Back to Journals » Drug, Healthcare and Patient Safety » Volume 18
Hypersensitivity Reaction to Hyaluronidase After Peribulbar Anesthesia for Cataract Surgery: Two Case Reports
Authors Cheng C, Han Y, Liu X, Yu W, Yang N
Received 4 June 2025
Accepted for publication 3 February 2026
Published 10 February 2026 Volume 2026:18 543301
DOI https://doi.org/10.2147/DHPS.S543301
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Siew Siang Chua
Cheng Cheng,1– 3 Yanfeng Han,1– 3 Xiaoxi Liu,1– 3 Weiwei Yu,1– 3 Nannan Yang1– 3
1Eye Institute of Shandong First Medical University, Qingdao Eye Hospital of Shandong First Medical University, Qingdao, Shandong, People’s Republic of China; 2State Key Laboratory Cultivation Base, Shandong Provincial Key Laboratory of Eye Diseases, Qingdao, Shandong, People’s Republic of China; 3School of Ophthalmology, Shandong First Medical University, Jinan, Shandong, People’s Republic of China
Correspondence: Nannan Yang, Email [email protected]
Background: Hypersensitivity reaction to hyaluronidase, though rare, can occur following regional anesthesia in ophthalmic surgery and may mimic serious conditions such as orbital cellulitis. Prompt recognition is critical to avoid misdiagnosis and unnecessary interventions.
Case Presentation: We report two cases of hypersensitivity reaction following hyaluronidase-augmented peribulbar anesthesia for cataract surgery. Case 1: A 90-year-old female with no prior allergy history developed progressive periorbital edema extending to the ipsilateral face and neck within 7 hours after surgery. Infection and hemorrhage were excluded via ultrasound. The reaction resolved promptly with antihistamines and systemic corticosteroids. Case 2: A 69-year-old female developed progressive bilateral periorbital edema extending to the forehead, accompanied by moderate pain within 7 hours postoperatively. While her C-reactive protein (CRP) level was within normal limits on the day of surgery, it rose significantly to 33.92 mg/L on postoperative day 1. Given this clinical and laboratory progression, an empirical and prophylactic therapeutic protocol was initiated, including a short course of systemic antibiotics alongside intensified anti-inflammatory treatment. All bacterial and fungal cultures returned negative, confirming a non-infectious etiology. Both patients achieved complete resolution of symptoms with uneventful recoveries maintained at both the one-week and one-month postoperative follow-up visits.
Conclusion: These cases illustrate that hyaluronidase hypersensitivity, though uncommon, should be considered in the differential diagnosis of acute postoperative periorbital inflammation. A combination of clinical vigilance, targeted imaging, and judicious use of laboratory tests is key to distinguishing this condition from infectious complications. Early diagnosis and a structured management approach are crucial to ensure patient safety and optimal outcomes.
Keywords: hyaluronidase, hypersensitivity reaction, allergy, peribulbar anesthesia, cataract surgery
Introduction
Hyaluronidase, an enzyme that hydrolyzes hyaluronic acid in the extracellular matrix, plays a pivotal role in enhancing tissue permeability and facilitating the diffusion of injected fluids or medications.1 Clinically, it is widely utilized in various medical fields, including ophthalmology, dermatology, and anesthesiology, to improve drug absorption, reduce tissue edema, and accelerate the resolution of extravasated fluids.2–4 Despite its broad therapeutic applications, hypersensitivity reaction with an estimated incidence of approximately 0.05%~0.1% have been documented in the literature.5,6 These adverse events, ranging from localized erythema to systemic anaphylaxis, underscore the importance of recognizing its potential of hypersensitivity reactions, even in populations without prior exposure history.7–9
Regional blocks remain a cornerstone technique in ocular surgeries, such as cataract extraction and vitreoretinal procedures, due to its efficacy in achieving rapid and profound analgesia.10 To optimize anesthetic dispersion and prolong its duration, hyaluronidase is frequently co-administered with local anesthetics.2 The addition of hyaluronidase enhances tissue penetration, reduces intraoperative discomfort, and minimizes the volume of anesthetic required, thereby lowering the risk of complications such as orbital hemorrhage or mechanical nerve injury.7 Its role in improving surgical outcomes has solidified its routine use in ocular anesthesia protocols.
Although hyaluronidase-associated hypersensitivity reaction in peribulbar or retrobulbar anesthesia are exceedingly rare, their clinical implications can be severe.9 Reported risk factors include prior exposure to hyaluronidase or hypersensitivity to insect venoms, given the common animal-derived (bovine/ovine) source of the enzyme. However, reaction can also occur unpredictably in patients without such history.5 To date, only a handful of cases have been reported globally, highlighting the need for heightened awareness among clinicians.5 In this article, we present two novel cases of acute hypersensitivity reaction following hyaluronidase-augmented peribulbar anesthesia, detailing their clinical manifestations and management strategies. These cases contribute to the growing body of evidence on hyaluronidase-related hypersensitivity reactions and emphasize the necessity for vigilant monitoring and preparedness in clinical settings.
Case 1
A nonagenarian female with a history of left eye phacoemulsification with posterior chamber intraocular lens implantation 22 days prior presented for elective right eye cataract surgery. Significant comorbidities included insulin-dependent type 2 diabetes mellitus, controlled essential hypertension, and stable coronary artery disease, with a documented ophthalmic history of resolved diabetic keratopathy.
Peribulbar anesthesia was administered using a 1:1 mixture of 2% lidocaine hydrochloride (6 mL; Shandong Hualu Pharmaceutical Co., Ltd.) and hyaluronidase 75 IU (Shanghai First Biochemical Pharmaceutical Co., Ltd). The procedure was completed without complications. At approximately 4 hours postoperatively, during routine rounds, the patient presented with periorbital redness, swelling, and visible subcutaneous bruising around the right eye. Visual acuity was counting fingers at 50 cm (CF/50cm), with an intraocular pressure (IOP) of 28 mmHg. This was initially presumed to be minor subcutaneous hemorrhage related to the local anesthetic injection. The swelling, however, progressed substantially. By 7 hours postoperatively, it had extended to involve the ipsilateral hemiface. Further progression to the anterior cervical region was noted at around 12 hours after surgery, at which time her vision had changed to CF/30cm and IOP had decreased to 16 mmHg. A routine non-contrast computed tomography (CT) scan of the neck was obtained to exclude alternative diagnoses. Imaging findings demonstrated diffuse soft tissue thickening with associated edema in the right hemifacial region and cervical soft tissue compartments.
Ultrasonic B-mode imaging revealed the absence of peribulbar and retrobulbar hemorrhage compared with the preoperative findings (Figure 1a), thereby excluding these conditions from the differential diagnoses (Figure 1b). The nonagenarian patient maintained stable vital signs with afebrile status throughout observation. Hematological analysis demonstrated normal leukocyte counts (4.2 × 109/L) and mildly elevated high-sensitivity C-reactive protein (hs-CRP: 10.8 mg/L; reference <10.0 mg/L). Based on the delayed hypersensitivity presentation (symptom onset >6 hours post-exposure), orbital cellulitis was ruled out. Therapeutic intervention comprised combination therapy: oral loratadine (10 mg daily for 3 days), intravenous infusion of dexamethasone (20 mg single dose), and intramuscular promethazine (25 mg single dose). To address the acute stress response, the care team implemented targeted psychological support for both the patient and family members. Clinical reassessment at 8-hour follow-up revealed marked reduction of periorbital edema without laryngeal involvement, permitting safe discharge. Subsequent evaluations confirmed sustained recovery: all symptoms had completely resolved by the one-week visit, and the patient remained stable at the one-month and six-month follow-ups, with 0.92 logarithm of the minimal angle resolution (logMAR) (commensurate with decimal visual acuity 0.12) and an intraocular pressure of 9.6 mmHg.
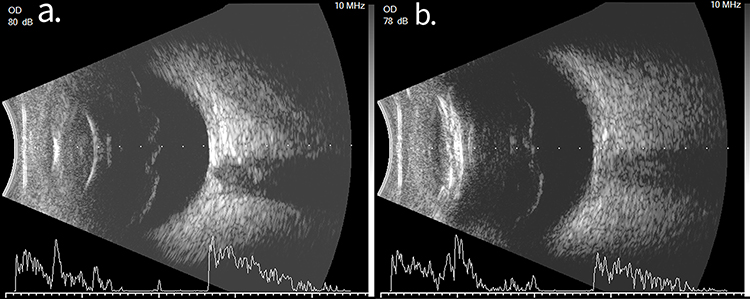 |
Figure 1 Pre- and post-operative B-mode ultrasound images of Case 1. Comparative imaging showing the ocular condition: (a) Normal preoperative anatomy before surgery. (b) B-scans showed eyelid edema without retrobulbar hemorrhage at 12 hours postoperatively after symptom onset. |
Case 2
A 69-year-old female patient underwent uncomplicated phacoemulsification with posterior chamber intraocular lens implantation in the right eye under peribulbar anesthesia. The anesthetic regimen consisted of 3 mL 2% lidocaine (Shandong Hualu Pharmaceutical Co., Ltd., China) mixed with 3 mL 1% ropivacaine (Shijiazhuang Fourth Pharmaceutical Co., Ltd., China) and 15 IU hyaluronidase (Kaifeng Kang Nuo Pharmaceutical Co., Ltd., China).
The procedure was successfully completed without intraoperative complications. However, periorbital edema involving the right upper eyelid occurred 4 hours after surgery and progressed to the ipsilateral forehead and contralateral eyelid in the 7 hours of the postoperative period. At the postoperative assessment conducted around 7 hours later, associated symptoms included inability to open the eyelids secondary to severe periorbital edema, moderate ocular pain (numerical rating scale [NRS] 5/10), and frontal headache. Vital parameters remained within normal ranges (blood pressure 154/91 mmHg, heart rate 66 beats per minute, respiratory rate 16 breaths per minute, and body temperature 36.3°C, afebrile).
Compared with the preoperative B-mode orbital ultrasonography (Figure 2a), postoperative ultrasonic B-mode imaging demonstrated diffuse periocular soft tissue edema (Figure 2b). Initial laboratory evaluation showed elevated leukocytosis (13.54×109/L; reference 3.5–9.5×109/L) with normal C-reactive protein (<10 mg/L). Despite no prior history of anesthetic hypersensitivity, the acute presentation suggested type I hypersensitivity reaction to hyaluronidase.
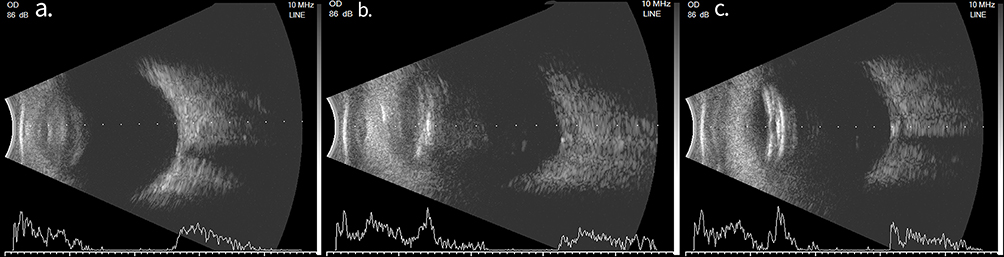 |
Figure 2 Sequential ultrasound findings in Case 2. B-scans illustrate the temporal progression of the hypersensitivity reaction. (a) Normal preoperative anatomy. (b) Early postoperative scan at around 7 hours showed eyelid and periocular edema. (c) By postoperative day 1, imaging reveals progression to a faint T-sign. |
Emergency management included: intramuscular promethazine 25 mg, intravenous infusion of dexamethasone 10 mg, 20% mannitol 250 mL intravenous infusion over 30 minutes. Serial monitoring revealed paradoxical inflammatory progression, with CRP rising to 33.92 mg/L (reference <10.0 mg/L) 24 hours later. Repeat ultrasonography showed widening of the retrobulbar Tenon’s space in the right eye, forming a characteristic T-sign configuration with the optic nerve (Figure 2c). In the setting of clinical improvement, the presence of elevated inflammatory markers and imaging findings consistent with possible scleritis warrant consideration of a bacterial infection or an atypical infectious process. Therefore, a therapeutic protocol was initiated based on empirical and prophylactic principles. This included: a short course of intravenous cefuroxime sodium (1.5 g daily for two days) to provide broad-spectrum coverage against common ocular pathogens while awaiting microbiological results, supplemented with topical gatifloxacin 0.5% eye drops. Anti-inflammatory management was intensified with topical prednisolone acetate 1% administered every 2 hours. By postoperative day 1, the patient’s facial swelling had shown moderate improvement compared to the day of surgery (Figure 3a and b). Postoperative day 2 orbital magnetic resonance imaging (MRI) of both eyes revealed that the previously noted short T2 signal in the right eye had nearly resolved. Subsequent bacterial and fungal cultures returned negative, supporting the initial diagnosis of a severe non-infectious inflammatory reaction. The empirical antibiotic was therefore discontinued after the planned two-dose course, and subsequent management was focused solely on controlling the immune-mediated response.
 |
Figure 3 Time course of edema resolution in Case 2. Facial photographs taken at (a) 7 hours, (b) 1 day, and (c) 5 days after surgery. The series illustrates the progression from acute, severe postoperative edema to its complete resolution following appropriate management. |
Complete resolution of the edema was achieved by postoperative day 5 (Figure 3c). At the 25-day follow-up, the best-corrected visual acuity (BCVA) had improved to 0.6 (0.2 logMAR) from a preoperative level of hand motion, with a stable intraocular pressure (IOP) of 10.5 mmHg. Further recovery was observed at the 1-month visit, with BCVA reaching 0.8 (0.1 logMAR) and IOP measuring 12 mmHg. By the 2-month follow-up, visual acuity in the right eye was maintained at 0.8 (0.2 logMAR), with an IOP of 10.3 mmHg.
A comparative summary of the demographic characteristics, clinical presentation, management, and outcomes of the two cases is provided in Table 1. As illustrated in Table 1, both cases shared a similar timeframe of symptom onset but exhibited marked differences in the intensity of the inflammatory response and the consequent need for escalated therapy. This comparative overview underscores the variable clinical spectrum of hypersensitivity reaction to hyaluronidase.
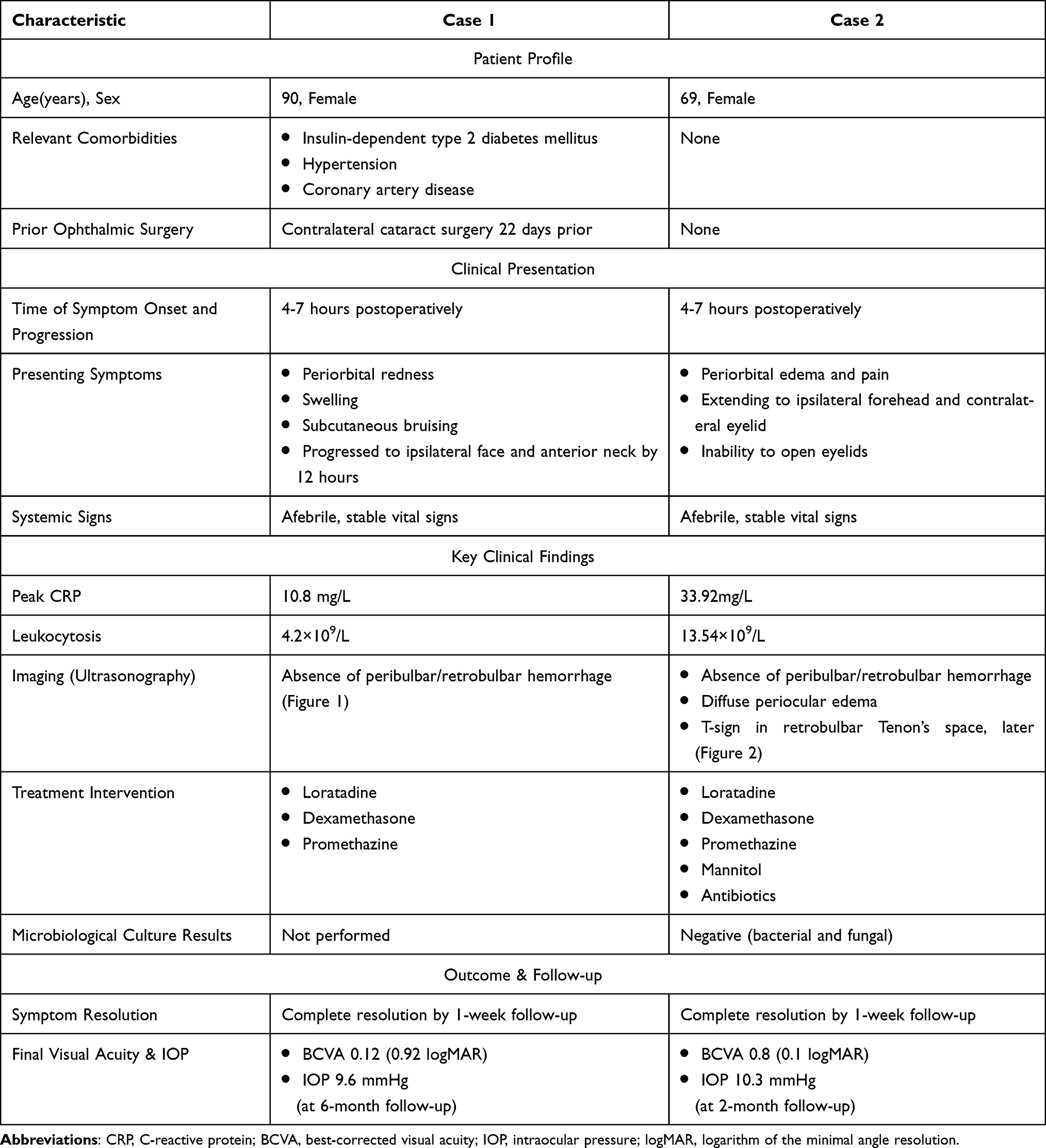 |
Table 1 Comparative Summary of Two Cases of Hyaluronidase Allergy After Peribulbar Anesthesia for Cataract Surgery |
Discussion
The presented cases highlight the critical importance of recognizing hyaluronidase-induced hypersensitivity reaction in ophthalmic practice, particularly given the enzyme’s widespread use to enhance the diffusion of local anesthetics or therapeutic agents.5,7 Although hypersensitivity reactions to hyaluronidase are rare, with an estimated incidence of 0.05% to 0.1% in clinical settings,4,11 their potential severity—ranging from localized edema to life-threatening anaphylaxis—necessitates heightened vigilance during administration and post-procedural monitoring.6,12,13 The two cases presented herein illustrate the challenge of medical diagnosis and emergency management of acute hypersensitivity reactions to hyaluronidase. While the final suspected diagnosis in both cases was consistent with this rare adverse event, the diagnostic pathway—particularly for Case 2—was fraught with confounding factors that necessitate careful analysis.
Key identified risk factors for hyaluronidase hypersensitivity include: prior exposure to the enzyme (sensitization), and pre-existing hypersensitivity to insect (eg, wasp) venom, likely due to cross-reactive IgE antibodies.5,11,14,15 This is consistent with the established pathomechanism, wherein animal-derived hyaluronidase (commonly sourced from bovine or ovine testicular extracts) can act as a trigger for such cross-reactive antibodies, particularly in individuals with pre-existing sensitivities to insect venoms or other animal proteins.16–18 This risk profile aligns with Case 1, whose recent contralateral surgery may have served as a sensitizing event. The patient’s pre-existing conditions of hypertension and diabetes were well-controlled and, based on current evidence, are not considered direct contributors to the pathogenesis of hyaluronidase hypersensitivity. In contrast, Case 2 had no prior ophthalmic surgery, which highlights that the absence of an obvious sensitizing history does not preclude a first-exposure reaction. This is in agreement with a previous review that most patients with hyaluronidase injection did not report a history of allergy or prior negative testing.5 Therefore, hyaluronidase hypersensitivity must remain a diagnostic consideration in any case of acute postoperative periorbital inflammation, irrespective of a negative allergy history. Prior to the peribulbar anesthesia, it is essential for surgeons and nurses to obtain a comprehensive medical history of patients to identify and minimize the patient-related risks (eg, active autoimmune disease, history of allergy, repeated exposure experience).19 For patients identified as high-risk, alternatives like recombinant human hyaluronidase (eg, rHuPH20) may offer a safer profile, though cost and availability remain barriers in resource-limited settings.20
As highlighted in the literature, hypersensitivity reaction to hyaluronidase can present with striking clinical and radiological similarities to infectious orbital cellulitis, creating a significant diagnostic challenge.3 In our cases, both patients remained afebrile and systemically stable throughout their clinical course. In Case 1, given the marked and rapid resolution of symptoms following treatment with corticosteroids and antihistamines alone, a localized hypersensitivity reaction was considered the most plausible diagnosis. The presentation in Case 2 was more complex, with notable leukocytosis and elevated CRP prompting empirical antibiotic coverage. However, the negative bacterial and fungal cultures provided evidence against an active infection. Furthermore, her clinical improvement followed the combined regimen, and recovery was sustained which is consistent with the resolution pattern once managed.3,5,8,12 The management of hyaluronidase hypersensitivity hinges on immediate recognition and protocol-driven intervention.21,22
Despite advances in hypersensitivity reactions and allergy management, gaps persist in clinical awareness, particularly in ophthalmic specialist agencies where emergency preparedness may be suboptimal. The cases underscore the imperative for standardized protocols, including staff training in anaphylaxis management and ready access to emergency intervention.
Limitations
Our report has several limitations that warrant acknowledgment, stemming primarily from its retrospective and observational nature. First, the diagnosis of hyaluronidase hypersensitivity reaction in both cases remains presumptive, as it was not confirmed by definitive allergy testing due to the retrospective recognition of the reaction and the patients’ subsequent discharge. While confirmatory testing (eg, serum tryptase, skin prick testing) was not standard preoperative care and might have limitations, it could provide supportive evidence for the diagnosis.5,23,24 As skin testing itself carries a risk of provoking severe reaction, necessitating cautious implementation of specialist allergy testing should be undertaken in controlled environments.5,11 Second, as elaborated in the diagnostic analysis, the presentation in Case 2 contained significant confounding factors—including elevated markers classically associated with infection (leukocytosis, CRP) and a T-sign on ultrasound—that introduce diagnostic uncertainty. While the clinical course, negative cultures, and response to therapy collectively support a severe allergic etiology, a concurrent or alternative inflammatory process cannot be ruled out with absolute certainty. These limitations highlight the critical need for prospective evaluations and systematic allergy testing in similar cases to establish more definitive diagnostic criteria.
Conclusion
Hyaluronidase hypersensitivity reaction, though uncommon, should prompt a high index of clinical suspicion, preparedness and multidisciplinary collaboration. The cases described herein reinforce that even routine procedures could be associated with allergic, hypersensitivity or inflammatory reaction, the etiology of which may be ambiguous. Given the absence of confirmatory allergy testing and the presence of confounding factors, such as elevated infectious markers in Case 2, the diagnosis remains presumptive. Nevertheless, these observations underscore the importance of a structured and cautious approach to perioperative risk management, integrating clinical assessment, laboratory and imaging findings, and microbiological correlation to differentiate adverse events (such as hypersensitivity reaction) from infectious complications. Proactive recognition, clear documentation of suspected allergens, and multidisciplinary readiness are essential to guide management and ensure patient safety. Further studies with systematic allergy testing are needed to better define diagnostic criteria and risk stratification for this potential complication.
Ethical Approval
The publication of this case report was reviewed and approved by the Medical Ethics Management Committee of Qingdao Eye Hospital, Shandong First Medical University (Approval No. QE-2025-73).
Informed Consent
Written informed consent has been obtained from the patients for the publication of this case report and any accompanying images. The consent form explicitly states that the patient’s images and clinical data can be used for scientific publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Weber GC, Buhren BA, Schrumpf H, Wohlrab J, Gerber PA. Clinical applications of hyaluronidase. Adv Exp Med Biol. 2019;1148:255–8. doi:10.1007/978-981-13-7709-9_12
2. Mohankumar A, Rajan M. Role of hyaluronidase as an adjuvant in local anesthesia for cataract surgery. Indian J Ophthalmol. 2023;71(7):2649–2655. doi:10.4103/IJO.IJO_2515_22
3. Raichura ND, Alam MS, Jaichandran VV, Mistry S, Mukherjee B. Hyaluronidase allergy mimicking orbital cellulitis. Orbit. 2018;37(2):149–153. doi:10.1080/01676830.2017.1383465
4. Venkatakrishnan JV. Hypersensitivity reaction to injection hyaluronidase after multiple eye surgery: presentation, management, and preventive strategies. Indian J Ophthalmol. 2024;72(8):1216–1218. doi:10.4103/IJO.IJO_3309_23
5. Guliyeva G, Huayllani MT, Kraft C, Lehrman C, Kraft MT. Allergic complications of hyaluronidase injection: risk factors, treatment strategies, and recommendations for management. Aesthetic Plast Surg. 2024;48(3):413–439. doi:10.1007/s00266-023-03348-5
6. Alcubierre R, Sanchez-Dalmau BF, Mousavi K. Compressive optic neuropathy secondary to an allergic reaction to hyaluronidase. Neuropatía óptica compresiva secundaria a reacción alérgica a hialuronidasa. Arch Soc Esp Oftalmol. 2019;94(9):441–444. doi:10.1016/j.oftal.2019.03.017
7. Gupta A, Moharana B, Saini R, Gupta A. Pretreatment with systemic corticosteroid can mask early symptoms of hypersensitivity reaction to hyaluronidase following peribulbar block. BMJ Case Rep. 2022;15(3):e247208. doi:10.1136/bcr-2021-247208
8. Rajalakshmi AR, Kumar MA. Hyaluronidase hypersensitivity: a rare complication of peribulbar block. Indian J Ophthalmol. 2016;64(2):160–162. doi:10.4103/0301-4738.179717
9. Wu L, Liu X, Jian X, et al. Delayed allergic hypersensitivity to hyaluronidase during the treatment of granulomatous hyaluronic acid reactions. J Cosmet Dermatol. 2018;17(6):991–995. doi:10.1111/jocd.12461
10. Pucchio A, Pur DR, Dhawan A, Sodhi SK, Pereira A, Choudhry N. Anesthesia for ophthalmic surgery: an educational review. Int Ophthalmol. 2023;43(5):1761–1769. doi:10.1007/s10792-022-02564-3
11. Murray G, Convery C, Walker L, Davies E. Guideline for the safe use of hyaluronidase in aesthetic medicine, including modified high-dose protocol. J Clin Aesthet Dermatol. 2021;14(8):E69–E75.
12. Halliday L, Sia PI, Durkin S, Selva D. Atypical case of hyaluronidase allergy with orbital compartment syndrome and visual loss. Clin Exp Ophthalmol. 2018;46(5):563–564. doi:10.1111/ceo.13128
13. Katahanas G, Van Nieuwenhuysen C, Park J, McKelvie J, McLintock C. Hypersensitivity reaction to hyaluronidase following peribulbar anesthesia: a case series. Can J Ophthalmol. 2021;56(6):e187–e189. doi:10.1016/j.jcjo.2021.04.014
14. Leibovitch I, Tamblyn D, Casson R, Selva D. Allergic reaction to hyaluronidase: a rare cause of orbital inflammation after cataract surgery. Graefes Arch Clin Exp Ophthalmol. 2006;244(8):944–949. doi:10.1007/s00417-005-0190-5
15. Borchard K, Puy R, Nixon R. Hyaluronidase allergy: a rare cause of periorbital inflammation. Australas J Dermatol. 2010;51(1):49–51. doi:10.1111/j.1440-0960.2009.00593.x
16. Kang SY, Lee SY, Kim JC, Chung BY, Park CW, Kim HO. Delayed hypersensitivity of hyaluronidase: a case report. J Eur Acad Dermatol Venereol. 2022;36(9):e691–e693. doi:10.1111/jdv.18133
17. Bertlich M, Hartmann D, Freytag S, French LE, Oppel E. Sensitization against medical hyaluronidase in patients with confirmed hypersensitivity against hymenoptera species and its clinical implications. Br J Dermatol. 2024;191(6):1000–1007. doi:10.1093/bjd/ljae290
18. Ruëff F, Bauer A, Becker S, et al. Diagnosis and treatment of hymenoptera venom allergy: S2k guideline of the German Society of Allergology and Clinical Immunology (DGAKI) in collaboration with the arbeitsgemeinschaft für berufs- und umweltdermatologie e.V. (ABD), the Medical Association of German Allergologists (AeDA), the German Society of Dermatology (DDG), the German Society of Oto-Rhino-Laryngology, Head and Neck Surgery (DGHNOKC), the German Society of Pediatrics and Adolescent Medicine (DGKJ), the Society for Pediatric Allergy and Environmental Medicine (GPA), German Respiratory Society (DGP), and the Austrian Society for Allergy and Immunology (ÖGAI). Allergol Select. 2023;7:154–190. doi:10.5414/ALX02430E
19. Baranska-Rybak W, Lajo-Plaza JV, Walker L, Alizadeh N. Late-Onset reactions after hyaluronic acid dermal fillers: a consensus recommendation on etiology, prevention and management. Dermatol Ther. 2024;14(7):1767–1785. doi:10.1007/s13555-024-01202-3
20. Rosengren S, Dychter SS, Printz MA, et al. Clinical immunogenicity of rHuPH20, a hyaluronidase enabling subcutaneous drug administration [published correction appears in AAPS J. 2015;17(6):1523-4. doi: 10.1208/s12248-015-9822-9]. AAPS J. 2015;17(5):1144–1156. doi:10.1208/s12248-015-9782-0
21. Gurnani B, Kaur K. Successful management of delayed hyaluronidase hypersensitivity after subtenon’s anesthesia during the COVID-19 pandemic: a rare case report. Indian J Pharmacol. 2023;55(1):59–61. doi:10.4103/ijp.ijp_995_21
22. Kraft MT, Kraft CT. Management of hyaluronidase allergies: the importance of specialist evaluation. Aesthet Surg J. 2024;44(11):NP850–NP851. doi:10.1093/asj/sjae160
23. Jung H. Hyaluronidase: an overview of its properties, applications, and side effects. Arch Plast Surg. 2020;47(4):297–300. doi:10.5999/aps.2020.00752
24. Park AR, Kim WM, Heo BH. Delayed allergic reaction to secondary administrated epidural hyaluronidase. Korean J Pain. 2015;28(2):153–155. doi:10.3344/kjp.2015.28.2.153
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.