Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 11
Husband’s Support and Wife’s Decision to Children’s Dental Visit: Is There Any Relationship?
Authors Bramantoro T, Indrastie N ![]() , Hariyani N
, Hariyani N ![]() , Setyowati D
, Setyowati D
Received 23 July 2019
Accepted for publication 12 November 2019
Published 29 November 2019 Volume 2019:11 Pages 367—371
DOI https://doi.org/10.2147/CCIDE.S224336
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Taufan Bramantoro,1 Nuraini Indrastie,2 Ninuk Hariyani,1 Dini Setyowati1
1Department of Dental Public Health, Faculty of Dental Medicine, Universitas Airlangga, Surabaya, Indonesia; 2Graduate School of Dental Science, Faculty of Dental Medicine, Universitas Airlangga, Surabaya, Indonesia
Correspondence: Taufan Bramantoro
Department of Dental Public Health, Faculty of Dental Medicine Universitas Airlangga, Campus A UNAIR Jl. Prof. Dr. Moestopo No. 47, Surabaya 60132, East Java, Indonesia
Tel +62 31 5030255
Email [email protected]
Background: Early childhood caries (ECC) is the most common dental caries in children. The 2013 Indonesian basic health survey showed that there were still many children in developmental age affected by dental caries. Parents’ participation is very necessary in guiding, giving understanding, reminding, and providing facilities so that children can maintain their overall oral hygiene. Hence, parents can prevent plaque accumulation and the occurrence of caries in children.
Objective: This study aimed to determine the effect of husbands’ support on the decision of mothers to take their children to the dentist.
Subjects and methods: This study used a cross-sectional method. The samples from this study were 95 mothers from 3 kindergartens in Surabaya. Ninety-five mothers were randomly chosen as research respondents and filled out the research questionnaires. The data obtained were processed using statistical analysis to determine the correlation.
Results: Research respondents with low husband support (subjective norms) who did not take their children to the dentist had a significant value (p = 0.004) compared to the study respondents with high husband support who did not bring their children to the dentist (p = 0.093).
Conclusion: Mothers with low support from husbands tend to have the attitude not to take their children to do routine dental and oral examinations.
Keywords: children dental care, dental health, health behavior, social support, theory of planned behavior
Introduction
Oral health is an important part of general health and it can be considered as a reflection of general health. Poor oral health can have a detrimental effect on general health because several oral diseases are associated with chronic diseases. Based on the results of the 2013 Indonesian basic health survey, the prevalence of caries sufferers in Indonesia was 72.6%, with 31.1% of residents received dental and oral treatment. In East Java province, the second largest province in Indonesia, 28.6% of the population had problems with dental and oral health. Among those who had dental and oral problems, 30% of the population received treatment from dental medical personnel, while 70% did not.1
The most common dental caries in children is early childhood caries (ECC). The high prevalence of ECC is found in some developing countries and its severity increase with age. Whereas healthy primary teeth is important for speech, mastication, prevention of poor oral habits, and helpful as a guide for permanent tooth eruptions. The 2013 Indonesian basic health survey showed as many as 28.9% children aged 5–9 years have oral problems, while children aged 1–4 year is at 10.4%. The damage caused by caries of primary teeth usually requires maintenance of restoration and lifelong maintenance.2
The secondary data obtained at one of the health centers in Surabaya showed pulpitis was the disease that ranked sixth out of the 15 most listed diseases in the Ketabang Health Center and caries in children was the main problem. Based on the primary data from the preliminary survey in 3 schools (kindergartens) in Surabaya, the occurrence of caries in children reached 80.4%. This percentage is considered high because more than three-quarters of the samples experienced dental caries. This is reinforced by the minimum number of dental visit to the health center. Based on the data from the dental polyclinic in one of the health centers in Surabaya, the number of patients aged 0–6 years who came for treatment due to dental pain in the period of 3 months was only 7.88% out of the total coverage of children visitors of the health center.
Children under the age of 5 generally spend most of their time with parents and caretakers, especially during preschool. These early years involve primary socialization that shapes children’s habits, including the habit of maintaining dental health, and the behavior of the closest person is believed to be able to shape children’s habits. Parents are considered as the biggest influence for children to do something and the positive influence of parents can determine the level of dental health of children. Families with good communication have better dental health than those with poorer family relationships. Research also shows that mothers with higher education have better knowledge on the importance of primary teeth,3 and those with lower levels of education have poor levels of oral health knowledge.4
It can be said that mothers has an important role in the development of children’s behavior, and it is not uncommon for a mother to ask for an opinion from her husband before deciding on an issue. Husbands’ motivation sometimes affects the behavior of the mother in determining an action. Asking for husbands’ advice is important in making health decisions, especially decisions involving costs. Mothers also often consider the husbands’ advice as the primary decision maker in the family.5
In the preliminary survey, researchers interviewed several mothers and found that one of the factors that influenced the low behavior of mothers to visit dental and oral health centers was the lack of support from husbands to provide advice and decisions about oral and dental health. This is what the researchers wanted to explore further as one of the factors that might influence the realization of the 2030 Caries-Free Indonesia program. This study aimed to determine the relationship between husband’s support and the mother’s decision to make a dental visit for their children. The selection of schools is in accordance with the places of the preliminary survey conducted by the researchers.
Materials and Methods
Ethical approval for conducting this study has been obtained from The Research Ethic Committee of the Faculty of Dentistry Universitas Airlangga number 156/HRECC.FODM/VII/2018. This study used a cross-sectional method with data on children’s dental and oral health problems in 2018 from one of the health centers in Surabaya as the primary data. The respondents of this study were 95 mothers of children (aged 4–6 years old) randomly selected from 3 kindergartens in Surabaya.
After signing the written informed consent as approved by the local Research Ethic Committee, mothers as respondents were asked to fill out questionnaires in the form of questions that could provide an overview of the characteristics of parents, the frequency of visits to the dentist, and the reason for conducting or not conducting children’s dental visit to dentist.
The data obtained were processed and cross-tabulated using IBM SPSS 20 applications. Correlations were analyzed by cross-tabulation using chi-square with husbands’ support as an independent variable and children’s dental visit as dependent variable.
Results
Table 1 showed that out of a total of 95 mothers, most of whom are less than 40 years of age with final education was primary to high school level. Most respondents are housewives, and one third of respondents have never taken their children to dentists.
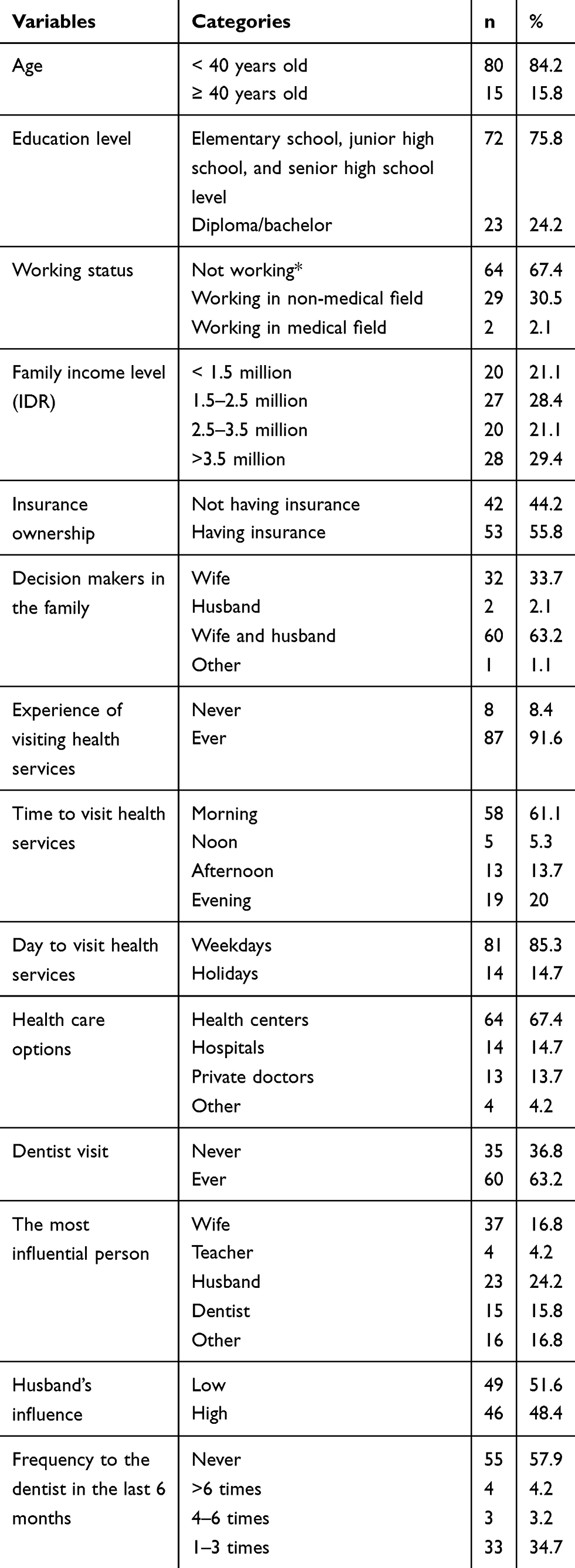 |
Table 1 Characteristics of Respondents Who Can Provide an Outline Description of Social Class as Well as Knowledge, Attitudes, Influence of Subjective Norms, Beliefs About Behavior, and Intention to Bring Children to Have Their Teeth Checked by a Dentist |
Of the total 95 respondents, 85.3% of them preferred to visit the health centers on holidays, and the remaining 14.7% preferred to come to visit the health centers on weekdays. Of the research respondents who chose holidays, 69.1% of them had taken their children to health services. Whereas of those who chose weekdays, only 28.6% of research respondents have brought their children to health centers. 57.9% of the respondents had never been to the dentist in the past 6 months.
Based on Table 2, the characteristics of respondents who have P value <0.05 were those who do not have health insurance (0.005), respondents with low intentions (0.038), respondents who have never visited health services (0.004), respondents who are unemployed, have low education, and have high intention but with low husbands’ support (0.004).
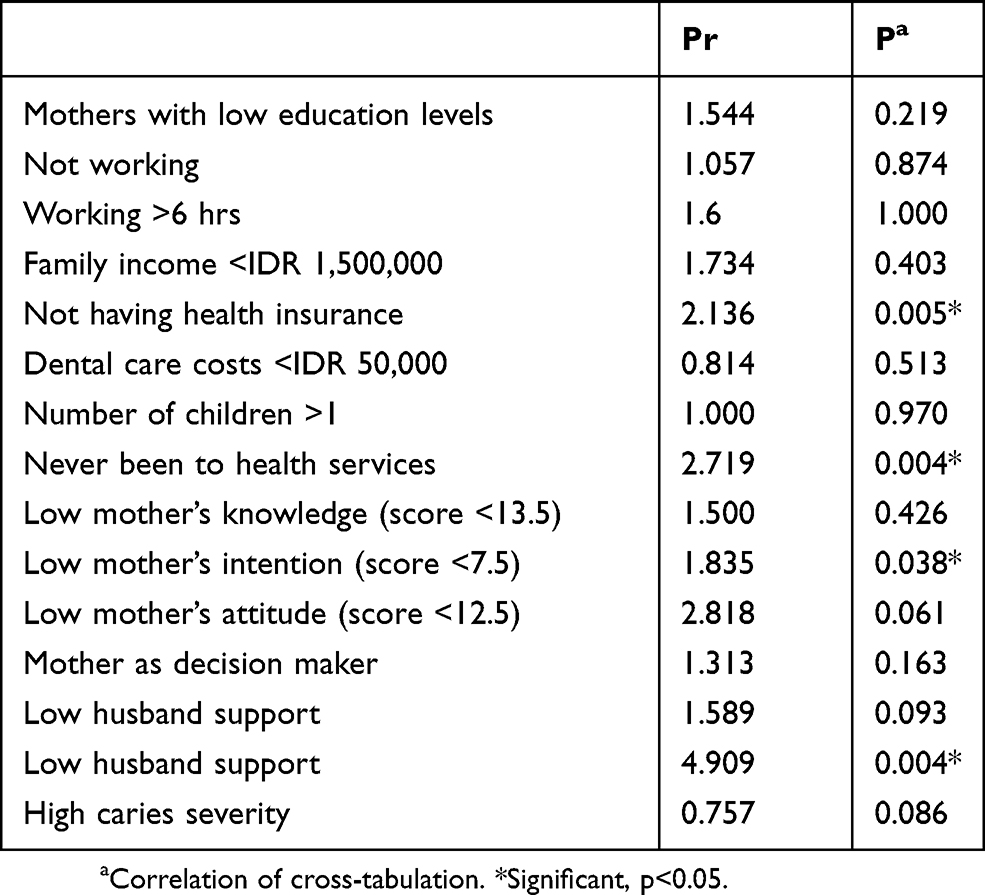 |
Table 2 Cross-Tabulation of Characteristic with a Visit to the Dentist. The Characteristics Listed in the Table are the Categories of Respondents Who Have a Tendency Not to Take Children to the Dentist Based on the Prevalence Ratio |
As many as 54% of the research respondents who did not work had low education but high intention to take the children to the dentist with a low influence of the husband (score below the median; 10.5) claimed that they never take their children to dentists. This percentage was higher than the number of respondents with a tendency to take their children to the dentist even though with low husband support (44.9%).
Based on Table 3, respondents with low intentions (scores below the median; 7.5) claimed that they never taken their children to dental and oral health services (58.8%). Whereas the respondents with high intention of study who never taken their children to dental and oral health services reached to 32.1%.
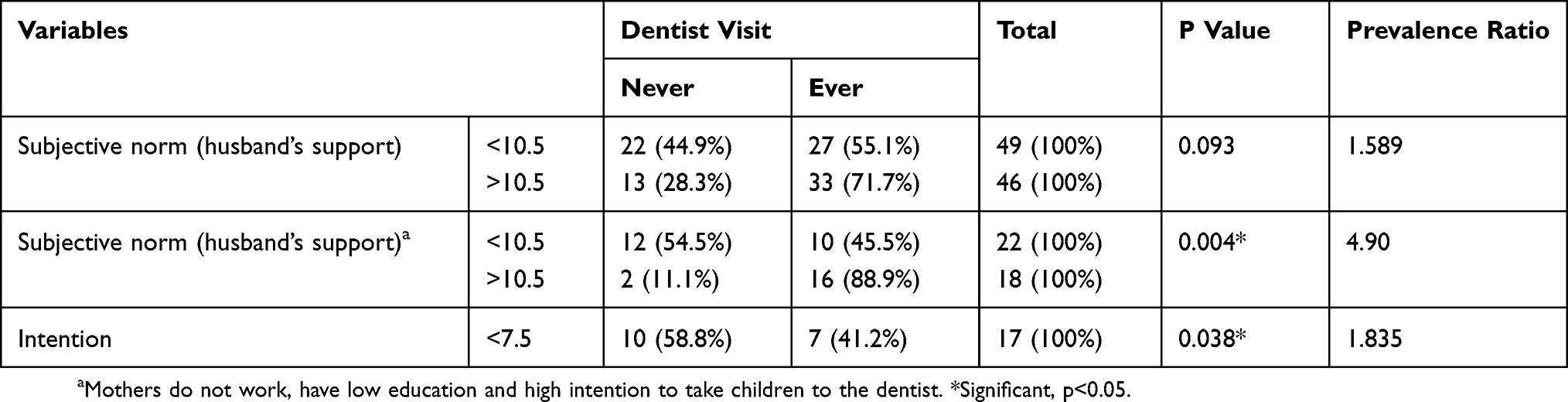 |
Table 3 Cross-Tabulation of the Frequency of Subjective Norms and Intention to Visit a Dentist |
Discussion
Preschool children’s behavior is strongly influenced by their primary environment, especially mothers. Parents’ behavior also has a great influence to their children’s dental visits. A study revealed that besides education, intelligence, attention, and someone’s interest towards something can influence someone’s knowledge. In this study, it applies to mothers in getting information from health workers and the respondents’ willingness to get dental and oral health information from various sources.6
Mothers who obtain a lot of information on dental health tend to take their children to the dentist.7 Sometimes, mothers get support or advice from other related family members to take their children to health services. Husbands are the other family member who can influence and improve mothers’ behavior towards childrens’ dental visit.8
In this study, 58.8% of research respondents with low intention had behavior that never taken their children to dental and oral health centers. Parents with low intentions chose not to go to the dentist because they consider that their children’s oral problem as a minor problem, and believe that caries is basically a genetic problem and therefore beyond control. These parents prefer not to go to dentists and they take their children only when there is pain. An annual visits were considered sufficient.9
Husbands’ role in the decision of the mothers to take their children to the dentist is part of the theory of planned behavior’s subjective norm. Subjective norm refers to the perceptions of social normative pressure to engage in a behavior. This norms is based on beliefs about the perceived judgment of significant others (for example, friends, family, dentists) regarding the behavior.10
According to the results of this study, subjects with low support from husbands tended not to take their children to dentists with 0.04 significance value (p). This number is consistent with other studies which showed that gender still plays a role in family decision making.11 Other research that has been done about the behavior and subjective norms of couples and doctors in determining children’s fever treatment decisions also showed that husbands play a role in determining the decision.12
A research conducted in Nepal,13 showed the dominance of men in the fields of labor, economy, education and politics has long been recognized so that men are considered the main pillar in a household. Men are given with a key role in managing finance, health and other matters. The role of men also influences knowledge in a family, so men also play an important role in decisions, including health aspects.14
Over time, there have been various changes in perceptions and roles prevalent in the family, especially between a husband and a wife. Changes in perceptions and roles are influenced by the existence of social changes caused by industrialization. This leads to the opening of women’s opportunities to get higher education and also broader employment opportunities. This condition creates a different perception for women about their role in the family. The new perception also has an impact on the husbands’ role as the head of the family. The empowerment of women in a family will increase if they have a job outside the home. Social and economic developments also have an impact on changes in cultural values that apply in an environment that influence decision making in the family structure to determine the expenditure of goods or services that will be used.15 The result of this study matched reversely with the theory. Low husbands support on mothers who did not work, had low level of education, but high intention to go to the dentist, significantly affect their behavior not to take their children to the dentist. This result showed that mothers with narrow perspective and environment tend to do what husbands said, instead of taking actions based on what they would do in case of providing healthcare for their children.
In another study, it was also found that in low social classes, husbands had a dominant role in the family. This theory suits to subjects who did not work that husbands play an important role in determining the decision to go to health services. Husbands who are financially capable and have a role to fulfill family needs play a role as decision makers. Although wives are given space to argue, in the end, wives will usually follow the final decision made by husbands.15,16
Conclusion
Based on this study, it can be concluded that low husbands support affects mothers’ behavior, tend not to take their children to the dentist. Therefore, husbands’ support can be used as a supporting factor for the mother to make a decision about childrens’ dental visit.
Acknowledgments
We would like to show our gratitude to Ketabang Public Health Center and Community Empowerment Program, Faculty of Dental Medicine, Universitas Airlangga, activists (Nadya Adina Zuhdi and friends), and also Department of Dental Public Health for supporting this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Indonesian Ministry of Health. Basic Health Survey of Republic of Indonesia. Jakarta: Indonesian Ministry of Health; 2013.
2. Wigen TI, Wang NJ. Parental influences on dental caries development in preschool children: an overview with emphasis on recent Norwegian research. Nor Epidemiol. 2012;22(1):13–19. doi:10.5324/nje.v22i1.1515
3. Jain R, Oswal KC, Chitguppi R. Knowledge, attitude and practices of mothers toward their children’s oral health: a questionnaire survey among subpopulation in Mumbai (India). J Dent Res Sci Dev. 2014;1:40–45. doi:10.4103/2348-3407.135073
4. Szatko F, Wierzbicka M, Dybizbanska E, Struzycka I, Iwanicka-Frankowska E. Oral health of polish three-year-olds and mother’s oral health-related knowledge. Community Dent Health. 2004;21:175–180.
5. Edwards D. Ketika Anak Sulit Diatur: Panduan Bagi Para Orang Tua Untuk Mengubah Masalah Perilaku Anak. Bandung: PT Mizan Pustaka; 2006.
6. Chacko V, Shenoy R, Prasy HE, Agarwal S. Self-reported awareness of oral health and infant oral health among pregnant women in Mangalore, India – a prenatal survey. Int J Health Rehabil Sci. 2013;2(2):109–115.
7. Grembowski D, Spiekerman C, Milgrom P. Linking mother and child access to dental care. Pediatrics. 2008;122(4):e805–14. doi:10.1542/peds.2008-0118
8. Anderson CL, Reynolds TW, Gugerty MK. Husband and wife perspectives on farm household decision-making authority and evidence on intra-household accord in Rural Tanzania. World Dev. 2017;90:169–183. doi:10.1016/j.worlddev.2016.09.005
9. Vermaire JH, Hoogstraten J, van Loveren C, Poorterman JH, van Exel NJ. Attitudes towards oral health among parents of 6-year-old children at risk of developing caries. Community Dent Oral. 2010;38:507–520. doi:10.1111/j.1600-0528.2010.00558.x
10. den Branden SV, den Broucke SV, Leroy R, Declerck D, Hoppenbrouwers K. Predicting oral health-related behaviour in the parents of preschool children: an application of the theory of planned behaviour. Health Educ J. 2015;74(2):221–230.
11. Scanzoni J, Szinovacz M. Family Decision-Making: A Developmental Sex Role Model. Sage: Beverly Hills; 1980.
12. Walsh A, Edwards H, Fraser J. Attitudes and subjective norms: determinants of parents’ intentions to reduce childhood fever with medications. Health Educ Res. 2009;24(3):531–545. doi:10.1093/her/cyn055
13. McPherson RA, Tamang J, Hodgins S, et al. Process evaluation of a community-based intervention promoting multiple maternal and neonatal care practices in rural Nepal. BMC Pregnancy Childbirth. 2010;10:31. doi:10.1186/1471-2393-10-31
14. Varkey LC, Mishra A, Das A, et al. Involving Men in Maternity Care in India. New Delhi: Population Council; 2004.
15. Samsinar MS, Zawawi D, Teo BH. Factors affecting wives’ role structure in urban family purchase decision making. Pertanika J Soc. 2013;21:189–200.
16. Tajuddin SKA, Shamsuddin K. Decision making behaviour related to wife’s reproductive health in bidayuh men in rural part of East Malaysia. IOSR-JNHS. 2015;4(1):56–63.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.