Back to Journals » Advances in Medical Education and Practice » Volume 17
How to Implement Structured Case-Based Resource Sessions Within the Medical Curriculum
Authors Tobón GJ
Received 9 January 2026
Accepted for publication 28 March 2026
Published 16 April 2026 Volume 2026:17 594899
DOI https://doi.org/10.2147/AMEP.S594899
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Gabriel J Tobón1,2
1Department of Medical Microbiology, Immunology and Cell Biology, Southern Illinois University School of Medicine, Springfield, IL, USA; 2Department of Internal Medicine, Division of Rheumatology, Southern Illinois University School of Medicine, Springfield, IL, USA
Correspondence: Gabriel J Tobón, Department of Medical Microbiology, Immunology and Cell Biology, Southern Illinois University School of Medicine, 825 N. Rutledge St, Room 2610, Springfield, IL, 62702, USA, Email [email protected]
Background: Medical education is shifting from traditional lectures toward active, learner-centered approaches. Although case-based learning (CBL) is widely used, there is limited practical guidance on how to implement structured, scalable Case-Based Resource Sessions (CBRS) as a faculty-guided alternative to both lectures and resource-intensive problem-based learning (PBL).
Methods: This paper presents a practical five-step guide for implementing structured CBRS, developed over 5 years of iterative experience in pathology and immunology courses at Southern Illinois University School of Medicine (≈75 students per year).
Results: The guide includes: (1) defining learning objectives using Bloom’s taxonomy, (2) realistic case selection and development, (3) session structuring with progressive disclosure, (4) skilled facilitation using interactive tools and Socratic questioning, and (5) structured feedback and assessment. Key benefits observed include improved student engagement, knowledge retention, clinical reasoning, and preparation for clinical rotations.
Conclusion: CBRS represent a valuable, resource-efficient addition to the medical curriculum. Challenges and best practices for successful implementation are discussed to support educators in adopting this approach.
Keywords: case-based resource sessions, medical education, active learning, clinical reasoning, case-based learning, problem-based learning
Introduction
Medical education is undergoing a sustained transition from traditional lecture-based instruction toward more active, learner-centered approaches.1,2 Among these, case-based learning (CBL) has emerged as an effective strategy to promote clinical reasoning, knowledge integration, and application of foundational sciences to clinical practice.3–8
Despite its widespread adoption and demonstrated effectiveness, there remains a critical gap in the literature. While numerous studies have evaluated the outcomes of CBL,8–10 there is limited practical guidance on how to systematically design and implement structured, scalable case-based sessions within real-world medical curricula. Existing frameworks often describe general principles but provide insufficient operational detail for educators seeking reproducible sessions across courses and institutions.9 This lack of structured implementation guidance can lead to variability in quality, inconsistency in learning outcomes, and challenges in faculty adoption.
In this context, Case-Based Resource Sessions (CBRS) are recommended as a faculty-guided, structured, and scalable adaptation of CBL. CBRS are defined here as whole-class or large-group sessions that use realistic clinical cases with progressive disclosure and interactive tools (eg, polls, concept maps). Unlike traditional CBL reported in the literature, CBRS emphasize scalability and consistent faculty guidance while remaining less resource-intensive than problem-based learning (PBL), which typically involves small-group, student-driven inquiry.4 This design positions CBRS as a practical bridge between conventional lectures and resource-heavy PBL.
The aim of this manuscript is to provide a practical, theory-informed five-step framework for implementing CBRS. The framework is grounded in established educational principles—including backward design (which prioritizes defining learning outcomes first), Bloom’s taxonomy (to target higher-order cognitive skills such as analysis and clinical reasoning), and active learning strategies—and has been refined over 5 years of iterative implementation in pathology and immunology courses at Southern Illinois University School of Medicine.
The primary goals of CBRS—engaging learners, improving knowledge retention, promoting critical thinking, and enhancing clinical decision-making—are supported by evidence from active-learning literature.7 By simulating realistic clinical scenarios that integrate pathophysiology, diagnosis, and management, CBRS help students transition from classroom learning to clinical rotations and board examinations with greater confidence and competence. The interactive nature of these sessions, supported by digital tools, further stimulates participation and collaborative learning in a low-stakes environment.
Materials and Methods
This five-step guide was developed through 5 years of iterative implementation and continuous refinement of CBRS in the pathology and immunology (M2) courses at Southern Illinois University School of Medicine (approximately 75 students per year). Cases were created from de-identified patient records and faculty clinical experience and were progressively refined through annual student feedback surveys, faculty peer review, and quality improvement cycles. The framework is grounded in established educational design principles, including:
- Backward design (Wiggins & McTighe, 2005), which prioritizes the definition of desired learning outcomes before developing instructional activities and assessments;11
- Bloom’s taxonomy12 (Anderson & Krathwohl, 2001),13 to ensure that learning objectives target higher-order cognitive skills such as “apply,” “analyze,” and “evaluate” rather than simple recall;
- Active learning principles, which have been consistently associated with improved knowledge retention, clinical reasoning, and student performance compared with traditional lectures.7
Additional development elements included explicit alignment with course-level learning outcomes, integration across disciplines (pathophysiology, diagnosis, and treatment), progressive refinement of case structure and facilitation strategies, and adaptation to large-group teaching environments. This iterative, theory-informed process resulted in a structured, reproducible, and scalable five-step model designed to enhance clarity, reproducibility, and practical utility for medical educators.
Results
The Five-Step Framework for CBRS Implementation
The successful implementation of CBRS follows a structured five-step framework developed through iterative institutional experience. Each step is designed to ensure clarity, reproducibility, and scalability while promoting higher-order clinical reasoning.
Step 1: Define Learning Outcomes
The process begins with clearly defined learning outcomes aligned with course objectives and institutional competencies. Using Bloom’s taxonomy, outcomes prioritize higher-order cognitive skills (apply, analyze, evaluate) in the domains of pathophysiology, diagnosis, and management. Rather than focusing solely on broad curricular goals, outcomes specify what learners should be able to analyze, interpret, or apply during the session.
Step 2: Case Selection and Development
High-quality, clinically authentic cases are central to CBRS. Cases are developed through a systematic process: 1) selection of a clinical topic aligned with the defined learning outcomes; 2) compilation of realistic, de-identified patient data (history, physical examination, laboratory results, and imaging) drawn from institutional records and/or faculty clinical experience; 3) structuring with progressive disclosure and embedded questions addressing pathophysiology, differentials, diagnosis, and management; 4) ensuring diversity in patient demographics (age, sex, ethnicity, socioeconomic factors); and 5) iterative refinement through peer review by at least two faculty members to confirm accuracy, appropriate complexity, and authenticity. Cases are calibrated to students’ knowledge level and formatted in a USMLE-style structure.
Step 3: Structure the Session
A consistent session format enhances educational value and active engagement. The session follows a structured sequence: 1) case introduction, 2) initial analysis by learners, 3) guided discussion with progressive disclosure of information, 4) clarification of key concepts, and 5) summary and consolidation of learning points.
Step 4: Facilitation
Effective facilitation is essential for maintaining focus and promoting deep reasoning. The facilitator guides discussion using Socratic questioning (eg, “What is the primary issue in this case?”, “What additional information is required?”, “What are the alternative diagnoses?”), addresses misconceptions with rational explanations, and encourages broad participation. Interactive tools such as audience response systems, polls, and concept maps are employed to enhance engagement, particularly in large-group settings, while ensuring efficient time management.
Step 5: Assessment and Feedback Assessment
It is formative and integrated throughout the session. Immediate feedback is provided on learner responses, with explicit discussion of the reasoning behind correct and incorrect answers. Key learning points are reinforced using tools such as concept maps, flowcharts, or summary frameworks to consolidate knowledge and support long-term retention.14
Box 1 summarizes the five recommended steps for implementing a successful CBRS.
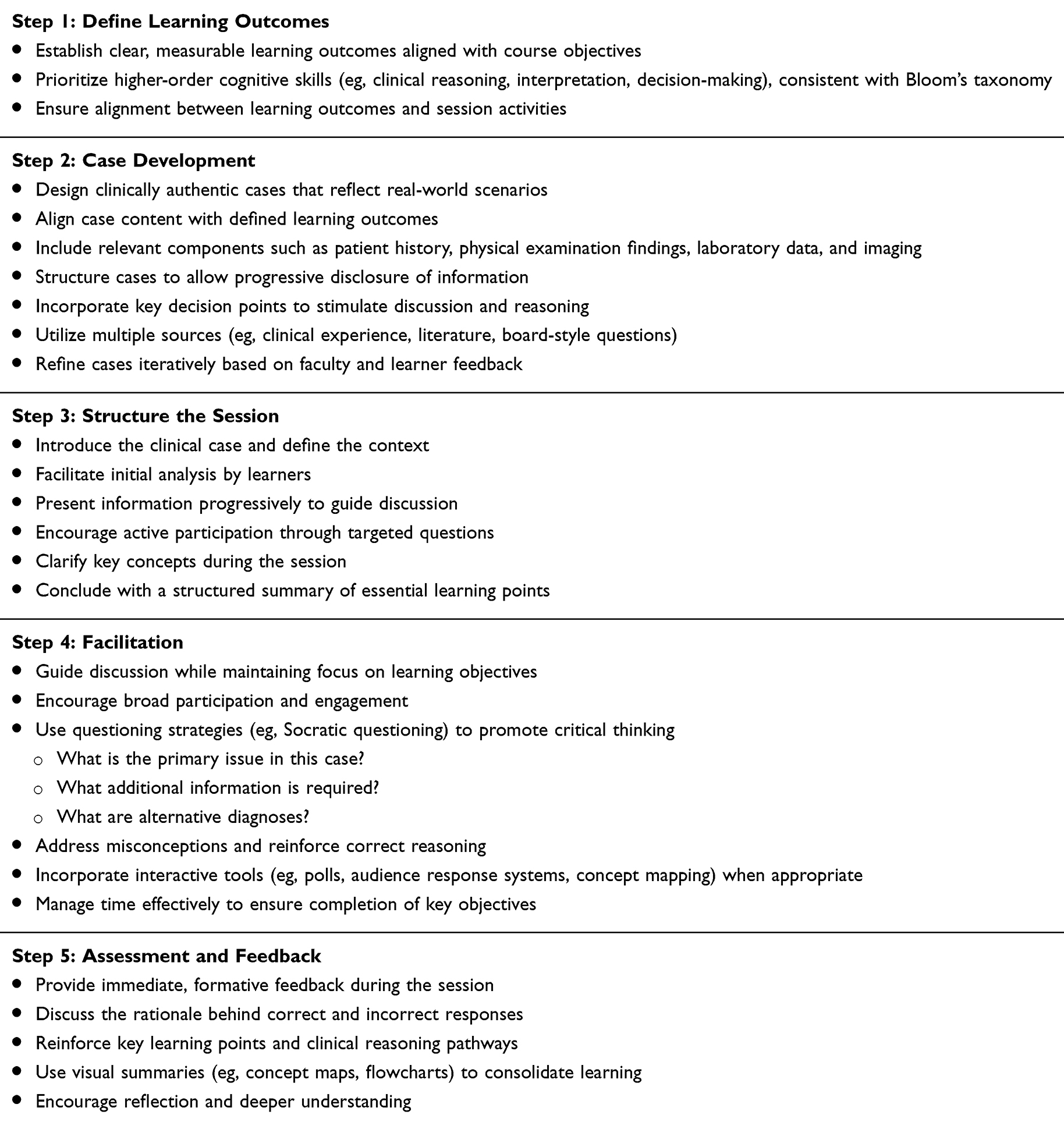 |
Box 1 Step-by-Step Framework for Implementing Case-Based Resource Sessions (CBRS) |
Discussion
This manuscript presents a structured, theory-informed five-step framework for implementing CBRS within medical education. Rather than proposing an entirely novel pedagogical approach, the work offers a clear and operational articulation of best practices that are often applied inconsistently across institutions. By integrating established educational principles such as backward design and Bloom’s taxonomy, the framework ensures that sessions are both interactive and purposefully aligned with learning outcomes, thereby promoting higher-order clinical reasoning.
A key contribution of CBRS lies in its emphasis on scalability and practicality. Unlike traditional small-group PBL, which is resource-intensive, or conventional CBL that may lack consistent structure in large-group settings, CBRS are specifically designed as a faculty-guided, whole-class model that bridges lectures and more intensive active-learning formats. This distinction makes the approach particularly feasible for integration into existing medical curricula.
To maximize the effectiveness of CBRS, educators should foster a safe learning environment that encourages open dialogue and broad participation. Incorporating interdisciplinary perspectives and leveraging digital technologies—such as audience response systems, polls, concept maps, and multimedia cases—can further enrich the learning experience and maintain student engagement.
Nevertheless, implementing CBRS is not without challenges. Developing high-quality, authentic cases is time- and resource-intensive, and effective facilitation requires skilled faculty. Some students may initially resist the shift from familiar lecture-based formats. To overcome these barriers, institutions can establish shared case repositories, implement faculty development programs focused on case writing and Socratic questioning, and introduce CBRS early in the curriculum to help students become accustomed to this interactive method.
The framework presented here acknowledges that many individual elements of CBRS are already practiced in various forms. Its primary value lies in providing a reproducible, scalable structure that can reduce variability in implementation and support broader adoption across courses and institutions.
Limitations and Future Directions
This work is based on experiential implementation and iterative refinement within a single institution and does not include formal quantitative evaluation of learning outcomes. Future research should rigorously assess the impact of CBRS on student engagement, knowledge retention, clinical reasoning skills, and preparedness for clinical rotations. Comparative studies with traditional lectures, standard CBL, and PBL would further strengthen the evidence base and help refine the framework.
Conclusion
CBRS provide a structured, practical, and scalable approach to integrating CBL within medical curricula. By aligning learning outcomes, case design, facilitation, and feedback, the proposed five-step framework offers a reproducible model that enhances active learning and clinical reasoning.
Rather than representing a paradigm shift, this framework articulates best practices in a clear and operational manner, supporting more consistent and effective implementation across courses and institutions. CBRS serve as a valuable complement or alternative to traditional lectures and resource-intensive PBL, promoting greater student engagement, knowledge retention, and preparation for clinical rotations.
Although implementation challenges remain, the benefits of CBRS make them a worthwhile addition to the evolving medical curriculum and a useful tool in shaping competent future physicians.
Ethical Approval
No ethical approval was required as this study was based on the author’s own experience. No primary data are presented.
Funding
This study did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Thomas BC, Tiarks GC, Al-Eyd G, Rajput V. Keeping lectures alive in undergraduate medical education: current status, evolution, and future goals. Cureus. 2025;17(7):e87784. doi:10.7759/cureus.87784
2. Zeng HL, Chen DX, Li Q, Wang XY. Effects of seminar teaching method versus lecture-based learning in medical education: a meta-analysis of randomized controlled trials. Med Teach. 2020;42(12):1343–6. doi:10.1080/0142159X.2020.1805100
3. Salehi AM, Ramezani M, Khanlarzadeh E, Khatiban M, Ahmadian M, Alizadeh Z. Design, implementation, and evaluation of case-based learning aimed at improving undergraduate medical students’ satisfaction, attitude, knowledge, and skills in the anatomy course: an interventional study. J Med Educ Curric Dev. 2025;12:23821205251317942. doi:10.1177/23821205251317942
4. Zhao W, He L, Deng W, Zhu J, Su A, Zhang Y. The effectiveness of the combined problem-based learning (PBL) and case-based learning (CBL) teaching method in the clinical practical teaching of thyroid disease. BMC Med Educ. 2020;20(1):381. doi:10.1186/s12909-020-02306-y
5. Varma B, Karuveettil V, Fernandez R, et al. Effectiveness of case-based learning in comparison to alternate learning methods on learning competencies and student satisfaction among healthcare professional students: a systematic review. J Educ Health Promot. 2025;14:76. doi:10.4103/jehp.jehp_510_24
6. Nair SP, Shah T, Seth S, Pandit N, Shah GV. Case based learning: a method for better understanding of biochemistry in medical students. J Clin Diagn Res. 2013;7(8):1576–1578. doi:10.7860/JCDR/2013/5795.3212
7. Freeman S, Eddy SL, McDonough M, et al. Active learning increases student performance in science, engineering, and mathematics. Proc Natl Acad Sci U S A. 2014;111(23):8410–8415. doi:10.1073/pnas.1319030111
8. Miller CJ, McNear J, Metz MJ. A comparison of traditional and engaging lecture methods in a large, professional-level course. Adv Physiol Educ. 2013;37(4):347–355. doi:10.1152/advan.00050.2013
9. Daly R, Tunney E, Spooner M, Offiah G, Flood K, Kent F. Case-based learning (CBL) in undergraduate health professions education: a realist review. Med Educ. 2026. doi:10.1111/medu.70179
10. Xiong X, Xu J, Luo M, et al. Efficacy of problem-based learning combined with case-based learning versus lecture-based learning in orthopedic education: a systematic review and meta-analysis. BMC Med Educ. 2025;25(1):1357. doi:10.1186/s12909-025-07741-3
11. Wiggins G, McTighe J. Understanding by Design.
12. Bloom BS, Krathwohl DR. Taxonomy of educational objectives: the classification of educational goals. In: Handbook I: Cognitive Domain. New York: Longmans, Green; 1956.
13. Anderson LW, Krathwohl DR, editors. A Taxonomy for Learning, Teaching, and Assessing: A Revision of Bloom’s Taxonomy of Educational Objectives. Boston, MA: Allyn & Bacon; 2001.
14. Traylor B, Fenner E, Western A, et al. Concept mapping plays a complementary role in optimizing the effectiveness of interactive simulations in medical student learning of bacterial sepsis pathophysiology. Med Sci Educ. 2025;35(3):1537–1549. doi:10.1007/s40670-025-02348-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.