Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Hyperbaric Oxygen Therapy Upregulates Neurotrophic Factors to Ameliorate Post-Stroke Depression: A Randomized Sham-Controlled Trial
Authors Tang M, Gong S, He J, Wu X, Shi M, Yang M, Shi L, Huang L, Li L, Zhou D, Zhao Y ![]()
Received 13 October 2025
Accepted for publication 11 February 2026
Published 26 February 2026 Volume 2026:22 573494
DOI https://doi.org/10.2147/NDT.S573494
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rakesh Kumar
Min Tang,1,2,* Shuang Gong,2,* Jiayue He,1,* Xiangping Wu,3 Meijun Shi,1 Mei Yang,1 Lingli Shi,1 Ling Huang,1 Longhui Li,1 Dongsheng Zhou,1 Yuanzhi Zhao1
1Department of Psychiatry, Affiliated Kangning Hospital of Ningbo University, Ningbo, People’s Republic of China; 2Department of Neurology, Ningbo Rehabilitation Hospital, Ningbo, People’s Republic of China; 3Department of Psychiatry, Affiliated Women and Children’s Hospital of Ningbo University, Ningbo, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuanzhi Zhao, Department of Psychiatry, Affiliated Kangning Hospital of Ningbo University, Ningbo, 315000, People’s Republic of China, Email [email protected] Dongsheng Zhou, Department of Psychiatry, Affiliated Kangning Hospital of Ningbo University, Ningbo, 315000, People’s Republic of China, Email [email protected]
Background: Post-stroke depression (PSD) affects 29– 52% of stroke survivors, with inflammation as a key pathophysiological mechanism. Hyperbaric oxygen therapy (HBOT) may modulate neurorestoration, but clinical evidence is limited. While meta-analytic evidence suggests HBOT may benefit PSD symptoms, high-quality randomized controlled trials employing rigorous sham-control and concurrently investigating neurotrophic mechanisms remain scarce.
Patients and Methods: In this randomized, double-blind, sham-controlled trial, 61 PSD patients were allocated to HBOT (n=29) or Sham-HBOT (n=32) groups, respectively. HAMD, NIHSS and MBI scores and serum Brain-Derived Neurotrophic Factor (BDNF), and beta-Nerve Growth Factor (beta-NGF), were evaluated at baseline as well as 2 and 4 weeks after HBOT intervention. The primary outcome was the change in the 17-item Hamilton Depression Rating Scale (HAMD-17) score from baseline to week 4, analyzed in the modified intention-to-treat population. The trial was registered (ChiCTR2100053522).
Results: HAMD scores decreased significantly in the HBOT group vs sham-group at weeks 2 (p=0.017) and 4 (p< 0.01). Serum BDNF and beta-NGF, levels were significantly elevated in the HBOT group (all p< 0.01). Reductions in HAMD scores correlated with increases in BDNF (r = 0.66, p < 0.05) and beta-NGF (r = 0.47, p =0.01). HAMD scores decreased significantly in the HBOT group compared to the sham-group, with the between-group difference reaching significance at week 2 (p=0.017) and week 4 (p< 0.001). Exploratory subgroup analyses by stroke type (ischemic vs hemorrhagic) and age (dichotomized at the median of 65 years) were conducted and these analyses revealed no significant interaction between treatment group and either stroke subtype or age subgroup on the change in HAMD-17 scores (all p > 0.05), suggesting a consistent trend of HBOT effect across these subgroups within this limited sample.
Conclusion: This preliminary trial suggests that a 4-week course of HBOT may alleviate depressive symptoms in PSD patients, an effect associated with increased serum BDNF and β-NGF levels. Given the limited sample size and short follow-up, its long-term efficacy and clinical positioning require validation in larger trials with extended follow-up.
Keywords: hyperbaric oxygen therapy, post-stroke depression, Hamilton depression scale, serum neurotrophic factors
Introduction
Stroke patients were more likely to suffer from psychiatric disorders due to physical disabilities, diminished daily living skills, and reduced social functioning. And most stroke patients suffered from post-stroke depression (PSD).1 The pooled prevalence of PSD varied from 29% to 52% within the five-year period following stroke.2 In comparison to stroke patients without depression, PSD patients have an apparent cognitive impairment and poor recovery, reducing their quality of life and increasing the load on families and society. PSD patients has a 35-fold greater chance of dying than stroke patients without depression, underscoring the urgent need to rapidly identify and treat depression after stroke.3
The brains of patients with post-stroke depression (PSD) often suffer from ischemia and/or hypoxia, triggering a series of pathophysiological changes. Cerebral ischemia can lead to bioenergetic failure, excitotoxicity, and neuronal damage, which subsequently result in the impaired signaling and downregulation of key neurotrophic factors.4 Deficiencies in Important neurotrophic factors support, including brain-derived neurotrophic factor (BDNF), beta-nerve growth factor (β-NGF), are important hallmarks of PSD pathogenesis.5,6 The compromised production and signaling of neurotrophic factors like BDNF and β-NGF in the injured brain region contributes to impaired neuronal survival, synaptic plasticity, and neural network integrity, which are central to mood regulation and cognitive function.5–9 According to the “Neurotrophic Hypothesis of Depression,” impaired neurotrophic signaling serves as a pivotal mechanism underlying synaptic and broader brain functional alterations in Major Depressive Disorder (MDD). These factors play a fundamental role in the establishment, maintenance, and adaptive plasticity of neural networks.10 Therefore, therapeutic strategies aimed at enhancing broader neurotrophic support are considered promising interventions for PSD.
Hyperbaric oxygen therapy (HBOT) is a non-invasive and non-pharmacological therapy based on exposure to pure oxygen in a sealed environment at a pressure exceeding 1 atmosphere absolute (ATA).11 HBOT could deliver oxygen to body tissues in high-pressure and oxygen-rich sealed environments, leading to the increased tissue oxygen content and improved brain function. HBOT has demonstrated safety and effectiveness in combating various neurological and psychiatric diseases with long-lasting therapeutic effects and minimal side effects. Meta analysis confirms that HBOT can generate clinical benefits by improving depressive symptoms of PSD.12,13 Multiple studies have confirmed that HBOT can enhance neuroprotective effects by promoting the expression of neurotrophic factors (NTFs). For example, in a traumatic brain injury (TBI) rat model, HBOT significantly upregulated the expression of various neurotrophic factors (such as NGF, BDNF, GDNF, and NT-3), thereby improving the neuropathological state.14 In conclusion, HBOT was demonstrated to produce clinical benefits by improving depressive symptoms in PSD, potentially linked to upregulated neurotrophic signaling. However, high-quality randomized controlled trials evaluating HBOT for PSD remain scarce, particularly those employing rigorous sham-control and concurrently investigating its potential neurotrophic mechanism.
Accordingly, the present investigation was designed as a randomized controlled trial to evaluate the clinical efficacy of hyperbaric oxygen therapy (HBOT) in individuals with post-stroke depression (PSD). A particular focus was placed on assessing its impact on neurotrophic factor levels and associated behavioral abnormalities. Therefore, this study aimed to evaluate the efficacy of HBOT on depressive symptoms in PSD patients via a randomized, double-blind, sham-controlled trial and explore whether it is associated with changes in serum BDNF and β-NGF levels.
Materials and Methods
Study Design
Employing a double-blind, randomized, parallel-group, sham-controlled design, this prospective single-center study evaluated HBOT efficacy in PSD patients. Both participants and outcome assessors were blinded to group allocation Randomization sequence generation and allocation were performed by an independent statistician. Research nurses enrolled participants but had no access to allocation sequences, ensuring allocation concealment. The study protocol was approved by the Ethics Committee of the Affiliated Kangning Hospital of Ningbo University (Approval No.: NBKNYY-2021-LC-34). All participants provided written informed consent before enrollment. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Supplementary materials include the CONSORT flowchart (Figure S1) and the exploratory subgroup analyses by stroke type and age (Supplementary Table S1). Participants were recruited from the stroke inpatient units of The Affiliated Kangning Hospital of Ningbo University and Ningbo Rehabilitation Hospital between May 2022 and July 2023. This study was conducted in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines.15 The protocol, along with the statistical analysis plan, was prospectively registered at the Chinese Clinical Trial Registry (Identifier: ChiCTR2100053522; accessible at: http://www.chictr.org.cn/showproj.aspx?proj=140799.
Inclusion criteria included: (1) diagnosed as stroke by CT or MRI based on the World Health Organization (WHO) definition, with an age range of 30–80 years; (2) meeting the DSM-5 diagnostic criteria for depression, defined by a score ≥ 8 on the 24-item Hamilton Rating Scale for Depression (HAMD-24);16 (3) without severe intellectual, cognitive, or comprehension/expression impairments (eg, aphasia); (4) being conscious with stable vital signs; (5) both the patient and their family members were fully informed of the study procedures and potential risks and provided written informed consent. The HAMD-24 was used for screening and inclusion (cut-off ≥ 8), while the 17-item Hamilton Depression Rating Scale (HAMD-17) was used as the primary efficacy endpoint for assessment.
Exclusion criteria included: (1) history of other mental illnesses and substance-use disorders; (2) use of antidepressant drugs in the past month; (3) intracranial infection, intracranial effusion or tumor occupation; (4) severe diseases of vital organs such as heart, liver, kidney, epilepsy, and glaucoma; (5) contraindications to HBOT; (6) those who did not follow the prescribed treatment plan or had poor compliance.
Patients diagnosed by ≥ 2 psychiatrists and meeting inclusion criteria were provided comprehensive information on study objectives, procedures, potential benefits, and risks. After obtaining written informed consent, participants underwent 1:1 randomization to HBOT or sham-HBOT groups via a computer-generated sequence, supervised by a blinded researcher. Demographic (age, gender) and clinical baseline data were collected. Blinded assessors performed standardized scale evaluations at baseline, week 2, and week 4 post-treatment. Inflammatory cytokines were assayed at baseline and week 4.
Note on Outcomes and Trial Registration
The trial was registered with a comprehensive list of planned exploratory secondary outcomes. However, based on data completeness, feasibility of assessment in our participant population, and a focus on the core clinical features of Post-Stroke Depression (PSD), the present analysis reports on the key secondary outcomes of neurological function (NIHSS), activities of daily living (MBI), and global cognition (MMSE). Some registered exploratory measures (eg, specific neurophysiological tests) were not included in the final analysis due to practical constraints and incomplete datasets, ensuring the robustness and interpretability of the findings presented here. This analysis focuses on the core clinical outcomes and the pre-specified biomarkers (BDNF, β-NGF). All analyses are based on the modified intention-to-treat population.
Basic Treatment
Upon enrollment, all participants remained on standardized post-stroke maintenance therapy. This regimen encompassed management of cerebral circulation, antiplatelet aggregation, control of blood lipids and blood pressure, anticoagulation when indicated, neural nutritional support, and neurorehabilitation training. Throughout the study duration, no participants received supplemental antidepressant medications.
HBOT Procedures
All interventions were conducted in a multi-place hyperbaric chamber (Yantai Hongyuan Oxygen Industry, China). The treatment course consisted of 20 sessions administered five days per week over four weeks. In the active HBOT arm, participants received 100% oxygen via mask at 2.0 atmospheres absolute (ATA) for 90 minutes, incorporating a 5-minute air break after every 20 minutes of oxygen breathing. Compression and decompression phases were conducted at a rate of 1.0 meter per minute. The sham control protocol involved breathing 21% oxygen (room air) at 1.03 ATA for an identical 90-minute duration. To enhance blinding, the chamber pressure for the sham group was briefly increased to 1.2 ATA with accompanying airflow noise during the initial five minutes, then gradually reduced to 1.03 ATA over the subsequent five minutes at a decompression rate of 0.4 m/min. Upon trial completion, participants were informally asked to guess their group allocation. The proportion of correct guesses was near chance level in both groups (HBOT: 51.7%; Sham:53.1%), suggesting that participant blinding was largely maintained under the protocol used.
Neuropsychological Assessment
All participants underwent comprehensive neuropsychological and clinical assessments at baseline, week 2, and week 4 post-treatment. The primary endpoint, depression severity, was assessed using the Hamilton Depression Rating Scale (HAMD-17), with scores ≥7 indicating depression and <7 remission. Secondary outcomes included:
Global cognitive function was assessed using the Mini-Mental State Examination (MMSE).17 The level of functional independence in activities of daily living (ADL) was measured by the Modified Barthel Index (MBI), which yields a score ranging from 0 to 100.18
Blinded, experienced psychiatrists conducted all face-to-face assessments.
Neurotrophic Factors
Following 8 min centrifugation at 3000 rpm, the blood samples were kept at −80 °C until further testing. BDNF and beta-NGF ELISA kits (Proteintech, USA) were used in the study. Standard curves were established for the determination of the concentrations of each cytokine according to the manufacturers’ instructions.
Sample Size
Sample size was calculated based on HAMD score changes from pilot data. With α=0.05, β=0.20, expected mean difference of 4.5 points (SD=3.8), and 20% attrition rate, 33 participants per group were required (G*Power 3.1).
Statistics
Statistical analyses were performed using SPSS (version 22.0) and R Studio (version 4.5.0). Graphical presentations were created with GraphPad Prism (version 8). Normality of continuous variables was tested using the Shapiro–Wilk test, and homogeneity of variance was assessed using Levene’s test. As some neurotrophic factor data violated normality assumptions, Quade’s nonparametric analysis of covariance was employed for between-group comparisons using baseline values as covariates. To compare baseline characteristics between the HBOT and sham groups, χ2 tests, independent samples t-tests, or Mann–Whitney U-tests were applied based on data type. Changes in neuropsychological scores over time were evaluated with a two-way mixed-design analysis of variance (ANOVA), with Group as the between-subjects factor and Time (baseline, post-treatment) as the within-subjects factor. Between-group Neurotrophic factors changes were analyzed using Quade’s ANCOVA or ANCOVA. Effect sizes were reported as partial η2. Neurotrophic factors-neuropsychological score correlations used Pearson’s or Spearman’s tests. All analyses for primary and secondary outcomes were based on a modified intention-to-treat (mITT) principle, including all randomized participants who had at least one post-baseline assessment. Missing data (7.6%, 5/66) due to scheduling conflicts or mild claustrophobia were handled using multiple imputation by chained equations (MICE package in R), with age, baseline HAMD, NIHSS, BDNF, and β-NGF scores included in the imputation model. Sensitivity analysis showed that per-protocol analysis yielded results consistent in direction with the mITT analysis. A p-value of less than 0.05 was considered statistically significant.
Results
A total of 80 patients with PSD were assessed for eligibility. Fourteen were excluded, with reasons being ineligibility (n=7) or declining to participate (n=7). The remaining 66 participants were randomly assigned to either the HBOT group or the sham-HBOT group (33 per group).
During the trial, five participants withdrew (HBOT group: 4 due to scheduling conflicts [n=2] or mild claustrophobia that developed during the course of HBOT [n=2]; sham group:1 due to scheduling conflict). The CONSORT diagram detailing participant flow through the study is provided in Figure S1.
Exploratory subgroup analyses by stroke type (ischemic vs hemorrhagic) and age (dichotomized at the median of 65 years) were conducted and are summarized in Supplementary Table S1. These analyses revealed no significant interaction between treatment group and either stroke subtype or age subgroup on the change in HAMD-17 scores (all p > 0.05), suggesting a consistent trend of HBOT effect across these subgroups within this limited sample. Consequently, 61 patients (29 in the HBOT group and 32 in the sham group) completed the entire 2-week intervention and the subsequent 4-week follow-up assessments. Stopping rules included: (1) ≥3 serious adverse events related to HBOT, (2) protocol violation rate >15%, or (3) futility probability >80% (none occurred). Treatment adherence was 96.7% in HBOT group (mean sessions: 19.3/20) and 98.1% in sham group (mean: 19.6/20). Protocol fidelity was confirmed through random chamber parameter checks (10% of sessions).
Demographic and Clinical Characteristics
The demographic and clinical characteristics of the participants at baseline are summarized in Table 1. Mean age was 67.25 ± 11.56 years (HBOT) and 61.79 ± 15.53 years (sham). Males comprised 59.4% (19/32) and 69.0% (20/29) of the HBOT and sham groups, respectively. Groups were comparable in demographics, medications, and comorbidities (all p > 0.05).
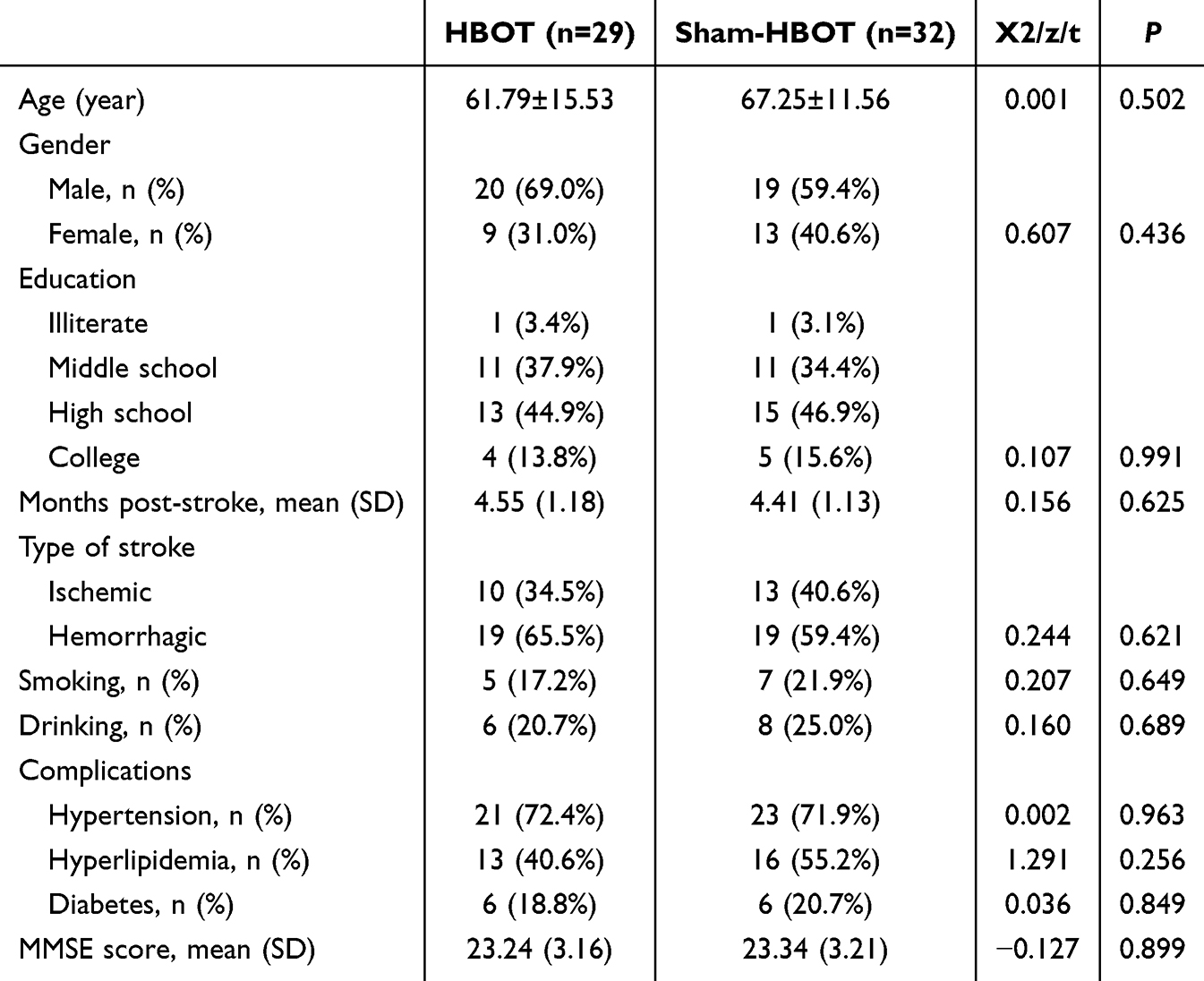 |
Table 1 General Characteristics of the Subjects |
Clinical Outcomes
Primary Outcomes
For HAMD scores (Figure 1 and Table 2), a significant interaction between Time and Group was observed in (F = 144.456, p < 0.001). Significant main effects were also found for both Time (F = 294.662, p < 0.001) and Group (F = 22.934, p < 0.001,). Simple effects analysis confirmed lower HAMD scores in the HBOT vs sham group at week 2 (p = 0.017) and week 4 (p < 0.001). Significant reductions from baseline occurred at weeks 2 and 4 within both groups (all p < 0.05).
 |
Table 2 Primary Outcomes |
 |
Figure 1 Changes in Hamilton Depression Rating Scale (HAMD) scores across the study timepoints (Baseline, Week 2, and Week 4). |
Secondary Outcomes
For NIHSS scores (Table 3 and Figure 2), the repeated-measures ANOVA indicated a statistically significant Time × Group interaction (F = 21.691, p < 0.001) and a main effect of Time (F = 152.832, p < 0.001). However, the main effect of Group was not significant (F = 0.508, p = 0.479).
 |
Table 3 Secondary Outcomes |
 |
Figure 2 Changes in National Institutes of Health Stroke Scale (NIHSS) scores across the study timepoints (Baseline, Week 2, and Week 4). |
Simple effects analysis showed lower NIHSS scores in HBOT vs sham only at week 4 (p < 0.05). Both groups improved significantly from baseline to weeks 2 and 4 (all p < 0.05).
Analysis of the Modified Barthel Index (MBI) scores revealed a statistically significant main effect for Time (F=30.730, p<0.001), indicating measurable improvements in activities of daily living (ADL) in both cohorts over the study period. Post-hoc tests confirmed significant within-group increases from baseline to both the 2-week and 4-week assessments (all p<0.05). However, neither the Time × Group interaction (F=0.958, p=0.359) nor the main effect of Group (F=0.424, p=0.517) reached significance. This pattern of results suggests that the degree of improvement in functional independence was comparable between the HBOT and sham intervention groups.
The Levels of Neurotrophic Factors
Serum levels of the measured neurotrophic factors are summarized in Table 4. Quade’s nonparametric analysis of covariance revealed a statistically significant difference in week 4 BDNF levels between groups after adjusting for baseline. The adjusted median BDNF was significantly higher in the HBOT group compared to the sham-HBOT group, with a median difference of 966.16 pg/mL (95% CI: 934.42, 997.90). The effect size Cliff’s d = 0.54 (95% CI: 0.08–0.51) indicated a large effect size.
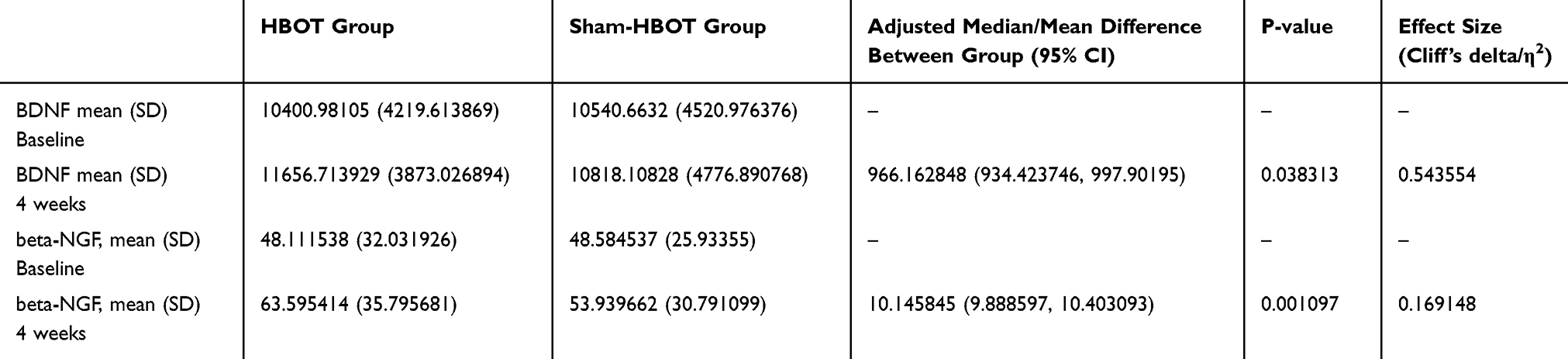 |
Table 4 Between-Group Comparison of Neurotrophic Factor Levels in Baseline and 4 weeks (Quade’s Nonparametric Analysis of Covariance and ANCOVA Adjusted for Baseline) |
ANCOVA with baseline adjustment confirmed a significantly higher expression of beta-NGF in the HBOT group compared with the Sham-HBOT group (95% CI:9.89, 10.40, p < 0.01). After adjusting for baseline values, the between-group difference in adjusted means was 10.15 pg/mL, corresponding to a medium effect size (η2 > 0.06).
Correlation Between the Reduction of HAMD and the Changes of Neurotrophic Factors
Figures 3 and 4 showed a positive correlation the results of exploratory correlation analyses, revealing a positive association between the reduction of HAMD and the changes of neurotrophic factors (for BDNF, r = 0.66, p < 0.05; for beta-NGF, r = 0.47, p =0.01).
 |
Figure 3 Scatter plot illustrating the correlation between the reduction in Hamilton Depression Rating Scale (HAMD) scores and the change in serum beta-Nerve Growth Factor (β-NGF) levels. |
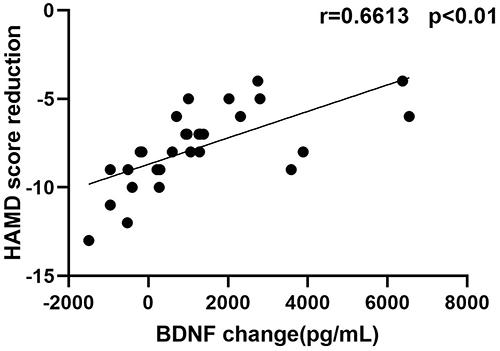 |
Figure 4 Scatter plot illustrating the correlation between the reduction in Hamilton Depression Rating Scale (HAMD) scores and the change in serum Brain-Derived Neurotrophic Factor (BDNF) levels. |
Adverse Reactions
In the study, none of subjects experienced significant adverse reactions during the treatment. Only the Sham-HBOT group had two cases of mild dizziness, which resolved on their own after rest and did not affect routine treatment. Therefore, no special treatment was further performed.
Discussion
To our knowledge, this represents the first randomized, double-blind, sham-controlled trial designed to evaluate the effects of HBOT on both the depressive symptomatology and circulating neurotrophic factor profiles of patients diagnosed with PSD. A significant reduction in depressive symptoms, measured by the HAMD scale, was observed in the HBOT cohort. This improvement, evident at both 2 and 4 weeks post-treatment, was accompanied by a rise in serum levels of the neurotrophic factors BDNF and β-NGF. Moreover, improvements in HAMD scores were positively correlated with increases in neurotrophic factors. These findings suggest that HBOT may alleviate depressive symptoms in PSD, an effect that was accompanied by—and statistically correlated with—increased serum levels of BDNF and β-NGF. This association provides preliminary support for the hypothesis that neurotrophic and neuroplastic mechanisms are involved in the therapeutic response to HBOT in PSD.5–9,19
PSD, as a common complication of stroke, involves complex pathophysiological mechanisms such as inflammatory processes, altered neuroplasticity, and dysregulation of neurotrophic factors.20–22 The increase in BDNF is closely associated with neuroprotection and synaptic plasticity, while β-NGF is critical for the survival of cholinergic neurons in the basal forebrain, partially explaining the comprehensive benefits of HBOT in improving cognition and mood in PSD patients.2,20 For instance, Robinson and Jorge noted in their review that altered neurotrophic responses and neuroplasticity are relevant etiological factors in PSD, and antidepressant treatments can promote recovery by enhancing neurotrophic factor levels.2 Similarly, Feng et al emphasized the central role of inflammatory pathways in PSD, with changes in BDNF expression linked to depression severity.20
The ability of HBOT to elevate neurotrophic factor levels may stem from its fundamental physiological function of correcting local cerebral ischemia and hypoxia.23 Our observed upregulation of neurotrophic factors can be interpreted within the framework of the Hyperoxic-Hypoxic Paradox (HHP).24,25 Repeated intermittent hyperoxia during HBOT may paradoxically induce hypoxia-like signaling (eg, stabilization of hypoxia-inducible factor-1α, HIF-1α), triggering an endogenous repair program that includes promoting angiogenesis, eurogenesis, and the expression of neurotrophic factors like BDNF and β-NGF.26,27 Although our study did not directly measure hypoxia indicators, literature suggests that PSD pathophysiology includes cerebrovascular deregulation, neuroinflammation, and oxidative stress.1,2,20 The therapeutic mechanisms of HBOT in this context are likely multifactorial. By dramatically increasing arterial oxygen partial pressure and diffusion capacity, HBOT may first improve cerebral oxygen delivery and energy metabolism in the ischemic penumbra.23,28 This can help mitigate excitotoxicity and reduce oxidative stress. Furthermore, the hyperoxic environment may modulate microglial activation and downregulate pro-inflammatory cytokines, potentially breaking a key vicious cycle in PSD.20,21 Collectively, these actions create a favorable microenvironment for neuronal survival and repair.19,29 In this improved environment, the capacity of neurons and glial cells to synthesize and release key neurotrophic factors like BDNF and β-NGF is restored.29 The elevation of BDNF is particularly important as it promotes synaptic remodeling, neurogenesis, and neuronal survival through activation of relevant pathways, directly contributing to antidepressant efficacy.19
Compared to existing PSD treatments, our results support HBOT as a complementary therapy. Traditional antidepressants have proven efficacy but may come with side effects or delayed onset.30 HBOT, by physically modulating hypoxia and inflammation, could offer more direct neuroprotective benefits. As a non-pharmacological, physical therapy. HBOT may offer a different side effect profile and potentially more directly target cerebral ischemia/hypoxia, a core pathophysiology of PSD. Additionally, Fan et al found that PSD involves specific brain circuit adaptations, such as altered prefrontal cortex connectivity, which may relate to neurotrophic factor-mediated repair mechanisms.31 Our results extend this perspective, suggesting that HBOT may optimize circuit adaptability by enhancing neurotrophic support. The likely explanation for the null between-group difference in MBI is that the recovery of activities of daily living is a long-term, multidimensional process. The 4-week HBOT protocol primarily targeted acute modulation of mood and the neurochemical environment. Its intensity and duration may be insufficient to translate into macroscopic gains in functional independence exceeding the control group within this short timeframe. Furthermore, accumulating evidence suggests that 40–60 daily HBOT sessions are generally required to achieve robust and durable effects on neuroplasticity and functional recovery.28 This relatively short course may explain the limited effects on NIHSS and MBI observed here.
However, this study has limitations. The small sample size (n=61) and single-center design may limit generalizability. The final analyzed sample size fell slightly short of the target calculated from pilot data, which may have reduced statistical power and made effect size estimates less precise. The single-center design and relatively homogeneous cohort limit external validity. Andersen pointed out that PSD diagnosis and heterogeneity can affect treatment response, with etiological differences between early and late PSD potentially leading to inconsistent efficacy.32 Furthermore, the short follow-up period (only 4 weeks), a common timeframe for assessing acute-phase antidepressant efficacy, prevents assessment of long-term efficacy and relapse risk, aligning with the view emphasized by Das and Rajanikant that PSD management requires long-term monitoring.30 Future research should expand samples and conduct multicenter randomized trials to validate the durability and safety of HBOT. Combining psychological interventions may enhance efficacy, as suggested by Kneebone and Dunmore, who noted the potential of strategies like cognitive-behavioral therapy in PSD management.33
Collectively, our findings indicate that HBOT not only mitigates depressive symptoms in PSD but also elevates circulating neurotrophic factors, thereby lending clinical support to the involvement of inflammatory and neuroplasticity mechanisms in PSD. To build upon these results, subsequent research ought to incorporate extended follow-up periods, employ advanced techniques like neuroimaging to elucidate underlying brain circuit adaptations,31 and integration with other treatment modalities to optimize comprehensive management of PSD patients.
Conclusion
In conclusion, this preliminary study suggests that a 4-week course of HBOT may alleviate depressive symptoms in PSD patients, an effect associated with increased serum BDNF and β-NGF levels. These findings offer initial support for the neurobiological mechanisms of HBOT in PSD. However, given the limited sample size and short follow-up duration of this trial, these conclusions require confirmation in larger-scale, longer-term randomized studies. Future research should explore optimized HBOT protocols (eg, extended sessions) and evaluate their long-term benefits in combination with standard care.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request. Deidentified participant data, the study protocol, and statistical analysis plan will be made available to qualified researchers upon publication, subject to a data use agreement, via Email to the corresponding author. Data will be accessible for 5 years after publication.
Acknowledgments
We thank Prof. Wei Cui for manuscript revision assistance. An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR, Inc. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Author Contributions
All authors meet the authorship criteria outlined by the International Committee of Medical Journal Editors (ICMJE). Their specific contributions include: participation in study conception/design, data acquisition, analysis, or interpretation; drafting or critically reviewing the manuscript for important intellectual content; final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreement to be accountable for all aspects of the work.
Funding
Natural Science Foundation of Ningbo (2021J276); Zhejiang Province Medical and Health Technology Project (2022KY1174, 2023KY1126); Ningbo Science and Technology Innovation Yongjiang 2035 Key Technology Breakthrough Plan (2024Z191).
Disclosure
All authors declare no biomedical financial interests or potential conflicts of interest for this work.
References
1. Medeiros GC, Roy D, Kontos N, Beach SR. Post-stroke depression: a 2020 updated review. Gen Hosp Psychiatry. 2020;66:70–11. doi:10.1016/j.genhosppsych.2020.06.011
2. Robinson RG, Jorge RE. Post-stroke depression: a review. Am J Psychiatry. 2016;173(3):221–231. doi:10.1176/appi.ajp.2015.15030363
3. Razmara A, Valle N, Markovic D, et al. Depression is associated with a higher risk of death among stroke survivors. J Stroke Cerebrovasc Dis. 2017;26(12):2870–2879. doi:10.1016/j.jstrokecerebrovasdis.2017.07.006
4. Zhan Q, Kong F. Mechanisms associated with post-stroke depression and pharmacologic therapy. Front Neurol. 2023;14:1274709. doi:10.3389/fneur.2023.1274709
5. Galvez-Contreras AY, Campos-Ordonez T, Lopez-Virgen V, Gomez-Plascencia J, Ramos-Zuniga R, Gonzalez-Perez O. Growth factors as clinical biomarkers of prognosis and diagnosis in psychiatric disorders. Cytokine Growth Factor Rev. 2016;32:85–96. doi:10.1016/j.cytogfr.2016.08.004
6. Yang L, Zhang Z, Sun D, et al. Low serum BDNF may indicate the development of PSD in patients with acute ischemic stroke. Int J Geriatr Psychiatry. 2011;26(5):495–502. doi:10.1002/gps.2552
7. Aloe L, Rocco ML, Bianchi P, Manni L. Nerve growth factor: from the early discoveries to the potential clinical use. J Transl Med. 2012;10:239. doi:10.1186/1479-5876-10-239
8. Martinowich K, Lu B. Interaction between BDNF and serotonin: role in mood disorders. Neuropsychopharmacology. 2008;33(1):73–83. doi:10.1038/sj.npp.1301571
9. Zhang E, Liao P. Brain-derived neurotrophic factor and post-stroke depression. J Neurosci Res. 2020;98(3):537–548. doi:10.1002/jnr.24510
10. Fries GR, Saldana VA, Finnstein J, Rein T. Molecular pathways of major depressive disorder converge on the synapse. Mol Psychiatry. 2023;28(1):284–297. doi:10.1038/s41380-022-01806-1
11. Ortega MA, Fraile-Martinez O, Garcia-Montero C, et al. A general overview on the hyperbaric oxygen therapy: applications, mechanisms and translational opportunities. Medicina. 2021;57(9):864. doi:10.3390/medicina57090864
12. Liang XX, Hao YG, Duan XM, Han XL, Cai XX. Hyperbaric oxygen therapy for post-stroke depression: a systematic review and meta-analysis. Clin Neurol Neurosurg. 2020;195:105910. doi:10.1016/j.clineuro.2020.105910
13. Fu Q, Duan R, Sun Y, Li Q. Hyperbaric oxygen therapy for healthy aging: from mechanisms to therapeutics. Redox Biol. 2022;53:102352. doi:10.1016/j.redox.2022.102352
14. Xing P, Ma K, Li L, Wang D, Hu G, Long W. The protection effect and mechanism of hyperbaric oxygen therapy in rat brain with traumatic injury. Acta Cir Bras. 2018;33(4):341–353. doi:10.1590/s0102-865020180040000006
15. Stevely A, Dimairo M, Todd S, et al. An investigation of the shortcomings of the CONSORT 2010 statement for the reporting of group sequential randomised controlled trials: a methodological systematic review. PLoS One. 2015;10(11):e0141104. doi:10.1371/journal.pone.0141104
16. Kovacs M, Rush AJ, Beck AT, Hollon SD. Depressed outpatients treated with cognitive therapy or pharmacotherapy. A one-year follow-up. Arch Gen Psychiatry. 1981;38(1):33–39. doi:10.1001/archpsyc.1981.01780260035003
17. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198.
18. Alsubiheen AM, Choi W, Yu W, Lee H. The effect of task-oriented activities training on upper-limb function, daily activities, and quality of life in chronic stroke patients: a randomized controlled trial. Int J Environ Res Public Health. 2022;19(21):14125. doi:10.3390/ijerph192114125
19. Kim J, Yang M, Kim J, et al. Developmental and degenerative modulation of brain-derived neurotrophic factor transcript variants in the mouse hippocampus. Int J Dev Neurosci. 2014;38:68–73. doi:10.1016/j.ijdevneu.2014.08.001
20. Feng X, Ma X, Li J, et al. Inflammatory pathogenesis of post-stroke depression. Aging Dis. 2024;16(1):209–238. doi:10.14336/AD.2024.0203
21. Ke X, Deng M, Wu Z, et al. miR-34b-3p inhibition of eIF4E causes post-stroke depression in adult mice. Neurosci Bull. 2023;39(2):194–212. doi:10.1007/s12264-022-00898-7
22. Yang Z, Zhao Y, Wang Y, et al. Echinacoside ameliorates post-stroke depression by activating BDNF signaling through modulation of Nrf2 acetylation. Phytomedicine. 2024;128:155433. doi:10.1016/j.phymed.2024.155433
23. Huang L, Obenaus A. Hyperbaric oxygen therapy for traumatic brain injury. Med Gas Res. 2011;1(1):21. doi:10.1186/2045-9912-1-21
24. Efrati S, Ben-Jacob E. Reflections on the neurotherapeutic effects of hyperbaric oxygen. Expert Rev Neurother. 2014;14(3):233–236. doi:10.1586/14737175.2014.884928
25. Efrati S, Fishlev G, Bechor Y, et al. Hyperbaric oxygen induces late neuroplasticity in post stroke patients--randomized, prospective trial. PLoS One. 2013;8(1):e53716. doi:10.1371/journal.pone.0053716
26. Ahmadi F, Khalatbary AR. A review on the neuroprotective effects of hyperbaric oxygen therapy. Med Gas Res. 2021;11(2):72–82. doi:10.4103/2045-9912.311498
27. Hadanny A, Efrati S. The Hyperoxic-Hypoxic Paradox. Biomolecules. 2020;10(6):958. doi:10.3390/biom10060958
28. Borlongan CV, Hadanny A. Why provide 40 sessions of hyperbaric oxygen therapy to patients with traumatic brain injury? Med Gas Res. 2025;15(1):132–133. doi:10.4103/mgr.MEDGASRES-D-24-00029
29. Spielman LJ, Gibson DL, Klegeris A. Incretin hormones regulate microglia oxidative stress, survival and expression of trophic factors. Eur J Cell Biol. 2017;96(3):240–253. doi:10.1016/j.ejcb.2017.03.004
30. Das J, Rajanikant GK. Post stroke depression: the sequelae of cerebral stroke. Neurosci Biobehav Rev. 2018;90:104–114. doi:10.1016/j.neubiorev.2018.04.005
31. Fan Y, Wang L, Jiang H, et al. Depression circuit adaptation in post-stroke depression. J Affect Disord. 2023;336:52–63. doi:10.1016/j.jad.2023.05.016
32. Andersen G. Post-stroke depression: diagnosis and incidence. Eur Psychiatry. 1997;12(Suppl 3):255s–60s. doi:10.1016/S0924-9338(97)89093-1
33. Kneebone II, Dunmore E. Psychological management of post-stroke depression. Br J Clin Psychol. 2000;39(1):53–65. doi:10.1348/014466500163103
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.