")
Back to Journals » Patient Preference and Adherence » Volume 17
How is Patient Adherence Possible? A Novel Mechanistic Model of Adherence Based on Humanities
Authors Reach G
Received 29 April 2023
Accepted for publication 19 June 2023
Published 18 July 2023 Volume 2023:17 Pages 1705—1720
DOI https://doi.org/10.2147/PPA.S419277
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Gérard Reach
Education and Health Promotion Laboratory, Sorbonne Paris Nord University, Bobigny, Île-de-France, 93000, France
Correspondence: Gérard Reach, Education and Health Promotion Laboratory, Sorbonne Paris Nord University, Rue Marcel Cachin, Bobigny, Île-de-France, 93000, France, Email [email protected]
Abstract: Patient non-adherence is a major contemporary medical issue because of its consequences in terms of frequency, morbidity and mortality, and health care costs. This article aims to propose a mechanistic model of adherence based on the tenet that non-adherence is the default option, as long-term adherence in chronic diseases requires sustained effort. The real question becomes, how is patient adherence possible? By focusing on adherent patients, the paper explains the mental mechanisms of adherence using concepts largely drawn from humanities, philosophy of mind, and behavioral economics and presents the findings of empirical studies supporting these hypotheses. The analysis first demonstrates the relationship between patient adherence and temporality and the influence of character traits. Further, it points out the importance of habit, which allows adherence to become non-intentional, thereby sparing patients’ cognitive efforts. Finally, it points out the importance of the quality of the interaction between the person with a chronic disease and the health professional. These features explain why adherence is a syndrome (the healthy adherer phenotype), separating people into those who are safe and those who are at risk of non-adherence, non-control of diabetes, and complications. The concepts presented in this article summarize 20 years of personal clinical and philosophical reflection on patient adherence. They are mainly illustrated by examples from diabetes care but can be applied to all chronic diseases. This novel model of adherence has major practical and ethical implications, explaining the importance of patient education and shared medical decision-making in chronic disease management.
Keywords: adherence, intentionality, temporality, character traits, habit, trust
Introduction
Although the phenomenon of patient non-adherence is known since Hippocrates,1 it was in 1979 that this problem entered the medical literature, initially under the term “non-compliance”, defined as the discrepancy between patients’ behavior and medical prescriptions.2 It is a common phenomenon that affects, for example, one-third of people with type 2 diabetes,3 and it can occur at all three stages of treatment realization: initiation, implementation, and persistence.4 This distinction is important because non-adherence is mostly observed in chronic diseases.5 Non-adherence has significant consequences such as adverse effects on treatment effectiveness,6 morbidity and mortality,7,8 and health care costs.8–10 In 2003, the World Health Organization published a report claiming that increasing the effectiveness of interventions to improve adherence would have a greater impact on health than any biomedical advance.5 Many models have been proposed to describe the causes of non-adherence, and they generally involve the nature of the treatment, the characteristics of the patient, the organization of the health care system, and the quality of the therapeutic relationship.5,11,12 Generally, models provide a simplified explanation of a phenomenon, and while most models describe the determinants associated with the phenomenon to be described, they fail to address its underlying mental mechanisms.
Hence, this article aims to adopt a novel approach based on an analysis of these mechanisms made possible by the analytical philosophy of the mind and behavioral economics. This approach is grounded on the tenet that adherence should be considered as the repeated performance of different actions. This idea13 was published in 2008 in this Journal14 and 2015 as a book published in the “Philosophy and Medicine” series of Springer, entitled “The Mental Mechanisms of Patient Adherence to Long Term Therapies, Mind and Care”.15
In this case, it is inappropriate to speak of “adherent behavior”, as this term is too vague and may result in a failure to study the underlying mechanisms. Indeed, a behavior is an observable phenomenon that is statistically associated with different determinants. However, there is no guarantee that these determinants have a causal effect on the behavior. On the contrary, as we will show later, an action can be defined as an event that is caused by a reason. Considering adherence as an action introduces into its analysis a large part of the philosophy of the mind and behavioral economics. Indeed, both disciplines provide powerful tools to analyze the mechanisms of human actions by showing how rationality carries the seeds of irrationality and how human reasoning can be biased by the use of heuristics and by the effect of emotions. Therefore, the method used in the interdisciplinary approach in this article proposes hypotheses based on these two disciplines and tests them through empirical studies, the results of which are reported. By adopting such an approach, we arrive at a surprising conclusion that could represent a new paradigm. Non-adherence may well be the default option, with only some patients managing, with considerable effort, to perform the unnatural action of practicing a treatment over the long term. The real question then becomes, how is patient adherence possible? Answering this typically philosophical question would have considerable heuristic value in defining ways to improve adherence.
This article will consider the following, in the order given: (1) The philosophical concepts of action, intention, volition, sustained effort in a long-term project, resolution, and foresight; (2) the reasons why it is natural not to be adherent in the context of chronic disease management simply because it involves by definition a relationship with temporality; (3) the influence of cognitive biases and emotions in human decisions; (4) the importance of character traits explaining the syndromic nature of adherence and non-adherence; (5) the role of habit, which makes it possible to redefine the place of intentionality in adherence; and (6) the importance of the quality of the interaction between the person with a chronic disease and the health professional. Finally, we will propose a new typology of people with a chronic disease and conclude by showing the practical and ethical implications of such an investigation.
Philosophical Concepts
Action
This discussion begins13 with the recognition that a patient following or not following prescribed treatment is an action. In the case of adherence, the action is, for example, taking medicine, refusing a cigarette, walking briskly for 30 min, undergoing an examination requested by the doctor, or going to a consultation. Similarly, non-adherence, such as not taking a pill, can also be considered an action in some cases,13–15 which explains the concept of intentional non-adherence.16
Figure 1 illustrates a functionalist model of the mental mechanisms that lead to action.15 It is important to consider that this figure, which can be applied to any human action, is relevant to explain both adherence and non-adherence. Generally speaking, to do something, one must have knowledge (ie, know what to do), skills (ie, know how to do it), the desire for something to happen, and the belief acting will fulfill that desire. Human actions are also influenced by other types of mental states, especially emotions (eg, fear). Emotions can be triggered by the occurrence of an event and, in turn, they can lead to a revision of our beliefs and desires, which justifies the arrows of Figure 1: For instance, I am taking a quiet walk in the forest. The event is my observation of the presence of a snake, which triggers my fear, which leads me to revise my beliefs (I thought I was safe in the forest) and desires (I am no more walking quietly; I am running away).17
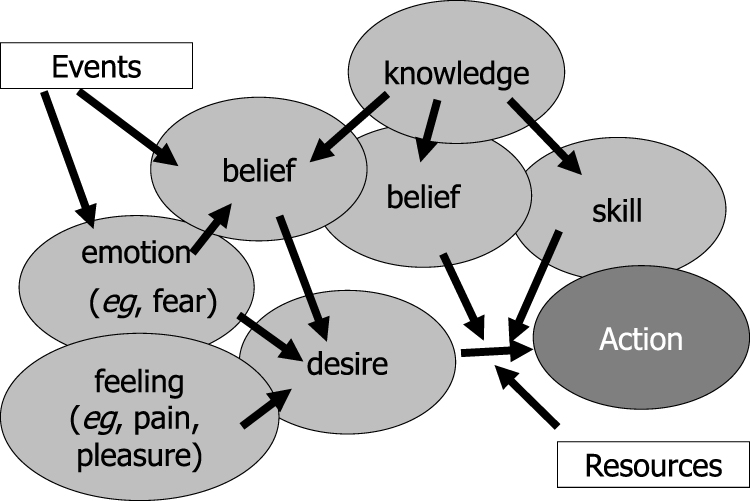 |
Figure 1 Functionalist model explaining the realization of action. Notes: This model can be applied to all our actions, eg, increasing the dose of insulin if blood glucose is high. The desire–belief pair represents the main pro-attitude causing this action, playing an instrumental role; eg, the desire to avoid the recurrence of hyperglycemia and the belief that increasing the insulin dose will satisfy this desire. In addition, the patient must have knowledge (eg, that insulin lowers blood glucose) and skills (knowing how to decide on the insulin dose). Emotions also influence desires, such as fear of weight gain, which may reduce the desire to avoid hyperglycemia. Furthermore, other beliefs may also alter this desire, such as the belief that increasing the insulin dose will result in the risk of hypoglycemia. Thus, beliefs, in addition to the instrumental role that makes them the driver of our actions, can perform another role associated with emotions. These two types of mental states are triggered by events (for example, the recent occurrence of hypoglycemia). In addition, in this figure, we have represented the possible effect of feelings (such as pain and pleasure) and the involvement of exogenous factors as resources necessary for the realization of the action. This “physiology of the mind” is described in detail in the cited reference. Reach G. The Mental Mechanisms of Patient Adherence to Long Term Therapies: Mind and Care, Foreword by Pascal Engel, Philosophy and Medicine Series, Springer, 2015. This figure was adapted from a figure published in The Mental Mechanisms of Patient Adherence to Long-Term Therapies, Mind and Care, by Gérard Reach Springer © 2015, with Springer’s permission for reprint.15 |
Feelings such as pain or pleasure may also be involved. Finally, it is clear that to act, one must have the necessary resources. All these factors describe “the reason” for acting. In a seminal essay entitled “Actions, reasons, and causes”, contemporary philosopher Donald Davidson showed that they not only explain the action but also cause it (Causal Theory of Action).18 An action can thus be seen as an event caused by a reason. Figure 1 points out the direct importance of the desire–belief couple, as already described by David Hume,19 and of emotions. Note that the figure provides a simplified view of an eminently complex process. Certainly, the legend offers a concrete example of how these different mental states are stimulated. However, the simplistic nature of such a representation should not be ignored. For example, the figure does not show second-order desires and beliefs (eg, I desire to desire, I believe that this belief is false) that express the essence of reflexivity.
Intention, Volition, Effort, Resolution, and Habit
Philosopher John Searle helped introduce the notion of intention into the philosophical analysis of action. He noted that an action is preceded by the formation of an “intention in action” specific to that action (eg, the intention to take the pill precedes the action of taking it), which in turn is caused by a “prior intention” (eg, the intention to stay healthy causes the formation of the intention to take the pill).20
Immediately before the action is carried out, there is a mental event, which is the formation of a volition that John Locke had described as that moment when one puts oneself in the posture to act.21 In contemporary times, philosopher Joëlle Proust notes that one is aware of being in a state of volition by the sensation of effort it implies. For a long-term project, such as writing a philosophical treatise, where one cannot do things in one go, this state of volition with the effort it implies must be brought into play each time one has to carry out the successive actions that enable the project’s completion.22 Philosopher Richard Holton has proposed that it is the role of resolutions, which are a special type of intention, to enable one to pursue a project.23 We have proposed that the formation of an intention and a resolution are the two stages of moving into a state of contemplation and maintenance,24 described in the Trans-Theoretical model of Change of Prochaska and DiClemente.25 Another type of solution to avoid giving up on a long-term project and remaining in Prochaska’s maintenance stage could be to establish a habit.24,26 The role of habit has been pointed out by Triandis in his Theory of Interpersonal Behavior.27
Weakness of the Will (Akrasia)
Trope and Liberman’s Construal Level Theory proposes that the mind tends to classify concepts into two types: high-level, which is abstract and future-oriented, and low-level, which is concrete and immediate-based. For example, if we think about reading at a high level, we might consider that it enriches the mind, whereas, at a low level, we might recall the book we are currently reading.28 Long-term treatment adherence might in this context be a high-level, abstract, future-oriented concept, and non-adherence a low-level, concrete, present-oriented concept.24
People often choose the small, immediate reward even if reason says that it would be better to be patient, thus showing irrationality. One instance of irrationality is represented by the phenomenon of the weakness of will, described by Aristotle as akrasia. It was analyzed by Donald Davidson in two famous essays entitled “How is weakness of will possible?” and “Paradoxes of irrationality”, which proposed that weakness of will is due to a failure to apply a principle of rationality, that dictates that when making a choice, one should perform the action, which, all things well considered, should lead to the best outcome.29,30
Foresight, Temporal Horizon, and Willpower
On these philosophical grounds, we have proposed that adherence to long-term treatments may require the application of a principle of foresight that dictates giving priority to the future.14 However, there is a difficulty with this: Shane Frederick asked teenagers and adults aged 20, 30, 40, and 50 to say how similar they would be to their current appearance in 5, 10, 20, 30, and 40 years. He showed that the degree of similarity decreases over time and that this decrease was much more rapid in young people, especially teenagers.31 This suggests that foresight (being able to picture the person one wishes to protect through adherence) may be a difficult task in the long term, especially with diseases such as type 1 diabetes when they occur in adolescents. This difficulty of prioritizing the future was perceived by philosopher Derek Parfit:32
My concern for my future may correspond to the degree of connectedness between me now and myself in the future. Since connectedness is nearly always weaker over longer periods, I can rationally care less about my further future.
The capacity for foresight corresponds to what has been described as the temporal horizon, ie, the window of time that an individual can perceive and plan for. This period is shorter in people with low incomes,33 which may be consistent with the effect of social deprivation on adherence.34 It also corresponds to the concept of consideration of future consequences,35 which has an impact on the achievement of healthy behaviors.36 It may to some extent be innate, that is, genetically determined,37 or influenced by the social context. It may also represent the capacity for delayed gratification that Walter Mischel showed in his marshmallow test in 4-year-old children (managing not to eat a marshmallow for 20 minutes when they have been told that if they succeed they will get two) to be related to the ability to accomplish long-term projects,38 although Mischel’s seminal article describing the delayed gratification test has recently been the subject of controversy.39,40
More generally, the capacity of foresight may represent a component of will-power, a concept described by Holton in an article already cited23 entitled “How is the strength of will possible”, which mirrors Davidson’s article (How is weakness of the will possible).29 Holton defines will-power as a general faculty that enables one ‘to abide by all of one’s resolutions: resolutions not to drink, not to smoke, to eat well, to exercise, to work hard, not to watch daytime television, or whatever.’ Incidentally, people endowed with will-power can therefore be considered adherent concerning all the tasks they must perform,14 which explains why adherence is a syndrome within the healthy adherer concept, as will be explained later. Will-power is considered by some philosophers and psychologists, like Roy Baumeister, as a muscle that can be trained and exhausted. It may therefore not be just a metaphor, and it has even been proposed to be dependent on an energy substrate, glucose.41,42
Foresight versus Impulsivity
Temporal horizon, which focuses on the long term and corresponds to this ability of foresight should not be confused with a concept that focuses on the short term and defines a patient/impatient character, that is, impulsivity. Long-term planning ability and inhibition of impulsivity are part of executive functions. Research on “neuroeconomics”43 has made it possible to locate the brain area of these functions in the prefrontal cortex, which gradually takes control of primitive central limbic structures, the area of impulsivity.44–46 This takeover can be considered both from a phylogenetic (the appearance of the patience function during evolution)47 and ontogenetic (its development during the transition from adolescence to adulthood) point of view.48
As we will see in the next section, impulsive (impatient) people, when faced with an intertemporal choice between a small close reward and a large remote reward, choose the small reward.
Patient Non-Adherence as a Default Option Due to Intertemporal Choice
Hyperbolic Value Discounting and Intertemporal Choice
This section explains why it is natural for patient non-adherence to emerge as the default option in chronic disease treatment. To begin, consider that an item is valued less if it is not received immediately. It has been shown empirically that value discounting is best described by a hyperbolic function, such as V(t) = V(t0)/(1+kt).49 Time discounting can be described by the value of k, which is a coefficient of impatience or impulsiveness and varies between individuals. When one has a strong preference for the present and is faced with an intertemporal choice between a small, close reward and a large, distant reward, the fact that the discounting function is hyperbolic then leads to a preference reversal as one approaches the small reward, whose value appears to increase asymptotically, appearing to exceed that of the distant reward.50,51
Sociologist Jon Elster used this phenomenon to propose an alternative explanation for the weakness of will (akrasia). Contrary to Davidson, he argues that people display apparent irrationality (ie, preferring a near, small reward to a far, large reward) simply because they change their minds because of the preference reversal explained by the hyperbolic nature of time discounting.52
There is now a rich literature showing empirically that present preference is higher in smokers,53 people with alcoholism54 and other addictions,55 people with overweight and obesity,56–58 and in adolescents compared to adults, with patience increasing progressively with age, well beyond the age of 25, which may explain the risk of addiction at that age.59
Adherence as an Intertemporal Choice
Long-term treatment adherence should represent an intertemporal choice since the reward for non-adherence is concrete and received immediately, whereas the reward for adherence (ie, avoiding disease complications) is abstract and distant. However, a first empirical study did not find a relationship between the degree of impulsivity, determined by a fictitious monetary choice, on the one hand, and health behaviors, such as flu vaccination, and adherence to antihypertensive or cholesterol-lowering medication, on the other hand.60 We were the first to show an association between medication adherence, measured with a self-questionnaire, and degree of patience assessed through a simple monetary choice. We asked 90 outpatients with type 2 diabetes treated in a prevention center whether they would choose €500 today, €800 in four months, or €1500 in one year. Of these options, 47, 4, and 39 patients chose €500, €800, and €1500, respectively. Only nine participants were classified as non-adherent to medication based on their responses to the questionnaire. None of them gave the most patient response to the fictitious monetary scenario (P = 0.005), and none had an HbA1c level < 7% (P = 0.011). In addition, multivariate analysis indicated that impatience (not waiting a year) was an independent determinant of having an HbA1c level ≥ 7% (RR = 5.1 (1.7–15.4), P = 0.004).61 These preliminary results were confirmed in other studies we conducted in different settings with people with diabetes or gout.62–66 One of these studies showed that in multivariate analysis, patience with a monetary choice and a long temporal horizon were associated with adherence, and that non-adherence and a short time horizon were associated with a high HbA1c level.65
There is now consistent evidence in the literature for an association between preference for the future and adherence to treatment for various diseases such as prediabetes,67 type 1 diabetes,68 type 2 diabetes and hypertension,69–72 heart failure,73 asthma,74 multiple sclerosis,75 or the initiation of preventive aspirin therapy76 and hormonal therapy in breast cancer.77 Consideration of future consequences moderates the effect of emotions on weight gain.78 Finally, there is emerging evidence that episodic future thinking, ie, thinking about positive future events when faced with an intertemporal choice, reduces delay discounting.79 This may represent an approach to overcome its negative effect on patient adherence. However, the value of delay discounting as a marker has been discussed, due to its lack of specificity and sensitivity.80 This may be due to the complexity of the mechanisms of human behavior, which may temper its effect and which will be considered below.
Effect of Heuristics and Emotions in Human Decisions: Implications for Adherence
Indeed, preference for the present is not the only mental phenomenon that leads to patient non-adherence. The human mind is plagued by cognitive biases that are the result of its use of heuristics, ie, short circuits of thought that allow it to reason quickly and that have been described in the work of Daniel Kahneman and Amos Tversky.81,82 Furthermore, individuals’ decisions are influenced by emotions, both positive and negative (Figure 1). The power of heuristics and emotions in human decisions can be seen in a positive light from an evolutionary perspective, since heuristics allow people to make quick decisions and since emotions have a formative role in our cognition.83 However, they represent a source of bias in our reasoning.
For example, the availability heuristic is used to estimate the frequency of an event by the ease of retrieving its occurrence in our memory. However, we tend to overestimate the frequency of rare events.84 Furthermore, we remember unfortunate events more easily,85 and we hate to lose more than we like to win, a loss aversion described in Kahneman and Tversky’s Prospect Theory.86 These concepts of behavioral economics could influence the occurrence of patient non-adherence, in particular by giving more importance to possible side effects than to the benefits of treatment. They could contribute to the lack of decision or status quo. This tendency to do nothing is observed more often when the decision is difficult, in case of lack of time, when emotions are involved,87 either anticipatory or anticipated. The former are immediate and visceral affects, such as fear, anxiety, or dread, which are felt when one has to perform a risky action. However, anticipated emotions are not felt immediately but are those that one imagines feeling as a consequence of the decision, for example, regret or shame.88
A few years ago, we asked people with type 1 diabetes what insulin dose they would decide to take based on blood glucose readings from their treatment records, and we knew which ones they had taken. We observed that in a theoretical exercise, they were much more likely to increase their insulin dose than they had done in real life.89 We subsequently reinterpreted this observation, which we had simply attributed to fear of hypoglycemia, using the concept of heuristics described above (Figure 2).90
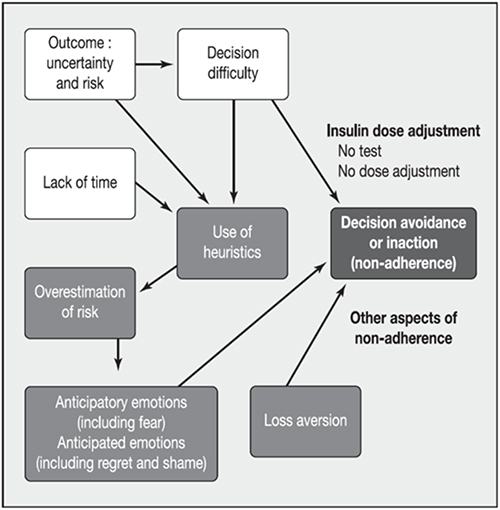 |
Figure 2 Involvement of heuristics and emotions in patient non-adherence. Notes: Explanatory model of the tendency to inaction (lack of adjustment of the insulin dose, and more generally hesitation to initiate treatment): role of uncertainty making the decision difficult and lack of time, leading to the use of heuristics and thus to an overestimation of the risk of unfortunate events, and implication of emotions and aversion to losses. Reprinted from Diabetes Metab, volume 39, Reach G. A psychophysical account of patient non-adherence to medical prescriptions. The case of insulin dose adjustment. 50–55, Copyright (2013), with permission from Société Francophone du Diabète, published by Elsevier Masson SAS. All rights reserved.90 |
Importance of Personality Traits in Adherence, Explaining the Syndromic Nature of Adherence and Non-Adherence
The Healthy Adherer Concept
Next, it is important to note the relevance of personality traits in patient adherence. In all randomized clinical trials, in which data are available for patients in the placebo group, a strange effect is observed: mortality is lower in patients adherent to the placebo compared to their non-adherent counterparts.91 This has led to the healthy adherer concept: patients who are adherent to nothing (a placebo) are adherent to everything, eg, have healthy health behaviors, which explains their lower mortality. In the context of diabetes, this may contribute to the effect of the combination of healthy behaviors on the onset of diabetes and the rate of morbidity and mortality.92
Adherence as a Syndrome
This suggests that adherence is a syndrome. We have shown in a study involving 1875 people with gout that patients who were adherent to uricosuric agents were also adherent to dietary recommendations, were more likely to be non-smokers, and were more likely to measure their blood uric levels than non-adherent patients.66 Similarly, people with osteoporosis who are adherent to bisphosphonates are also more adherent to statins and to undergoing preventive examinations such as colonoscopy and mammography.93 The same holds for patients who are adherent to statins.94 This effect may also explain the association of non-adherence with smoking and excessive alcohol consumption.95,96
Character Traits
This syndromic nature of adherence and non-adherence seems to suggest the intervention of character traits, which, for philosopher Paul Ricœur, represent the set of distinctive marks that allow a human being to be identified as an individual.97 We have already mentioned the effect of a patient or impatient character. Another trait that may be involved in being adherent or non-adherent is obedience. For instance, we have demonstrated in three independent studies of people with diabetes63,64 or gout66 that declaring wearing a seatbelt in the back of a car or being obedient to recommendations in general,98 or more specifically to the doctor’s or pharmacist’s recommendations regarding nutrition,99 is associated with medication adherence. Interestingly, in our study of people with gout,66 we showed a strong statistical association (P < 0.001) between being patient (preferring a distant reward in a fictitious monetary choice) and being obedient (reporting wearing a seatbelt in the back of a car). This may suggest an association between the brain areas or the genomics that support these two traits. Finally, disobedience, which leads to non-adherence, could be an aspect of the psychological concept of reactance, defined as refusing to do something because one is asked to do it, which responds to the feeling that one’s freedom is threatened.100 The link between reactance and adherence to medication has been noted in the literature.101
We have also observed that a chance locus of control and pessimism are significantly associated with medication non-adherence,64 and we also reported an association between non-adherence and depressive tendency, sadness, and pessimism, whereas internal locus of control, cautiousness, and non-risk-taking were associated with adherence.64,99 These observations are consistent with other data in the literature: for example, a systematic review showed that internal locus of control was associated with adherence and that external or chance loci were associated with non-adherence.102 Furthermore, there is a link between personality traits and adherence to treatment and consumption of health services.103 A more specific examination of the personality characteristics of the Big Five personality inventory (agreeableness, conscientiousness, extraversion, neuroticism, and openness) suggested that neuroticism was negatively associated with medication adherence in older people104 and in people with type 2 diabetes,105 whereas agreeableness and conscientiousness were positively related to medication adherence.106 Neuroticism was also found to be negatively associated with lifestyle (exercise and diet) in people with type 2 diabetes,107 while conscientiousness was associated with self-monitoring of blood glucose and medication adherence.108 Similar associations between these personality traits and adherence were found in people with asthma.109 In a 2006 meta-analysis of 33 studies, extraversion (r = 0.23), neuroticism (r = - 0.11), and conscientiousness (r = 0.20) were identified as correlates of physical activity.110 The existence of personality traits reflecting person invariance is not, however, incompatible with the possibility of distinct behaviors when people are confronted with different situations.111
Habit and Intentionality in Patient Adherence
A common observation is that it is easier to do something when you are used to it (eg, combing one’s hair in the morning). We have seen above that any decision preceded by an intention requires a cognitive effort. This is why habit is present in the human mind. According to philosopher Félix Ravaisson in his 1837 thesis, people do not live without habit but instead develop habits, choose them, and structure themselves by them.112 In the case of patient adherence, the important thing could therefore be to start performing the treatment actions, and to do so long enough for a good habit to be formed. Twenty years ago, we proposed that adherence be defined as a “habit of action”.13 One study showed that saying that one takes one’s medication correctly or that one carries out one’s daily exercise is correlated with saying that one does it more or less automatically.113 Stronger habit was found to be associated with better oral contraceptive adherence. Having a fixed time of day to take the pill was associated with habit strength and pill adherence; however, having a fixed place to store the pill was associated with habit strength but not with pill adherence.114 A study showed that unintentional non-adherence, which is often simply forgetfulness, increases during the first six months of treatment, so this period may represent a window for helping the patient to develop “good habits”.115 However, the time taken to achieve automaticity in an action such as eating fruit at lunch was found to be variable. It ranged from 18 to 254 d, with a median value of 66 days.116
We have shown in three independent studies that saying that one generally sticks to one’s habits is associated with medication adherence.64,98,99 Figure 3 shows how the role of habit in adherence can be placed in the framework of the relationship between intentionality and adherence. Just as a distinction is made between unintentional and intentional non-adherence,16 a distinction can be made between intentional adherence, which requires the formation of an intention, and unintentional adherence, which relies on habit.98 The two arrows in the Figure suggest that an episode of unintentional non-adherence may lead to intentional non-adherence,117 if the patient observes the absence of untoward consequences (arrow 1) and that adherence may initially be intentional to give way to unintentional adherence through habit (arrow 2). Moreover, unintentional (habit-related) adherence is characterized by an absence of intention, as if patients no longer needed to think about their treatment: in many conditions, people display an apparent lack of reflection, and it is only later that they offer a rational explanation for what has happened. This can be interpreted in light of Daniel Kahneman’s two systems of thought: system 2 is a reflective system where one thinks whereas system 1 is where heuristics act and is a non-cognitive system with habit acting at this level.82 In this case, we can complete our interpretation of Figure 2 as follows: when one faces difficult decisions where uncertainty and risks abound, and when time is short, heuristics and loss aversion come into play. These are cognitive biases and not cognitive processes (ie, the agent does not decide to use heuristics): in Kahneman’s distinction between system 2, reflexive, and system 1, heuristic driven, only the former involves “thought”.
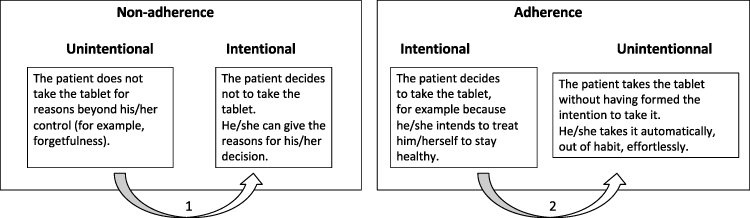 |
Figure 3 Intentionality and adherence. Notes: Both non-adherence and adherence can be intentional or non-intentional. An episode of unintentional non-adherence may lead to intentional non-adherence, if the patient observes the absence of untoward consequences (arrow 1). Adherence may initially be intentional to give way to unintentional adherence through habit (arrow 2). |
Importance of the Quality of the Care Relationship: The Pivotal Role of Trust
Several studies demonstrated the effect of patients’ trust in the doctor on their adherence. Specifically, the percentage of non-adherent patients (low drug purchase) is lower when they say they are involved in the treatment decision and have a trusting relationship with their doctor.118 Another study showed that hypertensive patients are more likely to accept “one more drug” if they trust their doctor.119 It has even been proposed that trust is a “modifiable factor” in non-adherence.120 A recent qualitative study in people with type 2 diabetes showed that gaining patients’ trust, effective patient-provider communication, patient-centered decision-making, and ensuring continuity of care improve both insulin acceptance and adherence.121
We found an association between trust in the physician and adherence in the three studies that looked for it.64,98,99 One of these studies98 showed that feeling involved in decisions, being sufficiently informed about the medication and the disease, and feeling that the doctor understood the patient’s problems and took his/her needs into account was positively associated with trust, and trust was in turn associated with the absence of intentional non-adherence and with the presence of non-intentional adherence by habit; older patients had more trust in the doctor, which is consistent with data in the literature122,123 and may contribute to the positive effect of age on adherence.3
Figure 4 attempts to present the mechanisms that lead to adherence described herein, showing the respective implications of the patient’s character traits, physician’s attitude, and social context. These factors are interrelated. For example, the age of the patient, which is a determinant of adherence in chronic disease,3 being better in older patients, may intervene by decreasing impulsivity, orienting patients toward their future, and increasing trust. As shown in Figure 1, the realization of an action requires the presence of adequate resources, which introduce the importance of the psychosocial context shown in Figure 4 (which has not been developed in this article). In particular, the level of health literacy124 is important and ambiguous; inadequate and adequate literacy was found to be associated with unintentional and intentional non-adherence, respectively.125
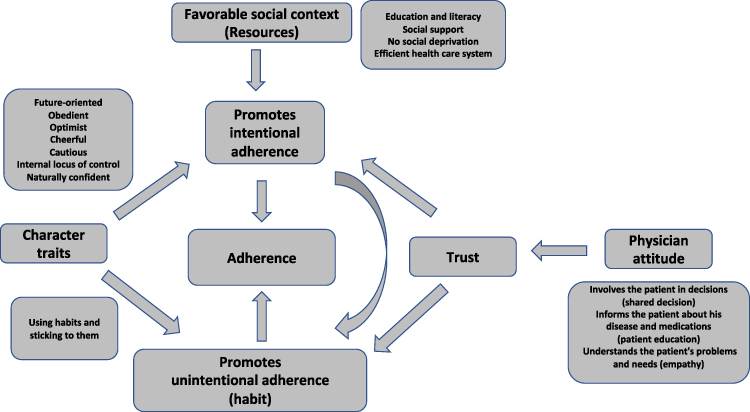 |
Figure 4 Integrated mechanistic model of adherence: how is patient adherence possible?. Notes: The model shows that there are two gateways to adherence: promoting both intentional and unintentional adherence. Trust, generated by a positive physician’s attitude, plays a central role in linking patient and physician-related determinants. The vertical curved arrow linking intentional and unintentional adherence suggests that in the first step, one has to make an effort to be adherent and that this effort can gradually give way to the force of habit. |
Who are the Adherent Patients? A New Safe/Unsafe Typology of People with Chronic Disease
Using Multiple Correspondence Analysis on the data of 600 people with type 2 diabetes, we recently discovered that they could be divided into two groups.99 Those in the first group were in general adherent and never showed intentional non-adherence, they had an HbA1c level in target, had no diabetes complications, considered the burden of diabetes and quality of life tolerable, reported no adverse effects of treatment, were not bothered by hypoglycemia, reported having received sufficient information about the disease and treatment, had a BMI < 30 kg/m2, were not prone to depression, were rather optimistic and naturally cheerful, were obedient, had full trust in the doctor, said that they stick to their habits, were older than 61 years, were often in a high professional category, and did not think that a support program would be useful to them. Patients of the second group were non-adherent and had the opposite characteristics. We proposed to call this new typology “Safe/Unsafe”. “Safe” patients, who were adherent, could be those who benefit from the mechanisms described in Figure 4.
Interestingly, and somewhat tragically, patients in the “unsafe” typological category said that they thought they would change a lot over the next ten years and that preparing for their future was very important. Not surprisingly, they said that a support program would be helpful. However, they were not adherent to taking medication. This suggests that non-adherence may well fall within the philosophical paradox of irrationality mentioned above.29,30
Discussion
First, a warning about the validity of the method used and the conclusions that can be drawn from this analysis: the very fact that this is a narrative review based on the author’s approach described above may have lead to confirmation bias in the selection of the references. This bias is not lost on the author, who welcomes this criticism and asks readers whether they possess data that would allow the conclusions of this article to be refuted in a Popperian sense.
Second, the different philosophical concepts in this article often reflect the same thing, described under different names. For example, we have discussed the different concepts covered by the principle of foresight and the analogy between the involvement of Searle’s intention-in-action and Locke’s volition. Similarly, prior intention may transition to intention-in-action within the framework of Kahneman’s slow system 2 whereas recourse to Holton’s willpower or habit is automatic, unconscious, and may come under fast system 1. Finally, there is an analogy between the two minds, intuitive and narrative, theory, recently being applied to the treatment of type 1 diabetes,126 and Kahneman’s systems 1 and 2.
Third, as shown in Figure 1, human action can be accomplished only if the agent has the necessary resources. This is suggestive of the crucial role of the social environment in patients’ ability to be adherent, which this article has only touched on, for example, by mentioning the effect of social deprivation or health literacy on adherence and which would have required further development. This explains the inclusion of social factors, that is, a favorable social context (resources) that includes education and literacy, social support, the absence of social deprivation, and an efficient health care system, in the model in Figure 4.
Fourth, one’s response to a hypothetical monetary choice may depend on the state of social deprivation, specifically poverty. Our studies have consistently observed an association between social deprivation and an impatient response (€500) to a hypothetical monetary choice, but this link does not imply a causal relation. Interestingly, a recent study showed that people’s perceptions of their income are more strongly associated with their impulsivity determined by a fictitious monetary choice as opposed to their real income.127
Fifth, regarding our observation of insulin dose adjustments, Figure 2 proposes an explanation using heuristics. However, another interpretation is possible: in the real exercise, the patients were in a hot state and acted under the impulse of their Kahneman system 1 whereas in the theoretical exercise, they took time to reflect within the framework of their system 2 thinking.
Finally, the model in Figure 1 represents a functionalist model of action but does not identify where it all happens in the brain. In a famous experiment, Benjamin Libet showed that the mental states described in this figure, which reflect the formation of an intention, occur after changes in brain function have been detected.128 Thus, these mental states may represent nothing but an epiphenomenon. Jaegwon Kim demonstrated that everything happens at the neuronal level and that mental states have no causal effect.129 A full discussion would be outside the scope of this article; indeed we arrive here at a philosophical question, perhaps the most difficult there is: do we have a mind or just a brain?
Conclusion
This article attempts to describe how patient adherence is possible. Given the limits of human rationality, this reflection leads us to propose an important role for the involvement of a principle of foresight that gives priority to the future which, as we have seen, has many representations in philosophical and psychological literature. In a more profound philosophical way, it could be analogous to the Spinozian concept of conatus (everything, in so far as it is in itself, endeavors to persist in its own being)130 and the Freudian concept of eros (this life drive which seeks to force together and hold together the portions of living substance.)131
The conception of adherence presented in this article concerns not only medication taking but also the use of modern tools in type 1 diabetes.132 We suggest that it may be relevant to all chronic diseases. By showing the importance of a doctor’s attitude, involving the patient in the decision, taking an interest in the patient’s problems and needs, and giving information about treatment and diseases, it gives full weight to patient education and the concepts of shared decision-making and patient-centered medicine, the importance of which is recognized in diabetes care133 and should be applied to all chronic diseases.134 In a recent study, we investigated the impact of the importance placed on medication by older adult patients who take between 5 and 10 different medicines (polypharmacy). A high intentional non-adherence score was negatively associated with high medication importance (P = 0.003). In addition, the importance that a patient assigns to medication was positively associated with their habitual treatment taking (P = 0.03). This suggests the need to explain the importance of medicine as an important aspect of patient education.135
There is also an implication for daily practice; by insisting that non-adherence in chronic diseases is the default option, it should encourage caregivers to avoid blaming non-adherent and to praise adherent patients for their efforts; that is, to show empathy and understanding in both cases. Furthermore, considering the patient as a person (incidentally, one no longer says “diabetic patients” but “people with diabetes” in scientific papers) has also an ethical implication,136 the recognition of the patient’s right to autonomy and refusal of treatment, which would be incorrect to describe as non-adherence: by recognizing the existence of intentional non-adherence, they show that the desire to improve adherence is not self-evident and must be critically evaluated for each individual patient.
Finally, for a physician, the act of prescribing treatment also represents an action that has the same mechanisms as those that lead patients to engage in the treatment, described in Figure 1. We proposed that physicians’ clinical inertia137 has the same logical structure as patients’ non-adherence.138 For instance, we suggested that both phenomena be described as clinical myopia due to a preference for the present.139 In this article, we showed that the doctor–patient relationship is key to the issue of adherence. Therefore, we posit that a sane doctor–patient relationship that leads to shared decision-making may also be a way to avoid physicians’ clinical inertia. This final reunion between patients’ non-adherence and physicians’ clinical inertia is not out of place and rather suggests that the caregiver be also considered as a person, that is, a being endowed with imperfect rationality. This extends the concept of patient-centered medicine to a more general person-centered medicine that involves both physician and patient. The considerations developed herein may well lead to a paradigm shift in medicine, to be introduced in medical education.140,141
Disclosure
GR reports personal fees as a speaker at symposia organized by Novo-Nordisk, Lilly, Novartis, Sanofi-Aventis, Merck-Serono, GSK, Ipsen, Abbott-Pharma, BMS, Pfizer, Roche-Pharma, Roche-Diagnostics, Abbott-Diagnostics, Lifescan, Bayer-Diagnostics, Dexcom, BioGen, AbbVie, Servier, Novartis, Takeda, and Mylan-Viatris (lectures on patients’ adherence, doctors’ clinical inertia, patient education, and hospitality in the hospital); and personal fees as a participant in the scientific boards of Lifescan, Bayer Diagnostics, Lilly, Sanofi-Aventis, Novo-Nordisk, Abbott, Takeda, and Timkl.
References
1. Hippocrates. On decorum, 14. Available from: https://archive.org/stream/hippocrates02hippuoft/hippocrates02hippuoft_djvu.txt.
2. Sackett DL, Haynes RB. Compliance with Therapeutic Regimens. Baltimore: Johns Hopkins University Press; 1979:1–7. Available from: http://hdl.handle.net/10822/782244.
3. Briesacher BA, Andrade SE, Fouayzi H, Chan KA. Comparison of drug adherence rates among patients with seven different medical conditions. Pharmacotherapy. 2008;28:437–443. PMID: 18363527. doi:10.1592/phco.28.4.437
4. Vrijens B, De Geest S, Hughes DA, et al. ABC Project Team. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73:691–705. PMID: 22486599. doi:10.1111/j.1365-2125.2012.04167.x
5. World Health Organization report. Adherence to long-term therapies, evidence for action. Geneva: WHO Library Cataloguing-in-Publication Data; 2003:196. Available from: https://apps.who.int/iris/bitstream/handle/10665/42682/9241545992.pdf;jsessionid=D4900D0810E9ABED6D6D296E742B9A27?sequence=1.
6. Farmer AJ, Rodgers LR, Lonergan M, et al. Adherence to oral glucose-lowering therapies and associations with 1-Year HbA1c: a retrospective cohort analysis in a large primary care database. Diabetes Care. 2016;39:258–263. PMID: 26681714. doi:10.2337/dc15-1194
7. Curtis SE, Boye KS, Lage MJ, Garcia-Perez LE. Medication adherence and improved outcomes among patients with type 2 diabetes. Am J Manag Care. 2017;23:e208–e214. PMID: 28850793.
8. Khunti K, Seidu S, Kunutsor S, Davies M. Association between adherence to pharmacotherapy and outcomes in type 2 diabetes: a meta-analysis. Diabetes Care. 2017;40:1588–1596. PMID: 28801474. doi:10.2337/dc16-1925
9. Ho PM, Rumsfeld JS, Masoudi FA, et al. Effect of medication nonadherence on hospitalization and mortality among patients with diabetes mellitus. Arch Intern Med. 2006;166:1836–1841. PMID: 17000939. doi:10.1001/archinte.166.17.1836
10. Mennini FS, Marcellusi A, von der Schulenburg JM, et al. Cost of poor adherence to anti-hypertensive therapy in five European countries. Eur J Health Econ. 2015;16:65–72. PMID: 24390212. doi:10.1007/s10198-013-0554-4
11. Peh KQE, Kwan YH, Goh H, et al. An adaptable framework for factors contributing to medication adherence: results from a systematic review of 102 conceptual frameworks. J Gen Intern Med. 2021;36:2784–2795. PMID: 33660211. doi:10.1007/s11606-021-06648-1
12. Dolgin K. The SPUR Model: a Framework for Considering Patient Behavior. Patient Prefer Adherence. 2020;14:97–105. PMID: 32021121; PMCID: PMC6970605. doi:10.2147/PPA.S237778
13. Reach G. Application de la théorie causale de l'action à l'analyse de l'observance thérapeutique [Application of the causal theory of action to analysis of therapeutic non-adherence]. Presse Med. 2000;29:1939–1946. PMID: 11244626. PMID: 11244626.
14. Reach G. A novel conceptual framework for understanding the mechanism of adherence to long-term therapies. Patient Prefer Adherence. 2008;2:7–19. PMID: 19920939; PMCID: PMC2770416.
15. Reach G. The mental mechanisms of patient adherence to long term therapies. Philosophy Med. 2015. doi:10.1007/978-3-319-12265-6
16. Lehane E, McCarthy G. Intentional and unintentional medication non-adherence: a comprehensive framework for clinical research and practice? A discussion paper. Int J Nurs Stud. 2007;44:1468–1477. PMID: 16973166. doi:10.1016/j.ijnurstu.2006.07.010
17. Livet P. Émotions et rationalité morale, [Emotions and moral rationality] Paris Presses Universitaires de France, coll. Sociologies. 2002;304:23.
18. Davidson D. Actions, reasons and causes. J of Philosophy. 1963;23:655–700. doi:10.2307/2023177
19. Hume D. A treatise of human nature (1739). Norton, Oxford: Oxford University Press; 2000:744. Available from: https://global.oup.com/academic/product/a-treatise-of-human-nature-9780198751724?cc=fr&lang=en&#.
20. Searle J. Intentionality, an essay in the philosophy of mind. New York, New York: Cambridge University Press; 1983:292. Available from: https://www.cambridge.org/fr/academic/subjects/philosophy/philosophy-general-interest/intentionality-essay-philosophy-mind?format=PB.
21. Locke J. An Essay Concerning Human Understanding (1689). Nidditch Oxford: Clarendon Press; 1975:784. Available from: https://www.oxfordscholarlyeditions.com/display/10.1093/actrade/9780198243861.book.1/actrade-9780198243861-book-1.
22. Proust J. La nature de la volonté. Paris: Gallimard; 2005:363.
23. Holton R. How is strength of will possible? In: Stroud S, Tappolet C, editors. Weakness of Will and Practical Irrationality. Oxford: Clarendon Press; 2003:39–67.
24. Reach G. Obstacles to patient education in chronic diseases: a trans-theoretical analysis. Patient Educ Couns. 2009;77:192–196. PMID: 19505787. doi:10.1016/j.pec.2009.05.005
25. Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward an integrative model of change. J Consult Clin Psychol. 1983;51:390–395. PMID: 6863699. doi:10.1037//0022-006x.51.3.390
26. Reach G. Role of habit in adherence to medical treatment. Diabet Med. 2005;22:415–420. PMID: 15787666. doi:10.1111/j.1464-5491.2004.01449.x
27. Triandis HC. Values, Attitudes and Interpersonal Behavior. In: Page MM, editor. Nebraska Symposium on Motivation. University of Nebraska Press; 1979:195–260. PMID: 7242748.
28. Trope Y, Liberman N. Temporal construal. Psychol Rev. 2003;110:403–421. PMID: 12885109. doi:10.1037/0033-295x.110.3.403
29. Davidson D. How Is Weakness of the Will Possible? In: Feinberg J, editor. Moral Concepts. Oxford: Oxford University Press; 1969.
30. Davidson D. Paradoxes of Irrationality. In: Problems of Rationality. Oxford: Oxford University Press; 1982.
31. Frederick S. Time preference and identity. In: Loewenstein G, editor. Time and Decision, Economic and Psychological Perspectives on Intertemporal Choice. Russel Sage Foundation; 2003:89–113.
32. Parfit D. Reasons and Persons. Oxford: Clarendon Press; 1984:313–314. Available from: https://global.oup.com/academic/product/reasons-and-persons-9780198249085?cc=fr&lang=en&.
33. Jones BA, Landes RD, Yi R, Bickel WK. Temporal horizon: modulation by smoking status and gender. Drug Alcohol Depend. 2009;104 Suppl 1:S87–S93. PMID: 19446407. doi:10.1016/j.drugalcdep.2009.04.001
34. Wamala S, Merlo J, Bostrom G, Hogstedt C, Agren G. Socioeconomic disadvantage and primary non-adherence with medication in Sweden. Int J Qual Health Care. 2007;19:134–140. PMID: 17449480. doi:10.1093/intqhc/mzm011
35. Strathman A, Gleicher F, Boninger DS, Edwards CS. The consideration of future consequences: weighing immediate and distant outcomes of behavior. J Pers Soc Psychol. 1994;66:742–752. doi:10.1037/0022-3514.66.4.742
36. Guo M, Lou Y, Zhang N. Consideration of future consequences and self-control mediate the impact of time perspectives on self-rated health and engagement in healthy lifestyles among young adults. Curr Psychol. 2022;1–11. doi:10.1007/s12144-022-03135-6
37. Reach G. Is there an impatience genotype leading to non-adherence to long-term therapies? Diabetologia. 2010;53:1562–1567. PMID: 20407742. doi:10.1007/s00125-010-1755-3
38. Mischel W, Shoda Y, Rodriguez MI. Delay of gratification in children. Science. 1989;244:933–938. PMID: 2658056. doi:10.1126/science.2658056
39. Watts TW, Duncan GJ, Quan H. Revisiting the marshmallow test: a conceptual replication investigating links between early delay of gratification and later outcomes. Psychol Sci. 2018;29(7):1159–1177. PMCID: PMC6050075. doi:10.1177/0956797618761661
40. Doebel S, Michaelson LE, Munakata Y. Good things come to those who wait: delaying gratification likely does matter for later achievement (A Commentary on Watts, Duncan, & Quan, 2018). Psychol Sci. 2020;31(1):97–99. PMCID: 31850827. doi:10.1177/0956797619839045
41. Gailliot MT, Baumeister RF. The physiology of willpower: linking blood glucose to self-control. Pers Soc Psychol Rev. 2007;11:303–327. PMID: 18453466. doi:10.1177/1088868307303030
42. Baumeister RF, Tice DM, Vohs KD. The strength model of self-regulation: conclusions from the second decade of willpower research. Perspect Psychol Sci. 2018;13:141–145. PMID: 29592652. doi:10.1177/1745691617716946
43. Zak PJ, Goodenough OR, Zak PJ. Neuroeconomics. Philos Trans R Soc Lond B Biol Sci. 2004;359:1737–1748. PMID: 15590614. doi:10.1098/rstb.2004.1544
44. Shulman EP, Smith AR, Silva K, et al. The dual systems model: review, reappraisal, and reaffirmation. Dev Cogn Neurosci. 2016;17:103–117. PMID: 26774291. doi:10.1016/j.dcn.2015.12.010
45. Bickel WK, Snider SE, Quisenberry AJ, Stein JS, Hanlon CA. Competing neurobehavioral decision systems theory of cocaine addiction: from mechanisms to therapeutic opportunities. Prog Brain Res. 2016;223:269–293. PMID: 26806781. doi:10.1016/bs.pbr.2015.07.009
46. Friedman NP, Robbins TW. The role of prefrontal cortex in cognitive control and executive function. Neuropsychopharmacology. 2022;47:72–89. PMID: 34408280. doi:10.1038/s41386-021-01132-0
47. Vanderveldt A, Oliveira L, Green L. Delay discounting: pigeon, rat, human--does it matter? J Exp Psychol Anim Learn Cogn. 2016;42:141–162. PMID: 26881899. doi:10.1037/xan0000097
48. Luciana M. Adolescent brain development in normality and psychopathology. Dev Psychopathol. 2013;25:1325–1345. PMID: 24342843. doi:10.1017/S0954579413000643
49. Rachlin H, Raineri A, Cross D. Subjective probability and delay. J Exp Anal Behav. 1991;55:233–244. PMID: 2037827. doi:10.1901/jeab.1991.55-233
50. Ainslie G. Précis of Breakdown of Will. Behav Brain Sci. 2005;28:635–650. PMID: 16262913. doi:10.1017/S0140525X05000117
51. Elster J, Loewenstein G. Choice Over Time. New York: Russell Sage; 1992.
52. Elster J. Davidson on weakness of will and self-deception. In: Edwin HL, editor. The Philosophy of Donald Davidson, the Library of Living Philosophers. Open Court; 1999:425–442.
53. Barlow P, McKee M, Reeves A, Galea G, Stuckler D. Time-discounting and tobacco smoking: a systematic review and network analysis. Int J Epidemiol. 2017;46:860–869. PMID: 27818375. doi:10.1093/ije/dyw233
54. MacKillop J. The behavioral economics and neuroeconomics of alcohol use disorders. Alcohol Clin Exp Res. 2016;40:672–685. PMID: 26993151. doi:10.1111/acer.13004
55. Bickel WK, Johnson MW, Koffarnus MN, MacKillop J, Murphy JG. The behavioral economics of substance use disorders: reinforcement pathologies and their repair. Annu Rev Clin Psychol. 2014;10:641–677. PMID: 24679180. doi:10.1146/annurev-clinpsy-032813-153724
56. Barlow P, Reeves A, McKee M, Galea G, Stuckler D. Unhealthy diets, obesity and time discounting: a systematic literature review and network analysis. Obes Rev. 2016;17:810–819. PMID: 27256685. doi:10.1111/obr.12431
57. Bickel WK, Freitas-Lemos R, Tomlinson DC, et al. Temporal discounting as a candidate behavioral marker of obesity. Neurosci Biobehav Rev. 2021;129:307–329. PMID: 34358579. doi:10.1016/j.neubiorev.2021.07.035
58. Sukumar JS, Vaughn JE, Tegge A, Sardesai S, Lustberg M, Stein J. Delay discounting as a potential therapeutic target for weight loss in breast cancer survivors. Cancers. 2022;14:1134. PMID: 35267441. doi:10.3390/cancers14051134
59. Christakou A, Brammer M, Rubia K. Maturation of limbic corticostriatal activation and connectivity associated with developmental changes in temporal discounting. Neuroimage. 2011;54:1344–1354. PMID: 20816974. doi:10.1016/j.neuroimage.2010.08.067
60. Chapman GB, Brewer NT, Coups EJ, Brownlee S, Leventhal H, Leventhal EA. Value for the future and preventive health behavior. J Exp Psychol Appl. 2001;7:235–250. PMID: 11676102. doi:10.1037/1076-898X.7.3.235
61. Reach G, Michault A, Bihan H, Paulino C, Cohen R, Le Clésiau H. Patients’ impatience is an independent determinant of poor diabetes control. Diabetes Metab. 2011;37:497–504. PMID: 21550831. doi:10.1016/j.diabet.2011.03.004
62. Lebeau G, Consoli SM, Le Bouc R, et al. Delay discounting of gains and losses, glycemic control and therapeutic adherence in type 2 diabetes. Behav Processes. 2016;132:42–48. PMID: 27663668. doi:10.1016/j.beproc.2016.09.006
63. Reach G. Obedience and motivation as mechanisms for adherence to medication: a study in obese type 2 diabetic patients. Patient Prefer Adherence. 2011;5:523–531. PMID: 22114466. doi:10.2147/PPA.S24518
64. Reach G, Pellan M, Crine A, Touboul C, Ciocca A, Djoudi Y. Holistic psychosocial determinants of adherence to medication in people with type 2 diabetes. Diabetes Metab. 2018;44:500–507. PMID: 30031714. doi:10.1016/j.diabet.2018.06.001
65. Reach G, Boubaya M, Brami Y, Lévy V. Disruption in time projection and non-adherence to long-term therapies. Patient Prefer Adherence. 2018;12:2363–2375. PMID: 30519002. doi:10.2147/PPA.S180280
66. Reach G, Chenuc G, Maigret P, Elias-Billon I, Martinez L, Flipo RM. Implication of character traits in adherence to treatment in people with gout: a reason for considering nonadherence as a syndrome. Patient Prefer Adherence. 2019;13:1913–1926. PMID: 31806940. doi:10.2147/PPA.S227329
67. Epstein LH, Paluch RA, Stein JS, et al. Delay discounting, glycemic regulation and health behaviors in adults with prediabetes. Behav Med. 2021;47:194–204. PMID: 32275202. doi:10.1080/08964289.2020.1712581
68. Stoianova M, Tampke EC, Lansing AH, Stanger C. Delay discounting associated with challenges to treatment adherence and glycemic control in young adults with type 1 diabetes. Behav Processes. 2018;157:474–477. PMID: 29958994. doi:10.1016/j.beproc.2018.06.013
69. Karl FM, Holle R, Schwettmann L, Peters A, Laxy M. Time preference, outcome expectancy, and self-management in patients with type 2 diabetes. Patient Prefer Adherence. 2018;12:1937–1945. PMID: 30288034. doi:10.2147/PPA.S175045
70. Sansbury B, Dasgupta A, Guthrie L, Ward M. Time perspective and medication adherence among individuals with hypertension or diabetes mellitus. Patient Educ Couns. 2014;95:104–110. PMID: 24480361. doi:10.1016/j.pec.2013.12.016
71. Campbell JA, Williams JS, Egede LE. Examining the relationship between delay discounting, delay aversion, diabetes self-care behaviors, and diabetes outcomes in U.S. adults with type 2 diabetes. Diabetes Care. 2021;44(4):893–900. PMID: 33568402. doi:10.2337/dc20-2620
72. Krousel-Wood M, Peacock E, Bradford WD, et al. Time preference for immediate gratification: associations with low medication adherence and uncontrolled blood pressure. Am J Hypertens. 2022;35:256–263. PMID: 34788786. doi:10.1093/ajh/hpab175
73. Chew HSJ, Sim KLD, Choi KC, Chair SY. Relationship between self-care adherence, time perspective, readiness to change and executive function in patients with heart failure. J Behav Med. 2020;43:1–11. PMID: 31312975. doi:10.1007/s10865-019-00080-x
74. Brandt S, Dickinson B. Time and risk preferences and the use of asthma controller medication. Pediatrics. 2013;131:e1204–e1210. PMID: 23478866. doi:10.1542/peds.2011-2982
75. Bruce JM, Bruce AS, Lynch S, et al. Probability discounting of treatment decisions in multiple sclerosis: associations with disease knowledge, neuropsychiatric status, and adherence. Psychopharmacology. 2018;235:3303–3313. PMID: 30244284. doi:10.1007/s00213-018-5037-y
76. Zhu J, Shi Y, Li J, Zhang Z. Role of risk attitude and time preference in preventive aspirin use adherence. J Eval Clin Pract. 2020;26:819–825. PMID: 31478307. doi:10.1111/jep.13274
77. Vaughn JE, Ammermann C, Lustberg MB, Bickel WK, Stein JS. Delay discounting and adjuvant endocrine therapy adherence in hormone receptor-positive breast cancer. Health Psychol. 2021;40:398–407. PMID: 34323542. doi:10.1037/hea0001077
78. Bénard M, Bellisle F, Etilé F, et al. Impulsivity and consideration of future consequences as moderators of the association between emotional eating and body weight status. Int J Behav Nutr Phys Act. 2018;15:84. PMID: 30189878. doi:10.1186/s12966-018-0721-1
79. Epstein LH, Paluch RA, Biondolillo MJ, et al. Effects of 6-month episodic future thinking training on delay discounting, weight loss and HbA1c changes in individuals with prediabetes. J Behav Med. 2022;45:227–239. PMID: 35006500. doi:10.1007/s10865-021-00278-y
80. Bailey AJ, Romeu RJ, Finn PR. The problems with delay discounting: a critical review of current practices and clinical applications. Psychol Med. 2021;51:1799–1806. PMID: 34184631. doi:10.1017/S0033291721002282
81. Tversky A, Kahneman D. Judgment under uncertainty: heuristics and biases. Science. 1974;185:1124–1131. PMID: 17835457. doi:10.1126/science.185.4157.1124
82. Kahneman D. Thinking, Fast and Slow. Harlow, Essex: Allen Lane; 2011:9780141033570.
83. Baumeister RF, Vohs KD, DeWall CN, Zhang L. How emotion shapes behavior: feedback, anticipation, and reflection, rather than direct causation. Pers Soc Psychol Rev. 2007;11:167–203. PMID: 18453461. doi:10.1177/1088868307301033
84. Slovic P, Fischhoff B, Lichtenstein S. Facts vs fears: understanding perceived risk. In: Kahneman D, Slovic P, Tversky A, editors. Judgment Under Uncertainty: Heuristics and Biases. Cambridge: Cambridge University Press; 1982:544.
85. Baumeister RF, Bratslavsky E, Finkenauer C, Vohs KD. Bad is stronger than good. Rev Gen Psychol. 2001;5:323–370. doi:10.1037/1089-2680.5.4.323
86. Kahneman D, Tversky A. Prospect Theory: an analysis of decision under risk. Econometrica. 1979;47:263–292. doi:10.2307/1914185
87. Anderson CJ. The psychology of doing nothing: forms of decision avoidance result from reason and emotion. Psychol Bull. 2003;129:139–167. PMID: 12555797. doi:10.1037/0033-2909.129.1.139
88. Loewenstein GF, Weber EU, Hsee CK, Welch N. Risk as feelings. Psychol Bull. 2001;127:267–286. PMID: 11316014. doi:10.1037/0033-2909.127.2.267
89. Choleau C, Albisser AM, Bar-Hen A, et al. A novel method for assessing insulin dose adjustments by patients with diabetes. J Diabetes Sci Technol. 2007;1:3–7. PMID: 19888373. doi:10.1177/193229680700100102
90. Reach G. A psychophysical account of patient non-adherence to medical prescriptions. The case of insulin dose adjustment. Diabetes Metab. 2013;39:50–55. PMID: 23103031. doi:10.1016/j.diabet.2012.08.009
91. Simpson SH, Eurich DT, Majumdar SR, et al. A meta-analysis of the association between adherence to drug therapy and mortality. BMJ. 2006;333:15. PMID: 16790458. doi:10.1136/bmj.38875.675486.55
92. Zhang Y, Pan XF, Chen J, et al. Combined lifestyle factors and risk of incident type 2 diabetes and prognosis among individuals with type 2 diabetes: a systematic review and meta-analysis of prospective cohort studies. Diabetologia. 2020;63:21–33. PMID: 31482198. doi:10.1007/s00125-019-04985-9
93. Curtis JR, Xi J, Westfall AO, et al. Improving the prediction of medication compliance: the example of bisphosphonates for osteoporosis. Med Care. 2009;47:334–341. PMID: 19194337. doi:10.1097/MLR.0b013e31818afa1c
94. Brookhart MA, Patrick AR, Dormuth C, et al. Adherence to lipid-lowering therapy and the use of preventive health services: an investigation of the healthy user effect. Am J Epidemiol. 2007;166:348–354. PMID: 17504779. doi:10.1093/aje/kwm070
95. Solberg LI, Desai JR, O’Connor PJ, Bishop DB, Devlin HM. Diabetic patients who smoke: are they different? Ann Fam Med. 2004;2:26–32. PMID: 15053280. doi:10.1370/afm.36
96. Ahmed AT, Karter AJ, Liu J. Alcohol consumption is inversely associated with adherence to diabetes self-care behaviours. Diabet Med. 2006;23:795–802. PMID: 16842486. doi:10.1111/j.1464-5491.2006.01878.x
97. Ricœur P. Soi-même comme un autre. Paris: Seuil; 1990:432.
98. Reach G, Benarbia L, Bruckert E, et al. Intentionality in adherence to long-term therapies. Results from an online survey of 3001 patients with cardio-metabolic pathologies in France. Patient Prefer Adherence. 2021;15:1739–1753. PMID: 34408407. doi:10.2147/PPA.S318116
99. Reach G, Benarbia L, Benhamou PY, et al. An Unsafe/safe typology in people with type 2 diabetes: bridging patients’ expectations, personality traits, medication adherence, and clinical outcomes. Patient Prefer Adherence. 2022;16:1333–1350. PMID: 35642243. doi:10.2147/PPA.S365398
100. Miron AM, Brehm JW. Reactance Theory - 40 Years Later. Zeitschrift für Sozialpsychologie. 2006;37(1):9–18. doi:10.1024/0044-3514.37.1.9
101. Fogarty JS. Reactance theory and patient noncompliance. Soc Sci Med. 1997;45:1277–1288. PMID: 9381240. doi:10.1016/s0277-9536(97)00055-5
102. Náfrádi L, Nakamoto K, Schulz PJ. Is patient empowerment the key to promote adherence? A systematic review of the relationship between self-efficacy, health locus of control and medication adherence. PLoS One. 2017;12:e0186458. PMID: 29040335. doi:10.1371/journal.pone.0186458
103. Taboada-Vázquez A, Gonzalez-Rodriguez R, Gandoy-Crego M, Clemente M. Personality variables as predictors of health services consumption. Int J Environ Res Public Health. 2021;18:5161. PMID: 34068016. doi:10.3390/ijerph18105161
104. Linkievicz NM, Sgnaolin V, Engroff P, Behr Gomes Jardim G, Cataldo A. Association between Big Five personality factors and medication adherence in the elderly. Trends Psychiatry Psychother. 2022;44:e20200143. PMID: 33834686. doi:10.47626/2237-6089-2020-0143
105. Hazrati-Meimaneh Z, Amini-Tehrani M, Pourabbasi A, et al. The impact of personality traits on medication adherence and self-care in patients with type 2 diabetes mellitus: the moderating role of gender and age. J Psychosom Res. 2020;136:110178. PMID: 32623192. doi:10.1016/j.jpsychores.2020.110178
106. Axelsson M, Brink E, Lundgren J, Lötvall J. The influence of personality traits on reported adherence to medication in individuals with chronic disease: an epidemiological study in West Sweden. PLoS One. 2011;6:e18241. PMID: 21464898. doi:10.1371/journal.pone.0018241
107. Novak JR, Anderson JR, Johnson MD, et al. Does personality matter in diabetes adherence? Exploring the pathways between neuroticism and patient adherence in couples with type 2 diabetes. Appl Psychol Health Well Being. 2017;9:207–227. PMID: 28401663. doi:10.1111/aphw.12087
108. Skinner TC, Bruce DG, Davis TM, Davis WA. Personality traits, self-care behaviours and glycaemic control in type 2 diabetes: the Fremantle diabetes study Phase II. Diabet Med. 2014;31:487–492. PMID: 24147848. doi:10.1111/dme.12339
109. Cheung MM, LeMay K, Saini B, Smith L. Does personality influence how people with asthma manage their condition? J Asthma. 2014;51:729–736. PMID: 24690024. doi:10.3109/02770903.2014.910220
110. Rhodes RE, Smith NE. Personality correlates of physical activity: a review and meta-analysis. Br J Sports Med. 2006;40:958–965. PMID: 17124108. doi:10.1136/bjsm.2006.028860
111. Mischel W, Shoda Y. A cognitive-affective system theory of personality: reconceptualizing situations, dispositions, dynamics, and invariance in personality structure. Psychol Rev. 1995;102:246–268. PMID: 7740090. doi:10.1037/0033-295x.102.2.246
112. Ravaisson F. De L’habitude (1837). Paris: Payot; 1997:144. Available from: https://fr.wikisource.org/wiki/De_l%E2%80%99habitude_(Ravaisson).
113. Phillips LA, Cohen J, Burns E, Abrams J, Renninger S. Self-management of chronic illness: the role of ‘habit’ versus reflective factors in exercise and medication adherence. J Behav Med. 2016;39:1076–1091. PMID: 26980098. doi:10.1007/s10865-016-9732-z
114. Murphy J, Eustace N, Sarma KM, Molloy GJ. Habit strength and adherence to oral contraceptives: the role of time- and place-based cues. Int J Behav Med. 2018;25:431–437. PMID: 29856008. doi:10.1007/s12529-018-9729-9
115. Molloy GJ, Messerli-Bürgy N, Hutton G, Wikman A, Perkins-Porras L, Steptoe A. Intentional and unintentional non-adherence to medications following an acute coronary syndrome: a longitudinal study. J Psychosom Res. 2014;76:430–432. PMID: 24745787. doi:10.1016/j.jpsychores.2014.02.007
116. Lally P, Van Jaarsfeld CHM, Potts HWW, Wardle J. How are habits formed: modelling habit formation in the real world. Eur J Soc Psychol. 2010;40:998–1009. doi:10.1002/ejsp.674
117. Gadkari AS, McHorney CA. Unintentional non-adherence to chronic prescription medications: how unintentional is it really? BMC Health Serv Res. 2012;12:98. PMID: 22510235. doi:10.1186/1472-6963-12-98
118. Ratanawongsa N, Karter AJ, Parker MM, et al. Communication and medication refill adherence: the Diabetes Study of Northern California. JAMA Intern Med. 2013;173:210–218. PMID: 23277199. doi:10.1001/jamainternmed.2013.1216
119. Zikmund-Fisher BJ, Hofer TP, Klamerus ML, Kerr EA. First things first: difficulty with current medications is associated with patient willingness to add new ones. Patient. 2009;2:221–231. PMID: 20634991. doi:10.2165/11313850-000000000-00000
120. Nguyen GC, LaVeist TA, Harris ML, Datta LW, Bayless TM, Brant SR. Patient trust-in-physician and race are predictors of adherence to medical management in inflammatory bowel disease. Inflamm Bowel Dis. 2009;15:1233–1239. PMID: 19177509. doi:10.1002/ibd.20883
121. Mathew BK, De Roza JG, Liu C, et al. Which aspect of patient-provider relationship affects acceptance and adherence of insulin therapy in type 2 diabetes mellitus? A qualitative study in primary care. Diabetes Metab Syndr Obes. 2022;15:235–246. PMID: 35153494. doi:10.2147/DMSO.S344607
122. Bailey PE, Leon T. A systematic review and meta-analysis of age-related differences in trust. Psychol Aging. 2019;34:674–685. PMID: 31169379. doi:10.1037/pag0000368
123. Zhao DH, Rao KQ, Zhang ZR. Patient trust in physicians: empirical evidence from Shanghai, China. Chin Med J. 2016;129:814–818. PMID: 26996477. doi:10.4103/0366-6999.178971
124. Pourhabibi N, Mohebbi B, Sadeghi R, et al. Determinants of poor treatment adherence among patients with type 2 diabetes and limited health literacy: a scoping review. J Diabetes Res. 2022;2022:2980250. PMID: 35832786. doi:10.1155/2022/2980250
125. Lindquist LA, Go L, Fleisher J, Jain N, Friesema E, Baker DW. Relationship of health literacy to intentional and unintentional non-adherence of hospital discharge medications. J Gen Intern Med. 2012;27:173–178. PMID: 21971600. doi:10.1007/s11606-011-1886-3
126. Messer LH, Sousa K, Cook PF. Applying two minds theory to self-management of Type 1 diabetes. Res Nurs Health. 2019;42(6):500–508. PMID: 31587327. doi:10.1002/nur.21983
127. Najdzionek P, McIntyre-Wood C, Amlung M, MacKillop J. Incorporating socioeconomic status into studies on delay discounting and health via subjective financial status: an initial validation in tobacco use. Exp Clin Psychopharmacol. 2023;31(2):475–481. PMID: 36595454. doi:10.1037/pha0000628
128. Libet B, Gleason CA, Wright EW, Pearl DK. Time of conscious intention to act in relation to onset of cerebral activity (readiness-potential). The unconscious initiation of a freely voluntary act. Brain. 1983;106:623–642. doi:10.1093/brain/106.3.623
129. Kim J. Physicalism, or Something Near About. Princeton Monographs in Philosophy; 2005:200.
130. Spinoza, Ethics, III, Prop. 6.
131. Freud S. Beyond the Pleasure Principle. New York: Norton Library; 1990.
132. Reach G. Decisions in the Psychology of Glucose Monitoring. J Diabetes Sci Technol. 2019;13:1169–1174. PMID: 31200613. doi:10.1177/1932296819854109
133. Davies MJ, D’Alessio DA, Fradkin J, et al. Management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia. 2018;61:2461–2498. PMID: 30288571. doi:10.1007/s00125-018-4729-5
134. Kayyali R, Gebara SN, Hesso I, et al. Shared decision making and experiences of patients with long-term conditions: has anything changed? BMC Health Serv Res. 2018;18(1):763. PMID: 30305085. doi:10.1186/s12913-018-3575-y
135. Reach G, Calvez A, Sritharan N, et al. Patients’ perceived importance of medication and adherence in polypharmacy, a quantitative, cross-sectional study using a questionnaire administered in three doctors’ private practices in France. Drugs Real World Outcomes. 2023. PMID: 36997772. doi:10.1007/s40801-023-00361-7
136. Reach G. Patient education, nudge, and manipulation: defining the ethical conditions of the person-centered model of care. Patient Prefer Adherence. 2016;10:459–468. PMID: 27103791. doi:10.2147/PPA.S99627
137. Phillips LS, Branch WT, Cook CB, et al. Clinical inertia. Ann Intern Med. 2001;135:825–834. PMID: 11694107. doi:10.7326/0003-4819-135-9-200111060-00012
138. Reach G. Clinical Inertia, a Critique of Medical Reason, Foreword by Jon Elster and Joel Ménard. Springer; 2015; doi:10.1007/978-3-319-09882-1
139. Reach G. Patient non-adherence and healthcare-provider inertia are clinical myopia. Diabetes Metab. 2008;34:382–385. PMID: 18706843. doi:10.1016/j.diabet.2008.02.008
140. Reach G. Simplistic and complex thought in medicine: the rationale for a person-centered care model as a medical revolution. Patient Prefer Adherence. 2016;10:449–457. PMID: 27103790. doi:10.2147/PPA.S103007
141. Reach G. Pour une médecine humaine, étude philosophique d’une rencontre [For a humane medicine, a philosophical investigation of an encounter]. Paris, Hermann. English version in preparation; 2022. Available from: https://www.editions-hermann.fr/livre/pour-une-medecine-humaine-reach-gerard.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.