collinearity among them (Supplementary Table 2). Based on the above variables, eight machine learning algorithms were employed to construct prognostic models, including Coxboost, GBM, Lasso Cox, PlsRcox, RSF, SuperPC, Survivalsvm, and Xgboost. These eight survival models have been validated in the test set and were shown to effectively distinguish high-risk patients from low-risk patients (Figure 6A–H). Additionally, time-dependent ROC analysis was performed to assess patient survival at one, three, and five years. The results indicate relatively poor predictive performance in the first and third years (Figure 6I and J), while significant improvement was observed in the fifth year (Figure 6K). Among them, the PlsRcox, Coxboost, and Xgboost algorithms demonstrated the best predictive performance, with area under the curve (AUC) values of 0.747, 0.733, and 0.728, respectively. Based on this analysis, we identified variables associated with prognosis and established models capable of predicting the prognosis of ALS patients. Therefore, six variables associated with ALS prognosis were identified, and three reliable ALS prognostic models were established.
Figure 6 Continued. Figure 6 Construction and validation of prognostic models. (A) Construction and validation of survival curves for high-risk and low-risk groups by Coxboost algorithm. (B) Construction and validation of survival curves for high-risk and low-risk groups by GBM algorithm. (C) Construction and validation of survival curves for high-risk and low-risk groups by Lasso Cox algorithm. (D) Construction and validation of survival curves for high-risk and low-risk groups by PlsRcox algorithm. (E) Construction and validation of survival curves for high-risk and low-risk groups by RSF algorithm. (F) Construction and validation of survival curves for high-risk and low-risk groups by SuperPC algorithm. (G) Construction and validation of survival curves for high-risk and low-risk groups by Survivalsvm algorithm. (H) Construction and validation of survival curves for high-risk and low-risk groups by Xgboost algorithm. (I) The predictive efficiency of the risk signature in receiver operating characteristic curves at the first year. (J) The predictive efficiency of the risk signature in receiver operating characteristic curves at the third year. (K) The predictive efficiency of the risk signature in receiver operating characteristic curves at the fifth year. In each panel: Train set (upper graph); Test set (lower graph).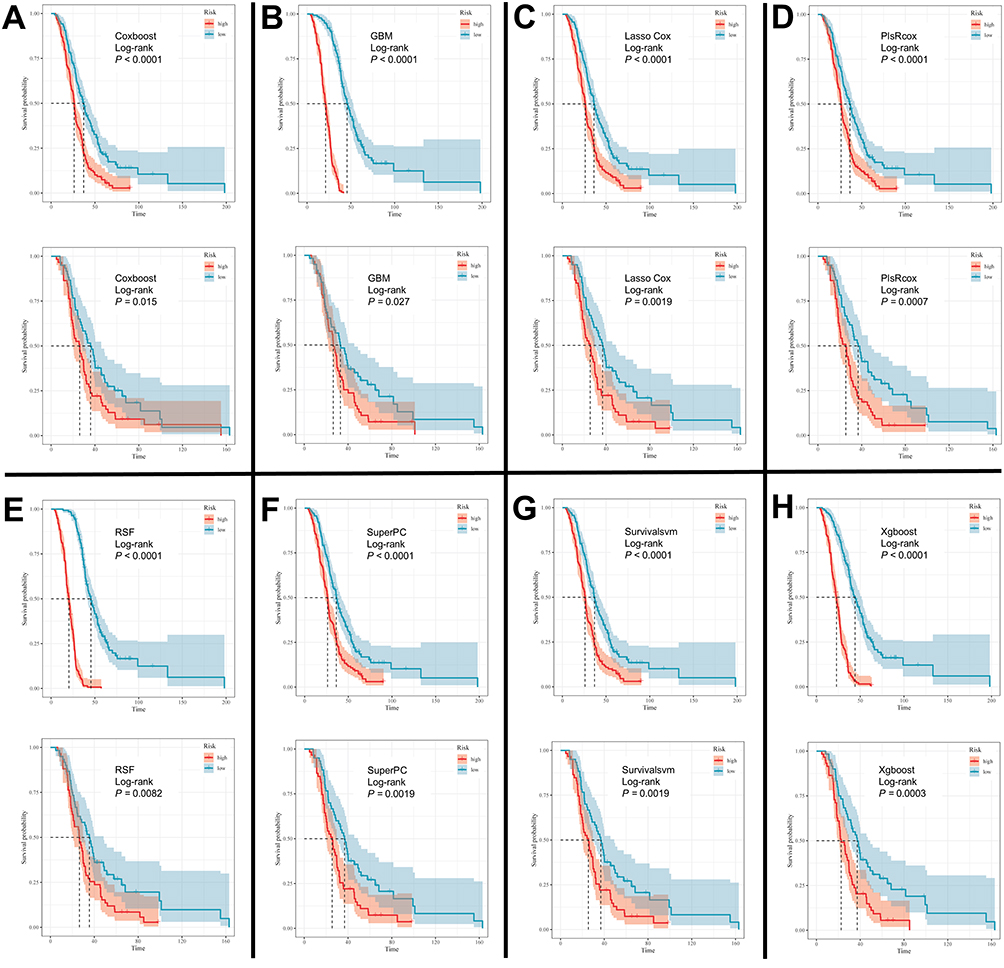
Validation of Chemotactic Subtypes in External Test Set
Transcriptome sequencing data from peripheral blood samples of 32 ALS patients from the First Affiliated Hospital of Sun Yat-sen University were used as an external validation set (Supplementary Table 3). Similar to the data from GSE112676 and GSE112680, the external dataset showed consistent proportions of peripheral blood immune cell abundance across different subgroups. For instance, male patients exhibited higher levels of “T cells CD4 memory activated” and “NK cells resting” in the external test set (Figure 7A). Although there were no significant differences in immune cell abundance across subgroups defined by site of onset or age of onset, a similar trend was observed (Figure 7B and C). Then, 17 chemokines or chemokine receptors were used to distinguish ALS subtypes in the external test set. When the ALS patients were divided into two groups, significant differences were observed between the groups (Figure 7D). Although no significant difference was observed, the age of onset in group A2 was earlier, consistent with the test set (Figure 7E). Due to the small sample size of the external test set, no significant differences were observed in gender, or site of onset (Supplementary Figure 3A and B). Finally, the above 6 variables (Supplementary Table 1) and eight algorithms were used to construct a prognostic model in external test set. Lasso Cox, SuperPC, Survivalsvm, and Xgboost successfully distinguished the high-risk group and the low-risk group (Figure 7F–I), while Coxboost, GBM, RSF, and PlsRcox failed (Supplementary Figure 3C–F). In summary, the external test set confirmed the chemotactic subtypes and prognostic models for ALS patients.
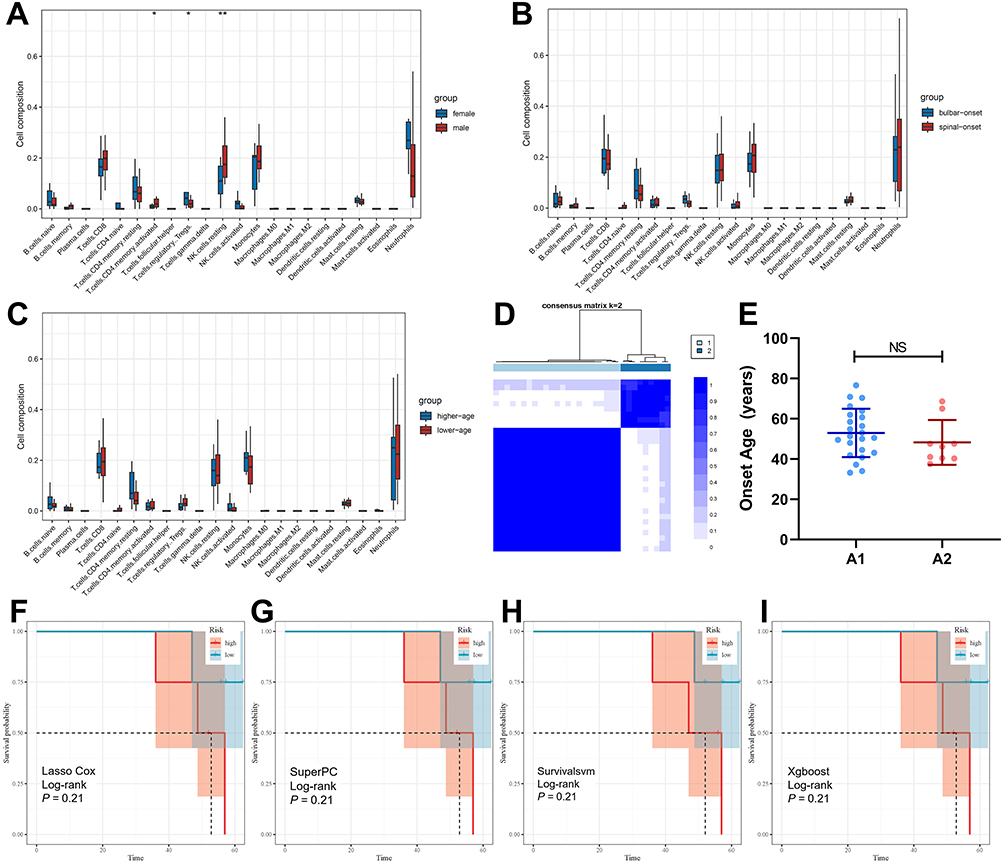 |
Figure 7 Validation of chemotactic subtypes in external test set. (A) Differences in peripheral blood immune cells between male and female ALS patients. (B) Differences in peripheral blood immune cells between bulbar-onset and spinal-onset ALS patients. (C) Differences in peripheral blood immune cells between higher-age and lower-age ALS patients of external test set. (D) Consensus matrices of A groups in chemotactic subtypes. (E) Differences in age of onset between group A1 and group A2. (F) External validation of survival curves for high-risk and low-risk groups by Lasso Cox algorithm. (G) External validation of survival curves for high-risk and low-risk groups by SuperPC algorithm. (H) External validation of survival curves for high-risk and low-risk groups by Survivalsvm algorithm. (I) External validation of survival curves for high-risk and low-risk groups by Xgboost algorithm. *P < 0.05, **P < 0.01. Abbreviation: NS, no significance. |
Discussion
The median survival time for ALS patients is typically only 3–5 years, with a poor prognosis and significant individual variation.14 This study aims to establish a new subtype classification for ALS and develop prognostic models to predict survival duration in ALS patients. In this study, chemotactic subtypes of ALS were constructed based on the expression levels of peripheral blood chemokines and their receptors. Additionally, we used eight algorithms to develop prognostic models for ALS patients. Finally, we validated these results using an external test set from the First Affiliated Hospital of Sun Yat-sen University.
ALS patients exhibit an abnormal abundance of immune cells in peripheral blood. In our study, ALS patients showed elevated expression levels of neutrophils and monocytes, though CD8+ T cells did not change significantly. Flow cytometry also validated this finding.5 Gender, age of onset, and site of onset are important clinical characteristics of ALS patients.15 Increasing age and male gender are two significant risk factors for ALS, with an incidence ratio of 1.5:1 between males and females.16 Bulbar ALS is considered one of the most severe ALS because the appearance of bulbar symptoms is linked to a quicker decline in function and a reduced survival period.17 Additionally, we found that the abundance of peripheral blood immune cells varies among ALS patients of different genders, ages of onset, sites of onset. Typically, peripheral immune cells cannot directly affect the central nervous system (CNS). However, ALS patients exhibit impaired blood-brain barrier function, which allows peripheral immune cells to infiltrate the CNS under the influence of chemokines, thereby affecting neuronal function and activity.18–20 Therefore, this study focused on the expression levels of chemokines and their receptors to classify subtypes of ALS patients.
In this study, “T cells CD4 naive” and CCL23 were identified as prognostic protective factors for ALS, while CCR8 and CXCR4 were identified as risk factors. Naive CD4 T cells possess potent differentiation potential. Under stimulation by cytokines such as interleukins and transforming growth factors, naive CD4 T cells can differentiate into Th1, Th2, Th17, and Treg cells.21 A high abundance of naive CD4 T cells may indicate strong immunoregulatory potential. In ALS, a higher proportion of naive CD4 T cells may be associated with longer survival.22 There are currently no studies on CCL23 and CCR8 in ALS. Our research indicated that CCL23 may exert a protective effect against ALS, potentially through its chemotactic action on resting T cells rather than activated T cells, ultimately mitigating inflammatory responses.23 Previous studies have similarly identified a significant increase in CXCR4 in the peripheral blood of ALS patients.24 Furthermore, treatment with CXCR4 antagonists has been shown to improve pathology and prolong survival in ALS mouse models.25 In summary, differences exist in the expression of chemokines and their receptors in the peripheral blood of ALS patients, and the causes and implications of these differences require further investigation.
This study classified ALS patients into either the A1/A2 or B1/B2/B3 chemotactic subtypes. Patients in group A1 had a later age of onset. The biological functions of group A1 patients are associated with protein synthesis, metabolism, and transport. Their molecular functions are related to the Rho signaling pathway, which suggests abnormal GTPase function. Patients in23 group A2 had higher Treg abundance in their peripheral blood, and their biological functions were predominantly immune-related, indicating robust immune regulatory capacity. Similar to group A1, group B1 patients exhibited enhanced protein synthesis, metabolism, and transport capabilities associated with the Rho signaling pathway. Additionally, group B1 patients are associated with mitochondrial autophagy and the Parkin signaling pathway. GO and KEGG analyses revealed that group B2 patients were enriched for IL-1β, Toll-like receptors (TLRs), and the Ras pathway. TLRs are receptors for IL-1β, and Ras is downstream of TLRs, which is associated with inflammatory responses.26,27 In ALS, a high level of IL-1β is considered an unfavorable factor because it increases inflammation in the ALS microenvironment and accelerates disease progression.28 Additionally, elevated IL-1β levels have been observed in the peripheral blood of ALS patients.29 Thus, the peripheral and central inflammatory levels of patients in group B2 may be elevated. Immunosuppressants may be more effective for this group. Patients in group B3 exhibited earlier age of onset. Our preliminary findings indicate that younger-onset ALS patients tend to progress more slowly and have a better prognosis.30 Furthermore, patients in group B3 exhibited upregulation of the Wnt signaling pathway activity, which also serves as a self-protective signal for degenerating neurons.31 In summary, the precise classification of ALS patients based on chemokines and their receptors is feasible and may provide insight into therapeutic approaches.
Based on the results of the univariate Cox regression analysis, we constructed ALS prognostic models using eight algorithms. Each algorithm could distinguish between high-risk and low-risk groups. Furthermore, time-dependent ROC analysis accurately predicted survival at the five-year mark after diagnosis in ALS patients. However, it did not effectively distinguish patient survival outcomes during the first and the third years. This may be because ALS patients typically have a relatively long time after diagnosis, though by the fifth year, a significant number of patients have already passed away. When the model was validated using an external test set, Lasso Cox, SuperPC, Survivalsvm, and Xgboost successfully distinguished between the high-risk and low-risk groups. However, due to the small sample size, the differences were not statistically significant. Coxboost, GBM, RSF, and PlsRcox are derived from tree-based models, which are low interpretability. Consequently, they struggle to effectively distinguish high-risk patients when sample sizes are small. In summary, this study successfully developed prognostic models for ALS patients.
Conclusion
In this study, we identified heterogeneity in the proportions of peripheral blood immune cells among ALS patients. ALS could be subtyped based on the expression levels of CCRs. Finally, our study successfully established a prognostic model for ALS based on the clinical characteristics and expression levels of CCRs.
Abbreviations
ALS, amyotrophic lateral sclerosis; CCRs, chemokine and chemokine receptors; Tregs, regulatory T cells; DEGs, differentially expressed genes; CCP, consensus cluster plus; GBM, gradient boosting machine; RSF, Random Survival Forests; ROC, receiver operating characteristic; AUC, area under curve; CI, Confidence Interval; GO, gene ontology; KEGG, Kyoto Encyclopedia of Genes and Genomes; GSEA, gene set enrichment analysis; GSVA, gene set variation analysis; NK, natural killer; CNS, central nervous system; TLR, Toll-like receptors.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by Ethic Committee for clinical research and animal trials of the First Affiliated Hospital, Sun Yat-sen University ([2021]260). This study has obtained informed consent from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the National Natural Science Foundation of China (82271448), Guangdong Provincial Clinical Research Center for Neurological Diseases (2020B1111170002), Guangdong Province International Cooperation Base for Early Intervention and Functional Rehabilitation of Neurological Diseases (2020A0505020004), Guangzhou Major Difficult and Rare Diseases Project (2024MDRD02), Guangdong Provincial Engineering Center for Major Neurological Disease Treatment, Guangdong Provincial Translational Medicine Innovation Platform for Diagnosis and Treatment of Major Neurological Disease, Guangzhou Clinical Research and Translational Center for Major Neurological Diseases.
Disclosure
All authors declare that they have no conflict of interest.
References
1. Xu L, Chen L, Wang S, et al. Incidence and prevalence of amyotrophic lateral sclerosis in urban China: a national population-based study. J Neurol Neurosurg Psychiatry. 2020;91(5):520–15. doi:10.1136/jnnp-2019-322317
2. Goutman SA, Hardiman O, Al-Chalabi A, et al. Recent advances in the diagnosis and prognosis of amyotrophic lateral sclerosis. Lancet Neurol. 2022;21(5):480–493. doi:10.1016/S1474-4422(21)00465-8
3. Feldman EL, Goutman SA, Petri S, et al. Amyotrophic lateral sclerosis. Lancet. 2022;400(10360):1363–1380. doi:10.1016/S0140-6736(22)01272-7
4. Bede P, Lope J. Biomarker development in amyotrophic lateral sclerosis: challenges and viable strategies. Eur J Neurol. 2022;29(7):1867–1868. doi:10.1111/ene.15372
5. Murdock BJ, Zhou T, Kashlan SR, Little RJ, Goutman SA, Feldman EL. Correlation of Peripheral Immunity With Rapid Amyotrophic Lateral Sclerosis Progression. JAMA Neurol. 2017;74(12):1446–1454. doi:10.1001/jamaneurol.2017.2255
6. Beers DR, Henkel JS, Zhao W, Wang J, Appel SH. CD4+ T cells support glial neuroprotection, slow disease progression, and modify glial morphology in an animal model of inherited ALS. Proc Natl Acad Sci U S A. 2008;105(40):15558–15563. doi:10.1073/pnas.0807419105
7. Beers DR, Henkel JS, Zhao W, et al. Endogenous regulatory T lymphocytes ameliorate amyotrophic lateral sclerosis in mice and correlate with disease progression in patients with amyotrophic lateral sclerosis. Brain. 2011;134(Pt 5):1293–1314. doi:10.1093/brain/awr074
8. Xin J, Wainwright DA, Mesnard NA, Serpe CJ, Sanders VM, Jones KJ. IL-10 within the CNS is necessary for CD4+ T cells to mediate neuroprotection. Brain Behav Immun. 2011;25(5):820–829. doi:10.1016/j.bbi.2010.08.004
9. Jin M, Günther R, Akgün K, Hermann A, Ziemssen T. Peripheral proinflammatory Th1/Th17 immune cell shift is linked to disease severity in amyotrophic lateral sclerosis. Sci Rep. 2020;10(1):5941. doi:10.1038/s41598-020-62756-8
10. Coque E, Salsac C, Espinosa-Carrasco G, et al. Cytotoxic CD8+ T lymphocytes expressing ALS-causing SOD1 mutant selectively trigger death of spinal motoneurons. Proc Natl Acad Sci U S A. 2019;116(6):2312–2317.
11. Garofalo S, Cocozza G, Porzia A, et al. Natural killer cells modulate motor neuron-immune cell cross talk in models of Amyotrophic Lateral Sclerosis. Nat Commun. 2020;11(1):1773. doi:10.1038/s41467-020-15644-8
12. Murdock BJ, Goutman SA, Boss J, Kim S, Feldman EL. Amyotrophic Lateral Sclerosis Survival Associates With Neutrophils in a Sex-specific Manner. Neurol Neuroimmunol Neuroinflamm. 2021;8(2). doi:10.1212/NXI.0000000000000953
13. Hughes CE, Nibbs RJB. A guide to chemokines and their receptors. FEBS J. 2018;285(16):2944–2971. doi:10.1111/febs.14466
14. Liao Y, Cai H, Luo F, et al. Three nervous system-specific expressed genes are potential biomarkers for the diagnosis of sporadic amyotrophic lateral sclerosis through a bioinformatic analysis. BMC Med Genomics. 2023;16(1):15. doi:10.1186/s12920-023-01441-x
15. Al-Chalabi A, Hardiman O. The epidemiology of ALS: a conspiracy of genes, environment and time. Nat Rev Neurol. 2013;9(11):617–628. doi:10.1038/nrneurol.2013.203
16. Xu X, Shen D, Gao Y, et al. A perspective on therapies for amyotrophic lateral sclerosis: can disease progression be curbed? Transl Neurodegener. 2021;10(1):29. doi:10.1186/s40035-021-00250-5
17. Shellikeri S, Keith J, Black SE, Zinman L, Yunusova Y. Neuropathology of Speech Network Distinguishes Bulbar From Nonbulbar Amyotrophic Lateral Sclerosis. J Neuropathol Exp Neurol. 2020;79(3):284–295. doi:10.1093/jnen/nlz130
18. Zhao W, Beers DR, Thonhoff JR, et al. Immunosuppressive Functions of M2 Macrophages Derived from iPSCs of Patients with ALS and Healthy Controls. iScience. 2020;23(6):101192. doi:10.1016/j.isci.2020.101192
19. Nógrádi B, Molnár K, Kristóf R, et al. The CCL2-CCR2 axis drives neuromuscular denervation in amyotrophic lateral sclerosis. Nat Commun. 2025;16(1):7053. doi:10.1038/s41467-025-62351-3
20. Zhang J, Liu Y, Liu X, et al. Dynamic changes of CX3CL1/CX3CR1 axis during microglial activation and motor neuron loss in the spinal cord of ALS mouse model. Transl Neurodegener. 2018;7(1):35. doi:10.1186/s40035-018-0138-4
21. Cardenas MA, Kissick HT. Stem-like cells at the center of CD4 T cell differentiation. Trends Cell Biol. 2025. doi:10.1016/j.tcb.2025.06.004
22. Li C, Zhu Y, Chen W, et al. Circulating NAD+ Metabolism-Derived Genes Unveils Prognostic and Peripheral Immune Infiltration in Amyotrophic Lateral Sclerosis. Front Cell Dev Biol. 2022;10:831273. doi:10.3389/fcell.2022.831273
23. Korbecki J, Kojder K, Simińska D, et al. CC Chemokines in a Tumor: a Review of Pro-Cancer and Anti-Cancer Properties of the Ligands of Receptors CCR1, CCR2, CCR3, and CCR4. Int J Mol Sci. 2020;21(21):1.
24. Perner C, Perner F, Stubendorff B, et al. Dysregulation of chemokine receptor expression and function in leukocytes from ALS patients. J Neuroinflammation. 2018;15(1):99. doi:10.1186/s12974-018-1135-3
25. Rabinovich-Nikitin I, Ezra A, Barbiro B, Rabinovich-Toidman P, Solomon B. Chronic administration of AMD3100 increases survival and alleviates pathology in SOD1(G93A) mice model of ALS. J Neuroinflammation. 2016;13(1):123. doi:10.1186/s12974-016-0587-6
26. Tang S, Chen T, Yu Z, et al. RasGRP3 limits Toll-like receptor-triggered inflammatory response in macrophages by activating Rap1 small GTPase. Nat Commun. 2014;5(1):4657. doi:10.1038/ncomms5657
27. Hurtado-Navarro L, Cuenca-Zamora EJ, Zamora L, et al. NLRP3 inflammasome activation and symptom burden in KRAS-mutated CMML patients is reverted by IL-1 blocking therapy. Cell Rep Med. 2023;4(12):101329. doi:10.1016/j.xcrm.2023.101329
28. Meissner F, Molawi K, Zychlinsky A. Mutant superoxide dismutase 1-induced IL-1beta accelerates ALS pathogenesis. Proc Natl Acad Sci U S A. 2010;107(29):13046–13050. doi:10.1073/pnas.1002396107
29. Lu C-H, Allen K, Oei F, et al. Systemic inflammatory response and neuromuscular involvement in amyotrophic lateral sclerosis. Neurol Neuroimmunol Neuroinflamm. 2016;3(4):e244. doi:10.1212/NXI.0000000000000244
30. Huang S, Zheng M, Lin J, et al. Natural history and remarkable psychiatric state of late-onset amyotrophic lateral sclerosis in China. Acta Neurol Scand. 2022;146(1):24–33. doi:10.1111/ane.13598
31. Li D, Wei Y, Yang R, et al. An unrecognized mechanism of self-protection in degenerating neurons mediated by astrocytic YAP through Wnts/β-catenin/EAAT2 signaling in C9orf72-poly-GA mice. Theranostics. 2025;15(16):8176–8201. doi:10.7150/thno.113599
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.