Back to Journals » International Journal of Nanomedicine » Volume 20
Hydrogel-Based Vaccines: A Promising Approach for Cancer Immunotherapy
Authors Zhang W, Zhang Q, Cai J, He J, Xu Z ![]() , Chen X, Chen G
, Chen X, Chen G
Received 29 March 2025
Accepted for publication 30 August 2025
Published 18 September 2025 Volume 2025:20 Pages 11389—11415
DOI https://doi.org/10.2147/IJN.S526305
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Dongwoo Khang
Wenqin Zhang,1,* Qingfu Zhang,2,* Jiaodi Cai,1 Jin He,3 Zhijie Xu,4 Xiang Chen,5 Guoqun Chen1
1Department of Pathology, The Fourth Hospital of Changsha (The Affiliated Changsha Hospital of Hunan Normal University), Changsha, Hunan, 410006, People’s Republic of China; 2Department of Urology, The Affiliated Taian City Central Hospital of Qingdao University, Tai’an, Shandong, 271018, People’s Republic of China; 3Department of Medical Equipment, Xiangya Changde Hospital, Changde, Hunan, 415000, People’s Republic of China; 4Department of Pathology, Xiangya Hospital, Central South University, Changsha, Hunan, 410008, People’s Republic of China; 5Department of Pathology, Changsha Hospital of Traditional Chinese Medicine (Changsha Eighth Hospital), Changsha, Hunan, 410023, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guoqun Chen, Department of Pathology, The Fourth Hospital of Changsha (The Affiliated Changsha Hospital of Hunan Normal University), Changsha, Hunan, 410006, People’s Republic of China, Email [email protected] Xiang Chen, Department of Pathology, Changsha Hospital of Traditional Chinese Medicine (Changsha Eighth Hospital), Changsha, Hunan, 410023, People’s Republic of China, Email [email protected]
Abstract: Cancer vaccines, as a cornerstone of personalized immunotherapy, inhibit malignant growth through activation of a comprehensive immune defense mechanism across the organism. However, the immunosuppressive tumor environment (TME) and evasion mechanisms produced by tumors, coupled with the suboptimal immunogenic activation from vaccine-based approaches, collectively constrain therapeutic outcomes in precision immuno-oncology. Consequently, cancer vaccines have yet to realize their broad clinical translation into routine patients. Achieving controlled biodistribution and optimized pharmacokinetics of therapeutic immunization platforms within biological systems, thereby instigating durable and vigorous antitumor immunity, remains a significant challenge. To overcome these limitations, innovative administration platforms are under investigation, with hydrogel-based matrices gaining traction as effective vehicles owing to their inherent physicochemical advantages. Furthermore, recent years have witnessed accelerated advancements in hydrogel-based systems for anticancer immunization. This analysis systematically outlines the therapeutic implementations and functional mechanisms of cancer vaccines, followed by an analysis of the structural and functional properties of hydrogel-based delivery carrier. We then categorize hydrogel-based cancer vaccines and summarize their current application situation. Subsequently, a detailed overview of antitumor immune cascades orchestrated by hydrogel-integrated immunization platforms is methodically presented. Finally, we conclude with forward-looking perspectives on hydrogel-mediated therapeutic vectors.
Keywords: cancer immunotherapy, cancer vaccines, hydrogel, tumor immunity
Introduction
Neoplastic diseases persist as a predominant contributor to global health deterioration and premature mortality,1 underscoring the critical demand for innovative therapeutic modalities. Conventional oncological interventions such as surgical resection, radiation therapy, and cytotoxic agents,2,3 have significant limitations, promoting the rise of immunotherapy as a promising approach for combating various cancers.4 Currently, cancer immunotherapy mainly comprises immune checkpoint (eg, programmed cell death ligand-1/PD-L1, cytotoxic T-lymphocyte-associated antigen-4/CTLA-4) blockades (ICBs), adoptive cell transfer (eg, T cell, natural killer cells, macrophages) and vaccines therapy.5 These therapeutic approaches leverage endogenous immune defenses against malignancies to target neoplastic cells, suppressing oncogenesis while reducing relapse and metastatic dissemination.6 The year 1986 marked the inaugural regulatory authorization by the US Food and Drug Administration (FDA) of synthetic interferon-α, a pioneering immunomodulatory agent, for deployment in tumor-targeting therapeutic regimens.7,8 Immunotherapeutic approaches have achieved remarkable progress in the clinical management of diverse malignancies, including non-small cell lung carcinoma, gastric adenocarcinoma, and cutaneous melanoma.9,10 However, several challenges persist in the practical application of immunotherapy, including insufficient immune response and the risk of adverse effects. Continued efforts to explore personalized treatment strategies and optimize combination therapies are also essential for improving patient outcomes.
Among these above-mentioned approaches of cancer immunotherapy, cancer vaccines have become important weapons to fight against tumors. Traditional vaccines, which include whole inactivated organisms or attenuated pathogens, have limitations in term of safety and efficacy when applied to cancer. Recent advancements have introduced novel vaccine candidates, including DNA, RNA, peptides and tumor cell lysates, which are under extensive research.11 Vaccines can recognize and eradicate tumor cells by eliciting specific immune response and establishing immunological memory through targeting tumor antigens.12 For example, Sipuleucel-T, a pioneering immunotherapeutic agent sanctioned by the FDA in 2010, demonstrated significant survival benefit in castration-resistant prostate carcinoma cohorts during Phase III investigations.13 However, its broad clinical application has been hindered by high costs, limited treatment efficacy, and the need for multiple injections. In addition, several other cancer vaccines are currently in the preclinically or clinically stage, but have not yet been approved by the FDA.14,15 The clinical effectiveness of anticancer vaccines is frequently compromised by immunosuppressive TME characteristics and neoplastic immune evasion strategies. Additionally, vaccines are prone to rapid clearance at the injection site, and certain tumor antigens with low immunogenicity may only evoke a weak immune response. Without repeated injections into the cancer host, there is also a lack of sufficient vaccines to stimulate a continuous and robust immune response.16,17 Consequently, a critical imperative exists to develop innovative approaches that overcome current barriers and optimize the therapeutic performance of vaccine-based immunotherapies within clinical oncology practice.18
To overcome existing barriers in application of cancer vaccines, the development of optimal vaccine delivery platforms has garnered significant attention. Among these novel delivery strategies, hydrogel-based systems have gained prominence as versatile biomaterial matrices for therapeutic immunization agents, demonstrating potential to optimize immunotherapeutic outcomes. Hydrogel is a biomaterial composed of a network of hydrophilic polymers, emulating the architectural and functional attributes of native extracellular matrices (ECM).19 As a delivery carrier, hydrogels can encapsulate substances such as water, proteins and drugs, effectively preserving their structure and function.20,21 Hydrogel-based systems have garnered considerable interest as delivery matrices owing to their favorable safety profiles, superior biocompatibility, controlled biodegradation kinetics, and high payload encapsulation efficiency.22 In cancer therapy, hydrogels are expected to maximize the efficacy of cancer vaccines. On one hand, hydrogels protect vaccines from in vivo degradation, owing to their extracellular matrix (ECM)-like structure, which is composed of a highly porous network. On the other hand, therapeutic immune activation of anticancer immunization agents can be amplified via multimodal adjuvant interactions engineered into hydrogel-based delivery matrices.23,24 Additionally, hydrogels not only allow for minimally invasive injection near tumor sites but also enable the controlled, spatiotemporal release of vaccine agents.25 This approach yields reduced systemic toxicity while promoting durable tumor-specific immunoreactivity within biological systems. Therefore, understanding the current application status of hydrogel-based vaccines and optimizing their properties is crucial for advancing cancer immunotherapy.
This analysis methodically synthesizes current advances in hydrogel-based cancer vaccines and their role in optimizing therapeutic performance across solid tumor management paradigms. Specifically, we begin by presenting a detailed analysis of the general application and mechanisms of vaccines involved in cancer treatment. Next, we delve into the distinctive characteristic of hydrogels, highlighting their potential in vaccine delivery. We then classify hydrogel-based vaccines and critically evaluate their current status and application in cancer therapy. Subsequently, we summarize the underlying mechanisms by which hydrogel-based cancer vaccines modulate host immune response. Finally, we conclude with a prognostic analysis of emerging opportunities and translational barriers inherent to associated with hydrogel-based cancer vaccines.
Cancer Vaccines: A New Era in Treatment
Vaccines have long been employed for decades as prophylactic countermeasures against a diverse spectrum of infectious and clinically significant pathologies. With continuous advancements in vaccine technology, they are increasingly being explored for the prophylactic and therapeutic paradigms for diverse oncological indications. Currently, cancer vaccines are categorized into two main categories: preventive and therapeutic vaccines, differentiated by their target demographics and clinical implementation objectives. Prophylactic vaccines are designed to protect healthy individuals by preventing viral infections that can lead to virus-associated cancers. For example, HPV and HBV vaccines have been sanctioned for clinical use by the FDA to prevent virus-associated malignancies, specifically cervical carcinoma (HPV) and HBV-related hepatocarcinogenesis.26 However, prophylactic vaccines have a relatively limited scope of protection, as they are ineffective against cancers that have already happened. Conversely, therapeutic cancer vaccines are engineered for individuals with established malignancies, inducing tumor-specific immune activation that facilitates targeted recognition and elimination of neoplastic cells. These therapeutic cancer vaccines provide a potent defense mechanism to prevent tumor progression, metastasis carcinoma and recurrence. Therefore, the development of novel therapeutic vaccines targeting existing cancers remains an active and ongoing area of research. Several promising therapeutic cancer vaccines are currently under clinical trials, as outlined in Table 1.
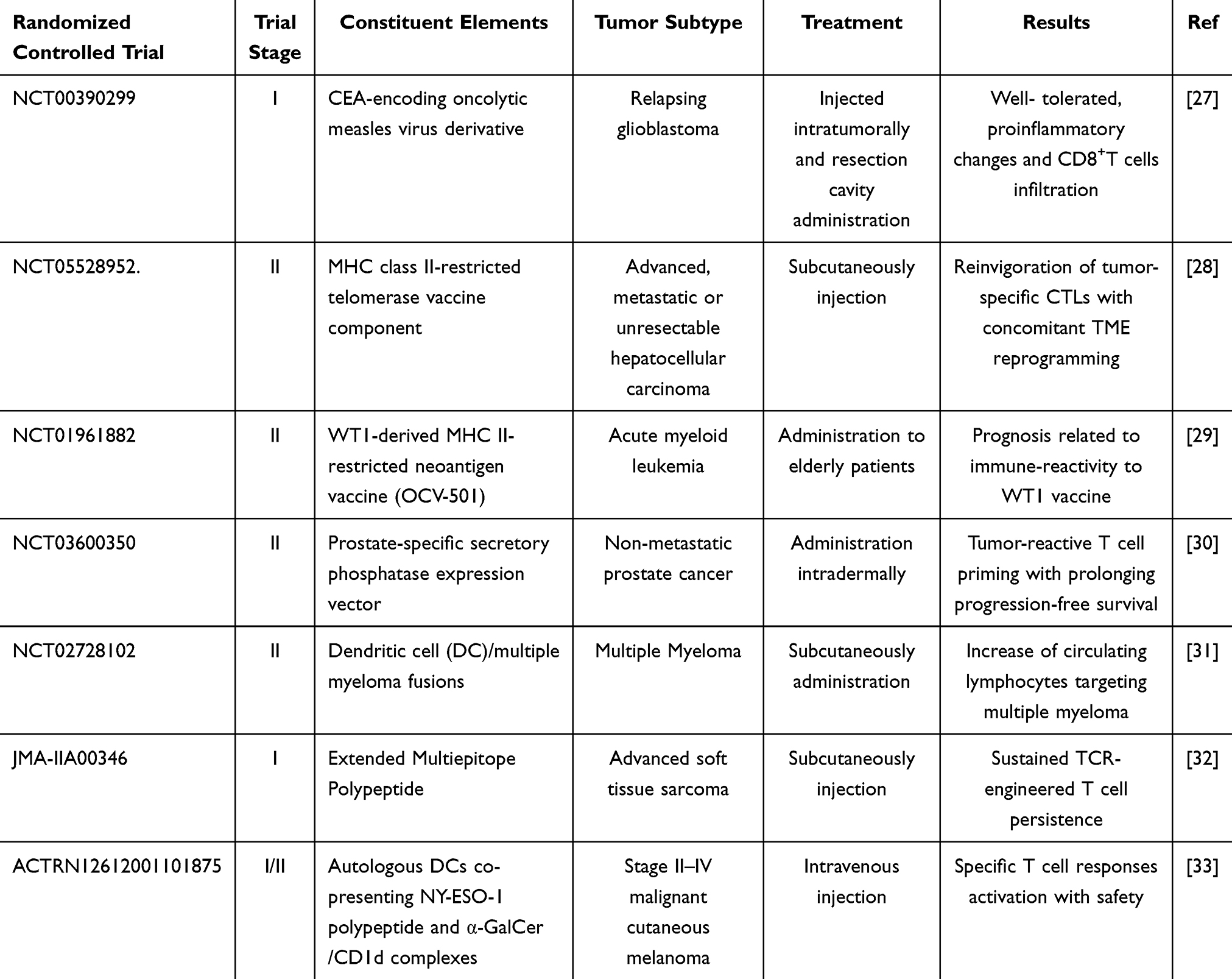 |
Table 1 Emerging Cancer Vaccine Candidates Under Active Clinical Investigation |
Exogenous vaccines are primarily delivered to the host through various methods, including polymeric microspheres, scaffolds, hydrogels or microneedles.34–37 Once introduced into the body, cancer vaccines leverage endogenous immune pathways to selectively eradicate malignant cells through antigenic recognition, initiating a tailored immunological cascade. Notably, tumor-specific immunity involves both humoral and cellular immunity induced by cancer vaccines.38,39 Mechanistically, vaccines containing antigens are internalized and processed by professional antigen-presenting cells (APCs), with dendritic cells (DCs) serving as the principal mediators of this uptake mechanism. During immune activation, cytokines initiate a signaling cascade that enhances DC recruitment and functional maturation, thereby optimizing antigen presentation. Mature DCs subsequently traffic to lymphoid tissues, where processed antigens are displayed through MHC molecules for recognition by T cell receptors (TCRs) on naïve T lymphocytes. Critical to this process, full T cell activation necessitates dual signaling: primary antigen-specific recognition through MHC-TCR engagement and secondary co-stimulatory signals mediated by molecules like CD28/B7-1,2 complexes. Post-activation, naïve T cells undergo differentiation into effector subtypes – CD4+ T helper (Th) cells, CD8+ cytotoxic T lymphocytes (CTLs), and memory T cells – each executing distinct immunological roles. In antitumor immunity, vaccine-derived antigens are preferentially loaded onto MHC-I complexes by antigen-presenting cells, enabling CD8+ T cell priming. These activated cytotoxic lymphocytes subsequently infiltrate tumor microenvironments to mediate direct neoplastic cell destruction. Parallel MHC-II-mediated antigen presentation to CD4+ T cells induces helper cell differentiation, with resultant interferon-γ and interleukin-2 secretion augmenting CTL-mediated cytotoxicity. The humoral response involves B cell antigen capture via surface immunoglobulins followed by MHC-II-restricted presentation to helper T cells. This cognate interaction induces CD40 ligand upregulation on T cells, which engages CD40 receptors on B lymphocytes to drive plasma cells differentiation and memory cell formation. Mature plasma cells secrete tumor-targeting antibodies that mediate complement activation, antibody-dependent cellular phagocytosis (ADCP) and antibody-dependent cellular cytotoxicity (ADCC) through Fc receptor engagement on innate immune cells, establishing systemic immunosurveillance against malignant cells (Figure 1).
 |
Figure 1 General function mechanism of cancer vaccine. Created in BioRender. Wenqin, Z. (2025) https://BioRender.com/ d9hih0q. Abbreviations: DCs, dendritic cells; Th cell, T helper cell; CTL, cytotoxic T lymphocyte; BCR, B cell receptor; ADCP, antibody-dependent cellular phagocytosis; ADCC,: antibody dependent cellular cytotoxicity; IFN-γ, interferon-γ; IL-2, interleukin-2. |
Although cancer vaccines have made notable progress in clinical studies, challenges such as low immunogenicity and inefficient delivery system continue to limit their widespread application in cancer treatment. Additionally, the immunosuppressive TME and immune evasion mechanism produced by tumor cells further impede the efficacy of cancer vaccines. To overcome these obstacles, hydrogels have risen as innovative delivery vehicles (as depicted in Figure 2). Research demonstrates their ability to preserve cancer vaccines from enzymatic breakdown in vivo, while orchestrating spatiotemporally programmed payload distribution within biological systems. Moreover, the incorporation of immune adjuvants within hydrogels can also enhance the immunogenicity of cancer vaccines, thereby initiating a robust immune response in host. The systematic comparative analysis between traditional cancer vaccines and hydrogel cancer vaccines is depicted in Table 2. Given these advantages, hydrogel-based cancer vaccines warrant further investigation and attention as a potential breakthrough in cancer therapy.
 |
Table 2 Traditional Cancer Vaccines vs Hydrogel Cancer Vaccines: Comparison |
 |
Figure 2 Comparison of conventional cancer vaccine and hydrogel-based cancer vaccine. Their advantages and limitations are listed in corresponding dashed or solid boxes, respectively. Created in BioRender. Wenqin, Z. (2025) https://BioRender.com/ qkezscp. |
Characteristics of Hydrogels
Hydrogel is designed as a three-dimensional, across-linked macromolecular network.40 Hydrogel matrices are predominantly engineered from biopolymers such as collagen, alginate, chitosan, and hyaluronic acid (HA), or synthetic counterparts including polyacrylamide, polyethylene glycol (PEG), and polyvinyl alcohol (PVA). These hydrogels also incorporate crosslinking agents, such as chemical materials (eg, glutaraldehyde, ethylene glycol dimethacrylate) or physical forces (eg, hydrogen bonds, ionic interactions). The three-dimensional crosslinked networks of hydrogels endow them with exceptional swelling capacity in aqueous media without structural destruction, together with tunable mechanical characteristics, such as adjustable stiffness, elasticity, and tensile strength. Notably, hydrogel incorporates a significant amount of water or biological fluids. Hydrogel materials derive their functional properties from their aqueous composition-water constituting approximately 99% of their mass. This inherent hydration confers exceptional biocompatibility and facilitates enzymatic or hydrolytic biodegradation in physiological settings, particularly within aqueous biological systems like human tissues.22,41 The hydrophilic structure of hydrogel contributes to its reduced off-target toxicity and side-effects in the host.
Emerging innovations in nanomedicine are revolutionizing the engineering of nanocomposite hydrogel systems functionalized with precisely size-tuned nanoparticles (NPs, 1–100 nm). These nanoscale additives not only strengthen the hydrogel’s mechanical integrity by interfacial interactions but also confer stimuli-sensitive behavior to microenvironmental cues, including pH gradients, thermal fluctuations, photonic inputs, and electromagnetic fields. For instance, gold nanoparticles transduce near-infrared light into thermal energy, which selectively activates temperature-sensitive hydrogel phase transitions to achieve spatiotemporally precise payload release. In intravesical bladder cancer therapy, superparamagnetic Fe₃O₄ nanoparticles enable remote manipulation of hydrogels via magnetic fields, useful in targeted delivery or dynamic tissue scaffolds.42 Besides, nanoparticles serve as precision therapeutic vectors, through transporting anti-cancer drugs as nanocarriers. The incorporation of nanoparticles in hydrogels contributes to controlled spatiotemporal release of chemotherapy drugs and reduces their systemic toxicity. For example, hydrogel matrices incorporating curcumin-loaded poly(lactic-co-glycolic acid) (PLGA) nanoparticles43 establish a tandem delivery system for hydrophobic chemotherapeutics like 5-fluorouracil44 or paclitaxel,45 keeping their sustained release and prevent them from degradation in vivo. Notably, PLGA-NPs46 have been approved by FDA as a kind of biodegradable material in clinical studies, and are considered as a promising vaccines carrier.47 Currently, nanotechnology combination with cancer vaccines has also made some progress in development of immunotherapy, that enable effective load and transportation and maintain stability of tumor antigens. Hence, emerging nanotechnology results in the production of nanovaccines constructed by nanoparticles.48 A nanoparticle-based immunotherapeutic vaccine may be inhaled or taken orally into the host. Upon absorption by APCs, nanoparticles can facilitate the generation of pro-inflammatory cytokines (eg, IL-1β, IL-12p70) while concurrently upregulating chemokine ligands (CXCL9, CCL5). This dual action facilitates the CXCR3/CCR5-guided infiltration of cytotoxic CD8+ T cells and NK cells into immunologically “cold” tumor microenvironments, thereby converting localized immune activation into systemic antitumor immunity.49 Modifying the properties of nanoparticles can enhance the tissue targeting of nanovaccines, thus improving their absorption efficiency. Taking advantage of these properties, hydrogels are used to encapsulate nanovaccines to optimize their delivery system in some researches. Recent studies have reported that nanocomposite hydrogel vaccines engineered with PLGA-NPs46 and CPMV nanoparticles,50 when incorporated into vaccines encapsulated in hydrogels, effectively suppress tumor growth, locoregional recurrence, and metastatic outgrowth. An injectable polymer-nanoparticle (PNP) hydrogel technology delivers lipid nanoparticle (LNP)-encapsulated messenger RNA (mRNA) to APCs using a modular targeting strategy. This approach enhances both the magnitude and quality of the germinal center reaction, establishing an immunological niche in vivo.51 In addition, TSA-based nanovaccines synergized with PD-1 checkpoint blockade antibodies effectively suppress the locoregional tumor recurrence and metastatic dissemination, while simultaneously triggering specific and durable immune memory in the host.52 This paradigm underscores the potential of converging patient-derived nanovaccines, hydrogel-enabled spatiotemporal delivery, and ICIs rewiring to overcome resistance mechanisms in advanced malignancies.
Hydrogels can be injected, implanted, or sprayed onto subjects.22 These versatile delivery methods make hydrogel-based systems minimally invasive, improving operational feasibility and patient compliance. In current cancer therapies, injectable hydrogels carrying vaccines can be administered to nearly any part of the host, including tumor sites, via a syringe.53 Hydrogels are broadly categorized by physiological stimulus responsiveness into thermo-sensitive and non-sensitive types. At room temperature, hydrogel is in a flowable fluid state, allowing for easy administration. Once administered into warmer physiological environment (~37°C), thermosensitive hydrogels undergo temperature-driven conformational reorganization, transitioning from a liquid-phase “sol” state to a semi-solid “gel” matrix in situ.54 This temperature-triggered sol-gel transition enables minimally invasive delivery. The injectable sol facilitates administration, while subsequent gelation ensures localized confinement and sustained release of payloads (eg, antigens/drugs), exploiting intrinsic body heat. This responsiveness further allows dynamic modulation of release kinetics during local temperature fluctuations, such as inflammation. Unlike thermo-sensitive variants, non-sensitive hydrogels form stable networks via mechanisms independent of physiological temperature. Gelation occurs through: ionic crosslinking (eg, alginate/Ca²⁺), covalent bonding (photo-/enzyme-initiated in PEG/HA systems), physical interactions (H bonding, hydrophobic forces), or enzymatic reactions (eg, fibrin/thrombin). These hydrogels are either injectable (solidifying post-injection via specific triggers) or pre-formed (surgically implanted). Examples include alginate, fibrin, collagen, and crosslinked synthetics (eg, PEG-DA). Their primary strengths include broader material selection with proven biocompatibility predictable, and stable release profiles achieved through controlled polymer chemistry, crosslink density, and porosity. Though lacking thermo-sensitive gels’ environmental responsiveness, their release kinetics exhibit superior stability against physiological fluctuations. Both thermo-sensitive and non-sensitive hydrogels serve as powerful platforms for advanced biomedical applications, particularly sustained delivery of vaccines. Thermo-sensitive variants enable injectable, temperature-triggered depot formation with potential for intelligent release. Non-sensitive types leverage broader material diversity to achieve precisely tunable stability, though requiring distinct gelation triggers or administration. Selection depends critically on the therapeutic agent, target release kinetics, administration route, and material constraints.
To enable in situ injection and prevent the rapid metabolism of hydrogel cargoes by liver and gut wall, injectable hydrogels with diverse properties are increasingly used in research applications (Table 3). By cross-linking different materials, a variety of hydrogels can be fabricated, including sulfated chitosan hydrogel, HA-based hydrogel, supramolecular and PEG-b-poly(L-alanine) hydrogel. Moreover, cells, such as DCs, can survive within the hydrogel matrix due to its favorable network structure. The porous nature of hydrogel serves as a platform that supports communication between DCs and tumor cells.55 Inside the hydrogel, sustained tumor antigen internalization by DCs drives their phenotypic maturation and subsequent lymphoid trafficking to draining lymph nodes, culminating in MHC-mediated antigen presentation to naïve T lymphocytes.56
 |
Table 3 Examples of Hydrogel Formulation Applicated in Cancer Vaccines |
As an emerging delivery carrier, hydrogels can be used to transport drugs, vaccines, bioactive molecules or cells, or participate in tissue engineering in the application of biomedicine.62,63 In addition, hydrogels are also increasingly engineered as adjuvants to synergistically amplify vaccine potency. For example, aluminum hydroxide gel is a well-established adjuvant in vaccine formulations. It helps maintain the stability of antigenic ingredients during vaccine storage and use, thereby avoiding their degradation. Aluminum hydroxide gel is commonly incorporated into subunit vaccine formulations, including diphtheria-tetanus-pertussis (DTP) combinations and hepatitis A prophylaxis. By retaining antigenic substances at the vaccination site, it prolongs DCs/lymphocytes engagement with the antigenic payload, thereby promoting the production of antibodies and enhancing vaccine effectiveness. In addition, positively charged multidomain peptide hydrogel, K2, is also utilized as a vaccine adjuvant to activate Th cells to participate in humoral immunity.64 Current clinical investigations of hydrogel vaccines demonstrate promising outcomes. In a study administering a hydrogel patch delivering tetanus and diphtheria antigens to 27 healthy participants, booster immunization was subsequently provided to a subset. No severe local or systemic adverse events were observed with this system. Notably, elevated antibody titers persisted for ≥1 year post-administration, consistently exceeding pre-vaccination baselines.65 ViscoGel, a chitosan-based hydrogel adjuvant, was co-administered via single intramuscular injection with the Haemophilus influenzae type b model vaccine Act-HIB to healthy subjects. No tolerability or safety concerns emerged. Compared to solo Act-HIB recipients, cohorts receiving ViscoGel-adjuvanted vaccination exhibited significantly elevated interferon-γ (IFN-γ) responses to Act-HIB in PBMCs. Critically, the hydrogel platform reversed vaccination-induced suppression of IFN-γ production toward both the target antigen and heterologous influenza epitopes.66
In cancer immunotherapy, hydrogels exhibit high storage capacity for antigen-based vaccines and various immunoadjuvants additionally.67 Cancer vaccines often work synergistically with immunoadjuvants, with hydrogel serving as a delivery medium.68 Both immunoadjuvants and hydrogels can enhance immune stimulation in vaccine recipients. Hydrogels protect these components from degradation and enable the controlled, sustained release of vaccines in vivo, thereby reducing dosing frequency and prolonging the duration of the antitumor immune response.69
Categories of Hydrogel-Based Cancer Vaccines
Hydrogel-formulated cancer vaccines primarily function encapsulating tumor antigens, which trigger a specific immunity targeting tumors. Tumor antigens can originate from tumor-associated proteins, DNA/RNA or tumor cells, and are then encapsulated in special hydrogels for cancer treatment. For example, the tumor-associated glycoprotein TROP2 can be effectively integrated into an oxidized dextran-based polymeric matrix for localized delivery via subcutaneous administration in preclinical studies of aggressive mammary carcinoma lacking estrogen, progesterone, and HER2 receptors. This method significantly inhibits tumor cells growth and achieves complete tumor regression in 50% of treated subjects with receptor-negative breast malignancies.70 Yuta Yoshizaki et al have reported that DCs and ovalbumin (OVA) as the antigen are encapsulated in a temperature-responsive biodegradable hydrogel. Upon injection into a mouse lymphoma model, this approach induces dendritic cells activation, potentiating antigen processing and improving treatment efficacy.61 Similarly, Chao Gao et al have demonstrated that the engineered thermoresponsive chitosan-based delivery system co-encapsulating an immunostimulatory mRNA (LIRF5) and CXCL5-targeting siRNA promotes M1 polarization, thus inhibiting tumor growth, thereby improving the therapeutic efficacy in a pancreatic cancer model.71
Based on the source of these tumor antigens, cancer vaccine immunogens are stratified into tumor-associated antigens (TAAs) and tumor-specific antigens (TSAs), the latter colloquially termed neoantigens.72 TAAs are the proteins or molecules expressed on the surface or inside of tumor cells, which can also be found in normal cells, arising from host’s genes without mutations. TAAs exhibit ubiquitous overexpression, aberrant expression or different structure modification across malignant tissues, whereas retain baseline expression in select healthy cell populations, such as carcinoembryonic antigen, alpha-fetoprotein, mucin 1. Constitutive TAA expression in normal tissues induces central/peripheral tolerance, promoting immune ignorance toward these self-antigens. Furthermore, their non-exclusive tumor expression limits immunogenicity, typically eliciting weak antitumor responses.73 Clinically validated vaccine platforms have historically leveraged these antigens for therapeutic development. Conversely, non-self-antigens constitute tumor-specific antigens (TSAs), primarily generated by somatic mutations. Neoantigens—such as those derived from mutated genes like KRAS—represent a key subset. Certain viral antigens (eg, HPV E6/E7 in cervical cancer) also qualify as TSAs. These antigens exhibit exclusive tumor cell expression, absent in normal tissues.74 Relative to TAAs, TSAs exhibit superior immunogenicity, driving robust T-cell responses. Owing to their tumor-restricted expression profiles and enhanced immune activation potential, neoantigens are regarded as ideal candidates for personalized cancer vaccines.75 The existing studies have shown that hydrogel-based cancer vaccines come in various forms, including DNA/RNA, protein, peptides, and vaccines based on DCs or tumor cells. Additionally, cancer vaccines frequently incorporate immunoadjuvants - non-antigenic substances that potentiate immune responses against tumor antigens. Examples include mineral salts, saponins, oil-in-water emulsions, immune potentiators (eg, STING, NOD-like, or Toll-like receptor agonists), cytokines, and microbial components (viruses/bacteria). By amplifying the immune system’s reaction, these adjuvants generate significantly stronger, broader, and more durable responses than immunization with antigens alone. Accordingly, tumor antigens are often paired with diverse immunoadjuvants to enhance their immunogenicity, thereby forming hydrogel-based vaccines against cancers (as shown in Table 4). Subsequent sections systematically delineate the classification and current application status of cancer vaccines, with analytical emphasis on the components encapsulated in hydrogels.
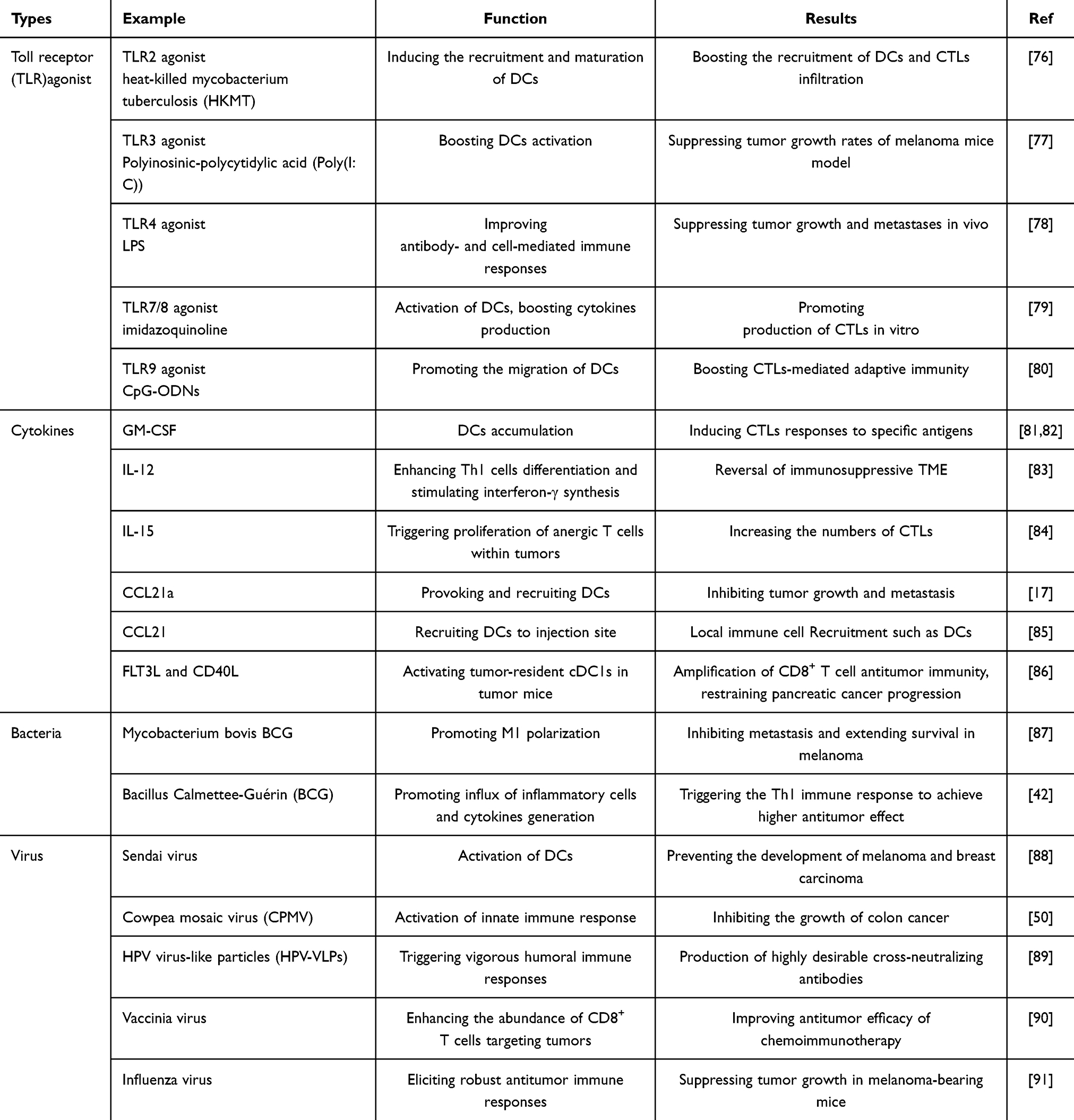 |
Table 4 Summary of Immunoadjuvants Types in Hydrogel-Based Cancer Vaccines |
DNA Based Vaccines
Circular plasmid DNA are primarily employed to construct DNA vaccines, which encode specific tumor antigens.30 For some self-antigens that are difficult to synthesize, time-consuming and costly, plasmid DNA serves as an alternative due to its tunability, thermal stability and cost-effectiveness. Once introduced into the body, plasmid DNA can be transcribed and subsequently translated into the corresponding tumor antigens, priming MHC class I-restricted CTL responses via cross-presentation mechanisms in immunocompetent hosts. Although DNA vaccines offer many advantages, there are still deficiencies that need to be addressed in practical applications. DNA vaccines encounter barriers such as nuclease-mediated catabolism within biological systems, and lower transfection efficiency, which can lead to insufficient antigen expression and weak immunogenicity, thus failing to trigger a robust immune response.
Smart hydrogel, such as poly(methacrylicacid)/poly(N-vinylpyrrolidone) multilayer hydrogel, is increasingly recognized as effective delivery platforms for DNA vaccines, enhancing their loading capacity and enabling controlled release of the vaccine contents. Such kind of hydrogel synergistically helps DNA vaccines work more effectively.92 For example, vaccines encapsulating plasmid DNA encoding for a tumor-associated idiotype antigen, through a thermoresponsive polysaccharide matrix, stimulate dendritic cells recruitment and activation in a B cell lymphoma mouse model. The combinatorial therapeutic platform utilizing immunosuppressive interleukin-10 (IL-10) silencing siRNA via the hydrogel, this approach amplifies the cytolytic activity of CTLs and CD4+ T cells, significantly increasing total survival rate versus monotherapy controls in lymphoma-bearing BALB/c murine models.93 Besides, hydrogels made from special materials also enhance the therapeutic efficacy of DNA vaccines. A hydrogel constructed from HA and levodopa (DOPA), loaded with OVA-expressing plasmid promotes DCs infiltration and induces the generation of OVA-specific antibody, thus inhibiting tumor growth in human lung carcinoma. This hydrogel delivery system provides a minimally invasive approach for DNA administration. After administration in vivo, the structure of DOPA conjugated with HA maintains the stability of hydrogel and OVA- expressing plasmid. The hydrogel with such unique structure also keeps the sustaining release of DNA vaccines in vivo, extending their retention time and strengthening the specific humoral immune response.94
These studies indicate that hydrogel-based DNA vaccines exhibit substantial therapeutic potential for tumor treatment. The smart hydrogel designed with special biodegradable and biocompatible polymers leads to their controlled degradation, subsequently regulating the release of DNA plasmid to recruit APCs such as DCs. Mass production of safe, hydrogel-based DNA vaccines for in situ tumor administration may pave the way for personalized therapeutics.
RNA Based Vaccines
Synthetic messenger RNA (mRNA)-based vaccines exploit endogenous ribosomal machinery to affect the translation of tumor antigens, thereby initiating specific immune response against tumors.95 Compared to DNA vaccines, RNA vaccines offer advantages such as simplicity, safety and production flexibility. Through crossing cell membrane, RNA vaccines, represented by mRNA, enable ribosome-mediated biosynthesis of tumor-specific polypeptides, avoiding their potential integration into the genome of cell nucleus.96 However, RNA vaccines still face challenges such as inherent instability, susceptibility to degradation, and low transfection efficiency.
Hydrogel delivery systems engineered for RNA encapsulation demonstrate enhanced ribonucleic acid integrity preservation and spatiotemporal biodistribution control, allowing them to effectively reach targeted cells or tissues. For example, a photopolymerizable hydrogel made with gelatin methacryloyl has been reported to significantly achieve enhancement in mRNA transfection and translation efficiency, through ROS-mediated endosomal escape mechanisms in mesenchymal stem cells of human.97 The engineered graphene oxide-polyethylenimine hydrogel encapsulating OVA-encoding mRNA has been shown to deliver mRNA to APCs without degradation, thus eliciting clonal expansion of antigen-specific CD8+T lymphocytes, ultimately achieving tumor volume reduction in B16-F10 syngeneic melanoma-bearing C57BL/6 murine systems.98 With a single subcutaneous administration, this hydrogel effectively protects mRNA from enzymatic degradation and enables its sustained release, thereby activating specific immune cells to achieve durable and effective anti-tumor immunity. Besides, hydrogel containing siRNA or miRNA can also inhibit protein translation by interacting with corresponding mRNA, thus participating in tumor immunity to fight against cancers. Ankur Singh et al reported that IL-10 siRNA delivered by hydrogel successfully silences the expression of immunosuppressive IL-10, through interacting with corresponding mRNA to induce its degradation. That further leads to increased DCs homing to tumor-draining lymph nodes, while potentiating Th1 polarization of CD4+ T cell precursors in A20 cell-derived B-cell lymphoma murine xenografts.93 Similarly, miRNA-205 and miRNA-182 delivered by hydrogel achieves sequence-specific oncogene silencing through RNA interference (RNAi) pathways, ultimately suppressing malignant cells growth and metastatic in triple-negative breast cancer (TNBC) xenografts.99 The application of hydrogel significantly prevents siRNA and miRNA from being decomposed in vivo, thereby achieving the intervention of relevant mRNA target to treat cancers.
Although hydrogel delivery significantly improves the stability of RNA vaccines, several issues remain to be addressed. Because of intratumoral genomic diversity, the same type of tumor can present different TSAs in individuals. Therefore, current translational efforts tend to focus on designing personalized RNA vaccines targeting specific TSAs. In addition to RNA vaccines delivery, combining chemotherapy drug, such as DOX, with other cancer treatment strategies via hydrogel delivery is expected to maximum the therapeutic efficacy of RNA vaccines.
Protein or Peptides Based Vaccines
Proteins of tumor antigen, or peptides consisting of 8–35 amino acids, presented on tumor cells, are often employed in protein or peptides-based cancer vaccines.100–102 These vaccines are relatively simple to produce, store, transport and safe,103 but their lower immunogenicity may lead to unsatisfied antigen processing and presenting, thereby causing limited T cells-mediated immune responses. Additionally, the short survival time of proteins and peptides in vivo reduces their ability to induce lasting immune responses. Notably, short peptides-based vaccines may cause immune tolerance of host, instead of eliciting anti-tumor immunity.104 Furthermore, the proportion of people, who is most likely to benefit, may be restrained by human leukocyte antigen, when subjected to peptides-based vaccines.105
Beyond the use of protein OVA as a model tumor antigen, proteins extracted from surgically removed tumors can be loaded into star-shaped polyethylene glycol-oxidized dextran copolymer matrices to create a hydrogel-based vaccine (DCHVax). When administrated subcutaneously, DCHVax recruits DCs in situ, stimulating tumor-specific immunity, thus suppressing the growth of residual tumors in various murine tumor models.106 Peptides constituted by dozens of amino acids are utilized as peptides-based vaccines, which are expressed on tumor cells and possess at least one antigen epitope of T or B cells.107 For example, human basic fibroblast growth factor (bFGF), an oncogenic driver overexpressed across multiple malignancies, contributes to their proliferation. Consequently, peptides derived from the immunodominant regions of the heparin-binding domain of bFGF, or namely truncated bFGF (tbFGF) are used to construct peptide vaccines.78,108 A thermosensitive hydrogel containing tbFGF peptides has been reported to elicit CTL-mediated adaptive immunity and specific antibody production, effectively suppressing primary neoplastic progression and distal metastatic colonization in lung adenocarcinoma murine systems.78 Hyaluronic acid hydrogel containing neoantigen peptides, such as PancVax, composed of AddaVaxTM adjuvant with a STING agonist, is implanted at the tumor site in pancreatic adenocarcinoma (PDAC) mice via surgery. This approach promotes tumor-specific T cell priming and clonal proliferation, thereby preventing local tumor relapse in PDAC mice following incomplete resection surgery.109 These hydrogels achieve easy-to-operate transportation of protein or peptides vaccines, and control their spatiotemporally on-going delivery to trigger a specific immune response in vivo.
Although hydrogel delivery systems for protein or peptide vaccines improve their stability, low immunogenicity of protein or peptides still hinders their widespread application. Therefore, immunoadjuvants have been added to protein/peptides vaccines and co-embedded in hydrogels to increase their immunogenicity in vivo.43,110 Additionally, self-assembling peptides with multiple antigen epitopes, which can trigger more vigorous immune response, may may offer a valuable strategy for enhancing hydrogel-based peptide vaccine efficacy.111,112
Dendritic Cells-Based Vaccines
DCs serve as pivotal orchestrators of adaptive immunity, distinguished by their unparalleled capacity to internalize, process, and display antigens with high efficiency.113 As specialized sentinel cells, they bridge innate and adaptive immune responses by activating naïve T lymphocytes through MHC-peptide complex presentation and co-stimulatory signaling, thereby initiating antigen-specific immune cascades critical for pathogen clearance and tumor surveillance. Especially in anti-tumor immune response, DCs can activate tumor-specific T cells, such as CTLs, to target and eliminate tumor cells. Consequently, DCs have been harnessed to fabricate DCs-based vaccines in cancer therapy.114,115 Traditionally, exogenous DCs originate from autologous peripheral blood cells and turn to be mature by tumor antigens stimulation, and then are delivered to patients as DCs vaccines.116 Following in vivo lymphoid trafficking, mature dendritic cells prime naïve CD8+T lymphocytes through MHC class I-restricted antigen presentation coupled with co-stimulatory cues, thereby initiating antigen-specific cytotoxic T lymphocyte responses critical for adaptive immune defense. However, the clinical potential of DC-based vaccines remains constrained by biological challenges, including the transient survival kinetics of activated dendritic cells in vivo and the immunosuppressive mechanisms inherent to tumor ecosystems.
As the appealing transportation system, hydrogels are employed to deliver DCs to participate in DCs vaccines-based cancer immunotherapy. For instance, DCs and tumor antigens encapsulated in peptide nanofibrous hydrogels are subcutaneously administered to tumor-bearing mice, resulting in the enhanced lymphoid recruitment and migration of endogenous DCs, therefore driving amplified intratumoral infiltration of effector CD8+T cell populations. This biomaterial-mediated strategy achieves significant tumor suppression and prolongs survival duration in the mice.117 The usage of nanofibrous hydrogels ensures the survival and duration of DCs in vivo. Besides, such hydrogels containing tumor antigens stimulate both exogenous DCs maturation and autologous DCs accumulation to capture antigens released by hydrogels. Additionally, the use of hydrogels containing activated DCs and interleukin-15 superagonist, which are constructed by polysaccharide alginate, are peritumorally injected to murine melanoma model. This strategy facilitates cytotoxic CD8+ T cell sequestration within alginate-based scaffolds and neoplastic lesions, achieving robust suppression of progressive malignancies while extending survival duration in melanoma-challenged murine models.84 Such kind of hydrogels can keep their structures and contents stable in vivo for a long time, decreasing the frequency of dosing and systemic exposure by local administration.
To maximize the therapeutic potential of DCs vaccines, hydrogel delivery systems are being studied in combination with immunotherapy strategies. For example, CaCO3 biomineralized hydrogel containing TAAs from mouse breast cancer cells-DCs fusion cells was injected into triple-negative breast cancer mice. This biomaterial platform enhanced vaccine immunogenicity through dual mechanisms: sustaining TAAs release to promote endogenous dendritic cell maturation while maintaining lymph node trafficking capacity, ultimately driving tumor-specific CD8+ T cell responses that correlated with improved therapeutic outcomes. The structure of CaCO3 biomineralized hydrogels also promotes M1 polarization to mitigate the immunosuppression of TME, where repolarized myeloid cells synergize with reinvigorated cytotoxic T lymphocytes to dismantle immunosuppressive networks.118 The use of DC vaccines combined with tumor antigens or coupled with cytokines or immunoadjuvants, and delivered through hydrogels with personalized structures, demonstrates significant potential for optimizing treatment outcomes in cancer immunotherapy.119
Tumor Cells-Based Vaccines
As a form of patient-individualized antigen, tumor cells-based vaccines are widely used in practice. These vaccines are made from whole tumor cell antigens or products derived from tumor cells, such as tumor cell membranes, tumor-derived extracellular vesicles (EVs), and tumor cell lysates. However, the inherent limitations of unmodified tumor cell-derived vaccines, characterized by rapid enzymatic degradation and systemic clearance post-administration, frequently compromise APC-mediated antigen processing efficiency, resulting in attenuated adaptive immune responses against malignancies. To address these pharmacokinetic challenges, engineered hydrogel matrices have emerged as a predominant biomaterial platform for achieving targeted co-delivery and spatiotemporal control of tumor-associated antigens while maintaining vaccine bioactivity throughout therapeutic windows.120,121
Autologous or Allogeneic Tumor Cells-Based Vaccines
Comparable to their products, whole tumor cell-based vaccines release a full range of TSAs and TAAs. Therapeutic induction of immunogenic cell death (ICD) in neoplastic cells represents a strategic approach to generate tumor-associated antigens exhibiting enhanced immunostimulatory properties.122 This modality of programmed cellular demise can be elicited through radiation-based interventions, photoactivated therapies, virolytic agents, and specific chemotherapeutic compounds including oxaliplatin, taxanes, and cyclophosphamide.123 Mechanistically, the ICD process generates critical immunostimulatory signals through liberation of key damage-associated molecular patterns (DAMPs), including high mobility group box 1 (HMGB1)124 and extracellular ATP,125 which orchestrate dendritic cell activation through dual mechanisms: facilitating phenotypic maturation via pattern recognition receptor engagement while simultaneously establishing chemotactic gradients for immune cell trafficking.126 Dying tumor cells also expose calreticulin protein on their surface, allowing APCs to capture and present tumor antigens, thus inducing CTL-mediated adaptive immunity.57 In short, ICD serves to reprogram immunosuppressive tumor milieus into immune-responsive neoplastic ecosystems through initiation of regulated cell death cascades, thereby priming a robust immune response to attack tumor cells. Consequently, ICD induction is often employed to initiate potent antitumor immunity in vaccines therapy containing tumor cells.
In the development of whole-cell vaccine platforms for oncological applications, tumor cells can originate from autologous or allogeneic sources. Regardless of their origin, the proliferative capacity of these tumor cells is abrogated, while their immunogenicity is preserved. Autologous tumor cell vaccines are developed using tumor cells derived from patients or tumor models, triggering the endogenous tumor-targeting immunity via synchronized liberation of clonotypic tumor-associated epitopes. For example, autologous tumor cells obtained through surgery undergo ICD to form a tumor cell-based vaccine, which is delivered to a tumor mouse model using a hydrogel constructed from mannan and polyethyleneimine. This hydrogel offers a simple and feasible method of delivering the autologous tumor cell-based vaccine. The vaccine effectively triggers CTLs-mediated immune response to suppress tumor recurrence.127 In addition, hydrogel containing neoplasm-derived vaccine platforms enable remotely triggered antigen liberation spatiotemporally through near-infrared (NIR) laser irradiation, eliciting specific tumor immunity to prevent metastasis and recurrence after tumor surgery.128 NIR laser irradiation, in combination with a photosensitizer, also induces ICD of autologous tumor cells loaded in Fmoc-KCRGDK-functionalized phenylboronic acid hydrogel matrices. The hydrogel achieves biomolecular recognition of malignant cells with overexpressed sialic acid, undergoing thermoresponsive sol-gel phase transition precisely within post-resection tumor niches, thus providing a sustained immune stimulus. This approach further inhibits the relapse of postoperative melanoma and colorectal tumors by generating reactive oxygen species (ROS), optimizing DCs immunocompetence, further expanding tumor-specific CD8+ cytotoxic T lymphocytes.129
Notably, autologous cancer cells undergoing oncolysis (ACCO) can also result in oncolysis immunization against cancer.130 A hydrogel is injected into cavity created by tumor resection, establishing a scaffold, and degrades to release the contained autologous tumor cells. ROS from adjacent trauma sites induces ACCO, enhancing immunogenicity and achieving antitumor immunization, ultimately restraining metastasis and recurrence of tumors.131 Additionally, ACCO vaccines can function as a prophylactic vaccine when delivered to mice in advance using a generalized framework hydrogel. This approach builds enduring and specific immune memory targeting TSAs. When tumors are orthotopically transplanted in the vaccinated mice, the immune status improves, coupled with CD8+ cytotoxic T cells homing to tumor beds increasingly.132
Personalized tumor cells-based vaccines not only utilize autologous tumor cells encapsulated directly by hydrogel in vitro but also apply hydrogel contents to induce tumor cells death in situ in tumor mice, thus facilitating synchronized liberation of intact tumor antigenic payloads. Such in situ tumor vaccines (ITV) are derived from ICD of the primary tumor using hydrogel loaded with DOX. Upon injection in vivo, the hydrogel exhibits ROS-responsive release of DOX, which induces ICD to liberate whole tumor antigens, forming ITV that suppresses malignant cells development through triggering effective anti-tumor immunity.133,134
For allogenic tumor cell-based cancer vaccines, both tumor cells carrying antigens,135 NIR laser irradiation-induced ICD of live mouse breast cancer cells,136 and immunogenically dying tumor cells119 are encapsulated in hydrogel and delivered to the host via a minimally invasive method. The hydrogel’s engineered architecture establishes a protective immunogenic niche for the allogenic tumor cells vaccines and controls the spatiotemporal and sustained release of tumor antigens. These hydrogel-based allogenic tumor cell vaccines have been shown to enhance DCs accumulation, then initiating a vigorous effector T immune response against various cancers.
Tumor Cell Membranes-Based Vaccines
Regarding tumor cells products, tumor cell membranes can be obtained in various ways to construct membranes-based vaccines. Hydrogel decorated with tumor cell membranes, constructed from oxidized sodium alginate (OSA), is subcutaneously injected into breast tumor mice. The decomposition of OSA orchestrates spatiotemporally controlled liberation of tumor-associated antigenic payloads derived from the tumor cell membrane. This effectively promotes DCs maturation, thereby stimulating T-cell-mediated immunity to inhibit tumor relapse.59 Additionally, autologous tumor cell membranes encapsulated in polysaccharide hydrogels, which provide a repertoire of tumor antigens, effectively suppress tumor relapse in the postoperative B16F10 murine model.137 Postoperative tumoral specimens are also used to form vaccines by isolating their tumor cell membranes, which can activate tumor-specific CD8+ cytotoxic T lymphocyte immunity to eradicate malignant cells through thermoresponsive hydrogel-based delivery systems.138 Moreover, mitoxantrone and curcumin are employed to trigger ICD, after which tumor cell membranes are extracted to form membranes-coated vaccines with tumor-specific antigens, such as HPV16 E744-62 peptides. Sodium alginate hydrogel is used to deliver this vaccine, achieving controlled release of a spectrum of tumor antigens from the tumor cell membranes, thus eliciting antitumor immunity and inhibiting the growth of HPV-related tumors.57
Tumor Derived EVs-Based Vaccines
EVs are lipid bilayer-bounded vesicles derived from the endosomal compartment.139 EVs function as sophisticated biomolecular shuttles, encapsulating a diverse repertoire of signaling moieties—including proteomic complexes and nucleic acid species—that undergo intercellular trafficking from source cells to acceptor cell populations.140 Tumor-derived EVs have been found to contribute to tumorigenesis through substance transfer or signaling transduction between cells.141 However, in some cases, tumor-derived EVs can stimulate specific antitumor immunity by providing multiple TAAs and TSAs. Study has reported that tumor-secreted EVs-encapsulated antigens are delivered by bio-adhesive macroporous hydrogels, which can adhere to tissues and recruit immune cells through controlled liberation of antigens and chemokines. This further results in the recruitment of numerous DCs to capture these antigens in situ, then eliciting tumor-specific CD8+T immune response.81
Tumor Cell Lysates-Based Vaccines
Compared to other tumor products, tumor cell lysates provide a broad array of TAAs and TSAs, making them a cost-effective and safe source of tumor antigens.142 A hydrogel vaccine system composed of tumor cell lysates can continuously release these tumor antigens to trigger antitumor immune response. In melanoma-bearing mice, vaccines made from tumor cell lysates encapsulated in hydrogel effectively stimulate DC maturation, thus promoting CTL infiltration at the tumor site.77,143–145 In colon cancer mice model, vaccines formed from tumor cell lysates enhance the activity of CTLs through thermo-responsive hydrogel delivery, thereby suppressing tumor cells growth.60,80 Additionally, tumor cell lysates-based hydrogel vaccines can elicit clonally restricted antitumor immunity for prophylactic suppression of locoregional recurrence and distal metastatic dissemination, when injected at the surgical site in postsurgical mice.146
Currently, tumor cell-based vaccines are more widely used due to their comprehensive tumor antigen repertoire (Figure 3). Moreover, chemotherapy drugs, such as DOX, are often combined with tumor cell-based vaccines to treat cancers. This combinatorial immunotherapeutic platform augments tumor-associated antigen immunogenicity, while concurrently mitigating systemic cytotoxicity inherent to traditional chemotherapeutic regimens. While hydrogel-based platforms offer advantages in spatiotemporal regulation of tumor-associated antigen liberation and augmentation of whole-cell vaccine immunogenicity, existing challenges must be addressed, including the potential for autoimmunity or immunosuppressive effects, as well as the invasive procedure required to obtain autologous tumor cells through tumor biopsies or surgery.
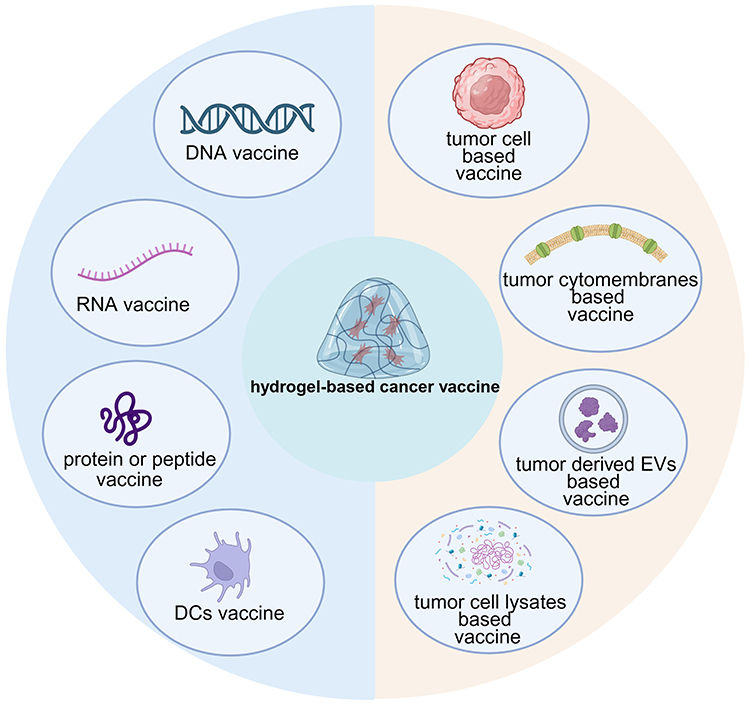 |
Figure 3 Categories of hydrogel-based cancer vaccines. Created in BioRender. Wenqin, Z. (2025) https://BioRender.com/ p0bndby. Abbreviations: DCs, dendritic cells; EVs, extracellular vesicles. |
Overall, hydrogels encapsulating DNA, RNA, proteins or peptides, DCs, or tumor cells combined with immunoadjuvants are widely applied in cancer vaccine research. Each approach has inherent strengths and limitations. A comparison of their specific advantages and disadvantages is summarized in Table 5.
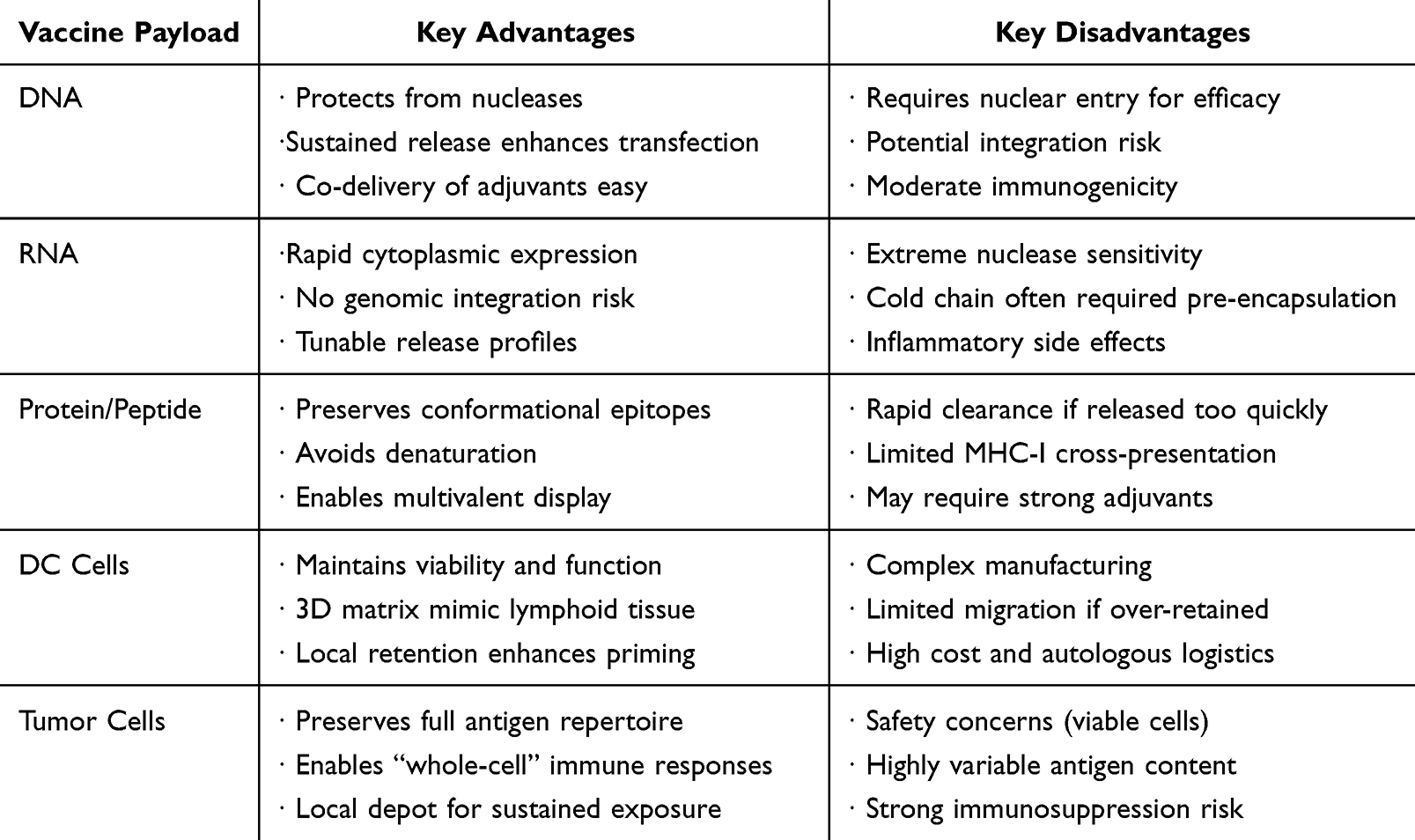 |
Table 5 Comparison of Different Kinds of Hydrogel-Based Cancer Vaccines |
Relevant Tumor Immune Mechanism Mediated by Hydrogel-Based Cancer Vaccines
After being injected into the host through hydrogel delivery, most contemporary cancer vaccines are engineered to orchestrate antitumor immune responses through spatiotemporally controlled liberation of tumor-associated antigens. The efficacy of these cancer vaccines primarily depends on the host’s cellular immunity, particularly the activation of CTL-mediated immunity against tumors. In addition, immune mechanisms regarding other innate, adaptive, and humoral elements have also been found in various studies of hydrogel vaccines-based tumor immunotherapy (Figure 4).
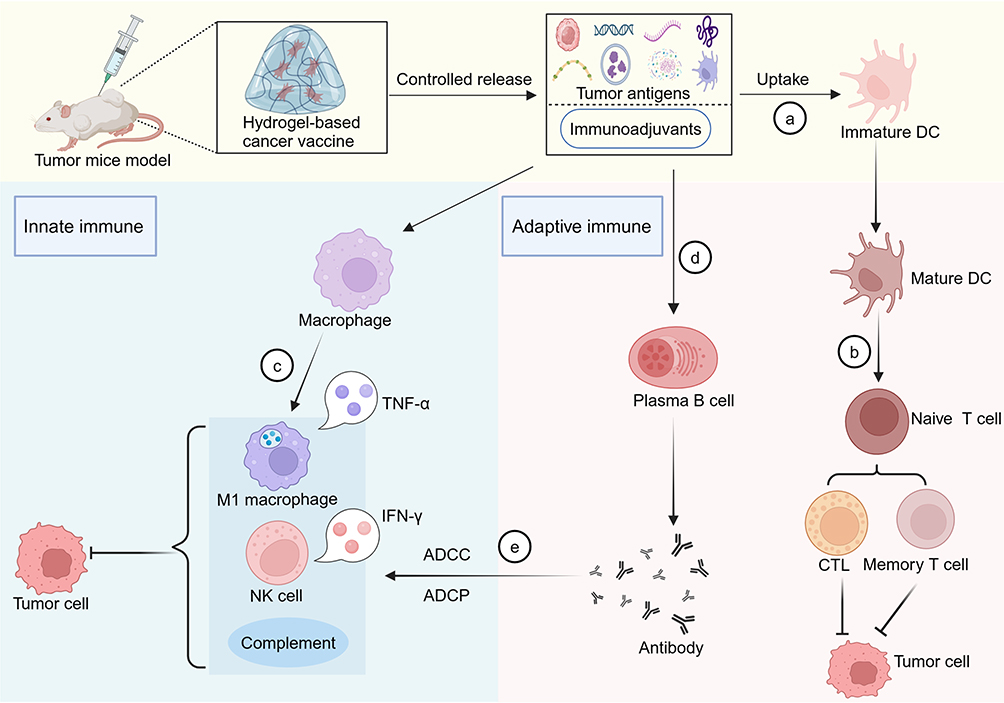 |
Figure 4 Related tumor immune mechanism mediated by hydrogel-based cancer vaccines. Once injected into tumor mice, vaccines constructed by tumor-based antigens like DNA, RNA, protein, tumor cells and immunoadjuvants can be controlled released by hydrogel in vivo. (a) These antigens are absorbed by immature DCs, thus promoting the maturation of DCs. (b) Mature DCs process and present these antigens to naïve T cells, that further boosts the activation of CTLs and memory T cells to attack tumor cells. (c) The release of cancer vaccine encapsulated by hydrogel can stimulate M1 polarization to inhibit tumor cells. (d) The release of tumor-based antigens also stimulates the activation of plasma B cells to secret antibodies. (e) Antibodies produced by humoral immunity can induce ADCC and ADCP of M1, NK cells and complement to kill tumor cells, accompanied by M1 macrophages secreting TNF-α and NK cells secreting IFN-γ. Created in BioRender. Wenqin, Z. (2025) https://BioRender.com/ ydv8muh. Abbreviations: DCs, dendritic cells; CTL, cytotoxic T lymphocytes; NK cell, natural killer cell; TNF-α, tumor necrosis factor α; IFN-γ, interferon-γ; ADCP, antibody-dependent cellular phagocytosis; ADCC, antibody dependent cellular cytotoxicity. |
Activation of DCs
As critical APCs, DCs serve as pivotal immunoregulatory sentinels, orchestrating crosstalk between innate pathogen recognition and adaptive lymphocyte activation. Within adaptive immunity, DCs play an essential role in capturing and presenting tumor antigens and migrating to lymph nodes, thus transmitting antigenic information to naive T cells.147 The establishment of clonally restricted antitumor immunity is contingent upon the complete maturation of DCs and their efficient processing of antigens. Numerous studies have revealed that cancer vaccines can stimulate DC activation, thereby promoting effective anti-tumor immune response through hydrogel delivery. For example, DOX and CpG embedded within a hydrogel enhance tumor antigen uptake by DCs and their maturation through in situ injection.133 Cancer vaccine like Bridge-Vax, when combined with GM-CSF, have been reported to boost DCs activation via hydrogel delivery.137 Tumor EVs and GM-CSF encapsulated in macroporous hydrogels have been found to recruit and activate DCs to capture and present EVs containing antigens.81 In addition, cGAMP nanoparticles-constructed hydrogel, containing STING agonist and ICD inducer, contributes to localized STING pathway activation, thus boosting DCs maturation through STING-IRF3-dependent type I interferon secretion.148 These studies emphasize that DCs activation is crucial in the process of cancer vaccines-induced antitumor immunity.
Activation of Effector or Memory T Cells
Among the antitumor cellular immune response, effector CD8+ T cells function as central cytotoxic effectors, executing tumoricidal activity through secreting granzymes and perforin.149 Peptide like melittin, self-assembling peptide RADA32, tumor lysates, and CpG co-constituted in hydrogel vaccines have been shown to boost CTLs infiltration into TME, thus suppressing tumor growth in melanoma model.143 Resected autologous tumors are used to construct personalized vaccines, such as Angel-Vax, which, when delivered via hydrogel, trigger CTLs-mediated immune response against remaining tumors in mice.127 A nanofibrous trivalent peptide-based hydrogel vaccine has also been reported to amplify CTL immune response, thereby restraining the growth of B16 tumor cells.68
The adaptive immune response induces clonal diversification of naïve CD8+ T cells into effector populations, while concurrently establishing heterogeneous memory T cell compartments to build immune memory. Upon encountering the same tumor stimuli, memory T cells are activated more rapidly and effectively.150 Hydrogel vaccines, such as those based on ACCO and CpG,132 and autologous tumor cells,128 can establish long-lasting and specific immune memory targeting tumor antigens, thereby preventing tumor recurrence and metastasis. DOX, nanoparticles, and immune adjuvants like imiquimod,151 or tumor cell-derived cytomembranes and CpG152 encapsulated in hydrogel also facilitate memory T cells activation. The studies indicate that hydrogel-based cancer vaccines can activate effector or memory T cells to participate in tumor immunity during cancer treatment.
Macrophage Polarization
Macrophages can exert either anti-tumor or pro-tumor functions depending on their activation phenotype. Tumor-associated macrophages (TAMs), predominantly M2-polarized myeloid subsets within the tumor microenvironment (TME), establishes an immunosuppressive circuit, enabling tumor immune evasion and therapeutic resistance.153 TAMs exhibit phenotypic plasticity in response to extrinsic signaling cues, undergoing immunostimulatory reprogramming into pro-inflammatory M1-like macrophages, which exert anti-tumor effects, or alternative M2 macrophages, which promote tumor progression.154 The M2-like properties of TAMs can pose challenges to cancer vaccines. As a result, researchers are focusing on developing cancer vaccines that induce M1 macrophage polarization, enhancing the therapeutic efficacy. For instance, hydrogel loaded with DOX has been shown to trigger ICD of malignant cells, boosting the polarization of M1-like phenotypes in situ vaccination in tumor models.134,155 BCG lysates encapsulated in hydrogel also induce M1 macrophage polarization when injected near tumors in melanoma model.87 A DC vaccine based on CaCO3 biomineralized hydrogel has been shown to facilitate M1 macrophage polarization to reverse the suppressive TME.118 These studies indicate that various types of cancer vaccines embedded in hydrogel have the potential to improve the suppressive TME by inducing M1 macrophage polarization.
Humoral Immunity
Some studies suggest that cancer vaccines not only activate the host’s cellular immunity but also participate in humoral immunity to achieve therapeutic efficacy.156 Humoral immunity mainly involves antibody-mediated B cells immune response. Tumor-bearing hosts can produce antibodies targeting multiple tumor antigens.157 A self-assembling D-tetra-OVA encapsulated in hydrogel has demonstrate spatiotemporally controlled humoral immunomodulation in vivo.158 Co-assembled peptides and antigens embedded in hydrogels were found to boost antibody generation.112 OVA expressing plasmid and GM-CSF encapsulated in hydrogel can induce OVA antibody production to eradicate melanoma.94 These studies demonstrate that self-assembling peptides and protein antigen delivered by hydrogel can also induce antibody production in established tumor models. These antibodies may execute tumoricidal activity through polyfunctional mechanisms, such as complement production, ADCP, or ADCC.
Innate and Adaptive Immune
While antitumor immunity mainly refers to adaptive T cell-mediated immunity, the initiation, coordination, and perpetuation of these responses also require the involvement of innate immune cells.159 Innate immune cells DCs, macrophages and monocytes, serve as primary immunologic gatekeepers, encountering external antigens and transfers them to T cells, thereby eliciting adaptive immunity. Simultaneously, innate immune cells are capable of initiating self-immune response such as ADCP and ADCC.160 These mechanisms mediate target cell elimination and pathogen clearance through cytolytic activity and cellular engulfment executed by innate immunologic sentinels, including NK cells and macrophages. Multifunctional vaccines, such as NOCC-CpG/OX-M based on hydrogel, promote M1 polarization through ADCP and ADCC, activating a cascade of myeloid-driven immunostimulation that licenses neoantigen-specific CTL clonal expansion via DC-mediated cross-presentation.161 Besides, cytokines like IL-6 and GM-CSF also enhance innate immunity, thus priming the host’s adaptive immunity. Li et al reported that HPV E7 peptide and the immunomodulatory agent β-glucan encapsulated in hydrogel can drive the production of myeloid-derived proinflammatory mediators (IL-1β, TNF-α, IL-6) that license DCs immunogenic maturation, thus improving the specific anti-tumor adaptive T cell response.162
Collectively, hydrogel-based delivery significantly enhances cancer vaccine efficacy by amplifying immune responses compared to non-hydrogel counterparts. Key advantages are detailed Table 6.
 |
Table 6 Comparison Between Hydrogel and Non-Hydrogel-Based Cancer Vaccines |
Conclusions and Future Remarks
The comprehensive analysis describes the characteristics of physicochemical and immunomodulatory attributes of oncovaccines and polymeric hydrogel networks, providing an overview of current types of hydrogel-based cancer vaccines, finally summarizing the relevant anti-tumor immune mechanisms involved in cancer vaccines therapy. In general, hydrogels mimic the extracellular matrix, offering excellent biocompatibility as a delivery carrier. Vaccination of hydrogel-based cancer vaccines achieves a minimally invasive strategy for in vivo tumor treatment, even allowing in situ administration at tumor sites. Injectable hydrogels maintain the structure and properties of cancer vaccines, protecting them from degradation in vivo. Coupled with various immunoadjuvants, the immunogenicity of cancer vaccines is significantly enhanced, thus triggering potent antitumor immunity. Furthermore, the controlled spatiotemporal release of vaccines components by hydrogels ensures sustained stimuli for prolonged antitumor immune response, eliminating the need for repeated injections of cancer vaccines. Prophylactic and therapeutic cancer vaccines, delivered effectively via hydrogels, can prime tumor-targeted adaptive immunity, ultimately suppressing primary tumor progression, postsurgical neoplastic resurgence, and distal metastatic dissemination in tumor-bearing model. To optimize the efficacy of tumor antigen-based vaccines, chemotherapeutic drugs such as DOX, cyclophosphamide, taxol, or immune checkpoint inhibitors (ICI) like anti-PD-L1and anti-CTLA4 antibodies are often integrated into hydrogel-based cancer vaccines.133,144,163,164 Such combined application of these therapeutic strategies improves the outcomes of tumor treatment.58 In conclusion, bioengineered hydrogel scaffolds containing cancer vaccines show significant promise as a potential tool in precision immuno-oncology.
The design of hydrogel-based cancer vaccines demands precise engineering of physicochemical architecture, as elements including polymer composition, porosity, and mechanical properties critically govern immune cell recruitment, activation, and spatial distribution. The choice of polymeric constituents-including HA, alginate, PEG or polypeptide derivatives-governs biocompatibility, degradation kinetics, and ligand presentation. Natural polymers such as HA contain endogenous CD44-binding motifs that facilitate DCs adhesion and TLR-mediated activation.165 Synthetic alternatives like PEG-acrylate166 enable modular conjugation of peptide antigens or immunostimulants (eg, CpG-ODN). Critically, polymer hydrophilicity and surface charge determine protein adsorption patterns, thereby modulating antigen retention and bioavailability. Cationic hydrogels preferentially adsorb negatively charged nucleic acid adjuvants, potentiating STING or TLR9 signaling in APCs.167 Pore architecture critically regulates cellular infiltration and mass transport dynamics. Macropores (>50um) enable rapid recruitment of DCs, macrophages, and lymphocytes, whereas interconnected nanopores (10–100 nm) sustain prolonged elution of tumor antigens and cytokines.168 This structural hierarchy synergizes with payload kinetics to determine immune response quality. Future iterations should prioritize in vivo-degradable polymers featuring tunable viscoelasticity and heterotypic porosity to orchestrate sequential immunity: rapid innate cell recruitment, efficient antigen presentation, and durable effector T-cell memory.
The clinical translation of hydrogel vaccines confronts significant scalability challenges in manufacturing, storage stability, and distribution logistics. Production limitations include batch-to-batch crosslinking variability compromising antigen loading efficiency and sterilization-induced degradation of thermosensitive immunomodulators.169 Solutions may encompass continuous microfluidic fabrication with real-time rheological monitoring, aseptic photoinitiated click chemistry, and lyophilization maintaining >95% bioactivity. Storage/transport barriers stem from temperature-dependent structural collapse,170 evidenced by 40–60% reduced swelling ratios and >30% antigen leakage during freeze-thaw cycles, which may be addressed through trehalose-based cryoprotection, thermo-responsive solid-state formulations, and passively cooled smart packaging. Economically, while production costs exceed traditional platforms, hydrogel vaccines demonstrate compelling value via 85–92% cold chain reduction, 3–5 times antigen retention enabling 40% fewer boosters, and 4–7% wastage rates versus 18–50% for cold chain-dependent alternatives.171 Their 24-month ambient stability contrasts sharply with conventional vaccines’ 3-6-month refrigerated shelf life, achieving reductions of distribution cost in resource-limited regions.172 Consequently, despite higher initial costs, hydrogel platforms enable transformative decentralized vaccination with amplified economic advantages during pandemics and for thermolabile biotherapeutics. Hydrogel vaccines enable a transformative shift toward thermostable, decentralized immunization. Scalable clinical translation hinges on overcoming manufacturing constraints via continuous production and stabilized dry-state architectures. Economic validation confirms viability across high-value oncology applications and global health settings where cold chain dependencies limit vaccine access.
Acknowledgments
This study was supported by grants from the Project of Changsha Natural Science Foundation (kq2502299), the Natural Science Foundation of Hunan Province (2024JJ5560, 2024JJ9523), and the Tai’an Science and Technology Innovation Development Project (Policy Guidance Category) Project No. 2023NS255. The graphical abstract Created in BioRender. Wenqin, Z. (2025) https://BioRender.com/ avrw531.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that this paper was conducted without any financial or business relationship that could be considered as a potential conflict of interest.
References
1. Dhiman A, Sharma R, Singh RK. Target-based anticancer indole derivatives and insight into structure‒activity relationship: a mechanistic review update (2018-2021). Acta Pharmaceutica Sinica B. 2022;12(7):3006–3027. doi:10.1016/j.apsb.2022.03.021
2. Tsimberidou AM, Fountzilas E, Nikanjam M, Kurzrock R. Review of precision cancer medicine: evolution of the treatment paradigm. Cancer Treatment Rev. 2020;86:102019. doi:10.1016/j.ctrv.2020.102019
3. Cercek A, Csd R, Strombom P, et al. Adoption of total neoadjuvant therapy for locally advanced rectal cancer. JAMA Oncol. 2018;4(6):e180071. doi:10.1001/jamaoncol.2018.0071
4. Liu M, Xie D, Hu D, et al. In situ cocktail nanovaccine for cancer immunotherapy. Adv Sci. 2023;10(31):e2207697. doi:10.1002/advs.202207697
5. Gotwals P, Cameron S, Cipolletta D, et al. Prospects for combining targeted and conventional cancer therapy with immunotherapy. Nat Rev Cancer. 2017;17(5):286–301. doi:10.1038/nrc.2017.17
6. Couzin-Frankel J. Breakthrough of the year 2013. Cancer immunotherapy. Science. 2013;342(6165):1432–1433. doi:10.1126/science.342.6165.1432
7. Quesada JR, Hersh EM, Manning J, et al. Treatment of hairy cell leukemia with recombinant alpha-interferon. Blood. 1986;68(2):493–497. doi:10.1182/blood.V68.2.493.493
8. Riley RS, June CH, Langer R, Mitchell MJ. Delivery technologies for cancer immunotherapy. Nat Rev Drug Discovery. 2019;18(3):175–196. doi:10.1038/s41573-018-0006-z
9. Cai L, Li Y, Tan J, Xu L, Li Y. Targeting LAG-3, TIM-3, and TIGIT for cancer immunotherapy. J Hematol Oncol. 2023;16(1):101. doi:10.1186/s13045-023-01499-1
10. Yang L, Feng Y, Liu X, et al. DYNC2H1 mutation as a potential predictive biomarker for immune checkpoint inhibitor efficacy in NSCLC and melanoma. Investig New Drugs. 2025;43:199–213. doi:10.1007/s10637-024-01495-3
11. Liu Y, Yan Q, Zeng Z, Fan C, Xiong W. Advances and prospects of mRNA vaccines in cancer immunotherapy. Biochimica Et Biophysica Acta Reviews on Cancer. 2024;1879(2):189068. doi:10.1016/j.bbcan.2023.189068
12. Pan H, Liu P, Zhao L, et al. Immunogenic cell stress and death in the treatment of cancer. Sem Cell Develop Biol. 2024;156:11–21. doi:10.1016/j.semcdb.2023.10.007
13. Pw K, Cs H, Nd S, et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. New Eng J Med. 2010;363(5):411–422. doi:10.1056/NEJMoa1001294
14. Furukawa J, Kakei Y, Murakami S, et al. Safety and efficacy of oral cancer vaccine B440 in patients with PD-1/PD-L1 inhibitor-resistant advanced urothelial cancer: a study protocol for a Phase 1 multicenter, open-label, single-arm clinical trial. BMC Cancer. 2025;25(1):195. doi:10.1186/s12885-025-13514-4
15. Yang J, Hong W, Shi H, et al. Trivalent recombinant protein vaccine induces cross-neutralization against XBB lineage and JN.1 subvariants: preclinical and phase 1 clinical trials. Nat Commun. 2024;15(1):10778. doi:10.1038/s41467-024-55087-z
16. van der Burg SH. Correlates of immune and clinical activity of novel cancer vaccines. Sem Immunol. 2018;39:119–136. doi:10.1016/j.smim.2018.04.001
17. Ji P, Sun W, Zhang S, et al. Modular Hydrogel Vaccine for Programmable and Coordinate Elicitation of Cancer Immunotherapy. Adv Sci. 2023;10(22):e2301789. doi:10.1002/advs.202301789
18. Bouzid R, Peppelenbosch M, Buschow SI. Opportunities for conventional and in situ cancer vaccine strategies and combination with immunotherapy for gastrointestinal cancers, a review. Cancers. 2020;12(5):1121. doi:10.3390/cancers12051121
19. Wang EY, Sarmadi M, Ying B, Jaklenec A, Langer R. Recent advances in nano- and micro-scale carrier systems for controlled delivery of vaccines. Biomaterials. 2023;303:122345. doi:10.1016/j.biomaterials.2023.122345
20. Vázquez-González M, Willner I. Stimuli-responsive biomolecule-based hydrogels and their applications. Angewandte Chemie. 2020;59(36):15342–15377. doi:10.1002/anie.201907670
21. Zhong R, Talebian S, Mendes BB, et al. Hydrogels for RNA delivery. Nat Mat. 2023;22(7):818–831. doi:10.1038/s41563-023-01472-w
22. Correa S, Grosskopf AK, Lopez Hernandez H, et al. Translational Applications of Hydrogels. Chem Rev. 2021;121(18):11385–11457. doi:10.1021/acs.chemrev.0c01177
23. Falcone N, Ermis M, Dg T, et al. Peptide hydrogels as immunomaterials and their use in cancer immunotherapy delivery. Adv Healthcare Mat. 2023;12(27):e2301096. doi:10.1002/adhm.202301096
24. Lei L, Huang D, Gao H, He B, Cao J, Peppas NA. Hydrogel-guided strategies to stimulate an effective immune response for vaccine-based cancer immunotherapy. Sci Adv. 2022;8(47):eadc8738. doi:10.1126/sciadv.adc8738
25. Huang P, Wang X, Liang X, et al. Nano-, micro-, and macroscale drug delivery systems for cancer immunotherapy. Acta biomaterialia. 2019;85:1–26. doi:10.1016/j.actbio.2018.12.028
26. Stanley M. Tumour virus vaccines: hepatitis B virus and human papillomavirus. Phil Transactions Royal Soc London Series B Biol Sci. 2017;372(1732). doi:10.1098/rstb.2016.0268
27. Galanis E, Ke D, Keith AS, et al. Carcinoembryonic antigen-expressing oncolytic measles virus derivative in recurrent glioblastoma: a phase 1 trial. Nat Commun. 2024;15(1):493. doi:10.1038/s41467-023-43076-7
28. Vienot A, Jacquin M, Rebucci-Peixoto M, et al. Evaluation of the interest to combine a CD4 Th1-inducer cancer vaccine derived from telomerase and atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma: a randomized non-comparative Phase II study (TERTIO - PRODIGE 82). BMC Cancer. 2023;23(1):710. doi:10.1186/s12885-023-11065-0
29. Naoe T, Saito A, Hosono N, et al. Immunoreactivity to WT1 peptide vaccine is associated with prognosis in elderly patients with acute myeloid leukemia: follow-up study of randomized phase II trial of OCV-501, an HLA class II-binding WT1 polypeptide. Cancer Immunol Immunother. 2023;72(8):2865–2871. doi:10.1007/s00262-023-03432-4
30. McNeel DG, Emamekhoo H, Eickhoff JC, et al. Phase 2 trial of a DNA vaccine (pTVG-HP) and nivolumab in patients with castration-sensitive non-metastatic (M0) prostate cancer. J Immunother Cancer. 2023;11(12):e008067. doi:10.1136/jitc-2023-008067
31. Dj C, Shah N, Wu J, et al. Randomized phase II trial of dendritic cell/myeloma fusion vaccine with lenalidomide maintenance after upfront autologous hematopoietic cell transplantation for multiple myeloma: BMT CTN 1401. Clin Cancer Res. 2023;29(23):4784–4796. doi:10.1158/1078-0432.CCR-23-0235
32. Ishihara M, Nishida Y, Kitano S, et al. A phase 1 trial of NY-ESO-1-specific TCR-engineered T-cell therapy combined with a lymph node-targeting nanoparticulate peptide vaccine for the treatment of advanced soft tissue sarcoma. Int J Cancer. 2023;152(12):2554–2566. doi:10.1002/ijc.34453
33. Dasyam N, Kj S, Barrow C, et al. A randomised controlled trial of long NY-ESO-1 peptide-pulsed autologous dendritic cells with or without alpha-galactosylceramide in high-risk melanoma. Cancer Immunol Immunother. 2023;72(7):2267–2282. doi:10.1007/s00262-023-03400-y
34. Thirumalaikumar E, Vimal S, Sathishkumar R, et al. DNA vaccine incorporated poly (lactic-co-glycolic) acid (PLGA) microspheres offer enhanced protection against Aeromonas hydrophila infection. Int J Biol Macromol. 2023;253(Pt 5):127182. doi:10.1016/j.ijbiomac.2023.127182
35. Chen S, Tan Z, Liao P, et al. Biodegradable microrobots for DNA VACCINE DELIvery. Adv Healthcare Mat. 2023;12(21):e2202921. doi:10.1002/adhm.202202921
36. Lu Y, Wu F, Duan W, et al. Engineering a “PEG-g-PEI/DNA nanoparticle-in- PLGA microsphere” hybrid controlled release system to enhance immunogenicity of DNA vaccine. Mat Sci Eng C Mat Biol Appl. 2020;106:110294. doi:10.1016/j.msec.2019.110294
37. Malla R, Srilatha M, Farran B, Nagaraju GP. mRNA vaccines and their delivery strategies: a journey from infectious diseases to cancer. Mol Ther. 2024;32(1):13–31. doi:10.1016/j.ymthe.2023.10.024
38. Saxena M, van der Burg SH, Melief CJM, Bhardwaj N. Therapeutic cancer vaccines. Nat Rev Cancer. 2021;21(6):360–378.
39. Chen DS, Mellman I. Oncology meets immunology: the cancer-immunity cycle. Immunity. 2013;39(1):1–10. doi:10.1016/j.immuni.2013.07.012
40. Li Y, Yang HY, Lee DS. Advances in biodegradable and injectable hydrogels for biomedical applications. J Controlled Release. 2021;330:151–160. doi:10.1016/j.jconrel.2020.12.008
41. Adu-Berchie K, Mooney DJ. Biomaterials as local niches for immunomodulation. Accounts Chem Res. 2020;53(9):1749–1760. doi:10.1021/acs.accounts.0c00341
42. Zhang D, Sun P, Li P, et al. A magnetic chitosan hydrogel for sustained and prolonged delivery of Bacillus Calmette-Guérin in the treatment of bladder cancer. Biomaterials. 2013;34(38):10258–10266. doi:10.1016/j.biomaterials.2013.09.027
43. Liu X, Feng Z, Wang C, et al. Co-localized delivery of nanomedicine and nanovaccine augments the postoperative cancer immunotherapy by amplifying T-cell responses. Biomaterials. 2020;230:119649. doi:10.1016/j.biomaterials.2019.119649
44. Yuan J, Sun W, Zhang Z, et al. 5-Fluorouracil/curcumin loaded silk fibroin hydrogel for the adjuvant therapy in colorectal cancer. Biomat Adv. 2025;168:214108. doi:10.1016/j.bioadv.2024.214108
45. Wang J, Yu N, Tang Y, Cheng Y, Li H. FDA-approved hydrogel-mediated in situ sonodynamic and chemotherapeutic therapy for pancreatic cancer. Pharmaceuticals. 2024;17(12):1666. doi:10.3390/ph17121666
46. Bobbala S, Tamboli V, McDowell A, Mitra AK, Hook S. Novel injectable pentablock copolymer based thermoresponsive hydrogels for sustained release vaccines. AAPS J. 2016;18(1):261–269. doi:10.1208/s12248-015-9843-4
47. Rocha CV, Gonçalves V, da Silva MC, Bañobre-López M, Gallo J. PLGA-based composites for various biomedical applications. Int J Mol Sci. 2022;23(4):2034. doi:10.3390/ijms23042034
48. Gurunathan S, Thangaraj P, Wang L, Cao Q, Kim JH. Nanovaccines: an effective therapeutic approach for cancer therapy. Biomed Pharmacother Biomed Pharmacother. 2024;170:115992.
49. Zhang M, Chen W, Ju Y, Zhao H, Wang C. Polymer-protein nanovaccine synthesized via reactive self-assembly with potential application in cancer immunotherapy: physicochemical and biological characterization in vitro and in vivo. Macromol Rapid Commun. 2023;44(23):e2300438. doi:10.1002/marc.202300438
50. Nkanga CI, Steinmetz NF. Injectable hydrogel containing cowpea mosaic virus nanoparticles prevents colon cancer growth. ACS Biomat Sci Eng. 2022;8(6):2518–2525. doi:10.1021/acsbiomaterials.2c00284
51. El M, Jh K, Ck J, et al. Generation of an inflammatory niche in a hydrogel depot through recruitment of key immune cells improves efficacy of mRNA vaccines. Sci Adv. 2025;11(15):eadr2631. doi:10.1126/sciadv.adr2631
52. Zheng P, He J, Yang Z, et al. Neoantigen-based nanovaccine in combination with immune checkpoint inhibitors abolish postsurgical tumor recurrence and metastasis. Small. 2023;19(50):e2302922. doi:10.1002/smll.202302922
53. Wang F, Xie M, Huang Y, et al. In Situ vaccination with an injectable nucleic acid hydrogel for synergistic cancer immunotherapy. Angewandte Chemie. 2024;63(4):e202315282. doi:10.1002/anie.202315282
54. Cui R, Wu Q, Wang J, et al. Hydrogel-by-design: smart delivery system for cancer immunotherapy. Front Bioeng Biotechnol. 2021;9:723490. doi:10.3389/fbioe.2021.723490
55. Umeki Y, Saito M, Kusamori K, et al. Combined encapsulation of a tumor antigen and immune cells using a self-assembling immunostimulatory DNA hydrogel to enhance antigen-specific tumor immunity. J Controlled Release. 2018;288:189–198. doi:10.1016/j.jconrel.2018.09.007
56. Luo R, Wan Y, Liu G, et al. Engineering self-assembling peptide hydrogel to enhance the capacity of dendritic cells to activate in vivo T-cell immunity. Biomacromolecules. 2024;25:1408–1428. doi:10.1021/acs.biomac.3c00511
57. Liu Q, Hu Y, Zheng P, et al. Exploiting immunostimulatory mechanisms of immunogenic cell death to develop membrane-encapsulated nanoparticles as a potent tumor vaccine. J Nanobiotechnol. 2023;21(1):326. doi:10.1186/s12951-023-02031-w
58. Long W, Li S, Yang Y, et al. Self-cross-linked chitosan/albumin-bound nanoparticle hydrogel for inhibition of postsurgery malignant glioma recurrence. ACS Appl Mat Interfaces. 2023. doi:10.1021/acsami.3c12873
59. Nie X, Shi C, Chen X, et al. A single-shot prophylactic tumor vaccine enabled by an injectable biomembrane hydrogel. Acta biomaterialia. 2023;169:306–316. doi:10.1016/j.actbio.2023.08.010
60. Yang Y, Wang N, Tian X, et al. Synergy of polydopamine nanovaccine and endostar alginate hydrogel for improving antitumor immune responses against colon tumor. Int J Nanomed. 2022;17:4791–4805. doi:10.2147/IJN.S372048
61. Yoshizaki Y, Horii K, Murase N, Kuzuya A, Ohya Y. Development of immune cell delivery system using biodegradable injectable polymers for cancer immunotherapy. Int J Pharmaceut. 2024;652:123801. doi:10.1016/j.ijpharm.2024.123801
62. Maiti S, Maji B, Yadav H. Progress on green crosslinking of polysaccharide hydrogels for drug delivery and tissue engineering applications. Carbohydrate Polymers. 2024;326:121584. doi:10.1016/j.carbpol.2023.121584
63. Wang Y, Wang Z, Lu W, Hu Y. Review on chitosan-based antibacterial hydrogels: preparation, mechanisms, and applications. Int J Biol Macromol. 2024;255:128080. doi:10.1016/j.ijbiomac.2023.128080
64. Euliano EM, Pogostin BH, Agrawal A, et al. A TLR7 agonist conjugated to a nanofibrous peptide hydrogel as a potent vaccine adjuvant. Adv Healthcare Mat. 2025;14(3):e2402958. doi:10.1002/adhm.202402958
65. Hirobe S, Matsuo K, Quan YS, et al. Clinical study of transcutaneous vaccination using a hydrogel patch for tetanus and diphtheria. Vaccine. 2012;30(10):1847–1854. doi:10.1016/j.vaccine.2011.12.130
66. Neimert-Andersson T, Binnmyr J, Enoksson M, et al. Evaluation of safety and efficacy as an adjuvant for the chitosan-based vaccine delivery vehicle ViscoGel in a single-blind randomised Phase I/IIa clinical trial. Vaccine. 2014;32(45):5967–5974. doi:10.1016/j.vaccine.2014.08.057
67. Sinad KVG, Ebubechukwu RC, Chu CK. Recent advances in double network hydrogels based on naturally-derived polymers: synthesis, properties, and biological applications. J Mat Chem B. 2023;11(48):11460–11482. doi:10.1039/D3TB00773A
68. Song H, Su Q, Nie Y, et al. Supramolecular assembly of a trivalent peptide hydrogel vaccine for cancer immunotherapy. Acta biomaterialia. 2023;158:535–546. doi:10.1016/j.actbio.2022.12.070
69. Li J, Mooney DJ. Designing hydrogels for controlled drug delivery. Nat Rev Mat. 2016;1(12). doi:10.1038/natrevmats.2016.71
70. Liu T, Si X, Liu L, et al. Injectable nano-in-gel vaccine for spatial and temporal control of vaccine kinetics and breast cancer postsurgical therapy. ACS Nano. 2024;18(4):3087–3100. doi:10.1021/acsnano.3c08376
71. Gao C, Cheng K, Li Y, et al. Injectable immunotherapeutic hydrogel containing RNA-loaded lipid nanoparticles reshapes tumor microenvironment for pancreatic cancer therapy. Nano Lett. 2022;22(22):8801–8809. doi:10.1021/acs.nanolett.2c01994
72. Smith CC, Selitsky SR, Chai S, Armistead PM, Vincent BG, Serody JS. Alternative tumour-specific antigens. Nat Rev Cancer. 2019;19(8):465–478. doi:10.1038/s41568-019-0162-4
73. Hu Z, Ott PA, Wu CJ. Towards personalized, tumour-specific, therapeutic vaccines for cancer. Nat Rev Immunol. 2018;18(3):168–182. doi:10.1038/nri.2017.131
74. Wagner S, Mullins CS, Linnebacher M. Colorectal cancer vaccines: tumor-associated antigens vs neoantigens. World J Gastroenterol. 2018;24(48):5418–5432. doi:10.3748/wjg.v24.i48.5418
75. Picard E, Verschoor CP, Ma GW, Pawelec G. Relationships between immune landscapes, genetic subtypes and responses to immunotherapy in colorectal cancer. Front Immunol. 2020;11:369. doi:10.3389/fimmu.2020.00369
76. Lemdani K, Seguin J, Lesieur C, et al. Mucoadhesive thermosensitive hydrogel for the intra-tumoral delivery of immunomodulatory agents, in vivo evidence of adhesion by means of non-invasive imaging techniques. Int J Pharmaceut. 2019;567:118421. doi:10.1016/j.ijpharm.2019.06.012
77. Song H, Huang P, Niu J, et al. Injectable polypeptide hydrogel for dual-delivery of antigen and TLR3 agonist to modulate dendritic cells in vivo and enhance potent cytotoxic T-lymphocyte response against melanoma. Biomaterials. 2018;159:119–129. doi:10.1016/j.biomaterials.2018.01.004
78. Shi HS, Gong CY, Zhang HL, et al. Novel vaccine adjuvant LPS-Hydrogel for truncated basic fibroblast growth factor to induce antitumor immunity. Carbohydrate Polymers. 2012;89(4):1101–1109. doi:10.1016/j.carbpol.2012.03.073
79. Stickdorn J, Stein L, Arnold-Schild D, et al. Systemically administered TLR7/8 agonist and antigen-conjugated nanogels govern immune responses against tumors. ACS Nano. 2022;16(3):4426–4443. doi:10.1021/acsnano.1c10709
80. Yang F, Shi K, Hao Y, et al. Cyclophosphamide loaded thermo-responsive hydrogel system synergize with a hydrogel cancer vaccine to amplify cancer immunotherapy in a prime-boost manner. Bioactive Mat. 2021;6(10):3036–3048. doi:10.1016/j.bioactmat.2021.03.003
81. Han J, Bhatta R, Wang H. Bio-adhesive macroporous hydrogels for in situ recruitment and modulation of dendritic cells. Cell Mol Bioeng. 2023;16(4):355–367. doi:10.1007/s12195-023-00770-2
82. Meng F, Li L, Lin Z, et al. Biosynthetic neoantigen displayed on bacteria derived vesicles elicit systemic antitumour immunity. J Extracellular Vesicles. 2022;11(12):e12289. doi:10.1002/jev2.12289
83. Oh E, Oh JE, Hong J, et al. Optimized biodegradable polymeric reservoir-mediated local and sustained co-delivery of dendritic cells and oncolytic adenovirus co-expressing IL-12 and GM-CSF for cancer immunotherapy. J Controlled Release. 2017;259:115–127. doi:10.1016/j.jconrel.2017.03.028
84. Hori Y, Stern PJ, Hynes RO, Irvine DJ. Engulfing tumors with synthetic extracellular matrices for cancer immunotherapy. Biomaterials. 2009;30(35):6757–6767. doi:10.1016/j.biomaterials.2009.08.037
85. Fenton OS, Tibbitt MW, Appel EA, Jhunjhunwala S, Webber MJ, Langer R. Injectable polymer-nanoparticle hydrogels for local immune cell recruitment. Biomacromolecules. 2019;20(12):4430–4436. doi:10.1021/acs.biomac.9b01129
86. Liu X, Zhuang Y, Huang W, et al. Interventional hydrogel microsphere vaccine as an immune amplifier for activated antitumour immunity after ablation therapy. Nat Commun. 2023;14(1):4106. doi:10.1038/s41467-023-39759-w
87. Kremenovic M, Chan AA, Feng B, et al. BCG hydrogel promotes CTSS-mediated antigen processing and presentation, thereby suppressing metastasis and prolonging survival in melanoma. J Immunother Cancer. 2022;10(6):e004133. doi:10.1136/jitc-2021-004133
88. Zheng B, Peng W, Gan L, et al. Sendai virus-based immunoadjuvant in hydrogel vaccine intensity-modulated dendritic cells activation for suppressing tumorigenesis. Bioactive Mat. 2021;6(11):3879–3891. doi:10.1016/j.bioactmat.2021.04.002
89. Marin A, Chowdhury A, Valencia SM, et al. Next generation polyphosphazene immunoadjuvant: synthesis, self-assembly and in vivo potency with human papillomavirus VLPs-based vaccine. Nanomed. 2021;33:102359. doi:10.1016/j.nano.2021.102359
90. Han HD, Song CK, Park YS, et al. A chitosan hydrogel-based cancer drug delivery system exhibits synergistic antitumor effects by combining with a vaccinia viral vaccine. Int J Pharmaceut. 2008;350(1–2):27–34. doi:10.1016/j.ijpharm.2007.08.014
91. Yang Y, Hu Y, Yang Y, et al. Tumor vaccine exploiting membranes with influenza virus-induced immunogenic cell death to decorate polylactic coglycolic acid nanoparticles. ACS Nano. 2025;19(3):3115–3134. doi:10.1021/acsnano.4c00654
92. Alford A, Tucker B, Kozlovskaya V, et al. Encapsulation and ultrasound-triggered release of G-Quadruplex DNA in multilayer hydrogel microcapsules. Polymers. 2018;10(12):1342. doi:10.3390/polym10121342
93. Singh A, Qin H, Fernandez I, et al. An injectable synthetic immune-priming center mediates efficient T-cell class switching and T-helper 1 response against B cell lymphoma. J Controlled Release. 2011;155(2):184–192. doi:10.1016/j.jconrel.2011.06.008
94. Duong HTT, Thambi T, Yin Y, et al. Degradation-regulated architecture of injectable smart hydrogels enhances humoral immune response and potentiates antitumor activity in human lung carcinoma. Biomaterials. 2020;230:119599. doi:10.1016/j.biomaterials.2019.119599
95. Imani S, Tagit O, Pichon C. Neoantigen vaccine nanoformulations based on chemically synthesized minimal mRNA (CmRNA): small molecules, big impact. NPJ Vaccines. 2024;9(1):14. doi:10.1038/s41541-024-00807-1
96. Liu MA. A comparison of plasmid DNA and mRNA as vaccine technologies. Vaccines. 2019;7(2):37. doi:10.3390/vaccines7020037
97. Athirasala A, Patel S, Menezes PP, et al. Matrix stiffness regulates lipid nanoparticle-mRNA delivery in cell-laden hydrogels. Nanomedicine. 2022;42:102550. doi:10.1016/j.nano.2022.102550
98. Yin Y, Li X, Ma H, et al. In situ transforming RNA nanovaccines from polyethylenimine functionalized graphene oxide hydrogel for durable cancer immunotherapy. Nano Lett. 2021;21(5):2224–2231. doi:10.1021/acs.nanolett.0c05039
99. Wang W, Liu X, Ding L, Jin HJ, Li X. RNA hydrogel combined with MnO(2) nanoparticles as a nano-vaccine to treat triple negative breast cancer. Front Chem. 2021;9:797094. doi:10.3389/fchem.2021.797094
100. Meng Z, Zhang Y, She J, et al. Ultrasound-mediated remotely controlled nanovaccine delivery for tumor vaccination and individualized cancer immunotherapy. Nano Lett. 2021;21(3):1228–1237. doi:10.1021/acs.nanolett.0c03646
101. Lee ALZ, Yang C, Gao S, Hedrick JL, Yang YY. Subcutaneous vaccination using injectable biodegradable hydrogels for long-term immune response. Nanomedicine. 2019;21:102056. doi:10.1016/j.nano.2019.102056
102. Wang Z, Liang C, Shi F, et al. Cancer vaccines using supramolecular hydrogels of NSAID-modified peptides as adjuvants abolish tumorigenesis. Nanoscale. 2017;9(37):14058–14064. doi:10.1039/C7NR04990K
103. DeMaria PJ, Bilusic M. Cancer Vaccines. Hematology/Oncol Clin North Am. 2019;33(2):199–214. doi:10.1016/j.hoc.2018.12.001
104. Ta T, Yh K, Ge K, et al. The long multi-epitope peptide vaccine combined with adjuvants improved the therapeutic effects in a glioblastoma mouse model. Front Immunol. 2022;13:1007285. doi:10.3389/fimmu.2022.1007285
105. Panya A, Thepmalee C, Sawasdee N, Saengmuang S, Luangwattananun P, Yenchitsomanus PT. Enhancing cholangiocarcinoma immunotherapy with adoptive T cells targeting HLA-restricted neoantigen peptides derived from driver gene mutations. Biomed Pharmacother Biomed Pharmacother. 2023;168:115827. doi:10.1016/j.biopha.2023.115827
106. Yu Z, Xu Y, Yao H, et al. A simple and general strategy for postsurgical personalized cancer vaccine therapy based on an injectable dynamic covalent hydrogel. Biomat Sci. 2021;9(20):6879–6888. doi:10.1039/D1BM01000J
107. Khazaei S, Varela-Calviño R, Rad-Malekshahi M, et al. Self-assembled peptide/polymer hybrid nanoplatform for cancer immunostimulating therapies. Drug Delivery Transl Res. 2024;14(2):455–473. doi:10.1007/s13346-023-01410-y
108. Luo Z, Peng X, Shi H, Gong C, Qian Z, Yang L. Comparison of the protective effects of truncated bFGF and native bFGF against murine lung carcinoma. Int J Mol Med. 2011;28(1):3–8. doi:10.3892/ijmm.2011.676
109. Delitto D, Dj Z, Chen F, et al. Implantation of a neoantigen-targeted hydrogel vaccine prevents recurrence of pancreatic adenocarcinoma after incomplete resection. Oncoimmunology. 2021;10(1):2001159. doi:10.1080/2162402X.2021.2001159
110. Chen G, Xiong W, Gu Z, et al. Mannosylated engineered trichosanthin-legumain protein vaccine hydrogel for breast cancer immunotherapy. Int J Biol Macromol. 2022;223(Pt A):1485–1494. doi:10.1016/j.ijbiomac.2022.11.045
111. Wang Z, Shang Y, Tan Z, et al. A supramolecular protein chaperone for vaccine delivery. Theranostics. 2020;10(2):657–670. doi:10.7150/thno.39132
112. Wang Z, Ren C, Shang Y, et al. Co-assembled supramolecular nanofibers with tunable surface properties for efficient vaccine delivery. Front Chem. 2020;8:500. doi:10.3389/fchem.2020.00500
113. Palucka AK, Ueno H, Fay JW, Banchereau J. Taming cancer by inducing immunity via dendritic cells. Immunolog Rev. 2007;220:129–150. doi:10.1111/j.1600-065X.2007.00575.x
114. Qian D, Liu Y, Zheng J, Cai J. Dendritic cell therapy for neurospoagioma: immunomodulation mediated by tumor vaccine. Cell Death Discovery. 2024;10(1):11. doi:10.1038/s41420-023-01782-7
115. Gautam N, Ramamoorthi G, Champion N, Han HS, Czerniecki BJ. Reviewing the significance of dendritic cell vaccines in interrupting breast cancer development. Mol Aspects Med. 2024;95:101239. doi:10.1016/j.mam.2023.101239
116. Li P, Jia L, Bian X, Tan S. Application of engineered dendritic cell vaccines in cancer immunotherapy: challenges and opportunities. Current Treatment Options Oncol. 2023;24(12):1703–1719. doi:10.1007/s11864-023-01143-7
117. Yang P, Song H, Qin Y, et al. Engineering dendritic-cell-based vaccines and PD-1 blockade in self-assembled peptide nanofibrous hydrogel to amplify antitumor T-cell immunity. Nano Letters. 2018;18(7):4377–4385. doi:10.1021/acs.nanolett.8b01406
118. Huo W, Yang X, Wang B, et al. Biomineralized hydrogel DC vaccine for cancer immunotherapy: a boosting strategy via improving immunogenicity and reversing immune-inhibitory microenvironment. Biomaterials. 2022;288:121722. doi:10.1016/j.biomaterials.2022.121722
119. Yang A, Bai Y, Dong X, et al. Hydrogel/nanoadjuvant-mediated combined cell vaccines for cancer immunotherapy. Acta biomaterialia. 2021;133:257–267. doi:10.1016/j.actbio.2021.08.014
120. Pamplona R, González-Lana S, Ochoa I, Martín-Rapún R, Sánchez-Somolinos C. Evaluation of gelatin-based hydrogels for colon and pancreas studies using 3D in vitro cell culture. J Mat Chem B. 2024;12(12):3144–3160. doi:10.1039/D3TB02640J
121. Degerstedt O, O’Callaghan P, Clavero AL, et al. Quantitative imaging of doxorubicin diffusion and cellular uptake in biomimetic gels with human liver tumor cells. Drug Delivery Transl Res. 2024;14(4):970–983. doi:10.1007/s13346-023-01445-1
122. Fucikova J, Kepp O, Kasikova L, et al. Detection of immunogenic cell death and its relevance for cancer therapy. Cell Death Dis. 2020;11(11):1013. doi:10.1038/s41419-020-03221-2
123. Singh T, Bhattacharya M, Mavi AK, et al. Immunogenicity of cancer cells: an overview. Cell Signal. 2024;113:110952. doi:10.1016/j.cellsig.2023.110952
124. Liu YB, Chen XY, Yu BX, et al. Chimeric peptide-engineered self-delivery nanomedicine for photodynamic-triggered breast cancer immunotherapy by macrophage polarization. Small. 2023;20:e2309994. doi:10.1002/smll.202309994
125. Zhang Q, Huang W, Yuan M, et al. Employing ATP as a new adjuvant promotes the induction of robust antitumor cellular immunity by a PLGA nanoparticle vaccine. ACS Appl Mat Interfaces. 2020;12(49):54399–54414. doi:10.1021/acsami.0c15522
126. Moriya T, Kitagawa K, Hayakawa Y, et al. Immunogenic tumor cell death promotes dendritic cell migration and inhibits tumor growth via enhanced T cell immunity. iScience. 2021;24(5):102424. doi:10.1016/j.isci.2021.102424
127. He T, Shi Y, Kou X, et al. Antigenicity and adjuvanticity co-reinforced personalized cell vaccines based on self-adjuvanted hydrogel for post-surgical cancer vaccination. Biomaterials. 2023;301:122218. doi:10.1016/j.biomaterials.2023.122218
128. Wang T, Wang D, Yu H, et al. A cancer vaccine-mediated postoperative immunotherapy for recurrent and metastatic tumors. Nat Commun. 2018;9(1):1532. doi:10.1038/s41467-018-03915-4
129. Fang L, Zhao Z, Wang J, et al. Engineering autologous tumor cell vaccine to locally mobilize antitumor immunity in tumor surgical bed. Sci Adv. 2020;6(25):eaba4024. doi:10.1126/sciadv.aba4024
130. Cerqueira OLD, Clavijo-Salomon MA, Cardoso EC, et al. Combined p14ARF and interferon-β gene transfer to the human melanoma cell line SK-MEL-147 promotes oncolysis and immune activation. Front Immunol. 2020;11:576658. doi:10.3389/fimmu.2020.576658
131. Li J, Zhang P, Zhou M, Liu C, Huang Y, Li L. Trauma-responsive scaffold synchronizing oncolysis immunization and inflammation alleviation for post-operative suppression of cancer metastasis. ACS Nano. 2022;16(4):6064–6079. doi:10.1021/acsnano.1c11562
132. Li J, Yan Y, Zhang P, et al. A cell-laden hydrogel as prophylactic vaccine and anti-PD-L1 amplifier against autologous tumors. J Controlled Release. 2022;351:231–244. doi:10.1016/j.jconrel.2022.09.027
133. Zhang H, Zhang Y, Hu H, et al. In situ tumor vaccine for lymph nodes delivery and cancer therapy based on small size nanoadjuvant. Small. 2023;19(33):e2301041. doi:10.1002/smll.202301041
134. Gong S, Liang X, Zhang M, et al. Tumor microenvironment-activated hydrogel platform with programmed release property evokes a cascade-amplified immune response against tumor growth, metastasis and recurrence. Small. 2022;18(50):e2107061. doi:10.1002/smll.202107061
135. Sa B, Warren SR, Oa A, et al. Injectable cryogel-based whole-cell cancer vaccines. Nat Commun. 2015;6:7556. doi:10.1038/ncomms8556
136. Wang F, Gao J, Wang S, et al. Near infrared light activation of an injectable whole-cell cancer vaccine for cancer immunoprophylaxis and immunotherapy. Biomat Sci. 2021;9(11):3945–3953. doi:10.1039/D1BM00542A
137. Kou X, He T, Zhang M, et al. A multivalent personalized vaccine orchestrating two-signal activation rebuilds the bridge between innate and adaptive antitumor immunity. Small Methods. 2023;7:e2300019. doi:10.1002/smtd.202300019
138. Ye X, Liang X, Chen Q, et al. Surgical tumor-derived personalized photothermal vaccine formulation for cancer immunotherapy. ACS Nano. 2019;13(3):2956–2968. doi:10.1021/acsnano.8b07371
139. Amina SJ, Azam T, Dagher F, Guo B. A review on the use of extracellular vesicles for the delivery of drugs and biological therapeutics. Expert Opinion Drug Delivery. 2024;21:45–70. doi:10.1080/17425247.2024.2305115
140. Liu X, Cao Y, Wang S, Liu J, Hao H. Extracellular vesicles: powerful candidates in nano-drug delivery systems. Drug Delivery Transl Res. 2024;14(2):295–311. doi:10.1007/s13346-023-01411-x
141. Zhang W, Yan Y, Peng J, et al. Decoding roles of exosomal lncRNAs in tumor-immune regulation and therapeutic potential. Cancers. 2022;15(1):286. doi:10.3390/cancers15010286
142. González FE, Gleisner A, Falcón-Beas F, Osorio F, López MN, Salazar-Onfray F. Tumor cell lysates as immunogenic sources for cancer vaccine design. Human Vaccines Immunotherapeut. 2014;10(11):3261–3269. doi:10.4161/21645515.2014.982996
143. Yang K, Zhou Y, Huang B, et al. Sustained release of tumor cell lysate and CpG from an injectable, cytotoxic hydrogel for melanoma immunotherapy. Nanoscale Adv. 2023;5(7):2071–2084. doi:10.1039/D2NA00911K
144. Song H, Yang P, Huang P, Zhang C, Kong D, Wang W. Injectable polypeptide hydrogel-based co-delivery of vaccine and immune checkpoint inhibitors improves tumor immunotherapy. Theranostics. 2019;9(8):2299–2314. doi:10.7150/thno.30577
145. Chen Y, Zhang L, Shi H, et al. Thermosensitive hydrogel delivery of BCG lysates and tumor antigens: a novel strategy for melanoma immunoprevention and therapeutics. Biochem Biophys Res Commun. 2025;745:151215. doi:10.1016/j.bbrc.2024.151215
146. Lu Y, Wu C, Yang Y, et al. Inhibition of tumor recurrence and metastasis via a surgical tumor-derived personalized hydrogel vaccine. Biomat Sci. 2022;10(5):1352–1363. doi:10.1039/D1BM01596F
147. Gn S, Cn Z, Xu R, et al. Enhanced antitumor immunity by targeting dendritic cells with tumor cell lysate-loaded chitosan nanoparticles vaccine. Biomaterials. 2017;113(191–202):191–202. doi:10.1016/j.biomaterials.2016.10.047
148. Sl C, Hm L, Cp L, et al. Robust and sustained STING pathway activation via hydrogel-based in situ vaccination for cancer immunotherapy. ACS Nano. 2024;18(43):29439–29456. doi:10.1021/acsnano.3c12337
149. Jm S, Rh H, Canner D, et al. Conventional type I dendritic cells maintain a reservoir of proliferative tumor-antigen specific TCF-1(+) CD8(+) T cells in tumor-draining lymph nodes. Immunity. 2021;54(10):2338–2353.e2336. doi:10.1016/j.immuni.2021.08.026
150. Mueller SN, Mackay LK. Tissue-resident memory T cells: local specialists in immune defence. Nat Rev Immunol. 2016;16(2):79–89. doi:10.1038/nri.2015.3
151. Zhang L, Zhang J, Xu L, et al. NIR responsive tumor vaccine in situ for photothermal ablation and chemotherapy to trigger robust antitumor immune responses. J Nanobiotechnol. 2021;19(1):142. doi:10.1186/s12951-021-00880-x
152. Wang D, Xue M, Chen J, et al. Macrophage-derived implantable vaccine prevents postsurgical tumor recurrence. Biomaterials. 2021;278:121161. doi:10.1016/j.biomaterials.2021.121161
153. Fu LQ, Du WL, Cai MH, Yao JY, Zhao YY, Mou XZ. The roles of tumor-associated macrophages in tumor angiogenesis and metastasis. Cell Immunol. 2020;353:104119. doi:10.1016/j.cellimm.2020.104119
154. Nowak M, Klink M. The role of tumor-associated macrophages in the progression and chemoresistance of ovarian cancer. Cells. 2020;9(5):1299. doi:10.3390/cells9051299
155. Wang C, Jing Y, Yu W, et al. Bivalent gadolinium ions forming injectable hydrogels for simultaneous in situ vaccination therapy and imaging of soft tissue sarcoma. Adv Healthcare Mat. 2023;12:e2300877. doi:10.1002/adhm.202300877
156. Qin X, Yang T, Xu H, et al. Dying tumor cells-inspired vaccine for boosting humoral and cellular immunity against cancer. J Controlled Release. 2023;359:359–372. doi:10.1016/j.jconrel.2023.05.044
157. Gabba A, Attariya R, Behren S, et al. MUC1 glycopeptide vaccine modified with a GalNAc glycocluster targets the macrophage galactose C-type lectin on dendritic cells to elicit an improved humoral response. J Am Chem Soc. 2023;145(24):13027–13037. doi:10.1021/jacs.2c12843
158. Zhang Y, Hu Z, Li X, et al. Amino acid sequence determines the adjuvant potency of a D-tetra-peptide hydrogel. Biomat Sci. 2022;10(12):3092–3098. doi:10.1039/D2BM00263A
159. Vivier E, Artis D, Colonna M, et al. Innate lymphoid cells: 10 years on. Cell. 2018;174(5):1054–1066. doi:10.1016/j.cell.2018.07.017
160. Ma S, Li X, Mai Y, Guo J, Zuo W, Yang J. Immunotherapeutic treatment of lung cancer and bone metastasis with a mPLA/mRNA tumor vaccine. Acta biomaterialia. 2023;169:489–499. doi:10.1016/j.actbio.2023.07.059
161. Liang X, Li L, Li X, et al. A spontaneous multifunctional hydrogel vaccine amplifies the innate immune response to launch a powerful antitumor adaptive immune response. Theranostics. 2021;11(14):6936–6949. doi:10.7150/thno.58173
162. Li D, Li W, Zheng P, et al. A “trained immunity” inducer-adjuvanted nanovaccine reverses the growth of established tumors in mice. J Nanobiotechnol. 2023;21(1):74. doi:10.1186/s12951-023-01832-3
163. Jing Z, Jie L, Sunxiang Q, Haifeng N, Jie F. Injectable zwitterionic cryogels for accurate and sustained chemoimmunotherapy. J Mat Chem B. 2023;11(12):2733–2744. doi:10.1039/D3TB00170A
164. Tang S, Tang R, Chen G, et al. Personalized neoantigen hydrogel vaccine combined with PD-1 and CTLA-4 double blockade elicits antitumor response in liver metastases by activating intratumoral CD8 + CD69 + T cells. J Immunother Cancer. 2024;12(12):e009543. doi:10.1136/jitc-2024-009543
165. Chi R, Pan L, Yang Z, et al. Oxaliplatin-loaded amphiphilic hyaluronic acid nanohydrogel formed via interfacial reactions enhances the therapeutic effect of targeted tumor. Int J Biol Macromol. 2025;284(Pt 2):138118. doi:10.1016/j.ijbiomac.2024.138118
166. Mitsuhashi K, Inagaki NF, Ito T. Moldable tissue-sealant hydrogels composed of in situ cross-linkable polyethylene glycol via thiol-michael addition and carbomers. ACS Bioma Sci Eng. 2024;10(5):3343–3354. doi:10.1021/acsbiomaterials.3c01755
167. Zhou S, Cheng F, Zhang Y, Su T, Zhu G. Engineering and delivery of cGAS-STING immunomodulators for the immunotherapy of cancer and autoimmune diseases. Accounts Chem Res. 2023;56(21):2933–2943. doi:10.1021/acs.accounts.3c00394
168. Liang S, Fu S, Yuan S, et al. Screening natural cholesterol analogs to assemble self-adjuvant lipid nanoparticles for antigens tagging guided therapeutic tumor vaccine. Adv Mat. 2025;37(27):e2419182. doi:10.1002/adma.202419182
169. Li J, Ding Q, Wang H, et al. Engineering smart composite hydrogels for wearable disease monitoring. Nano-Micro Letters. 2023;15(1):105. doi:10.1007/s40820-023-01079-5
170. Zhang X, Li D, Yang X, et al. Hydro-locking in hydrogel for extreme temperature tolerance. Science (New York, NY). 2025;387(6737):967–973. doi:10.1126/science.adq2711
171. Bianco S, Hasan M, Ahmad A, et al. Mechanical release of homogenous proteins from supramolecular gels. Nature. 2024;631(8021):544–548. doi:10.1038/s41586-024-07580-0
172. Rana MM, Demirkaya C, la Hoz Siegler HD. Beyond needles: immunomodulatory hydrogel-guided vaccine delivery systems. Gels. 2024;11(1):7. doi:10.3390/gels11010007
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Advancing Cancer Immunotherapy Using Lipid Nanoparticle-Based Approaches
Prazeres PHDM, Costa da Silva GH, Azevedo GV, Alves da Silva NJ, Carvalho Costa PA, Da Silva WN, Lobo AO, Guimaraes PPG
International Journal of Nanomedicine 2025, 20:12283-12305
Published Date: 8 October 2025