Back to Archived Journals » Open Access Surgery » Volume 8
How many meals should you skip before undergoing a colonoscopy? A randomized controlled trial: association between duration of abstinence from solid food to cleanliness of the bowel in patients undergoing elective colonoscopy
Authors Abdul Aziz DA ![]() , Peow LH, Zakaria J, Mohd Nor M, Abdul Latiff Z
, Peow LH, Zakaria J, Mohd Nor M, Abdul Latiff Z
Received 26 September 2014
Accepted for publication 3 December 2014
Published 29 January 2015 Volume 2015:8 Pages 9—20
DOI https://doi.org/10.2147/OAS.S74996
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Cataldo Doria
Dayang A Abdul Aziz,1 Loh H Peow,2 Jasiah Zakaria,2 Mahmud M Nor,3 Zarina A Latiff4
1Pediatric Surgery Unit, Department of Surgery, UKM Medical Center, Kuala Lumpur, Malaysia; 2Department of Surgery, Hospital Tuanku Jaafar, Seremban, Malaysia; 3Department of Surgery, Universiti Sains Islam, 4Department of Pediatrics, UKM Medical Center, Kuala Lumpur, Malaysia
Purpose: An ideal cleansing regime to prepare a clean colon is important for yielding best results during colonoscopy. Many centers practice strict dietary modifications – ie, skipping more than one solid meal 1 or 2 days before the procedure with the consumption of a bowel cleansing agent. No formal studies have been performed to determine how long a patient should withhold solid meals during bowel preparation prior to an outpatient colonoscopy.
Materials and methods: A randomized prospective controlled trial was carried out with patients who underwent elective colonoscopy at a tertiary general hospital in Malaysia for 7 months’ duration. Patients were randomized into one of two groups. Group A patients abstained from a solid diet for 24 hours (the last solid meal was breakfast the day before the colonoscopy). Group B patients abstained from a solid diet 14 hours prior to the colonoscopy (the last solid meal was dinner the day before the colonoscopy). We standardized the time for the oral intake of sodium phosphosoda in both groups. The Boston Bowel Preparation Scale was used to grade the cleanliness between the two groups and a score ≥2 was taken as clean bowel preparation.
Results: A total of 178 patients (each arm had 89 patients) were recruited for this study. Group A showed a mean bowel cleanliness score of 3. Group B showed a mean bowel cleanliness score of 2.5. However, there was a significant difference in bowel cleanliness between the groups (P≤0.05).
Conclusion: Abstinence of solid food for either 24 hours or 14 hours prior to the colonoscopy both produced clean bowel preparation scores. Patients who can afford to skip more meals should stop solid food intake at 24 hours prior to colonoscopy. However, for patients who are not able to fast for long, they should be allowed to take solid food up to 14 hours prior to the procedure, thus reducing the need to over-starve them.
Keywords: bowel preparation, solid meals, colonoscopy
Introduction
Colonoscopy was first introduced in 1969.1 As the years passed, many advances have occurred. Colonoscopy is widely accepted and is currently practiced as one of the safest procedures to be carried out as an outpatient.1 Nowadays, elective colonoscopy has become an essential procedure used in the screening of colorectal cancers. In nonemergency cases, it is routinely used for examining patients with a history of chronic per rectal bleeding, or altered bowel habits such as constipation or persistent diarrhea. Preparing a clean colon using a good cleansing regimen is important for yielding the best results during a colonoscopy.2 Lesions can be missed (coupled with a prolonged procedure) as a result of failure to cleanse the bowel adequately.3,4 Ideal bowel preparation needs to meet the following criteria: it should be convenient with simple instructions; it should have a short period of dietary restriction; it should be safe – ie, minimizing the side effects associated with purgatives; and it should offer tolerable taste and volume for patients.5
Currently, there is not a single universal bowel preparation protocol for outpatient colonoscopy. From various guidelines, there have been no formal studies performed to advise how long a patient should withhold solid meals during bowel preparation prior to an outpatient colonoscopy. In pediatric patients, although there is no standard protocol for bowel preparation, patients are usually only started on a liquid diet on the evening prior to the day of the procedure. It is only logical that the more time a patient is allowed to continue his or her normal diet (ie, more time until the introduction of a liquid diet during bowel preparation), the greater the patient’s acceptance and compliance when undergoing bowel preparation. Such a user-friendly approach would be beneficial for elderly patients and those with comorbid illnesses such as diabetes mellitus and hypertension. In most local hospitals, patients are advised to stop consuming solid meals about 24 hours before the day of the colonoscopy. Patients are usually allowed solids at breakfast on the day (24 hours) before colonoscopy. At the tertiary general hospital where this study was carried out, patients who undergo elective colonoscopy abstain from solid food 24 hours prior to the colonoscopy, which means that patients are allowed to take their normal breakfast, and then this is followed by clear fluids from the afternoon the day before the colonoscopy. Patients will be kept totally nil by mouth from 12 am until the colonoscopy is done. This regime has yielded good colon cleanliness at colonoscopy, but this has not been scientifically proven. However, in pediatric patients, a group of clinicians allow patients to consume solids until much later, about dinner time (ranging from 6–8 pm). The average abstinence from solids is 12–14 hours. This regime seems to work even in older pediatric patients (late teens) who are taking a normal adult diet. However, there is no scientific data to prove this either. Therefore, we are extrapolating that if this approach works for older children, it could work for adults as well. An extensive literature review of the pediatric populations did not single out any specific time to abstain from solid food, but almost all of the literature agreed that the later the abstinence to solid food, the better is the patient’s compliance.6–8 The aim of this study was to analyze whether we were able to achieve clean bowel preparation by allowing our patients to take solid foods up until dinner time 1 day before the procedure, which was around 14 hours prior to the colonoscopy, and to compare this with the usual standard that we use, which was abstinence from solid food after breakfast the day prior to the procedure (ie, 24 hours prior to the colonoscopy).
The American Society of Gastroenterology, British Society of Gastroenterology, and Gastroenterological Society of Australia each have general guidelines and recommendations for bowel preparation.9,10 One of the important components in various methods of bowel preparation is the restriction of diet from solids. Some bowel preparations may require 1–3 days of a clear liquid diet in addition to laxative administration. Though this may yield good bowel preparation results, it is time consuming, inconvenient, and may be uncomfortable for the patient.11 Most of the evidence supporting these regimens comes from studies of colon cleansing for radiography.11 A study of inpatients undergoing colonoscopy showed that a clear liquid diet before bowel preparation was the only diet modification that improved the quality of the preparation.12 Recently, another study showed that strict adherence to a liquid diet 24–48 hours before colonoscopy is one of the reasons why patients have difficulty adhering to current regimens.13 In the American Society of Gastroenterology guidelines, a fluid diet was recommended 3–4 days prior for bowel preparation, whereas in the Gastroenterology Society in Cleveland guidelines, patients are allowed one last meal of solid foods up until 24 hours prior to the colonoscopy.14 The latest 2011 guidelines from the National Health Services in the United Kingdom, which is used by University College London Hospital, recommends that patients should take a liquid diet 2 days prior to the colonoscopy.15
Materials and methods
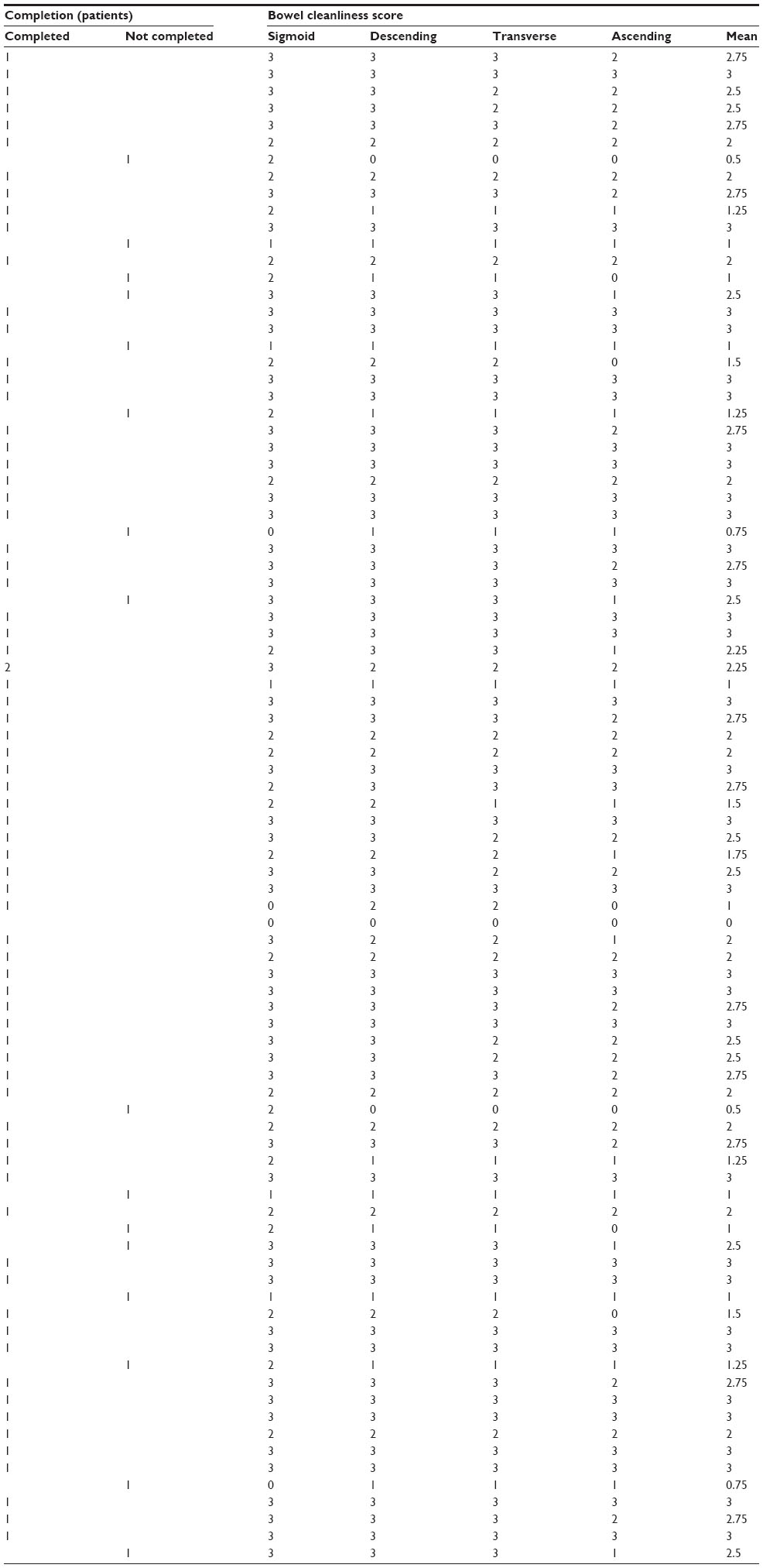
The primary objective of this study was to compare the outcome of bowel cleanliness with regards to the duration of abstinence from solid foods at 24 hours compared to 14 hours for patients undergoing elective colonoscopy. The oral purgative usage was standardized for both groups of patients. We also assessed the colonoscopy completion rate between the two groups. Patients undergoing elective outpatient colonoscopy were prospectively randomized manually into one of two groups (Figure 1). All patients were screened for the inclusion or exclusion criteria before being recruited into the study. The inclusion criteria for this study included all elective patients subjected to bowel preparation as outpatients, patients aged 15–65 years, patients who were able to follow instructions, and those who had consent provided by either the parents or caretaker for the 15–18-year-old patients and patients with American Society of Anesthesiology I, II, or III. The exclusion criteria were patients who presented with intestinal obstruction, clinically ill patients, patients who were not able to follow instructions, patients with a colostomy or those who had a history of large bowel resection, patients with constipation, patients who had renal failure, or any patients who were not willing to take oral sodium phosphosoda for bowel preparation. Randomization was done by instructing the patient to pick up an envelope from a group of preshuffled envelopes in a box, which decided which group the patient would be in (either group A or group B). Patients in group A (24 hours) were instructed to have their last solid meal at 8 am, 1 day prior to the colonoscopy, followed by selected nourishing fluids. Group B patients (14 hours) were instructed to have their last solid meal at 6 pm, 1 day prior to the colonoscopy, followed by selected nourishing fluids. Both groups of patients were required to drink 45 mL of oral sodium phosphosoda at 10 pm 1 day prior to and at 6 am on the day of the colonoscopy. Patients were advised to take a lot of clear fluids (minimum of 2,000 mL) after drinking oral sodium phosphosoda. All patients were kept nil by mouth from 12 am on the day of the procedure to prevent aspiration in case sedation was required during the colonoscopy. Patients would come at the instructed time, and the colonoscopists were blinded to which group the patients belonged to; they would then perform the colonoscopy, assessing the cleanliness of the patient’s bowel using the visual scale of the Boston Bowel Preparation Scale (BBPS) (Figure 2). Before proceeding with the colonoscopy, patients were asked by the attending nurse if they had complied with the bowel preparation given to them. The cleanliness of the bowel was then documented on a premade sheet, according to each segment of the colon (ie, sigmoid, descending colon, transverse colon, and ascending colon) (Table 1). The mean cleanliness score of the bowel for each patient was then calculated.
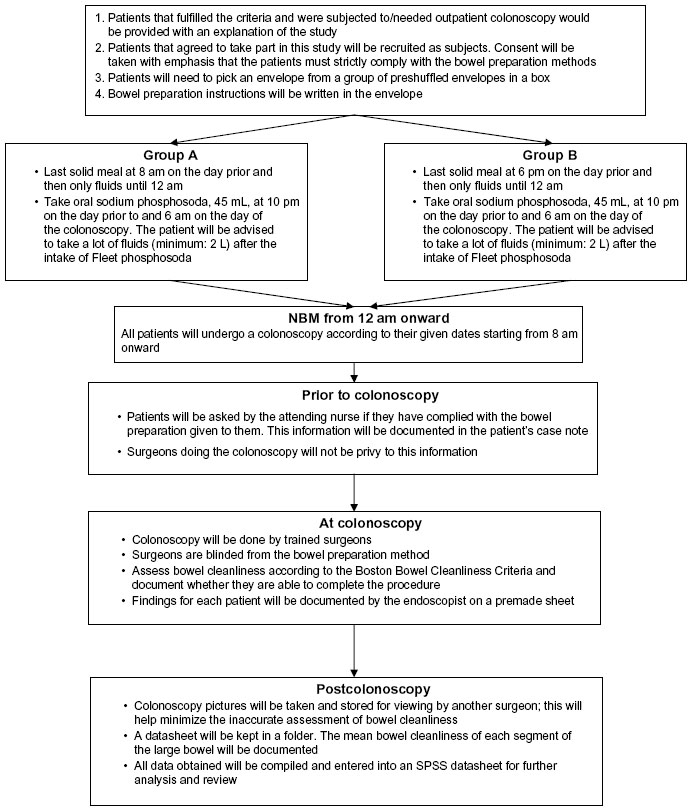 | Figure 1 Flow chart of randomization. |
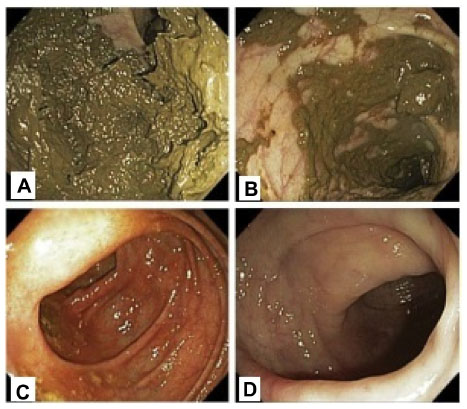 | Figure 2 The Bowel Cleanliness Score according to visual scale of Boston Bowel Preparation Scale. |
 | Table 1 Colonoscopist bowel cleanliness scoring sheet |
In order to compare the cleanliness of various bowel preparations, various scales have been used throughout the years, which include the Ottawa Scale and Aronchick Scales.16 However, Boston University has created and validated the BBPS in 2009.17 Currently, this scale is used as a valid and reliable instrument for colonoscopy-orientated research; it also takes into account the use of oral purgatives, as well as any attempts at washing and suction of the bowel by the endoscopist. This means that we would be able to standardize and compare any improvements and changes in any type of bowel preparation methods. Although the original BBPS from 2009 did not specify which score (0–3) would be considered as a clean bowel, a group of researchers from Spain recently reported successful improvisation of grading of the BBPS, in which a score ≥2 was considered to be indicative of a clean bowel.18 Our study also used the same scoring method.
The sample size was calculated based on prior data which indicated that the failure rate among controls was 0.1 and that the true failure rate for experimental subjects was 0.003;7,19 we would thus need to study 74 experimental subjects and 74 control subjects to be able to reject the null hypothesis that the failure rates for experimental and control subjects were equal with a probability (power) of 0.8. The type I error probability associated with this test for the null hypothesis was 0.05. We then used an uncorrected chi-squared statistic to evaluate the null hypothesis. A 20% dropout rate was incorporated; hence, the total sample size was 178 samples – ie, 89 samples in each arm.
This research was approved by the UKM Medical Center Medical Research and Ethics Committee (approval code: FF-041-2013) and all patients gave their written consent before recruitment and randomization in this study. Data regarding each patient’s demographics, indication for colonoscopy, bowel cleanliness mean score, and completion of colonoscopy were prospectively documented on a datasheet that was later transferred into the SPSS datasheet.
The main outcome was the mean score of bowel cleanliness for the patients in each group. A mean score ≥ 2 was taken as a clean bowel.16 The secondary outcome of this study was the successful completion of the colonoscopy. Completion of the colonoscopy was defined as the visualization of the appendiceal orifice and ileocecal valve, or if the terminal ileum was intubated. Statistical analysis was performed using the Mann–Whitney U test. The completed colonoscopy was compared using the chi-square test. A probability value <0.05 was considered significant (P≤0.05).
We were able to reduce the bias between operators during this study. Colored pictorial images of the BBPS were printed and placed on the colonoscopy monitor for reference by the colonoscopist. The colonoscopist was also briefed regarding the scoring method prior to starting the procedure. Each procedure had pictures taken and stored for viewing by another colonoscopist. This minimized operator bias to bowel cleanliness, and assisted at arriving to a better mean score of the BBPS.
In order to achieve a good outcome in this study, a house officer would call each patient 3 days prior to the procedure day to remind each patient to follow the instructions of the chosen bowel methods properly. Several studies have shown that if only written instructions were given to a patient, he or she would improperly follow the bowel preparation method.20,21
Results
A total of 178 patients were recruited in the 7-month study. None of the patients withdrew their consent during the study. Eighty-nine patients were recruited in group A and group B, separately. Most of the patients that underwent elective colonoscopy were middle-aged, ranging from 41–60 years old. The average age of the patients was 55 years old. The majority of patients were female (52.8%). Among the ethnicity groups, 54 patients were Malays, 72 patients were Chinese, and 49 patients were Indian. Three patients were foreigners from Myanmar and Bangladesh (Table 2). With regards to indications for colonoscopy, 57 patients underwent colonoscopy for per rectal bleeding, 90 patients had altered bowel habits, 13 patients underwent colonoscopy for screening in view of high-risk familial colorectal malignancy, two patients underwent the procedure for suspected recurrent colonic polyps, and 16 patients underwent the procedure for abdominal pain or distension (Figure 3).
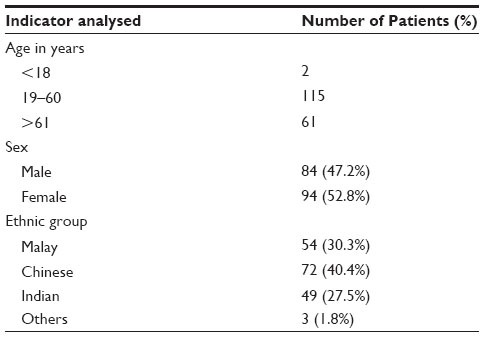 | Table 2 Demographic analysis of the 178 patients |
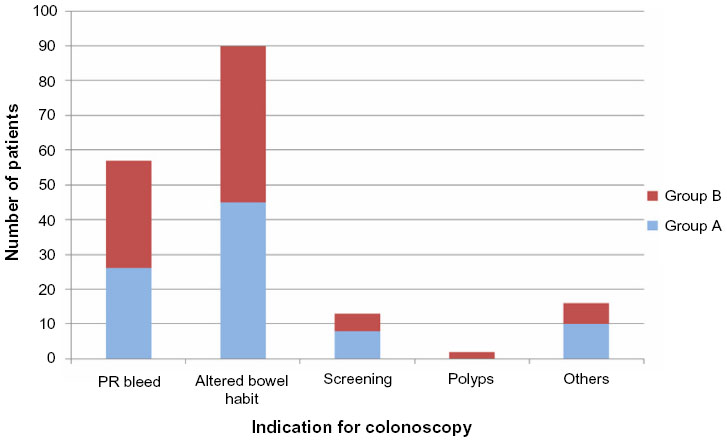 | Figure 3 Indication for colonoscopy for 178 patients (group A and group B). |
A total of 153 patients successfully completed the colonoscopy procedure; the overall completion rate was 86.5%. Out of the 24 patients for whom the colonoscopy was not completed, eight patients were from group A and 16 patients were from group B. These patients were not recruited again as a study subject, but they were rescheduled for another colonoscopy date (Figure 3).
The normality of data was analyzed using the Kolmogorov–Smirnov test, which showed that normality was not assumed. Thus, both groups of data were compared using the Mann–Whitney U test. The bowel cleanliness rating of the patients who did not complete the colonoscopy were included in the bowel cleanliness average. The mean bowel cleanliness score for patients in group A was 3.0. The mean bowel cleanliness score for patients in group B was 2.5. Although both groups yielded a score of >2 (ie, clean), the P-value was 0.006, hence there was a significant difference between the bowel cleanliness score of the two groups (ie, P-value ≤0.05) (Table 3). In group A, ten patients had a mean bowel cleanliness score of <2, but only six of them did not complete the procedure (ie, it was likely that 6.7% of patients in group A failed to complete the colonoscopy secondary to an unclean bowel). In group B, 21 patients had a mean bowel cleanliness score of <2, but only 12 of them did not complete the procedure (ie, it was likely that 13.4% of patients in group B did not complete the colonoscopy procedure secondary to an unclean bowel). Ninety-two percent (92%) of patients from group A completed the procedure when compared to 82% of patients from group B (the rate of completion of the colonoscopy between the two groups was compared using the chi-square test; the P-value was 0.052 – ie, there was no significant difference between the two groups; P-value ≥0.05) (Table 4). Details of the bowel cleanliness score for each group are shown in Tables 5 and 6.
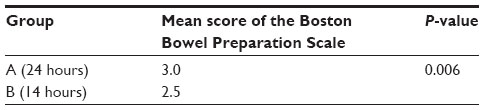 | Table 3 Mann–Whitney U test for comparison of the mean Boston Bowel Preparation Score between group A and group B |
 | Table 4 Outcome of the completion of colonoscopy between group A and group B using the chi-square test |
 | Table 5 Details of the bowel cleanliness score for group A |
 | Table 6 Details of the bowel cleanliness score for group B |
Discussion
Preparing a good clean bowel has always been a challenging task for the colonoscopist. There are a few components in bowel preparation, including the timing of the last solid meal, the bowel purgative medication used, and the patient’s compliance.22,23 Long hours of abstinence from a solid meal is one of the main problems affecting the compliance to bowel preparation.24 This problem is probably more evident among patients in extreme ages and those who suffer from diabetes mellitus and gastritis. A lot of studies have been conducted to analyze the best preparation method for a clean bowel. Abstinence from a solid meal is equally important in bowel preparation. To date, there have been no studies conducted to determine the appropriate duration that patients should withhold from consuming a solid diet. However, a few clinical trials addressing diet in bowel preparation have been carried out. Scott et al randomized 200 patients undergoing colonoscopy with oral sodium phosphate to either light or normal breakfast, which showed no significant differences. Aoun et al25 took this a step further and evaluated the effectiveness of an unrestricted diet on the day before colonoscopy and showed satisfactory results.
Physiologically, the meals taken by a person will reach the terminal ileum within 6 hours.26 It is estimated that on average, the first remnants of the meal travel through the first third of the colon in 6 hours, the second third in 9 hours, and they reach the distal part of the colon (the sigmoid colon) in 12 hours.26 The transport is much slower from the sigmoid colon to the anus.26 If patients have their last solid meals earlier at 8 am, the digested food is expected to reach at least the second-third of the colon before the cleansing of the bowel begins. Theoretically, bowel cleanliness in patients whose last solid meal is at 8 am (24 hours prior) should be better compared to those who had their last solid meal at 6 pm 1 day prior to the colonoscopy. It is postulated if the last solid meal is at 6 pm, 1 day prior to the colonoscopy, the digested food should reach the second-third of the large bowel by 6 am; cleansing the bowel after this should yield acceptable results as well. In our study, the mean BBPS score was 3.0 for patients who abstained from a solid meal for 24 hours. The mean BBPS score was 2.5 for patients who abstained from a solid meal for 14 hours. Although there was a significant difference (P≤0.05), both groups produced acceptable and good bowel preparation, resulting in colonoscopy completion. As there was no statistical significance with respect to the completion rate of the colonoscopy between the two groups, we concluded that shortening the duration of abstaining from a solid diet for up to 14 hours prior to the colonoscopy was feasible to yield an adequately clean colon. This finding is to be taken as evidence to not over-starve patients prior to a colonoscopy. We believe this user-friendly dietary manipulation is beneficial for any patients who are unable to be taken off solid meals for a long period of time despite being allowed to have liquids.
There were two limitations in this study. Firstly, the mean score of cleanliness of the bowel was inevitably low in cases where the colonoscopist was unable to negotiate the colonoscope past a dirty segment of the bowel. For example, when a colonoscopist encountered a dirty sigmoid area, he assumed that the proximal bowel was equally as dirty, and he therefore abandoned the procedure. However, based on physiology, we know that it would have been possible that the proximal bowel could be clean, as all digested food would have traveled distally. Secondly, additional data collection and analysis performed on the patients’ attitudes and levels of satisfaction toward group B preparation should have been done. On a positive note, a number of patients from group B have provided verbal feedback that they were pleased to be able to take their last solid meal at 6 pm, 1 day prior to the colonoscopy, instead of missing solid meals for an extra 10 hours.
Conclusion
Abstinence from solid food at 24 hours prior to colonoscopy was proven to yield significantly good bowel cleanliness during this study; but this meant that patients were not allowed to have two other main meals (ie, lunch and dinner). Abstinence from solid food at 14 hours prior to colonoscopy also resulted in significantly good bowel cleanliness during the procedure, and it led to a good completion rate of 82%. In this group, patients were allowed to have all three main meals a day prior to the colonoscopy (ie, breakfast, lunch and dinner). Abstaining from solid food for either 24 hours or 14 hours prior to colonoscopy had produced clean bowel preparation scores. Perhaps patients who can afford to skip more meals should only need to stop their solid food intake at 24 hours prior to the colonoscopy. However, patients who are not able to tolerate abstinence from solid meals for long periods of time (despite being able to take liquids) should be allowed to take solid food up to 14 hours prior to the procedure, thus reducing the need to over-starve them. We would also like to recommend that any guidelines for bowel preparation that require patients to avoid solid meals for more than 24 hours prior to a colonoscopy be re-examined.
Acknowledgment
The authors would like to thank the UKM Medical Center and the Tuanku Jaafar Hospital Seremban for providing ethics approval and for their support throughout this research.
Disclosure
The authors report no conflicts of interest in this work.
References
Wolff WI. Colonoscopy: history and development. Am J Gastroenterol. 1989;84(9):1017–1025. | |
Cohen SM, Wexner SD, Binderow SR, et al. Prospective, randomized, endoscopic-blinded trial comparing precolonoscopy bowel cleansing methods. Dis Colon Rectum. 1994;37(7):689–696. | |
Burke CA, Church JM. Enhancing the quality of colonoscopy: the importance of bowel purgatives. Gastrointest Endosc. 2007;66(3):565–573. | |
Froehlich F, Wietlisbach V, Gonvers JJ, Burnand B, Vader JP. Impact of colonic cleansing on quality and diagnostic yield of colonoscopy: the European Panel of Appropriateness of Gastrointestinal Endoscopy European multicenter study. Gastrointest Endosc. 2005;61(3):378–384. | |
YI A-Rahim, M Falchuk. Bowel preparation for flexible sigmoidoscopy and colonoscopy. Available from: http://www.uptodate.com/contents/bowel-preparation-for-colonoscopy-and-flexible-sigmoidoscopy-in-adults. Accessed December 2, 2014. | |
Abubakar K, Goggin N, Gormally S, Durnin M, Drumm B. Preparing the bowel for colonoscopy. Arch Dis Child. 1995;73(5):459–461. | |
Barkun A, Chiba N, Enns R, et al. Commonly used preparations for colonoscopy: efficacy, tolerability, and safety – a Canadian Association of Gastroenterology position paper. Can J Gastroenterol. 2006;20(11):699–710. | |
Jimenez-Rivera C, Haas D, Boland M, Barkey JL, Mack DR. Comparison of two common outpatient preparations for colonoscopy in children and youth. Gastroenterol Res Pract. 2009;2009:518932. | |
Hawes RH, Lowry A, Deziel D. A consensus document on bowel preparation before colonoscopy: Prepared by a task force from the ASCRS, ASGE and SAGES. 2006. Gastrointest Endosc. 63(7):894–910. | |
Connor A, Tolan D, Hughes S, Carr N, Tomson C. Consensus guidelines for the safe prescription and administration of oral bowel-cleansing agents. 2012. Available from: http://www.bsg.org.uk/clinical-guidelines/endoscopy/prescription-and-administration-of-oral-bowel-cleansing-agents.html. Accessed December 2, 2014. | |
Abuksis G, Mor M, Segal N, et al. A patient education program is cost-effective for preventing failure of endoscopic procedures in a gastroenterology department. Am J Gastroenterol. 2001;96(6):1786–1790. | |
Reilly T, Walker G. Reasons for poor colonic preparation with inpatients. Gastroenterol Nurs. 2004;27(3):115–117. | |
Scott SR, Raymond PL, Thompson WO, Galt DJ. Efficacy and tolerance of sodium phosphates oral solution after diet liberalization. Gastroenterol Nurs. 2005;28(2):133–139. | |
Atreja A, Nepal S, Lashner BA. Making the most of currently available bowel preparations for colonoscopy. Cleve Clin J Med. 2010;77(5):317–326. | |
University College London Hospitals NHS Foundation Trust. Bowel Preparation. Available from: Guidelines. http://www.uclhwomenscancer.com/useful-downloads.asp. Accessed December 2, 2014. | |
Rostom A, Jolicoeur E. Validation of a new scale for the assessment of bowel preparation quality. Gastrointest Endosc. 2004;59(4):482–486. | |
Lai EJ, Calderwood AH, Doros G, Fix OK, Jacobsen BC. The Boston Bowel Preparation Scale: a valid and reliable instrument for colonoscopy-oriented research. Gastrointest Endosc. 2009;69(3):620–625. | |
Ibáñez M, Parra-Blanco A, Zaballa P, et al. Usefulness of an intensive bowel cleansing strategy for repeat colonoscopy after preparation failure. Dis Colon Rectum. 2011;54(12):1578–1584. | |
Chilton AP, O’Sullivan M, Cox MA, Loft DE, Nwokolo CU. A blinded, randomized comparison of a novel, low-dose, triple regimen with fleet phospho-soda: a study of colon cleanliness, speed and success of colonoscopy. Endoscopy. 2000;32(1):37–41. | |
Gagovic V, Rex DK. Gastroenterologists’ patient instructions for oral sodium phosphate solution for colonoscopy preparation: a survey among gastroenterologists in the state of Indiana. J Clin Gastroenterol. 2008;42(10):1070–1073. | |
Chung YW, Han DS, Park KH, et al. Patient factors predictive of inadequate bowel preparation using polyethylene glycol: a prospective study in Korea. J Clin Gastroenterol. 2009;43(5):448–452. | |
Modi C, Depasquale JR, Digiacomo WS, et al. Impact of patient education on quality of bowel preparation in outpatient colonoscopies. Qual Prim Care. 2009;17(6):397–404. | |
Rex DK, Imperiale TF, Latinovich DR, Bratcher LL. Impact of bowel preparation on efficiency and cost of colonoscopy. Am J Gastroenterol. 2002;97(7):1696–1700. | |
McCray S, Balaban DH. The gourmet colon prep. Pract Gastroenterol. 2007;56:41–57. | |
Aoun E, Abdul-Baki H, Azar C, et al. A randomized single-blind trial of split-dose PEG-electrolyte solution without dietary restriction compared with whole dose PEG-electrolyte solution with dietary restriction for colonoscopy preparation. Gastrointest Endosc. 2005;62(2):213–218. | |
Barrett K, Brooks H, Boitano S, Barman S. Gastrointestinal Motility. In:Ganong’s review of medical physiology. New York: Mc Graw-Hill; 2013:476. Available from: https://emergencypedia.files.wordpress.com/2013/04/ganong-pdf.pdf. Accessed December 2, 2014. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.