Back to Journals » Research and Reports in Urology » Volume 18
Hydrocelectomy Complication Rates in the United States
Authors Head DJ, Raman JD, Clark RK ![]()
Received 21 February 2026
Accepted for publication 1 May 2026
Published 3 June 2026 Volume 2026:18 601188
DOI https://doi.org/10.2147/RRU.S601188
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Panagiotis J Vlachostergios
Dennis J Head, Jay D Raman, Roderick K Clark
Penn State Health Milton S. Hershey Medical Center, Hershey, PA, USA
Roderick K Clark, Email [email protected]
Introduction and Objectives: Hydrocelectomy is the gold standard treatment for hydrocele. European data showed complication rates between 16% and 25%, however the rate within the United States has not been assessed. We examined the postoperative complication, emergency department visit, readmission and re-operation rates after hydrocelectomy in the United States.
Methods: We performed a retrospective cohort study of 27,418 individuals who underwent hydrocelectomy in the United States between 2004 and 2024 identified through the TriNetX US Network using ICD-10 and CPT codes. Patients were excluded for age < 18 years, testicular neoplasm, and orchiectomy. The primary outcome was rate of any surgical complication, emergency department (ED) visit, readmission, or reoperation within 90 days of hydrocelectomy. Statistical analysis was performed with R software and using t-tests.
Results: The mean age of our cohort was 51 years. The complication group had higher proportions of older (p < 0.001), African American (p < 0.001), and patients with hypertension, diabetes, and coagulation defects (p < 0.001).
The risk of complications was 13% within 90 days of surgery. The ED visit rate was 6.7%, surgical complication rate of 5.6%, readmission rate of 2.6%, and reoperation rate of 2.6%. Of surgical complications, 25% were bleeding, 13% were infection, and 63% were inflammatory or unspecified complications. The median ED visit was day 14 (IQR 6– 41) and the median reoperation was at day 21 (IQR 9– 38). Patients had a 9.2% rate of overall complications in the first month after surgery, after which the risk decreased.
Conclusion: The rate of complications after hydrocelectomy in the United States is 13%, with 9% occurring in the first 30 days. There was a 2.8% risk of surgical intervention within 90 days. We recommend close follow-up in the first month to evaluate for developing complications, especially for patients with hypertension, diabetes, or coagulation defects.
Keywords: hydrocele, surgical outcomes, postoperative complications, readmission, risk factors, TriNetX
Introduction
A hydrocele is a benign collection of fluid between the parietal and visceral layers of the tunica vaginalis and can range in size from barely palpable to a bulging collection of 1 liter of fluid or more.1 Hydrocelectomy, the gold standard of hydrocele treatment, has multiple variations all of which include incision of the tunica vaginalis and either eversion or excision of the tunica vaginalis to prevent further accumulation of fluid.2 Although hydrocelectomy is the most definitive treatment for hydroceles, it is associated with complications.2 Several studies have reported hydrocelectomy complication rates ranging from 16% to 27%, but were limited in sample size and assessment of risk factors.3–7 Accurate data on the complication rate is critical for preoperative counselling of patients.
Given the common nature of hydroceles, it is essential for urologic practices to be versed on rates of adverse events associated with surgical repair. Therefore, the purpose of our study is to quantify the rate of hydrocelectomy complications in the United States and explore associated risk factors.
Methods
This study reviewed data queried data from the US Collaborative Network on TriNetX to analyze complication rates associated with hydrocelectomy surgeries. We identified 27,418 individuals who underwent hydrocelectomy in the United States between 2004 and 2024 using diagnosis and procedural codes (Appendix 1). Exclusions were for age<18 years, testicular neoplasm, and orchiectomy. The primary outcome was rate of any emergency department (ED) visit, complication, readmission, or reoperation within 90 days of hydrocelectomy. Statistical analysis used summary statistics, t-tests, and chi-squared tests. This study was conducted in accordance with the Declaration of Helsinki. This retrospective study is exempt from informed consent. The data reviewed is a secondary analysis of existing data, does not involve intervention or interaction with human subjects, and is de-identified per the de-identification standard defined in Section §164.514(a) of the HIPAA Privacy Rule. The process by which the data is de-identified is attested to through a formal determination by a qualified expert as defined in Section §164.514(b)(1) of the HIPAA Privacy Rule. This formal determination by a qualified expert refreshed on December 2020.
Results
Our analysis included 27,418 patients with a mean age of 51 years (SD ± 20) (Table 1). The overall complication rate was 13.2% within 90 days of surgery. The ED visit rate was 6.7%, complication rate was 5.6%, hospital admission rate was 2.6%, and reoperation rate was 2.6%. Within 7 days of surgery, 1.3% of patients had complications and 1.9% had an ED visit, while at 14 days the rates increased to 2.9% and 3.3%, respectively.
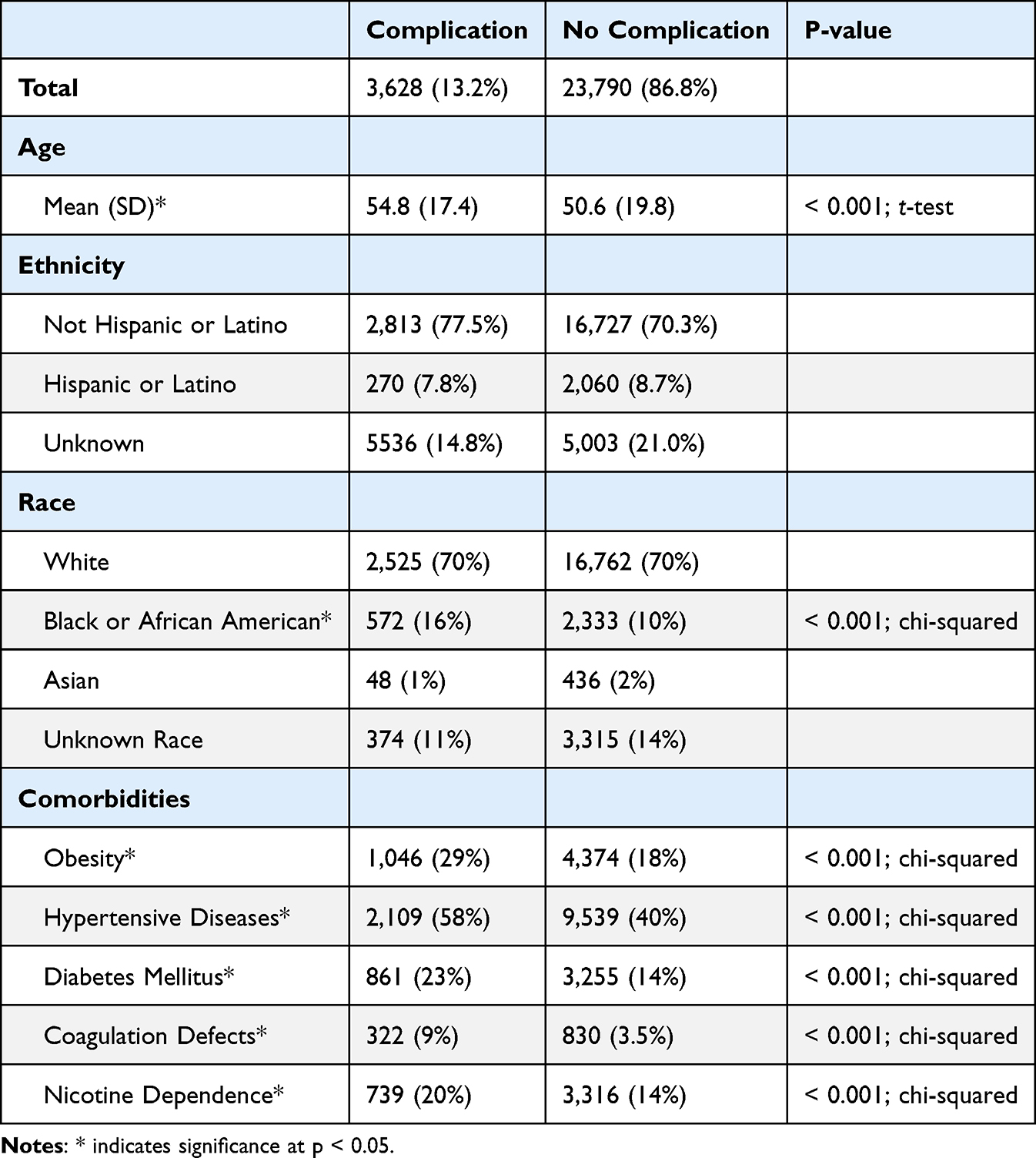 |
Table 1 Hydrocelectomy Cohort Characteristics |
Of complications, 25% were hematoma, 13% were infection, and 63% were inflammation related or unspecified procedural complications. The median ED visit was day 14 (IQR 6–41) and the median reoperation was at day 21 (IQR 9–38). Patients had a 9.2% rate of overall complications in the first month after surgery, after which the risk rapidly decreased (Figure 1).
 |
Figure 1 Rates of adverse events. |
The complications group had higher proportions of older patients (mean of 55 vs 51 years old; p < 0.001) and African-American patients (15.8% vs 9.8%; p < 0.001). The complications group had higher proportions of patients diagnosed with obesity (29% vs 18%; p < 0.001), hypertensive disease (58% vs 40%; p < 0.001), diabetes mellitus (23% vs 14%; p < 0.001), coagulation defects (9% vs 3.5%; p < 0.001), and nicotine dependence (20% vs 14%; p < 0.001).
Discussion
In this large cohort study, we found that hydrocelectomy was associated with a 13% complication rate, including 7% rate of ED visits and 3% rate of reoperation within 90 days of surgery. Complications were documented in 6% of patients and were mainly composed of unspecified disorders of the skin and genital inflammation, while hematoma occurrence was listed for 25% of these patients (1.5% of overall cohort).
Other studies have reported similar complication rates ranging from 16% to 27%, but all have smaller cohorts.3–7 A Swedish study retrospectively examined 9,174 cases of surgically managed hydroceles which found a 17.5% rate of surgical complications within 30 days of the operation.3 A similar retrospective analysis was performed in Finland with a cohort of 866 patients who underwent hydrocelectomy which reported a 90-day complication rate of 16% and a 25% rate of unplanned emergency room visits.4
In addition to complication rates, our study identified risk factors associated with higher proportions of complications. These include greater patient age, Black or African American race, obesity, hypertensive disease, diabetes mellitus, coagulation defects, and nicotine dependence. These associations may be discussed with patients regarding surgical optimization, risk of complications and expectations for healing. These comorbidities may be associated with poor wound healing while the race association could be due to residual confounding, access-to-care differences or coding limitations rather than a direct biological effect.
Our study was limited by its retrospective nature and reliance on electronic medical records. Certain details could not be verified, such as the reasons for ED visits and readmissions, and, as such, were only temporally associated with the procedure. Using the TriNetX database we were unable to accurately assess the details of the surgical care, such as operative technique, antibiotic use, drain use, hydrocele size, operative technique, drain use, antibiotic prophylaxis, surgeon experience and follow-up care. We also note that there is significant overlap between individuals who have complications reported (eg, first admitted to hospital via emergency department and then proceed to operating room). Given these limitations, large retrospective datasets can be useful for identifying postoperative return visits and patient-level risk patterns, and these findings help guide follow-up planning after common surgical procedures.8
Conclusion
The rate of complications after hydrocelectomy in the United States is 13%, with 9% occurring in the first 30 days. There was a 2.8% risk of surgical intervention within 90 days. We recommend patient optimization prior to surgery and close follow-up in the first month to evaluate for developing complications, particularly for patients with obesity, hypertension, diabetes, nicotine dependence, or coagulation defects, although even with these interventions the complication rate may be similar. Future research should focus on prospective patient optimization practices prior to hydrocelectomy.
Data Sharing Statement
The data that support the findings of this study are available from the TriNetX.
Analytics Network. https://trinetx.com.
Ethics Statement
All data were deidentified, obtained through TriNetX Analytics Network. This study was conducted in accordance with the Declaration of Helsinki. This study used de‑identified data from the TriNetX research network and was therefore exempt from institutional review board review under U.S. federal regulations governing research with publicly available, de‑identified data (45 CFR 46.104(d)(4)).
Acknowledgments
The abstract of this paper was presented at the American College of Surgeons Clinical Congress as a poster with interim findings. The poster’s abstract was published in ‘Scientific Forum Abstracts’ section in the Journal of the American College of Surgeons 241(5):p S547-S557, November 2025. DOI: 10.1097/XCS.0000000000001573.
Author Contributions
DJ‑H performed the data analysis and drafted the research letter. JD‑R and RK‑C critically revised the manuscript for important intellectual content. RK‑C conceived, designed, and supervised the study. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work, including the accuracy and integrity of the research.
Disclosure
The authors have no conflicts of interest to disclose for this work.
References
1. Dagur G, Gandhi J, Suh Y, et al. Classifying hydroceles of the pelvis and groin: an overview of etiology, secondary complications, evaluation, and management. Curr Urol. 2017;10(1):1–5. doi:10.1159/000447145
2. Rioja J, Sánchez-Margallo FM, Usón J, Rioja LA. Adult hydrocele and spermatocele. BJU Int. 2011;107(11):1852–1864. doi:10.1111/j.1464-410X.2011.10353.x
3. Lundström KJ, Söderström L, Jernow H, Stattin P, Nordin P. Epidemiology of hydrocele and spermatocele; incidence, treatment and complications. Scand J Urol. 2019;53(2–3):134–138. doi:10.1080/21681805.2019.1600582
4. Mäki-Lohiluoma L, Kilpeläinen TP, Järvinen P, Söderström HK, Tikkinen KAO, Sairanen J. Risk of complications after hydrocele surgery: a retrospective multicenter study in Helsinki Metropolitan Area. Eur Urol Open Sci. 2022;43:22–27. doi:10.1016/j.euros.2022.06.008
5. Swartz MA, Morgan TM, Krieger JN. Complications of scrotal surgery for benign conditions. Urology. 2007;69(4):616–619. doi:10.1016/j.urology.2007.01.004
6. Kiddoo DA, Wollin TA, Mador DR. A population based assessment of complications following outpatient hydrocelectomy and spermatocelectomy. J Urol. 2004;171(2 Pt 1):746–748. doi:10.1097/01.ju.0000103636.61790.43
7. Hicks N, Gupta S. Complications and risk factors in elective benign scrotal surgery. Scand J Urol. 2016;50(6):468–471. doi:10.1080/21681805.2016.1204622
8. Biza MH, Mengistie CT, Mengistie BT, et al. Patterns and predictors of readmission among sepsis survivors in a tertiary emergency department in Ethiopia. IJID Reg. 2026;18:100808. doi:10.1016/j.ijregi.2025.100808
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.