Back to Journals » Risk Management and Healthcare Policy » Volume 14
How Has the COVID-19 Pandemic Changed BMI Status and Physical Activity – Its Associations with Mental Health Conditions, Suicidality: An Exploratory Study
Authors Auny FM, Akter T ![]() , Guo T, Mamun MA
, Guo T, Mamun MA ![]()
Received 26 February 2021
Accepted for publication 24 May 2021
Published 18 June 2021 Volume 2021:14 Pages 2527—2536
DOI https://doi.org/10.2147/RMHP.S308691
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Farzana Mahzabin Auny,1,2,* Tahmina Akter,1,3,* Tianyou Guo,4 Mohammed A Mamun1,5
1CHINTA Research Bangladesh, (Centre for Health Innovation, Networking, Training, Action and Research – Bangladesh), Savar, Dhaka, 1342, Bangladesh; 2Department of Public Health, Global Communicable Disease, University of South Florida, Tampa, USA; 3Department of Epidemiology, Bangladesh University of Health Sciences, Dhaka, Bangladesh; 4Exercise Psychophysiology Laboratory, Institute of KEEP Collaborative Innovation, School of Psychology, Shenzhen University, Shenzhen, Guangdong Province, 518060, People’s Republic of China; 5Department of Public Health and Informatics, Jahangirnagar University, Savar, Dhaka, 1342, Bangladesh
*These authors contributed equally to this work
Correspondence: Tianyou Guo
Exercise Psychophysiology Laboratory, Institute of KEEP Collaborative Innovation, School of Psychology, Shenzhen University, Shenzhen, Guangdong Province, 518060, People’s Republic of China
Email [email protected]
Mohammed A Mamun
Director, CHINTA Research Bangladesh, Savar, Dhaka, 1342, Bangladesh
Tel +88-1738592653
Email [email protected]
Background: The COVID-19 pandemic has psycho-socially impacted people of all age groups. The consequences related to this crisis may increase the suicide mortality rate as reported in prior pandemics. Although many studies have been conducted identifying suicidal behavior attributing factors, there is a lack of knowledge on the associations of body mass index (BMI) and physical activities, their changes, and suicidal behavior, which were explored herein for the first time.
Methods: An online-based, cross-sectional study was carried out with a total of 324 Bangladeshi people (mean age = 26.99 ± 8.17 years). The measures included questions on socio-demographics, health-related variables, physical activities-related variables, and mental health problems (eg, depression, anxiety and suicidal behavior).
Results: About 41.0% and 29.3% of the participants reported being depressed and anxious, respectively, whereas suicidal behavior after the pandemic’s inception was found to be 6.5%. Although the role of BMI status either prior to or during the pandemic in mental health conditions was not statistically significant, the changes of BMI status were (that is, those with decreasing BMI status compared to no change in BMI status were at greater risk of depression and anxiety, which was followed by increasing BMI status). Besides having no outside space for exercise and performing more physical activities prior to the pandemic were reported to increase anxiety levels, but no significant associations between changes in physical exercise frequency and other mental health problems were observed.
Conclusion: In summary, the present findings showed that people with either decreased or increased BMI status after the inception of the pandemic were at greater risk of mental instabilities, which is a concern which should be considered when adopting any preventive approaches.
Keywords: anxiety, body mass index, COVID-19, depression, pandemic and mental health, physical activities, psychological impact, suicidal behavior, suicide in Bangladesh
Introduction
The ongoing COVID-19 pandemic has already disrupted people’s quality of life.1–4 The outbreak originated from Wuhan, China, one year ago; still, it is not controlled. As all of the countries were attacked by the virus, people were at higher risk of being infected except those following preventive measures.5 In this regard, the Government of Bangladesh, and likely other countries, imposed lockdown and suggested necessary preventive measures to mitigate social interaction to suppress the disease transmission.6 But, the expeditiously spreading and highly deadly nature of the virus has significantly impacted people’s mental health due to social isolation, fear of an epidemic, financial strain, uncertainty about the future etc., as consequences of lockdown related confinement.7,8 Studies conducted across the world suggest increased mental health effects such as depression, anxiety, mood disturbances, post-traumatic stress, sleep problems, paranoia, low self-esteem, loss of self-control, and so forth in both people infected with the virus or not.7–9 Besides, other outbreak-related psychosocial effects, including fear of death, solitude or loneliness, boredom, distress, social alienation or contagion, also contribute to long-term psychiatric suffering as well as thoughts of suicide.7 During and after prior outbreaks, suicidality rates unexpectedly increased; for instance, Cheung et al10 observed elderly suicide mortality increment in Hong Kong as an effect of the 2003 SARS pandemic. In the COVID-19 pandemic context, a similar assertion has already been established.11–14
Several studies based on media reports rapidly assessed the nature and reasons of suicide related to COVID-19. For example, Dsouza et al5 and Mamun et al15 investigated the suicide case of Indian people in general and celebrities, respectively; in the same manner, Bangladeshi,16,17 Pakistani,18 even global19,20 suicide cases were assessed. But, limited studies investigating suicidal behavior related to COVID-19 have been conducted throughout the world. For instance, 17.5% and 4.9% suicidal ideation and attempted suicide rates, respectively, were reported in the US based on a survey conducted within the first week of April 2020,21 whereas another US study conducted in June 24–30, 2020, claimed that 10.7% of the participants seriously considered thinking for suicide in the past 30 days.22 Similarly, 18% and 5% of the UK participants reported experiencing suicide (or self-harm) thoughts and attempts, respectively, within the first month of lockdown.23 About 7.6% of Colombian people had high suicide risk (assessing the four items CES-D-IS (9/12 cutoff point)).24 However, two Bangladeshi studies assessing suicidal behavior reported the prevalence rate as 5% to 6.1%,25,26 to the best of our knowledge.25,26
The risk factors and/or reasons of COVID-19-related suicidal behaviors were also investigated. For instance, high perceived stress related to COVID-19, risk of depressive episode, and insomnia were reported as risk factors of higher suicide risk in Columbia;24 similar findings were reported by Killgore et al.27 Whereas female gender, Black, Asian and minority ethnic groups, economic disadvantage, unemployment, disability, chronic physical illnesses, psychiatric disorders and being COVID-19 positive were the risk factors.23 In Bangladesh, being female, young, divorced, having no children, cigarette smoker, and having comorbid diseases, higher fear related to COVID-19, and insomnia were observed as risk predictors for suicidality.25,26
Evidence suggests a positive relationship between BMI increment and psychiatric conditions such as depression, anxiety, mania, panic attacks, social phobia, suicidal ideation etc.28 Similarly, during the COVID-19 pandemic-related lockdown, people were confined which leads to performing less physical activities, which has been reported to increase their psychological burden.29–32 Moderate to regular frequency physical exercises result in immune‐modulatory effects, which instigate multi-step processes in the organ system to boost up the immune system and provide an anti-inflammatory response. Thus, less physical activities resulted because of long-term confinement related to the COVID-19 pandemic, worsening mood profiles and increasing psychological impact.33 Vice-versa COVID-19 related mental health problems also negatively impact behavioral intention of performing regular physical activities.34 More specifically, individuals with a higher BMI had increased perceived burdensomeness, which is the pathway of suicide completion.34 A systematic review and meta-analysis claimed that being less physically active was associated with higher suicidality.35 But, there has been no study in Bangladesh investigating the associations of body mass index (BMI) and physical activities, their changes, and suicidal behavior, which was explored herein for the first time in the COVID-19 pandemic context.
Methods
Study Procedure, Participants, and Ethics
An online-based cross-sectional study was conducted among the general Bangladeshi people utilizing a structured questionnaire. Participants were surveyed in the month of November 2020; a total of 326 people participated, and after omission of incomplete questionnaires, 324 samples were finally analyzed (mean age = 26.99 ± 8.17 years). The study followed the highest degree of ethical standards. The study protocol was initially reviewed and supported by the CHINTA Research Bangladesh. To oversee the project, an external ethics board approval was granted by the Institute of Allergy and Clinical Immunology of Bangladesh (Reference number: IRBIACIB/CEC/03202028/653). In addition, before partaking in the online survey, along with mandatorily providing informed consent, the participants were informed about ethical aspects as suggested by the Helsinki Declaration, 2013.
Measures
The survey questionnaire included questions regarding socio-demographics, health-related variables, physical activities-related variables, and mental health problems (eg, depression, anxiety and suicidal behavior). A short description of the studied variables is given in the following paragraphs.
Sociodemographic Factors
The basic socio-demographic information including gender, age, current residence (eg, village, Upazila [sub-city], or district [city]), type of house (eg, lower, middle or high quality) and occupation (eg, student, service holder, health care professional, businessman, engineer, housewife, other) were asked in the survey.
Health-Related Measures
A dichotomous response (ie, yes/no) was used to assess if the participants tested positive for COVID-19. Besides, a 4-point Likert scale (never to always) concerning experiencing COVID-19 like symptoms was also assessed. Self-reported anthropometric measurement relating to body mass index (BMI) was collected based on prior to and during the COVID-19 pandemic, where before and 6 months after the outbreak were considered for reporting weight and height. Lastly, the changes in BMI status after the lockdown were calculated in considering the anthropometric measurement changes prior to the pandemic.
Physical Activity-Related Variables
First of all, having (or not having) outdoor space for performing physical activities near the participants’ residence was asked. The status of performing physical activities [ie, engaging in cricket, football, fitness exercise, etc., for at least 30 minutes once a day36] was asked based on prior to and during the COVID-19 period. Physical activity frequency of a week was also investigated herein, similar to Maugeri et al.31 Lastly, the changes in physical exercise status after the lockdown were calculated compared to physical exercise prior to the pandemic.
Depression
For assessing depression, the Patient Health Questionnaire (PHQ-2) scale was used.37,38 The scale consists of two items (eg, “little interest or pleasure in doing things” and “feeling down, depressed, or hopeless”), and participants were supposed to respond on a 4-point Likert scale (0= not at all to 3=nearly every day). The total score ranges from 0 to 6, and a score of ≥ 3 is considered as the presence of depression.37,38 The Cronbach’s alpha was 0.76.
Anxiety
For assessing anxiety, the Generalized Anxiety Disorder (GAD-2) scale was used.37,39 The scale consists of two items (eg, “feeling nervous, anxious or on edge” and “not being able to stop or control worrying”), and participants were supposed to respond on a 4-point Likert scale (0= not at all to 3=nearly every day). The total score ranges from 0 to 6, and a score of ≥ 3 is considered as the presence of anxiety.37,39 The Cronbach’s alpha was 0.76.
Suicidal Behavior
For assessing suicidal behaviors, the prior studies conducted either prior to or during the COVID-19 periods were followed.21,22,40,41 Consistent with the concept of suicidal behavior (ie, thinking about ending your life, making a plan to go ahead with it, and attempting to end your life42), the present study used a single-item for assessing suicidal behavior. Which was, “do you think about committing suicide, and are these thoughts persistent and have you moved forward to plan and/or attempt it?”.25,26 For assessing suicidal behavior history, one year before the inception of the pandemic was considered, whereas the current suicidal behavior was evaluated considering the pandemic’s inception to survey time.
Statistical Analysis
Initially, collected data from the Google Forms were entered into Microsoft Excel 2019 and were cleaned and prepared for formal analysis in IBM SPSS Statistics. Frequencies, percentages, ANOVA tests, and chi-squared tests were performed investigating relationships with the outcome variables. Depression, anxiety, and current suicidal behavior were considered the outcome variables in the present study. However, a value of p< 0.05 was set as statistically significant with 95% confidence interval for the tests.
Results
Characteristics of the Participants
Of the total sample (N=324), the majority of the participants were male (65.7%) and young adults (38.6%). Over half of them were students (53.4%) and lived in a high-quality house (58.3%) and district area (50%) (Table 1). About 62.3% reported experiencing COVID-19 like symptoms, but only 7.4% tested positive for the virus. Nearly half of the participants (ie, 49.1%) reported an increment in their BMI status during the COVID-19 period, whereas 31.8% reported decreasing of it (Table 2). Correspondingly, about 44.1% reported no changes in their weekly frequency of performing physical activities, whereas a 38.9% reduction was found (Table 3).
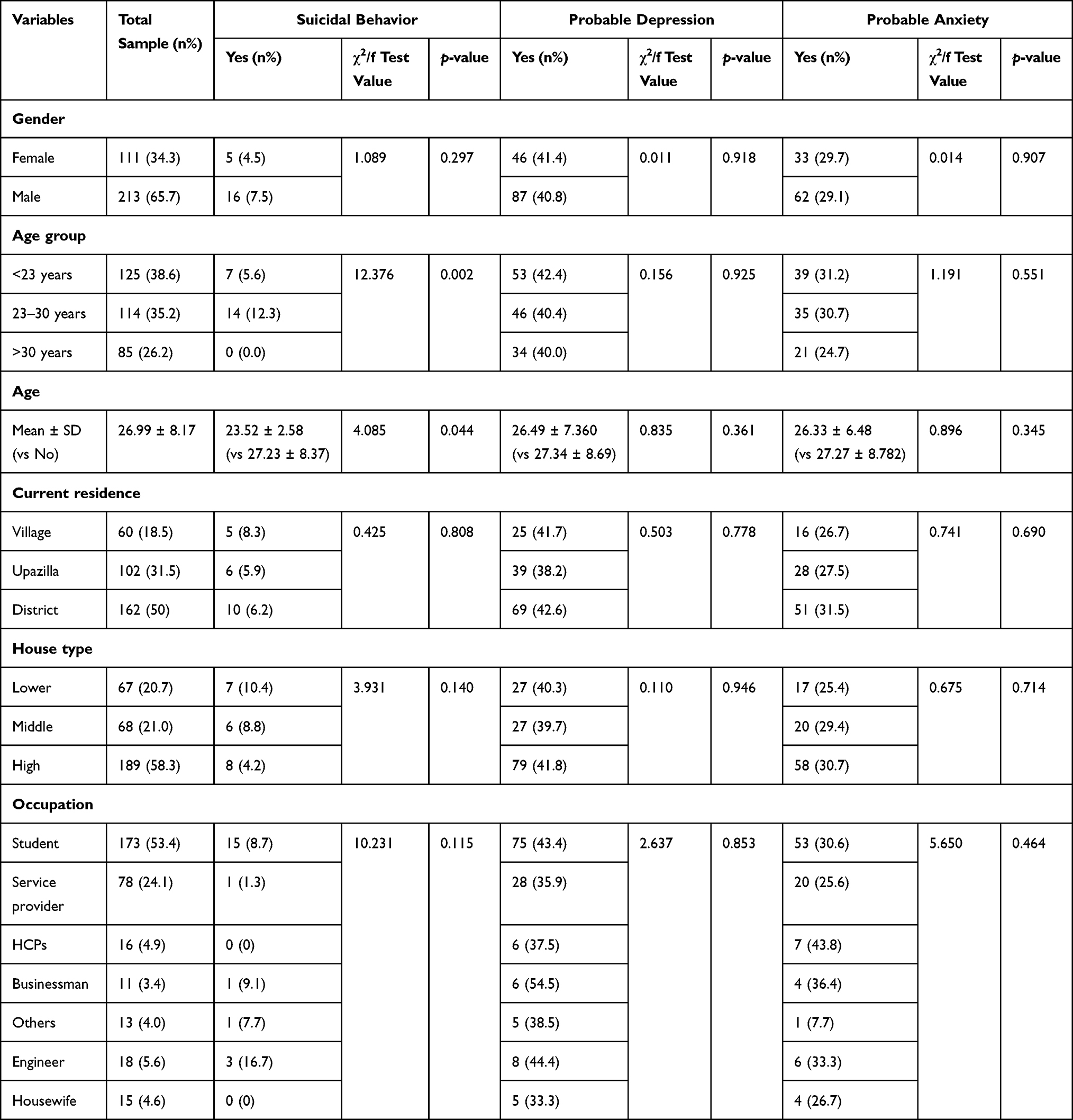 |
Table 1 Associations Between the Socio-Demographic Variables and Mental Health Problems |
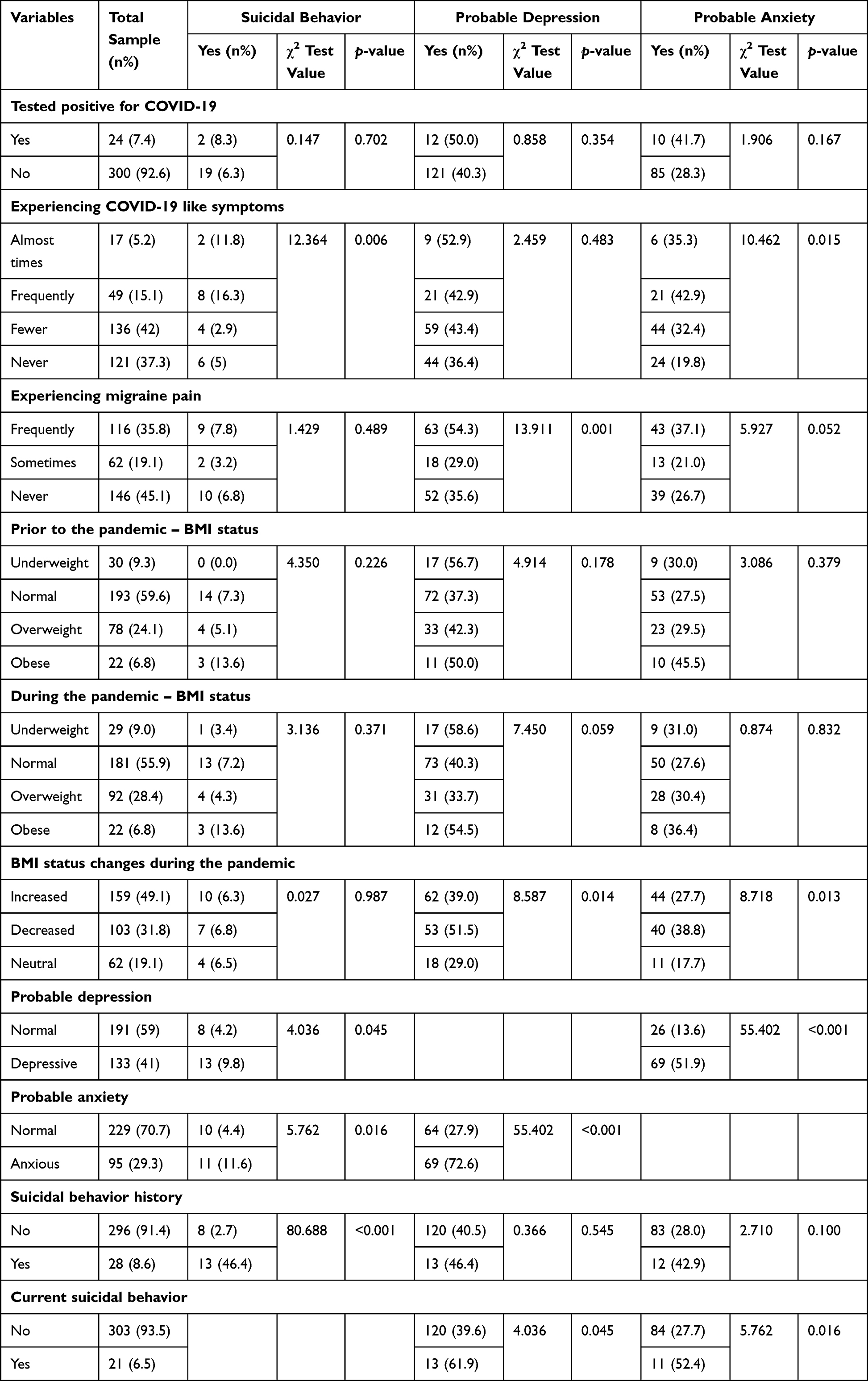 |
Table 2 Associations Between the Health-Related Variables and Mental Health Problems |
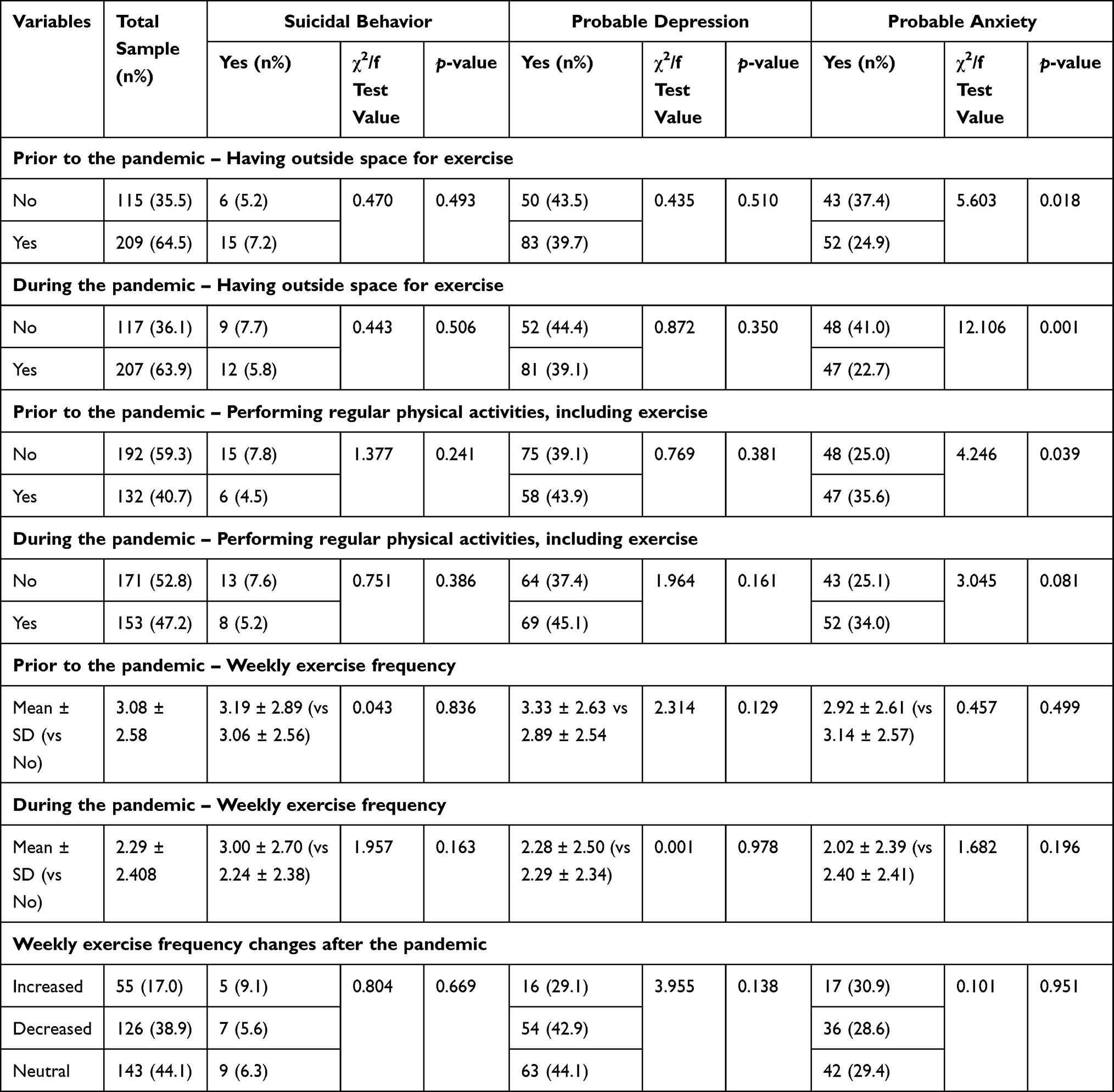 |
Table 3 Associations Between the Physical Activity-Related Variables and Mental Health Problems |
Prevalence of Mental Health Problems
About 41.0% and 29.3% of the participants reported being depressed and anxious, respectively, whereas only 6.5% were found to have suicidal behavior after the pandemic inception (Figure 1).
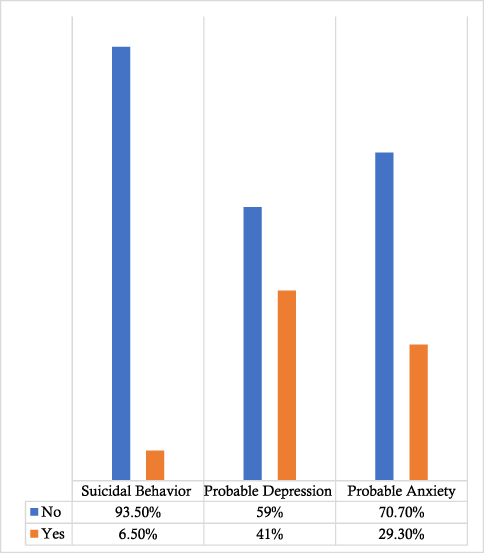 |
Figure 1 Prevalence of mental health problems. |
Associations Between the Studied Variables and Mental Health Problems
The role of socio-demographics (except age) was not significantly associated with any of the mental health conditions. Similarly, there was no significant relationship between the participants being infected with COVID-19 and mental suffering; but, experiencing more COVID-19-like symptoms was significantly responsible for increasing suicidal behavior and anxiety rates (ie, χ2=12.364, p=0.006; and χ2=10.462, p=0.015; respectively). In addition, participants experiencing migraine pain had significantly increased the risk of mental health problems. But, the associations were heterogeneously distributed; that is, participants suffering from moderate migraine pain had a lower tendency of being depressed and anxious (ie, χ2=13.911, p<0.001; and χ2=5.927, p=0.052; respectively) (Table 2).
There was no significant role of BMI status, either prior to or during the pandemic, in mental health conditions, but the changes of BMI status were significantly associated with depression and anxiety (ie, χ2=8.587, p=0.014; and χ2=8.718, p=0.013; respectively). That is, participants reporting decreasing BMI status (compared to no changes of BMI status) were at greater risk of depression and anxiety, which was followed by increasing BMI status (Table 2). Besides, having no outside space for exercise, performing more physical activities was reported to be associated with rising anxiety prevalence rates (Table 3). In addition, there were significant positive relationships between depression, anxiety, and suicidal behavior; that is, participants suffering from depression and anxiety were at a higher risk of suicidality. But, the suicidal behavior history was not associated with any of the outcome variables (ie, current suicidal behavior, depression, and anxiety) (Table 2).
Discussion
The COVID-19-related lockdown and preventive measures taken to control disease transmission have undoubtedly disrupted people’s quality of life. Evidence suggests that preventative measures like social movement restriction, being isolated or quarantined etc., have a negative impact on mental health.7,8 For instance, many of the quarantined people during the SARS outbreak period in 2003 did not think that they should have been placed into quarantine,43 which reflects the fact that people are at greater risk of mental and emotional instabilities due to confinement. Besides, there is an excellent effect on the economy – leading to people losing their jobs, along with other stressors such as fear of being infected, experiencing more deaths, the uncertainty of essential supplies (eg, food, water, clothes etc.), inadequate information and misinformation, and stigma etc., all exacerbate mental suffering.7,8
About 6.5% of the present respondents reported suicidal behavior after the inception of the COVID-19 pandemic in Bangladesh, which is remarkably similar to the prior studies. More specifically, the first-ever Bangladeshi study assessing COVID-19 suicidal behavior reported the rate as 5% from a survey study conducted between 1 and 10 April 2020.26 After that study (8 to 25 April 2020), the prevalence rate was reported as 6.1% in a comparative study among the general population and healthcare professionals.25 Although these three studies shared the same method for assessing suicidal behavior, time exposure for considering the suicidal behavior’s prevalence rate was somewhat different. Along with the time exposure, experiencing more lockdown-related obstructions was anticipated to increase the present study’s suicidal behavior rate, but no detectable increment was found herein.
About 41.0% and 29.3% of the present participants reported experiencing symptoms of depression and anxiety, respectively. Considering the COVID-19-related psychiatric epidemiological studies of South Asian countries (including Bangladesh), a recent systematic review pooled the prevalence rates of depression and anxiety and found them to be 34.1% (28.9–39.4%) and 41.3% (34.7 – 48.1%) respectively.44 The same study also observed that Bangladeshi people were the most psychologically vulnerable within this subcontinent. That is, the pooled prevalence rates for depression and anxiety were reported to be 48.2% (34.8 – 61.8%) and 52.3% (41 – 63.6%), respectively.44 Although the present study rates seemed lower than the pooled rates, many people were still suffering from mental health problems.
People are facing an unprecedented, life-altering crisis as a result of the COVID-19 pandemic. Steps such as 'social distancing' and 'shelter in place' are expected to act as a new normal yet to come.5 To take attention away from all negative feelings (eg, fatigue, boredom etc.), people may start unhealthy dietary habits (eg, emotional eating habits, disordered eating etc.), especially those who have high objective self-consciousness,45 resulting in a large effect on diet patterns and quality of food, and increased weight gain during the lockdown period.46,47 Overweight or obesity can be a risk factor for poor mental health, which can also cause higher suicidality rate.48 During the COVID-19 pandemic, 49% of the present sample reported increased BMI status, whereas 31.8% reported a decrease. There were significant associations between the changes in BMI status and mental health. The participants reporting changes in their BMI status were more significantly prone to suffer from depression and anxiety (where BMI status decreasing was at higher risk), although suicidality was not associated with it. As aforementioned, the BMI status changes lead to suffering from more psychiatric conditions, with the mediation of perceived feelings of burdensomeness,28,34 which can be a red-flag sign for mental health vulnerabilities.
Regular physical activity and exercise which cause sweat production mediate the release of hormones (eg, endorphins, serotonin, norepinephrine, etc.) and helps with relaxation.36,49 Thus, following the benefits of physical activities are limited to physical health and help reduce mental and emotional suffering.50 More specifically, individuals performing more than 5 hours physical activity a week were reported to be 60% less likely to suffer from depression compared to those who performed 2 h, as reported in a recent study.51 In contrast, performing fewer physical activities are alleged to be associated with higher suicidal risk.35 However, the present finding supported that being more active in performing physical activities leads to higher anxiety, but this had no significant role in relation to either depression or suicidal behavior. Besides, the present study observed changes in engagement with physical activities during the COVID-19 pandemic compared to before the pandemic, but no significant role in relation to either decrease or increase in physical activities and mental health conditions was found. In contrast to the present finding, an Italian study conducted during the pandemic reported a decreased tendency of physical activities, which had a profoundly negative impact on psychological wellbeing.31 Perceptibly, there is no explanation for such a finding reported herein, which is subjected to further studies.
The findings from the present study may be limited by their nature (cross-sectional study), sampling technique (convenience), sample size (small), and response-related probable errors (recall bias). Besides, being the study nature exploratory, the psychosocial antecedents are not properly framed in a proper theoretical ground, which may evaluate mental states’ effects on a putative psychosocial model. Therefore, further studies considering more rigorous methodologies (eg, longitudinal study) with representative samples are required to generalize the findings.
Conclusion
This study’s findings emphasize how important the role of physical activity and normal BMI status is to minimize the COVID-19-related psychological burden and suicidal behavior. As an exploratory study investigating the role of BMI status and physical activities, and their changes in psychological health, the findings may help facilitate further studies and help policy-makers establish appropriate strategies.
Acknowledgments
The authors would also like to mention that the project was run by the CHINTA Research Bangladesh, which was formerly known as the Undergraduate Research Organization. Besides, the authors would like to thank Professor Dr. Pradip Sen Gupta, Head of the Department of Epidemiology, Bangladesh University of Health Sciences, for his enormous support throughout the project. In addition, Mahmudul Hasan's efforts in cross-checking the analysis during the article production time, is highly appreciated.
Funding
Dr. Tianyou Guo has to acknowledge the funding support that they receive: Attentional Bias Characteristics and Eye Movement Desensitization Intervention of PTSD (NSF:31871115).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Samlani Z, Lemfadli Y, Ait Errami A, Oubaha S, Krati K. The impact of the COVID-19 pandemic on quality of life and well-being in Morocco. Arch Commun Med Public Heal. 2020;130–134. doi:10.17352/2455-5479.000091
2. Algahtani FD, Hassan SUN, Alsaif B, Zrieq R. Assessment of the quality of life during covid-19 pandemic: a cross-sectional survey from the kingdom of saudi arabia. Int J Environ Res Public Health. 2021;18(3):1–12. doi:10.3390/ijerph18030847
3. Islam MZ, Khoorshid Riaz B, Sumaiya Efa S, Farjana S, Mahmood F. Health-related quality of life of adult COVID-19 patients following one-month illness experience since diagnosis: findings of a cross-sectional study in Bangladesh. medRxiv. 2021. doi:10.1101/2021.02.19.21252073
4. Bartels MMTJ, Gal R, van der Velden JM, Verhoeff JJC, Verlaan JJ, Verkooijen HM. Impact of the COVID-19 pandemic on quality of life and emotional wellbeing in patients with bone metastases treated with radiotherapy: a prospective cohort study. Clin Exp Metastasis. 2021;38(2):209–217. doi:10.1007/s10585-021-10079-x
5. Dsouza DD, Quadros S, Hyderabadwala ZJ, Mamun MA. Aggregated COVID-19 suicide incidences in India: fear of COVID-19 infection is the prominent causative factor. Psychiatry Res. 2020;290:e113145. doi:10.1016/j.psychres.2020.113145
6. Islam SMDU, Bodrud-Doza M, Khan RM, Haque MA, Mamun MA. Exploring COVID-19 stress and its factors in Bangladesh: a perception-based study. Heliyon. 2020;6(7):e04399. doi:10.1016/j.heliyon.2020.e04399
7. Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020;395(10227):912–920. doi:10.1016/S0140-6736(20)30460-8
8. Pedrosa AL, Bitencourt L, Fróes ACF, et al. Emotional, behavioral, and psychological impact of the COVID-19 pandemic. Front Psychol. 2020;11:2635. doi:10.3389/fpsyg.2020.566212
9. Hossain MM, Sultana A, Purohit N. Mental health outcomes of quarantine and isolation for infection prevention: a systematic umbrella Review of the Global Evidence. Epidemiol Health. 2020;42:e2020038. doi:10.4178/epih.e2020038
10. Cheung YT, Chau PH, Yip PSF. A revisit on older adults suicides and Severe Acute Respiratory Syndrome (SARS) epidemic in Hong Kong. Int J Geriatr Psychiatry. 2008;23(12):1231–1238. doi:10.1002/gps.2056
11. Hernández-Calle D, Martínez-Alés G, Mediavilla R, Aguirre P, Rodríguez-Vega B, Bravo-Ortiz MF. Trends in psychiatric emergency department visits due to suicidal ideation and suicide attempts during the COVID-19 pandemic in Madrid, Spain. J Clin Psychiatry. 2020;81(5). doi:10.4088/JCP.20l13419
12. Killgore WDS, Cloonan SA, Taylor EC, Allbright MC, Dailey NS. Trends in suicidal ideation over the first three months of COVID-19 lockdowns. Psychiatry Res. 2020;293:113390. doi:10.1016/j.psychres.2020.113390
13. Radeloff D, Papsdorf R, Uhlig K, Vasilache A, Putnam K, von Klitzing K. Trends in suicide rates during the COVID-19 pandemic restrictions in a major German city. Epidemiol Psychiatr Sci. 2021;e30:16. doi:10.1017/S2045796021000019
14. Soto-Sanz V, Falcó R, Piqueras JA. Socio-emotional strengths against psychopathology and suicidal ideation in fear of Covid-19. Res Sq. 2020. doi:10.21203/rs.3.rs-73382/v1
15. Mamun MA, Syed NK, Griffiths MD. Indian celebrity suicides before and during the COVID-19 pandemic and their associated risk factors: evidence from media reports. J Psychiatr Res. 2020;131:177–179. doi:10.1016/j.jpsychires.2020.09.002
16. Bhuiyan AKMI, Sakib N, Pakpour AH, Griffiths MD, Mamun MA. COVID-19-related suicides in Bangladesh due to lockdown and economic factors: case study evidence from media reports. Int J Ment Health Addict. 2020. doi:10.1007/s11469-020-00307-y
17. Mamun MA, Griffiths MD. First COVID-19 suicide case in Bangladesh due to fear of COVID-19 and xenophobia: possible suicide prevention strategies. Asian J Psychiatr. 2020;51:102073. doi:10.1016/j.ajp.2020.102073
18. Mamun MA, Ullah I. COVID-19 suicides in Pakistan, dying off not COVID-19 fear but poverty?–The forthcoming economic challenges for a developing country. Brain Behav Immun. 2020;87:163–166. doi:10.1016/j.bbi.2020.05.028
19. Griffiths MD, Mamun MA. COVID-19 suicidal behavior among couples and suicide pacts: case study evidence from press reports. Psychiatry Res. 2020;289:113105. doi:10.1016/j.psychres.2020.113105
20. Manzar MD, Albougami A, Usman N, Mamun MA. COVID-19 suicide among adolescents and youths during the lockdown: an exploratory study based on media reports. J Child Adolesc Psychiatr Nurs. 2021;34(2):139–146. doi:10.1111/jcap.12313
21. Ammerman BA, Burke TA, Jacobucci R, McClure K. Preliminary investigation of the association between COVID-19 and suicidal thoughts and behaviors in the US. J Psychiatr Res. 2021;134:32–38. doi:10.1016/j.jpsychires.2020.12.037
22. Czeisler MÉ, Lane RI, Petrosky E, et al. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic—United States, June 24 –30, 2020. Morb Mortal Wkly R. 2020;69(32):1049. doi:10.15585/mmwr.mm6932a1
23. Iob E, Steptoe A, Fancourt D. Abuse, self-harm and suicidal ideation in the UK during the COVID-19 pandemic. Br J Psychiatry. 2020;217(4):543–546. doi:10.1192/bjp.2020.130
24. Caballero-Domínguez CC, Jiménez-Villamizar MP, Campo-Arias A. Suicide risk during the lockdown due to coronavirus disease (COVID-19) in Colombia. Death Stud. 2020;1–6. doi:10.1080/07481187.2020.1784312
25. Mamun MA, Akter T, Zohra F, et al. Prevalence and risk factors of COVID-19 suicidal behavior in Bangladeshi population: are healthcare professionals at greater risk? Heliyon. 2020;6(10):e05259. doi:10.1016/j.heliyon.2020.e05259
26. Mamun MA, Sakib N, Gozal D, et al. The COVID-19 pandemic and serious psychological consequences in Bangladesh: a population-based nationwide study. J Affect Disord. 2021;279:462–472. doi:10.1016/j.jad.2020.10.036
27. Killgore WDS, Cloonen SA, Taylor EC, Fernandez F, Grandner MA, Dailey NS. Suicidal ideation during the COVID-19 pandemic: the role of insomnia. Psychiatry Res. 2020;290:113134. doi:10.1016/j.psychres.2020.113134
28. Mather AA, Cox BJ, Enns MW, Sareen J. Associations of obesity with psychiatric disorders and suicidal behaviors in a nationally representative sample. J Psychosom Res. 2009;66(4):277–285. doi:10.1016/j.jpsychores.2008.09.008
29. López-Bueno R, Calatayud J, Ezzatvar Y, et al. Association between current physical activity and current perceived anxiety and mood in the initial phase of COVID-19 confinement. Front Psychiatry. 2020;11:729. doi:10.3389/fpsyt.2020.00729.
30. López-Bueno R, Calatayud J, Andersen LL, et al. Immediate impact of the COVID-19 confinement on physical activity levels in Spanish adults. Sustain. 2020;12(14):5708. doi:10.3390/su12145708
31. Maugeri G, Castrogiovanni P, Battaglia G, et al. The impact of physical activity on psychological health during Covid-19 pandemic in Italy. Heliyon. 2020;6(6):e04315. doi:10.1016/j.heliyon.2020.e04315
32. Chouchou F, Augustini M, Caderby T, Caron N, Turpin NA, Dalleau G. The importance of sleep and physical activity on well-being during COVID-19 lockdown: reunion island as a case study. Sleep Med. 2020;77:297–301. doi:10.1016/j.sleep.2020.09.014
33. Codella R, Chirico A, Lucidi F, Ferrulli A, La Torre A, Luzi L. The immune-modulatory effects of exercise should be favorably harnessed against COVID-19. J Endocrinol Invest. 2020. doi:10.1007/s40618-020-01403-5
34. Dutton GR, Bodell LP, Smith AR, Joiner TE. Examination of the relationship between obesity and suicidal ideation. Int J Obes. 2013;37(9):1282–1286. doi:10.1038/ijo.2012.224
35. Vancampfort D, Hallgren M, Firth J, et al. Physical activity and suicidal ideation: a systematic review and meta-analysis. J Affect Disord. 2018;225:438–448. doi:10.1016/j.jad.2017.08.070
36. Disu TR, Anne NJ, Griffiths MD, Mamun MA. Risk factors of geriatric depression among elderly Bangladeshi people: a pilot interview study. Asian J Psychiatr. 2019;44:163–169. doi:10.1016/j.ajp.2019.07.050
37. Löwe B, Wahl I, Rose M, et al. A 4-item measure of depression and anxiety: validation and standardization of the patient health questionnaire-4 (PHQ-4) in the general population. J Affect Disord. 2010;122(1–2):86–95. doi:10.1016/j.jad.2009.06.019
38. Kroenke K, Spitzer RL, Williams JBW. The patient health questionnaire-2: validity of a two-item depression screener. Med Care. 2003;41(11):1284–1292. doi:10.1097/01.MLR.0000093487.78664.3C
39. Kroenke K, Spitzer RL, Williams JBW, Monahan PO, Löwe B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med. 2007;146(5):317–325. doi:10.7326/0003-4819-146-5-200703060-00004
40. Jahan S, Araf K, Griffiths D, Gozal MD, Mamun MA. Depression and suicidal behaviors among Bangladeshi mothers of children with Autism Spectrum Disorder: a comparative study. Asian J Psychiatr. 2020;51:e101994. doi:10.1016/j.ajp.2020.101994
41. Mamun MA, Rayhan I, Akter K, Griffiths M. Prevalence and predisposing factors of suicidal ideation among the university students in Bangladesh: a single-site survey. Int J Ment Health Addict. 2020. doi:10.1007/s11469-020-00403-z
42. Turecki G, Brent DA. Suicide and suicidal behaviour. Lancet. 2016;387(10024):1227–1239. doi:10.1016/S0140-6736(15)00234-2
43. Hawryluck L, Gold WL, Robinson S, Pogorski S, Galea S, Styra R. SARS control and psychological effects of quarantine, Toronto, Canada. Emerg Infect Dis. 2004;10(7):1206–1212. doi:10.3201/eid1007.030703
44. Hossain MM, Rahman M, Trisha NF, et al. Prevalence of anxiety and depression in South Asia during COVID-19: a systematic review and meta-analysis. Heliyon. 2021;7(4):e06677. doi:10.1016/j.heliyon.2021.e06677
45. Moynihan AB, Tilburg WAP, Van, Igou ER, Wisman A, Donnelly AE, Mulcaire JB. Eaten up by boredom: consuming food to escape awareness of the bored self. Front Psychol. 2015;6:369. doi:10.3389/fpsyg.2015.00369
46. Jia P, Liu L, Xie X, et al. Impacts of COVID-19 lockdown on diet patterns among youths in China: the COVID-19 Impact on Lifestyle Change Survey (COINLICS). Appetite. 2020;158:105015. doi:10.1016/j.appet.2020.105015
47. Araiza AM, Lobel M. Stress and eating: definitions, findings, explanations, and implications. Soc Personal Psychol Compass. 2018;12(4):e12378. doi:10.1111/spc3.12378
48. Daly M, Robinson E, Sutin AR. Perceived overweight and suicidality among US adolescents from 1999 to 2017. Int J Obes. 2020;44(10):2075–2079. doi:10.1038/s41366-020-0620-9.
49. Wang S, Ma W, Wang S-M, Yi X. A cross sectional examination of the relation between depression and frequency of leisure time physical exercise among the elderly in Jinan, China. Int J Environ Res Public Health. 2018;15(9):2041. doi:10.3390/ijerph15092041
50. De Wit LM, Fokkema M, van Straten A, Lamers F, Cuijpers P, Penninx BWJH. Depressive and anxiety disorders and the association with obesity, physical, and social activities. Depress Anxiety. 2010;27(11):1057–1065. doi:10.1002/da.20738
51. Bhamani MA, Khan MM, Karim MS, Mir MU. Depression and its association with functional status and physical activity in the elderly in Karachi, Pakistan. Asian J Psychiatr. 2015;14:46–51. doi:10.1016/j.ajp.2014.12.004
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.