Back to Journals » International Journal of Women's Health » Volume 17
How Resilience Mitigates Depression After IVF-ET Failure: A Moderated Mediation Model of Hope, Social Relations, and Income in China
Authors Wang X, Yang M, Zhang Y, Zhang Y ![]() , Lin Y
, Lin Y ![]() , Sun S, Jiang L
, Sun S, Jiang L
Received 26 June 2025
Accepted for publication 14 October 2025
Published 25 October 2025 Volume 2025:17 Pages 3865—3879
DOI https://doi.org/10.2147/IJWH.S549816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Xiaoyu Wang,1 Mengye Yang,2 Yan Zhang,2 Yan Zhang,1 Yiwen Lin,1 Shijing Sun,1 Ling Jiang1
1Department of Nursing, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, Suzhou, People’s Republic of China; 2Reproductive Genetic Center, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, Suzhou, People’s Republic of China
Correspondence: Ling Jiang, Department of Nursing, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, 26th Daoqian Road, Suzhou, 215000, People’s Republic of China, Email [email protected] Mengye Yang, Reproductive Genetic Center, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, 26th Daoqian Road, Suzhou, 215000, People’s Republic of China, Email [email protected]
Background: Failed in vitro fertilization–embryo transfer (IVF-ET) cycles may exacerbate depressive symptoms among women. Resilience is widely recognized as a protective factor for psychological well-being. However, its role in alleviating depressive symptoms among women failed IVF-ET cycles in China remains insufficiently explored.
Purpose: To explore how resilience affects depressive symptoms among women failed IVF-ET cycles in China, where strong emphasis is placed on family lineage.
Patients and Methods: The cross-sectional study included 315 women failed IVF-ET cycles between June and December 2024. The 10-item Connor-Davidson Resilience Scale, the Patient Health Questionnaire, the Chinese version of the Herth Hope Index, and the social and marital relations subscales of the Fertility Quality of Life Scale were used for measurements. A moderated mediation model was tested in Mplus 8.3 to examine the direct and indirect effects of resilience on depressive symptoms, with hope and social relations as mediators and household income and healthcare payment methods as moderators.
Results: Resilience is negatively related to depressive symptoms, with hope and social relations acting as mediators. Additionally, household income moderates the pathway through which resilience influences depressive symptoms via hope, whereas the method of healthcare payment does not exhibit a moderating effect.
Conclusion: Resilience plays a critical role in mitigating depressive symptoms among women failed IVF-ET cycles in China, exerting both direct and indirect effects through the pathways of hope and social relations. Socioeconomic factors also serve as moderators in this process. To effectively support this population, the health system should integrate cultural context into the design of interventions by providing targeted psychological and social support and advocating for policy-level economic assistance.
Keywords: depressive symptoms, resilience, failed IVF-ET cycles, mental health, socioeconomic factors
Introduction
In recent years, the prevalence of infertility among women has risen globally.1 In vitro fertilization–embryo transfer (IVF-ET) remains the main assisted reproductive therapy (ART) for infertility. However, the process of this treatment is complex, involving multiple medical procedures, such as ovarian stimulation, egg retrieval, embryo culture, and embryo transfer.2 It is often associated with high financial costs, physical discomfort, and uncertain outcomes, all of which can contribute to a substantial psychological burden for women, increasing their risk of depressive symptoms.3 A prospective cohort study conducted in China with 432 women undergoing IVF-ET, including both first-time patients and those undergoing repeated cycles, found a positive correlation between the number of IVF-ET cycles and the severity of depressive symptoms.4 Moreover, a longitudinal study showed that women exhibited an increase in depressive symptoms after unsuccessful treatment and a decrease after successful treatment. More than 20% of women failed IVF-ET cycles showed subclinical forms of depression six months later.5 Given the substantial psychological impact of IVF-ET failure, it is crucial to investigate the underlying mechanisms that contribute to depressive symptoms in this population.
Resilience is widely recognized as a critical factor influencing psychological health outcomes. While resilience is defined by the American Psychological Association as “the process of adapting well in the face of adversity, trauma, tragedy, threats or even significant sources of threat”,6 its meaning is deeply embedded within cultural contexts. In the western cultures, resilience often emphasizes self-reliance and personal mastery when confronting challenges.7,8 This contrasts with the perspective in China, where Confucian philosophy frames adversity as a positive opportunity to cultivate willpower, and underscores the crucial role of harmonious interpersonal relations in adaptation.7 Within this collectivist context, resilience is reinforced not only by personal strengths but also by fulfilling social expectations.9 This cultural divergence presents a challenge for measurement. For example, studies using the Connor-Davidson Resilience Scale (CD-RISC)—a tool originally developed with American samples—have found that its “Control” factor does not emerge as an independent dimension in Chinese populations.10,11 This discrepancy suggests that collectivist values in China lead individuals to prioritize adapting through reliance on interpersonal networks rather than solely on personal control.7,10 The abbreviated version, CD-RISC-10, effectively captures individuals’ capacity for recovery in the face of adversity. Although its unidimensional structure does not explicitly reflect collectivist values and familial expectations, it demonstrates strong reliability, validity, and cross-cultural applicability in the Chinese context.11,12 This may be attributable to the fact that its items, such as “I can grow stronger through hardship”, resonate closely with the Confucian notion of “thriving through adversity”. Furthermore, Cheng et al demonstrated that the CD-RISC-10 exhibits measurement invariance across depressed and non-depressed groups in China, further supporting its utility in research on depressive symptoms.12
Although existing studies have established the link between resilience and depressive symptoms, they have focused on the populations like patients with chronic illnesses or adolescents.13–15 There is limited research on women who have experienced failed in IVF-ET cycles. This gap is especially significant in China, where collectivist culture and Confucian values deeply shape women’s mental health,16,17 and may influence how resilience function. Therefore, the specific mechanisms through which resilience protects against depressive symptoms in this population remain poorly understood, necessitating further studies.
Previous study has suggested that resilience influences depressive symptoms through two key pathways: an internal psychological resource and an external social resource.17,18 In the Chinese context, resilience is deeply intertwined with relational resources, including social and marital support.7 However, infertility can disrupt these relationships through social stigma, spousal blame, and negative reactions from family—experiences common for women in China.19,20 While strained relationships undermine resilience and worsen depression, supportive and harmonious relations can facilitate recovery.7,14 Thus, the ability to build and maintain supportive interpersonal relations may be another key mediator through which resilience protects against depressive symptoms.
Beyond supportive interpersonal relations, personal strengths are also essential.19 Hope, as a positive personal resource, plays a key role in this process. As defined by Snyder, hope is “a positive motivational state that is based on an interactively derived sense of successful agency (goal-directed energy) and pathways (planning to meet goals)”.21 This motivational state encourages individuals to set and pursue goals, which helps them cope with and adapt effectively to stressors. In this regard, many researchers propose a direct relationship between hope and resilience.22,23 A prospective cohort study demonstrated a positive correlation between resilience and hope, with resilience emerging as a crucial predictor of psychological distress.24 And a systematic review and meta-analysis, including 22 longitudinal studies, revealed a medium association between low levels of hope in the early stages and subsequent depressive symptoms.25 Accordingly, we speculate that hope may function as an intermediary process through which resilience alleviates depressive symptoms.
Moreover, the environmental context is very influential on resilience in the process of stress adaptation, with socioeconomic factors being a critical element.18 Prior to July 1, 2023, assisted reproductive treatments were entirely self-financed in China, which imposed a substantial financial burden on infertile patients. On that date, Beijing became the first region to incorporate 16 assisted reproductive technologies into the medical insurance reimbursement system.26 This milestone marked the inception of medical insurance coverage for assisted reproduction in China. By June 2025, 31 provinces in mainland China, along with the Xinjiang Production and Construction Corps, had gradually incorporated certain assisted reproductive services into their medical insurance schemes, including oocyte retrieval, embryo culture, and embryo transfer.27 Against this policy backdrop, it is of substantial practical relevance to investigate whether healthcare payment methods influence depressive symptoms among women failed IVF-ET cycles. What’s more, existing research indicates that socioeconomic factors, including household income and healthcare payment methods, can improve individuals’ access to medical care and treatment opportunities, which may enhance individuals’ hope for future, potentially safeguarding them from depressive symptoms.28,29 And Kimhi demonstrated that higher resilience is associated with higher levels of hope; however, economic pressure undermines this positive expectation.28 And a qualitative study focused on the psychological distress of infertile patients reported that the high costs of fertility treatments, combined with limited insurance coverage, impose a substantial economic burden on couples undergoing ART.30 This financial strain leads to deteriorating relationships among couples, family members, and friends, further exacerbating mental distress.31 Therefore, when exploring the mechanisms underlying psychological distress in women failed IVF-ET cycles, the consideration of socioeconomic factors is particularly important, as they are essential for understanding mental health outcomes and developing effective intervention strategies.
In reviewing the existing literature, we propose a moderated mediation model that incorporates hope and interpersonal relations (social relations or marital relations) as mediators, with household income and healthcare payment methods serving as moderating variables (see Figure 1). The following hypotheses are proposed: H1: Resilience may be negatively correlated with depressive symptoms; H2: Resilience may be positively correlated with hope and interpersonal relations (including social and marital relations); H3: Household income and healthcare payment methods may affect depressive symptoms, resilience, hope, and interpersonal relations; H4: Hope and interpersonal relations may mediate the relationship between resilience and depressive symptoms; and H5: The indirect effect of resilience on depressive symptoms through hope/interpersonal relations may be moderated by household income/healthcare payment methods. The primary objective of this study is to provide a supplementary understanding of depressive symptoms in women failed IVF-ET cycles in China. Additionally, we seek to offer scientific references for the development of effective mental health promotion strategies, specifically tailored to the cultural and psychological factors unique to Asian populations.
 |
Figure 1 Conceptual mode. |
Methods
Study Design
A cross-sectional study design was used in this study.
Participants and Procedure
This cross-sectional study was conducted from June 2024 to December 2024 at a reproductive center of a tertiary hospital, China, where approximately 4,700 ART cycles are performed annually. In accordance with the requirement for a minimum sample size of 200 for structural equation modeling,32 as well as the principle that the sample size should be at least 10 times for each variable in regression analysis,33 a total of 315 women failed IVF-ET cycles were finally recruited through a convenience sampling method to participate in the study. The inclusion criteria were as follows: (1) a clinically diagnosis of infertility, defined as the failure to achieve successful pregnancy after 12 months of regular, unprotected sexual intercourse;34 (2) a history of IVF-ET failure, defined as biochemical pregnancy loss (serum HCG levels negative 14 days post-embryo transfer) or clinical pregnancy loss (the absence of at least one gestational sac with fetal heartbeat, as determined by ultrasound 4 to 5 weeks post-embryo transfer);35,36 (3) age≥ 20 years, which is the legal marriage age for women in China, along with a marriage certificate, as it is an essential document in order to seek fertility treatment in China; (4) no recent psychological treatment or counseling; (5) voluntary informed consent to participate. The exclusion criteria included: (1) either partner had biological children; (2) illiteracy or a low educational level that would impede understanding of the questionnaire.
A paper-based questionnaire was employed in this study. Data collection was conducted by a researcher who had undergone standardized training to ensure consistency throughout the process. Prior to the formal distribution of the questionnaire, a small-scale pilot test was conducted, which involved 10 participants meeting the inclusion criteria, to assess the applicability and validity of the scales within the context of this study. The data from the pilot test participants were excluded from the formal statistical analysis. Before the formal collection of the questionnaires, the researcher provided each participant with a detailed briefing on the study’s objectives and procedures, ensuring comprehensive understanding. All participants provided written informed consent prior to participation. To minimize potential environmental biases, all questionnaires were completed in a quiet, uninterrupted consultation room. During completion, the researcher provided individual guidance to the participants, ensuring that the questionnaires were completed in accordance with standardized instructions. The guidance was limited to explaining the terminology and questions in the questionnaire, without involving the study content itself, which avoided any inadvertent influence on the participants’ responses and safeguarding the objectivity and validity of the data. After completion, the researcher verified that all sections of the questionnaire had been filled out and addressed any missing values immediately. The response rate and validity of distributed questionnaires were both 100%.
Ethical Consideration
The study was approved by the Ethics Committee of Suzhou Municipal Hospital (K-2024-169-K02) and was conducted in accordance with the principles set forth in the Helsinki Declaration.
Measures
Demographic Data
Sociodemographic and disease-related data were collected through paper-based questionnaires and medical record system in the survey. The data included patients’ age, residential area, educational level, infertility duration, healthcare payment methods, employment status, annual household income, number of IVF-ET failed cycles, and whether the patient had resigned from work due to IVF-ET treatment. According to 2023 classification of annual household income in China, households with an income below 100,000 China yuan (CNY) were classified as “low income”; those earning between 100,000 and 200,000 CNY were categorized as “moderate income”; and those with an income of 200,000 CNY or more were classified as “high income”.37
Resilience
The 10-item Connor-Davidson Resilience Scale (CDRISC-10), developed by Campbell-Sills and Stein, was used to assess the participants’ resilience.38 This scale consists of 10 items (eg, I can grow stronger through hardship), each rated on a 5-point Likert scale (from 0 = never to 4 = always), with a total score ranging from 0 to 40. Higher total score indicates greater resilience. The Chinese version of the scale has also demonstrated favorable internal consistency and test–retest reliability.11 The Cronbach’s α for this study was 0.934.
Depressive Symptoms
The depressive symptoms were assessed using the Patient Health Questionnaire (PHQ-9), which is based on the nine diagnostic criteria for depression outlined in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR).39 Each item (eg, feeling nervous, anxious, or on edge) is rated on a 4-point scale. The total score ranges from 0 to 27, with higher scores indicating greater levels of depressive symptoms. Standard cut-off points are 5, 10, 15, and 20 for mild, moderate, moderately severe, and severe depressive symptoms, respectively. The Cronbach’s α for this scale was 0.824 in this study.
Hope
The Chinese version of the Herth Hope Index (HHI) was used to assess participants’ levels of hope. The HHI consists of 12 items across three dimensions: temporality and future (eg, I have a positive outlook toward life), positive readiness and expectancy (eg, I can see a light at the end of the tunnel), and interconnectedness (eg, I feel all alone).40 All items are measured on a 4-point Likert scale (1 = completely disagree, 4 = completely agree), with items 3 and 6 being reverse scored. The total score of the scale is the sum of the scores for all items, with higher scores indicating a greater level of hope. The HHI has been widely used in China and demonstrates high reliability and validity, with a Cronbach’s α of 0.881 in this study.
Interpersonal Domain
The interpersonal domain was assessed using the Fertility Quality of Life scale (FertiQoL), a globally validated instrument designed to evaluate quality of life in individuals with infertility. The scale was developed by the experts from European Society of Human Reproduction and Embryology (ESHRE) and American Society for Reproductive Medicine (ASRM).41 The core module (core-FertiQoL) comprises two domains: personal and the interpersonal.42 As this study focused on interpersonal relations, only the interpersonal domain was utilized. This domain includes two dimensions: social relations (eg, Have you felt socially isolated because of fertility problems?) and marital relations (eg, “Have fertility problems strengthened your commitment to your partner?”). Both subscales were rated on a five-point Likert scale (0 = always, 4 = never), yielding raw scores ranging from 0 to 24. These scores could be converted into standardized scores ranging from 0 to 100, and the conversion formula is the original score multiplied by 25 and divided by the number of items in the dimension.42 Higher scores reflect better quality of social or marital relations. In the present study, Cronbach’s α was 0.710 for the social relations subscale and 0.706 for the marital relations subscale.
Statistical Analysis
Data analyses were conducted using SPSS (Version 27.0; IBM) and Mplus (Version 8.3) software. To ensure data accuracy, Confirmatory Factor Analysis (CFA) was initially conducted using Mplus 8.3 to evaluate the latent structure of the measurement instruments. In accordance with Podsakoff ‘s recommendations, Harman’s single-factor test was applied to assess common method variance.43 The reliability of the scales was evaluated using Cronbach’s alpha (α) to confirm internal consistency.
Descriptive statistics were calculated to examine the participants’ sociodemographic characteristics and psychological variables. Considering that depressive symptoms followed a skewed distribution, Spearman correlation analysis was employed to examine the bivariate relationships between the primary study variables. Subsequently, independent-samples t-tests and one-way analyses of variance (ANOVAs), followed by post-hoc tests, were conducted to examine differences in depressive symptoms, resilience, hope, social relations and marital relations across sociodemographic variables (eg, age, annual household income), and disease-related variables (eg, infertility duration, number of failed IVF-ET cycles).
To further explore the potential mechanisms underlying depressive symptoms, a preliminary analysis was conducted using ordinary least squares (OLS) regression. First, the relationship between demographic characteristics (number of IVF-ET failed cycles, age, residence, education level, and infertility duration) and depressive symptoms was examined. Next, socioeconomic factors (household income, healthcare payment methods, employment status, and whether resignation due to IVF-ET for reproductive planning) were incorporated into the model to assess their independent effects. Finally, psychosocial factors (resilience, social relations, and hope) were introduced to construct a multi-level regression model. Based on the OLS regression result, a moderated mediation analysis was performed using Structural Equation Modeling (SEM) in Mplus 8.3. Mediation and moderation effects were tested by analyzing the statistical significance of each path model. Given the skewed distribution of depressive symptoms data, maximum likelihood estimation (ML) with bootstrapped standard errors was employed. This method is robust to non-normality and suitable for models with both continuous and categorical variables.44 All statistical tests were two-tailed, with significance set at the 0.05 level. A bootstrapping procedure was employed to test the significance of the total and indirect effects, with 5000 bootstrap samples drawn.45 Coefficients with 95% confidence intervals excluding zero were considered statistically significant. Given that household income is a multicategorical variable and healthcare payment method is binary, these were represented in the model using dummy variables generated through indicator coding, in accordance with the principles of Hayes and Preacher.46 The low-income and self-pay groups served as reference categories for comparing direct and indirect effects with the moderate/high-income and medical insurance payment groups. In the SEM analysis, model fit was evaluated using several fit indices, including χ2-goodness-of-fit, the Root Mean Square Error of Approximation (RMSEA; values < 0.10 indicate acceptable fit), the Standardized Root Mean Residual (SRMR; values < 0.08 indicate good fit), the Comparative Fit Index (CFI; values > 0.90 indicate reasonable fit) and the Tucker-Lewis Index (TLI; values > 0.90 suggest acceptable fit).47
Results
Confirmatory Factor Analysis
The measurement model was constructed, incorporating five distinct latent constructs: depressive symptoms, resilience, hope, social relations, and marital relations. The fit indices for this model indicated an overall acceptable fit, with CFI = 0.870, TLI = 0.861, SRMR = 0.064, and RMSEA = 0.056. Subsequently, a one-factor model was tested. The one-factor model exhibited poor fit to the data, with CFI = 0.644, TLI = 0.626, SRMR = 0.086, and RMSEA = 0.091. Therefore, our theoretical model outperformed the one-factor model, showing that the data in this study do not exhibit common method variance.
Demographic Characteristics
A total of 315 women failed IVF-ET cycles participated in this study. In the initial phase of the study, 362 women who met the inclusion and exclusion criteria were invited to participate; however, 47 declined, resulting in a response rate of 87.02%. The main reasons for refusal included reluctance to discuss fertility-related topics, lack of time due to work commitments, and personal disinterest. All participants completed the comprehensive questionnaire, which ensured the reliability of the data. Detailed information is shown in Table 1.
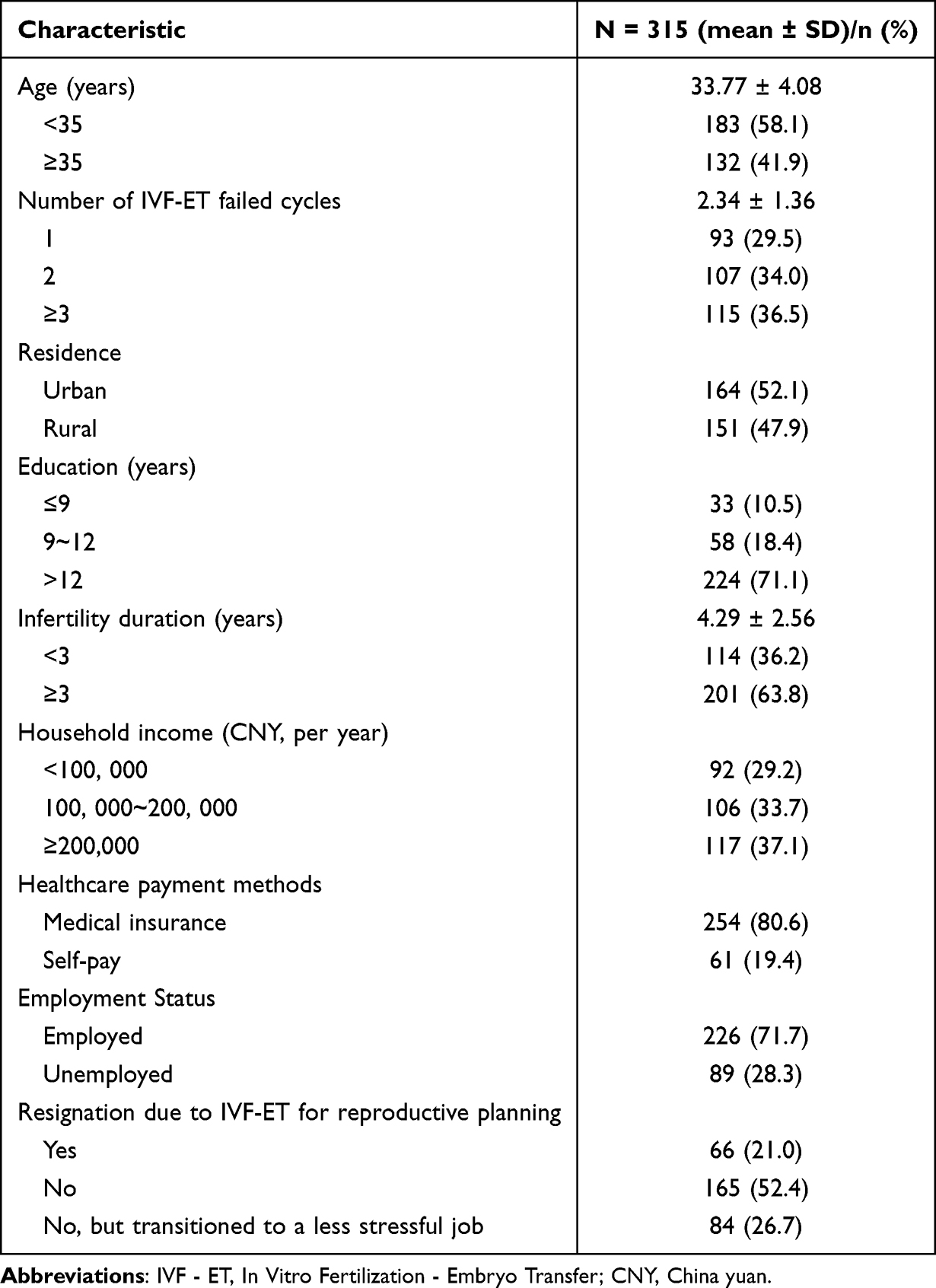 |
Table 1 Baseline Characteristics of the Participants (N = 315) |
Preliminary Analyses
The means, standard deviations (SDs), and Spearman correlations of the variables are presented in Table 2. The results showed that the mean PHQ-9 score among women failed IVF-ET cycles in China was approximately 5, corresponding to the threshold of mild depressive symptoms. Further analyses revealed significant differences in resilience, hope, social relations, and marriage relations among the no-depression, mild-depression, and moderate-to-severe depression groups (Appendix 1).
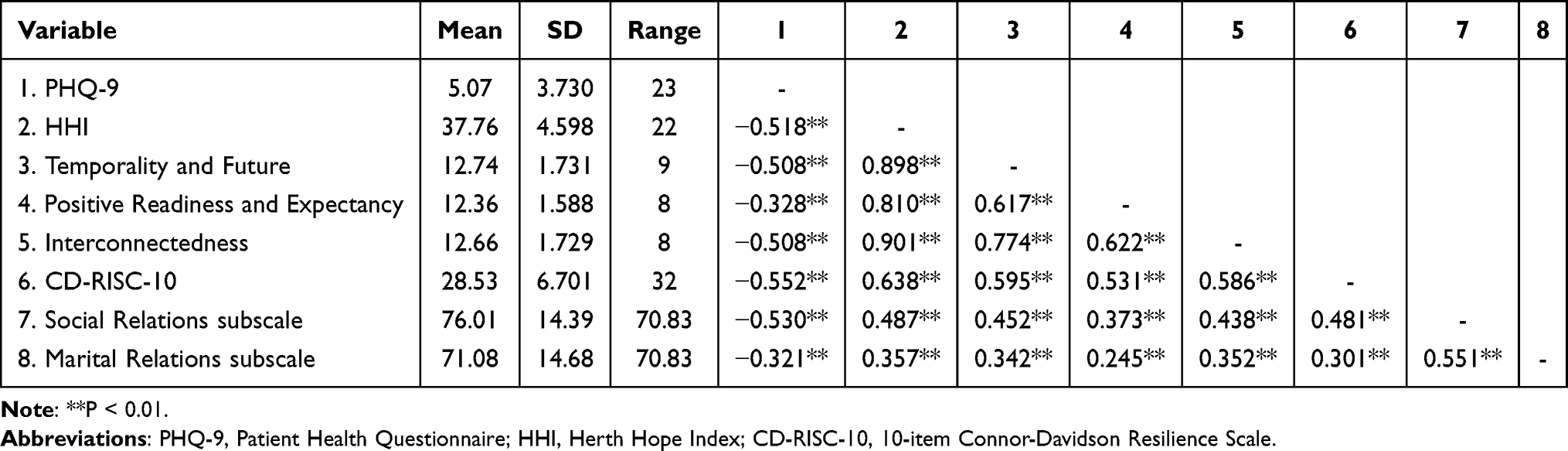 |
Table 2 Descriptive Statistics and Bivariate Correlation Across the Primary Study Variables (N = 315) |
Correlation analyses showed that depressive symptoms was negatively correlated with resilience (r= - 0.552, P < 0.01), social relations (r= - 0.530, P < 0.01), marital relations (r= -0.321, P < 0.01) and hope (r= -0.518, P < 0.01), as well as its dimensions, including temporality and future (r = -0.508, P < 0.01), positive readiness and expectancy (r = -0.328, P < 0.01), and interconnectedness (r= -0.508, P < 0.01). Additionally, resilience was positively correlated with hope (r = 0.638, P < 0.01), social relations (r = 0.481, P < 0.01) and marital relations (r = 0.301, P < 0.01). According to the effect size criteria proposed by Cohen (1992) for correlation coefficients (ρ = 0.1 for small, ρ = 0.3 for medium, and ρ = 0.5 for large effect),48 the smallest correlation coefficient was 0.301 in this study, indicating a medium effect size. And the effect sizes for the majority of the remaining correlation coefficients surpassed the threshold for a large effect size.
Among participants with different household income levels, significant differences were observed in depressive symptoms, resilience, hope, social relations, and marital relations (P < 0.001) (Table 3). Post-hoc pairwise comparisons further revealed that individuals with lower household income exhibited higher levels of depressive symptoms and lower scores in hope, resilience, social relations, and marital relations. Compared to those with medical insurance coverage, self-paying patients reported more severe depressive symptoms and lower levels of hope (P < 0.05) (Table 3). In addition, women with an infertility duration exceeding three years, and those aged under 35 years also reported higher levels of depressive symptoms (P < 0.05) (Appendix 2).
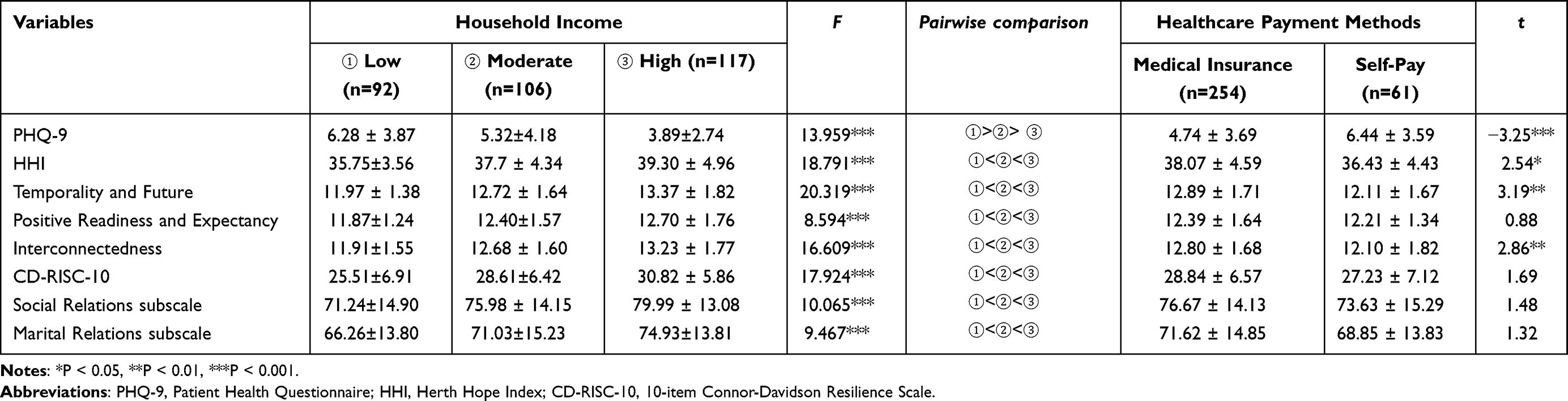 |
Table 3 Group Differences in Primary Variables by Household Income Levels and Healthcare Payment Methods (N = 315) |
OLS Regression Analysis
The OLS regression results show that the R² values for Model 1 and 2 are below 0.2, whereas the value increases to 0.445 in Model 3, which indicates that psychosocial factors substantially enhance model’ s explanatory power for depressive symptoms among women failed IVF-ET cycles in China. In Model 2, both household income and healthcare payment methods show significant association with depressive symptoms (β = -0.20, P < 0.01; β = 0.16, P < 0.01), while age and infertility duration were also significantly related (β= -0.17, P < 0.01; β= 0.21, P < 0.001). In Model 3, hope, resilience, and social relations are all significantly and negatively associated with depressive symptoms (β = -0.18, P < 0.05; β = -0.25, P < 0.001; β = -0.31, P < 0.001). Notably, marital relations does not exhibit statistical significance (β = 0.01, P > 0.05). Detailed results are presented in Table 4.
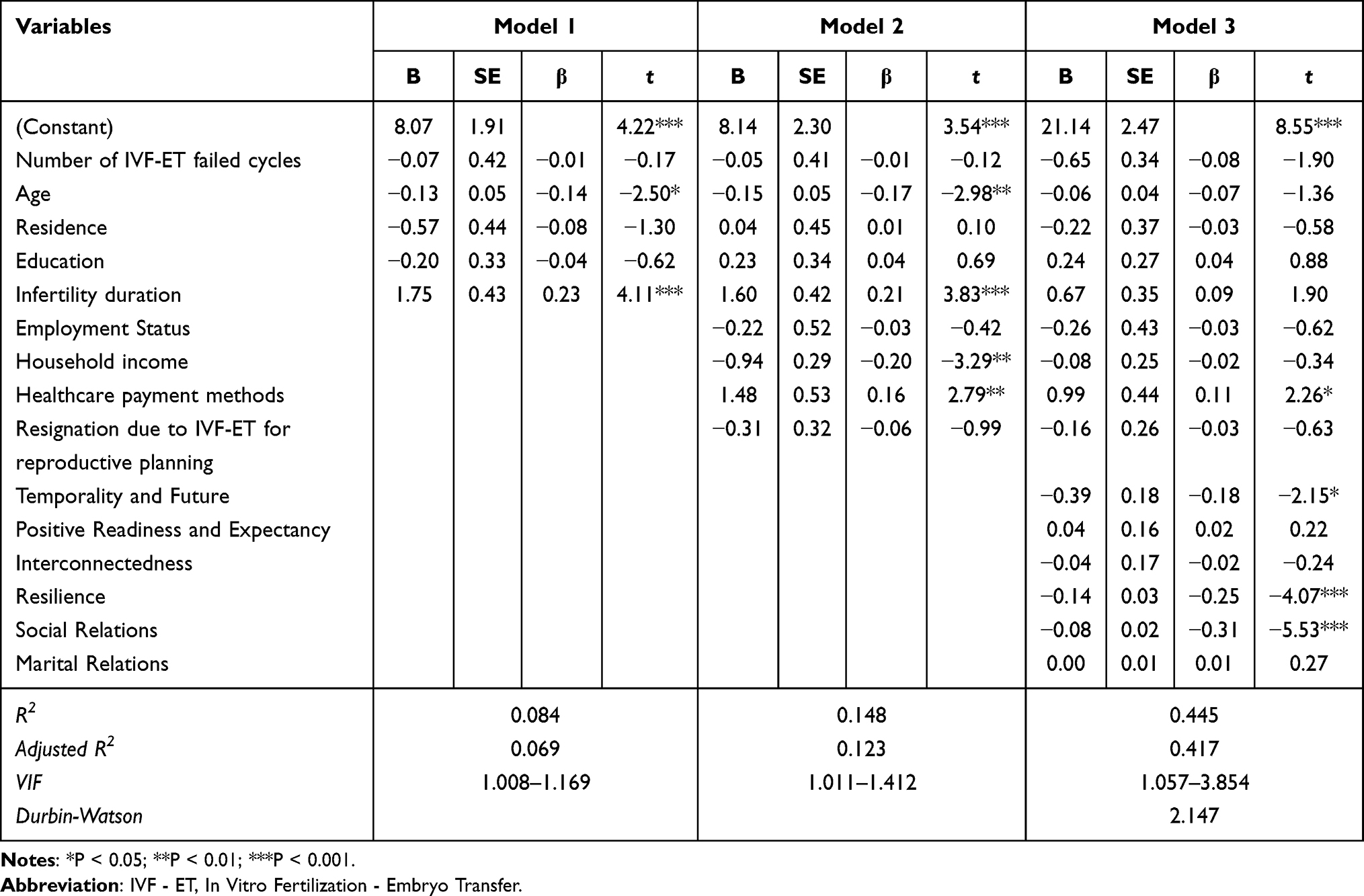 |
Table 4 OLS Regression Estimates of Depressive Symptoms Among Women Failed IVF-ET Cycles by Socioeconomic and Psychosocial Variables |
Moderated Mediation Analysis
Based on the results of the OLS regression analysis, a moderated mediation analysis was conducted to further explore the underlying mechanisms of depressive symptoms. In this analysis, resilience, depressive symptoms, hope (specifically the Temporality and Future dimension), social relations, and household income served as the predictor, dependent variable, mediator, and moderator, respectively. The infertility duration and age were controlled as covariates. The moderated mediation model demonstrated an acceptable fit (χ2 (5) = 21.955, P <0.01; CFI=0.961; SRMR=0.030). The results of the moderated mediation analysis are presented in Figure 2, corresponding to Table 5. Resilience showed a significant negative association with depressive symptoms (β = -0.147, P < 0.001, 95% CI = [-0.212, -0.083]). And resilience exerted significant positive effects on hope (β = 0.102, P < 0.001, 95% CI = [0.058, 0.148]) and social relations (β = 1.096, P < 0.001, 95% CI = [0.698, 1.469]). Both indirect effects through hope and social relations were statistically significant (β = -0.149, P < 0.01, 95% CI = [-0.254, -0.058]; β = -0.132, P < 0.001, 95% CI = [-0.195, -0.077]). The total effect of resilience on symptoms of depression was -0.427 (P < 0.001). The direct effect and the indirect effects accounted for 34.43% and 65.57% of the total effect, respectively. Moreover, the interaction between household income and resilience emerged as a significant positive predictor of hope (β = 0.141, P < 0.05, 95% CI = [0.035, 0.247]). Specifically, the moderating effect was significant in the high household income group (β = 0.083, P < 0.05, 95% CI = [0.021, 0.143]). However, household income did not exhibit a significant moderating effect on the association between resilience and social relations (β = -0.498, P > 0.05, 95% CI = [-1.422, 0.414]).
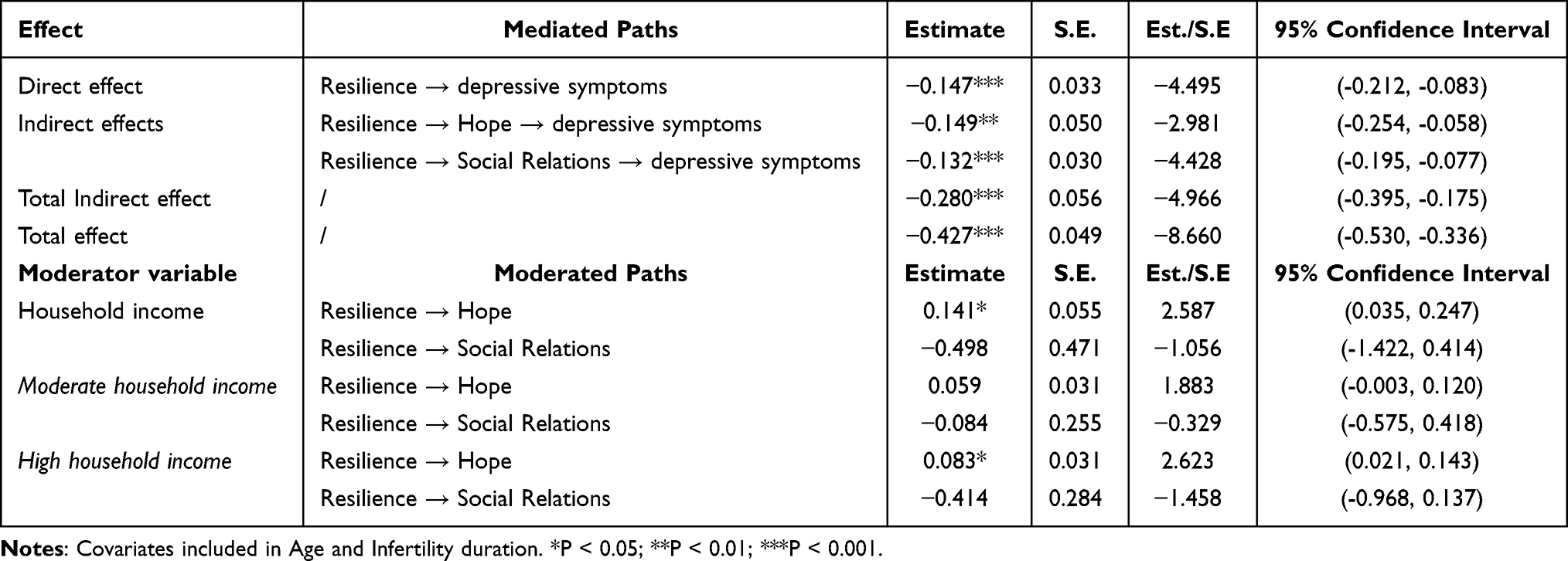 |
Table 5 Moderated Mediation Analyses with Household Income as a Moderator |
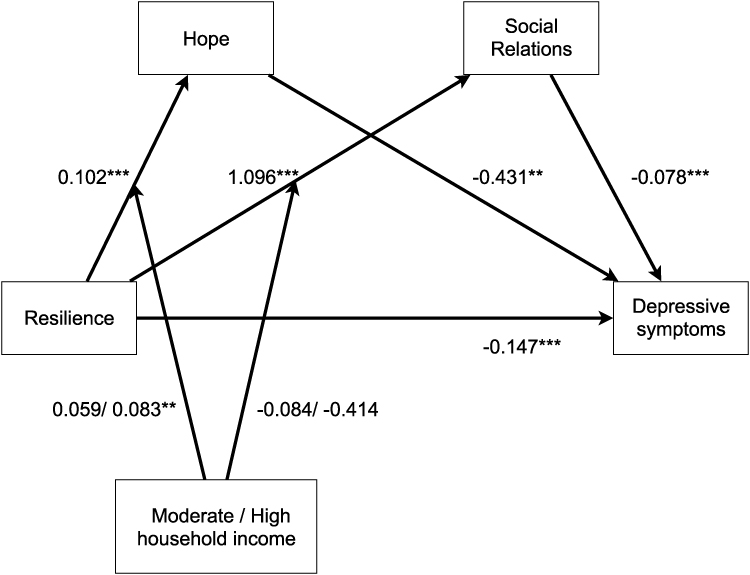 |
Figure 2 Moderated mediation model with household income as a moderator. **P < 0.01; ***P < 0.001. |
When healthcare payment methods were considered as a moderator, the results remained similar to the previous analysis, with detailed findings provided in Appendix 3 and Appendix 4. The moderated mediation model demonstrated acceptable fit (χ2 (5) =21.180, P <0.01; CFI=0.958; SRMR=0.041). The indirect effects through hope and social relations were statistically significant (β = -0.070, P < 0.01, 95% CI = [-0.118, -0.027]; β = -0.071, P < 0.001, 95% CI = [-0.105, -0.041]), as well as the total mediation effect (β = -0.140, P < 0.001, 95% CI = [-0.196, -0.090]). The direct effect and the indirect effects accounted for 51.22% and 48.78% of the total effect, respectively. Furthermore, the moderating effect of healthcare payment methods on the pathways from resilience to hope and resilience to social relations was not statistically significant (β = 0.033, P > 0.05, 95% CI = [-0.033, 0.102]; β = -0.348, P > 0.05, 95% CI = [-0.816, 0.115]).
Discussion
This study investigated the relationship between resilience and depressive symptoms among Chinese women who have experienced failed IVF-ET cycles, revealing a nuanced interplay of psychological, social, and economic factors. Our principal findings show that while higher resilience is associated with fewer depressive symptoms, this protective effect is largely mediated by hope and social relations. Furthermore, household income moderated the pathway through hope, highlighting the critical role of socioeconomic context.
The present study demonstrates that higher resilience is associated with lower levels of depressive symptoms, which supports our first hypothesis and aligns with previous studies.49–51 A meta-analysis including 28 studies further showed that resilience can reduce depressive symptoms by approximately 40%.52 Based on this evidence, resilience is particularly relevant for women failed IVF-ET cycles, as they are often exposed to pronounced emotional and social stressors.
We found that resilience operates through two distinct pathways: an internal resource (hope) and a crucial external resource (social relations). According to Snyder’s Hope Theory, hope facilitates positive coping strategies through agency and pathways.21 For women failed IVF-ET cycles, hope helps them to maintain a positive outlook and engage in constructive coping strategies, such as adjusting reproductive plans or seeking further medical support, which can buffer against feelings of helplessness after a failed cycle. Notably, our findings suggest that in the Chinese cultural context, social relations play a more significant role than marital relations in mitigating depression. This may be due to the strong emphasis on family lineage and collectivist values,53 where infertility is often viewed as a shared family issue.19,54 The understanding and acceptance from a broader social network—including family and friends—may be more critical in alleviating the social stigma and pressure than spousal support alone.
This study demonstrates that lower household income is associated with increased depressive symptoms and lower resilience, hope, and social relations, which is consistent with previous findings.51,55 Moreover, the indirect effect of resilience on depressive symptoms via hope is moderated by household income, with a stronger moderating effect observed in the high-income group. This may be attributed to the fact that higher household income enhances access to treatment and support services, which in turn foster a greater sense of hope for the future and help alleviate depressive symptoms.56 However, household income did not exhibit a statistically significant moderating effect on the indirect pathway from resilience to depressive symptoms via social relations. This may also be explained by the cultural characteristics of collectivism. In China, the practice of “co-residence and common property”, in which different generations live together and share their income, is the primary manifestation of a collectivist culture.57 Regardless of income level, women failed IVF-ET cycles often rely on their family members, or friends for emotional support. Therefore, differences in household income may have limited influence on the association between resilience and social relations.
This study demonstrates that healthcare payment methods significantly influence depressive symptoms and levels of hope among women failed IVF-ET cycles in China. However, this socioeconomic factor did’t show moderating effect on the indirect pathways from resilience to depressive symptoms via hope or social relations. Several factors may account for these discrepancies. First, the self-paying group in this study included only 61 participants, and the relatively small sample size may reduce statistical power, thus limiting the detection of moderating effects. Second, these findings may be attributed to the recent introduction and uneven implementation of ART insurance policies across provinces in China, where each locality formulates its own regulations in the absence of unified national standards. Regional disparities exist in service pricing, reimbursable items, and reimbursement frequency.58,59 The relevant policy was implemented on July 1, 2024, in Jiangsu Province, where the study hospital is located. This policy incorporated limited reimbursable items and capped reimbursement at three cycles.59 Women are still required to cover a portion of treatment costs, and those failed IVF-ET cycles may bear an even greater financial burden. Given the short duration of policy implementation and the restrictions on reimbursement items and frequency, the impact of healthcare payment methods on psychosocial outcomes in this population may be difficult to detect. Future studies should explore the comprehensive implementation of medical insurance policies and the long-term effects of heterogeneous insurance implementation, with particular attention to how differences in service pricing, coverage scope, and reimbursement frequency restrictions shape the psychological well-being of women failed IVF-ET cycles.
Clinical Implication
Living with failed IVF-ET cycles induces complex psychological reactions in infertile women. This study found that resilience exerts significant direct and indirect effects on depressive symptoms, with the indirect effects being mediated by hope and social relations. These findings showed that for women failed IVF-ET cycles in China, interventions should not only foster personal strengths (eg, hope) but also be tailored to the country’s distinctive sociocultural and policy context. In clinical practice, longitudinal follow-up can be employed to dynamically evaluate women’s psychological adaptation trajectories during the progressive refinement of medical insurance policies, which can provide empirical reference to inform the implementation or modification of national health policies. Regarding intervention strategies, approaches such as expressive writing, group support, and mindfulness training may reinforce women’s positive psychological resources and cultivate renewed expectations for the future.60 Furthermore, involving family members and spouses in the intervention process may enhance social support networks and mitigate social pressures and family conflicts associated with infertility. Additionally, it is essential to prioritize the identification of high-risk groups, such as women with low income or an infertility duration of more than three years. Timely screeningfor depressive symptoms, followed by stratified and tailored interventions, should be implemented to achieve precise care and optimize intervention effects.
Limitations and Future Directions
There are several limitations to this study. First, the participants were recruited from a single site. This design was intended to focus on a specific region and minimize the confounding influence of inter-regional heterogeneity. Accordingly, data were collected at the largest reproductive medical center in southern Jiangsu, which offers a representative profile of the local population. Nevertheless, this regional restriction may limit the external validity of the findings. Future studies should increase the sample size, incorporate multiple regions, and account for regional characteristics, such as differences in socioeconomic development and healthcare policy implementation to provide a more comprehensive understanding of the Chinese context and thereby enhance external validity. Second, certain subgroups had relatively small sample sizes, particularly the self-pay group (n = 61), which may have limited statistical power and reduced the generalizability of the results. Third, only a limited set of demographic and clinical variables was collected, which may restrict the ability to comprehensively characterize the sample. Moreover, the CD-RISC-10 does not explicitly capture collectivist values or familial expectations. Although the inclusion of interpersonal relations scales partially addressed this gap, in-depth cultural dimensions remain underexplored. Future studies could employ qualitative approaches to further elucidate the role of cultural factors in the assessment and interpretation of resilience. Finally, the cross-sectional design precludes causal inference, restricting the findings to associative relationships. Future studies should adopt longitudinal designs to investigate the long-term effects of psychosocial factors on depressive symptoms in this specific population while controlling for potential confounders.
Conclusion
The present study demonstrates that resilience has both direct and indirect effects on the depressive symptoms in women failed IVF-ET cycles, with the latter being mediated by hope and social relations. Additionally, the study found that household income moderates the effect of resilience on hope. In light of these findings, clinical healthcare providers can develop intervention strategies targeting the pathways influencing depressive symptoms in women failed IVF-ET cycles in China, thereby promoting reproductive health.
Data Sharing Statement
The data that support the findings of this study are available on request from Xiaoyu Wang or Ling Jiang. The data are not publicly available due to privacy or ethical restrictions.
Ethics Approval Statement
The study was approved by the Ethics Committee of Suzhou Municipal Hospital (K-2024-169-K02) and was conducted in accordance with the principles set forth in the Helsinki Declaration.
Acknowledgments
The authors would like to thank Dr. Mo Zhou for providing expert statistical advice and for reviewing the statistical analyses prior to submission.
Funding
This research was supported by the Connotation Construction Foundation of Preponderant Nursing Discipline in Nanjing Medical University; Nursing Department Cohort Project and Evidence-Based Nursing Practice Project of Suzhou Municipal Hospital [Project Number: SZFCXKHL202402]; the Research Project of Suzhou Gusu Health Talent [Project Number: GSWS2023061]; and the Science and Technology Innovation Development (Soft Science Research) Project funded by the Economic and Technological Bureau and the Finance Bureau of Gusu District, Suzhou.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Salari N, Babajani F, Hosseinian-Far A. et al. Global prevalence of major depressive disorder, generalized anxiety, stress, and depression among infertile women: a systematic review and meta-analysis. Arch Gynecol Obstet. 2024;309(5):1833–1846. doi:10.1007/s00404-024-07444-y
2. American Society for Reproductive Medicine. Male fertility journey; 2023. Available from: https://www.reproductivefacts.org/patient-journeys/male-fertility-journey/.
3. Liu X, Zhong E, Li J, et al. Investigation for anxiety and depression situation in couples receiving in vitro fertilization and embryo transfer (IVF-ET) with donor sperm and associated influencing factors. Neuropsychiatr Dis Treat. 2023;19:1359–1367. doi:10.2147/NDT.S411362
4. Ni Y, Shen H, Yao H, et al. Differences in fertility-related quality of life and emotional status among women undergoing different IVF treatment cycles. Psychol Res Behav Manag. 2023;16:1873–1882. doi:10.2147/PRBM.S411740
5. Verhaak CM, Smeenk JMJ, Van Minnen A, Kremer JAM, Kraaimaat FW. A longitudinal, prospective study on emotional adjustment before, during and after consecutive fertility treatment cycles. Hum Reprod. 2005;20(8):2253–2260. doi:10.1093/humrep/dei015
6. S SM, L BT, C D, F MJ. Resilience and Mental Health: Challenges Across the Lifespan. Cambridge University Press; 2011.
7. Xie Q, Wong DFK. Culturally sensitive conceptualization of resilience: a multidimensional model of Chinese resilience. Transcult Psychiatry. 2021;58(3):323–334. doi:10.1177/1363461520951306
8. González-Navarro P, Talavera-Escribano E, Zurriaga-Lloréns R, Llinares-Insa LI. Culture, work, and subjective well-being: the role of LMX and resilience in Spanish and Chinese cultures. Int J Environ Res Public Health. 2019;16(24):4945. doi:10.3390/ijerph16244945
9. Chen B, Chao G, Qian C, Liu X, Zhang CQ. How can Confucian self-cultivation enhance academic engagement among Chinese college students? Examining the mediating roles of resilience and peace of mind. J Affect Disord. 2025;386:119415. doi:10.1016/j.jad.2025.119415
10. Yu X, Zhang J. Factor analysis and psychometric evaluation of the Connor-Davidson Resilience Scale (CD-RISC) with Chinese people. Soc Behav Personal Int J. 2007;35(1):19–30. doi:10.2224/sbp.2007.35.1.19
11. Wang L, Shi Z, Zhang Y, Zhang Z. Psychometric properties of the 10-item Connor-Davidson Resilience Scale in Chinese earthquake victims. Psychiatry Clin Neurosci. 2010;64(5):499–504. doi:10.1111/j.1440-1819.2010.02130.x
12. Cheng C, Dong D, He J, Zhong X, Yao S. Psychometric properties of the 10-item Connor–Davidson Resilience Scale (CD-RISC-10) in Chinese undergraduates and depressive patients. J Affect Disord. 2020;261:211–220. doi:10.1016/j.jad.2019.10.018
13. Bhamani SS, Zahid N, Zahid W, et al. Association of depression and resilience with fertility quality of life among patients presenting to the infertility centre for treatment in Karachi, Pakistan. BMC Public Health. 2020;20:1607. doi:10.1186/s12889-020-09706-1
14. Fernandez-Ferrera C, Llaneza-Suarez D, Fernandez-Garcia D, Castañon V, Llaneza-Suarez C, Llaneza P. Resilience, perceived stress, and depressed mood in women under in vitro fertilization treatment. Reprod Sci. 2021;29(3):816–822. doi:10.1007/s43032-021-00685-1
15. To QG, Vandelanotte C, Cope K, et al. The association of resilience with depression, anxiety, stress and physical activity during the COVID-19 pandemic. BMC Public Health. 2022;22:491. doi:10.1186/s12889-022-12911-9
16. Husain W, Imran M. Infertility as seen by the infertile couples from a collectivistic culture. J Community Psychol. 2021;49(2):354–360. doi:10.1002/jcop.22463
17. Ha JY, Ban SH. Effect of resilience on infertile couples’ quality of life: an actor–partner interdependence model approach. Health Qual Life Outcomes. 2020;18:295. doi:10.1186/s12955-020-01550-6
18. Kumpfer KL. Factors and processes contributing to resilience. In: Resilience and Development: Positive Life Adaptations. 2002.
19. Hu JY, Wu YD, Xiao Z, et al. A mixed-methods study on negative psychological states of infertile women undergoing assisted reproductive treatment. Sci Rep. 2025;15:20916. doi:10.1038/s41598-025-06397-9
20. Lee J, Kim S, Nam SH. “Living with silence and Shame”: a meta-synthesis of women’s lived experiences of infertility-related stigma. Int J Womens Health. 2025;17:2699–2713. doi:10.2147/IJWH.S539531
21. Snyder CR. Hope theory: rainbows in the mind. Psychol Inq. 2002;13(4):249–275. doi:10.1207/s15327965pli1304_01
22. Chu Y, Zhang Y, Wang S, Dai H. Resilience mediates the influence of hope, optimism, social support, and stress on anxiety severity among Chinese patients with cervical spondylosis. Front Psychiatry. 2022;13:997541. doi:10.3389/fpsyt.2022.997541
23. Long LJ. Hope and PTSD. Curr Opin Psychol. 2022;48:101472. doi:10.1016/j.copsyc.2022.101472
24. Shan Y, Liu X, Chen W, et al. Predictors of psychological resilience trajectories in patients with knee arthroplasty: a longitudinal study. J Adv Nurs. 2023;79(5):1926–1938. doi:10.1111/jan.15421
25. Tang P, Kostyrka-Allchorne K, Butura AM, Phillips-Owen J, Sonuga-Barke E. Reciprocal developmental pathways between future-related thinking and symptoms of adolescent depression and anxiety: a systematic review and meta-analysis of longitudinal studies. Clin Psychol Rev. 2024;112:102465. doi:10.1016/j.cpr.2024.102465
26. Beijing incorporates 16 therapeutic assisted reproductive technologies into medical insurance coverage. Available from: https://ybj.beijing.gov.cn/mtgz/202306/t20230615_3136062.html.
27. Deepening medical insurance reform in the 14th five-year plan period: implications for socioeconomic development. Available from: http://www.nhsa.gov.cn/art/2025/7/24/art_14_17369.html.
28. Kimhi S, Eshel Y, Marciano H, Adini B. Prediction of hope and morale during COVID-19. Front Psychol. 2021;12:739645. doi:10.3389/fpsyg.2021.739645
29. Mikocka-Walus A, Stokes M, Evans S, Olive L, Westrupp E. Finding the power within and without: how can we strengthen resilience against symptoms of stress, anxiety, and depression in Australian parents during the COVID-19 pandemic? J Psychosom Res. 2021;145:110433. doi:10.1016/j.jpsychores.2021.110433
30. Dube L, Nkosi-Mafutha N, Balsom AA, Gordon JL. Infertility-related distress and clinical targets for psychotherapy: a qualitative study. BMJ Open. 2021;11(11):e050373. doi:10.1136/bmjopen-2021-050373
31. Njogu A, Njogu J, Mutisya A, Luo Y. Experiences of infertile women pursuing treatment in Kenya: a qualitative study. BMC Womens Health. 2022;22:364. doi:10.1186/s12905-022-01950-4
32. Lambert, Lambert LS, Lisa S. Beyond significance testing: reforming data analysis methods in behavioral research. Organ Res Methods. 2007;19(4):713–716. doi:10.1177/1094428107307913
33. Riley RD, Ensor J, Snell KIE, et al. Calculating the sample size required for developing a clinical prediction model. BMJ. 2020;368:m441. doi:10.1136/bmj.m441
34. Practice Committee of the American Society for Reproductive Medicine. Electronic address: [email protected]. Definitions of infertility and recurrent pregnancy loss: a committee opinion. Fertil Steril. 2020;113(3):533–535. doi:10.1016/j.fertnstert.2019.11.025
35. Feng Q, Li W, Li W, et al. The presence, clarity, and consistency of definitions in pregnancy outcomes in infertility trials: a systematic review. Hum Reprod. 2025;40(4):654–663. doi:10.1093/humrep/deaf022
36. Zegers-Hochschild F, Adamson GD, de Mouzon J, et al. International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) revised glossary of ART terminology, 2009. Fertil Steril. 2009;92(5):1520–1524. doi:10.1016/j.fertnstert.2009.09.009
37. National Bureau of Statistics of China. 2023 national economy rebounds and high-quality development is steadily advancing;2024. Available from: https://www.stats.gov.cn/sj/xwfbh/fbhwd/202401/t20240117_1946624.html.
38. Campbell-Sills L, Stein MB. Psychometric analysis and refinement of the Connor-davidson Resilience Scale (CD-RISC): validation of a 10-item measure of resilience. J Trauma Stress. 2007;20(6):1019–1028. doi:10.1002/jts.20271
39. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
40. Chan KS, Li HCW, Chan SWC, Lopez V. Herth hope index: psychometric testing of the Chinese version. J Adv Nurs. 2012;68(9):2079–2085. doi:10.1111/j.1365-2648.2011.05887.x
41. Boivin J, Takefman J, Braverman A. The fertility quality of life (FertiQoL) tool: development and general psychometric properties. Hum Reprod Oxf Eng. 2011;26(8):2084–2091. doi:10.1093/humrep/der171
42. Fertility quality of life tool. Cardiff University; 2015. Available from: http://sites.cardiff.ac.uk/fertiqol/background/.
43. Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88(5):879–903. doi:10.1037/0021-9010.88.5.879
44. MacKinnon D. Introduction to Statistical Mediation Analysis. Taylor & Francis Group; 2008.
45. Edwards JR, Lambert LS. Methods for integrating moderation and mediation: a general analytical framework using moderated path analysis. Psychol Methods. 2007;12(1):1–22. doi:10.1037/1082-989X.12.1.1
46. Hayes AF, Preacher KJ. Statistical mediation analysis with a multicategorical independent variable. Br J Math Stat Psychol. 2014;67(3):451–470. doi:10.1111/bmsp.12028
47. Wang J, Wang X. Structural Equation Modeling: Applications Using Mplus. Wiley Series in Probability and Statistics; 2012.
48. Cohen J. A power primer. Psychol Bull. 1992;112(1):155–159. doi:10.1037//0033-2909.112.1.155
49. Khan NH, Shahnawaz MG, Patel A, Kashyap P, Singh CB. Resilience among involuntarily childless couples and individuals undergoing infertility treatment: a systematic review. Hum Fertil Camb Engl. 2023;26(6):1562–1583. doi:10.1080/14647273.2023.2219400
50. Watters ER, Aloe AM, Wojciak AS. Examining the associations between childhood trauma, resilience, and depression: a multivariate meta-analysis. Trauma Violence Abuse. 2023;24(1):231–244. doi:10.1177/15248380211029397
51. Yan Y, Ma Y, Xu L, Lv Y. Impact of perceived social support on anxiety and depression in women undergoing in vitro fertilization-embryo transfer: the role of psychological resilience. J Assist Reprod Genet. 2025;42(1):231–242. doi:10.1007/s10815-024-03308-1
52. Hajure M, Alemu SS, Abdu Z, et al. Resilience and mental health among perinatal women: a systematic review. Front Psychiatry. 2024;15:1373083. doi:10.3389/fpsyt.2024.1373083
53. Liu K, Dou S, Qin W, et al. Association between quality of life and resilience in infertile patients: a systematic review. Front Public Health. 2024;12:1345899. doi:10.3389/fpubh.2024.1345899
54. Du K, Dong Y. The dyadic interaction model of relationship quality and the impact of attachment orientation and empathy on infertile couples in China. Nurs Open. 2021;8(5):2664–2672. doi:10.1002/nop2.819
55. Jaffe J, Diamond MO. Reproductive Trauma: Psychotherapy with Infertility and Pregnancy Loss Clients. American Psychological Association; 2011.
56. Farley Ordovensky Staniec J, Webb NJ. Utilization of infertility services: how much does money matter? Health Serv Res. 2007;42(3 Pt 1):971–989. doi:10.1111/j.1475-6773.2006.00640.x
57. Gong W, Zhu M, Gürel B, Xie T. The lineage theory of the regional variation of individualism/collectivism in China. Front Psychol. 2021;11:596762. doi:10.3389/fpsyg.2020.596762
58. Fujian Province incorporates assisted reproduction into the health insurance coverage. Available from: http://www.nhsa.gov.cn/art/2024/7/31/art_14_13411.html.
59. Jiangsu Provincial People’s Government. Inclusion of assisted reproductive services in Jiangsu’s Medical Insurance System. 2024. Available from: http://www.jiangsu.gov.cn/art/2024/9/4/art_60085_11343524.html.
60. Pennebaker JW. Cognitive, emotional, and language processes in disclosure. Cognition Emotion. 2010;10(6):601–626.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.