Back to Journals » Cancer Management and Research » Volume 13
Human Polycomb Protein 2 (hPC2) as a Novel Independent Prognostic Marker in Nasopharyngeal Carcinoma
Authors Wu M, Yang L, Hou X, Wang Z, Zhang J
Received 1 March 2021
Accepted for publication 24 June 2021
Published 20 July 2021 Volume 2021:13 Pages 5775—5784
DOI https://doi.org/10.2147/CMAR.S308884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjeev K. Srivastava
Mei Wu,1 Li Yang,1 Xiaojuan Hou,1 Ziyuan Wang,1 Jianqing Zhang2
1Diagnosis and Treatment Center of Otorhinolaryngology, People’s Hospital of Xinjiang Uygur Autonomous Region, Urumqi, 830001, Xinjiang, People’s Republic of China; 2Department of Radiotherapy People’s Hospital of Xinjiang Uygur Autonomous Region, Urumqi, 830001, Xinjiang, People’s Republic of China
Correspondence: Mei Wu
Diagnosis and Treatment Center of Otorhinolaryngology, People’s Hospital of Xinjiang Uygur Autonomous Region, No. 91 Tianchi Road, Tianshan District, Urumqi, 830001, Xinjiang, People’s Republic of China
Tel +86-0991-8563721
Fax +86-0991-8563692
Email [email protected]
Purpose: Human polycomb protein 2(hPC2) is a vital component of polycomb repressive complex 1(PRC1). It plays a critical role in tumorigenesis and progression. However, whether HPC2 expression affects the prognosis of patients with nasopharyngeal carcinoma (NPC) is currently unclear. In the present study, we investigated the expression of hPC2and elucidated its clinical prognostic significance in NPC.
Patients and Methods: The expression of hPC2 in 180 NPCs samples was examined by immunohistochemistry (IHC) and evaluated by H-score staining intensity. Receiver operator characteristic (ROC) curve analysis was performed to determine cut-off values of hPC2 expression. The chi-square test, Kaplan–Meier (Log rank test), and the Cox proportional hazards model were utilized to analyze the data.
Results: We found hPC2 is highly expressed in 48.3% of NPC specimens, which significantly correlated with T stage (p=0.032), N stage (p=0.006), and clinical stage (p=0.003). Kaplan–Meier analysis indicated that NPCs with high hPC2 expression tended to have a lower cumulative rates of overall survival (OS, p< 0.001), recurrence-free survival (RFS, p=0.001), and distant metastasis-free survival (DMFS, p=0.003). In the NPCs subgroup, T3–T4, N2–N3, and stages III–IV, high hPC2 expression also had a prognostic impact on worse outcome in terms of OS, RFS, and DMFS. More importantly, multivariate analyses demonstrated that hPC2 expression was an independent prognostic factor for OS (hazard ratio [HR], 95% (confidence interval [CI]), p=0.001), RFS (HR, 95% CI, p=0.018), and DMFS (HR, 95% CI, p=0.022).
Conclusion: We present evidence that high expression of hPC2 correlated with poorer prognosis in NPC. hPC2 could serve as a novel prognostic biomarker and might be a promising therapeutic target for NPC.
Keywords: hPC2, immunohistochemistry, prognosis, tumor stage
Introduction
Nasopharyngeal carcinoma (NPC) is a malignant tumor that originates from the superior mucosal epithelium of the nasopharyngeal cavity. The incidence of NPC is characterized by a distinct geographical distribution. In 2018, the International Agency for Research on Cancer (IRAC) estimated over 70% new cases occur in East and Southeast Asia.1 The estimated age-standardized incidence rate of NPC is about 0.4 new cases per 100,000 individuals in North America, while the incidence rate is less than 3.0 per 100,000 person-years in China.2 As the most common cancer in the head and neck regions, the main risk factors1 of NPC include environmental factors, history of Epstein-Barr (EBV) virus infection, smoking, drinking, habitual consumption of preserved foods, and genetic susceptibility.3–5 Intensity-modulated radiotherapy (IMRT) is still the main therapeutic approach for NPC, however, for patients with advanced stage disease, the 5 year survival rate is 50–60%.6 Aberrant gene expression has been associated with malignant progression and poor prognosis in patients with NPC.7–9
Human polycomb protein 2(hPC2) also known as Chromobox homolog 4 (CBX4), is a member of the polycomb repressive complex 1(PRC1). PcG-PRC1 complex, which acts by chromatin remodeling and histone modification, plays a pivotal role in the lineage differentiation of the embryonic mesoderm layer.10 CBX4 is a protein-coding gene with chromatin binding and protein ligase activity, and is involved in related signaling pathways including cell senescence and small ubiquitin-related modifiers(SUMOs).11 Accumulating evidence has demonstrated that dysregulation of hPC2 is involved in many malignancies. The expression of CBX4/hPC2 has also been correlated with the clinical prognosis of hepatocellular carcinoma, osteosarcoma, and breast cancer.12–14 However, the expression pattern and prognostic significance of CBX4/hPC2 remain unclear in NPC. Herein, we used Immunohistochemistry (IHC) to detect the expression of hPC2 and investigated its prognostic value in NPC.
Materials and Methods
Patients and Specimens
A total of 180 subjects were recruited from the Xinjiang Autonomous Region People’s Hospital from January 2000 to December 2013. The archived paraffin biopsy tissue specimens corresponding to the patients’ follow-up visits were collected and sectioned. The histological type was established for head and neck tumors according to the World Health Organization (WHO) 2006 classification, and the TNM stage of NPC was defined using the AJCC Cancer Staging Manual, 7th Edition.15 NPC patients were enrolled based on the following criteria: absence of distant metastasis at the first presentation, initial diagnosis histopathologically confirmed, and no history of anti-tumor treatments before diagnosis. The exclusion criteria were the presence of other malignant tumors, previous antitumor treatment, death from non-tumor-related reasons, and incomplete follow-up data. We calculated the overall survival (OS) from the end of radiotherapy until death or the last follow-up. Recurrence-free survival (RFS) was defined as the interval from the date of radiotherapy completion to the date of first recurrence or the last follow-up. Distant metastasis-free survival (DMFS) was defined as the interval from the end of radiotherapy to the date of first distant organ metastasis or end of follow-up. All recurrences or distant metastases were confirmed by nasal endoscopy, magnetic resonance imaging (MRI), or computed tomography (CT) imaging. The present study was approved by the Ethics Committee of Xinjiang Autonomous Region People’s Hospital. Informed, written consent was obtained from all participants and the entire study was performed according to the principles of the Declaration of Helsinki.
Immunohistochemistry
A total of 180 NPC tissue samples were collected. Briefly, the formalin-fixed paraffin-embedded (FFPE) tissue blocks were cut into 4-μm paraffin sections were then dried in the oven at 60°C for 60min. Immunohistochemistry (IHC) staining was performed according to the streptavidin-peroxidase method, sections were dewaxed in preheated xylene and rehydrated through incubation in an ethanol gradient (100%, 95%, 85%, 75%),then immersed in 3% hydrogen peroxide (H2O2) for 15 min. Antigen retrieval was performed by heating in a pressure cooker with citrate buffer (pH 6.0) for 5 min, followed by recovery at room temperature (25°C),Non-specific binding was blocked with 5% non-immunologic goat serum (Zhongshan Golden bridge Biotechnology, Beijing China) for 30 min at room temperature and was followed by incubation with the rabbit polyclonal anti-hPC2 (Bethyl, Cat. No. IHC 00668,1:100 dilution) overnight at 4°C in a humidified chamber. After washing with PBS, a secondary antibody (Gene Tech, Cat. No 500710) was incubated at room temperature for 30min. Slides were rinsed in PBS and peroxidase substrate DAB was added for color development for 3min. The sections were counterstained with hematoxylin, dehydrated in a graded series of ethanol (75%, 85%, 95%, 100%),followed by xylene, and cover slipped. Known positive human breast cancer tissue slide was used as positive control, the primary antibody was replaced by IgG from normal goat serum as a negative control, and PBS was applied as the blank control.
Immunohistochemical Evaluation
The slides were evaluated independently by two pathologists blinded to the clinicopathological and follow-up information. A semiquantitative scoring criterion for IHC was used, in which both staining intensity and the percentage of positive cells were scored. The color score was based on the staining intensity (colorless: 0; mild brown: 1; moderate brown: 2; and strong brown: 3).Under a 100-fold upright optical microscope, five random visual fields were counted for each sample section, one score was given according to the percentage of positive staining cells in each field, with a range from 0–100 by 5 increments (0, 5, 10 … 100). Another score was given based on the staining intensity category, and varied from 0 to 3 (0, 1, 2, 3). The H-score in each field was calculated by multiplying the above two scores (H-score=1×I1+2×I2+3×I3), and the final H-score was obtained as the average H-score value ranging from 0 to 300.16 We used the ROC curve to determine the cut-off value17 of hPC2expression in NPC. According to the ROC curve analysis, the cut-off value 160 was used to divide the patients into two groups: samples with IHC score below or equal to the threshold were defined as low expression, while samples with IHC score above the threshold were defined as high-expression.
Statistical Analysis
Statistical analysis was performed using SPSS Software, version 16.0 (SPSS Inc., Chicago, IL, USA). A receiver-operating characteristic (ROC) curve analysis was used to determine the immunohistochemical cut-off value for high or low expression. Survival curves were plotted using the Kaplan–Meier method and compared using the Log rank test. The Cox proportional hazards model was used for univariate and multivariate survival analysis. Significant variables in the univariate analysis were selected for the multivariate analysis. In all analyses, a 2-tailed, p-value<0.05 was considered statistically significant.
Results
Expression of hPC2 In clinical NPC Samples and Cut-Off Value for hPC2 Expression
hPC2 was expressed in 91.7% (165/180) of NPCs; positive staining was mainly located in the nucleus (Figure 1). The number of samples with high expression and low expression were 48.3% (87/180) and 51.7% (93/180), respectively (Table 1). A ROC curve for the sensitivity and specificity of the clinicopathological parameters were plotted and 160 was chosen as the cut-off value for separating hPC2 expression levels, sensitivity and specificity was 91.3% and 87.5% respectively. The area under the curve (AUC) values for each variables were calculated (Figure 2).
 |
Table 1 Correlation Between the hPC2 Expression and Clinicopathological Features in NPC |
 |
Figure 1 Representative immunohistochemical images of hPC2protein in NPC. The score indicates intensity of staining. (A) Score=0, negative staining; (B) score=1, weak staining; (C) score=2, moderate staining; (D) score=3, strong staining, magnification, left panel 200x, right panel 400x. |
 |
Figure 2 Receiver operator characteristic (ROC) curve analysis was used to determinate the cut-off values for hPC2 expression in NPC. Sensitivity and 1-specificity for each clinical parameter were plotted. (A) Age, (B) WHO type, (C) T stage, (D) N stage, (E) clinical stage, and (F) survival status. |
Association Between Clinicopathological Characteristics and hPC2 Expression of NPC Patients
A total of 180 patients were enrolled, in this cohort with an median age of 50 years (range:0–88 years). Among the patients, 135 were males and 45 were females. Of these,75 were daily smokers (75/180, 41.7%). EBV status was detected using in situ hybridization(ISH) for EBV-encoded small RNA (EBER) (79.4%, 143/180).The detailed clinicopathological data are shown in Table 1. hPC2 expression was significantly correlated with T stage (p=0.032), N stage (p=0.006), and clinical stage (p=0.003). There was no relationship between hPC2 expression and age, sex, ethnic groups, or tumor differentiation (WHO type)(p>0.05).
Univariate and Multivariate Analysis of Survival Outcome for NPC
Univariate analysis showed that T stage, N stage, and clinical stage, and hPC2 expression were significantly correlated to OS, RFS, and DMFS (Table 2, p<0.05). Multivariate Cox proportional hazards regression analysis was conducted by applying significant prognostic factors identified in univariate analysis. Importantly,hPC2 expression was an independent prognostic factor for OS (HR:3.175,95% CI: 1.648–6.116), RFS (HR:2.235,95% CI: 1.149–4.346),and DMFS (HR:1.990,95% CI: 1.104–3.588). Another independent prognostic factor was clinical stage for OS (HR: 2.739, 95% CI: 1.536–4.886),RFS (HR:3.490,95% CI: 1.830–6.656),and DMFS (HR:1.990,95% CI: 1.342–4.256) (Table 3).
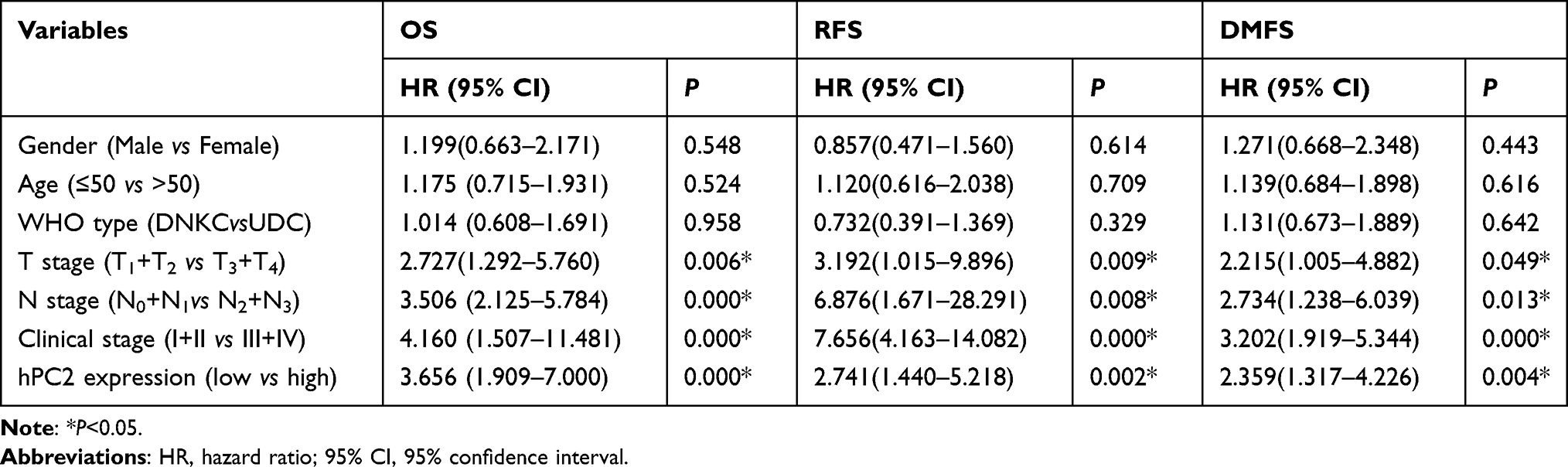 |
Table 2 Univariate Analyses of Potential Prognostic Factors for OS, RFS and DMFS in 180 NPC Patients |
 |
Table 3 Multivariate Analyses of Prognostic Factors on OS, RFS and DMFS in This Cohort |
Relationship Between hPC2 Expression and Clinical Outcomes
The patients were treated with either intensity-modulated radiotherapy (IMRT) or volumetric modulated arc therapy (VMAT) with a mean total dose of 70 Gray. Patients with advanced disease received cisplatin-based chemotherapy. Therapeutic responses were evaluated based on the WHO criteria. Local tumor recurrence and regional lymph node invasion was observed in 29.4% (53/180) of cases and in 33.9% (61/180) of cases with distant metastasis, During the follow-up period,35.6% (64/180) of cases died of NPC. We compared OS, RFS, and DMFS between the hPC2 low and high expression groups. OS, RFS, and DMFS of the high expression group was significantly decreased compared with the low expression group (OS,p<0.001; RFS,p=0.001; DMFS,p=0.003) (Figure 3A–C). The cumulative 5-year OS rates were 86.2% and 57.5%in subjects in the low and high expression groups, respectively. The cumulative 5-year RFS rates were 83.8% and 61.3% and the 5-year DMFS were 77.9% and 56.8% in the low and high expression groups, respectively. To further explore the effects of hPC2 expression on the above three clinical endpoints, subgroup analysis was performed stratified by factors closely related to hPC2 expression, including T stage, N stage, and clinical stage. Kaplan–Meier subgroup survival analysis for OS, RFS, and DMFS are presented in Figure 4. Analyses of OS demonstrated that hPC2 expression was a prognostic factor for T3–T4 (p=0.005, Figure 4A), N2–N3 (p=0.004, Figure 4B) and clinical stages III–IV (p=0.007, Figure 4C).Analyses of RFS showed an association with T3–T4 (p=0.003, Figure 4D), N2–N3 (p=0.021, Figure 4E), and clinical stage III–IV (p=0.011, Figure 4F). DMFS analysis revealed an association with T3–T4 (p=0.040, Figure 4G), N2–N3 (p=0.016, Figure 4H), and clinical stages III–IV (p=0.047, Figure 4I).
 |
Figure 3 Relationship between hPC2 expression and clinical outcome in NPC. The Kaplan–Meier survival curves were compared by the Log rank test. hPC2 high expression is a strong prognostic indicator of poor (A) overall survival, (B) recurrence-free survival, and (C) distant metastasis-free survival. |
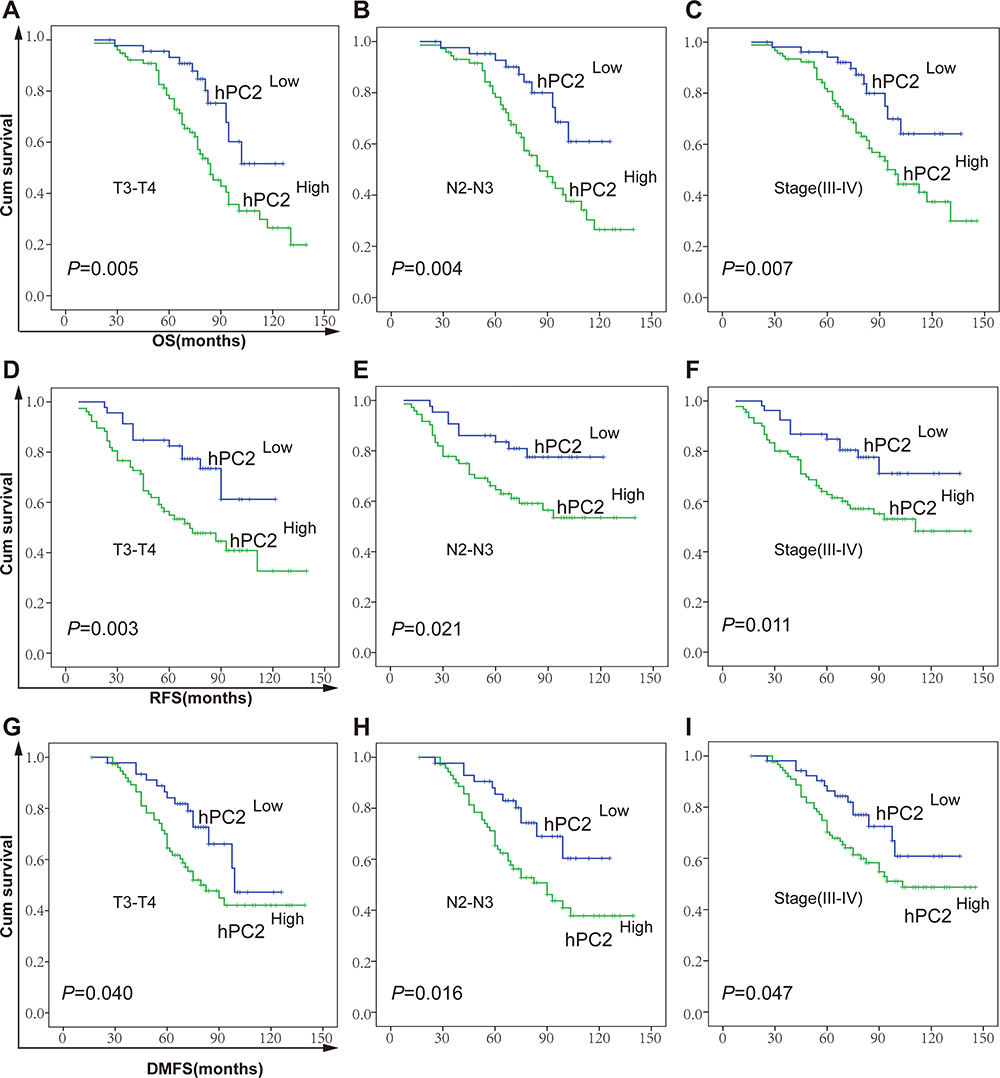 |
Figure 4 Analysis of hPC2 expression in related to OS, RFS, and DMFS of NPC patients. Survival analysis of hPC2 expression by the Kaplan–Meier method (Log rank test). Overall survival (OS) analysis for the subgroup of NPC patients with different hPC2 protein levels in stage T3-T4 (A), N2-N3 (B), TNM III–IV (C). Recurrence-free survival (RFS) analysis in stage T3–T4 (D), N2–N3 (E), TNM III–IV (F). Distant metastasis-free survival (DMFS) analysis in stage T3–T4 (G), N2–N3 (H), TNM III–IV (I). |
Discussion
Nasopharyngeal carcinoma (NPC) is a devastating disease with poorly differentiated and highly metastatic properties. Currently, no early or more accurate methods are available for the diagnosis of NPC, therefore, the majority of cases present with locally advanced stages at the time of initial diagnosis.18 Although NPCs are sensitive to radiation therapy, due to tumor heterogenicity, patients with the same clinical stage may achieve different clinical outcomes. It is of great importance to identify effective biological markers to distinguish poor prognosis subjects in order to suggest adjuvant therapy. Some EBV related proteins and microRNA signatures have been utilized as potential diagnostic and prognostic biomarkers, such as serum EBV-DNA,19 EBNA-1, and microRNA signatures (miR-22,miR-572, miR-638, and miR-1234), or EBERs, EBV-LMP1 expression in tumor tissue.20
In humans, hPC2 is located on chromosome 17q25.3,a region that comprises 560 amino acids and has a molecular weight of 61kDa. Unlike other PCG proteins,hPC2/CBX4 is an important E3 ubiquitin ligase,21,22 possessing diverse biological functions.23 It has been reported that HIF1 is a key tumor angiogenesis factor and is regulated by CBX4 in hepatocellular carcinoma.24 Furthermore, individuals with hepatocellular carcinoma and high CBX4 expression tend to be more sensitive to hepatic artery perfusion chemoembolization.25 hPC2 gene expression is markedly upregulated in many types of human cancers,CBX4 promotes cell cycle progression, and mediates tumor growth and metastasis.26–29 This evidence suggests that hPC2 plays an oncogenic role and serves as a potential therapeutic target. However, there have been conflicting results regarding tumor metastasis, CBX4 inhibits metastasis by directly repressing the transcription factor RUNX2 in colorectal cancer, in contrast,CBX4 promotes the invasion and metastasis of malignancies including osteosarcoma, breast cancer, and prostate carcinoma.30–33 Furthermore,Polycomb Repressive Complexes (PRC1 and PRC2) have emerged as therapeutic targets for malignant tumors. Inhibition of CBX4-YAP1 has recently been shown to reduce sorafenib resistance in HCC patients.34 Recently, it has been reported that PRC2-targeting agents exert synergistic effects on growth inhibition in NPC cells and the PRC2 subunits EZH2, EED, and H3K27Me3 are related to tumor invasiveness and metastasis.35
In the present study, the IHC results found that hPC2 expression was positive in 91.7% of NPCs, and hPC2 expression was correlated with clinical features such as T stage, N stage, and clinical stage. High hPC2 expression was associated with shorter OS, RFS, and DMFS, and survival as shown in Kaplan–Meier curves. Moreover, multivariate analysis confirmed that hPC2 expression and clinical stage were independent prognostic factors for OS, RFS, and DMFS. Our results confirmed that increased levels of hPC2/CBX4 expression significantly correlated with unfavorable prognosis. These findings are generally consistent with those reported in the literature. Thus, there is an urgent need to identify biomarkers useful for prognostic risk stratification as well as optimum treatment strategies for different patient subgroups. Herein, by stratifying the survival analysis we demonstrated that hPC2 expression was correlated with survival of NPC based onT3–4, N2–3, and clinical stages III–IV. As shown in Figure 4A–I, after stratification by T stage, N stage, and TNM stage, hPC2 expression was markedly correlated with prognosis, whereby higher hPC2 levels indicated a worse prognosis in stages T3–T4,N2–N3, and TNM II–III, suggesting that hPC2 could distinguish patients with poor prognosis from those with disease at the same clinical stage. These results suggested that high expression of hPC2 could be utilized to distinguish a group of patients with worse prognosis. Further, a multidisciplinary approach should be considered in order to optimize the patient management for prolonging survival. An obvious concern was that PRC2 subunit proteins were overexpressed in over 70% of NPC tumors, but these were not associated with survival in NPC patients.35 These results differ from our data, and may be attributed to differences in the study methodologies including: sample size, patient characteristics, scoring method for IHC evaluation, and definition of OS, RFS and DMFS.
The limitations in this study were as follows. First, this was a retrospective study, in which the proportion of stages III–IV patients included was higher than those in stages I–II, there may be a case selection bias. Second, although the H score method has been widely employed, different IHC scoring methods could lead to different results. Finally, prognosis was determined only based on the histological expression of hPC2. Serological detection of hPC2should be developed in the near future, and it is likely to be a useful predictive biomarker as tracking dynamic expression changes can act as an important indicator for monitoring, diagnosis and prognosis of NPC.
Taken together, our work provides compelling clinical evidence that hPC2 could serve as an independent prognostic marker for OS, RFS, and DMFS in NPC. High hPC2 expression in NPC was significantly related to advanced T stage, N stage, and clinical stage. Our findings suggest hPC2 as a novel prognostic biomarker and promising target for NPC. Future work evaluating hPC2 in NPC should shed light to better understand the underlying mechanisms promoting tumor progression.
Conclusion
We provide evidence that high hPC2 expression is associated with more advanced NPC stage. hPC2 acts as a novel independent risk factor affecting the prognosis of NPC, and high expression of hPC2 could represent an unfavorable marker for NPC.
Acknowledgments
Financial support: Natural Science Foundation of Xinjiang Uygur Autonomous Region (Grant No.2017D01C093).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen YP, Chan ATC, Le QT, et al. Nasopharyngeal carcinoma. Lancet. 2019;394(10192):64–80. doi:10.1016/S0140-6736(19)30956-0
2. Cao SM, Simons MJ, Qian CN. The prevalence and prevention of nasopharyngeal carcinoma in China. Chin J Cancer. 2011;30(2):114–119. doi:10.5732/cjc.010.10377
3. Jia WH, Qin HD. Non-viral environmental risk factors for nasopharyngeal carcinoma: a systematic review. Semin Cancer Biol. 2012;22(2):117–126. doi:10.1016/j.semcancer.2012.01.009
4. Xu FH, Xiong D, Xu YF, et al. An epidemiological and molecular study of the relationship between smoking, risk of nasopharyngeal carcinoma, and Epstein-Barr virus activation. J Natl Cancer Inst. 2012;104(18):1396–1410. doi:10.1093/jnci/djs320
5. Xu M, Yao Y, Chen H, et al. Genome sequencing analysis identifies Epstein-Barr virus subtypes associated with high risk of nasopharyngeal carcinoma. Nat Genet. 2019;51(7):1131–1136. doi:10.1038/s41588-019-0436-5
6. Lee AWM, Ng WT, Chan JYW, et al. Management of locally recurrent nasopharyngeal carcinoma. Cancer Treat Rev. 2019;79:101890. doi:10.1016/j.ctrv.2019.101890
7. Tang L, Xiong W, Zhang L, et al. circSETD3 regulates MAPRE1 through miR-615-5p and miR-1538 sponges to promote migration and invasion in nasopharyngeal carcinoma. Oncogene. 2021;40(2):307–321. doi:10.1038/s41388-020-01531-5
8. Tang Z, Chen W, Xu Y, et al. GSK3βmiR-4721, induced by EBV-miR-BART22, targets to enhance the tumorigenic capacity of NPC through the pathway. Mol Ther Nucleic Acids. 2020;22:557–571. doi:10.1016/j.omtn.2020.09.021
9. Liu N, He QM, Chen JW, et al. Overexpression of CIP2A is an independent prognostic indicator in nasopharyngeal carcinoma and its depletion suppresses cell proliferation and tumor growth. Mol Cancer. 2014;13(1):111. doi:10.1186/1476-4598-13-111
10. Kang X, Qi Y, Zuo Y, et al. SUMO-specific protease 2 is essential for suppression of polycomb group protein-mediated gene silencing during embryonic development. Mol Cell. 2010;38(2):191–201. doi:10.1016/j.molcel.2010.03.005
11. Ren X, Hu B, Song M, et al. Maintenance of nucleolar homeostasis by CBX4 alleviates senescence and osteoarthritis. Cell Rep. 2019;26(13):3643–3656.e3647. doi:10.1016/j.celrep.2019.02.088
12. Wang B, Tang J, Liao D, et al. Chromobox homolog 4 is correlated with prognosis and tumor cell growth in hepatocellular carcinoma. Ann Surg Oncol. 2013;20(S3):S684–692. doi:10.1245/s10434-013-3171-7
13. Yang J, Cheng D, Zhu B, et al. Chromobox homolog 4 is positively correlated to tumor growth, survival and activation of HIF-1α signaling in human osteosarcoma under normoxic condition. J Cancer. 2016;7(4):427–435. doi:10.7150/jca.13749
14. Zeng JS, Zhang ZD, Pei L, et al. CBX4 exhibits oncogenic activities in breast cancer via Notch1 signaling. Int J Biochem Cell Biol. 2018;95:1–8. doi:10.1016/j.biocel.2017.12.006
15. Liang W, Shen G, Zhang Y, et al. Development and validation of a nomogram for predicting the survival of patients with non-metastatic nasopharyngeal carcinoma after curative treatment. Chin J Cancer. 2016;35(1):98. doi:10.1186/s40880-016-0160-9
16. Lee HH, Wang YN, Xia W, et al. Removal of N-linked glycosylation enhances PD-L1 detection and predicts anti-PD-1/PD-L1 therapeutic efficacy. Cancer Cell. 2019;36(2):168–178.e164. doi:10.1016/j.ccell.2019.06.008
17. Fu J, Qiu H, Cai M, et al. Low cyclin F expression in hepatocellular carcinoma associates with poor differentiation and unfavorable prognosis. Cancer Sci. 2013;104(4):508–515. doi:10.1111/cas.12100
18. Zhang SQ, Pan SM, Liang SX, et al. Research status and prospects of biomarkers for nasopharyngeal carcinoma in the era of high‑throughput omics (review). Int J Oncol. 2021;58(4):1–12. doi:10.3892/ijo.2021.5188
19. Lam WKJ, Chan KCA, Lo YMD. Plasma Epstein-Barr virus DNA as an archetypal circulating tumour DNA marker. J Pathol. 2019;247(5):641–649. doi:10.1002/path.5249
20. Tsang CM, Lui VWY, Bruce JP, et al. Translational genomics of nasopharyngeal cancer. Semin Cancer Biol. 2020;61:84–100. doi:10.1016/j.semcancer.2019.09.006
21. Kagey MH, Melhuish TA, Wotton D. The polycomb protein Pc2 is a SUMO E3. Cell. 2003;113(1):127–137. doi:10.1016/S0092-8674(03)00159-4
22. Wotton D, Merrill JC. Pc2 and SUMOylation. Biochem Soc Trans. 2007;35(6):1401–1404. doi:10.1042/BST0351401
23. van Wijnen AJ, Bagheri L, Badreldin AA, et al. Biological functions of chromobox (CBX) proteins in stem cell self-renewal, lineage-commitment, cancer and development. Bone. 2021;143:115659. doi:10.1016/j.bone.2020.115659
24. Li J, Xu Y, Long XD, et al. Cbx4 governs HIF-1α to potentiate angiogenesis of hepatocellular carcinoma by its SUMO E3 ligase activity. Cancer Cell. 2014;25(1):118–131. doi:10.1016/j.ccr.2013.12.008
25. Jiao HK, Xu Y, Li J, et al. Prognostic significance of Cbx4 expression and its beneficial effect for transarterial chemoembolization in hepatocellular carcinoma. Cell Death Dis. 2015;6(3):e1689. doi:10.1038/cddis.2015.57
26. Chen Y, Du J, Wang Y, et al. MicroRNA-497-5p induces cell cycle arrest of cervical cancer cells in S phase by targeting CBX4. Onco Targets Ther. 2019;12:10535–10545. doi:10.2147/OTT.S210059
27. Zhu M, HuiKe J, Wei W, et al. Polycomb chromobox 4 enhances migration and pulmonary metastasis of hepatocellular carcinoma cell line MHCC97L. Sci China Life Sci. 2014;57(6):610–617. doi:10.1007/s11427-014-4663-9
28. Hu C, Zhang Q, Tang Q, et al. CBX4 promotes the proliferation and metastasis via regulating BMI-1 in lung cancer. J Cell Mol Med. 2020;24(1):618–631. doi:10.1111/jcmm.14771
29. Wang Z, Fang Z, Chen G, et al. Chromobox 4 facilitates tumorigenesis of lung adenocarcinoma through the Wnt/β-catenin pathway. Neoplasia. 2021;23(2):222–233. doi:10.1016/j.neo.2020.12.005
30. Wang X, Li L, Wu Y, et al. CBX4 suppresses metastasis via recruitment of HDAC3 to the Runx2 promoter in colorectal carcinoma. Cancer Res. 2016;76(24):7277–7289. doi:10.1158/0008-5472.CAN-16-2100
31. Wang X, Qin G, Liang X, et al. Targeting the CK1α/CBX4 axis for metastasis in osteosarcoma. Nat Commun. 2020;11(1):1141. doi:10.1038/s41467-020-14870-4
32. Sanyal S, Mondal P, Sen S, et al. SUMO E3 ligase CBX4 regulates hTERT-mediated transcription of CDH1 and promotes breast cancer cell migration and invasion. Biochem J. 2020;477(19):3803–3818. doi:10.1042/BCJ20200359
33. Zheng Z, Qiu K, Huang W. Long non-coding RNA (lncRNA) RAMS11 promotes metastatis and cell growth of prostate cancer by CBX4 complex binding to Top2α. Cancer Manag Res. 2021;13:913–923. doi:10.2147/CMAR.S270144
34. Zhao W, Ma B, Tian Z, et al. Inhibiting CBX4 efficiently protects hepatocellular carcinoma cells against sorafenib resistance. Br J Cancer. 2021;124(7):1237–1248. doi:10.1038/s41416-020-01240-6
35. Zhu J, Li L, Tong J, et al. Targeting the polycomb repressive complex-2 related proteins with novel combinational strategies for nasopharyngeal carcinoma. Am J Cancer Res. 2020;10(10):3267–3284.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.