Back to Journals » Cancer Management and Research » Volume 14
Hypoparathyroidism Risk After Total Endoscopic Thyroidectomy for Papillary Thyroid Cancer: A Comparison of the Transoral Vestibular and Breast Approaches
Authors Xu W, Teng C, Ding G ![]() , Zhao N
, Zhao N
Received 28 June 2022
Accepted for publication 9 August 2022
Published 15 August 2022 Volume 2022:14 Pages 2485—2492
DOI https://doi.org/10.2147/CMAR.S380024
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Wei Xu, Changsheng Teng, Guoqian Ding, Ning Zhao
Department of General Surgery, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Ning Zhao, Email [email protected]
Background: This study aimed to compare the risk of hypoparathyroidism between the transoral vestibular approach (TOVA) and the breast approach (BA) in patients undergoing total endoscopic thyroidectomy (TET) for papillary thyroid carcinoma (PTC).
Methods: The medical records of 121 PTC patients (all women) who underwent total TET from January 2015 to January 2021 were retrospectively analyzed. Patients were grouped according to surgical approach (BA or TOVA). Clinical status and concentrations of parathyroid hormone (PTH) and calcium were monitored in the perioperative period and 1, 6, and 12 months after surgery.
Results: The BA and TOVA groups comprised 101 and 20 patients, respectively. Clinicopathologic and characteristics and surgical data were comparable between the groups. Incidence of transient hypoparathyroidism was significantly lower in the TOVA group than the BA group (10% vs 63.4%; p < 0.01). Incidence of permanent hypoparathyroidism was comparable (5% vs 6.9%). Two days after TET, mean PTH concentration was significantly higher and incidence of abnormal PTH was significantly lower in the TOVA group. The incidence of abnormal calcium concentration 2 days after surgery was significantly lower in the TOVA group. One month after surgery, the mean calcium concentration was significantly higher in the TOVA group. Univariate and multivariate Cox regression analysis suggested that patients who underwent TOVA had a lower risk of transient hypoparathyroidism (hazard ratio 0.05, 95% confidence interval, 0.01– 0.23; p< 0.01). No clinicopathological factors examined were significantly associated with permanent hypoparathyroidism.
Conclusion: In patients undergoing TET for PTC, the incidence of transient hypoparathyroidism may be lower with the TOVA than the BA. Surgeons should be aware of the relatively high risk of transient hypoparathyroidism when performing the BA.
Keywords: hypoparathyroidism, endoscopic, thyroidectomy, papillary thyroid carcinoma, parathyroid hormone, surgery
Introduction
Papillary thyroid carcinoma (PTC) is common and accounts for approximately 90% of thyroid cancers and 1% of systemic malignant tumors in China.1 Total endoscopic thyroidectomy (TET) has a satisfactory cosmetic outcome and can be performed for removal of early benign lesions and PTC. The incision for TET via the breast approach (BA) is made at the junction of the areola and skin. As a result, the incision is well-concealed and can heal with little tension. Moreover, this area is not prone to hypertrophic scarring. The transoral vestibular approach (TOVA) has even better cosmetic results and is another option for surgeons and PTC patients.
Hypoparathyroidism is common after total thyroidectomy and almost always transient. Reported incidence rates of transient hypoparathyroidism range from 18% to 46%. Rates of permanent hypoparathyroidism range between 0% and 3%.2 The incidence of complications, including hypoparathyroidism, is similar between TET and open thyroidectomy.3,4 However, the BA and TOVA are different TET approaches and have different observation angles. The TOVA can provide excellent surgical exposure for PTC resection and allows direct access to both sides of the central neck with limited tissue dissection. We believe that the TOVA is superior to the BA in terms of parathyroid exposure and preservation and hypothesized that the TOVA is associated with lower risk of hypoparathyroidism. This study of patients undergoing TET for PTC was conducted to test our hypothesis.
Methods
Patients
After institutional review board approval, we retrospectively reviewed the medical records of patients with PTC who underwent TET from January 2015 to January 2021 in the Department of General Surgery in Beijing Friendship Hospital. In our institution, the records of thyroid cancer patients are maintained in a prospectively collected database. Criteria for inclusion in the study were as follows: 1) age ≥14 years, 2) PTC was diagnosed pathologically via examination of fine needle aspiration or surgical specimens, and 3) TET was performed as first-line treatment. We excluded patients with multiple primary malignancies, previous neck surgery; abnormal preoperative serum parathyroid hormone (PTH) or calcium concentration, and chronic renal failure. Those with incomplete clinicopathological data were also excluded. Patients were informed of the study content in both written and oral forms before the operation and signed informed consents. Patients were assigned to receive either the TOVA or BA according to patients’ preference or choices. This study was approved by the ethics committee and institutional review board of Beijing Friendship Hospital affiliated with Capital Medical University (number, 2021-P2-246-01) and written informed consent was signed by all patients. This study complied with the Declaration of Helsinki.
The following clinical and pathological data were recorded: patient age and sex; tumor number, size, location, and histopathology; surgical procedure; intraoperative neuromonitoring (IONM) findings; number of dissected lymph nodes; parathyroid status; parathyroid autotransplantation; recurrent laryngeal nerve invasion, vascular invasion, and background thyroid disease such as Hashimoto thyroiditis or nodular goiter.
Surgical Procedure
The BA and the TOVA were performed as previously described.5,6 TET was performed using IONM of the recurrent laryngeal nerve7 with the patient under general anesthesia in a supine position. Central lymph nodes, including the pre-laryngeal, pre-tracheal, and paratracheal nodes, were routinely dissected in all patients. The parathyroid gland was also explored in all. Autotransplantation was considered in patients with an ischemic or accidentally resected parathyroid.8 All patients received total thyroidectomy, and the methods of incision selection and establishing operation space were as follows.
BA
Three laparoscopic ports were inserted in double areola of 0.5cm, 0.5cm and 1cm, respectively. Approximately 100mL of swelling fluid was injected from the 1cm right areola incision, and then the subcutaneous tunnel constructed by blunt separation, and the flap was separated to the sternal notch. A 12mm trocar was placed and inflated with CO2 (8mmHg pressure). Under the guidance of a standard 10mm 30° laparoscope, the puncture device was inserted into the areola incision on both sides, the subcutaneous space was enlarged, and the platysma muscle was separated above the surgical field, up to the upper corner of thyroid cartilage, and on both sides to the middle part of the sternocleidomastoid muscles. The white line of the neck was cut longitudinally, the retractor was placed and the anterior cervical muscle was pulled to the outside to expose the thyroid.
TOVA
A transverse incision (2cm) was made in the middle of the oral vestibule and above the frenum of the lower lip. The submucosa was separated to the surface of the mandible, and the soft tissue was separated along the periosteum to the point where it crosses the mandible. Transverse incisions (0.5cm) were made at the oral mucosa 1 cm below the squabbles on both sides. Approximately 30mL of swelling fluid was injected into the subcutaneous tissue of the anterior cervical region in the direction of the three incisions. From the median incision, the subcutaneous space of the anterior cervical region was separated with a separating rod; after placement of a 12mm trocar it was inflated with CO2. With the guidance of a laparoscope, a 5mm trocar was inserted at each incision and the puncture direction was located outside the mental foramen. The platysma muscle was separated to the upper part of the surgical field, and the gap was gradually expanded to the superior sternal fossa on both sides to the middle of sternocleidomastoid muscle. The white line of the neck was cut longitudinally, the retractor was placed and the anterior cervical muscle was pulled to the outside to expose the thyroid.
Hypoparathyroidism Definitions and Follow-Up
Calcitriol (0.25 µg) and calcium carbonate (600–1200 mg) were administered daily to all patients after TET. Serum calcium was monitored daily. Those with serum calcium concentration <2 mmol/L or symptoms of hypocalcemia received intravenous calcium gluconate as appropriate (1–2 grams per day). Serum PTH concentration was measured 2 days after surgery. After discharge, patients were followed up 1, 6, and 12 months after surgery to evaluate symptoms and laboratory findings. Calcitriol and calcium dosages were adjusted accordingly. In our institution, normal serum PTH concentration is defined as 11 to 62 pg/mL; for serum calcium, normal concentration is defined as 2.11 to 2.52 mmol/L.
Hypoparathyroidism was defined by the presence of at least one of the following factors:9 1) serum PTH concentration <11 pg/mL, 2) normal PTH concentration with calcium concentration <2 mmol/L, and 3) symptoms of paralysis or seizures. Transient hypoparathyroidism was defined as hypoparathyroidism that recovered within 6 months. Permanent hypoparathyroidism was defined as hypoparathyroidism that persisted >6 months after surgery. Recovery of hypoparathyroidism was defined as the absence of hypoparathyroidism as defined above.
Statistical Analysis
Statistical analyses were performed using SPSS software version 19.0 (IBM Corp., Armonk, NY, USA). Continuous data are expressed as means with standard deviation. Categorical data are expressed as numbers with percentage. Patients were grouped according to surgical approach (BA or TOVA). Clinicopathological factors were compared between groups using Fisher’s exact test or Pearson’s χ2 test as appropriate. Survival was analyzed using the Kaplan–Meier method. Cox regression analysis was performed to estimate hazard ratios and 95% confidence intervals for potential risk factors for hypoparathyroidism. P<0.05 was considered significant.
Results
Patients
In total, 121 patients met inclusion criteria. All patients were women. The BA and TOVA groups comprised 101 and 20 patients, respectively. Mean age was 38.64 ± 8.32 years and 40.85 ± 8.33 years, respectively. As shown in Table 1, clinicopathologic characteristics and surgical data, including tumor size, number of tumors (single vs multiple) and background thyroid disease, were comparable between the groups.
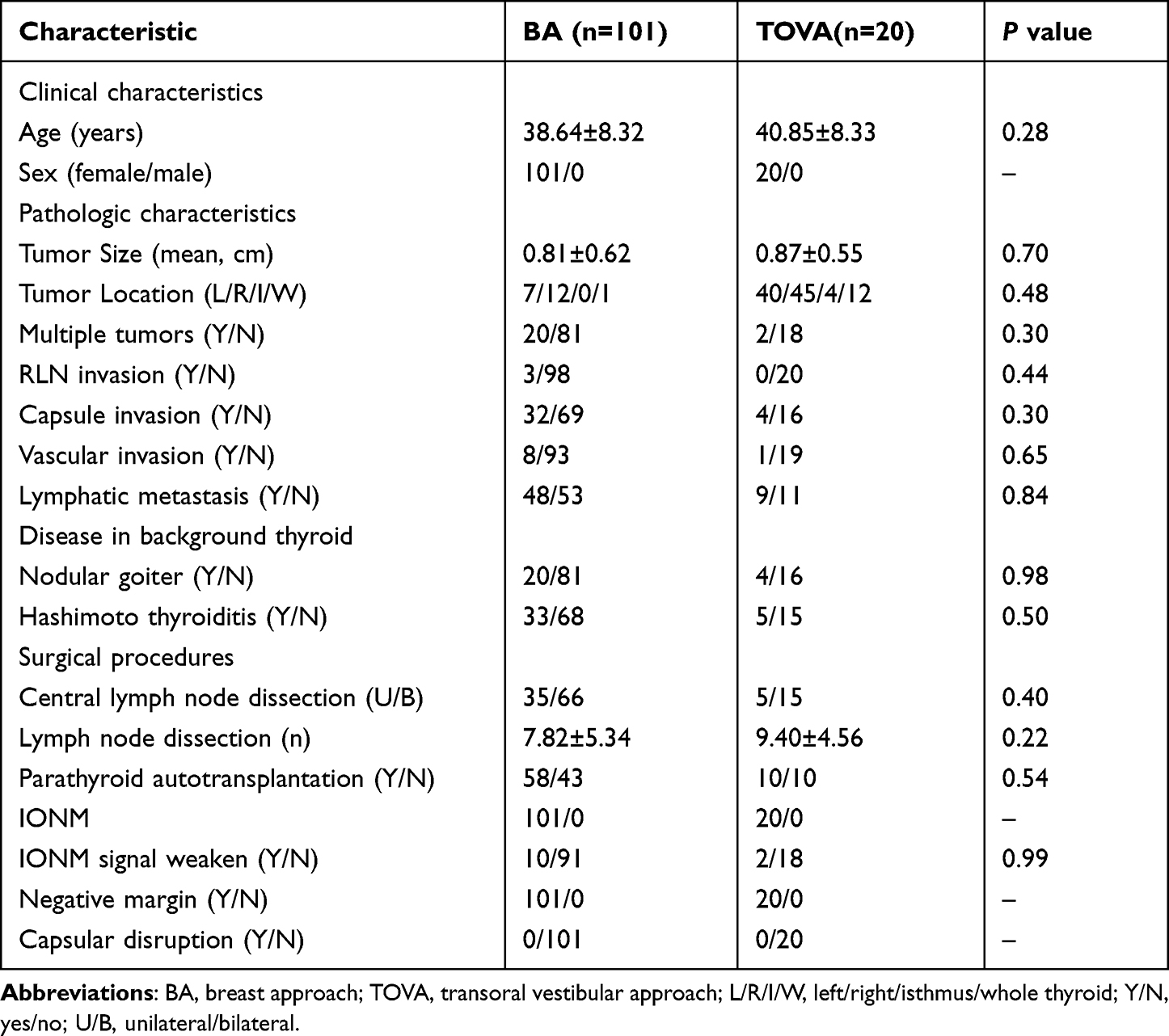 |
Table 1 Clinicopathologic Characteristics and Surgical Data According to Group |
Surgical Procedure
Bilateral central lymph node dissection was performed in 66 BA group patients and 15 TOVA group patients (65.3% vs 75.0%; p = 0.40). The number of dissected lymph nodes in the BA and TOVA groups was 7.82 ± 5.34 and 9.40 ± 4.56, respectively (p = 0.22). Autotransplantation was performed in 58 BA group patients and 10 TOVA group patients (57.4% vs 50.0%; p = 0.54). IONM signal weakening was observed in 10 BA group patients and 2 TOVA group patients (9.9% vs 10%; p = 0.99). Pathologic tumor margins were negative in all patients in each group. No tumor showed evidence of thyroid capsule disruption in either group (Table 1).
Hypoparathyroidism After TET
The incidence of transient hypoparathyroidism was significantly lower in the TOVA group than the BA group (10% vs 63.4%; p<0.01); however, the incidence of persistent hypoparathyroidism was comparable (5% vs 6.9%; p = 0.75; Table 2).
 |
Table 2 Hypoparathyroidism Incidence and Concentrations of Parathyroid Hormone and Calcium Over Time According to Group |
Two days after surgery, mean PTH concentration was significantly higher and incidence of abnormal PTH concentration was significantly lower in the TOVA group. Mean PTH concentration and incidence of abnormal PTH concentration did not significantly differ between the groups 1, 6, and 12 months after surgery.
The incidence of abnormal calcium concentration 2 days after surgery was significantly lower in the TOVA group. One month after surgery, the mean calcium concentration was significantly higher in the TOVA group. Otherwise, these two variables did not significantly differ between groups at the other follow-up time points (Table 2).
Univariate and multivariate Cox regression analysis suggested that patients who underwent TOVA had a lower risk of transient hypoparathyroidism (hazard ratio 0.05, 95% confidence interval, 0.01–0.23; p<0.01). No clinicopathological factors examined were significantly associated with permanent hypoparathyroidism (Table 3).
 |
Table 3 Univariate and Multivariate Analyses of Factors Associated with Transient and Persistent Hypoparathyroidism |
Discussion
In this study, more than half of patients undergoing TET for PTC experienced postoperative hypoparathyroidism and most cases were transient. Compared to the BA, the incidence of transient hypoparathyroidism was lower in patients who underwent the TOVA. Surgeons should be aware of the relatively high risk of transient hypoparathyroidism associated with the BA. To the best of our knowledge, our study is the first to compare incidence of hypoparathyroidism between different TET approaches in patients with DTC.
Based on rates reported in previous studies, the incidence of surgical hypoparathyroidism appears to be comparable between TET and open thyroidectomy. In a study of TET using the TOVA, Anuwong et al reported a 10.9% incidence.6 In another TOVA study, Lira et al reported transient and persistent hypocalcemia rates of 4.0% and 0.8%, respectively;3 yet another noted a 14.1% incidence of transient hypoparathyroidism.10 A meta-analysis of endoscopic and open thyroidectomy in PTC patients showed that rates of transient hypocalcemia after endoscopic resection ranged between 0.3% and 49%; those for permanent hypocalcemia ranged from 0% to 13%.11
The overall incidence of surgical hypoparathyroidism observed in our study (54.5%) was higher than previously reported rates. However, patients in the other studies predominantly underwent unilateral thyroidectomy or resection of benign thyroid lesions. Extensive neck dissection and bilateral neck exploration are independent risk factors for hypoparathyroidism.8 Many of our patients underwent bilateral dissection and all underwent parathyroid exploration; therefore, they had a higher risk of experiencing surgical hypoparathyroidism. Furthermore, the definition of hypoparathyroidism varied between studies and was often based on the presence of clinical symptoms. Moreover, postoperative monitoring and treatment protocols differed between studies, as did the degree of symptom relief after postoperative treatment.3–6,10,11 We believe that diagnosis of hypoparathyroidism based only on symptoms or need for treatment causes an underestimation of the real incidence. Therefore, we suggest routine monitoring of serum calcium and PTH concentrations to diagnose postoperative hypoparathyroidism and guide treatment.
Surgeon experience and the surgical approach used may affect the incidence of surgical hypoparathyroidism.11 Direct injury, devascularization, or inadvertent excision of the parathyroid glands can cause surgical hypoparathyroidism. These may all occur during lymph node dissection or parathyroid exploration during thyroidectomy for PTC,12,13 even with careful technique. Lymph nodes can be difficult to distinguish from adipose tissue during dissection and unintentional devascularization or removal of parathyroid glands can occur. To avoid leaving lymph node metastasis behind in patients with suspected PTC and parathyroid glands and/or lymph nodes that are difficult to distinguish, the entire lymph node area can be removed up front; then, the parathyroid glands can be searched for in the surgical specimen. Any confirmed parathyroid tissue can be transplanted into the sternocleidomastoid muscle.
Based on our TET experience, the difficulty of central lymph node dissection with the BA can be attributed to the clavicular head, which obscures the endoscopic view, causing a blind spot. With increased skill and experience, surgeons can avoid leaving metastatic lymph nodes behind. We have found that the lateral and reverse surgical fields of view increase the difficulty of locating and preserving the parathyroid glands. Compared with the BA, the TOVA provides better surgical visualization and a better observation angle to dissect the pretracheal and paratracheal nodes, which allows easier identification of the inferior parathyroid glands. Furthermore, the TOVA provides ideal visualization to dissect the thyroid along its capsule, which aids in preserving the superior parathyroid glands.
Preserving the parathyroid glands and their blood supply is the key to minimize risk of surgical hypoparathyroidism.8 If in situ preservation is not possible, unintentional removal occurs, or glandular blood supply is compromised, autotransplantation should be performed. We have found that in situ preservation is often difficult when resecting a suspected PTC and performing central lymph node dissection. Prompt recognition of devascularized or resected parathyroid glands is important, as autotransplantation can prevent permanent surgical hypoparathyroidism.14 The surgical approach did not affect recognition in our study: autotransplantation was performed in 57.4% of BA cases and 50% of TOVA cases. In addition, autotransplantation was not associated with transient or permanent hypoparathyroidism. Use of rapid PTH detection and nanocarbon technology during TET may assist with parathyroid gland identification.14 Although near-infrared autofluorescence is another potentially useful technique,15 we have not implemented it in our institution.
A less common cause of surgical hypoparathyroidism is secondary hypoparathyroid gland injury caused by postoperative hematoma or local inflammation.9,16 However, Li et al reported that these are rare after endoscopic thyroidectomy and have little impact on surgical hypoparathyroidism.11 Autoimmune thyroid disease such as Hashimoto thyroiditis has been reported as a risk factor for post-thyroidectomy hypoparathyroidism.17 However, in a retrospective study of 1054 thyroidectomy patients, Ritter et al reported that parathyroid tissue on the pathology report was the only independent risk factor for hypoparathyroidism; age, gender, neck dissection, thyroiditis, and malignancy were not.18 In our study of PTC patients, no clinicopathological feature was a risk factor for permanent hypoparathyroidism, which we attribute to the extensive experience of our TET surgical team.
This study has several limitations. First, it was retrospective in design and was conducted in a single center using a prospectively collected database; selection bias may have been introduced. Second, our definition of recovery from hypoparathyroidism may have captured only patients with clinically significant hypoparathyroidism; however, recovery was probably not affected by recall error or variations in calcium therapy. Third, some patients may not have required calcitriol or calcium supplementation to prevent symptoms of hypocalcemia; therefore, our observed incidence of symptomatic transient hypoparathyroidism may not reflect the real rate. A large-scale multicenter prospective study would be required to further investigate.
In conclusion, the surgical approach in patients undergoing TET for PTC may affect the incidence of surgical hypoparathyroidism, which appears to be lower with the TOVA than the BA. Surgeons should be aware of the relatively high risk of transient hypoparathyroidism when performing the BA.
Acknowledgment
We thank Liwen Bianji (Edanz) (https://www.liwenbianji.cn) for editing the language of a draft of this manuscript.
Disclosure
Wei Xu, Changsheng Teng, Guoqian Ding, and Ning Zhao have no conflicts of interest or financial ties to disclose.
References
1. Cao W, Chen H-D, Yu Y-W, Li N, Chen W-Q. Changing profiles of cancer burden worldwide and in China: a secondary analysis of the global cancer statistics 2020. Chin Med J. 2021;134(7):783–791. doi:10.1097/CM9.0000000000001474
2. Lim ST, Jeon YW, Gwak H, Suh YJ. Incidence, risk factors, and clinical implications of delayed hypoparathyroidism on postoperative day two following total thyroidectomy for papillary thyroid carcinoma. Endocr Pract. 2020;26(7):768–776. doi:10.4158/EP-2019-0544
3. Lira RB, De Cicco R, Rangel LG. Transoral endoscopic thyroidectomy vestibular approach: experience from a multicenter national group with 412 patients. Head Neck. 2021;43(11):3468–3475. doi:10.1002/hed.26846
4. Qu Y-Q, Han Y-B, Wang W-J, Zhang X-J, Ma G-H. Clinical analysis of total endoscopic thyroidectomy via breast areola approach in early differentiated thyroid cancer. J BUON. 2021;26:1022–1027.
5. Sasaki A, Nakajima J, Ikeda K, Otsuka K, Koeda K, Wakabayashi G. Endoscopic thyroidectomy by the breast approach: a single institution’s 9-year experience. World J Surg. 2008;32(3):381–385. doi:10.1007/s00268-007-9375-x
6. Anuwong A, Ketwong K, Jitpratoom P, Sasanakietkul T, Duh Q-Y. Safety and outcomes of the transoral endoscopic thyroidectomy vestibular approach. JAMA Surg. 2018;153(1):21–27. doi:10.1001/jamasurg.2017.3366
7. Wojtczak B, Kaliszewski K, Sutkowski K, Głód M, Barczyński M. The learning curve for intraoperative neuromonitoring of the recurrent laryngeal nerve in thyroid surgery. Langenbecks Arch Surg. 2017;402(4):701–708. doi:10.1007/s00423-016-1438-8
8. Kazaure HS, Sosa JA. Surgical Hypoparathyroidism. Endocrinol Metab Clin North Am. 2018;47(4):783–796. doi:10.1016/j.ecl.2018.07.005
9. Dedivitis Rogerio A, Aires Felipe T, Cernea Claudio R. Hypoparathyroidism after thyroidectomy: prevention, assessment and management. Curr Opin Otolaryngol Head Neck Surg. 2017;25(2):142–146. doi:10.1097/MOO.0000000000000346
10. Liu ZD, Li YJ, Wang Y, et al. Comparison of the transoral endoscopic thyroidectomy vestibular approach and open thyroidectomy: a propensity score-matched analysis of surgical outcomes and safety in the treatment of papillary thyroid carcinoma. Surgery. 2021;170(6):1680–1686. doi:10.1016/j.surg.2021.06.032
11. Li YJ, Zhou XD. Comparison between endoscopic thyroidectomy and conventional open thyroidectomy for papillary thyroid microcarcinoma: a meta-analysis. J Cancer Res Ther. 2016;12(2):550–555. doi:10.4103/0973-1482.157353
12. Gambardella C, Patrone R, Di Capua F, et al. The role of prophylactic central compartment lymph node dissection in elderly patients with differentiated thyroid cancer: a multicentric study. BMC Surg. 2019;24(18):110. doi:10.1186/s12893-018-0433-0
13. Gambardella C, Offi C, Patrone R, et al. Calcitonin negative Medullary Thyroid Carcinoma: a challenging diagnosis or a medical dilemma? BMC Endocr Disord. 2019;29(19):45. doi:10.1186/s12902-019-0367-2
14. Godlewska P, Benke M, Stachlewska-Nasfeter E, Gałczyński J, Puła B, Dedecjus M. Risk factors of permanent hypoparathyroidism after total thyroidectomy and central neck dissection for papillary thyroid cancer: a prospective study. Endokrynol Pol. 2020;71(2):126–133. doi:10.5603/EP.a2020.0006
15. Kim DH, Kim SW, Kang P. Near-infrared autofluorescence imaging may reduce temporary hypoparathyroidism in patients undergoing total thyroidectomy and central neck dissection. Thyroid. 2021;31(9):1400–1408. doi:10.1089/thy.2021.0056
16. Marotta V, Sciammarella C, Chiofalo MG, et al. Hashimoto’s thyroiditis predicts outcome in intrathyroidal papillary thyroid cancer. Endocr Relat Cancer. 2017;24(9):485–493. doi:10.1530/ERC-17-0085
17. Orloff Lisa A, Wiseman Sam M, Bernet Victor J, et al. American thyroid association statement on postoperative hypoparathyroidism: diagnosis, prevention, and management in adults. Thyroid. 2018;28(7):830–841. doi:10.1089/thy.2017.0309
18. Ritter K, Elfenbein D, Schneider DF, Chen H, Sippel RS. Hypoparathyroidism after total thyroidectomy: incidence and resolution. J Surg Res. 2015;197(2):348–353. doi:10.1016/j.jss.2015.04.059
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.