")
Back to Journals » Clinical Ophthalmology » Volume 16
Hydrogel Sealant for Closure of Clear Corneal Incisions in Combined Glaucoma Procedures
Authors Machiele RD , Guduru A, Herndon LW
Received 17 December 2021
Accepted for publication 10 March 2022
Published 19 March 2022 Volume 2022:16 Pages 861—865
DOI https://doi.org/10.2147/OPTH.S354531
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ryan D Machiele,1 Abhilash Guduru,2 Leon W Herndon2
1Department of Ophthalmology, University of North Carolina, Chapel Hill, NC, USA; 2Department of Ophthalmology, Duke University Medical Center, Durham, NC, USA
Correspondence: Leon W Herndon, Department of Ophthalmology, Duke University Medical Center, 2351 Erwin Road, Durham, NC, 27705, USA, Tel +1 919 681 3937, Fax +1 919 684 0547, Email [email protected]
Purpose: The purpose of this study is to determine whether ReSure hydrogel sealant is superior to standard suture for closure of clear corneal incisions in the setting of combined glaucoma procedures.
Setting: Glaucoma Department, Duke University Eye Center.
Design: This is a retrospective case series. Subjects studied were patients in a 6-year period undergoing combined phacoemulsification and glaucoma surgery. All cases were performed by the same surgeon. Wound closure methods correlated with discrete timeframes, as ReSure replaced suture midway through the study period, thereby establishing sutured closure as an analogous control group.
Methods: All cases included a phacoemulsification procedure requiring a 2.4 mm clear corneal incision. Upon completion of the phacoemulsification portion of the case, the wound was closed with either ReSure hydrogel or standard 10– 0 suture closure. The researchers assessed the rate of Seidel-positive corneal wound leak on postoperative day one.
Results: In all cases employing ReSure, no wound leak was observed at postoperative day one. Within the suture group, 3 cases showed Seidel positivity of the corneal incision. This equates to a statistically significant difference in wound leak frequency of 2.04% (P = 0.012); confidence interval, 0.21 to 5.82.
Conclusion: ReSure was able to maintain closure 100% of the time over hundreds of combined cases. Suture, though the standard of practice, did not perform to this level, presenting with 3 cases of spontaneous wound leak. We conclude that ReSure is highly effective and superior to suture in closure of clear corneal incisions in combined glaucoma procedures.
Keywords: ophthalmic, glue, suture, leak, MIGS, endophthalmitis
Introduction
Wound closure methods in the setting of cataract procedures have received investigative attention as of late. Insufficient closure of surgical wounds exposes the patient to a high risk of infection as well as hypotony and corneal decompensation. Suturing remains the gold standard of closure for surgical wounds, yet studies evaluating the effectiveness of wound closure have found that 24–34% of sutured corneal incisions demonstrate leakage under minimal strain (the force equivalent to a blink).1 In pursuit of a more reliable closure, compounds such as cyanoacrylate, fibrin glues, and polyethylene-glycol (PEG) based sealants have been implemented as adjunctive or replacement techniques. ReSure, a hydrogel PEG-based sealant, is currently the only sealant approved by the FDA for use in closing a leaking corneal incision.
ReSure has been extensively studied in the setting of simple cataract procedures, demonstrating a corneal wound leakage rate of less than 1%.2 The properties of this hydrogel sealant offer significant advantages: it is immunologically inert, it absorbs as the epithelium heals, and it does not expand as it polymerizes. ReSure is commonly employed in closure of leaking clear corneal wounds in simple cataract surgery but has not been studied in the setting of cases combining cataract surgery plus glaucoma surgery. These combined cases involve a much higher degree of manipulation of the wound due to the additional steps involved in filtration surgery, angle manipulation or placement of a drainage device. Additionally, combined glaucoma cases by design involve larger amplitude changes in intraocular pressure, which can also influence integrity of the clear corneal incision.3 Based on these mechanistic considerations, it is prudent to optimize wound integrity in these cases.
An estimated 20% of cataract procedures are performed in individuals with comorbid glaucoma and ocular hypertension.4 A large-volume study of endophthalmitis after cataract surgery recently found that endophthalmitis occurred four times as often in combined cases than standalone cataract surgeries.5 As utilization of combined procedures increases, these findings underscore the importance of optimizing wound closure. Thus, the purpose of this study is to evaluate the effectiveness of ReSure as a closure device in the setting of combined cataract and glaucoma procedures.
Materials and Methods
Study Design
This was a retrospective chart review of all patients undergoing combined phacoemulsification and glaucoma surgery in a six-year period. All surgeries were performed by the same surgeon (Leon W. Herndon) at the Duke University Eye Center, Durham, North Carolina, USA between July 22, 2013, and October 14, 2019. The study protocol was reviewed and approved by the Duke University Medical Center Institutional Review Board. The tenets of the Declaration of Helsinki and clinical practice guidelines were followed. Patients were advised of the nature of the study and informed consent was obtained.
Patients who underwent combined glaucoma and cataract surgery with either standard closure (single 10–0 corneal suture, placed 90 degrees to the incision using a buried-knot technique) or ReSure hydrogel sealant were included in the study. Closure was done prior to proceeding to the glaucoma procedure. Sutured closure and ReSure were used in discrete timeframes so that there was no overlap, suture being employed until July 2015, after which ReSure was exclusively used.
Procedures encompassed phacoemulsification combined with: Ahmed tube, Baerveldt tube (BVT), Baerveldt tube with bleb shutdown, double tube, Molteno tube, standard trabeculectomy, trabeculectomy with Ex-Press shunt, endoscopic cyclophotocoagulation (ECP), Gonioscopy-Assisted Transluminal Trabeculotomy (GATT) with ECP, trabeculectomy with double tube, tube revision, and Xen gel stent.
A total of 452 combined cases were included in the chart review. Inclusion required cases be comprised of both a phacoemulsification component and a glaucoma procedure. Combined cases that did not incorporate a phacoemulsification step were not included in the study. One case was excluded due to patient failure to show up to the postoperative day one (POD1) exam.
Data gathered included procedure performed, closure device used, postoperative day one presence of wound leak, and postoperative day one anterior chamber depth. Postoperative day one wound leak was assessed by performing Seidel testing without pressure. Anterior chamber depth was estimated using a 1–2mm slit lamp beam offset at 60 degrees to the patient.
Application of ReSure
All reviewed cases included a phacoemulsification procedure requiring a 2.4 mm clear corneal incision (CCI). ReSure has been approved by the FDA for intra-operative closure of CCI up to 3.5mm in length. The hydrogel sealant was prepared by placing 2 drops of buffered salt solution on the trilysine and FD&C Blue well. This was then mixed with the polyethylene glycol to create the liquid sealant. The incisions were dried thoroughly with a cellulose sponge and the sealant was applied to the surface of the incision with a nonabsorbent foam applicator tip. The sealant quickly polymerized, forming an adherent gel on the corneal surface.
Statistical Analysis
Outcomes were compared between the suture closure group and the ReSure closure group. A comparison of proportions calculation was performed on the two independent groups using an N-1 chi-squared test with one degree of freedom in order to assess statistical significance of the difference in wound leak rates between groups. Calculations were performed using MedCalc for Windows statistical software.
Results
Of the 452 combined cases studied, 147 employed suture for CCI closure while in 305 cases ReSure was used as an alternative to suture. In all 305 cases in which ReSure was applied, no wound leak was observed at POD1. Within the suture group, 3 cases showed spontaneous Seidel positivity of the CCI at POD1. This equates to a statistically significant difference in wound leak frequency of 2.04% (P = 0.0124); confidence interval, 0.21 to 5.82).
Recognizing that newer MIGS procedures have the advantage of producing less deformity of clear corneal wound incisions, we performed an additional calculation that excluded these procedures, finding a difference of 2.07% (P = 0.0154); confidence interval, 0.16 to 5.91).
Type and volume of surgery performed are illustrated in Table 1. Among the three cases that exhibited POD1 CCI wound leak, two were combined phacoemulsification and trabeculectomy with Ex-Press shunt, while one was combined phacoemulsification and Baerveldt tube. AC depth did not show an association with CCI wound leak, as the 3 cases manifesting wound leak on POD1 presented with a deep and well-formed AC. A total of 3 cases presented with shallow AC on POD1, but in all cases the CCI was Seidel negative and a bleb leak was found to be the cause. Additionally, we identified no correlation between the age of the patient and incidence of CCI wound leak.
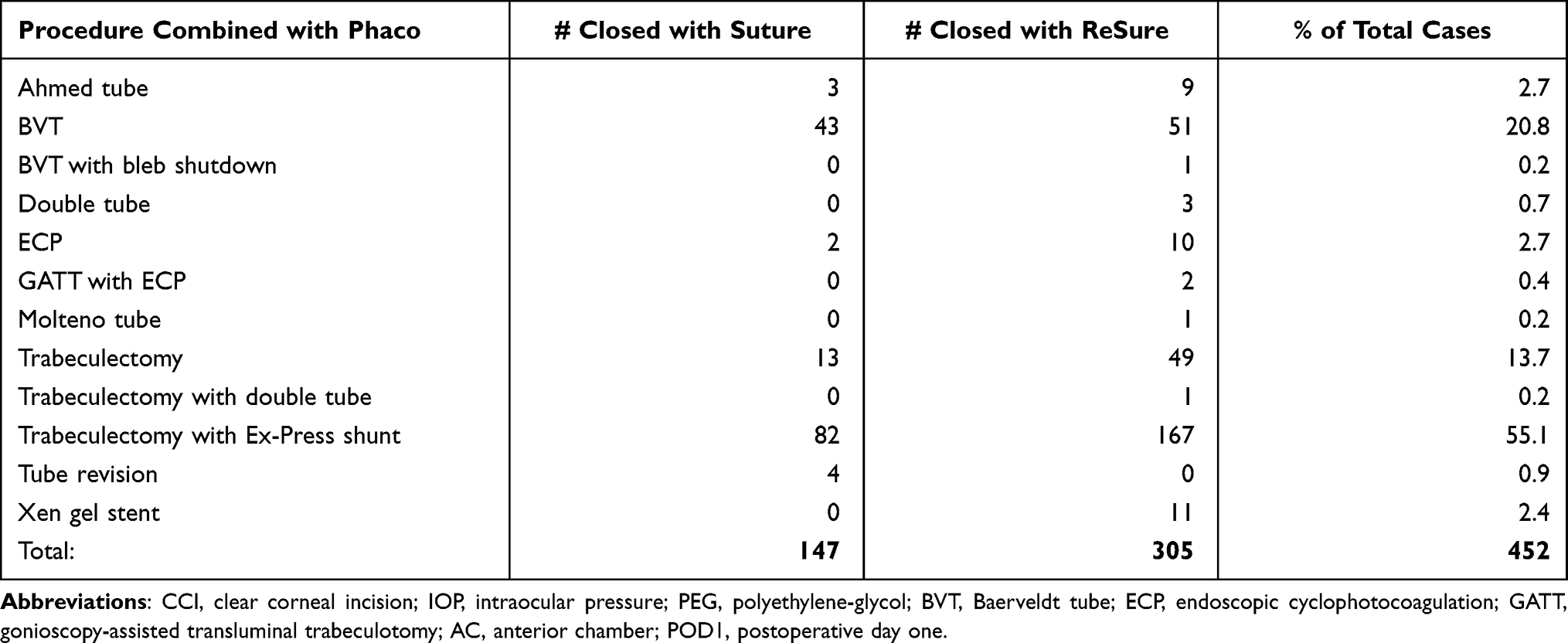 |
Table 1 Distribution of Combined Cases with Use of Either Sutured or Hydrogel Closure |
Discussion
Combined Procedures
This is the first study to examine whether ReSure could be a viable and possibly superior alternative to suturing as a means of wound closure in combined procedures. A literature review reveals only one paper exploring ReSure’s applications beyond simple cataract surgery —a case report—documenting its use in closure of trocar ports in the setting of a pars plana vitrectomy.6 Cataract and glaucoma are leading causes of visual impairment and are age-related processes which often co-occur. Both entities frequently require surgical intervention, and in many cases the requisite operations are performed simultaneously as a combined procedure.4 As the US population continues to age, it can be expected that the need for treatment of these age-related processes will continue to increase. The global prevalence of glaucoma in the population aged 40–80 years is 3.54%: this number has been steadily climbing and is forecasted to increase by 50% in the next 20 years.7 A myriad of micro-invasive glaucoma surgery (MIGS) procedures have been specifically designed for combined use in cataract removal, while phacoemulsification combined with trabeculectomy has long been performed.8 Combined procedures are therefore an increasingly relevant facet of the treatment landscape.
Whereas there is desirable benefit in combining cataract and glaucoma procedures, there are considerable risks which present opportunities for further advancement in technique and materials. Though combined cataract extraction and trabeculectomy are more effective in lowering IOP than phacoemulsification alone, postoperative management is more complicated as many studies have illustrated higher post-operative complication rates in combined procedures.9 In light of the increasing relevance of combined procedures, refinements will have enormous influence on surgical outcomes.
The Importance of Closure
Corneal wound closure is a crucial area of refinement. While sutureless clear corneal incisions are the mainstay of simple cataract procedures, the current standard of closure for combined cataract glaucoma cases calls for a single suture applied to the CCI. Sutured closure, however, has considerable disadvantages—sutured corneal wounds have been shown to leak with minimal force applied to the ocular surface.10 A study directly assessing the rate of CCI wound leak in eyes which had undergone uncomplicated cataract surgery with placement of either 10–0 nylon suture or ReSure sealant found a rate of Seidel positivity of 29.5% among the sutured group compared with 3.3% in the sealant group when minimal force was applied with a calibrated force gauge.2
Further evidence shows that a single radial suture applied to a CCI often results in a weakened wound.10 Corneal wound leakage is as a well-known pathway for infection – POD1 leak has been shown to carry a 44-fold increase in the risk for endophthalmitis.11 Endophthalmitis is a costly complication with a complex array of risk factors which must each be minimized. Intraoperative factors such as posterior capsular rupture have been shown to contribute greatly to risk of endophthalmitis (350% increased risk), while post-operative patient-related factors such as improper self-administration of antibiotic drops, ocular surface contact, and lack of handwashing have been shown to occur with remarkable frequency among the elderly.12,13
As an advancement in closure methods, ReSure stands to mitigate the risk of severe complications of wound leak such as endophthalmitis, particularly in combined cases which are known to have a four-fold higher risk of endophthalmitis.5 While none of the cases in our retrospective study developed endophthalmitis, the known risk of infection associated with wound leak highlights the importance of reliable CCI wound closure.
Value
The complications of wound leak are not without cost. A Seidel-positive wound can result in longer or more frequent clinic visits due to the need to repair and monitor. A leaking wound with severe complications is yet more costly; for example, endophthalmitis-associated morbidity and its management. For these reasons, obtaining a leak-free CCI closure is paramount. The significant difference in leak rate accompanying suture use highlights the potential value added by employing ReSure to gain a better closure. Retail cost for a package of ReSure is on average $30 greater than the cost of the standard 10–0 Nylon suture. Management of endophthalmitis following cataract surgery has been estimated to increase cost of treatment by $4893, more than doubling the ophthalmic charges.14 We therefore suggest that while employing ReSure may introduce a small additional cost to a combined procedure, its superiority in wound closure provides an overall added value and potential cost-savings via mitigating the need for additional intervention and risk of complications that are far more costly.
Time Efficiency
Beyond economic considerations, ReSure affords a time-saving benefit to patient and practitioner in bypassing post-operative suture removal. CCI suture is typically removed during the post-operative week 2 or 3 visit; eliminating this step in a follow-up exam can save time in a busy clinic while also sparing the patient any additional discomfort or stress. ReSure has been previously demonstrated to have no impact on surgery duration when compared with sutured closure, meaning there is a clear advantage in cumulative time-savings.15
Limitations
We recognize several limitations of this present study that will merit future investigation. Chiefly, this is a retrospective study, which poses limitations for the interpretation of our data. Our dataset would certainly benefit from corroboration with future randomized controlled trials. Additionally, endophthalmitis is a chief concern in this setting, yet overall, it is a rare complication. As such, our study was not sufficiently powered to detect any difference in development of endophthalmitis, instead focusing on poor wound integrity as a risk factor and corollary. Higher-volume future studies would be warranted to compare rates of endophthalmitis development between closure methods.
Conclusion
In this study we demonstrate that regardless of the type or complexity of the case, ReSure was able to maintain a watertight CCI 100% of the time over hundreds of combined cases. Suture, though the standard of practice, did not perform to this level, presenting with 3 cases of Seidel positive CCI leaks at POD1. ReSure has been shown to have no impact on postoperative IOP and is tolerated well by patients with no significant difference in level of ocular comfort compared with sutured closure.15 Given the statistically significant difference in surgical outcomes and the large volume of patients in this study, we conclude that ReSure is highly effective and superior to suture in closure of CCI in combined cataract and glaucoma procedures.
Disclosure
Dr Leon W Herndon reports grants from Ocular Therapeutix, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Masket S, Hovanesian J, Raizman M, et al. Use of a calibrated force gauge in clear corneal cataract surgery to quantify point-pressure manipulation. J Cataract Refract Surg. 2013;39(4):511–518. doi:10.1016/j.jcrs.2012.10.046
2. Masket S, Hovanesian JA, Levenson J, et al. Hydrogel sealant versus sutures to prevent fluid egress after cataract surgery. J Cataract Refract Surg. 2014;40(12):2057–2066.
3. Calladine D, Packard R. Clear corneal incision architecture in the immediate postoperative period evaluated using optical coherence tomography. J Cataract Refract Surg. 2007;33(8):1429–1435.
4. Budenz DL, Gedde SJ. New options for combined cataract and glaucoma surgery. Curr Opin Ophthalmol. 2014;25(2):141–147.
5. Pershing S, Lum F, Hsu S, et al. Endophthalmitis after Cataract surgery in the United States: a report from the intelligent research in sight registry, 2013-2017. Ophthalmology. 2020;127(2):151–158.
6. Ho VY, Shah GK, Liu EM. ReSure Sealant for Pars Plana Vitrectomy Wound Closure. Ophthalmic Surg Lasers Imaging Retina. 2015;46(10):1042–1044.
7. Tham YC, Li X, Wong TY, et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090.
8. Saheb H, Ahmed II. Micro-invasive glaucoma surgery: current perspectives and future directions. Curr Opin Ophthalmol. 2012;23(2):96–104.
9. Ogata-Iwao M, Inatani M, Takihara Y, et al. A prospective comparison between trabeculectomy with mitomycin C and phacotrabeculectomy with mitomycin C. Acta Ophthalmol. 2013;91(6):e500–501.
10. May WN, Castro-Combs J, Kashiwabuchi RT, et al. Bacterial-sized particle inflow through sutured clear corneal incisions in a laboratory human model. J Cataract Refract Surg. 2011;37(6):1140–1146. doi:10.1016/j.jcrs.2010.11.042
11. Wallin T, Parker J, Jin Y, et al. Cohort study of 27 cases of endophthalmitis at a single institution. J Cataract Refract Surg. 2005;31(4):735–741.
12. Herrinton LJ, Shorstein NH, Paschal JF, et al. Comparative Effectiveness of Antibiotic Prophylaxis in Cataract Surgery. Ophthalmology. 2016;123(2):287–294.
13. An JA, Kasner O, Samek DA, et al. Evaluation of eyedrop administration by inexperienced patients after cataract surgery. J Cataract Refract Surg. 2014;40(11):1857–1861.
14. Schmier JK, Hulme-Lowe CK, Covert DW, et al. An updated estimate of costs of endophthalmitis following cataract surgery among Medicare patients: 2010-2014. Clin Ophthalmol. 2016;10:2121–2127.
15. Nallasamy N, Grove KE, Legault GL, et al. Hydrogel ocular sealant for clear corneal incisions in cataract surgery. J Cataract Refract Surg. 2017;43(8):1010–1014.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.