")
Back to Journals » International Journal of Women's Health » Volume 15
How Do Women React to the COVID-19 Pandemic Period? Relationship Between Ego-Resiliency, Anxiety, Alcohol Consumption and Aggression Among Polish Women
Authors Florek S , Piegza M , Dębski P, Gorczyca P, Pudlo R
Received 28 April 2023
Accepted for publication 6 July 2023
Published 28 July 2023 Volume 2023:15 Pages 1219—1226
DOI https://doi.org/10.2147/IJWH.S419169
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Szymon Florek,1,* Magdalena Piegza,2,* Paweł Dębski,2,3,* Piotr Gorczyca,2,* Robert Pudlo1,*
1Department of Psychoprophylaxis, Faculty of Medical Sciences in Zabrze, Medical University of Silesia, Katowice, Poland; 2Department of Psychiatry, Faculty of Medical Sciences in Zabrze, Medical University of Silesia, Katowice, Poland; 3Institute of Psychology, Faculty of Social Sciences and Humanities, Humanitas University in Sosnowiec, Sosnowiec, Poland
*These authors contributed equally to this work
Correspondence: Szymon Florek, Email [email protected]
Purpose: There are many reports in the literature on the impact of the COVID-19 pandemic on mental health, including the condition of women. Most of these studies refer to a single time point, while there is a lack of studies controlling for selected parameters during different periods of the pandemic. This work aimed to determine the role of ego-resiliency in women’s adaptation to the COVID-19 pandemic.
Patients and Methods: The survey was conducted in two stages - all via online forms. A total of 762 Polish women took part in the overall project. The scales used in the study were the Ego-resiliency scale (ER89-R12), Generalized Anxiety Disorder 7 Scale (GAD-7), Alcohol Use Disorders Identification Test (AUDIT), and Buss-Perry Aggression Questionnaire (BPAQ). Statistical analysis was performed using Statistica 13.3.
Results: Women participating in the second study had significantly lower scores on ego-resilience and its components compared to the first study. In the first research, ego-resiliency and optimal regulation were statistically significantly correlated with anxiety, alcohol consumption, generalised aggression, verbal aggression and hostility, while openness to life experiences was correlated with alcohol consumption and hostility. The second part of the project highlighted new significant correlations between ego-resiliency and optimal regulation and physical aggression and anger, but a non-significant correlation of these variables with alcohol consumption. The effect of openness to life experiences on alcohol consumption and anxiety, evident in the first study, was no longer present in the second part of the study.
Conclusion: The lack of a significant effect of openness to life experience on alcohol consumption, lower ego-resiliency and optimal regulation scores are observed in the second part of the research, which might be an expression of adaptation to the COVID-19 pandemic. Ego-resiliency is a protective factor against aggression, while optimal regulation against anxiety among Polish women.
Keywords: COVID-19, women, resiliency, adaptation, anxiety, aggression
Introduction
The COVID-19 pandemic was a time in which many changes in mental health across sociological groups occurred.1 In addition to the mere presence of infectious disease, researchers from around the world sought to assess the potential mental health risks posed first by the lockdown restrictions,2 but also by the period of the pandemic itself, and the consequent attack from all sides with the latest information on COVID-19, often unfortunately also false.3
Until now, many scientific projects have been conducted to determine the impact of the COVID-19 pandemic on specific elements of mental health such as mood or anxiety. This meta-analysis showed that as many as 45% of COVID-19 patients experience depression, 47% of patients experience anxiety, a significantly higher percentage compared to before the pandemic outbreak.4 Of course, there has also been no shortage of studies touching on behavioural aspects such as aggressive behaviour,5 or alcohol consumption.6 This study found that aggression and alcohol consumption increased during the COVID-19 pandemic.6,7 It is worth noting, however, that most of these studies were produced between 2020 and 2021, so to speak, the initial period of the pandemic. Moreover, most of them are studies aimed at assessing selected parameters at a single point in time,6,7 and again only some of them are longitudinal.8 Unfortunately, the authors did not find any reliable data in the literature for assessing mental status from the end of the pandemic period - ie 2022 or 2023. However, it seems that the variables in question should slowly return to their pre-COVID-19 state.
Undoubtedly, the state of women’s mental health during the COVID-19 pandemic is a very important issue, as they are more susceptible than men to various emotional reactions resulting from the COVID-19 pandemic, and this can lead to many including pathological mechanisms for regulating these - such as increased alcohol consumption.6 The importance of the topic is also evidenced by the fact that, since the beginning of the pandemic, there has been a considerable amount of research specifically addressing women’s mental health issues during the COVID-19 pandemic.9 However, similar to those discussed above, they tend to cover a single point in time. Women’s mental health is particularly important during an epidemic threat for a number of different reasons. As evidenced by studies conducted outside the pandemic period, women are characterized by higher levels of anxiety than men,10 they also exhibit less aggressive behavior (already from adolescence onwards) and consume alcohol in smaller quantities.11,12 In this situation, it is difficult to determine unequivocally how detrimental the COVID-19 pandemic may be to women’s mental health. For this reason, it is extremely important to conduct research in this area.
One of the most important psychological characteristics of a health-promoting nature is ego-resiliency. The scale for ego-resiliency was first created by Block in 1996.13 In this first view of Block, mental resilience was supposed to be an element of personality, which is still emphasised in scientific studies today.14 In this approach, ego-resiliency is to be regarded as an enduring construct conditioning the individual’s responses to surrounding stimuli.15 However, according to some more modern approaches, resilience can be defined as a process that facilitates adaptation. Recently, research has been conducted using a relatively new scale to determine ego-resiliency,16 which has not yet been fully explored. In Block’s concept, ego-resiliency is related to the ability to flexibly adapt to the stimuli coming from the changing environment. Resiliency is therefore a feature that means the ability to increase and decrease control over the environment depending on the situation.17 So far, there is very little work using the Ego-resiliency scale relating directly to COVID-19.18–22 For this reason, this topic seems to be interesting and needs to be explored further to assess the possibility of using psychological resiliency in the face of potential further unexpected events in the future. The need for further research on ego-resiliency is also highlighted by other researchers, while pointing out the underdevelopment of its construct at the moment.23 These doubts mainly relate to the concept’s conflicts about resiliency, as well as the multidisciplinary nature of resiliency referring not only to psychology but also to genetics or neurobiology.24 Ego-resiliency is also a field of study among women. So far, research has been conducted in Poland on the resilience of women serving a sentence of imprisonment25 or experiencing domestic violence.26
The study was divided into two independent stages at different time intervals. The first part of the study was carried out on April 24–May 8, 2020. During this time, 4855 new cases of COVID-19 were recorded in Poland, 322 of whom died. The second part of our project was conducted on February 5, 2022 to March 6, 2022. During this time, 650,709 new cases were registered in Poland, of which 6229 people died. These data come from the official statistics of the Ministry of Health available on the government portal gov.pl and the official profiles of the Ministry of Health on portals such as Twitter and Facebook. This study is in some ways compatible with the understanding of ego-resiliency by some authors, whose work suggests the emergence of more longitudinal studies on resiliency.27
Aim of the Study
The present study aimed to assess ego-resiliency among Polish women and to identify potential health-promoting properties in interactions with other parameters studied, such as the intensity of anxiety, aggression or the level of alcohol consumption. In order to identify adaptive capacity to the pandemic, the study was divided into two parts as described above.
Materials and Methods
In different periods of the COVID-19 pandemic, two independent studies involving unrelated study groups were conducted. The survey was conducted entirely via the Internet. In the first stage, it was conditioned by legal and epidemiological constraints, while the next study was carried out in the same way to maintain the same methodology, which allows for a reliable comparison of the two trials. 413 women (age 18–66) took part in the first part, and 349 (age 18–59) in the second part. Before the research, a question was asked to the Bioethics Committee at the Medical University of Silesia in Katowice to assess whether the survey conducted via the Internet requires its consent. Negative responses were obtained in both cases. The inclusion criteria for both trials were the same and included reaching the age of 18 and giving informed consent to participate in the trial by accepting comprehensive instruction before the pre-questionnaire. This instruction contained information on the voluntary nature of the study and the possibility of withdrawing from it at any time. In order to identify exclusion criteria, pre-questionnaires were created, which included relevant questions about psychiatric treatment in the past, or the presence of important events in the year before study entry.
In both parts of the study, the psychometric scales: Ego-resiliency scale (ER89-R12), Generalized Anxiety Disorder 7 Scale (GAD-7), Alcohol Use Disorders Identification Test (AUDIT), and Buss-Perry Aggression Questionnaire (BPAQ) that had been described in detail in the previous study19 were used. The ER-89 consists of 12 questions and is used to measure ego-resiliency, which consists of optimal regulation (OR) and openness to life experiences (OL). The GAD-7 is a 7-question scale that measures anxiety intensity. The AUDIT consists of 10 questions answered on a 3- or 4-point scale and is designed to identify problematic alcohol use. The BPAQ is a scale that measures aggression along four dimensions - anger, hostility, verbal aggression and physical aggression and consists of 29 questions. Statistical analysis was performed using the Statistica 13.3 program. The Shapiro–Wilk test was used to assess the normality of distributions. The Wald-Wolfowitz test was used to compare the two unrelated study groups in terms of the variables studied. Within these groups, correlation analyses were performed using Spearman correlation coefficient. Linear regression models were also created. The level of statistical significance was assumed at α≤0.05.
Results
A comparative analysis between study groups from the first and second part of the study showed statistically significant differences in ego-resiliency and its component - optimal regulation (Table 1).
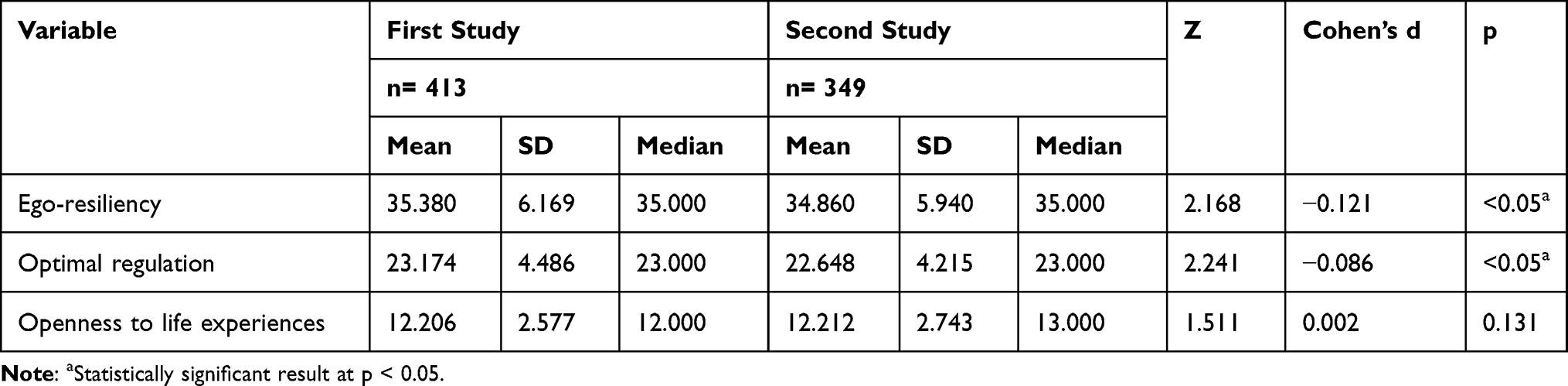 |
Table 1 Comparative Analysis of Ego-Resilience During the First and Second Pages of the Study, p <0.05 |
In the next step, correlation analyses were carried out separately for each of the time points (Table 2 and 3). In the first part of the study, moderately negative correlations between ego-resiliency and optimal regulation and anxiety were shown, and relatively weak negative correlations between these variables and generalized aggression. Weak positive correlations were shown between ego-resiliency and optimal regulation and verbal aggression, as well as weak positive correlations between all elements of resiliency and the intensity of alcohol consumption. Finally, resiliency and its components correlate with hostility in a moderately negative manner. The analysis of the second part of the study shows stronger negative correlations between anxiety and ego-resiliency and optimal regulation, similarly, stronger correlations occur with the level of generalized aggression. Ego-resiliency and optimal regulation have a weak negative correlation with the intensity of physical aggression and anger. Openness to life experience correlates only slightly positively with the level of alcohol consumption. In a weakly positive way, all three elements of ego-resiliency are related with verbal aggression, while quite strong, negative correlations are found between ego-resiliency and optimal regulation in relation to hostility. Hostility, in addition, correlates weakly and positively with openness to life experiences.
 |
Table 2 Relationship Between Ego-Resiliency and Its Components and Anxiety, Alcohol Consumption, Aggression in the First Part of Research |
 |
Table 3 Relationship Between Ego-Resiliency and Its Components and Anxiety, Alcohol Consumption, Aggression in the Second Part of Research |
For both time points, linear regression models were created to determine the effect of ego-resiliency and its components on the other variables studied (Table 4 and 5). In the analysis of the performed regressions, the impact of both ER components on the severity of anxiety is noted. What is more, in the first study, optimal regulation occurs to influence generalized aggression, while openness to life experiences presents impact on alcohol consumption. The situation is slightly different in the second period, where OL no longer affects alcohol consumption and the intensity of anxiety. Taking OR into consideration, it can be seen that in the second study the statistically significant influence of this variable on the intensity of anxiety and generalized aggression is still observed.
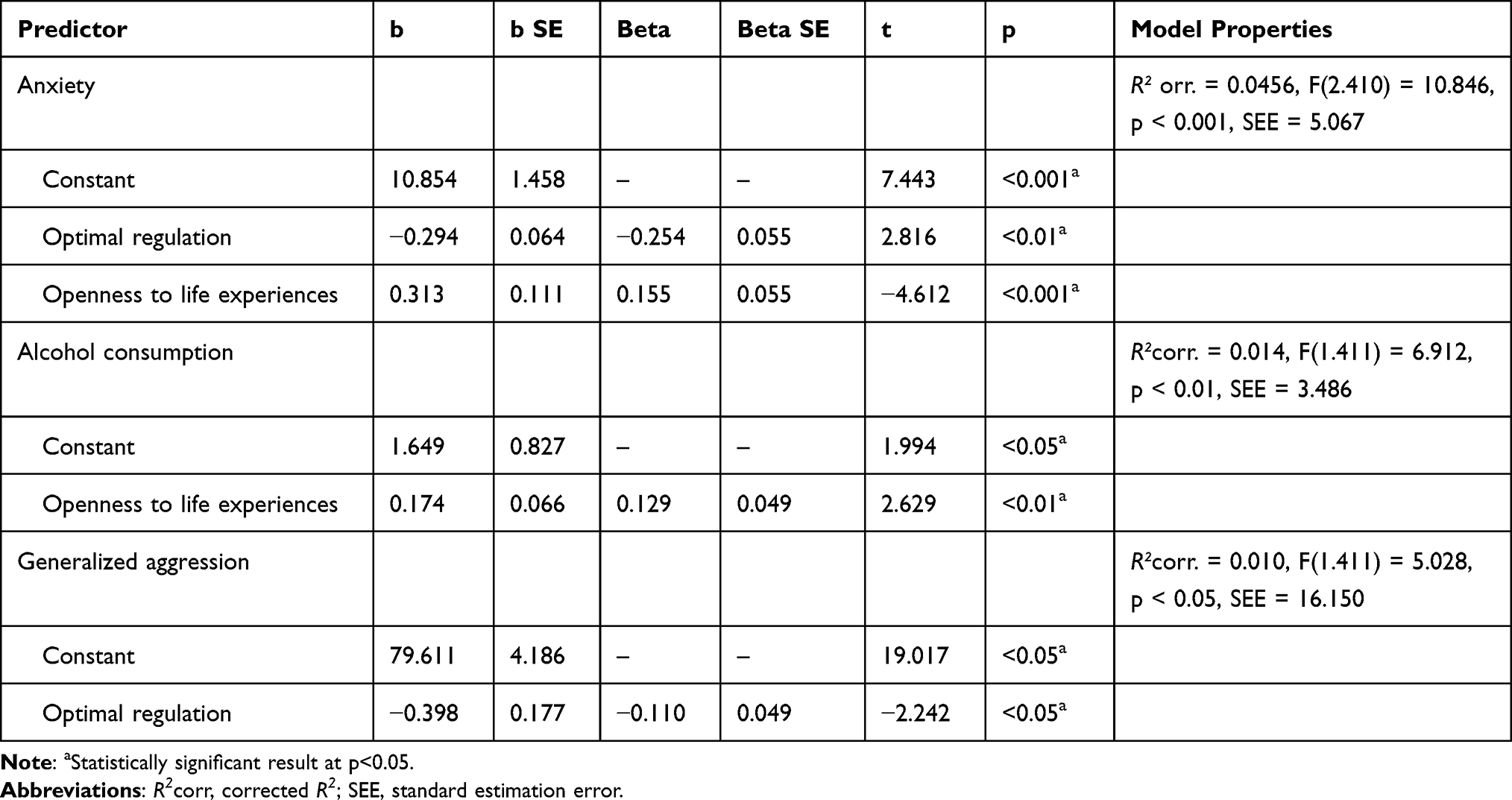 |
Table 4 Models of Regression of Anxiety, Alcohol Consumption and Generalized Aggression in the Light of Optimal Regulation and Openness to Life Experiences in the First Part of Research |
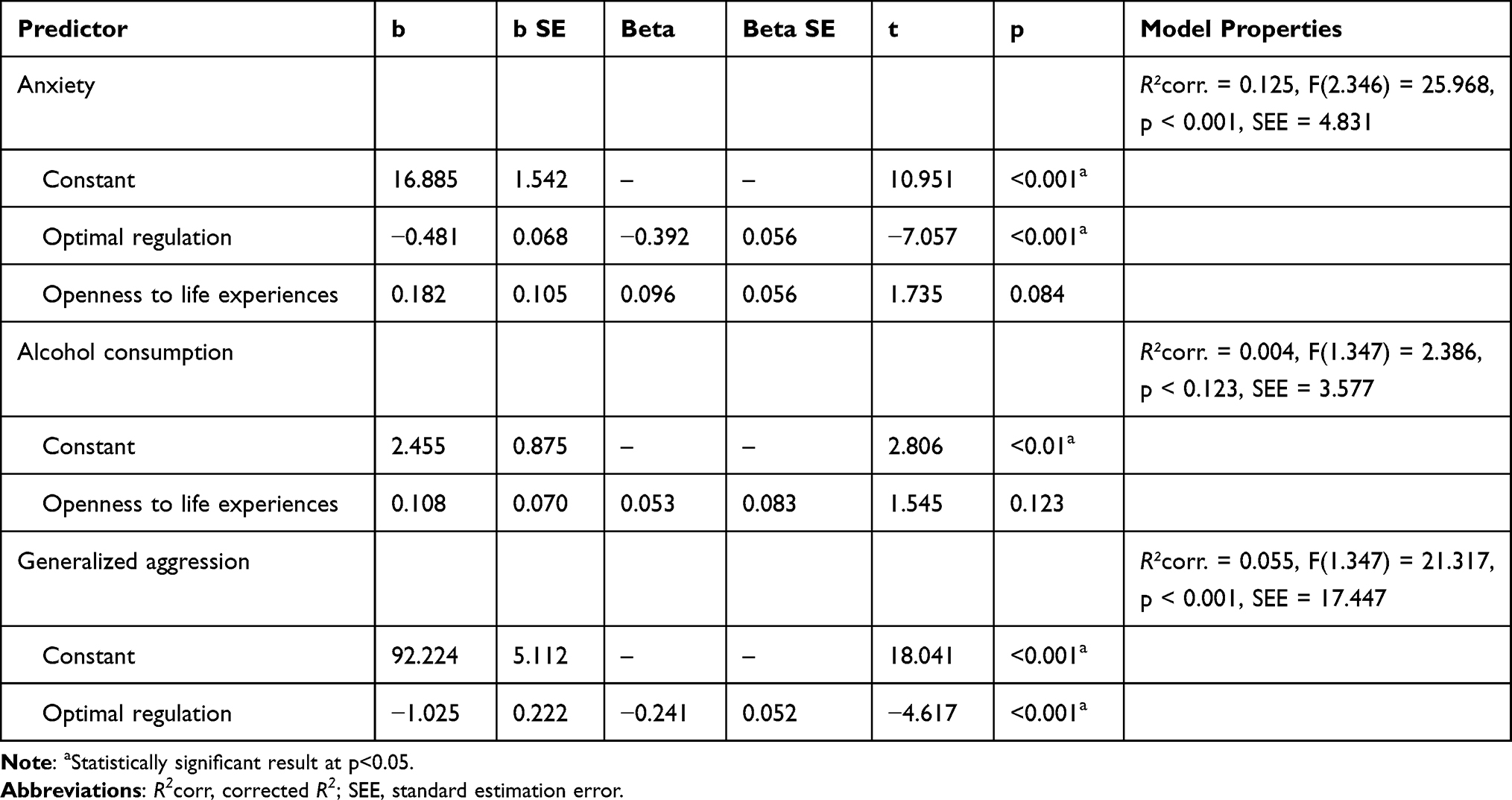 |
Table 5 Models of Regression of Anxiety, Alcohol Consumption and Generalized Aggression in the Light of Optimal Regulation and Openness to Life Experiences in the Second Part of Research |
Discussion
Our analysis showed a statistically significant differences between measures of ego-resiliency and optimal regulation at the two-time points. Women from the first study had higher levels of these parameters compared to women from the second part. As this is the first study using this scale at two different time points during the COVID-19 pandemic in Poland, there are no studies on similar observations. It could be said that resiliency similarly to other psychological traits undergoes adaptation according to generally accepted patterns in which, in response to a stimulus, the severity of a trait first increases and then gradually decreases to a level that the organism can accept as a new “zero point”.28 On the other hand, it should be noted that, according to some concepts, resiliency is supposed to be much more related to personality, which gives its stable character.14 In consequence, it should not be connected with a change in some period. However, given that the response to a pandemic according to Heitzman’s conception may exhaust the diagnostic criteria of an acute stress reaction,29 it seems reasonable to relate this situation to studies conducted among women with breast cancer. A diagnosis of breast cancer is also associated with shock and comes on suddenly, and can trigger a full-blown acute stress reaction in most women. As shown in these, the greatest increase in resilience was observed in the first stage of the disease, followed by a slow decline.30 Moreover, this is consistent with The Posttraumatic Growth (PTG) theory as described by Tedeschi and Calhoun.31 Nevertheless, in the study described here, the dynamics of the decrease in resilience can be described as quite rapid, as it covers a period of two years. However, this should not be surprising given that at the time of the second study (February 2022), COVID-19 incidence did not represent as strong an exposure to death as it had before, and the media also did not report on a daily basis the number of deaths and incidences of the disease. This observation suggests that the COVID-19 pandemic was such a powerful stressor that some seemingly unchanging human traits were modified under its influence. Nevertheless, further research in this area is needed to verify this hypothesis.
Our study showed that ego-resiliency and its optimal regulation component correlate negatively with anxiety severity at both testing dates. Furthermore, a statistically significant effect of optimal regulation on anxiety severity was also highlighted. These results are broadly in line with another study conducted during the COVID-19 pandemic.20 Also, similar results were obtained in another project by the authors, which analysed the responses of both male and female respondents.19 However, it is noteworthy that the same pattern of results was also obtained in a study among internally displaced people due to armed conflict conducted outside the COVID-19 pandemic period.32 Thus, it appears that these relationships have been well studied to date and are essentially common to both sexes. Nevertheless, somewhat in opposition stands the study by Kubo et al, in which neither negative correlations nor a significant effect of ego-resiliency on anxiety were showed.18 In contrast, our study highlighted a difference in the effect of openness to life experiences on anxiety. While a statistically significant effect was observed at the beginning of the pandemic, it was no longer present in the second term of the study. Taking into account that initially the effect was positive, ie a higher level of openness to life experiences increased anxiety, it seems that this change may be the result of adaptation to the conditions of the COVID-19 pandemic. As can be seen, optimal regulation strengthened its protective effect on anxiety. However, this observation is new and requires further research to confirm its relevance in adaptation processes.
An interesting observation is the relationship between ego-resiliency and alcohol consumption among female respondents. Comparing the two time points included in the study, there is a significant decrease in the role of ego-resiliency in the level of alcohol consumption. At the beginning of the pandemic, we observed a significant effect of openness about life experiences on alcohol consumption, which is no longer observed in February 2022. Furthermore, an earlier study highlighted positive weak correlations between alcohol consumption and ego-resilience and its subscales.19 In the second study - only the correlation of openness to life experiences with alcohol was found to be statistically significant. The correlations discussed are relatively new, and due to their low power, randomness cannot be excluded here. Furthermore, as described in studies conducted outside the pandemic period - resiliency should play a protective role against alcohol consumption.33,34 At the same time, it should be noted that openness to life experiences is directly related to the constant search for new experiences,35 which in our study may be reflected - also in the second term - by a positive correlation of this variable with alcohol consumption. However, this topic certainly requires further research and the data available to date are not sufficient to draw conclusions.
The present study highlighted the negative effect of optimal regulation on generalized aggression at both the first and second study dates. This is broadly in line with other studies conducted outside the pandemic period, which have shown a protective effect of ego-resiliency on aggression.36,37 Moreover, Ng et al showed that resiliency can have the effect of reducing aggression by directly reducing anxiety and depression, factors that have a direct effect on increasing the expression of aggression.36 Akbari, reports also that resiliency training reduces aggression levels in a statistically significant way.37 In our study, it turns out that at the beginning of the COVID-19 pandemic ego-resiliency and optimal regulation correlated negatively with generalized aggression and hostility, while positively with verbal aggression. Openness to life experiences correlated negatively only with hostility. In the second term of the study, broadly similar results were obtained, with ego-resiliency and optimal regulation correlating negatively with generalized aggression and all its components. Openness to life experiences correlated further negatively with hostility, but also weakly positively with verbal aggression. In general, these results are consistent with the reports presented above. Furthermore, as reported in a study of adolescents, resiliency has a protective effect on all forms of aggression in both girls and boys.38 To sum up, it can be observed that resiliency is a protective factor against general aggression. The relationship between ego-resiliency and verbal aggression requires further research.
Limitations and Strengths
It was decided to conduct the survey in two completely separate study groups, which limits the observation of the dynamics of change, as would be the case in a follow-up study. On the other hand, this allowed the survey to be conducted on a large study group. For this reason, they may be entirely different groups of women who only have internet use in common. It should therefore not be forgotten that the comparisons made in the article are only exploratory. Nevertheless, in view of the considerably limited number of cross-sectional studies on women’s mental state, this analysis seems extremely important despite its evident limitations. Certainly, another limitation is the form in which the survey was conducted via the Internet, which prevented individual interaction with each person surveyed and thus answering any questions. This was in the first stage due to the legal constraints of lockdown, while in the second stage, it was due to the need for methodological accuracy in conducting the survey in relation to the previous one. The advantage is that respondents were guaranteed full anonymity in both the first and second surveys, as they did not have to provide any contact details. This is particularly important given the variables under study could be sensitive issues for the survey participants. It should be clearly emphasized that the survey was not conducted on a representative group, which undoubtedly limits the extrapolation of its results.
Conclusion
In the group of Polish women, lower ego-resiliency and optimal regulation scores are observed in 2022 than in 2020, which may reflect adaptation to the COVID-19 pandemic. ER and OR could be in some way susceptible to changes under the influence of the external situation, including the process of adapting to the pandemic. What is more, ego-resiliency is a protective factor against aggression, while optimal regulation is responsible for lowering anxiety among Polish women.
Ethic Statement
Before the research, a question was asked to the Bioethics Committee at the Medical University of Silesia in Katowice to assess whether the survey conducted via the Internet requires its consent. Negative responses were obtained in both cases. This decision was dictated by the lack of need to process any personal data. The entire study was conducted in accordance with the Declaration of Helsinki.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hossain MM, Tasnim S, Sultana A, et al. Epidemiology of mental health problems in COVID-19: a review. F1000Res. 2020;9:636. doi:10.12688/f1000research.24457.1
2. Pieh C, Budimir S, Delgadillo J, et al. Mental health during COVID-19 Lockdown in the United Kingdom. Psychosom Med. 2021;83(4):328–337. doi:10.1097/PSY.0000000000000871
3. Su Z, McDonnell D, Wen J, et al. Mental health consequences of COVID-19 media coverage: the need for effective crisis communication practices. Global Health. 2021;17(1):4. doi:10.1186/s12992-020-00654-4
4. Deng J, Zhou F, Hou W, et al. The prevalence of depression, anxiety, and sleep disturbances in COVID-19 patients: a meta-analysis. Ann N Y Acad Sci. 2021;1486(1):90–111. doi:10.1111/nyas.14506
5. Mazza M, Marano G, Lai C, et al. Danger in danger: interpersonal violence during COVID-19 quarantine. Psychiatry Res. 2020;289:113046. doi:10.1016/j.psychres.2020.113046
6. Barbosa C, Cowell AJ, Dowd WN. Alcohol consumption in response to the COVID-19 pandemic in the United States. J Addict Med. 2021;15(4):341–344. doi:10.1097/ADM.0000000000000767
7. Cui J, Lu J, Weng Y, et al. COVID-19 impact on mental health. BMC Med Res Methodol. 2022;22(1):15. doi:10.1186/s12874-021-01411-w
8. Qu G, Zhen Q, Wang W, et al. Health-related quality of life of COVID-19 patients after discharge: a multicenter follow-up study. J Clin Nurs. 2021;30(11–12):1742–1750. doi:10.1111/jocn.15733
9. Almeida M, Shrestha AD, Stojanac D, et al. The impact of the COVID-19 pandemic on women’s mental health. Arch Womens Ment Health. 2020;23(6):741–748. doi:10.1007/s00737-020-01092-2
10. McLean CP, Asnaani A, Litz BT, et al. Gender differences in anxiety disorders: prevalence, course of illness, comorbidity and burden of illness. J Psychiatr Res. 2011;45(8):1027–1035. doi:10.1016/j.jpsychires.2011.03.006
11. Österman K, Björkqvist K, Lagerspetz K, et al. Cross-cultural evidence of female indirect aggression. Aggress Behav. 1998;24(1):1–8. doi:10.1002/(SICI)1098-2337(1998)24:1<1::AID-AB1>3.0.CO;2-R
12. Manwell LB, Ignaczak M, Czabala JC. Prevalence of tobacco and alcohol use disorders in Polish primary care settings. Eur J Public Health. 2002;12(2):139–144. doi:10.1093/eurpub/12.2.139
13. Block J, Kremen AM. IQ and ego-resiliency: conceptual and empirical connections and separateness. J Pers Soc Psychol. 1996;70(2):349–361. doi:10.1037//0022-3514.70.2.349
14. Dunkel CS, van der Linden D, Kawamoto T, et al. The general factor of personality as ego-resiliency. Front Psychol. 2021;12:741462. doi:10.3389/fpsyg.2021.741462
15. Olsson CA, Bond L, Burns JM, et al. Adolescent resilience: a concept analysis. J Adolesc. 2003;26(1):1–11. doi:10.1016/s0140-1971(02)00118-5
16. Chen Q, Gao W, Chen BB, et al. Ego-resiliency and perceived social support in late childhood: a latent growth modeling approach. Int J Environ Res Public Health. 2021;18(6):2978. doi:10.3390/ijerph18062978
17. Farkas D, Orosz G, Pietschnig J. Ego-resiliency reloaded: a three component model of general resiliency. PLoS One. 2015;10(3):e0120883. doi:10.1371/journal.pone.0120883
18. Kubo T, Sugawara D, Masuyama A. The effect of ego-resiliency and COVID-19-related stress on mental health among the Japanese population. Pers Individ Dif. 2021;175:110702. doi:10.1016/j.paid.2021.110702
19. Dębski P, Florek S, Piegza M, et al. Is it good to be resilient during the COVID-19 period? The role of ego-resiliency in the intensity of symptoms of anxiety, alcohol use and aggression among Polish people. Int J Occup Med Environ Health. 2021;34(2):289–300. doi:10.13075/ijomeh.1896.01766
20. Skalski S, Uram P, Dobrakowski P, et al. The link between ego-resiliency, social support, SARS-CoV-2 anxiety and trauma effects. Polish adaptation of the Coronavirus Anxiety Scale. Pers Individ Dif. 2021;171:110540. doi:10.1016/j.paid.2020.110540
21. Park YH, Kim IH, Jeong YW. Stress, and coping strategy of university students during COVID-19 in Korea: the mediating role of ego-resiliency. Acta Psychol. 2022;227:103615. doi:10.1016/j.actpsy.2022.103615
22. Goryczka A, Dębski P, Gogola AM, et al. Depressive and Anxiety symptoms and their relationships with ego-resiliency and life satisfaction among well-educated, Young Polish Citizens during the COVID-19 pandemic. Int J Environ Res Public Health. 2022;19(16):10364. doi:10.3390/ijerph191610364
23. Luthar SS, Cicchetti D, Becker B. The construct of resilience: a critical evaluation and guidelines for future work. Child Dev. 2000;71(3):543–562. doi:10.1111/1467-8624.00164
24. Szwajca K. Sprezystość (resilience) i odpowiedzi na doświadczenia urazowe--fascynujacy i trudny obszar badań [Resilience and responses to the experience of trauma--a fascinating but difficult study area]. Psychiatr Pol. 2014;48(3):563–572. Polish.
25. Tsirigotis K, Łuczak J. Resilience in women who experience domestic violence. Psychiatr Q. 2018;89(1):201–211. doi:10.1007/s11126-017-9529-4
26. Sygit-Kowalkowska E, Szrajda J, Weber-Rajek M, et al. Resilience as a predicator of mental health of incarcerated women. Psychiatr Pol. 2017;51(3):549–560. English, Polish. doi:10.12740/PP/OnlineFirst/62617
27. Kalisch R, Baker DG, Basten U, et al. The resilience framework as a strategy to combat stress-related disorders. Nat Hum Behav. 2017;1(11):784–790. doi:10.1038/s41562-017-0200-8
28. Myers DG. Psychology.
29. Heitzman J. Impact of COVID-19 pandemic on mental health. Psychiatr Pol. 2020;54(2):187–198. English, Polish. doi:10.12740/PP/120373
30. Izydorczyk B, Kwapniewska A, Lizinczyk S, et al. Psychological resilience as a protective factor for the body image in post-mastectomy women with breast cancer. Int J Environ Res Public Health. 2018;15(6):1181. doi:10.3390/ijerph15061181
31. Tedeschi RG, Calhoun LG. Posttraumatic growth: conceptual foundations and empirical evidence. Psychol Inq. 2004;15(1):1–18. doi:10.1207/s15327965pli1501_01
32. Mujeeb A, Zubair A. Resilience, stress, anxiety and depression among internally displaced persons affected by armed conflict. Pak J Clin Psychol. 2012;10(2):20–26.
33. Green KT, Beckham JC, Youssef N, et al. Alcohol misuse and psychological resilience among U.S. Iraq and Afghanistan era veterans. Addict Behav. 2014;39(2):406–413. doi:10.1016/j.addbeh.2013.08.024
34. Bartone PT, Hystad SW, Eid J, et al. Psychological hardiness and coping style as risk/resilience factors for alcohol abuse. Mil Med. 2012;177(5):517–524. doi:10.7205/MILMED-D-11-00200
35. Heinström J, editor. Chandos Information Professional Series, from Fear to Flow. Cambridge: Chandos Publishing; 2010.
36. Ng R, Ang RP, Ho MHR. Coping with anxiety, depression, anger and aggression: the mediational role of resilience in adolescents. Child Youth Care Forum. 2012;41(6):529–546. doi:10.1007/s10566-012-9182-x
37. Akbari B. Effectiveness of training psychological resilience on aggression and happiness among students. J Holist Nurs Midwifery. 2017;27(1):1–7. doi:10.18869/acadpub.hnmj.27.1.1
38. Mann J, Yadav VN. Aggression and resilience among adolescents. Indian J Health Wellbeing. 2016;7(11):1104–1106.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.