Back to Journals » Vascular Health and Risk Management » Volume 15
How To Support Smoking Cessation In Primary Care And The Community: A Systematic Review Of Interventions For The Prevention Of Cardiovascular Diseases
Authors Odorico M, Le Goff D ![]() , Aerts N
, Aerts N ![]() , Bastiaens H
, Bastiaens H ![]() , Le Reste JY
, Le Reste JY
Received 3 July 2019
Accepted for publication 14 September 2019
Published 31 October 2019 Volume 2019:15 Pages 485—502
DOI https://doi.org/10.2147/VHRM.S221744
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Video abstract presented by Michele Odorico.
Views: 1015
Michele Odorico,1 Delphine Le Goff,1 Naomi Aerts,2 Hilde Bastiaens,2 Jean Yves Le Reste1
1Department of General Practice, EA 7479 SPURBO, Université de Bretagne Occidentale (UBO – University of West Brittany), Brest, France; 2Department of Primary and Interdisciplinary Care, University of Antwerp, Antwerp, Belgium
Correspondence: Michele Odorico
Department of General Practice, EA 7479 SPURBO, Université de Bretagne Occidentale (UBO – University of West Brittany), 22 rue Camille Desmoulins, Brest 29238, France
Tel +33644973078
Email [email protected]
Introduction: Smoking is a major risk factor for cardiovascular diseases (CVDs) and for many types of cancers. Despite recent policies, 1.1 billion people are active smokers and tobacco is the leading cause of mortality and illness throughout the world. The aim of this work was to identify smoking cessation interventions which could be implemented in primary care and/or at a community level.
Methods: A systematic review of CVDs prevention guidelines was realized using the ADAPTE Process. These were identified on G-I-N and TRIP databases. Additionally, a purposive search for national guidelines was successfully undertaken. Guidelines focusing on non-pharmacological lifestyle interventions, published or updated after 2011, were included. Exclusion criteria were specific populations, management of acute disease and exclusive focus on pharmacological or surgical interventions. After appraisal with the AGREE II tool, high-quality guidelines were included for analysis. High-grade recommendations and the supporting bibliographic references were extracted. References had to be checked in detail where sufficient information was not available in the guidelines.
Results: Nine hundred and ten guidelines were identified, 47 evaluated with AGREE II and 26 included. Guidelines recommended that patients quit smoking and that health care professionals provided advice to smokers but failed to propose precise implementation strategies for such recommendations. Only two guidelines provided specific recommendations. In the guideline bibliographic references, brief advice (BA) and multiple session strategies were identified as effective interventions. These interventions used Prochaska theory, motivational interviewing or cognitive-behavioral therapies. Self-help documentation alone was less effective than face-to-face counseling. Community-based or workplace public interventions alone did not seem effective.
Discussion: Behavioral change strategies were effective in helping patients to give up smoking. BA alone was less effective than multiple session strategies although it required fewer resources. Evidence for community-based interventions effectiveness was weak, mainly due to the lack of robust studies.
Keywords: cardiovascular diseases, primary prevention, smoking cessation, primary health care
Introduction
Cardiovascular diseases (CVDs) are the leading cause of mortality worldwide. In 2016, they were responsible of 17.9 million of deaths, 31% of global mortality. Over 75% of deaths due to CVDs take place in low- and middle-income countries.1 In the last 20 years, mortality in low- and middle-income countries shifted from infectious diseases to CVDs. Current age standardized mortality rates in low-income countries are higher than those in developed countries.2 Additionally, global mortality by CVDs is expected to grow. By the year 2030, non-communicable diseases are projected to account for more than 75% of deaths worldwide, the majority being the result of CVDs.2
CVDs can be prevented by acting on modifiable risk factors. Tobacco consumption is a major risk factor for CVDs.1,3 The benefits of stopping smoking have a broad evidence base. Smoking cessation has been proved to be effective in reducing CVD-related morbidity and mortality.4,5,6,7 Smoking cessation is one of the most effective preventive measures: in secondary prevention it could reduce the risk of a new cardiovascular event by almost half.4
Considerable efforts have been made in recent years to control the epidemic in tobacco use. In 2003, the WHO adopted the WHO Framework Convention on Tobacco Control. It targeted national and regional organizations, providing the guiding principles required to reduce the prevalence of tobacco use. In 2008, the WHO proposed the MPOWER, a practical tool to implement this framework: monitor tobacco use and prevention policies, protect people from tobacco, offer help to quit, warn about the dangers, enforce bans on advertising, promotion and sponsorship, and raise taxes. Practical actions were price and tax measures, packaging and labelling regulations, smoking restriction in public places, advertising restrictions, provision of educational campaigns and cessation services.8,9 In 2019, 136 countries have implemented at least one of the key interventions to reduce tobacco demand.10
Despite recent policies, smoking is still a concern worldwide. 1.1 billion people are active smokers in 2019, 80% of them living in low- and middle-income countries. Total tobacco-attributable deaths increased from 5.4 million in 2004 to more than 8 million in 2019, representing the leading cause of death, illness and impoverishment.10,11 Tobacco use contributes to poverty via the direct cost of purchasing tobacco, the health care costs for tobacco-related diseases, as well as the lost human capital that results from morbidity and mortality.10,11 In high-income countries, the number of smokers is still high. In Europe, in 2016, 28.7% of the overall population smoked and tobacco was the leading cause of preventable death and disease in the UK.12,13
SPICES (Scaling-up Packages of Interventions for Cardiovascular disease prevention in selected sites in Europe and Sub-Saharan Africa) is an international implementation research project on CVDs non-pharmacological primary prevention. Different settings are involved in high and low- middle-income countries: France, United Kingdom, Belgium, Uganda and South Africa.
SPICES interventions will target the individual and the community level. Concerning smoking, this is the less implemented measure of the MPOWER: in 2019, only 23 countries were providing cessation services at the best-practice level.10
First step was to identify non-pharmacological effective interventions for CVDs primary prevention.14 The aim of this work was to identify evidence-based non-pharmacological effective smoking cessation interventions and their implementation strategies for use in a primary care setting and/or at a community level.
Materials And Methods
A systematic review of international CVD prevention guidelines and national guidelines of each participating country was carried out between September 2017 and January 2018 following the PRISMA statements criteria and using the ADAPTE procedure.15,16 The ADAPTE procedure provides a systematic approach to ensure quality standards for guideline development, evaluation and implementation.17 TRIP (Turning Research Into Practice) and G-I-N (Guidelines International Network) databases were searched for international guidelines. A purposive search for national guidelines was carried out using national health authority websites: the Haute Autorité de Santé for France; the Tijdschrift Huisarts and Nederland Huisartsen Genootschap guidelines for the Flemish part of Belgium; the National Institute for Care and Excellence (NICE) for United Kingdom; the European Society of Cardiology (ESC) within European countries and the WHO for Uganda. The South African researchers ensured that ESC guidelines were used in South Africa. Databases were searched for guidelines focusing on CVDs prevention and/or management of CVD risk factors, such as diabetes, hypertension, smoking, sedentary lifestyle, unhealthy diet, excess weight and obesity. Detailed research equations for each database are available in Annexure 1.
Guideline titles and summaries were analyzed for eligibility. Inclusion criteria were guidelines focusing on CVD primary prevention and/or management of CVD risk factors in an adult general population and to be applied in primary care or in a community setting. Only those published after 01/01/2012 were included. If different versions of the same guideline were found, only the most recent revision was included.
Exclusion criteria included; exclusive focus on specific populations (geriatric, infantile, socially deprived, etc.) or on secondary or tertiary prevention, exclusive focus on cardiovascular risk assessment, on pharmacological or surgical interventions, or on management of acute disease. Guidelines on specific conditions (eg, type 1 diabetes and familial hypercholesterolemia) were excluded as were those published before 01/01/2012 and not updated. The consortium agreed on this date in order to focus on recent guidelines with the most recently updated data. The research team considered that guideline authors would have reviewed and included literature published before 2012, so that no relevant data would have been missed.
Only guidelines published in English, French or Dutch were included. The lack of free full-text availability was an exclusion criterion as the research team assumed that a clinical practice guideline should be freely available. Two researchers completed this search independently, merging at the end.
Following the ADAPTE procedure, screened guidelines were eligible for quality evaluation with the AGREE II instrument (Appraisal of Guidelines for Research & Evaluation).18 AGREE II is a tool that assesses the quality of guidelines by evaluating their methodological rigor and transparency. It consists of 23 key items organized within 6 domains followed by a global rating (overall assessment [OA]). Each item is rated on a 7-point scale (7 being the best possible quality).
Full-text screened guidelines were evaluated independently by at least two researchers working blind and merging at the end. After discussion within the SPICES consortium, final inclusion was based on OA scores. We included guidelines with all OA scores superior or equal to 5 were excluded those with all OA scores below 5 or with OA scores around cut-off (one score of 4 and one of 5). Discrepant OA scores (more than 1-point difference and one score above 4) were discussed between appraisers and inclusion was based on a consensual decision taken with the researchers and a scientific committee of three senior researchers.
Data Extraction And Analysis
The included guidelines were analyzed, following the ADAPTE procedure, and a matrix of the extracted recommendations was created in order to facilitate the analysis.
Recommendations were included if they had an A or B level of evidence or 1++, 1+, 2++, 2+ for the NICE grading system and/or “Class 1” or “Strong” (regardless of the level of evidence). Bibliographic references which supported the included recommendations were listed to make further details on implementation strategies accessible. For guidelines without recommendation grades, references were included if they referred to randomized or non-randomized controlled trials, interventional cohort studies, or systematic reviews of such studies. Where few strategies had been described in the guidelines or where the description was too concise, the analysis of the full-text articles, from which the guidelines had been issued, was added. The aim was to fully describe the interventions used in such articles.
For these articles, inclusion and exclusion criteria were defined. Studies with a non-pharmacological lifestyle intervention for the primary prevention of CVDs in a general, adult population were included. Main outcomes had to be pertinent to primary care or commonly used for CVD risk assessment. Interventions had to be implemented in a primary care or community setting and had to be effective with a significant statistical difference. The objective of this work was the identification of effective interventions. Non-interventional studies and those on specific populations and on secondary or tertiary prevention population were excluded, as were studies in a hospital/clinic or university context or where patients were constantly monitored or supervised because that was deemed not feasible in a primary care context. Publication date was not an exclusion criterion. When different articles dealt with the same intervention they were identified, and duplicates were removed. Full-text articles were obtained on PubMed or via the University Web Library. If not available, the article in paper format was ordered via the library of the Université de Bretagne Occidentale.
Interventions and implementation strategies used in the included references were searched through the articles, especially in the method section, and described in detail and then summarized. Information was collected on the frequency and duration of the intervention, on the setting (eg, workplace or public event, individual or group sessions), on the material used (informative material, leaflets or videos), on the psychological model used and if mass media were involved. The status and background training (if provided) of those carrying out the interventions were noted. All data were collected in an excel matrix file.
Results
Guidelines selection process is shown in the PRISMA Flowchart (Figure 1).
 |
Figure 1 PRISMA Flowchart showing the guidelines selection process. |
Forty-seven guidelines were screened for quality evaluation with AGREE II tool. Full results are available in Annexure 2. Twenty-six guidelines on CVD primary prevention were included based on their AGREE II overall score (Table 1). They were to be considered among the best quality and the most pertinent for primary CVD prevention in a primary care or community setting.
 |
Table 1 Included Guidelines For CVD Prevention |
Guideline Analysis
Sixteen guidelines provided no recommendations on smoking. They focused on other risk factors, such as excess weight, sedentary lifestyle and unhealthy diet.19,20,23,26,28,30,35,36,38,39,41,43,31,32,33,34
Other guidelines recommended smoking cessation to prevent CVDs. It was recommended for all health care providers to advise smokers to quit, to provide information about methods to aid smoking cessation, including counselling services. Physicians were recommended to prescribe nicotine replacement therapy when indicated. No details, or very few, were found in the guidelines on how to advise smokers.21,25,27,29,37,42 Two guidelines focusing on smoking provided more detailed recommendations.22,40 The following recommendations were identified:
- It was recommended to assess smoking status in all patients and their families and to use the Fagerstrom test (2 or 6 questions) to assess tobacco addiction (grade A).
- If smoking cessation is not attainable, smoking reduction should be the target, as an intermediate step towards quitting completely (grade B).
- Health care professionals were recommended to provide consultations dedicated to giving up smoking. The use of different techniques was recommended, such as counselling, psychological support, cognitive-behavioral therapy or motivational interviewing. Goals should be agreed with the patient and self-help documents should be provided. Past experiences, individual preferences and bio-psycho-social status should be taken into consideration (grade A).
- Intervention should be matched to the behavioral stage of change of the smoker concerned (according to the Prochaska and DiClemente model44) and have an initial, intensive phase (weekly consultations) followed by a maintenance phase lasting 3 to 6 months (monthly sessions) (grade B).
- Health care professionals should appraise themselves of the level of knowledge found within the community regarding beliefs held about smoking and other CVD risk factors.
- Phone and/or internet follow-up and self-help, using eHealth technologies, could be alternatives even though they may be slightly less effective than face-to-face interventions (grade B).
- It was recommended to involve media and public educational campaigns (grade A) and schools (grade B) as part of multicomponent strategies to promote healthy lifestyles. School personnel and health care providers were recommended to set the example and to avoid smoking at work (class 1, grade A).
ESC guidelines provided public health recommendations which dealt with law making (eg, ban smoking in public places and set higher taxes on tobacco) and were consequently excluded because they were considered infeasible on a primary care level.5 NICE PH49 provided general recommendations on behavioral approaches (such as social support) and on health care system organization but no detailed interventions for stopping smoking.24
References Analysis
One thousand eighty-one articles were identified of all 26 included guidelines for CVD prevention. After inclusion and exclusion criteria had been applied, 310 articles were included. Sixty-three included targeting smoking in their intervention. Seventeen studies were excluded from this analysis either because they presented no smoking-related outcomes (N=5) or they showed no significant differences for such outcomes (N=12). They were first included because the intervention was effective for other outcomes. Finally, 46 studies providing an effective smoking cessation intervention were included for analysis.
Interventions Description
Interventions and implementation strategies were described in detail and then summarized.
Fifteen studies provided a multicomponent intervention (targeting multiple risk factors) including an effective smoking cessation component and 31 studies targeted smoking only.
All interventions targeted a modification of the risk behavior related to smoking. They can be classified as behavioral change communication strategies.
Although interventions were heterogenous among included articles, some types of strategies were identified: self-help strategies alone, brief advice (BA), multiple sessions behavioral change strategies and community-based interventions.
Self-help strategies are presented in Table 2. These articles studied self-help strategies alone without face-to-face counseling.
 |
Table 2 Included Articles (Alphabetical Order) With A Self-Help Intervention |
Self-help documentation focused on the need to make a personal decision, the steps to successful quitting, the frequent need for repeated efforts, and the importance of setting a specific quit date and using substitutes for smoking. Self-help approaches were less effective compared with face-to-face counseling.47
BA was defined as one or two short individual consultations to provide information on the potential harm caused by smoking, advice on how to quit and on where to search for help. BA strategies are presented in Table 3.
 |
Table 3 Included Articles (Alphabetical Order) With A Brief Advice Intervention |
BA was more effective than usual care (including very brief advice): results for RCT with intention to treat analysis (ITT) showed 4% to 11% more continuous abstinence at 12 months of follow-up. The measure of exhaled carbon monoxide showed it to be slightly, but non-significantly, more effective than BA alone, while BA plus lung age estimation with a portable spirometer was more effective than BA alone.49,54
Multiple session behavioral change strategies (Table 4) were implemented as a series of meetings with participants to raise awareness of behavioral risk, to help them change and prevent relapse.
 |
Table 4 Included Articles (Alphabetical Order) With A Multiple Session Intervention |
The study from Hollis et al was included in both the self-help and the multiple session strategies as it implemented both interventions effectively.45
Based on RCTs with ITT results, multiple session behavioral change strategies were more effective than usual care (+3 to 9% on 12 months continuous abstinence) but also than BA (+4 to 5%).
Eight studies focused on workplace (Table 5) for the implementation of multiple session strategies. The workplace was specified in order to link individual strategies with interventions, targeting all workers, such as workplace information campaigns (posters), newsletters, smoking restricted areas, local media campaign and social support among employees.78,79,80,81,82 Trained employees were successfully involved in the organization and intervention.80,81
 |
Table 5 Included Articles (Alphabetical Order) With A Multiple Session Intervention At The Workplace |
Three studies were linked in financial incentives but they did not seem very effective when compared with behavioral strategies.78,82,83 Three studies provided a BA intervention at the workplace, but with no or less involvement of the workplace structure and management.50,51,60
Community-Based Interventions
These were public interventions such as public campaigns carried out in the community and/or in workplaces (Table 6). They targeted the global CVD risk and were multi-component (diet, sedentary lifestyle, smoking).85,86,87,88,89
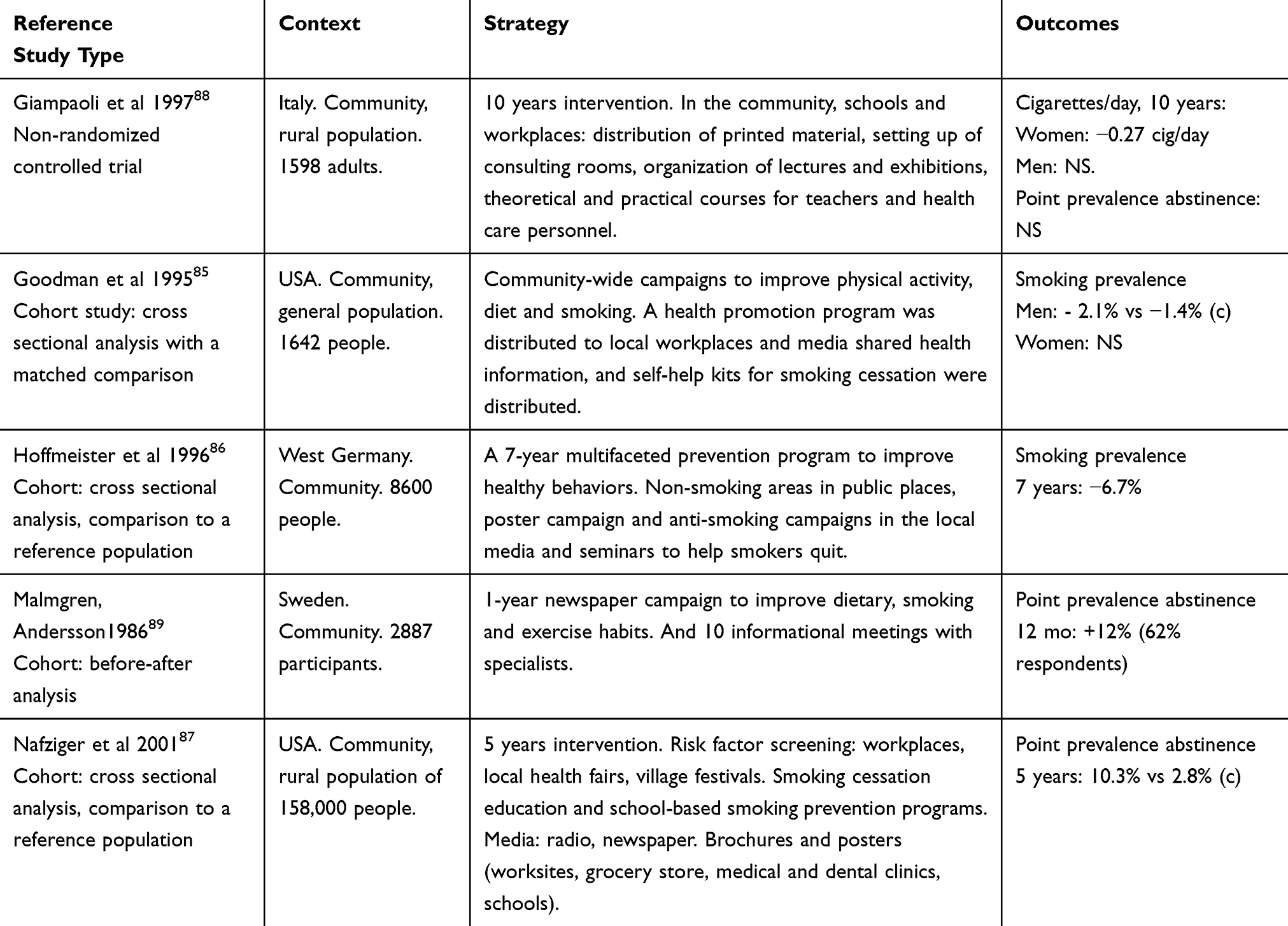 |
Table 6 Included Articles (Alphabetical Order) With Community-Based Interventions |
The efficacy of such interventions was unclear: none of the included studies was an RCT and none showed any statistical difference on continuous abstinence but only on point prevalence abstinence (last 7 days reported consumption).
Discussion
The objective of this work was to identify effective non-pharmacological interventions for smoking cessation to be used in a primary care or a community setting. A systematic review of guidelines, following the ADAPTE Process, included the best quality CVD prevention guidelines adapted to such settings. Health care professionals were recommended to screen for smoking, to give advice and support and to prescribe NRT when indicated. Guidelines globally failed to provide clear and detailed strategies to implement such recommended advice and support. Plus, they were centered on health care professionals. Recommendations for changes to law and to taxation were deemed infeasible in a primary care or community context and were excluded. Two guidelines only provided more detailed recommendations, such as the use of behavioral change strategies with an intensive and a maintenance phase, as well as the use of techniques such as motivational interviewing or the Prochaska stage of change theory.22,40
References analysis made it possible to specify implementation strategies for these recommendations. Although the included articles were seen to be heterogeneous in terms of the interventions, the settings and the outcomes, four main behavioral change strategies were identified.
Self-help materials showed a small positive effect in this review and in the literature, but they were less effective than face-to-face counseling.47,63,76,78,90 BA and multiple session behavioral change strategies were found to achieve better results than usual care or very BA (ie, 30 s to a couple of minutes).45,52,73 Relative risk (RR) for physician advice has been estimated to be 1.66 for smoking cessation.91 Such interventions seemed even more effective when a defined behavioral change technique was used (motivational interviewing, “Five A’s”, Prochaska model or cognitive-behavioral therapy).52,68,73 This was consistent with evidence in the literature summarized in two recent Cochrane reviews.92,93 More intensive multiple session strategies were more successful than BA.66 Similar results were found by other systematic reviews either for group or individual sessions: RR for abstinence was 1.22 to 1.57 for more intensive interventions compared with simple advice.91,94,95,96 It should also be taken into consideration that the more intensive the intervention it is, the more it impacts on time and resources.
Several effective workplace interventions were found in this review. Despite this, the role of the “workplace” itself in this effect was still unclear. Best quality studies, implementing effective workplace interventions in our review included multiple session behavioral change strategies. Implemented interventions might be as effective whether offered in the workplace or elsewhere.97 Spirometric lung age estimation was effective when added to BA in one study, but lung age did not differ among those who quit and those who did not. Smokers with poorer lung age were just as likely to quit as those with normal lung age. Other studies failed to show spirometry or lung age effective in promoting smoking cessation.98 Lung age biofeedback effect on smoking is still uncertain and concerns may be raised on the cost-effectiveness ratio.
Progressive and abrupt cessation showed similar long-term results.99 Evidence in the literature was insufficient to advocate aversive smoking techniques.100 Accordingly, only one article included in this review studied overt and symbolic aversion, but due to a small sample and a per protocol analysis, its results need to be interpreted with precaution.61 Money incentives were not very effective and their effect was time-limited.101 They did not seem a pertinent solution.
Diverse health care professionals were effective in leading such behavioral change interventions. This review showed evidence to indicate that trained community workers can successfully lead these interventions.52,66,78,82 This is important for settings where access to health care professionals is difficult.
Community-based public interventions, such as community events, mass media involvement and information campaigns, were identified in this review. They showed positive but small effects in non-controlled or non-randomized controlled trials which limited their strength. A systematic review found that community interventions had no effect, or a very limited effect, on quitting rates among adults. Among the 37 included studies, only 4 used random assignment of communities and largest and best conducted studies failed to detect a significant effect.102 Similarly, exclusive mass media interventions had an unclear effect mainly due to the lack of good quality studies.103 As smoking is also determined by the social context, the community approach still should be part of a smoking cessation project.
This review did not identify any intervention involving social media. The use of social media has been shown to be feasible and acceptable, although data are lacking regarding its effectiveness.104
Recent efforts to reduce smoking focused on anti-tobacco national policies, mass media communication and law-making. Less was done on the individual level. Cessation services were the least implemented component of MPOWER and physician interventions were not routinely provided, even in high-income countries.10,105,106 This review highlighted the efficacy of different behavioral change strategies that can be implemented in primary care and/or in the community. These approaches are highly cost-effective. BA seems more suitable for general practitioners or practice nurses because of the short duration of their consultation (5 to 20 mins in most countries).107 Pharmacists and dentist could play a major role as well.
Multiple session strategies, using a structured behavior change model (Prochaska Transtheoretical model, or motivational interviewing techniques) were seen to be more effective. Since they demand more time, they do not seem suitable for general practitioners worldwide.
This review showed that diverse health care professionals can successfully lead such interventions including lay health community workers.52,66,78,82 Training lay people to provide such behavioral change interventions could be a solution for public health authorities that deal with settings where access to care is difficult, such as low-income countries and regions in developed countries where physician availability is limited. Furthermore, involving lay people could strengthen the community approach of community-based smoking cessation projects.
Strengths And Limitations
International guidelines were reviewed following a validated and systematic protocol including their quality evaluation. Guidelines were selected, where pertinent for primary care or community context, by researchers who are primary care health care professionals (general practitioners and nurses).
This review might carry a selection bias. Studies were included if they showed a significant difference on primary outcomes. This could imply a bias concerning the effectiveness of these interventions. Since the references included arose from high-grade recommendations of the best quality international guidelines, these interventions were considered effective and this bias was therefore limited.
Multiple outcomes were found for smoking cessation interventions and the relevance of some outcomes is debatable and could involve a bias. Seven-day point prevalence abstinence was the most frequently recurring outcome in this review. Biochemical validation was frequent. An expert consensus stated that smoking cessation should be evaluated by 7-day point prevalence abstinence and prolonged abstinence at 6 and 12 months because shorter time intervals carry a very high probability of relapse.108 In this review, this bias concerned community interventions.
A publication bias was possible because this review protocol did not include a grey literature search. Nevertheless, different systematic reviews found similar results for the interventions described in this review.92,93,94
Conclusion
Multiple session behavioral change strategies including follow-up and self-help materials were the most effective interventions for smoking cessation in primary care or community context.
These were based on motivational interviewing, Prochaska and DiClemente stage of change theory or cognitive-behavioral therapies. BA was slightly less effective. Nonetheless, BA involves less time and fewer resources and it is more suitable for primary care. These interventions could be provided by physicians, nurses and other health care professionals. Adequately trained lay health workers were also shown to be successful in providing these interventions. Community-based and workplace public interventions without behavioral change strategies were not effective. Evidence for community-based interventions effectiveness was weak due to the lack of robust studies.
Acknowledgments
The authors would like to acknowledge the SPICES Team: Dr Geofrey Musinguzi, Pr Paul Van Royen, Pr Harm van Marwijk, Dr Linda Gibson, Dr Bowyer Mark, Pr Tholene Sodi, Pr Mbuyiselo Douglas. And the EA 7479 SPURBO team for the systematic review: Lucie Morvan, Anne Catherine Lecuyer, Christelle Le Gaffric, Hélène Roux, Marion Janyk, Nicolas Vimfles, Marion Le Bars, Pol-Maël Falhon, Louis Soulier, Cécile Guérin, Marine Réale, Hugo Vittori, Charlotte Donou, Eloïse Lissillour, Thomas Le Bras, Gabriel Eliot.
Author Contributions
All authors contributed toward data analysis, drafting and revising the paper, gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO - World Health Organisation. Cardiovascular diseases (CVDs). Available from: http://www.who.int/mediacentre/factsheets/fs317/en/. Published 2017.
2. WHO - World Health Organisation. A Global Brief on Hypertension: Silent Killer. Global Public Health Crisis; 2013. Available from: http://chronicconditions.thehealthwell.info/search-results/global-brief-hypertension-silent-killer-global-public-health-crisis.
3. Teo KK, Ounpuu S, Hawken S, et al. Tobacco use and risk of myocardial infarction in 52 countries in the INTERHEART study: a case-control study. Lancet. 2006;368(9536):647–658. doi:10.1016/S0140-6736(06)69249-0
4. Chow CK, Jolly S, Rao-Melacini P, Fox KAA, Anand SS, Yusuf S. Association of diet, exercise, and smoking modification with risk of early cardiovascular events after acute coronary syndromes. Circulation. 2010;121(6):750–758. doi:10.1161/CIRCULATIONAHA.109.891523
5. Piepoli MF, Hoes AW, Agewall S, et al. European guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2016;37(29):2315–2381. doi:10.1093/eurheartj/ehw106
6. Unal B, Critchley JA, Capewell S. Modelling the decline in coronary heart disease deaths in England and Wales, 1981–2000: comparing contributions from primary prevention and secondary prevention. BMJ. 2005;331(7517):614. doi:10.1136/bmj.38561.633345.8F
7. Qiao Q, Tervahauta M, Nissinen A, Tuomilehto J. Mortality from all causes and from coronary heart disease related to smoking and changes in smoking during a 35-year follow-up of middle-aged Finnish men. Eur Heart J. 2000;21(19):1621–1626. doi:10.1053/euhj.2000.2151
8. World Health Organization. WHO framework convention on tobacco control. Geneva; 2003. Available from: https://apps.who.int/iris/bitstream/handle/10665/78302/ea56r1.pdf?sequence=1&isAllowed=y.
9. World Health Organization. MPOWER; 2008. Available from: https://www.who.int/tobacco/mpower/mpower_report_six_policies_2008.pdf.
10. World Health Organization. WHO Report On Global Tobacco Epidemic, 2019; 2019. Available from: https://apps.who.int/iris/bitstream/handle/10665/326043/9789241516204-eng.pdf?ua=1.
11. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. doi:10.1371/journal.pmed.0030442
12. World Health Organization. World Health Statistics data visualizations dashboard. Tobacco smoking. WHO. Available from: http://apps.who.int/gho/data/node.sdg.3-a-viz?lang=en. Published 2016.
13. All Party Parliamentary Group on Smoking & Health. Fact sheets - action on smoking and health. Available from: https://ash.org.uk/information-and-resources/ash-fact-sheets/. Published 2019.
14. Peters DH, Adam T, Alonge O, Agyepong IA, Tran N. Implementation research: what it is and how to do it. BMJ. 2013;347:f6753. doi:10.1136/bmj.f6753
15. Moher D, Liberati A, Tetzlaff J, Altman DG, Altman D. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
16. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100. doi:10.1371/journal.pmed.1000100
17. The ADAPTE Collaboration. The ADAPTE process: resource toolkit for guideline adaptation. Version 2.0. 2009. Available from: http://www.g-i-n.net.
18. Brouwers MC, Kho ME, Browman GP, et al. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010;182(18):E839–E842. doi:10.1503/cmaj.090449
19. Eckel RH, Jakicic JM, Ard JD, et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk. Circulation. 2014;129(25suppl 2):S76–S99. doi:10.1161/01.cir.0000437740.48606.d1
20. Jensen MD, Ryan DH, Apovian CM, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association task force on practice guidelines and the obesity society. Circulation. 2014;129(25Suppl 2):S102–S138. doi:10.1161/01.cir.0000437739.71477.ee
21. Canadian Diabetes Association. Clinical practice guidelines for the prevention and management of diabetes in Canada. 2013. doi:10.1016/S1499-2671(13)00192-5
22. de Santé HA. Arrêt de La Consommation de Tabac : du Dépistage Individuel Au Maintien de l’abstinence En Premier Recours; 2014. Available from: https://www.has-sante.fr/portail/jcms/c_1718021/fr/arret-de-la-consommation-de-tabac-du-depistage-individuel-au-maintien-de-l-abstinence-en-premier-recours.
23. LeFevre ML. Behavioral counseling to promote a healthful diet and physical activity for cardiovascular disease prevention in adults with cardiovascular risk factors: u.s. preventive services task force recommendation statement. Ann Intern Med. 2014;161(8):587. doi:10.7326/M14-1796
24. NICE. Behaviour change: individual approaches. Public health guideline [PH49]. Available from: https://www.nice.org.uk/guidance/ph49. Published 2014.
25. NICE. Cardiovascular disease prevention | guidance and guidelines. 2010. Available from: https://www.nice.org.uk/guidance/ph25.
26. National Health and Medical Research Council. Clinical practice guidelines for the management of overweight and obesity in adults, adolescents and children in Australia. Available from: https://www.nhmrc.gov.au/guidelines-publications/n57. Published 2013.
27. National Vascular Disease Prevention Alliance. Guidelines for the management of absolute cardiovascular disease risk; 2012. Availabe from: https://www.heartfoundation.org.au/images/uploads/publications/Absolute-CVD-Risk-Full-Guidelines.pdf?.
28. Lennon SL, DellaValle DM, Rodder SG, et al. 2015 evidence analysis library evidence-based nutrition practice guideline for the management of hypertension in adults. J Acad Nutr Diet. 2017;117(9):1445–1458.e17. doi:10.1016/j.jand.2017.04.008
29. NICE. Cardiovascular disease: risk assessment and reduction, including lipid modification | guidance and guidelines. Available from: https://www.nice.org.uk/guidance/cg181. Published 2014.
30. NICE. Preventing excess weight gain. Available from: https://www.nice.org.uk/guidance/ng7. Published 2015.
31. NICE. Obesity prevention. Clinical guideline [CG43]. Available from: https://www.nice.org.uk/guidance/cg43. Published 2015.
32. NICE. Physical activity and the environment. Public health guideline [PH8]. Available from: https://www.nice.org.uk/guidance/ph8. Published 2008.
33. NICE. Physical activity: brief advice for adults in primary care. Public health guideline [PH44]. 2013. Available from: https://www.nice.org.uk/guidance/ph44.
34. NICE. Type 2 diabetes prevention: population and community-level interventions. Public health guideline [PH35]. 2011. Available from: https://www.nice.org.uk/guidance/ph35.
35. WHO - World Health Organization. Prevention and control of noncommunicable diseases : guidelines for primary health care in low resource settings. Available from: https://apps.who.int/iris/handle/10665/76173. Published 2012.
36. Brauer P, Connor Gorber S, Shaw E, et al. Recommendations for prevention of weight gain and use of behavioural and pharmacologic interventions to manage overweight and obesity in adults in primary care. CMAJ. 2015;187(3):184–195. doi:10.1503/cmaj.140887
37. Scottish Intercollegiate Guidelines Network. Risk estimation and the prevention of cardiovascular disease. SIGN 149. 2017. Available from: https://www.sign.ac.uk/sign-149-risk-estimation-and-the-prevention-of-cardiovascular-disease.html.
38. Moyer VA. Screening for and management of obesity in adults: U.S. preventive services task force recommendation statement. Ann Intern Med. 2012;157(5):373–378. doi:10.7326/0003-4819-157-5-201209040-00475
39. Community Preventive Services Task Force CPST. Team-based care to improve blood pressure control: recommendation of the community preventive services task force. Am J Prev Med. 2014;47(1):100–102. doi:10.1016/j.amepre.2014.03.003
40. NICE. Smoking: harm reduction. Public health guideline [PH45]. Available from: https://www.nice.org.uk/guidance/ph45. Published 2013.
41. Department of Veterans Affairs D of D. VA/DoD clinical practice guidelines: diagnosis and management of hypertension in the primary care setting; 2014. Available from: https://www.healthquality.va.gov/guidelines/CD/htn/.
42. Department of Veterans Affairs D of D. The management of dyslipidemia for cardiovascular risk reduction (Lipids). Available from: https://www.healthquality.va.gov/guidelines/CD/lipids/. Published 2014.
43. Department of Veterans Affairs D of D. VA/DoD clinical practice guidelines: management of obesity and overweight. Available from: https://www.healthquality.va.gov/guidelines/cd/obesity/. Published 2014.
44. Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward an integrative model of change. J Consult Clin Psychol. 1983;51(3):390–395. doi:10.1037/0022-006X.51.3.390
45. Hollis JF, Lichtenstein E, Mount K, Vogt TM, Stevens VJ. Nurse-assisted smoking counseling and medical settings: minimizing demands on physicians. Prev Med (Baltim). 1991;20(4):497–507. doi:10.1016/0091-7435(91)90047-8
46. Slama K, Karsenty S, Hirsch A. Effectiveness of minimal intervention by general practitioners with their smoking patients: a randomised, controlled trial in France. Tob Control. 1995;4(2):162–169. doi:10.1136/tc.4.2.162
47. Omenn GS, Thompson B, Sexton M, et al. A randomized comparison of Worksite-sponsored smoking cessation programs. Am J Prev Med. 1988; 4(5):261–267. doi:10.1016/S0749-3797(18)31159-0
48. Cohen SJ, Stookey GK, Katz BP, Drook CA, Smith DM. Encouraging primary care physicians to help smokers quit. A randomized, controlled trial. Ann Intern Med. 1989;110(8):648–652. doi:10.7326/0003-4819-110-8-648
49. Jamrozik K, Vessey M, Fowler G, Wald N, Parker G, Van Vunakis H. Controlled trial of three different antismoking interventions in general practice. Br Med J (Clin Res Ed). 1984;288(6429):1499–1503. doi:10.1136/bmj.288.6429.1499
50. Kadowaki T, Watanabe M, Okayama A, Hishida K, Ueshima H. Effectiveness of smoking-cessation intervention in all of the smokers at a worksite in Japan. Ind Health. 2000;38(4):396–403. doi:10.2486/indhealth.38.396
51. Lang T, Nicaud V, Slama K, et al. Smoking cessation at the workplace. Results of a randomised controlled intervention study. Worksite physicians from the AIREL group. J Epidemiol Community Health. 2000;54(5):349–354. doi:10.1136/JECH.54.5.349
52. Louwagie GMC, Okuyemi KS, Ayo-Yusuf OA. Efficacy of brief motivational interviewing on smoking cessation at tuberculosis clinics in Tshwane, South Africa: a randomized controlled trial. Addiction. 2014;109(11):1942–1952. doi:10.1111/add.12671
53. Maguire TA, McElnay JC, Drummond A. A randomized controlled trial of a smoking cessation intervention based in community pharmacies. Addiction. 2001;96(2):325–331. doi:10.1080/09652140020021062
54. Ojedokun J, Keane S, O?Connor K. Lung age bio-feedback using a portable lung age meter with brief advice during routine consultations promote smoking cessation? Know2quit multicenter randomized control trial. J Gen Pract. 2013;01(03):1–5. doi:10.4172/2329-9126.1000123
55. Pieterse ME, Seydel ER, DeVries H, Mudde AN, Kok GJ. Effectiveness of a minimal contact smoking cessation program for dutch general practitioners: a randomized controlled trial. Prev Med (Baltim). 2001;32(2):182–190. doi:10.1006/pmed.2000.0791
56. Russell MA, Wilson C, Taylor C, Baker CD. Effect of general practitioners’ advice against smoking. Br Med J. 1979;2(6184):231–235. doi:10.1136/bmj.2.6184.231
57. Severson HH, Peterson AL, Andrews JA, et al. Smokeless tobacco cessation in military personnel: A randomized controlled trial. Nicotine Tob Res. 2009;11(6):730–738. doi:10.1093/ntr/ntp057
58. Vetter NJ, Ford D. Smoking prevention among people aged 60 and over: a randomized controlled trial. Age Ageing. 1990;19(3):164–168. doi:10.1093/ageing/19.3.164
59. Wilson DH, Wakefield MA, Steven ID, Rohrsheim RA, Esterman AJ, Graham NM. Sick of Smoking”: evaluation of a targeted minimal smoking cessation intervention in general practice. Med J Aust. 1990;152(10):518–521. doi:10.5694/j.1326-5377.1990.tb125351.x
60. Windsor RA, Lowe JB, Bartlett EE. The effectiveness of a worksite self-help smoking cessation program: a randomized trial. J Behav Med. 1988;11(4):407–421. doi:10.1007/BF00844939
61. Barbarin OA. Comparison of symbolic and overt aversion in the self-control of smoking. J Consult Clin Psychol. 1978;46(6):1569–1571. doi:10.1037/0022-006X.46.6.1569
62. Canga N, De Irala J, Vara E, Duaso MJ, Ferrer A, Martínez-González MA. Intervention study for smoking cessation in diabetic patients: a randomized controlled trial in both clinical and primary care settings. Diabetes Care. 2000;23(10):1455–1460. doi:10.2337/diacare.23.10.1455
63. Cinciripini PM, Lapitsky LG, Wallfisch A, Mace R, Nezami E, Van Vunakis H. An evaluation of a multicomponent treatment program involving scheduled smoking and relapse prevention procedures: initial findings. Addict Behav. 1994;19(1):13–22. doi:10.1016/0306-4603(94)90047-7
64. Cinciripini PM, Lapitsky L, Seay S, Wallfisch A, Kitchens K, Van Vunakis H. The effects of smoking schedules on cessation outcome: can we improve on common methods of gradual and abrupt nicotine withdrawal? J Consult Clin Psychol. 1995;63(3):388–399. doi:10.1037/0022-006X.63.3.388
65. Hilberink SR, Jacobs JE, Bottema BJAM, de Vries H, Grol RPTM. Smoking cessation in patients with COPD in daily general practice (SMOCC): six months’ results. Prev Med (Baltim). 2005;41(5–6):822–827. doi:10.1016/j.ypmed.2005.08.003
66. Hollis JF, McAfee TA, Fellows JL, Zbikowski SM, Stark M, Riedlinger K. The effectiveness and cost effectiveness of telephone counselling and the nicotine patch in a state tobacco quitline. Tob Control. 2007;16:53–59. doi:10.1136/tc.2006.019794
67. Marcus BH, Albrecht AE, King TK, et al. The efficacy of exercise as an aid for smoking cessation in women: a randomized controlled trial. Arch Intern Med. 1999;159(11):1229–1234. doi:10.1001/archinte.159.11.1229
68. Marks DF, Sykes CM. Randomized controlled trial of cognitive behavioural therapy for smokers living in a deprived area of London: outcome at one-year follow-up. Psychol Health Med. 2002;7(1):17–24. doi:10.1080/13548500120101513
69. Meyer AJ, Nash JD, McAlister AL, Maccoby N, Farquhar JW. Skills training in a cardiovascular health education campaign. J Consult Clin Psychol. 1980;48(2):129–142. doi:10.1037/0022-006X.48.2.129
70. Neaton JD, Broste S, Cohen L, Fishman EL, Kjelsberg MO, Schoenberger J. The multiple risk factor intervention trial (MRFIT): VII. A comparison of risk factor changes between the two study groups. Prev Med (Baltim). 1981;10(4):519–543. doi:10.1016/0091-7435(81)90063-3
71. Nohlert E, Å T, Tillgren P, Johansson P, Rosenblad A, Helgason ÁR. Comparison of a high and a low intensity smoking cessation intervention in a dentistry setting in Sweden – a randomized trial. BMC Public Health. 2009;9(1):121. doi:10.1186/1471-2458-9-121
72. Perkins KA, Marcus MD, Levine MD, et al. Cognitive-behavioral therapy to reduce weight concerns improves smoking cessation outcome in weight-concerned women. J Consult Clin Psychol. 2001;69(4):604–613.
73. Soria R, Legido A, Escolano C, López Yeste A, Montoya J. A randomised controlled trial of motivational interviewing for smoking cessation. Br J Gen Pract. 2006;56(531):768–774.
74. Steptoe A, Doherty S, Rink E, Kerry S, Kendrick T, Hilton S. Behavioural counselling in general practice for the promotion of healthy behaviour among adults at increased risk of coronary heart disease: randomised trial. BMJ. 1999;319(7215):
75. Wood DA, Kinmonth AL, Davies GA, et al. Randomised controlled trial evaluating cardiovascular screening and intervention in general practice: principal results of British family heart study. Family Heart Study Group. BMJ. 1994;308(6924):313–320. doi:10.1136/BMJ.308.6924.313
76. Wu D, Ma GX, Zhou K, Zhou D, Liu A, Poon AN. The effect of a culturally tailored smoking cessation for Chinese American smokers. Nicotine Tob Res. 2009;11(12):1448–1457. doi:10.1093/ntr/ntp159
77. Cornuz J, Humair J-P, Seematter L, et al. Efficacy of resident training in smoking cessation: a randomized, controlled trial of a program based on application of behavioral theory and practice with standardized patients. Ann Intern Med. 2002;136(6):429–437. doi:10.7326/0003-4819-136-6-200203190-00006
78. Jason LA, Salina D, McMahon SD, Hedeker D, Stockton M. A worksite smoking intervention: a 2 year assessment of groups, incentives and self-help. Health Educ Res. 1997;12(1):129–138. doi:10.1093/her/12.1.129
79. Bertera RL. Behavioral risk factor and illness day changes with workplace health promotion: two-year results. Am J Heal Promot. 1993;7(5):365–373. doi:10.4278/0890-1171-7.5.365
80. Erfurt JC, Foote A, Heirich MA. Worksite wellness programs: incremental comparison of screening and referral alone, health education, follow-up counseling, and plant organization. Am J Heal Promot. 1991;5(6):438–448. doi:10.4278/0890-1171-5.6.438
81. Jason LA, Gruder CL, Martino S, Flay BR, Warnecke R, Thomas N. Work site group meetings and the effectiveness of a televised smoking cessation intervention. Am J Community Psychol. 1987;15(1):57–72. doi:10.1007/BF00919757
82. Jason LA, Lesowitz T, Michaels M, et al. A worksite smoking cessation intervention involving the media and incentives. Am J Community Psychol. 1989;17(6):785–799.doi:10.1007/BF00922738
83. Gomel M, Oldenburg B, Simpson JM, Owen N. Work-site cardiovascular risk reduction: a randomized trial of health risk assessment, education, counseling, and incentives. Am J Public Health. 1993;83(9):1231–1238. doi:10.2105/AJPH.83.9.1231
84. Groeneveld IF, Proper KI, van der Beek AJ, Hildebrandt VH, van Mechelen W. Short and long term effects of a lifestyle intervention for construction workers at risk for cardiovascular disease: a randomized controlled trial. BMC Public Health. 2011;11(1):836. doi:10.1186/1471-2458-11-836
85. Goodman RM, Wheeler FC, Lee PR. Evaluation of the heart to heart project: lessons from a community-based chronic disease prevention project. Am J Heal Promot. 1995;9(6):443–455. doi:10.4278/0890-1171-9.6.443
86. Hoffmeister H, Mensink GB, Stolzenberg H, et al. Reduction of coronary heart disease risk factors in the German cardiovascular prevention study. Prev Med (Baltim). 1996;25(2):135–145.
87. Nafziger AN, Erb TA, Jenkins PL, Lewis C, Pearson TA. The Otsego-Schoharie healthy heart program: prevention of cardiovascular disease in the rural US. Scand J Public Health Suppl. 2001;56:21–32.
88. Giampaoli S, Poce A, Sciarra F, et al. Change in cardiovascular risk factors during a 10-year community intervention program. Acta Cardiol. 1997;52(5):411–422.
89. Malmgren S, Andersson G. Who were reached by and participated in a one year newspaper health information campaign? Scand J Soc Med. 1986;14(3):133–140.
90. Hartmann-Boyce J, Lancaster T, Stead LF. Print-based self-help interventions for smoking cessation. Cochrane Database Syst Rev. 2014;(6). doi:10.1002/14651858.CD001118.pub3
91. Stead LF, Buitrago D, Preciado N, Sanchez G, Hartmann-Boyce J, Lancaster T. Physician advice for smoking cessation. Cochrane Database Syst Rev. 2013;(5). doi:10.1002/14651858.CD000165.pub4
92. Rice VH, Heath L, Livingstone-Banks J, Hartmann-Boyce J. Nursing interventions for smoking cessation. Cochrane Database Syst Rev. 2017;12:CD001188. doi:10.1002/14651858.CD001188.pub5
93. Lindson-Hawley N, Thompson TP, Begh R. Motivational interviewing for smoking cessation. Cochrane Database Syst Rev. 2015;(3). doi:10.1002/14651858.CD006936.pub3
94. Stead LF, Carroll AJ, Lancaster T. Group behaviour therapy programmes for smoking cessation. Cochrane Database Syst Rev. 2017;(3). doi:10.1002/14651858.CD001007.pub3
95. Lancaster T, Stead LF. Individual behavioural counselling for smoking cessation. Cochrane Database Syst Rev. 2017;(3). doi:10.1002/14651858.CD001292.pub3
96. Martín Cantera C, Puigdomènech E, Ballvé JL, et al. Effectiveness of multicomponent interventions in primary healthcare settings to promote continuous smoking cessation in adults: a systematic review. BMJ Open. 2015;5(10):e008807. doi:10.1136/bmjopen-2015-008807
97. Cahill K, Lancaster T. Workplace interventions for smoking cessation. Cochrane Database Syst Rev. 2014;(2). doi:10.1002/14651858.CD003440.pub4
98. Bize R, Burnand B, Mueller Y, Rège-Walther M, Camain J-Y CJ. Biomedical risk assessment as an aid for smoking cessation. Cochrane Database Syst Rev. 2012;12:CD004705. doi:10.1002/14651858.CD004705.pub4
99. Lindson-Hawley N, Aveyard P, Hughes JR. Reduction versus abrupt cessation in smokers who want to quit. Cochrane Database Syst Rev. 2012;(11). doi:10.1002/14651858.CD008033.pub3
100. Hajek P, Stead LF. Aversive smoking for smoking cessation. Cochrane Database Syst Rev. 2001;(3). doi:10.1002/14651858.CD000546.pub2
101. Cahill K, Hartmann-Boyce J, Perera R. Incentives for smoking cessation. Cochrane Database Syst Rev. 2015;(5). doi:10.1002/14651858.CD004307.pub5
102. Secker-Walker R, Gnich W, Platt S, Lancaster T. Community interventions for reducing smoking among adults. Cochrane Database Syst Rev. 2002;(2). doi:10.1002/14651858.CD001745
103. Bala MM, Strzeszynski L, Topor-Madry R. Mass media interventions for smoking cessation in adults. Cochrane Database Syst Rev. 2017;(11). doi:10.1002/14651858.CD004704.pub4
104. Naslund JA, Kim SJ, Aschbrenner KA, et al. Systematic review of social media interventions for smoking cessation. Addict Behav. 2017;73:81–93. doi:10.1016/j.addbeh.2017.05.002
105. Lindholm C, Adsit R, Bain P, et al. A demonstration project for using the electronic health record to identify and treat tobacco users. WMJ. 2010;109(6):335–340.
106. Rosenberg G, Crawford C, Bullock S, Petty R, Vohra J Smoking cessation in primary care: a cross-sectional survey of primary care health practitioners in the UK and the use of very brief advice; 2019. Available from: http://www.cancerresearchuk.org/.
107. Irving G, Neves AL, Dambha-Miller H, et al. International variations in primary care physician consultation time: A systematic review of 67 countries. BMJ Open. 2017;7(10):1–15. doi:10.1136/bmjopen-2017-017902
108. Cheung KL, de Ruijter D, Hiligsmann M, et al. Exploring consensus on how to measure smoking cessation. A Delphi study. BMC Public Health. 2017;17(1):890. doi:10.1186/s12889-017-4902-7
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.