")
Back to Journals » Research and Reports in Urology » Volume 15
How to Improve the Quality of Life of Patients with Prostate Cancer Treated with Hormone Therapy?
Authors Turco F, Di Prima L, Pisano C, Poletto S, De Filippis M, Crespi V, Farinea G, Cani M, Calabrese M, Saporita I, Di Stefano RF, Tucci M, Buttigliero C
Received 4 September 2022
Accepted for publication 7 January 2023
Published 19 January 2023 Volume 2023:15 Pages 9—26
DOI https://doi.org/10.2147/RRU.S350793
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Panagiotis J Vlachostergios
Fabio Turco,1,* Lavinia Di Prima,1,* Chiara Pisano,1 Stefano Poletto,1 Marco De Filippis,1 Veronica Crespi,1 Giovanni Farinea,1 Massimiliano Cani,1 Mariangela Calabrese,1 Isabella Saporita,1 Rosario Francesco Di Stefano,1 Marcello Tucci,2 Consuelo Buttigliero1
1Department of Oncology, University of Turin, at Division of Medical Oncology, San Luigi Gonzaga Hospital, Turin, Italy; 2Department of Medical Oncology, Cardinal Massaia Hospital, Asti, Italy
*These authors contributed equally to this work
Correspondence: Marcello Tucci, Department of Medical Oncology, Cardinal Massaia Hospital, Corso Dante Alighieri 202, Asti, 14100, Italy, Tel +393286754734, Email [email protected]
Abstract: Prostate cancer (PC) is a hormone-sensitive tumor. Androgen deprivation therapy (ADT) is the cornerstone of systemic therapy for patients with intermediate or high-risk localized, recurrent, and metastatic prostate cancer. Although generally well tolerated, ADT can lead to short- and long-term adverse events that can worsen the quality of life of patients with PC. In the last decade, the introduction of novel generation androgen receptor pathway inhibitors (ARPI) has resulted in an improvement in the prognosis of patients with metastatic PC when used in combination with ADT. The use of ARPI in increasingly early stages of the disease determines a longer exposure of patients to these treatments. Although ARPIs are normally well-tolerated drugs, they generally cause an increase in toxicity compared to ADT alone, being able to worsen some adverse events already induced by ADT or leading to the development of specific side effects. Although there are no specific treatments for all the adverse events induced by hormonal therapies, it is essential to know the possible toxicities induced by the different treatments and to start procedures to prevent and/or recognize and consequently treat them early in order to not compromise the quality of life of the patients with PC. The aim of this review is to describe the adverse events induced by hormonal therapies. We will first describe the side effects induced by both ADT and ARPI and then the specific adverse events of the different ARPIs. Furthermore, we will try to highlight the possible therapeutic options to prevent or mitigate the toxicity induced by hormone therapies in order to improve the quality of life of the patients with PC.
Keywords: prostate cancer, androgen deprivation therapy, androgen pathway inhibitors, management of adverse events
Introduction
Prostate cancer (PC) is the second most frequent cancer and the leading cause of cancer death among men.1,2 Due to the significant androgens dependence, since 1940 androgen deprivation therapy (ADT) has represented the cornerstone of systemic treatment for men with PC.3 According to the current international guidelines, ADT is used in patients with intermediate or high-risk localized, recurrent and metastatic PC.4,5 About 50% of patients with PC will receive ADT at some point during their treatment.6 ADT consists of bilateral orchiectomy or luteinizing hormone–releasing hormone (LHRH) agonists and antagonists.6,7 LHRH agonists and antagonists act by suppressing the hypothalamic–pituitary–gonadal axis, and consequently lowering the circulating testosterone levels.6,7 After chemical or surgery castration, the incorporation of androgens into the cell nucleus continues, as a result of their production by the adrenal glands. This can be counteracted by adding an antiandrogen to ADT.7,8 First-generation antiandrogens (eg bicalutamide) compete with circulating androgens for binding sites on the androgen receptor (AR) within the prostate cells.8 To date, bicalutamide is used for about a month to prevent the flare-up phenomenon in patients starting LH-RH agonist or as an alternative to ADT in combination with salvage radiotherapy in case of biochemical recurrence after radical prostatectomy.7,8
A better understanding of AR functioning and ADT resistance mechanisms has led to the development of novel generation androgen receptor pathway inhibitors (ARPI) such as abiraterone, enzalutamide, apalutamide and darolutamide.9–13 Initially used only in patients with metastatic PC who became resistant to ADT (metastatic castration-resistant prostate cancer, mCRPC),14–17 ARPI have subsequently been shown to be effective when used in combination with ADT in earlier settings of the disease such as patients with non-metastatic castration resistant (nmCRPC),13,18,19 metastatic hormone-sensitive (mHSPC) disease,10–12,20–25 and recently also in those with high-risk localized disease according to the STAMPEDE criteria.22 The anticipation of ARPIs in earlier stages of the disease resulted in longer exposure and deeper androgen suppression in patients with PC and consequently a higher risk of developing adverse events. For example, in the ARCHES trial, there was an increase in the frequency of adverse events in patients treated with ADT + enzalutamide according to the treatment duration: fatigue, hypertension, cognitive/memory impairment and falls occurred, respectively, in 24.1%, 8.6%, 4.5% and 3.7% of patients after a median treatment duration of 12.8 months21 while after a median treatment duration of 40.2 months they were 32.2%, 14.3%, 6.6% and 10.1%, respectively.23
Although both ADT and ARPI are generally well tolerated, they can still cause both short and long-term adverse events that can compromise quality of life and consequently treatment compliance of patients with PC.24–26 This review aims to describe the adverse events associated with ADT, first-generation antiandrogens and ARPI and to provide evidence-based strategies to mitigate or prevent them in order to try to improve the quality of life of patients with PC.
Cardiovascular Complications
In patients with PC cardiovascular diseases were the most common causes of non PC-related deaths.24,27 The role of ADT as a possible cardiovascular risk factor remains controversial.28–30
LHRH agonists are associated with increased low-density lipoprotein cholesterol and triglyceride levels, increased visceral fat, decreased lean body mass, increased insulin resistance, and decreased glucose tolerance.24,26,31 These changes can accelerate atherosclerosis and predispose the patient to coronary artery disease. ADT has also been associated with both arterial thromboembolic events and venous thromboembolic events, ultimately increasing the rate of acute myocardial infarction, heart failure, and arrhythmias, with overall increased cardiovascular morbidity and mortality.32–35 In a meta-analysis by Zhao et al including over 119.000 PC patients, ADT was associated with a significant risk of cardiovascular mortality [hazard ratio (HR) 1.17, 95% confidence interval (CI) 1.04–1.32, p= 0.01].28 In another meta-analysis, Bosco et al found a 38% increase in cardiovascular disease for patients with PC treated with ADT compared to those without [relative risk (RR) 1.38, 95% CI 1.29–1.48].31 In contrast, in a meta-analysis performed by Nguyen that included over 4.000 patients with PC the use of ADT lowers PC specific and all-cause mortality without increasing risk of cardiovascular death (RR, 0.93; 95% CI, 0.79–1.10; P = 0.41).30
The presence of pre-existing heart disease appears to be a risk factor for development of major adverse cardiac events (MACE) in patients with PC receiving ADT.33–35 O’Farrell et al showed that patients who experienced two or more MACE before initiation of ADT were at highest risk for developing cardiovascular disease during the first six months of therapy compared to an age-matched cohort from the general population.33 Ziehr et al found no association between ADT and cardiac-specific mortality in patients without cardiovascular comorbidity, while patients with a history of congestive heart failure or a previous myocardial infarction treated with ADT had a significantly higher risk of cardiac mortality compared to those without treatment (HR 3.28, 95% CI 1.01–10.64, p=0.048).34 Importantly, even short durations of ADT (3–6 months) appear to increase cardiovascular risk.35
An important area of debate is whether there is a different risk profile for cardiovascular events between LHRH agonists and antagonists. Studies in animal models suggest that LHRH agonists, but not antagonists, may induce atherosclerotic plaque instability and rupture36,37. The rupture of the atherosclerotic plaque is caused by a degradation of the cap connective tissue by infiltrating macrophages. Lymphocytes T-helper 1 (Th1) type are important macrophage activators and are the dominant T-cell type in atherosclerotic plaques. T cells express LHRH receptors, and activation of these receptors has been shown to stimulate T-cell expansion and differentiation into the Th1 phenotype, suggesting that LHRH agonists may promote destabilization of atherosclerotic plaques.38 In the last 3 years, the results of 3 randomized clinical trials have been published that evaluated the cardiovascular toxicity profile of LHRH agonists compared to antagonists.39–41 An open-label Phase 2 study randomized 80 patients with pre-existing MACE, to receive LHRH agonists or antagonists for 1 year and included new cardiovascular events as a secondary end point. In this trial, Margel et al found that patients using a LHRH antagonist were 18% less likely to experience a major cardiovascular or cerebrovascular at 12 months (p=0.032).39 The Phase III HERO trial compared the oral LHRH antagonist relugolix versus leuprolide among 622 patients with advanced PC.40 More than 90% of patients had cardiovascular risk factors and 15% had a history of MACE. In a prespecified safety analysis, patients treated with relugolix had a 2.9% incidence of MACE within the first 12 months of treatment compared to 6.2% in the leuprolide arm, which represented a 54% decrease in risk of developing MACE (HR 0.46, 95% CI 0.24–0.88).40 In patients with a prior medical history of MACE, the incidence of new MACE appeared to be more pronounced in the leuprolide arm (17.8% vs 3.6%).40 The PRONOUNCE trial is the first, international, randomized, Phase 3 trial to prospectively compare the cardiovascular safety of an LHRH antagonist (degarelix) and an LHRH agonist (leuprolide) in patients with PC and preexisting atherosclerotic cardiovascular disease.41 The trial was terminated early because of incomplete accrual and a low event rate. Regardless, subsequent MACE did not differ between antagonist and agonist at 1 year (5.5% v 4.1%, respectively; P= 0.53).41
The increased cardiovascular risk in patients treated with ADT may also be due to the body modifications and metabolic alterations it causes.42–45 ADT in fact determines an increase in body weight and percentage fat mass and a loss of muscle mass configuring the sarcopenic obesity profile. Patients with this metabolic profile have a decrease in absolute muscle strength, aerobic fitness, and general physical function, which overall may contribute to morbidity by increasing falls and fracture risk, which finally may negatively impact on overall survival.42–45 These changes are thought to occur soon after initiating therapy, sometimes as early as one month following treatment and these changes may persist up to two years beyond treatment cessation.45 The metabolic consequences of ADT include insulin resistance and changes to lipid profile with an increase in triglyceride and total cholesterol levels, predisposing to the developing a metabolic syndrome.26 A meta-analysis demonstrated a 75% higher risk of metabolic syndrome and a 36% higher risk of diabetes in patients on ADT compared to controls.42–46 Metformin and statins have been investigated as a potential treatment for ADT-induced metabolic changes with promising results. In a prospective, randomized study of 40 patients with PC, six months of metformin combined with exercise resulted in decreased abdominal girth, BMI, and blood pressure.46 Furthermore, in a systematic review and meta-analysis, He et al showed that ADT with metformin improves overall survival (OS) (HR = 0.72, 95% CI: 0.59–0.88, P = 0.001).47 In a systematic review of nearly 120,000 PC patients statin use was associated with a 27% reduction in the risk of overall mortality (HR 0.73, 95% CI 0.66–0.82).48 However, randomized controlled trials are warranted to validate these findings.
ADT is also associated with a prolongation of the QT interval and, therefore, theoretically increased risk of arrhythmia sudden cardiac death.49
Treatment with ARPI can also lead to an increased cardiovascular risk. In the meta-analysis by Iacovelli et al, including 6 phase 2 and 3 trials testing enzalutamide and abiraterone in mCRPC patients, the addition of ARPI to the ADT resulted in an increase in cardiovascular events of 36% compared with ADT alone (RR 1.36, 95% CI, 1.13–1.64; p=0.001), even if the absolute difference in terms of all- and grade 3–4 events incidence was small (14% and 4%, respectively).50 In particular, the addition of abiraterone resulted in a significant increase in cardiovascular toxicity, whereas enzalutamide does not.50 These results were confirmed by the meta-analysis by Moreira et al.51 The increased cardiovascular risk induced by abiraterone is determined by its mechanism of action. As a result of CYP17 inhibition, as well as a reduction in testosterone levels, abiraterone induces a decrease in glucocorticoid production and a compensatory increase in adrenocorticotrophic hormone (ACTH), resulting in a rise in steroids with mineralocorticoid properties upstream of CYP17A1, which may result in a syndrome of secondary mineralocorticoid excess, characterized by water retention, hypertension and the possible development of heart failure.50 On the other hand, enzalutamide has been associated with statistically significant QTc prolongation (mean increase of 3–6.5 ms from baseline during weeks 5–25).52
In a patient with PC, before starting treatment with ADT, it is important to take a careful medical history to investigate the presence of risk factors or cardiovascular diseases. Basal assessment should consist of blood tests including lipid and glycemic profile, ECG, blood pressure assessment and BMI calculation. In patients with a high cardiovascular risk or with cardiac comorbidities that are not well controlled it may be useful to perform a cardiological evaluation to try to optimize the patient’s cardiovascular profile before starting ADT. In these patients, it may be useful to use LHRH antagonists, although there is no clear evidence for this recommendation. In patients without cardiovascular risk factors, the same recommendations as for the general population are suggested. In particular, it is recommended to perform regular physical activity, to follow a varied and balanced diet, not to smoke and to limit the use of alcohol.24 When it is indicated to add an ARPI to the ADT it is suggested to also perform an echocardiogram. In case of cardiovascular comorbidities or impaired cardiac function, it is recommended to avoid treatment with abiraterone and to prefer another ARPI. In patients with a known history of QT prolongation or patients who are taking medications known to prolong the QT interval monitoring of ECG and serum electrolyte levels at baseline and during treatment with enzalutamide should be considered.52
Bone Health
Hormones play a crucial role in bone homeostasis.53,54 AR is present in chondrocytes and osteoblasts and the activated AR interacts with osteoblast precursors stimulate bone formation through upregulation of transforming growth factor (TGF) -β, insulin-like growth factors-1 (IGF-1) and fibroblast growth factor (FGF) and downregulate Interleukin 6 (IL-6), which stimulates osteoclastogenesis.53,54 Furthermore, dihydrotestosterone has been shown to reduce osteoprotegerin (OPG) levels, which stimulates osteoclast activity.53,54 Therefore, the use of hormone therapies that can reduce androgen levels, such as ADT inevitably, have a negative effect on bone health. From a molecular point of view testosterone deficiency promotes the activation of nuclear factor kappa B ligand (RANKL) production from osteoblasts, which contributes to the promotion of the differentiations and functions in osteoclasts leading to an increase in bone resorption and a reduction in bone mineral density (BMD).55 In addition, low testosterone levels lead to a reduction in the expression of IGF-1 and IGF-binding protein (IGF-BP) in osteoblasts, two molecules essential for differentiation and proliferation of chondrocytes and osteoblasts.53,54 Furthermore, the downregulation of OPG enhances osteoclast recruitment and activation leading to further worsening of bone loss.53,54
ADT-related loss of BMD is estimated to be around 4–6% per year with a more rapid loss during the first year of treatment (5–10%), which significantly exceeds that of normal age-related (0.5–1.0% per year) and postmenopausal women (1–2.3% per year), and is about two-fold that of women with breast cancer treated with aromatase inhibitors.56,57 Through the reduction of BMD, ADT increases the risk for patients with PC of developing osteoporosis and consequently of skeletal fractures. Taylor et al showed in more than 100.000 patients with PC that ADT increased risk of for skeletal fracture (RR 1.23, 95% CI, 1.10–1.38).58 In another large retrospective cohort study, men treated with ADT experienced more fragility fractures than matched controls (10.8% vs 3.2%; p < 0.0001). The use of ADT was also associated with a 1.82-fold increase in risk of hip fracture requiring hospitalisation.59 In addition, fractures are known to be associated with increased mortality risk, and thus may be an important prognostic factor for patients with PC. In fact, patients with PC experiencing a fracture had a 1.38-fold higher overall mortality risk than those who did not (95% CI, 1.34–1.43).55 Additionally, in patients with PC, bone health is frequently already suboptimal before starting ADT due to age and comorbidities. Cheung et al showed that before starting ADT, 11% of patients with PC had osteoporosis and 40% osteopenia.60 These results reflect the need for a thorough screening of bone loss prior to initiation of ADT. The gold standard for measuring BMD is Dual-energy X-ray absorptiometry (DEXA).61 However, in patients treated with ADT the risk of fracture is often independent of DEXA values and it is frequently misclassified when based only on DEXA measurement.62 This occurs because ADT determines not only a reduction in BMD (generally slow and reversible) but also a qualitative damage to the trabecular microstructure (often rapid and not reversible).62,63 In fact, the high bone turnover induced by ADT determines a thinning and then the perforation of bone trabeculae which increases the risk of skeletal fractures which, however, can not be measured by DEXA.63 In fact, in the study by Greenspan et al many of the patients with PC undergoing ADT who experienced a vertebral fracture had fewer trabecular plaques and a higher erosion index than men without fracture despite having a normal BMD value on DEXA.62
In patients with PC treated with ADT, fractures typically occur during the first year and this observation reinforces the fact that skeletal fragility is prominently dependent on rapid microarchitectural damage of the bone trabeculae rather than on the low bone mass.63 To improve fracture risk assessment, the World Health Organization has computed a FRAX algorithm that accounts for demographic risk factors, alcohol/tobacco/glucocorticoid use and other relevant past personal or familial history.63 The FRAX tool calculates the probability of risk for bone fracture for the next 10 years.63 However, this tool does not include ADT treatment among the risk factors for developing skeletal fractures, therefore the FRAX score may also underestimate the risk in patients with PC treated with ADT.63 According to the ESMO guidelines, the management of bone health in patients treated with ADT is based on the criteria of Coleman et al.64 All patients starting ADT should be recommended and adequate calcium intake (1200 mg daily total from diet and supplements) and vitamin D supplementation (800–2000 IU daily). Additionally, patients should be encouraged to make lifestyle changes such as trying to quit smoking, reducing alcohol consumption and increasing physical activity. In patients who have a T score <2 or the presence of at least 2 risk factors for fracture (age >65; T score <-1.5; smoking; BMI <24; family history of hip fracture; personal history of fragility fracture above age 50; oral glucocorticoid use for >6 months) the use of bone-protecting agents (BPA) should be considered.64 In patients who do not meet these criteria, the risk of fractures should be monitored by repeating a DEXA every 1–2 years.64 Since Coleman’s criteria are mainly based on the BMD value and considering that, as previously mentioned, BMD does not exactly reflect the fracture risk, the exclusive use of these criteria to establish the use of BPA can lead to under-treatment in patients with PC treated with ADT. Therefore, BPA should probably be used as primary prevention in all patients who initiate ADT regardless of Coleman’s criteria.65 BPA should be started as soon as possible in patients undergoing ADT considering that most fractures occur within one year of starting ADT. Finally, BPA should be performed for the entire duration of the ADT as the risk of fracture has been shown to increase with increasing duration of ADT. A new DEXA should be performed at the end of ADT to evaluate whether to continue treatment with BPA.65
The most commonly used BPAs to reduce the fracture risk of PC patients treated with ADT are bisphosphonates (eg 70mg alendronic acid per week) and denosumab (60mg every 6 months).55 Bisphosphonates are analogues of pyrophosphate, a normal component of the bone matrix and act by inhibiting the enzyme farnesyl diphosphonate synthase resulting in a reduced ability of the osteoclast to bind to bone, thus compromising their bone resorption activity.61 Instead, denosumab is a human monoclonal RANKL antibody that acts by inhibiting the RANK – RANKL pathway, thus hindering osteoclast activity.61 Bisphosphonates have been shown to be effective in preventing ADT-induced bone, or increasing lumbar spine and hip BMD, although they have not been shown to reduce the risk of fractures.55 Denosumab is the only BPA that showed to reduce the risk of fractures in patients with PC treated with ADT.55 In the multicenter, double-blind HALT trial denosumab every six months showed to reduce the incidence of new vertebral fractures at 3 years by 62% compared with placebo (relative risk 0.38, 95% CI 0.19–0.78, p = 0.006) in patients with non-metastatic PC undergoing ADT.66 Finally, in patients with metastatic castration-resistant PC (mCRPC), bisphosphonates (eg zoledronate 4mg every 4 weeks) and denosumab (120mg every 4 weeks) are used to reduce skeletal-related events, such as pathological fracture, radiotherapy to bone, surgery to bone, spinal cord compression and hypercalcaemia.67,68
While the relationship between ADT and bone health is known, there is little evidence on the effect of antiandrogens and ARPIs. In a prospective observational study, LHRH agonist plus bicalutamide did not result in a significant increase in osteopenia or osteoporosis compared to LHRH agonist alone in 312 patients with PC (p= 0.3688).69 On the contrary, Wang et al observed a 2.11-fold increase in fracture risk among patients treated with antiandrogens alone and the combination of LHRH agonist and antiandrogen had the greatest risk of fracture compared to antiandrogen and LHRH agonist monotherapy (OR = 3.48; 95% CI 3.07–3.96).59 There is also little evidence on the effect of intermittent ADT on bone health, although some results seem to suggest that it may lead to a reduction in fracture risk compared to continuous ADT.70 Results from PROSPER and SPARTAN trials suggest that treatment with ARPI further increases the fracture risk in patients with non-metastatic castration-resistant PC treated with long term ADT.18,19 Finally, in the PEACE-1 study, the addition of abiraterone to ADT + docetaxel in patients with metastatic hormone-sensitive PC was associated with a modest increase in bone loss over the first 2 years.71 Therefore, it is unclear if a more potent inhibition of testosterone activity may increase bone turnover leading to an increased risk of fractures.
Cognitive Disorders
Several studies have shown that ADT can produce a negative effect on cognitive functioning in about 25–50% of patients.72,73 Patients receiving ADT could experience difficulties with verbal memory, spatial abilities and attention.24,74 Impairment can already be evident 6–12 months after the beginning of treatment.75 Furthermore, ADT may be associated with development of depressive symptoms. Specifically, ADT has been associated with increased rates of major depression and worsening depressive symptoms without an increased risk of suicidality.76 An association has also been shown between low level of testosterone and the risk of dementia and/or Alzheimer disease.77 In the systematic review and meta-analysis conducted by Motlagh et al, the risk of new onset dementia and Alzheimer disease was higher in patients with PC who received ADT compared to those who did not (HR 1.21, 95% CI 1.11–1.33 and HR 1.16, 95% CI 1.09–1.24).77 Androgen receptor messenger RNA was found to be expressed in cortical brain regions that are critical for cognitive functions (eg the prefrontal cortex, parietal lobe and hippocampus). Studies used functional magnetic resonance imaging to assess the effect of ADT on cerebral structures showed a decrease in the gray matter volume in the frontopolar cortex, dorsolateral prefrontal cortex and primary motor cortex in patients with PC under ADT.78 Furthermore, a low testosterone level increases the production of extracellular beta amyloid protein and intracellular tau phosphorylation. Accumulation of these proteins in the central nervous system is a pathological feature of Alzheimer disease.79
The effect of ARPIs on the cognitive functions of PC patients has not been adequately evaluated in the pivotal studies.80 Apalutamide and enzalutamide, have been associated with adverse central nervous system-related events in patients with PC, including fatigue and mental impairment disorders.81 In contrast, limited data suggest fewer drug-related cognitive effects with abiraterone compared with enzalutamide.82,83 In clinical trials, darolutamide was not associated with a higher incidence of adverse cognitive effects.13 The alteration of cognitive functions reported with apalutamide and enzalutamide may be due to their penetration of the blood–brain barrier, whereas darolutamide has shown limited blood–brain barrier penetration in preclinical and clinical studies.81
Cognitive dysfunction may be more prevalent in real-world populations than in the carefully selected populations included in phase III studies. For example, in the observational AQUARiUS study, clinically meaningful worsening in perceived cognitive impairment was reported by 49% of patients treated with abiraterone and 76% of those who received enzalutamide (p = 0.05).82 By contrast, in REAAcT trial, patients treated with abiraterone or enzalutamide had almost no change from baseline in cognitive function over time.83
Based on these findings, all patients starting ADT should be counseled regarding possible neuropsychiatric side effects, including information about the connection between ADT and mental health24 (Table 1). Screening for cognitive dysfunction should be considered an integral part of standard management before initiation of hormone therapies. Furthermore, in patients with PC and diagnosed with depression or dementia it would be useful to perform a psychiatric or geriatric evaluation before starting hormone therapy. In addition, routine monitoring of cognitive function should be performed in patients receiving hormone therapies to detect any cognitive deficits as soon as possible and, if necessary, specialized neuropsychological evaluation should be performed. There are several simple questionnaires that can help the physician in recognizing the presence of cognitive alterations at an early stage, such as the Mini-Mental State Examination (MMSE), the Montreal Cognitive Assessment (MoCA) or Mini-Cog assessment.81 However, to date none of these tools are routinely used in clinical practice in monitoring PC patients treated with hormone therapies. A therapeutic strategy to improve the quality of life of patients with PC by reducing the risk of developing cognitive disorders could be represented by the use of intermittent hormonal therapy. In a trial with more than 1500 patients with mHSPC Hussain et al showed that intermittent ADT was associated with better mental health at month 3 (p=0.003) even if this improvement was not present at a longer follow-up.70
 |
Table 1 Summary of Adverse Events Associated with Hormone Therapies and Their Management |
Hot Flashes
Hot flashes are defined as an intense heat sensation, flushing and diaphoresis that usually involve the face and trunk, sometimes associated with anxiety and palpitations.24 They are one of the most frequent adverse events of ADT occurring in up to 80% of patients and it is reported as the most bothering from 27% of them.84
Hot flashes can be associated with sleep disturbance and may lead to a deterioration in quality of life.85 Moreover they may decrease compliance to ADT and are a major contributor to its discontinuation.24
Literature suggests that estrogen and androgen withdrawal disrupt the equilibrium of the neurotransmitters, norepinephrine and serotonin. This consequently affects the omeostatic mechanism in the thermoregulatory zone in the pre-optic zone of the hypothalamus.86 Antiandrogens have a significantly lower risk of hot flashes than LHRH agonists (<1% vs 45%) and intermittent ADT is associated with significantly better scores for hot flashes compared to continuous ADT (p<0.001).24,87
First in patients who report frequent hot flashes lifestyle modifications may be recommended, including avoidance of potential patient-identified triggers, commonly heat or spicy food88 (Table 1). In addition, several pharmacological hormonal and non-hormonal agents have been assessed in the treatment of hot flashes, however few evidences exist for their management.
In several small prospective studies, the use of diethylstilbestrol resulted in complete resolution of hot flashes in more than 70% of patients.86 A double-blind, randomized study showed a 75–80% reduction of hot flashes in patients treated with megestrol acetate versus placebo, but it is associated with an increase PC growth.89 Cyproterone acetate showed similar results without the risk of tumour progression.90
Gabapentin, used as an anticonvulsant and for treatment of neuropathic pain, was evaluated for the treatment of hot-flashes. In a randomized trial, 214 patients with PC treated with ADT were randomized to placebo, or gabapentin at the dosage of 300, 600 or 900 mg.91 There were reductions in hot flash scores by 22%, 23%, 32%, and 46%, respectively, without increased toxicity with gabapentin compared with placebo.91 Based on these data, gabapentin is a reasonable therapy to treat ADT-induced hot flashes with a starting dose at 300 mg daily augmentable up to 900 mg.
Venlafaxine, a serotonin-norepinephrine reuptake inhibitor used as antidepressant drug, was also tested in patients with PC with the aim of reducing hot flashes. In a randomized clinical trial in PC patients treated with ADT venlafaxine was compared to medroxyprogesterone acetate and cyproterone acetate and showed to reduce hot flashes of 47.2% although cyproterone and medroxyprogesterone obtained better results (−94.5% and −83.7% respectively).90
To mitigate the hot flashes in patients with PC treated with ADT, it has also been investigated the role of complementary medicine, such as the acupuncture. It leads to a decrease of hot flash symptoms by 89–95%, however, these results are not based on randomized clinical trials data.92 Finally, the use of intermittent ADT showed a reduction in hot flashes compared to continuous ADT (p<0.01).93
In the pivotal trials, the addition of ARPI to ADT appears to result in an increased incidence of hot flashes compared to ADT alone. In the AFFIRM16 and PREVAIL17 studies, 18–20% of patients treated with ADT + enzalutamide experienced hot flushes versus 8–10% of patients treated with ADT alone. In COU-AA-302 trial,15 patients experiencing hot flushes were 22% in the ADT + abiraterone group and 18% in the ADT alone group, respectively. Similar findings in the TITAN11 study where adding apalutamide to ADT resulted in an approximately 6% increase in hot flashes. On the other hand, darolutamide does not seem to increase the incidence of hot flushes: in the ARAMIS study,13 5.2% of patients in the darolutamide arm developed hot flushes versus 4.2% in the placebo group.
Breast Events
Breast events include gynecomastia and mastodynia, which may occur concurrently or separately. Gynecomastia occurs most commonly with antiandrogens while is a rare complication of ADT.94
ARPI does not appear to increase breast events compared to antiandrogen: in the Phase 3 study ENZAMET, the frequency of breast events was similar in patients treated with ADT + enzalutamide compared to ADT + antiandrogen.12 Several studies have demonstrated that both tamoxifen and radiotherapy are effective prophylactic treatments for breast events, but to date a prophylaxis treatment is not recommended24 (Table 1).
Fatigue
Fatigue is a common side effect of ADT which can worsen the quality of life of patients with PC reducing the patient’s level of independence.26 Fatigue may also be associated with depression.95 The prevalence of fatigue varies from 66% to 77% and it is more common in patients treated with an LHRH agonist than with peripheral AR antagonists. Furthermore, a longer duration of hormone therapy is associated with a higher level of fatigue.96
ARPIs can cause worsening of fatigue in patients with PC and between ARPIs enzalutamide and apalutamide seem to determine a higher incidence of fatigue probably due to their ability to pass the blood–brain barrier. In a recent randomized trial in the mCRPC setting, enzalutamide showed an higher risk for fatigue compared to abiraterone.97
Physical exercise and dietary counselling are considered the best first-line treatment interventions in order to mitigate ADT-induced fatigue (Table 1). Many trials showed that various exercise regimens can reduce fatigue in men receiving ADT, and the benefit was greater for patients reporting highest levels of fatigue.98 Current evidence for dietary interventions to mitigate the side effects of ADT is limited, and there are no specific dietary recommendations. In a pilot randomized control trial, Baguley et al showed that the Mediterranean-style dietary pattern has the potential to improve quality of life in patients with PC treated with ADT, but further exploration of this diet is warranted in a larger powered sample size to consolidate these findings.99 In general, patients starting hormone therapy should be advised to follow a healthy, varied and balanced diet according to WHO recommendations.
In patients treated with ARPI who experience fatigue that compromises the quality of life, a temporary withdrawal of ARPI may be considered, which generally results in improvement within a few days. Thereafter, ARPI treatment can be resumed at a reduced dose which generally results in a lower risk of fatigue.25
Anemia
Anemia is the most common haematological side effect in men receiving ADT. Testosterone promotes erythropoiesis by stimulating the differentiation of bone marrow erythroid stem cells and by increasing the renal production of erythropoietin.100 Decreased haemoglobin levels can be seen in up to 90% of patients receiving ADT, but the prevalence of symptomatic anaemia is lower (0–37%).101
Anemia is usually normocytic and normochromic and asymptomatic. However, in a minority of patients, especially who had metastatic disease with bone marrow infiltration or who had cardiovascular comorbidities, anaemia can become severe and may be associated with increased life-threatening complications.101
The hemoglobin level should be tested before starting the ADT and during the treatment period. If anemia is found, a dosage of vitamin B12, folate or iron should be performed and supplementary therapy should be started in case of deficiency24 (Table 1).
Sexual Disfunction
ADT impact on multiple domains of sexual function that may deeply affect the quality of life of patients with PC. ADT can cause a reduction in penis length and testicular atrophy which combined with alterations in weight, muscle mass, and gynecomastia, may have a detrimental impact on self-perceived body image leading to poor sexual function and decreased partner intimacy.102,104 The association between ADT, reduced libido and erectile disfunction is well known. A recent metanalyses showed that ADT resulted in a five to sixfold increased risk of reduced libido and in a threefold increased risk of erectile disfunction.102
In a cohort study of 250 patients undergoing intermittent ADT (LHRH agonist + antiandrogen), it was demonstrated a worsening of the sexual activity.104 From a baseline of 46% of patients reporting sexual activity, at 9 months only 13% of the men did so, and 10% reported moderate to high libido vs an initial 63%. The proportion of men feeling less masculine increased to 50% as a result of hormonal treatment, against 26% at baseline. During the off phase of the intermittent treatment, 52% of previously sexually active men resumed sexual activity. Levels of libido, masculinity and sexual activity recovered but not to baseline levels, thus showing that the side effects are only partially reversible in the majority of patients and should therefore be addressed both in patient in treatment and survivors.104
Before starting ADT patients should be adequately informed about the possible side effects on sexual activity. Referrals to psychosocial support groups and/or sex therapists should be offered to interested patients (Table 1). Erectile dysfunction may be treated with various interventions, including phosphodiesterase inhibitors; however, treatment efficacy may be poor without adequate mental and physical arousal.102 Intermittent ADT has been shown to improve sexual function and should be considered in appropriate patients. Hussain et al showed that patients with mHSPC treated with intermittent ADT had a better erectile function at month 3 (p<0.001) than patients treated with continuous ADT.70
Renal Toxicity
The use of ADT may increase the risk of acute kidney injury (AKI).103 In a study of more than 10,000 patients, ADT was associated with an increased risk of AKI when compared with never use (odds ratio 2.48, 95% CI 1.61–3.82).103 Testosterone appears to protect the kidneys by inducing vasodilation in the renal vessels, thus the use of ADT might increase the risk of damage to the glomerulus. Furthermore, ADT-induced hypogonadism leads to estrogen deficiency and estrogens play a protective role in ischemic renal injury by reducing glomerular endothelial permeability.103,105 Adding ARPIs to ADT does not appear to increase renal toxicity.105
An early recognition of renal impairment represents an important aspect to minimize the risk of renal injury. This can be accomplished by a routine use of glomerular filtration rate (eGFR) estimation rather than serum creatinine value alone (which may be in the normal range in older patients or those with muscle wasting) which should be evaluated before starting hormone therapy and during the treatment period.105
ARPI-Specific Adverse Events
As previously discussed, ARPIs can worsen some of the adverse events induced by ADT. However, ARPI-specific adverse events do exist and they differ among the various ARPIs.
Abiraterone
Abiraterone acetate is a steroidal antiandrogen which acts via selective and irreversible inhibition of cytochrome P450 17A1 (CYP17A1) and is used at a dosage of 1000mg/day.107 CYP17A1 is a key enzyme in cortisol and androgen biosynthesis.10 The inhibition of glucocorticoids synthesis, causing a compensatory increase in the ACTH and consequently an excess of mineralocorticoids which can cause hypokalemia, hypertension, peripheral edema and congestive heart failure. Therefore, glucocorticoid replacement therapy with low-dose prednisone (5–10mg/day) is required to minimize the incidence of mineralocorticoid excess symptoms106 (Table 2). In the pivotal study COU-AA-301 abiraterone was used in patients with mCRPC previously treated with docetaxel.14 In this trial 17% of patients treated with abiraterone experienced hypokalaemia, 10% developed hypertension, while fluid retention and edema and cardiac disorders occurred in 31% and 13%, respectively.14 Similar results were achieved in the COU-AA-302 study where abiraterone was used in patients who had not received prior docetaxel treatment.15 In this study, hypokalaemia occurred in 17% of patients, hypertension in 22% while fluid retention or edema and cardiac disorder in 28% and 19% of patients.105 Hypertension and hypokalemia were the main adverse events induced by abiraterone in the LATITUDE trial in which abiraterone was used in patients with mHSPC (37% and 20% respectively).20 In particular, grade 3 hypertension and hypokalaemia occurred in 20% and 11% of cases. 12% of the patients instead developed cardiac disorders.20 Finally, in the STAMPEDE study, 5% and 1% of patients with mHSPC developed grade 3 hypertension and hypokalaemia, respectively, while grade 3 cardiovascular changes occurred in 10% of patients.10 It is important to underline that while in the studies in the mCRPC setting (COU-AA-301 and COU-AA-302) patients received 10mg/day of prednisone in addition to abiraterone, in the studies in the mHSPC setting (LATITUDE and STAMPEDE) the patients randomized in the abiraterone arm they were concomitantly treated with 5mg/day of prednisone/prednisolone.10,14,15,20
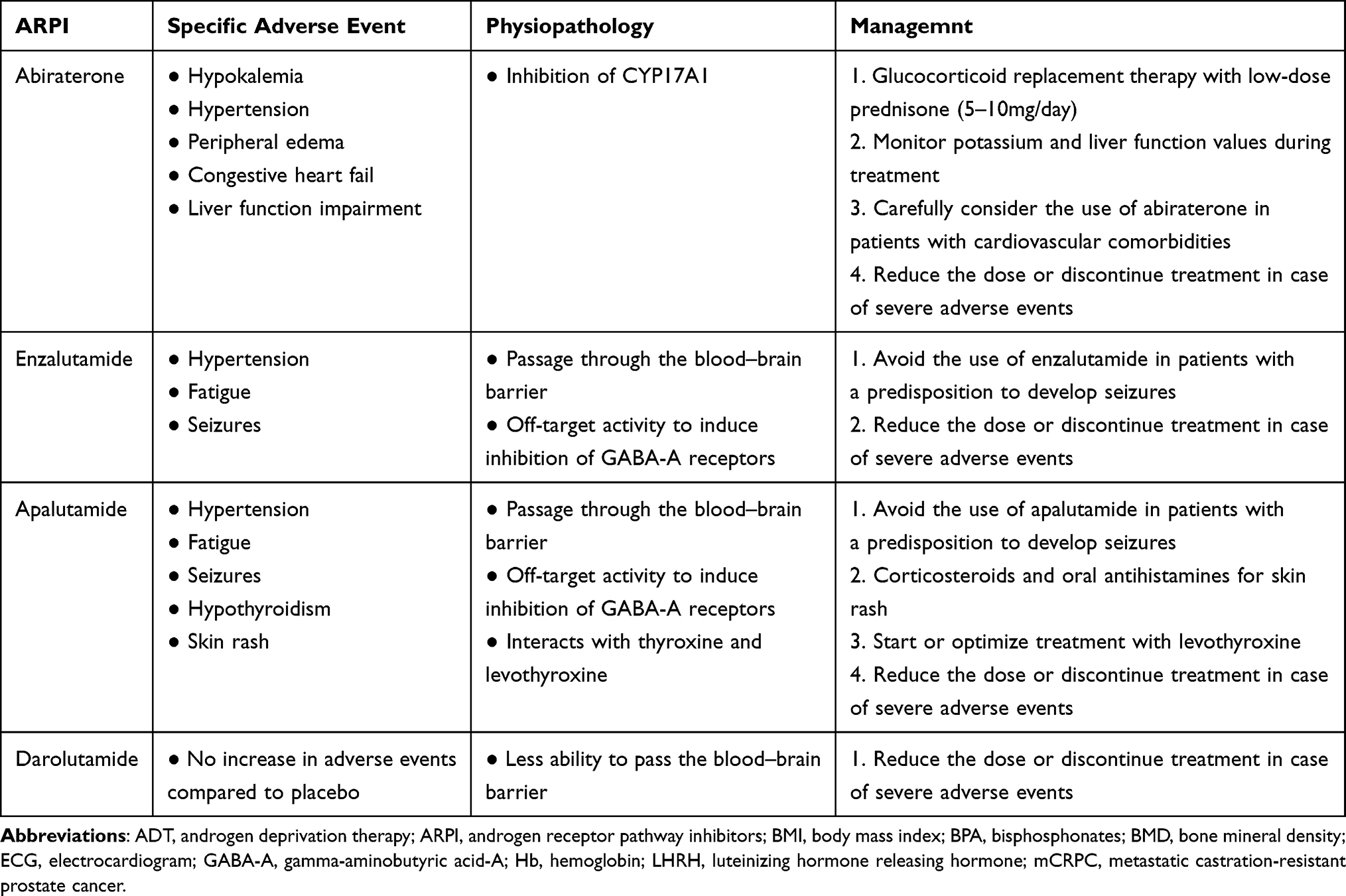 |
Table 2 Summary of ARPI-Specific Adverse Events and Their Management |
Abiraterone can also rarely cause liver function impairment with an increase in liver enzymes.25 In the previously mentioned studies 10–16% of patients experienced an increase in liver enzymes of which in 3–6% of grade ≥ 3.10,14,15,20 Currently, the mechanisms of liver function test increase on abiraterone are unknown. In patients with impaired hepatic function abiraterone should be considered carefully. During treatment follow-up, serum potassium, transaminase and bilirubin levels should be evaluated every 2 weeks for the first 3 months and thereafter monthly.107 In case of severe adverse events abiraterone should be discontinued. Treatment can be re-initiated at a reduced dose of 500mg/day once toxicity resolves or improves.107
Enzalutamide
Enzalutamide is a non-steroidal AR inhibitor and is administered at a dosage of 160mg/day.52 The most frequently reported adverse events associated with enzalutamide are hypertension and fatigue. Fatigue was the most frequent adverse event in patients with mCRPC treated with enzalutamide in the AFFIRM and PREVAIL study (34–36% of which 2–6% grade > 3), while hypertension occurred in approximately 13% of cases of which in 7% grade> 3 in these studies.16,17 Similar results occurred in the PROSPER study, in which enzalutamide caused fatigue and hypertension in approximately 33% and 12% of patients in patients with nmCRPC.18 Fatigue and hypertension occurred less frequently in patients with mHSPC treated with enzalutamide in the ARCHES and ENZAMET studies (6–19.6% and 8% respectively).12,21
Furthermore, enzalutamide can induce seizures due to their off-target activity of inducing an inhibition of GABA-A receptors, therefore enzalutamide should be avoided in patients with a predisposition to develop seizures.25 In the previously mentioned studies in which patients with a history of seizure or a condition that may confer a predisposition to seizure were excluded, seizure occurred in <1% of patients.12,16–18,21
In case of serious adverse event, it must be suspended and possibly restarted at a lower dosage of 80mg/day in case of improvement or resolution of toxicity. If the dosage of 80mg/day is well tolerated by the patient, it is possible to increase the dosage to 120mg/day52 (Table 2).
Apalutamide
Apalutamide is a non-steroidal AR inhibitor with a chemical structure similar to that of enzalutamide which is administered at a dosage of 240 mg/day.108 Like enzalutamide also apalutamide can cause fatigue, hypertension and risk of seizures. In the SPARTAN study which enrolled patients with nmCRPC, 30.4% of patients treated with apalutamide developed fatigue while hypertension occurred in 24.8% of cases (14.3% grade> 3).19 In this study, 2 patients (0.2%) experienced seizure.19 Fatigue and hypertension occurred less frequently in mHSPC patients treated with apalutamide in the TITAN study (19.7% and 17.7% respectively).11 Also in these studies, patients with a history of or predisposition to seizure could not be enrolled.11,19
Specific adverse effects of apalutamide are hypothyroidism and skin rash most commonly in the form of macular or maculo-papular lesions.25 In the previously mentioned studies, hypothyroidism occurred in 6.5–8.1% of patients, while 23.8–27.1% of patients experienced a skin rash of which in 5.2–6.3% grade> 3.11,19
In patients receiving apalutamide, clinicians should evaluate thyroid function at the beginning and during treatment. The management of hypothyroidism in most cases required only an increase in levothyroxine dose or a de novo initiation of thyroid replacement therapy (Table 2). In the case of skin rash, treatment options include topical corticosteroids, oral antihistamines, or even systematic corticosteroids, depending on the extent and severity of the skin rash.25 In patients with severe adverse reactions, apalutamide should be withheld to mitigate side effects and reinitiated at the reduced dose upon resolution of symptoms.25 Generally the therapy is restarted with a halved dose (120 mg/day) and if well tolerated the dose can be increased up to 180 mg/day.108
Darolutamide
Darolutamide is a non-steroidal AR inhibitor with a distinct chemical structure compared to apalutamide and enzalutamide which determines a reduced penetration of the blood–brain barrier and consequently a reduction of central nervous system side effects, such as fatigue, cognitive impairment and seizures. Darolutamide is administered at a dosage of 600 mg x2/day.109 Clinical trials evaluating darolutamide did not show an increase in adverse events compared to placebo.13 In patients with nmCRPC treated with darolutamide in the ARAMIS study, 12.1% of patients experienced fatigue (versus 8.7% of patients treated with placebo) and 6.6% of patients developed hypertension (versus 5.2% of patients treated with placebo).13 Similar results occurred in the ARASENS trial in which the addition of darolutamide to the ADT + docetaxel combination did not result in an increase in side effects compared to placebo.110
Although no clear recommendations exist, in patients presenting with serious or intolerable adverse reactions the darolutamide dosage should be reduced to half dose (600 mg/day) and increased up to 900 mg/day if well tolerated.109 (Table 2).
Conclusions
Hormonal therapies represent the cornerstone of the systemic treatment of PC.3 Although these are generally well-tolerated therapies, they can cause adverse events that can worsen the quality of life of patients and consequently compromise treatment compliance. The increasing use of ARPIs in earlier stages of the disease will lead to an increased exposure of patients to these treatments and consequently to their possible adverse events. Several studies have documented an important reduction in quality of life in patients with PC treated with hormonal therapies.26,111 A study including patients treated with ADT showed a statistically significant reduction in different quality of life items, such as mental health and general health, energy and concern regarding body image.111 Fatigue and depression induced by ADT can interfere with cognitive function, producing a significant reduction in the quality of life of patients with prostate cancer.26
Clinicians caring for patients with PC should adequately inform patients of the possibility of developing these adverse events and possible treatment options to mitigate them. Furthermore, patients starting hormone treatment should be carefully followed over time to diagnose and treat any adverse events early. It is useful to discuss with other specialists (eg cardiologist, psychiatrist or geriatrician) before starting hormone therapy in patients at increased risk of developing adverse events and the choice of treatment should take into account their evaluation. Moreover, in the management of adverse events caused by hormonal therapies it would be useful to perform a multidisciplinary evaluation by discussing with specific specialists. Furthermore, the use of specific validated questionnaires to assess treatment toxicities and to monitor patients’ quality of life should be implemented in clinical practice. Since we do not always have treatments available to improve the adverse events induced by hormonal therapies, the most studied therapeutic strategy is represented by the use of intermittent hormonal therapy. Several studies have demonstrated that intermittent ADT is associated with a reduced rate of side-effects and better quality of life than continuous ADT.70,87,93,104 However none of the trials that addressed intermittent versus continuous ADT in mHSPC patients showed a survival benefit but there was a constant trend towards improved OS with continuous ADT although most of these studies were non-inferiority trials.70,87,93,104 On the other hand, there is no evidence on intermittent hormonal therapy in patients with mHSPC treated with ADT + ARPI since all the trials that evaluated this combination did not provide for the use of intermittent therapy. It is possible that selected patients with mHSPC (eg patients with low disease burden who reach undetectable PSA values within a few months after starting hormonal therapy) may benefit from intermittent therapy in terms of reduction of side effects and improvement of quality of life without compromising the efficacy of the therapy. Therefore, future studies evaluating a de-intensification of treatments in patients with mHSPC are needed.
Also another possible approach to reduce the toxicity of hormone therapy is to postpone its start. In a prospective, randomized phase 2 study, Ost et al showed that metastasis-directed therapy (MDT) prolongs ADT free-survival in oligorecurrent PC patients (up to a maximum of 3 metastases) compared to observation (HR, 0.60; 80% CI, 0.40–0.90; log-rank p=0.11) with no grade 2 to 5 toxicity.112 In another phase 2 study, Philips et al showed that MDT improved median progression-free survival compared to observation (HR 0.30; 95% CI, 0.11–0.81; p=0.002) in oligorecurrent mHSPC patients (1–3 metastases) with no toxic effects of grade 3 or greater.113 Finally, the long-term results of these 2 studies confirmed the benefit of MDT in patients with oligorecurrent PC.114 The results of MDT are therefore promising in order to postpone the start of a systemic therapy and consequently its side effects. However, it must be emphasized that the control arm of the 2 studies was represented by observation which does not represent the standard of care of patients with metastatic PC. Future studies evaluating MDT vs standard of care systemic therapies in patients with mHSPC are needed.
Finally, future studies are needed to investigate some poorly studied adverse events of hormone therapies, such as cognitive alterations and to identify new therapeutic options to improve the quality of life of patients with PC. In fact, although several studies are ongoing that are evaluating the efficacy of new therapeutic options in patients with PC, there are few studies that are focusing on the management of treatment toxicities and on identifying strategies that can improve the quality of life of these patients.
Disclosure
Dr Fabio Turco reports grants from Bayer, personal fees from Recordati AG, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. 2021;71(3):209–249. doi:10.3322/caac.21660
2. National Cancer Institute. Cancer Stat Facts: Prostate Cancer. Available from: https://seer.cancer.gov/statfacts/html/prost.html.
3. Huggins C, Hodges CV. Studies on prostatic cancer. I. The effect of castration, of estrogen and androgen injection on serum phosphatases in metastatic carcinoma of the prostate. Cancer Res. 1941;1:293–297.
4. Schaeffer E, Srinivas S, Antonarakis ES, et al. NCCN guidelines insights: prostate cancer, version 1.2021. JNCCN. 2021;19(2):134–143.
5. Mottet N, Cornford P, van den Bergh RCN. EAU-EANM-ESTRO-ESUR-ISUP-SIOG guidelines on prostate cancer update; 2022.
6. Seidenfeld J, Samson DJ, Hasselblad V, et al. Single-therapy androgen suppression in men with advanced prostate cancer: a systematic review and meta-analysis. Ann Intern Med. 2000;132(7):566–577. doi:10.7326/0003-4819-132-7-200004040-00009
7. Eisenberger MA, Blumenstein BA, Crawford ED, et al. Bilateral orchiectomy with or without flutamide for metastatic prostate cancer. N Engl J Med. 1998;339(15):1036–1042. doi:10.1056/NEJM199810083391504
8. Gillatt D. Antiandrogen treatments in locally advanced prostate cancer: are they all the same? J Cancer Res Clin Oncol. 2006;132(Suppl 1):S17–S26. doi:10.1007/s00432-006-0133-5
9. Wadosky KM, Koochekpour S. Molecular mechanisms underlying resistance to androgen deprivation therapy in prostate cancer. Oncotarget. 2016;7(39):64447–64470. doi:10.18632/oncotarget.10901
10. James ND, de Bono JS, Spears MR, et al.; STAMPEDE Investigators. Abiraterone for prostate cancer not previously treated with hormone therapy. N Engl J Med. 2017;377(4):338–351. doi:10.1056/NEJMoa1702900
11. Chi KN, Agarwal N, Bjartell A, Chung BH; TITAN Investigators. Apalutamide for metastatic, castration-sensitive prostate cancer. N Engl J Med. 2019;381(1):13–24. doi:10.1056/NEJMoa1903307
12. Davis ID, Martin AJ, Stockler MR; ENZAMET Trial Investigators and the Australian and New Zealand Urogenital and Prostate Cancer Trials Group. Enzalutamide with standard first-line therapy in metastatic prostate cancer. N Engl J Med. 2019;381(2):121–131. doi:10.1056/NEJMoa1903835
13. Fizazi K, Shore N, Tammela TL, et al.; ARAMIS Investigators. Darolutamide in nonmetastatic, castration-resistant prostate cancer. N Engl J Med. 2019;380(13):1235–1246. doi:10.1056/NEJMoa1815671
14. de Bono JS, Logothetis CJ, Molina A, et al.; COU-AA-301 Investigators. Abiraterone and increased survival in metastatic prostate cancer. N Engl J Med. 2011;364(21):1995–2005. doi:10.1056/NEJMoa1014618
15. Ryan CJ, Smith MR, de Bono JS; COU-AA-302 Investigators. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med. 2013;368(2):138–148. doi:10.1056/NEJMoa1209096
16. Scher HI, Fizazi K, Saad F, et al.; AFFIRM Investigators. Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med. 2012;367(13):1187–1197. doi:10.1056/NEJMoa1207506
17. Beer TM, Armstrong AJ, Rathkopf DE, et al.; PREVAIL Investigators. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med. 2014;371(5):424–433. doi:10.1056/NEJMoa1405095
18. Hussain M, Fizazi K, Saad F, et al. Enzalutamide in men with nonmetastatic, castration-resistant prostate cancer. N Engl J Med. 2018;378(26):2465–2474. doi:10.1056/NEJMoa1800536
19. Smith MR, Saad F, Chowdhury S, et al.; SPARTAN Investigators. Apalutamide treatment and metastasis-free survival in prostate cancer. N Engl J Med. 2018;378(15):1408–1418. doi:10.1056/NEJMoa1715546
20. Fizazi K, Tran N, Fein L, et al.; LATITUDE Investigators. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med. 2017;377(4):352–360. doi:10.1056/NEJMoa1704174
21. Armstrong AJ, Szmulewitz RZ, Petrylak DP, et al. ARCHES: a randomized, phase III study of androgen deprivation therapy with enzalutamide or placebo in men with metastatic hormone-sensitive prostate cancer. J Clin Oncol. 2019;37(32):2974–2986. doi:10.1200/JCO.19.00799
22. Attard G, Murphy L, Clarke NW, et al.; Systemic Therapy in Advancing or Metastatic Prostate cancer: Evaluation of Drug Efficacy (STAMPEDE) investigators. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: a meta-analysis of primary results from two randomised controlled phase 3 trials of the STAMPEDE platform protocol. Lancet. 2022;399(10323):447–460. doi:10.1016/S0140-6736(21)02437-5
23. Armstrong AJ, Azad AA, Iguchi T, et al. Improved survival with enzalutamide in patients with metastatic hormone-sensitive prostate cancer. J Clin Oncol. 2022;40(15):1616–1622. doi:10.1200/JCO.22.00193
24. Kokorovic A, So AI, Serag H, et al. Canadian Urological Association guideline on androgen deprivation therapy: adverse events and management strategies. Can Urol Assoc J. 2021;15(6):E307–E322. doi:10.5489/cuaj.7355
25. Pyrgidis N, Vakalopoulos I, Sountoulides P. Endocrine consequences of treatment with the new androgen receptor axis-targeted agents for advanced prostate cancer. Hormones. 2021;20(1):73–84. doi:10.1007/s42000-020-00251-5
26. Tucci M, Leone G, Buttigliero C, et al. Hormonal treatment and quality of life of prostate cancer patients: new evidence. Minerva urologica e nefrologica. 2018;70(2):144–151. doi:10.23736/S0393-2249.17.03066-1
27. Elmehrath AO, Afifi AM, Al-Husseini MJ, et al. Causes of death among patients with metastatic prostate cancer in the US From 2000 to 2016. JAMA Netw Open. 2021;4(8):e2119568. doi:10.1001/jamanetworkopen.2021.19568
28. Zhao J, Zhu S, Sun L, et al. Androgen deprivation therapy for prostate cancer is associated with cardiovascular morbidity and mortality: a meta-analysis of population-based observational studies. PLoS One. 2014;9(9):e107516. doi:10.1371/journal.pone.0107516
29. Bosco C, Bosnyak Z, Malmberg A, Adolfsson J, Keating NL, Van Hemelrijck M. Quantifying observational evidence for risk of fatal and nonfatal cardiovascular disease following androgen deprivation therapy for prostate cancer: a meta-analysis. Eur Urol. 2015;68(3):386–396. doi:10.1016/j.eururo.2014.11.039
30. Nguyen PL, Je Y, Schutz FA, et al. Association of androgen deprivation therapy with cardiovascular death in patients with prostate cancer: a meta-analysis of randomized trials. JAMA. 2011;306(21):2359–2366. doi:10.1001/jama.2011.1745
31. Bosco C, Crawley D, Adolfsson J, Rudman S, Van Hemelrijck M. Quantifying the evidence for the risk of metabolic syndrome and its components following androgen deprivation therapy for prostate cancer: a meta-analysis. PLoS One. 2015;10(3):e0117344. doi:10.1371/journal.pone.0117344
32. Hak AE, Witteman JC, de Jong FH, Geerlings MI, Hofman A, Pols HA. Low levels of endogenous androgens increase the risk of atherosclerosis in elderly men: the Rotterdam study. J Clin Endocrinol Metab. 2002;87(8):3632–3639. doi:10.1210/jcem.87.8.8762
33. O’Farrell S, Garmo H, Holmberg L, Adolfsson J, Stattin P, Van Hemelrijck M. Risk and timing of cardiovascular disease after androgen-deprivation therapy in men with prostate cancer. J Clin Oncol. 2015;33(11):1243–1251. doi:10.1200/JCO.2014.59.1792
34. Ziehr DR, Chen MH, Zhang D, et al. Association of androgen-deprivation therapy with excess cardiac-specific mortality in men with prostate cancer. BJU Int. 2015;116(3):358–365. doi:10.1111/bju.12905
35. D’Amico AV, Denham JW, Crook J, et al. Influence of androgen suppression therapy for prostate cancer on the frequency and timing of fatal myocardial infarctions. J Clin Oncol. 2007;25(17):2420–2425. doi:10.1200/JCO.2006.09.3369
36. Knutsson A, Hsiung S, Celik S, et al. Treatment with a GnRH receptor agonist, but not the GnRH receptor antagonist degarelix, induces atherosclerotic plaque instability in ApoE(-/-) mice. Sci Rep. 2016;6:26220. doi:10.1038/srep26220
37. Hopmans SN, Duivenvoorden WC, Werstuck GH, Klotz L, Pinthus JH. GnRH antagonist associates with less adiposity and reduced characteristics of metabolic syndrome and atherosclerosis compared with orchiectomy and GnRH agonist in a preclinical mouse model. Urol Oncol. 2014;32(8):1126–1134. doi:10.1016/j.urolonc.2014.06.018
38. Tisseverasinghe S, Tolba M, Saad F, Gravis G, Bahoric B, Niazi T. Should prostate cancer patients with history of cardiovascular events be preferentially treated with luteinizing hormone-releasing hormone antagonists? J Clin Oncol. 2022;40(36):4173–4177. doi:10.1200/JCO.22.00883
39. Margel D, Peer A, Ber Y, et al. Cardiovascular morbidity in a randomized trial comparing GnRH agonist and GnRH antagonist among patients with advanced prostate cancer and preexisting cardiovascular disease. J Urol. 2019;202(6):1199–1208. doi:10.1097/JU.0000000000000384
40. Shore ND, Saad F, Cookson MS, et al.; HERO Study Investigators. Oral relugolix for androgen-deprivation therapy in advanced prostate cancer. N Engl J Med. 2020;382(23):2187–2196. doi:10.1056/NEJMoa2004325
41. Lopes RD, Higano CS, Slovin SF, et al.; PRONOUNCE Study Investigators. Cardiovascular safety of degarelix versus leuprolide in patients with prostate cancer: the primary results of the PRONOUNCE randomized trial. Circulation. 2021;144(16):1295–1307. doi:10.1161/CIRCULATIONAHA.121.056810
42. Berruti A, Dogliotti L, Terrone C, et al.; Gruppo Onco Urologico Piemontese (G.O.U.P.), Rete Oncologica Piemontese. Changes in bone mineral density, lean body mass and fat content as measured by dual energy x-ray absorptiometry in patients with prostate cancer without apparent bone metastases given androgen deprivation therapy. J Urol. 2002;167(6):2361–2367. doi:10.1016/S0022-5347(05)64985-3
43. Haseen F, Murray LJ, Cardwell CR, O’Sullivan JM, Cantwell MM. The effect of androgen deprivation therapy on body composition in men with prostate cancer: systematic review and meta-analysis. J Cancer Surviv. 2010;4(2):128–139. doi:10.1007/s11764-009-0114-1
44. Smith MR, Finkelstein JS, McGovern FJ, et al. Changes in body composition during androgen deprivation therapy for prostate cancer. J Clin Endocrinol Metab. 2002;87(2):599–603. doi:10.1210/jcem.87.2.8299
45. Cheung AS, Tinson AJ, Milevski SV, Hoermann R, Zajac JD, Grossmann M. Persisting adverse body composition changes 2 years after cessation of androgen deprivation therapy for localised prostate cancer. Eur J Endocrinol. 2018;179(1):21–29. doi:10.1530/EJE-18-0117
46. Nobes JP, Langley SE, Klopper T, Russell-Jones D, Laing RW. A prospective, randomized pilot study evaluating the effects of metformin and lifestyle intervention on patients with prostate cancer receiving androgen deprivation therapy. BJU Int. 2012;109(10):1495–1502. doi:10.1111/j.1464-410X.2011.10555.x
47. He K, Hu H, Ye S, Wang H, Cui R, Yi L. The effect of metformin therapy on incidence and prognosis in prostate cancer: a systematic review and meta-analysis. Sci Rep. 2019;9(1):2218. doi:10.1038/s41598-018-38285-w
48. Jayalath VH, Clark R, Katherine Lajkosz NE, Hamilton RJ, Hamilton RJ. Statin use and survival in men receiving androgen-ablative therapies for advanced prostate cancer: a systematic review and meta-analysis of cohort studies. J Clin Oncol. 2022;40(6_suppl):83. doi:10.1200/JCO.2022.40.6_suppl.083
49. Gagliano-Jucá T, Travison TG, Kantoff PW, et al. Androgen deprivation therapy is associated with prolongation of QTc Interval in men with prostate cancer. J Endocr Soci. 2018;2(5):485–496. doi:10.1210/js.2018-00039
50. Iacovelli R, Ciccarese C, Bria E, et al. The cardiovascular toxicity of abiraterone and enzalutamide in prostate cancer. Clin Genitourin Cancer. 2018;16(3):e645–e653. doi:10.1016/j.clgc.2017.12.007
51. Moreira RB, Debiasi M, Francini E, et al. Differential side effects profile in patients with mCRPC treated with Abiraterone or enzalutamide: a meta-analysis of randomized controlled trials. Oncotarget. 2017;8(48):84572–84578. doi:10.18632/oncotarget.20028
52. Astellas Pharma Canada Inc. XTANDI® product monograph. Markham, Ontario; 2013.
53. Shigehara K, Izumi K, Kadono Y, Mizokami A. Testosterone and bone health in men: a narrative review. J Clin Med. 2021;10(3):530. doi:10.3390/jcm10030530
54. Clarke BL, Khosla S. Androgens and bone. Steroids. 2009;74(3):296–305. doi:10.1016/j.steroids.2008.10.003
55. Cianferotti L, Bertoldo F, Carini M, et al. The prevention of fragility fractures in patients with non-metastatic prostate cancer: a position statement by the international osteoporosis foundation. Oncotarget. 2017;8(43):75646–75663. doi:10.18632/oncotarget.17980
56. Bargiota A, Oeconomou A, Zachos I, Samarinas M, Pisters L, Tzortzis V. Adverse effects of androgen deprivation therapy in patients with prostate cancer: focus on muscle and bone health. JBUON. 2020;25(3):1286–1294.
57. Edmunds K, Tuffaha H, Scuffham P, Galvão DA, Newton RU. The role of exercise in the management of adverse effects of androgen deprivation therapy for prostate cancer: a rapid review. Support Care Cancer. 2020;28(12):5661–5671. doi:10.1007/s00520-020-05637-0
58. Taylor LG, Canfield SE, Du XL. Review of major adverse effects of androgen-deprivation therapy in men with prostate cancer. Cancer. 2009;115(11):2388–2399. doi:10.1002/cncr.24283
59. Wang A, Obertová Z, Brown C, et al. Risk of fracture in men with prostate cancer on androgen deprivation therapy: a population-based cohort study in New Zealand. BMC Cancer. 2015;15:837. doi:10.1186/s12885-015-1843-3
60. Cheung AS, Pattison D, Bretherton I, et al. Cardiovascular risk and bone loss in men undergoing androgen deprivation therapy for non-metastatic prostate cancer: implementation of standardized management guidelines. Andrology. 2013;1(4):583–589. doi:10.1111/j.2047-2927.2013.00093.x
61. Bienz M, Saad F. Androgen-deprivation therapy and bone loss in prostate cancer patients: a clinical review. Bonekey Rep. 2015;4:716. doi:10.1038/bonekey.2015.85
62. Greenspan SL, Wagner J, Nelson JB, Perera S, Britton C, Resnick NM. Vertebral fractures and trabecular microstructure in men with prostate cancer on androgen deprivation therapy. J Bone Miner Res. 2013;28(2):325–332. doi:10.1002/jbmr.1771
63. Santini D, Berruti A, Di Maio M, et al. Bone health management in the continuum of prostate cancer disease: a review of the evidence with an expert panel opinion. ESMO Open. 2020;5(2):e000652. doi:10.1136/esmoopen-2019-000652
64. Coleman R, Hadji P, Body JJ, et al.; ESMO Guidelines Committee. Bone health in cancer: ESMO Clinical Practice Guidelines. Ann Oncol. 2020;31(12):1650–1663. doi:10.1016/j.annonc.2020.07.019
65. Turco F, Tucci M, Buttigliero C. Adverse event assessment in prostate cancer patients receiving androgen deprivation therapy: are we doing enough? Minerva Urol Nephrol. 2021;73(6):870–872. doi:10.23736/S2724-6051.21.04817-5
66. Smith MR, Egerdie B, Hernández Toriz N; Denosumab HALT Prostate Cancer Study Group. Denosumab in men receiving androgen-deprivation therapy for prostate cancer. N Engl J Med. 2009;361(8):745–755. doi:10.1056/NEJMoa0809003
67. Saad F, Gleason DM, Murray R; Zoledronic Acid Prostate Cancer Study Group. A randomized, placebo-controlled trial of zoledronic acid in patients with hormone-refractory metastatic prostate carcinoma. J Natl Cancer Inst. 2002;94(19):1458–1468. doi:10.1093/jnci/94.19.1458
68. Fizazi K, Carducci M, Smith M, et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: a randomised, double-blind study. Lancet. 2011;377(9768):813–822. doi:10.1016/S0140-6736(10)62344-6
69. Kim SH, Joung JY, Kim S, et al. Comparison of bone mineral loss by combined androgen block agonist versus GnRH in patients with prostate cancer: a 12 month-prospective observational study. Sci Rep. 2017;7:39562. doi:10.1038/srep39562
70. Hussain M, Tangen CM, Berry DL, et al. Intermittent versus continuous androgen deprivation in prostate cancer. N Engl J Med. 2013;368(14):1314–1325. doi:10.1056/NEJMoa1212299
71. Roubaud G, Kostine M, Raymond S. Bone mineral density in men with de novo metastatic castration-sensitive prostate cancer treated with or without Abiraterone plus prednisone in the PEACE-1 phase 3 trial. J Clin Oncol. 2022;40(6_suppl):19. doi:10.1200/JCO.2022.40.6_suppl.019
72. Wu LM, Tanenbaum ML, Dijkers MP, et al. Cognitive and neurobehavioral symptoms in patients with non-metastatic prostate cancer treated with androgen deprivation therapy or observation: a mixed methods study. Soc Sci Med. 2016;156:80–89. doi:10.1016/j.socscimed.2016.03.016
73. Wu LM, Diefenbach MA, Gordon WA, Cantor JB, Cherrier MM. Cognitive problems in patients on androgen deprivation therapy: a qualitative pilot study. Urol Oncol. 2013;31(8):1533–1538. doi:10.1016/j.urolonc.2012.07.003
74. McGinty HL, Phillips KM, Jim HS, et al. Cognitive functioning in men receiving androgen deprivation therapy for prostate cancer: a systematic review and meta-analysis. Support Care Cancer. 2014;22(8):2271–2280. doi:10.1007/s00520-014-2285-1
75. Gonzalez BD, Jim HS, Booth-Jones M, et al. Course and predictors of cognitive function in patients with prostate cancer receiving androgen-deprivation therapy: a controlled comparison. J Clin Oncol. 2015;33(18):2021–2027. doi:10.1200/JCO.2014.60.1963
76. Siebert AL, Lapping-Carr L, Morgans AK. Neuropsychiatric impact of androgen deprivation therapy in patients with prostate cancer: current evidence and recommendations for the clinician. Eur Urol Focus. 2020;6(6):1170–1179. doi:10.1016/j.euf.2020.05.014
77. Sari Motlagh R, Quhal F, Mori K, et al. The risk of new onset dementia and/or Alzheimer disease among patients with prostate cancer treated with androgen deprivation therapy: a systematic review and meta-analysis. J Urol. 2021;205(1):60–67. doi:10.1097/JU.0000000000001341
78. Finley SK, Kritzer MF. Immunoreactivity for intracellular androgen receptors in identified subpopulations of neurons, astrocytes and oligodendrocytes in primate prefrontal cortex. J Neurobiol. 1999;40(4):446–457. doi:10.1002/(SICI)1097-4695(19990915)40:4<446::AID-NEU3>3.0.CO;2-J
79. Verdile G, Laws SM, Henley D, et al.; AIBL Research Group. Associations between gonadotropins, testosterone and β amyloid in men at risk of Alzheimer’s disease. Mol Psychiatry. 2014;19(1):69–75. doi:10.1038/mp.2012.147
80. Marandino L, Vignani F, Buttigliero C, et al. Evaluation of cognitive function in trials testing new-generation hormonal therapy in patients with prostate cancer: a systematic review. Cancers. 2020;12(9):2568. doi:10.3390/cancers12092568
81. Wefel JS, Ryan CJ, Van J, Jackson JC, Morgans AK. Assessment and management of cognitive function in patients with prostate cancer treated with second-generation androgen receptor pathway inhibitors. CNS Drugs. 2022;36(5):419–449. doi:10.1007/s40263-022-00913-5
82. Thiery-Vuillemin A, Poulsen MH, Lagneau E, et al.; AQUARiUS Investigators. Impact of abiraterone acetate plus prednisone or enzalutamide on patient-reported outcomes in patients with metastatic castration-resistant prostate cancer: final 12-mo analysis from the observational AQUARiUS study. Eur Urol. 2020;77(3):380–387. doi:10.1016/j.eururo.2019.09.019
83. Shore ND, Saltzstein D, Sieber P, et al. Results of a Real-World Study of Enzalutamide And Abiraterone Acetate With Prednisone Tolerability (REAAcT). Clin Genitourin Cancer. 2019;17(6):457–463.e6. doi:10.1016/j.clgc.2019.07.017
84. Shore ND, Antonarakis ES, Cookson MS, et al. Optimizing the role of androgen deprivation therapy in advanced prostate cancer: challenges beyond the guidelines. Prostate. 2020;80(6):527–544. doi:10.1002/pros.23967
85. Sparasci D, Napoli I, Rossi L, et al. Prostate cancer and sleep disorders: a systematic review. Cancers. 2022;14(7):1784. doi:10.3390/cancers14071784
86. Jones JM, Kohli M, Loprinzi CL. Androgen deprivation therapy-associated vasomotor symptoms. Asian J Androl. 2012;14(2):193–197. doi:10.1038/aja.2011.101
87. Crook JM, O’Callaghan CJ, Duncan G, et al. Intermittent androgen suppression for rising PSA level after radiotherapy. N Engl J Med. 2012;367(10):895–903. doi:10.1056/NEJMoa1201546
88. Rhee H, Gunter JH, Heathcote P, et al. Adverse effects of androgen-deprivation therapy in prostate cancer and their management. BJU Int. 2015;115(Suppl 5):3–13. doi:10.1111/bju.12964
89. Loprinzi CL, Michalak JC, Quella SK, et al. Megestrol acetate for the prevention of hot flashes. N Engl J Med. 1994;331(6):347–352. doi:10.1056/NEJM199408113310602
90. Irani J, Salomon L, Oba R, Bouchard P, Mottet N. Efficacy of venlafaxine, medroxyprogesterone acetate, and cyproterone acetate for the treatment of vasomotor hot flushes in men taking gonadotropin-releasing hormone analogues for prostate cancer: a double-blind, randomised trial. Lancet Oncol. 2010;11(2):147–154. doi:10.1016/S1470-2045(09)70338-9
91. Loprinzi CL, Dueck AC, Khoyratty BS, et al. A phase III randomized, double-blind, placebo-controlled trial of gabapentin in the management of hot flashes in men (N00CB). Ann Oncol. 2009;20(3):542–549. doi:10.1093/annonc/mdn644
92. Ashamalla H, Jiang ML, Guirguis A, Peluso F, Ashamalla M. Acupuncture for the alleviation of hot flashes in men treated with androgen ablation therapy. Int J Radiat Oncol Biol Phys. 2011;79(5):1358–1363.
93. Calais da Silva FE, Bono AV, Whelan P. Intermittent androgen deprivation for locally advanced and metastatic prostate cancer: results from a randomised phase 3 study of the South European Uroncological Group. Eur Urol. 2009;55(6):1269–1277. doi:10.1016/j.eururo.2009.02.016
94. Nguyen PL, Alibhai SM, Basaria S, et al. Adverse effects of androgen deprivation therapy and strategies to mitigate them. Eur Urol. 2015;67(5):825–836. doi:10.1016/j.eururo.2014.07.010
95. Higano CS. Sexuality and intimacy after definitive treatment and subsequent androgen deprivation therapy for prostate cancer. J Clin Oncol. 2012;30(30):3720–3725. doi:10.1200/JCO.2012.41.8509
96. Storey DJ, McLaren DB, Atkinson MA, et al. Clinically relevant fatigue in men with hormone-sensitive prostate cancer on long-term androgen deprivation therapy. Ann Oncol. 2012;23(6):1542–1549. doi:10.1093/annonc/mdr447
97. Ternov KK, Sønksen J, Fode M, et al. Fatigue, health-related quality-of-life and metabolic changes in men treated with enzalutamide or Abiraterone acetate plus prednisone for metastatic castration-resistant prostate cancer: a randomised clinical trial (HEAT). Eur J Cancer. 2022;171:75–84. doi:10.1016/j.ejca.2022.04.034
98. Cormie P, Zopf EM. Exercise medicine for the management of androgen deprivation therapy-related side effects in prostate cancer. Urol Oncol. 2020;38(2):62–70. doi:10.1016/j.urolonc.2018.10.008
99. Baguley BJ, Skinner TL, Jenkins DG, Wright ORL. Mediterranean-style dietary pattern improves cancer-related fatigue and quality of life in men with prostate cancer treated with androgen deprivation therapy: a pilot randomised control trial. Clinical Nutr. 2021;40(1):245–254. doi:10.1016/j.clnu.2020.05.016
100. Coviello AD, Kaplan B, Lakshman KM, Chen T, Singh AB, Bhasin S. Effects of graded doses of testosterone on erythropoiesis in healthy young and older men. J Clin Endocrinol Metab. 2008;93(3):914–919. doi:10.1210/jc.2007-1692
101. Grossmann M, Zajac JD. Hematological changes during androgen deprivation therapy. Asian J Androl. 2012;14(2):187–192. doi:10.1038/aja.2011.102
102. Corona G, Filippi S, Comelio P, et al. Sexual function in men undergoing androgen deprivation therapy. Int J Impot Res. 2021;33(4):439–447. doi:10.1038/s41443-021-00418-7
103. Lapi F, Azoulay L, Niazi MT, Yin H, Benayoun S, Suissa S. Androgen deprivation therapy and risk of acute kidney injury in patients with prostate cancer. JAMA. 2013;310(3):289–296. doi:10.1001/jama.2013.8638
104. Ng E, Woo HH, Turner S, Leong E, Jackson M, Spry N. The influence of testosterone suppression and recovery on sexual function in men with prostate cancer: observations from a prospective study in men undergoing intermittent androgen suppression. J Urol. 2012;187(6):2162–2166. doi:10.1016/j.juro.2012.01.080
105. Saltalamacchia G, Frascaroli M, Bernardo A, Quaquarini E. Renal and cardiovascular toxicities by new systemic treatments for prostate cancer. Cancers. 2020;12(7):1750. doi:10.3390/cancers12071750
106. Attard G, Reid AH, Auchus RJ, et al. Clinical and biochemical consequences of CYP17A1 inhibition with Abiraterone given with and without exogenous glucocorticoids in castrate men with advanced prostate cancer. J Clin Endocrinol Metab. 2012;97(2):507–516. doi:10.1210/jc.2011-2189
107. European Medicines Agency. Annex 1- Summary of Product Characteristics. Available from: https://www.ema.europa.eu/en/documents/product-information/zytiga-epar-product-information_en.pdf.
108. European Medicines Agency. Part VI: Summary of the Risk Management Plan. Available from: https://www.ema.europa.eu/en/documents/rmp-summary/erleada-epar-risk-management-plan-summary_en.pdf.
109. European Medicines Agency. Summary of Risk Management Plan (RMP) for NUBEQA® (darolutamide). Available from: https://www.ema.europa.eu/en/documents/rmp-summary/nubeqa-epar-risk-management-plan-summary_en.pdf.
110. Smith MR, Hussain M, Saad F, et al.; ARASENS Trial Investigators. Darolutamide and survival in metastatic, hormone-sensitive prostate cancer. N Engl J Med. 2022;386(12):1132–1142. doi:10.1056/NEJMoa2119115
111. Fowler FJ Jr, McNaughton Collins M, Walker Corkery E, Elliott DB, Barry MJ. The impact of androgen deprivation on quality of life after radical prostatectomy for prostate carcinoma. Cancer. 2002;95(2):287–295. doi:10.1002/cncr.10656
112. Ost P, Reynders D, Decaestecker K, et al. Surveillance or metastasis-directed therapy for oligometastatic prostate cancer recurrence: a prospective, randomized, multicenter phase II trial. J Clin Oncol. 2018;36(5):446–453. doi:10.1200/JCO.2017.75.4853
113. Phillips R, Shi WY, Deek M, et al. Outcomes of observation vs stereotactic ablative radiation for oligometastatic prostate cancer: the ORIOLE phase 2 randomized clinical trial. JAMA Oncol. 2020;6(5):650–659. doi:10.1001/jamaoncol.2020.0147
114. Deek MP, Van der Eecken K, Sutera P, et al. Long-term outcomes and genetic predictors of response to metastasis-directed therapy versus observation in oligometastatic prostate cancer: analysis of STOMP and ORIOLE trials. J Clin Oncol. 2022;40(29):3377–3382. doi:10.1200/JCO.22.00644
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.