Back to Journals » Psychology Research and Behavior Management » Volume 16
How Impulsivity is Associated with Adolescent Depression: The Role of Substance Use, Gender and Social Support
Authors Lee TH, Liu HC, Huang YH, Sun FJ, Liu SI
Received 5 September 2023
Accepted for publication 26 November 2023
Published 7 December 2023 Volume 2023:16 Pages 4959—4970
DOI https://doi.org/10.2147/PRBM.S429923
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Tsung-han Lee,1 Hui-Ching Liu,1 Yu-Hsin Huang,1 Fang-Ju Sun,2 Shen-Ing Liu1
1Department of Child and Adolescent Psychiatry, MacKay Memorial Hospital, Taipei City, Taiwan; 2Department of Medical Research, MacKay Memorial Hospital, Taipei City, Taiwan
Correspondence: Shen-Ing Liu, Email [email protected]
Background: Some risk/protective factors of adolescent depression have been proposed but have not been comprehensively studied. Recent advances in neuroimaging techniques have provided greater insight into the underlying neuropsychiatric mechanisms of depression-related factors such as impulsivity, substance use, gender difference and social support. However, how these factors are interconnected and how they affect depression in the real world is poorly understood. This study aimed to explore the relationships between adolescent depression with trait impulsivity, substance use and gender. We also tested the hypothesis that social support may play a buffering role in preventing depression. By expanding the diathesis-stress model.
Methods: The adolescents enrolled in this study were grade 1 senior high school students from northern Taiwan (N = 5879), and they were assessed for depression, trait impulsivity, and tobacco/alcohol use. Hierarchical multiple linear regression was performed to control possible confounders, including other depression-related diathesis and sociodemographic variables. Gender differences were also analyzed by separately examining variables significantly associated with depression.
Results: A higher level of depression was associated with female gender, trait impulsivity, low self-esteem, negative attitude towards the future, tobacco use, alcohol use, family discord and difficulty in basic family needs. Good parental health, living with their biological family and social support were protective factors. Trait impulsivity was significantly associated with depression after controlling for the confounding factors. Gender-specific analysis showed that trait impulsivity and tobacco use had a significant synergistic interaction on female depression. Social support from parents/peers was significantly associated with depression, but social support from other family members/teachers was not.
Conclusion: The current study advances the understanding of adolescent depression and highlights that trait impulsivity, addictive substance use, social support and their interaction may play an influential role in the emergence of adolescent depression. Gender-specific research and treatment approach are also crucial, and more investigations are necessary.
Keywords: depression, impulsivity, social support, tobacco, gender, self-esteem
Introduction
Despite advances in screening tools and pharmacological/psychological interventions of adolescent depression,1–3 depression still causes a great burden on youths during the process of transition. These functional declines may include academic failure, substance use comorbidity, self-harm, suicidality and some sequelae could even persist into adulthood.4–6 Researchers have reported that even subclinical depression in adolescents may lead to long-term clinical and social complications.7
Thus, it is important to understand the risk/protective factors of depression. Nevertheless, the association between impulsivity and depression, and how this association is modulated by other factors such substance use, social support and gender is poorly understood. Advances in neuroimaging techniques and neuropsychiatric research have revealed that seemingly different mental disorders and psychological traits may share unique but interconnected neural substrates and neural biochemistry.8 For example, depression, impulsivity and substance use may share common functional abnormalities of the prefrontal cortex or reward systems;9,10 people with trait impulsivity are more prone to substance use, however, repeated exposure to addictive substances can subsequently lead to dopaminergic hypoactivity and even re-shaping the brain structure.11–13 However, in the field of managing and treating mental health problems, there is still a gap in our understanding of the interactions between depression, impulsivity, substance use and social support in the real world. Therefore, understanding these potential risk and protective factors of adolescent depression is essential to allow for timely preventions and tailored treatment approaches.14
The Stress-Diathesis Model of Depression and Trait Impulsivity
Among theories explaining adolescent depression, the stress-diathesis model is one of the most prominent.15–17 The cognitive vulnerability perspective is built on the framework of Beck’s theory,18 and current depression-related cognitive vulnerability theory includes a wide range of characteristics, such as dysfunctional attitude, low self-esteem, early maladaptive schema, and attribution bias.19,20 Current evidence has shown that stressors not only play the roles of current triggers but also act as early factors, which exert their effects by shaping personality traits in one’s early life.15,21 Several socio-contextual factors have been identified as stressors of adolescent depression, including family conflict, not living with parents, poor peer relationships,22,23 and lower socio-economic status.24–26
Although the relationship between trait impulsivity and adolescent suicidality is widely recognized27,28 and suicidality is known to be related to depression, the connection between trait impulsivity with adolescent depression has been less studied. Among the depression-prone diatheses, the importance of trait impulsivity has only recently been identified,29–32 and further investigations are needed.
Social Support and Substance Use
Beyond the traditional stress-diathesis model, accumulating evidence has shown that social support23,33,34 and addictive substance use35 are influential trajectory-altering factors for depression.
Some researchers have speculated that social support may act as a buffer between environmental adversity and cognitive vulnerability during the disorder emerging process of depression.36–38 For adults and the elderly, the importance of social support in preventing depression has been well-identified, and the effects from different supporting sources have been shown to be different among different age groups.39,40 However, there is still a lack of understanding of how various social relationships differently support adolescents from mental health problems.41
In contrast to merely viewing substance use as a risk factor for adolescent depression,39 it is currently believed that substance use has a more complex role in the etiology of adolescent depression. Substance use may simultaneously act as predisposing, comorbid or perpetuating factors for adolescent depression. Moreover, a bidirectional association may also exist between depression and substance use behavior.42,43
The Present Study
In the current study, we explored the risk and protective factors of adolescent depression using the stress-diathesis model including social support and substance use variables. Based on previous literature, we hypothesized that: (1) trait impulsivity may be positively associated with depression in adolescents after controlling for other predictive variables; (2) substance use, ie, tobacco use and hazardous alcohol use, may be an additional risk factor for depression; (3) there may be synergistic interplay between impulsivity and substance use; (4) social support from different relationships may have differing effects on depression; and (5) these effects may differ among girls and boys, since some researchers have reported that male and female responses to environmental stressors seem to differ.44–46
Method
Study Population and Recruitment
This study was part of the Taiwan Adolescent Self-harm Project (TASP). A total of 5879 adolescents from 14 senior high schools were recruited in northern Taiwan from October 2008 to March 2010. These schools account for 11.7% of all high schools in Taipei (9 urban, 3 suburban, and 2 rural schools according to the Taiwan-Fukien Demographic Fact Book). All of the selected high schools had well-equipped computer classrooms, and the participants independently filled out the self-administered questionnaires on computers to ensure anonymity. To avoid the risk of coercion, recruitment was performed by a master’s level research assistant, and the school staff were not involved. The study procedure and confidentiality issues were explained in detail to the participants by the research assistant, and written informed consent was obtained from all participants and their parents. This study was approved by the Institutional Review Board of our hospital and complied with the Declaration of Helsinki.
Measurements
The online questionnaire was interactive with a skip pattern design and took about 30 minutes to complete. The questionnaires included the Chinese version of the Patient Health Questionnaire (PHQ-9),47 the Chinese version of the Multidimensional Scale of Social Support (MDSS), the Chinese version of the Barratt Impulsiveness Scale Version 11 (BIS-11),48 the Rosenberg Self-Esteem Scale (RSES),49 the Alcohol Use Disorder Identification Test-Consumption (AUDIT-C),50 tobacco use habit and the participant’s attitude with regards to the future. Sociodemographic variables, which may reflect the participant’s socioeconomic level or be possible stressors, were also collected.
Depression
The outcome variable was the score of the PHQ-9, which is a 9-item self-report inventory based on the Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition (DSM-IV).50 The Chinese version of the PHQ-9 has been shown to have good internal consistency (alpha = 0.84) and acceptable test-retest reliability (ICC = 0.80) in adolescent populations.47
Sociodemographic Variables
The participant’s age, gender, school region, school ranking and family situation were collected. The family situation included living with their biological family, difficulty in basic family needs, parental education level, current parental health status, and the existence of family discord.
Social Support
The MDSS is a self-report questionnaire which measures social support from various sources. It can be tailored according to the needs of different studies,51 and past research has shown high consistency by alpha coefficient of internal reliability to its items.51,52 The four most common surrounding social support sources selected in this study included parents, other family members (such as siblings and relatives), peers and teachers, and the scores of different support sources were analyzed separately.
Psychological Characteristics
The diathesis factors in this study included impulsivity, self-esteem and attitude towards the future. Impulsivity was measured using the BIS-11, which is a 30-item self-report questionnaire.53 The Chinese version of the BIS-11 has been shown to have good internal consistency in Taiwanese adolescents.48 Self-esteem was measured using the Chinese version of the RSES,49 which consists of 10 items on self-respect and self-acceptance. The reliability and validity of the Chinese version of the RSES have also been demonstrated.54,55 Attitude towards the future was assessed by asking the question, “What is your attitude towards the future?” The results were coded as 0 for “positive”, 1 for “neutral/no opinion”, and 2 for “negative”.
Tobacco and Alcohol Use
All participants were asked about their habits of tobacco use and alcohol drinking behavior. The frequency and history of tobacco use were asked, and whether he/she currently used tobacco was coded for analysis. Alcohol drinking was assessed by the Alcohol Use Disorder Identification Test-Consumption (AUDIT-C), which is comprised of the first three questions of the full AUDIT. Hazardous alcohol drinking was defined as an AUDIT-C score ≥ 4, which has been shown to have good reliability.50
Statistical Analysis
Descriptive and analytical statistics were obtained using Statistics Package for Social Sciences (SPSS) version 23.0 (IBM). In descriptive analysis, we also examined gender differences in demographic variables, social support, psychological characteristics and tobacco/alcohol use. Risk and protective factors for depression were analyzed first using univariate regression analysis. The joint effect of the independent variables that were significant in univariate analysis was then assessed using multiple hierarchical regression analysis. The stress-diathesis theory was incorporated into the multiple regression models with a hierarchical approach by adding variables from distal predictors to proximal predictors. The order of predictor entry was chosen based on early to late chronological development. To examine the effect of different variables on depression, gender and environmental stress factors (school ranking, living with biological parents, difficulty in basic family needs, parental health status, family discord) were entered first in order to control for their effects (model 1). MDSS scores of parents, other family members, peers and teachers were added in model 2. Psychological characteristics (BIS-11, RSES and attitude towards the future) were added in model 3, and tobacco/alcohol use was added in the final step (model 4). Based on a well-documented gender pattern in depression, the associations between depression and each identified factor were separately assessed for the girls and boys (model 5). Depression and tobacco use were found to be significantly related in the girls, but the relationship was not significant in the boys.
Due to the gender differences in the associations between depression and tobacco use, we performed additional interaction analysis between the BIS-11 score and tobacco use to explore other potential associations with adolescent depression. The BIS-11 score was centered to the grand mean in order to reduce multicollinearity, and variables with significance in the previous hierarchical regressions were controlled. Figures illustrating the form of interaction were then created using regression lines between PHQ-9 score, tobacco use and BIS-11 score among the females and males. The cut-off level between high and low impulsivity was defined as a BIS-11 score of 68 (mean + SD),53 and previous studies have shown that people above this level tend to have more aggressiveness, faster cognitive tempo and instability on Conners continuous performance task.56 Simple slope analysis was used to aid interpretation of the interaction plots.
Results
Description of the Sample
Among the 5879 participants, the mean PHQ-9 score was 5.7 (SD = 4.6). The female students (n = 3544) had significantly higher PHQ-9 scores (p = 0.020) than the male students (n = 3355), with means (SD) of 6.1 (4.6) and 5.2 (4.6), respectively. This result was consistent with the theory that females may be more vulnerable to depression than males.57 Nearly one fifth of the participants did not live with their biological parents (Table 1). Compared to the girls’ parents, the boys’ parents had higher education levels (> 9 years, p < 0.001) better health status (p = 0.002 for the boys’ fathers, p = 0.004 for the boys’ mothers), suggesting that there may have been gender inequality in our study population. Compared to the boys, the girls received higher social support from their peers (p < 0.001) and teachers (p < 0.001). For diathesis, while there were no significant gender differences in trait impulsivity (BIS-11 score), the boys attained significantly higher self-esteem scores (RSES: 28.8 vs 27.9) and more positive attitude towards the future than the girls (53.7% vs 46%). Regarding substance use behaviors, significantly more of the boys had hazardous drinking (male: 13.5% vs female: 8%, p < 0.001) and current tobacco use (male: 5.7% vs female: 1.9%, p < 0.001) compared to the girls.
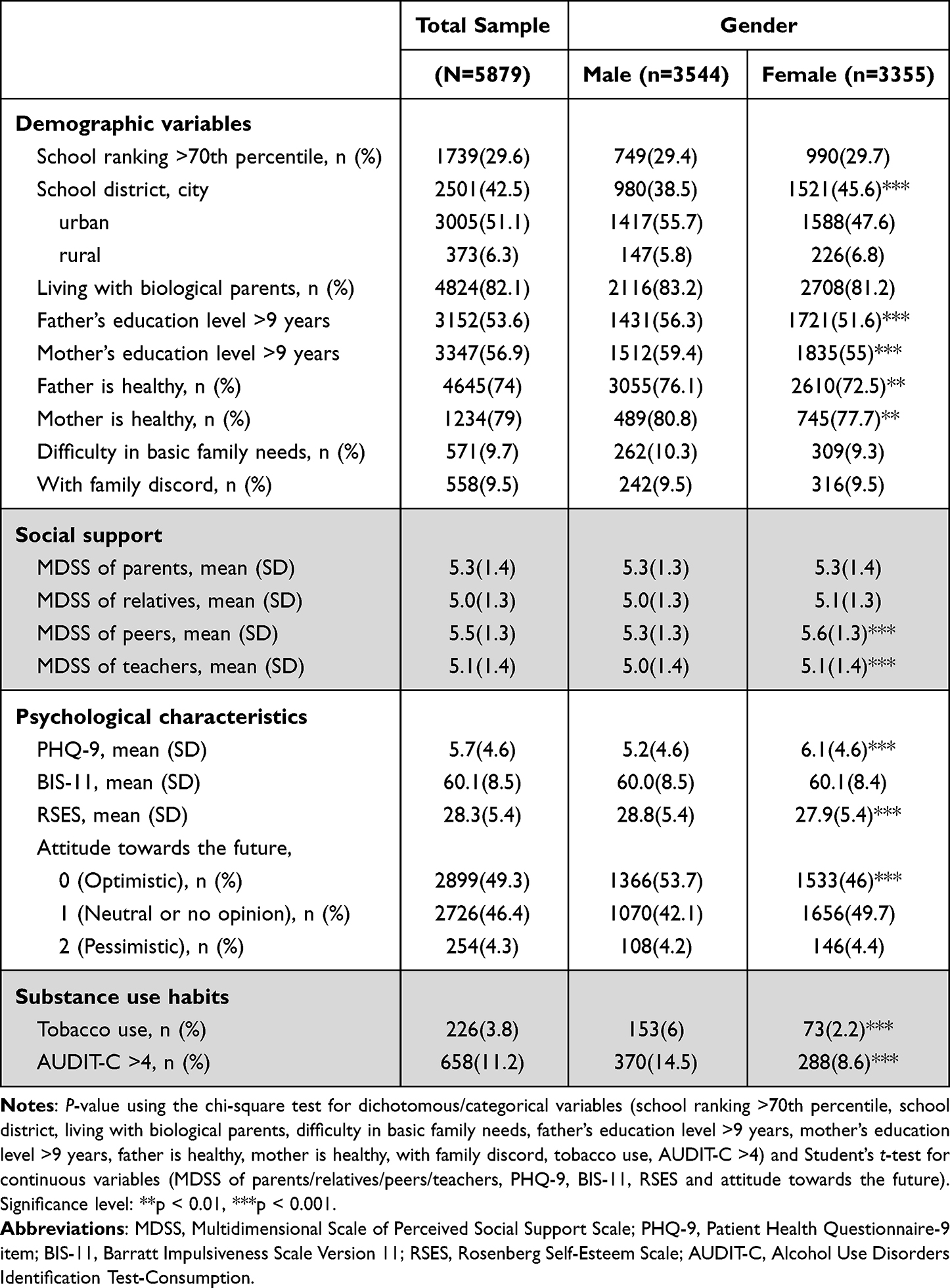 |
Table 1 Demographic Variables, Social Support, Psychological Characteristics and Substance Use Habits |
Univariate and Hierarchical Multiple Regressions
To reduce the number of variables, univariate regression analysis was used first to identify variables significantly associated with the PHQ-9. The results of univariate and hierarchical multiple regression analyses are presented in Table 2. In model 1, depression was predicted by female gender, living with biological parents, parents being unhealthy, having family discord, and difficulty in basic family needs. When MDSS scores were entered into the regression in model 2, depression was negatively associated with social support from the four most common sources (parents, other family members, peers and teachers).
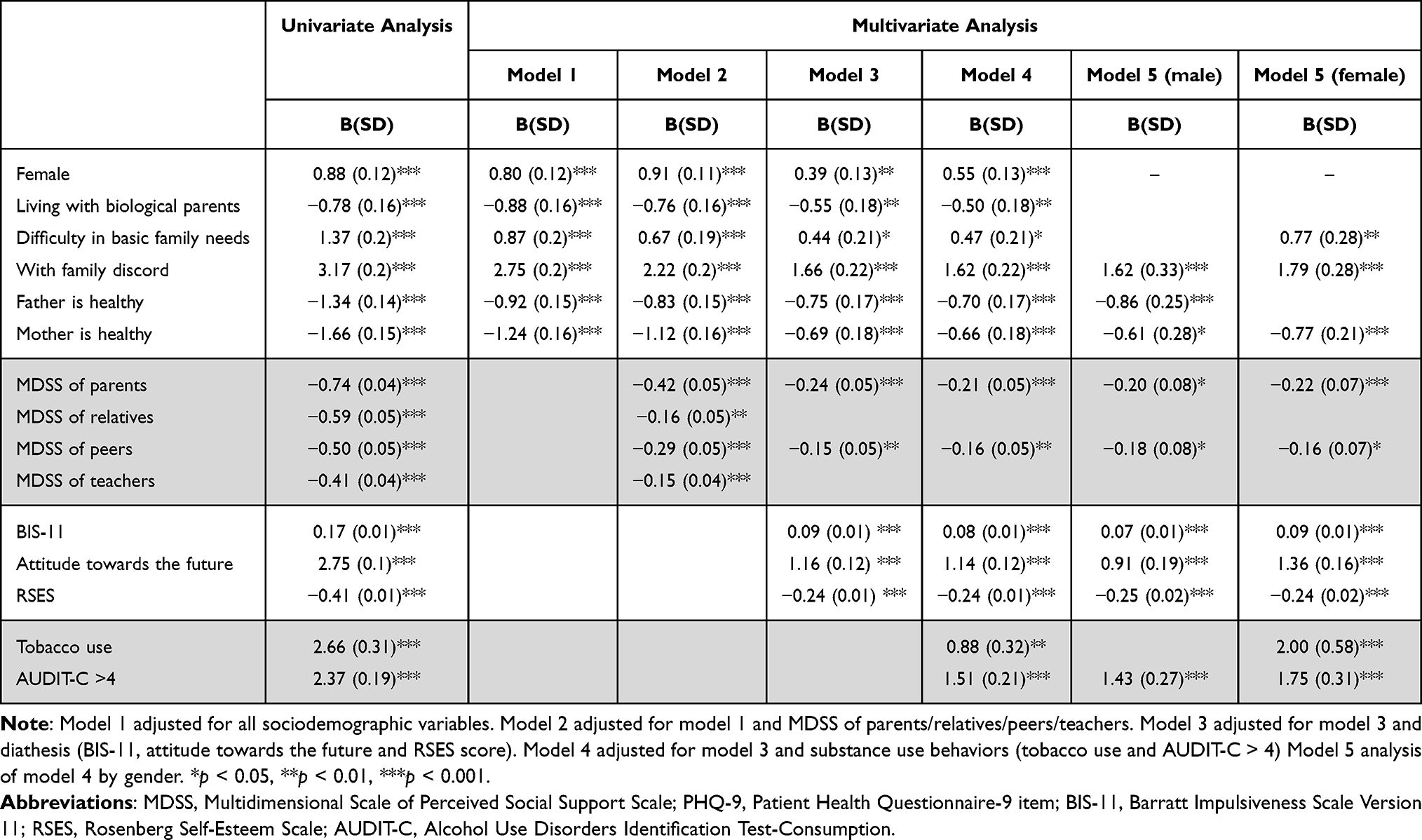 |
Table 2 Univariate Analysis and Hierarchical Stepwise Regression Examining Multivariate Correlates of PHQ-9 |
In model 3, we studied the effects of diathesis on depression after controlling for sociodemographic and social support variables. Depression was significantly associated with trait impulsivity, negative attitude towards the future and lower self-esteem. The MDSS scores of other family members/teachers lost their significance in model 3, while the other significant variables identified in model 2 remained significant. Model 4 included variables of substance use, and depression was significantly associated with current tobacco use and hazardous alcohol drinking. The three studied diatheses retained their significance after the adjustments.
We further analyzed gender differences in depression in model 5. For both genders, the risk factors for depression included higher impulsivity, negative attitude towards the future, low self-esteem, family discord, and alcohol use, while the protective factors included social support from parents/peers, and mothers having a good health status. Good health status of the father was a protective factor against depression only in the boys, and the girls were more vulnerable to the influences of difficulty in basic family needs and current tobacco use.
Interaction and Slope Analyses
Our results showed that trait impulsivity and substance use were highly correlated, and that trait impulsivity and depression may involve common neural substrates. Consequently, in order to explore why the correlation between girls’ tobacco use was significantly correlated with depression (B = 2, SD = 0.58) while boys’ tobacco use was not after controlling for the confounding variables, interaction analysis between impulsivity and tobacco use was carried out to further understand the gender differences. We found an interaction between trait impulsivity (BIS-11 score) and tobacco use in the girls rather than in the boys. The result was significant after controlling for potential interfering variables (p < 0.001, Table 3). The interactions were plotted separately by gender (Figure 1), and the figure illustrating females showed that when impulsive trait was superimposed with current tobacco use, the girls had a higher level of depression (female tobacco users: B = 5.154, standard error [SE] = 1.548, p = 0.002; female non-users: B = 1.943, SE = 0.215, p < 0.001). We also analyzed the alcohol use behavior, but we did not find similar differences between genders.
 |
Table 3 Analysis of Interactions Between Tobacco Use and Impulsivity in Terms of Gender |
 |
Figure 1 The Synergistic Effect of Impulsivity and Tobacco Use on Adolescent Female Depression. Note: Depression symptom scores of the Patient Health Questionnaire-9 were plotted as a function of impulsivity. Females (A) had significantly stronger interaction of impulsivity × tobacco use than males (B). |
Discussion
This study has three major findings. First, an association between impulsivity and adolescent depression was confirmed after controlling for confounding variables. Second, a synergistic effect between tobacco use and trait impulsivity was found in the female participants. Third, social support, especially from parents/peers, may protect adolescents from depression.
Associations Between Depression, Impulsivity and Other Diathesis
Of the etiologies of adolescent depression, diathesis (or personality trait) has been proposed to be an important factor. Among our studied diatheses, negative attitude towards the future is well-known as Beck’s model of cognitive triad of depression.58 The role of low self-esteem in depression is more complicated. Current evidence has shown that low self-esteem may be a precursor and a prolonging factor for adolescent depression, and low self-esteem may persist after depression remits.20,59,60 Our findings also support that these two diatheses are important factors for adolescent depression.
As the core of externalized spectrum of developmental disorders,61 impulsivity is present in many adolescent mental disorders, including substance use disorder, attention deficit/hyperactivity disorder, and bipolar spectrum. Nevertheless, the relationship between adolescent depression and trait impulsivity has not been fully elucidated. Our results are similar to past studies conducted in French and Tunisian populations, in that impulsive adolescents had higher levels of depression.29,31 In the previous studies, the sample sizes were relatively small, and only a limited number of confounders were controlled. A strength of this study is the large number of cases and potential predictors were controlled in the analysis. In our study, the correlations between depressive symptoms and impulsivity scores were significant in both genders after controlling for other depression-prone diatheses, substance use behavior and sociodemographic variables. This result is also compatible with other studies which have suggested that trait impulsivity and depression may share similar neural substrates, such as mesolimbic dopamine activity or aberrant connections between frontal pole and other brain areas.9,62,63 Therefore, trait impulsivity should also be considered when managing adolescent depression and pursuing the underlying etiologies.
Interactions Between Trait Impulsivity, Gender and Tobacco Use
Substance misuse was once viewed as a male-predominant problem due to its high incidence rate among males. The increasing rate of female addiction in recent years suggests that adolescent and young adult females are also vulnerable to addictive substance use.64,65 To explain the rising rate, some researchers have postulated that female users tend to experience higher pleasure responses on exposure to addictive substances and become addicted faster than males once they initiate substance use.66 The association between depression and adolescent tobacco smoking and alcohol drinking has been documented, and some researchers have speculated that males and females may have different pathways,67–71 however, the underlying pathophysiology of gender differences has not been fully explored.
Our findings may provide new insights into this issue. In our study population, when controlling for other predictors, tobacco use was associated with depression in the girls, but a similar association was not found in the boys. In order to understand why female tobacco users were more prone to depression, we performed interaction analysis, and the results showed a synergistic effect between trait impulsivity and female tobacco use. The synergic effect may suggest that, if trait impulsivity and tobacco use are superimposed, girls may have a higher level of depression. In past studies, impulsivity has been found to be a predisposing factor for tobacco use,71 and moderating effects between impulsivity, substance use and depression have been reported.46,72,73 However, few studies have examined gender differences. We speculate that the gender difference may be driven by both socio-contextual and biological factors. The higher incidence of tobacco use in boys may result from the influence of peer behavior, and their tobacco use behavior tends to be normalized in male subculture.74 Thereby, boys face lower psychosocial pressure if they initiate tobacco use. However, in the traditional value judgement of Taiwanese, girls are more discouraged from using tobacco and can face criticism if they do. This traditional value may be a protective factor for non-users from initiating tobacco use,75 but girls with higher impulsivity may be left as a vulnerable subgroup in young female population. Once initiating tobacco use, these girls may face higher pressure or even emotional problems. The above pressures and the depression-prone tendency of impulsivity result in a higher incidence of dysphoric mood and higher need for the stimulating and euphoric effects of tobacco. These effects can also accelerate the addictive cycle for these girls. The cross-sectional design of our study only allows for testing associations, and more comprehensive and longitudinal studies are needed to examine the causal relationships.
The Role of Social Support
In preventing depression, the main sources of social support may shift from childhood to later life,39 and some researchers suggest that the effects of different social relationships may differ according to one’s age.39,40 Earlier studies have proven the importance of social support for adolescents, and adolescents are known to receive social support from various sources.76,77 Nonetheless, there still remains a research gap of which supporting sources are more influential or crucial for adolescents to pass the transition period.
In our studied adolescents, four main sources of social support were analyzed, including parents, other family members, peers and teachers. Only support from parents and peers retained significance after controlling for covariates. Comparing our results with past research, we propose that there may be cultural variations between relationship-specific social support sources. In an Australian study, lack of family/teacher support predicted depression rather than lack of peer support,41 whereas in a study from the Mid-Atlantic United States, adolescent depression was associated with less parental/sibling/peer communication, and gender differences were found.78 In an Israeli study comparing the effects among family, friends, and school personnel, only family social support was prominent in protecting adolescents from depression. In a Japanese study focusing on the classroom, the role of teacher support was also important in reducing depressive score,34,79 but support from other sources was not compared. In past studies, parental support was mostly analyzed within the scope of family support, and this approach may hinder our understanding of the difference between them. Our results showed that parental support, as the pillars of most families, seemed to be different and more influential than support from other family members in buffering adolescents against depression. Combining our results with past research, it also seems that parental support plays a pivotal role in preventing adolescents from depression across most cultures. Social support from other sources is still crucial, but the effects vary according to the ethnicity or nationality of the youths. Advances in neuropsychiatry have also revealed that receiving social support or not may modulate neural responses in the amygdala and striatum activity,80,81 and that these circuits are related to happiness and reward sensitivity.82,83 Since different social support intertwine in one’s developmental trajectory, how they affect the adolescent development is a critical issue to be explored in future studies.
Limitations and Future Directions
This study has several limitations. First, while the sample size was large, the cross-sectional design only allows for the examination of correlations, but not the causal relationship or potential underlying mechanisms. Second, illicit substances were not included in our study, which limits the generalizability of our findings to other addictive substances. Third, self-report surveys are prone to response bias, including recall bias and social desirability bias.84 However, some evidence has demonstrated that young people are more inclined to report their emotional problems and substance use habits through anonymous school-based surveys, and this method has been proven to have higher validity.85,86 Fourth, although the recruited school-based population may represent the majority of adolescents in Taiwan, adolescents who dropped out of school may represent another population with different characteristics.87,88 Fifth, the studied population only included adolescents from 14 senior high schools in Taipei, and this may not fully represent the diversity of adolescent populations in other regions, countries or cultures. Further research and replication studies are needed to confirm our findings. Finally, early, middle and late adolescents have been considered to be different groups,21 and only the first grade of senior high school students were included in our study. In the Taiwanese education system, this age group has just passed the joint entrance examination and been assigned to different schools. Namely, they were just adapting to different environments, and this background made them appropriate candidates to be investigated.
Conclusion
Overall, our findings suggest that impulsivity is a non-negligible factor in the research field of adolescent depression. The interaction between trait impulsivity and tobacco use in female depression implies that girls and boys may have different pathways or pathophysiology in the process of developing depression.44,89,90 To manage the complex and unmet needs of adolescent depression, how social support protect adolescents from depression should also be a focus in clinical practice and future investigations.23,33
Ethics Approval and Informed Consent
This study was approved by the Institutional Review Board of Mackay Memorial Hospital. Written informed consent was obtained from all participants and their parents.
Acknowledgments
The authors thank all the students, parents, research assistants and teachers participating in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by grants from the Ministry of Science and Technology, Taiwan, R.O.C. (NSC 9802314-B-195-011 MY3).
Disclosure
The authors declare that there are no conflict of interests.
References
1. Weersing VR, Jeffreys M, Do MT, Schwartz KT, Bolano C. Evidence base update of psychosocial treatments for child and adolescent depression. J Clin Child Adolesc Psychol. 2017;46(1):11–43. doi:10.1080/15374416.2016.1220310
2. Forman-Hoffman VL, Viswanathan M. Screening for depression in pediatric primary care. Curr Psychiatry Rep. 2018;20(8):62. doi:10.1007/s11920-018-0926-7
3. MacQueen GM, Frey BN, Ismail Z, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 6. special populations: youth, women, and the elderly. Can J Psychiatry. 2016;61(9):588–603. doi:10.1177/0706743716659276
4. Johnson D, Dupuis G, Piche J, Clayborne Z, Colman I. Adult mental health outcomes of adolescent depression: a systematic review. Depress Anxiety. 2018;35(8):700–716. doi:10.1002/da.22777
5. Li H, Luo X, Ke X, et al. Major depressive disorder and suicide risk among adult outpatients at several general hospitals in a Chinese Han population. PLoS One. 2017;12(10):e0186143. doi:10.1371/journal.pone.0186143
6. Joshi SV, Jassim N, Mani N. Youth depression in school settings: assessment, interventions, and prevention. Child Adolesc Psychiatr Clin N Am. 2019;28(3):349–362. doi:10.1016/j.chc.2019.02.017
7. Sihvola E, Keski-Rahkonen A, Dick DM, et al. Minor depression in adolescence: phenomenology and clinical correlates. J Affect Disord. 2007;97(1–3):211–218. doi:10.1016/j.jad.2006.06.019
8. Filatova EV, Shadrina MI, Slominsky PA. Major depression: one brain, one disease, one set of intertwined processes. Cells. 2021;10(6):1283. doi:10.3390/cells10061283
9. Tanaka M, Szabó Á, Spekker E, Polyák H, Tóth F, Vécsei L. Mitochondrial impairment: a common motif in neuropsychiatric presentation? The link to the tryptophan–kynurenine metabolic system. Cells. 2022;11(16):2607. doi:10.3390/cells11162607
10. Ahrweiler N, Santana-Gonzalez C, Zhang N, et al. Neural activity associated with symptoms change in depressed adolescents following self-processing neurofeedback. Brain Sci. 2022;12(9):1128. doi:10.3390/brainsci12091128
11. Cushnie AK, Tang W, Heilbronner SR. Connecting circuits with networks in addiction neuroscience: a salience network perspective. Int J Mol Sci. 2023;24(10). doi:10.3390/ijms24109083
12. Goutaudier R, Joly F, Mallet D, et al. Hypodopaminergic state of the nigrostriatal pathway drives compulsive alcohol use. Molecular Psychiatr. 2023;28(1):463–474. doi:10.1038/s41380-022-01848-5
13. Jarcho JM, Wyngaarden JB, Johnston CR, Quarmley M, Smith DV, Cassidy CM. Substance abuse in emerging adults: the role of neuromelanin and ventral striatal response to social and monetary rewards. Brain Sci. 2022;12(3):352. doi:10.3390/brainsci12030352
14. Kassis W, Artz S, White J. Understanding depression in adolescents: a dynamic psychosocial web of risk and protective factors. Child Youth Care Forum. 2017;46(5):721–743. doi:10.1007/s10566-017-9404-3
15. Kalamatianos A, Canellopoulos L. A diathesis-stress model conceptualization of depressive symptomatology. Psychiatriki. 2019;30(1):49–57. doi:10.22365/jpsych.2019.301.49
16. Patten SB. Major depression epidemiology from a diathesis-stress conceptualization. BMC Psychiatry. 2013;13(1):19. doi:10.1186/1471-244x-13-19
17. Burke P, Elliott M. Depression in pediatric chronic illness. A diathesis-stress model. Psychosomatics. 1999;40(1):5–17. doi:10.1016/s0033-3182(99)71266-1
18. Beck AT. Depression: Clinical, Experimental, and Theoretical Aspects. Hoeber Medical Division, Harper & Row; 1967.
19. Stikkelbroek Y, Bodden DH, Kleinjan M, Reijnders M, van Baar AL, van Amelsvoort T. Adolescent depression and negative life events, the mediating role of cognitive emotion regulation. PLoS One. 2016;11(8):e0161062. doi:10.1371/journal.pone.0161062
20. Lin HC, Tang TC, Yen JY, et al. Depression and its association with self-esteem, family, peer and school factors in a population of 9586 adolescents in southern Taiwan. Psychiatry Clin Neurosci. 2008;62(4):412–420. doi:10.1111/j.1440-1819.2008.01820.x
21. Braet C, Van Vlierberghe L, Vandevivere E, Theuwis L, Bosmans G. Depression in early, middle and late adolescence: differential evidence for the cognitive diathesis-stress model. Clin Psychol Psychother. 2013;20(5):369–383. doi:10.1002/cpp.1789
22. Yap MB, Pilkington PD, Ryan SM, Jorm AF. Parental factors associated with depression and anxiety in young people: a systematic review and meta-analysis. J Affect Disord. 2014;156:8–23. doi:10.1016/j.jad.2013.11.007
23. Platt B, Cohen Kadosh K, Lau JY. The role of peer rejection in adolescent depression. Depress Anxiety. 2013;30(9):809–821. doi:10.1002/da.22120
24. Lorant V, Deliege D, Eaton W, Robert A, Philippot P, Ansseau M. Socioeconomic inequalities in depression: a meta-analysis. Am J Epidemiol. 2003;157(2):98–112. doi:10.1093/aje/kwf182
25. Ride J. Is socioeconomic inequality in postnatal depression an early-life root of disadvantage for children? Eur J Health Econ. 2019;20(7):1013–1027. doi:10.1007/s10198-019-01073-y
26. Pino EC, Damus K, Jack B, Henderson D, Milanovic S, Kalesan B. Adolescent socioeconomic status and depressive symptoms in later life: evidence from structural equation models. J Affect Disord. 2018;225:702–708. doi:10.1016/j.jad.2017.09.005
27. Renaud J, Berlim MT, McGirr A, Tousignant M, Turecki G. Current psychiatric morbidity, aggression/impulsivity, and personality dimensions in child and adolescent suicide: a case-control study. J Affect Disord. 2008;105(1–3):221–228. doi:10.1016/j.jad.2007.05.013
28. Lockwood J, Daley D, Townsend E, Sayal K. Impulsivity and self-harm in adolescence: a systematic review. Eur Child Adolesc Psychiatr. 2017;26(4):387–402. doi:10.1007/s00787-016-0915-5
29. d’Acremont M, Van der Linden M. How is impulsivity related to depression in adolescence? Evidence from a French validation of the cognitive emotion regulation questionnaire. J Adolesc. 2007;30(2):271–282. doi:10.1016/j.adolescence.2006.02.007
30. Fradkin Y, Khadka S, Bessette KL, Stevens MC. The relationship of impulsivity and cortical thickness in depressed and non-depressed adolescents. Brain Imaging Behav. 2017;11(5):1515–1525. doi:10.1007/s11682-016-9612-8
31. Khemakhem K, Boudabous J, Cherif L, et al. Impulsivity in adolescents with major depressive disorder: a comparative tunisian study. Asian J Psychiatr. 2017;28:183–185. doi:10.1016/j.ajp.2017.06.002
32. Sanches M, Scott-Gurnell K, Patel A, et al. Impulsivity in children and adolescents with mood disorders and unaffected offspring of bipolar parents. Compr Psychiatry. 2014;55(6):1337–1341. doi:10.1016/j.comppsych.2014.04.018
33. Bodner N, Kuppens P, Allen NB, Sheeber LB, Ceulemans E. Affective family interactions and their associations with adolescent depression: a dynamic network approach. Dev Psychopathol. 2018;30(4):1459–1473. doi:10.1017/S0954579417001699
34. Mizuta A, Noda T, Nakamura M, Tatsumi A, Ojima T. Class average score for teacher support and relief of depression in adolescents: a population study in Japan. J Sch Health. 2016;86(3):173–180. doi:10.1111/josh.12365
35. Hussong AM, Ennett ST, Cox MJ, Haroon M. A systematic review of the unique prospective association of negative affect symptoms and adolescent substance use controlling for externalizing symptoms. Psychol Addict Behav. 2017;31(2):137–147. doi:10.1037/adb0000247
36. Anderson SF, Sladek MR, Doane LD. Negative affect reactivity to stress and internalizing symptoms over the transition to college for Latinx adolescents: buffering role of family support. Dev Psychopathol. 2020;1–16. doi:10.1017/s095457942000053x
37. Takizawa T, Kondo T, Sakihara S, Ariizumi M, Watanabe N, Oyama H. Stress buffering effects of social support on depressive symptoms in middle age: reciprocity and community mental health. Psychiatry Clin Neurosci. 2006;60(6):652–661. doi:10.1111/j.1440-1819.2006.01579.x
38. Xu H, Liu X, Zeng P. The mediating role of social support in the relationship between psychological capital and depression among Chinese emergency physicians. Psychol Res Behav Manag. 2022;15:977–990. doi:10.2147/prbm.S360611
39. Gariépy G, Honkaniemi H, Quesnel-Vallée A. Social support and protection from depression: systematic review of current findings in Western countries. Br J Psychiatry. 2016;209(4):284–293. doi:10.1192/bjp.bp.115.169094
40. Tengku Mohd TAM, Yunus RM, Hairi F, Hairi NN, Choo WY. Social support and depression among community dwelling older adults in Asia: a systematic review. BMJ Open. 2019;9(7):e026667. doi:10.1136/bmjopen-2018-026667
41. Pössel P, Burton SM, Cauley B, Sawyer MG, Spence SH, Sheffield J. Associations between social support from family, friends, and teachers and depressive symptoms in adolescents. J Youth Adolesc. 2018;47(2):398–412. doi:10.1007/s10964-017-0712-6
42. Hersh J, Curry JF, Kaminer Y. What is the impact of comorbid depression on adolescent substance abuse treatment? Subst Abus. 2014;35(4):364–375. doi:10.1080/08897077.2014.956164
43. Wang PW, Lin HC, Yeh YC, Liu TL, Yen CF. The relation of substance use with different levels of depressive symptoms and the moderating effect of sex and age in Taiwanese adolescents. Compr Psychiatry. 2012;53(7):1013–1020. doi:10.1016/j.comppsych.2012.02.010
44. McGuinness TM, Dyer JG, Wade EH, McGuinness TM. Gender differences in adolescent depression. J Psychosoc Nurs Ment Health Serv. 2012;50(12):17–20. doi:10.3928/02793695-20121107-04
45. Kelly KM, Malecki CK. Social support, depression, and anxiety in female adolescents: associations and profiles. Child & Youth Care Forum. 2022;51(1):85–109. doi:10.1007/s10566-021-09617-1
46. Regan T, Harris B, Fields SA. Are relationships between impulsivity and depressive symptoms in adolescents sex-dependent? Heliyon. 2019;5(10):e02696. doi:10.1016/j.heliyon.2019.e02696
47. Tsai FJ, Huang YH, Liu HC, Huang KY, Huang YH, Liu SI. Patient health questionnaire for school-based depression screening among Chinese adolescents. Pediatrics. 2014;133(2):e402–9. doi:10.1542/peds.2013-0204
48. Li CS, Chen SH. Obsessive-compulsiveness and impulsivity in a non-clinical population of adolescent males and females. Psychiatry Res. 2007;149(1–3):129–138. doi:10.1016/j.psychres.2006.05.001
49. Rosenberg M, Malabar K. Conceiving the Self. New York: Basic Books; 1986.
50. Wu SI, Huang HC, Liu SI, et al. Validation and comparison of alcohol-screening instruments for identifying hazardous drinking in hospitalized patients in Taiwan. Alcohol Alcohol. 2008;43(5):577–582. doi:10.1093/alcalc/agn036
51. Neuling SJ, Winefield HR. Social support and recovery after surgery for breast cancer: frequency and correlates of supportive behaviours by family, friends and surgeon. Soc Sci Med. 1988;27(4):385–392. doi:10.1016/0277-9536(88)90273-0
52. Winefield HR, Winefield AH, Tiggemann M. Social support and psychological well-being in young adults: the multi-dimensional support scale. J Pers Assess. 1992;58(1):198–210. doi:10.1207/s15327752jpa5801_17
53. Patton JH, Stanford MS, Barratt ES. Factor structure of the Barratt impulsiveness scale. J Clin Psychol. 1995;51(6):768–774. doi:10.1002/1097-4679(199511)51:6
54. Lo MT, Chen SK, O’Connell AA. Psychometric properties and convergent validity of the Chinese version of the Rosenberg self-esteem scale. J Appl Meas. 2018;19(4):413–427.
55. Lin RC. Reliability and validity of the Rosenberg self-esteem scale on Chinese children. Natl Chung Cheng Univ. 1990;1:29–46.
56. Stanford MS, Mathias CW, Dougherty DM, Lake SL, Anderson NE, Patton JH. Fifty years of the Barratt impulsiveness scale: an update and review. Person Indiv Differ. 2009;47(5):385–395. doi:10.1016/j.paid.2009.04.008
57. Naninck EF, Lucassen PJ, Bakker J. Sex differences in adolescent depression: do sex hormones determine vulnerability? J Neuroendocrinol. 2011;23(5):383–392. doi:10.1111/j.1365-2826.2011.02125.x
58. Abela JR, D’Alessandro DU. Beck’s cognitive theory of depression: a test of the diathesis-stress and causal mediation components. Br J Clin Psychol. 2002;41(Pt 2):111–128. doi:10.1348/014466502163912
59. Leung CY, Leung GM, Schooling CM. Behavioral problem trajectories and self-esteem changes in relation with adolescent depressive symptoms: a longitudinal study. Soc Psychiatry Psychiatr Epidemiol. 2018;53(7):673–684. doi:10.1007/s00127-018-1508-z
60. Chang HJ, Lin MF, Lin KC. The mediating and moderating roles of the cognitive triad on adolescent suicidal ideation. Nurs Res. 2007;56(4):252–259. doi:10.1097/01.NNR.0000280611.00997.0e
61. Martel MM, Levinson CA, Lee CA, Smith TE. Impulsivity symptoms as core to the developmental externalizing spectrum. J Abnorm Child Psychol. 2017;45(1):83–90. doi:10.1007/s10802-016-0148-6
62. Zisner A, Beauchaine TP. Neural substrates of trait impulsivity, anhedonia, and irritability: mechanisms of heterotypic comorbidity between externalizing disorders and unipolar depression. Dev Psychopathol. 2016;28(4pt1):1177–1208. doi:10.1017/s0954579416000754
63. Johnson SL, Tharp JA, Peckham AD, Carver CS, Haase CM. A path model of different forms of impulsivity with externalizing and internalizing psychopathology: towards greater specificity. Br J Clin Psychol. 2017;56(3):235–252. doi:10.1111/bjc.12135
64. Riley AL, Hempel BJ, Clasen MM. Sex as a biological variable: drug use and abuse. Physiol Behav. 2018;187:79–96. doi:10.1016/j.physbeh.2017.10.005
65. Bobzean SA, DeNobrega AK, Perrotti LI. Sex differences in the neurobiology of drug addiction. Exp Neurol. 2014;259:64–74. doi:10.1016/j.expneurol.2014.01.022
66. Becker JB, McClellan ML, Reed BG. Sex differences, gender and addiction. J Neurosci Res. 2017;95(1–2):136–147. doi:10.1002/jnr.23963
67. Lam TH, Stewart SM, Ho SY, et al. Depressive symptoms and smoking among Hong Kong Chinese adolescents. Addiction. 2005;100(7):1003–1011. doi:10.1111/j.1360-0443.2005.01092.x
68. Wong DC, Chan SS, Lam TH. Depressive symptoms delayed quit attempts and shortened abstinence in young smokers of the hong kong youth quitline. Nicotine Tob Res. 2016;18(3):251–258. doi:10.1093/ntr/ntv065
69. Boden JM, Fergusson DM. Alcohol and depression. Addiction. 2011;106(5):906–914. doi:10.1111/j.1360-0443.2010.03351.x
70. Danzo S, Connell AM, Stormshak EA. Associations between alcohol-use and depression symptoms in adolescence: examining gender differences and pathways over time. J Adolesc. 2017;56:64–74. doi:10.1016/j.adolescence.2017.01.007
71. Bos J, Hayden MJ, Lum JAG, Staiger PK. UPPS-P impulsive personality traits and adolescent cigarette smoking: a meta-analysis. Drug Alcohol Depend. 2019;197:335–343. doi:10.1016/j.drugalcdep.2019.01.018
72. Felton JW, Shadur JM, Havewala M, Gonçalves S, Lejuez CW. Impulsivity moderates the relation between depressive symptoms and substance use across adolescence. J Clin Child Adolesc Psychol. 2020;49(3):365–377. doi:10.1080/15374416.2018.1537189
73. Felton JW, Shadur JM, Havewala M, Goncalves S, Lejuez CW. Impulsivity moderates the relation between depressive symptoms and substance use across adolescence. J Clin Child Adolesc Psychol. 2019;1–13. doi:10.1080/15374416.2018.1537189
74. Marsiglia FF, Yabiku ST, Kulis S, Nieri T, Parsai M, Becerra D. The influence of linguistic acculturation and gender on the initiation of substance use among Mexican heritage preadolescents in the borderlands. J Early Adolesc. 2011;31(2):271–299. doi:10.1177/0272431610363157
75. Soto C, Unger JB, Ritt-Olson A, Soto DW, Black DS, Baezconde-Garbanati L. Cultural values associated with substance use among Hispanic adolescents in Southern California. Subst Use Misuse. 2011;46(10):1223–1233. doi:10.3109/10826084.2011.567366
76. Newman BM, Newman PR, Griffen S, O’Connor K, Spas J. The relationship of social support to depressive symptoms during the transition to high school. Adolescence. 2007;42(167):441–459.
77. Barrera M, Garrison-Jones C. Family and peer social support as specific correlates of adolescent depressive symptoms. J Abnorm Child Psychol. 1992;20(1):1–16. doi:10.1007/bf00927113
78. Finan LJ, Ohannessian CM, Gordon MS. Trajectories of depressive symptoms from adolescence to emerging adulthood: the influence of parents, peers, and siblings. Dev Psychol. 2018;54(8):1555–1567. doi:10.1037/dev0000543
79. Mizuta A, Suzuki K, Yamagata Z, Ojima T. Teachers’ support and depression among Japanese adolescents: a multilevel analysis. Soc Psychiatry Psychiatr Epidemiol. 2017;52(2):211–219. doi:10.1007/s00127-016-1320-6
80. Inagaki TK, Ross LP. Neural correlates of giving social support: differences between giving targeted versus untargeted support. Psychosom Med. 2018;80(8):724–732. doi:10.1097/psy.0000000000000623
81. Kraus J, Roman R, Jurkovičová L, et al. Social support modulates subjective and neural responses to sad mental imagery. Behav. Brain Res. 2020;380:112433. doi:10.1016/j.bbr.2019.112433
82. Kawamichi H, Sugawara SK, Hamano YH, et al. Being in a romantic relationship is associated with reduced gray matter density in striatum and increased subjective happiness. Front Psychol. 2016;7:1763. doi:10.3389/fpsyg.2016.01763
83. Schreuders E, Braams BR, Blankenstein NE, Peper JS, Güroğlu B, Crone EA. Contributions of reward sensitivity to ventral striatum activity across adolescence and early adulthood. Child Dev. 2018;89(3):797–810. doi:10.1111/cdev.13056
84. Cheung AH, Cook S, Kozloff N, Chee JN, Mann RE, Boak A. Substance use and internalizing symptoms among high school students and access to health care services: results from a population-based study. Can J Public Health. 2019;110(1):85–92. doi:10.17269/s41997-018-0144-4
85. Brener ND, Billy JO, Grady WR. Assessment of factors affecting the validity of self-reported health-risk behavior among adolescents: evidence from the scientific literature. J Adolesc Health. 2003;33(6):436–457. doi:10.1016/s1054-139x(03)00052-1
86. Deighton J, Tymms P, Vostanis P, et al. The development of a school-based measure of child mental health. J Psychoeduc Assess. 2013;31(3):247–257. doi:10.1177/0734282912465570
87. Schepis TS, Teter CJ, McCabe SE. Prescription drug use, misuse and related substance use disorder symptoms vary by educational status and attainment in U.S. adolescents and young adults. Drug Alcohol Depend. 2018;189:172–177. doi:10.1016/j.drugalcdep.2018.05.017
88. Townsend L, Flisher AJ, King G. A systematic review of the relationship between high school dropout and substance use. Clin Child Fam Psychol Rev. 2007;10(4):295–317. doi:10.1007/s10567-007-0023-7
89. Morales-Vives F, Duenas JM. Predicting suicidal ideation in adolescent boys and girls: the role of psychological maturity, personality traits, depression and life satisfaction. Span J Psychol. 2018;
90. Hankin BL, Abramson LY. Development of gender differences in depression: description and possible explanations. Ann Med. 1999;31(6):372–379. doi:10.3109/07853899908998794
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Resilience and Depressive Symptoms Mediated Pathways from Social Support to Suicidal Ideation Among Undergraduates During the COVID-19 Campus Lockdown in China
Zhang X, Liu X, Mi Y, Wang W, Xu H
Psychology Research and Behavior Management 2022, 15:2291-2301
Published Date: 23 August 2022
Factors Predicting Mental Health Among Women in Low-Income Communities of a Changing Society: A Mixed-Methods Study
Roberts LR, Sadan V, Siva R, Sathiyaseelan M, Rosalind SE, Suresh P, Montgomery SB
International Journal of Women's Health 2023, 15:381-394
Published Date: 16 March 2023
The Effects of Cognitive Fusion on Depression in Primary School Principals During the COVID-19 Pandemic: The Mediating Role of Psychological Vulnerability and the Moderating Role of Self-Esteem
Lv J, Qiu Q, Ye B, Yang Q
Psychology Research and Behavior Management 2023, 16:1727-1739
Published Date: 8 May 2023
The Interconnection Between Social Support and Emotional Distress Among Individuals with Chronic Pain: A Narrative Review
Franqueiro AR, Yoon J, Crago MA, Curiel M, Wilson JM
Psychology Research and Behavior Management 2023, 16:4389-4399
Published Date: 27 October 2023
A Pilot Study of Symptoms of Major Depressive Disorder in Medical Students at an Osteopathic Medical School Before and After High-Stakes Examinations
Arabatzis TJ, Doroshenko J, Ashraf MA, Smith RM
Advances in Medical Education and Practice 2023, 14:1259-1271
Published Date: 9 November 2023