Back to Journals » OncoTargets and Therapy » Volume 8
Hyperthermia combined with 5-fluorouracil promoted apoptosis and enhanced thermotolerance in human gastric cancer cell line SGC-7901
Authors Liu T, Ye Y, Zhu A, Yang Z, Fu Y, Wei C, Liu Q, Zhao C, Wang G, Zhang X
Received 2 December 2014
Accepted for publication 16 March 2015
Published 27 May 2015 Volume 2015:8 Pages 1265—1270
DOI https://doi.org/10.2147/OTT.S78514
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jianmin Xu
Tao Liu,* Yan-Wei Ye,* A-li Zhu, Zhen Yang, Yang Fu, Chong-Qing Wei, Qi Liu, Chun-Lin Zhao, Guo-Jun Wang, Xie-Fu Zhang
Department of Gastrointestinal Surgery, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, People’s Republic of China
*These authors contributed equally to this work
Abstract: This study was designed to investigate the proliferation inhibition and apoptosis-promoting effect under hyperthermia and chemotherapy treatment, at cellular level. Human gastric cancer cell line SGC-7901 was cultivated with 5-fluorouracil at different temperatures. Cell proliferation and apoptosis were determined, and expression of Bcl-2 and HSP70 was measured at different treatments. Cell survival rates and inhibition rates in chemotherapy group, thermotherapy group, and thermo-chemotherapy group were drastically lower than the control group (P<0.05). For tumor cells in the thermo-chemotherapy group, survival rates and inhibition rates at three different temperatures were all significantly lower than those in chemotherapy group and thermotherapy group (P<0.05). 5-Fluorouracil induced apoptosis of SGC-7901 cells with a strong temperature dependence, which increased gradually with increase in temperature. At 37°C and 43°C there were significant differences between the thermotherapy group and chemotherapy group and between the thermo-chemotherapy group and thermotherapy group (P<0.01). The expression of Bcl-2 was downregulated and HSP70 was upregulated, with increase in temperature in all groups. Cell apoptosis was not significant at 46°C (P>0.05), which was probably due to thermotolerance caused by HSP70 accumulation. These results suggested that hyperthermia combined with 5-fluorouracil had a synergistic effect in promoting apoptosis and enhancing thermotolerance in gastric cancer cell line SGC-7901.
Keywords: gastric cancer, thermotherapy, 5-fluorouracil, Bcl-2, HSP70, thermotolerance
Introduction
Although the incidence of gastric cancer has decreased during the past years, it is still the fourth most common newly diagnosed cancer worldwide and the second leading cause of cancer-related death.1–3 The principal risk factors in development of gastric cancer are Helicobacter pylori infection, intestinal metaplasia, dysplasia, cigarette smoking, partial gastrectomy, and genetic factors.4 Gastric cancer is one of the most common gastrointestinal cancers in the People’s Republic of China, with characteristics such as high incidence, easy metastasis, and high mortality. The occurrence of gastric cancer is a multistage process, and the system has not been elucidated yet at this moment. Further exploration of the molecular mechanisms of gastric cancer development and the search for more effective clinical treatment has become one of the hotpots in current research.5–7 Thermotherapy is a new cancer treatment which is used following surgical, radiotherapy, chemotherapy, and biological treatments. Thermotherapy induces malignant cell apoptosis and has a synergistic effect with chemotherapy, resulting in improved outcomes and reduced side effects of chemotherapy, particularly in the later stages of malignancy or in tumors resistant to other treatments.8 Over the past decades, a variety of doses of 5-fluorouracil (5-FU) have been developed in clinical trials for the treatment of gastrointestinal tumors. The widely used chemotherapeutic agent, 5-FU, is important for oral cancer treatment. Clinical studies have shown that 5-FU-based chemotherapy and chemoradiotherapy improve the survival of patients with gastric cancer.9,10
The B-cell lymphoma-2 (Bcl-2) family of proteins play a key role in mitochondrial apoptosis as they regulate the permeability of the outer mitochondrial membrane and the release of cytochrome c.11–13 Additionally, the Bcl-2 family modulates the balance between mitochondrial fission and fusion and is thereby linked to mitochondrial physiology.14 Observations in human tumors and studies with genetically modified (transgenic or knockout) mice have shown that tumourigenesis can be driven by gain-of-function mutations in cell death antagonists (Bcl-2 overexpression) or loss-of-function mutations in cell death activators (loss of Bcl-2).
Heat shock proteins (HSPs) are highly conserved proteins whose synthesis is increased by a large variety of stressors, including heat shock.15,16 The 70-kDa HSP family (HSP70) acts as a molecular chaperone, and is involved in the folding of nascent polypeptide chains and translocation of precursor proteins across the membranes of cytoplasmic organelles.17,18 A number of studies have demonstrated that HSP70 is overexpressed in human gastric cancer and may contribute to the development and progression of this cancer.19,20 HSP70 is categorized into constitutive and inducible forms, which contribute to stress tolerance by increasing the chaperone activity in the cytoplasm. The inducible form of HSP70 has been proposed as a predictor or indicator for thermotolerance at either the cell or animal level.21,22
Materials and methods
Cell culture
The human gastric cancer SGC-7901 cell line (Molecular Biology Laboratory, Affiliated Tumor Hospital of Zhongshan Medical University, Guangdong, People’s Republic of China) was inoculated in the sterile culture flask with high-glucose Dulbecco’s Modified Eagle’s Medium (DMEM) (Thermo Fisher Scientific, Waltham, MA, USA) containing 10% fetal bovine serum (Thermo Fisher Scientific), 100 μg/mL penicillin (Thermo Fisher Scientific), and 100 mg/mL streptomycin (Thermo Fisher Scientific). Then the inoculum was placed in a 5% CO2 incubator (Japan BNA-311), at 37°C and with a relative humidity of 95% for 48 hours to reach the exponential growth phase. Subsequently, the culture was digested with 0.25% trypsin for 3 minutes, and then dissociated by using a plastic pipette to prepare a single-cell suspension at a concentration of 1×105/mL.
Experimental design
According to the research on the effects of 5-FU (Sigma-Aldrich Co., St Louis, MO, USA), the concentrations of which were 10, 50, 100, 500, and 1,000 μg/mL, respectively, on SGC-7901 cell apoptosis by the annexin V/propidium iodide method previously conducted in our laboratory (data unreleased), we selected 5-FU at a concentration of 500 μg/mL for follow-up studies of thermo-chemotherapy.
For each group, SGC-7901 cells were inoculated in 6-well sterile culture plates till they reached the exponential growth phrase. Three wells were used for the treatment and the other three wells were taken as the control group. The original medium was discarded before appropriate treatments were applied. 1) Control group: 2 mL high-glucose DMEM was added into the control wells and then the inoculum was cultured at 37°C for 24 hours. 2) Chemotherapy group: 2 mL high-glucose medium containing 5-FU (500 μg/mL) was added into the chemotherapy group wells, which were then cultured with the inoculum at 37°C for 24 hours. 3) Thermotherapy group: 2 mL high-glucose DMEM was added to the thermotherapy group wells and maintained in an incubator (5% CO2 and 95% relative humidity) at (40±0.2)°C, (43±0.2)°C, and (46±0.2)°C for 1 hour, respectively. Then, the inoculum was added and cultured at 37°C for 23 hours. 4) Thermo-chemotherapy group: 2 mL high-glucose DMEM containing 5-FU (500 μg/mL) was added to the thermo-chemotherapy group wells, immediately placed in an incubator (5% CO2 and 95% relative humidity) at (40±0.2)°C, (43±0.2)°C, and (46±0.2)°C for 1 hour, respectively. Subsequently, the inoculum was added and cultured at 37°C for 23 hours.
Cell survival rate
Cell suspensions of each of the treated cultures was diluted to contain similar number of cells, 0.9 mL of which was extracted and stained with 0.1 mL trypan blue (0.4%). Then, the mixture was observed under an inverted microscope within 3 minutes. Blue cells were those that were dead. The average was calculated from the values obtained from each of the three observations.
|

Cell proliferation
Cellular proliferation inhibition was determined by MTT assay. Tumor cells in the logarithmic growth phase were extracted into complete medium to prepare single-cell suspension, and then inoculated onto 96-well plates with 200 μL (~103) per well to receive therapy. The culture was maintained in an incubator (5% CO2) at 37°C for 48 hours. Subsequently, 20 μL MTT was added into the culture, which was centrifuged at 2,000× g for 5 minutes after cultivation for 4 hours. After removing the nutrient solution, the culture in each well was mixed with 150 μL DMSO (Sigma) and then vibrated in the micro-oscillator for 5 minutes to determine the OD value at 490 nm. The inhibition rate of cell proliferation was calculated as follows:
|

where, OD1 stands for the OD value measured in control group and OD2 for that measured in treated group.
Cell apoptosis
Tumor cells in the logarithmic growth phase were extracted from each treatment group to prepare a single-cell suspension and inoculated in the 50 mL culture flask (2×105). Then the culture was incubated at 37°C. Cells were collected after 48 hours and washed twice with PBS, the sediment of which was conserved with 300 μL DNA dye for 30 minutes at room temperature without light. Cells were stained with propidium iodide and anti-annexin-V antibody (BD Biosciences, San Jose, CA, USA) following the manufacturer’s protocol, and stained cells were detected by flow cytometry.
Western blot
Protein concentrations from isolated SGC-7901 cells were determined. The proteins were separated using sodium dodecyl sulfate-polyacrylamide gel electrophoresis gels (polyacrylamide concentration 100 g/L) and electrophoretically transferred to polyvinylidene difluoride (PVDF) membranes. The PVDF membranes were blocked with 5% skimmed milk at 37°C for 1 hour and probed with the primary antibody: mouse anti-human HSP70 (1:2,000), Bcl-2, or β-actin (1:1,000) monoclonal antibody overnight at 4°C. The labeled antibody was visualized by using horseradish peroxidase-conjugated goat anti-mouse immunoglobulin G (1:5,000) and enhanced chemiluminescence. The blots were washed with 1× Tris-buffered saline and Tween buffer for 10 minutes, three times between each step. The density of the targeted bands was quantified using the Quantity One 4.6.2 Imaging Analysis System (Bio-Rad Laboratories Inc., Hercules, CA, USA).
Statistical analysis
The experiments were all conducted in triplicate. Results were analyzed using analysis of variance (ANOVA; SPSS Inc. 13.0, Chicago, IL, USA) and indicated as means ± SD. P<0.05 represents for differences with statistical significance.
Results
Cell survival was reduced under hyperthermia and 5-FU treatment
Tumor cell survival rates were 100% before the treatment. Results showed that cell survival rates in the chemotherapy group, the thermotherapy group, and the thermo-chemotherapy group were drastically lower than the control group (P<0.05) (Table 1). For tumor cells in the thermo-chemotherapy group, survival rates at three different temperatures were all significantly lower than those in the chemotherapy and thermotherapy groups (P<0.05) (Table 1). In the thermo-chemotherapy group, survival rates at 43°C and 46°C were significantly lower than the control group (40°C) (P<0.01), and there was significant difference between 43°C and 46°C (P<0.05) (Figure 1A).
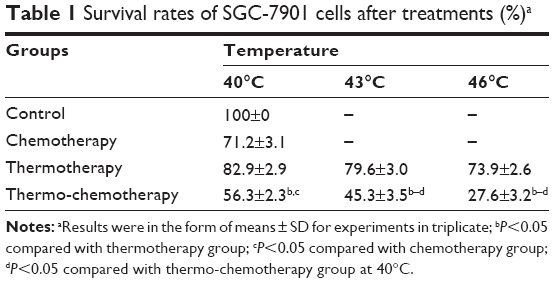 | Table 1 Survival rates of SGC-7901 cells after treatments (%)a |
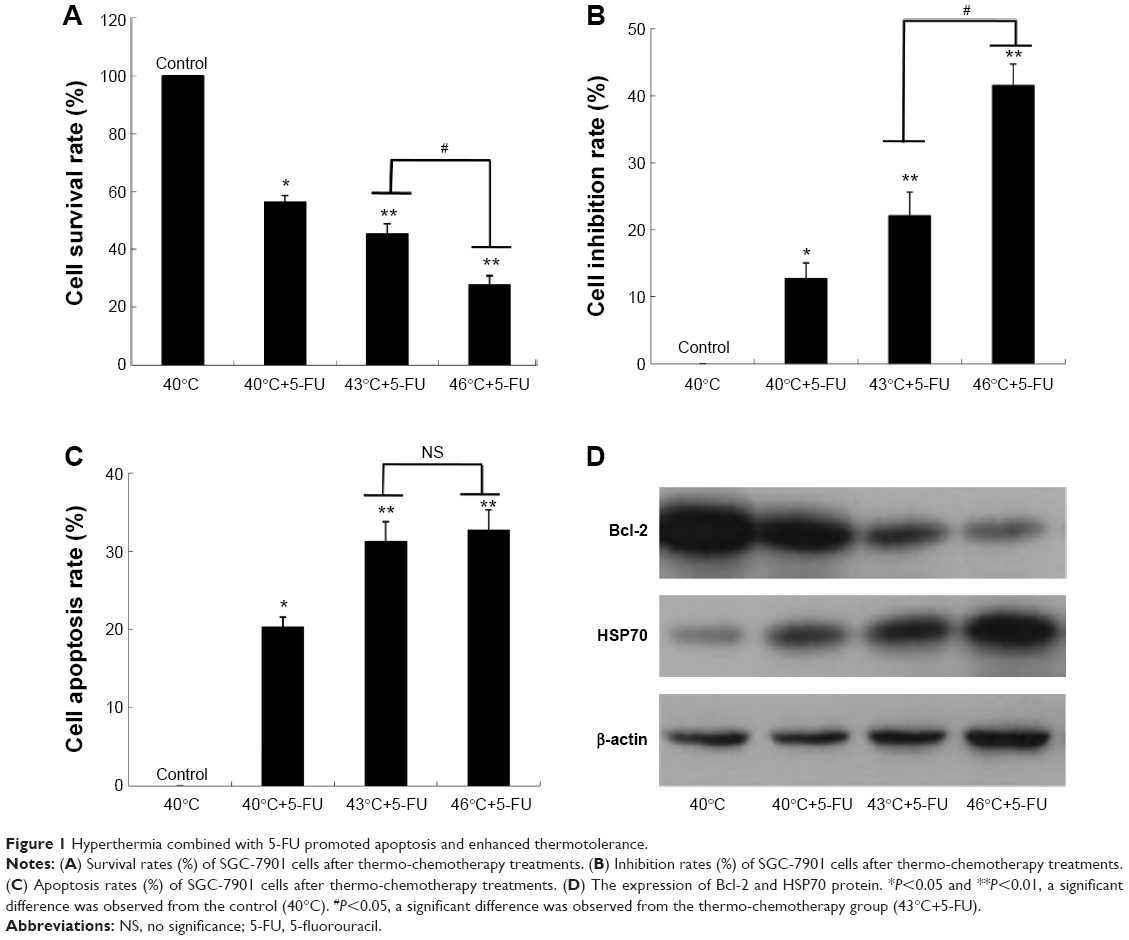 | Figure 1 Hyperthermia combined with 5-FU promoted apoptosis and enhanced thermotolerance. |
Hyperthermia and 5-FU inhibited cell proliferation
Inhibition of SGC-7901 cell proliferation in the thermo-chemotherapy group enhanced with increase in temperature, and was significantly lower than those of tumor cells in the thermotherapy and chemotherapy groups (P<0.05) (Table 2). Cell inhibition of SGC-7901 cells in the thermo-chemotherapy group at 43°C and 46°C was statistically different from the control group (40°C) (P<0.01), and the difference between cell inhibition rates at 43°C and 46°C was significant (P<0.05) (Figure 1B).
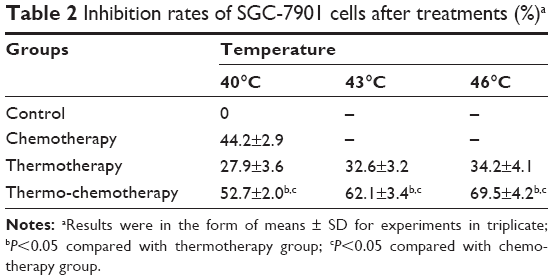 | Table 2 Inhibition rates of SGC-7901 cells after treatments (%)a |
Hyperthermia and 5-FU enhanced cell apoptosis
It is indicated that SGC-7901 cell apoptosis after treatment were all extremely higher than those in the control group (P<0.05). Cell apoptosis rates of the thermo-chemotherapy group were significantly increased in comparison to those of the thermotherapy and chemotherapy groups (P<0.05), which was in positive correlation with temperatures (Table 3). In the thermo-chemotherapy group, cell apoptosis rates at 43°C and 46°C were significantly lower than the control group (40°C) (P<0.01); however, there was no significant difference between 43°C and 46°C (P>0.05) (Figure 1C).
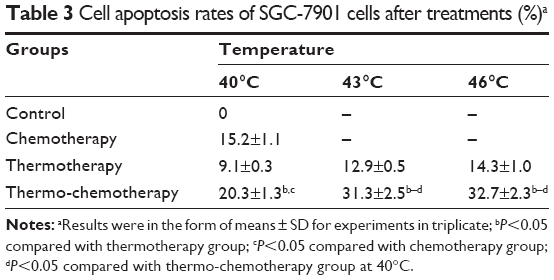 | Table 3 Cell apoptosis rates of SGC-7901 cells after treatments (%)a |
Effect of 5-FU and temperature on the expression of Bcl-2 and HSP70
Bcl-2 is a critical molecule for the regulation of apoptosis. The expression of Bcl-2 protein in SGC-7901 cells after treatment was significantly different from those in the control group, which decreased with increase in temperature (Figure 1D). Western blot analysis revealed that in comparison to cells incubated at 40°C, HSP70 accumulation increased with increase in temperature (Figure 1D).
Discussion
Combinations of multiple therapeutic approaches are an emerging trend for optimizing clinical disease management.23 It has been reported that hyperthermia is one of the most promising new multidisciplinary approaches for cancer therapy, especially the synergy of combined hyperthermia and chemotherapy.24,25 Synergistic interaction between hyperthermia and 5-FU has been observed in this study. Cell apoptosis rates in the thermotherapy group were higher than those in the control group, which might be due to thermo-denaturation of intracellular proteins and DNA and/or cytoplasmic destruction. Hence, raising the treatment temperature is effective in increasing the therapeutic efficacy. But in mono-thermotherapy, excessively high temperature would damage normal cells in vivo and cause heat-resistance of tumor cells. Consequently, maintaining moderate temperature is necessary to avoid undesirable phenomena during thermo-chemotherapy. Heat kills tumor cells directly. Moreover, it could improve the drug concentration in the cytoplasm of cancer cells due to the permeability change of cell membrane and enhance the chemotherapy effects. Additionally, immune function could be improved due to enhancement of lymphocyte activity. Bcl-2 expression was decreased. High expression of Bcl-2 protein is associated with cell abnormality, which constructs the biological basis of tumor cell resistance against chemotherapy. Bcl-2 protein expression of SGC-7901 cells was downregulated in the thermo-chemotherapy group. The toxic effects of thermo-chemotherapy might be related to the activation of the mitochondrial pathway in the process of cell apoptosis.
Results indicated that thermo-chemotherapy would have a greater effect on tumor cells proliferation than thermotherapy, with statistical significance. Thermo-chemotherapy with 5-FU (500 μg/mL) at 43°C was observed to be appropriate for clinical treatment of gastric cancer. Cell apoptosis at 46°C was not significant compared with 43°C, but it was significantly different compared with the control (40°C) group, which was probably due to thermotolerance caused by HSP70 accumulation at high temperature (Figure 1D). HSP70 is categorized into constitutive and inducible forms, which contribute to stress tolerance by increasing the chaperone activity in the cytoplasm.21,22 It is of great importance for the clinical application of thermo-chemotherapy, which would strengthen drug sensitivity of tumor cells or even resistant tumor cells and reduce drug consumption to alleviate possible clinical side effects.
Disclosure
The authors report no conflicts of interest in this work.
References
Fuchs CS, Tomasek J, Yong CJ, et al. Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): an international, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet. 2014;383(9911):31–39. | ||
Bertuccio P, Chatenoud L, Levi F, et al. Recent patterns in gastric cancer: a global overview. Int J Cancer. 2009;125(3):666–673. | ||
Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64(1):9–29. | ||
Okines A, Verheij M, Allum W, Cunningham D, Cervantes A. Gastric cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010;21(Suppl 5):v50–v54. | ||
Raida M, Schwabe W, Häusler P, et al. Prevalence of a common point mutation in the dihydropyrimidine dehydrogenase (DPD) gene within the 5′-splice donor site of intron 14 in patients with severe 5-fluorouracil (5-FU)-related toxicity compared with controls. Clin Cancer Res. 2001;7(9):2832–2839. | ||
Huehls AM, Wagner JM, Huntoon CJ, et al. Poly(ADP-Ribose) polymerase inhibition synergizes with 5-fluorodeoxyuridine but not 5-fluorouracil in ovarian cancer cells. Cancer Res. 2011;71(14):4944–4954. | ||
Ducreux M, Adenis A, Pignon J-P, et al. Efficacy and safety of bevacizumab-based combination regimens in patients with previously untreated metastatic colorectal cancer: final results from a randomised phase II study of bevacizumab plus 5-fluorouracil, leucovorin plus irinotecan versus bevacizumab plus capecitabine plus irinotecan (FNCLCC ACCORD 13/0503 study). Eur J Cancer. 2013;49(6):1236–1245. | ||
Xiao F, Liu B, Zhu Q-X. c-Jun N-terminal kinase is required for thermotherapy-induced apoptosis in human gastric cancer cells. World J Gastroenterol. 2012;18(48):7348. | ||
Endo F, Nishizuka SS, Kume K, et al. A compensatory role of NF-κB to p53 in response to 5-FU-based chemotherapy for gastric cancer cell lines. PLoS One. 2014;9(2):e90155. | ||
Fuchs C, Tepper J, Niedzwiecki D, et al. Postoperative adjuvant chemoradiation for gastric or gastroesophageal junction (GEJ) adenocarcinoma using epirubicin, cisplatin, and infusional (CI) 5-FU (ECF) before and after CI 5-FU and radiotherapy (CRT) compared with bolus 5-FU/LV before and after CRT: intergroup trial CALGB 80101. J Clin Oncol. 2011;29(15 Suppl):S4003. | ||
Youle RJ, Strasser A. The BCL-2 protein family: opposing activities that mediate cell death. Nat Rev Mol Cell Biol. 2008;9(1):47–59. | ||
Lessene G, Czabotar PE, Colman PM. BCL-2 family antagonists for cancer therapy. Nat Rev Drug Discov. 2008;7(12):989–1000. | ||
Danial NN. BCL-2 family proteins: critical checkpoints of apoptotic cell death. Clin Cancer Res. 2007;13(24):7254–7263. | ||
Martinou JC, Youle RJ. Mitochondria in apoptosis: Bcl-2 family members and mitochondrial dynamics. Dev Cell. 2011;21(1):92–101. | ||
Schlesinger MJ. Heat shock proteins. J Biol Chem. 1990;265(21):12111–12114. | ||
Jego G, Hazoumé A, Seigneuric R, Garrido C. Targeting heat shock proteins in cancer. Cancer Lett. 2013;332(2):275–285. | ||
Lee J, Kim J-H, Biter AB, Sielaff B, Lee S, Tsai FT. Heat shock protein (Hsp) 70 is an activator of the Hsp104 motor. Proc Natl Acad Sci U S A. 2013;110(21):8513–8518. | ||
Hartl FU. Molecular chaperones in cellular protein folding. Nature. 1996;381:571–580. | ||
Isomoto H, Oka M, Yano Y, et al. Expression of heat shock protein (Hsp) 70 and Hsp 40 in gastric cancer. Cancer Lett. 2003;198(2):219–228. | ||
Zhao ZG, Shen WL. Heat shock protein 70 antisense oligonucleotide inhibits cell growth and induces apoptosis in human gastric cancer cell line SGC-7901. World J Gastroenterol. 2005;11(1):73–78. | ||
Gabai VL, Meriin AB, Mosser DD, et al. Hsp70 prevents activation of stress kinases a novel pathway of cellular thermotolerance. J Biol Chem. 1997;272(29):18033–18037. | ||
Li GC, Mak JY. Re-induction of hsp70 synthesis: an assay for thermotolerance. Int J Hyperthermia. 2009;25(4):249–257. | ||
Li TJ, Huang CC, Ruan PW, et al. In vivo anti-cancer efficacy of magnetite nanocrystal-based system using locoregional hyperthermia combined with 5-fluorouracil chemotherapy. Biomaterials. 2013;34(32):7873–7883. | ||
Tang Y, McGoron AJ. Increasing the rate of heating: a potential therapeutic approach for achieving synergistic tumour killing in combined hyperthermia and chemotherapy. Int J Hyperthermia. 2013;29(2):145–155. | ||
Mirnezami R, Mehta A, Chandrakumaran K, et al. Cytoreductive surgery in combination with hyperthermic intraperitoneal chemotherapy improves survival in patients with colorectal peritoneal metastases compared with systemic chemotherapy alone. Br J Cancer. 2014;111(8):1500–1508. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.