")
Back to Journals » Clinical Interventions in Aging » Volume 13
Hospitalized frail elderly patients – atrial fibrillation, anticoagulation and 12 months’ outcomes
Authors Ekerstad N , Karlsson T, Söderqvist S , Karlson BW
Received 9 December 2017
Accepted for publication 8 March 2018
Published 26 April 2018 Volume 2018:13 Pages 749—756
DOI https://doi.org/10.2147/CIA.S159373
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Niklas Ekerstad,1,2 Thomas Karlsson,3 Sara Söderqvist,4 Björn W Karlson4,5
1Department of Cardiology, NU (NÄL-Uddevalla) Hospital Group, Trollhättan-Uddevalla-Vänersborg, Sweden; 2Department of Medical and Health Sciences, Division of Health Care Analysis, Linköping University, Linköping, Sweden; 3Health Metrics Unit, Institution of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; 4Department of Acute and Internal Medicine, NU (NÄL-Uddevalla) Hospital Group, Trollhättan-Uddevalla-Vänersborg, Sweden; 5Department of Molecular and Clinical Medicine, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
Background and objective: Multiple chronic conditions and recurring acute illness are frequent among elderly people. One such condition is atrial fibrillation (AF), which increases the risk of stroke up to fivefold. The aim of this study was to investigate the prevalence of AF among hospitalized frail elderly patients, their use of anticoagulation and their 12-month outcomes.
Patients and methods: This was a clinical observational study of acutely hospitalized frail patients over the age of 75 years. The CHA2DS2-VASc Score was used to evaluate ischemic stroke risk in patients with AF. Clinically relevant outcomes were the composite of ischemic stroke and/or bleeding within 12 months, which was considered as primary in the analysis, ischemic stroke/transient ischemic attack (TIA), mortality, bleeding and hospital care consumption. Student’s t-test, Fisher’s exact test, Mann–Whitney U test and a Cox proportional hazards model were used for the analyses.
Results: The prevalence of AF was 47%, and 63% of them were prescribed an anticoagulant. AF patients without anticoagulation were older, more often females, more often in residential care, and they had worse Mini Nutritional Assessment and activities of daily living scores. Of the patients without anticoagulation, 56% had a documented contraindication. In univariate analysis, there were significantly more events among AF patients without anticoagulation regarding the composite outcome of ischemic stroke and/or bleeding (hazard ratio [HR] 3.65, 95% CI = 1.70–7.86; p < 0.001). When adjusting for potential confounders in Cox regression analysis, the difference remained significant (HR 4.54, 95% CI = 1.83–11.25; p = 0.001).
Conclusion: The prevalence of AF in a hospitalized frail elderly population was 47%. Of these, 63% were prescribed anticoagulation therapy. Almost half of the patients without stroke prophylaxis had no documented contraindication. At 1 year, there were significantly more events in terms of ischemic stroke and/or bleeding among AF patients without anticoagulation therapy than among those with.
Keywords: frail elderly, atrial fibrillation, anticoagulants, outcomes, patient safety
Introduction
Background
The elderly population is growing worldwide, resulting in an expected more than doubling of the number of individuals over 80 years of age, from 125 to 434 million, until 2050.1 Among elderly people, multiple chronic conditions and recurring acute illness demanding hospitalization are frequent. One of these conditions is atrial fibrillation (AF).
Frailty is a biological, multi-dimensional syndrome with reduced physiological reserves and vulnerability to stressors.2–4 Frailty is highly associated with functional decline, activity limitations, and prolonged recovery. It also predicts a high risk of institutionalization and death.5–7 The prevalence of frailty in older people has been reported to vary up to 60%.8 Frail elderly patients constitute a high percentage of the individuals treated in specialized hospital acute care units.9,10
Age-related physiological changes, comorbidity, functional impairment and polypharmacy often interact in frail elderly patients. It is important to provide safe and effective pharmacological care for these patients, balancing potential benefits and risks. In a recent publication, it was indicated that although adverse drug reactions (ADRs) are important causes of re-hospitalization, underuse of evidence-based drug treatment might be an even more frequent and important cause.11
AF is a common arrhythmia. A prevalence of 38% was recently reported in a frail elderly population.12 AF is often classified into three different types: paroxysmal, persistent and permanent.13 It is associated with increased morbidity and mortality,14 particularly with an increased risk of arterial embolization, and most feared are cerebral ischemic injuries.13,14
The treatment strategy for AF is primarily focused on stroke prevention, but also includes rate and rhythm control. Anticoagulants are used for stroke prevention and can be divided into low-molecular-weight heparin (LMWH) or oral anticoagulants (OACs). OACs can be further divided into vitamin K antagonists (VKAs) or non-vitamin K antagonist oral anticoagulants (NOACs).15 Among available NOACs, three are factor Xa inhibitors (apixaban, rivaroxaban and edoxaban) and one a direct thrombin inhibitor (dabigatran). The most commonly used VKA is warfarin.13,16
Importance
AF increases the risk of stroke up to fivefold.14 For frail elderly patients, stroke is associated with an increased risk of severe functional decline and loss of health-related quality of life. Many of the factors associated with an increased risk of stroke, eg, age ≥75 years, prior ischemic stroke, thromboembolism, hypertension, heart failure and diabetes mellitus are also associated with an increased risk of bleeding, eg, intracranial hemorrhage and gastrointestinal bleeding, contributing to difficult treatment decisions regarding anticoagulation therapy.17,18
According to guidelines, patients with CHA2DS2-VASc ≥2 (see “Measurements” section) should be prescribed an OAC.13,16 The Swedish National Board of Health and Welfare has stated that ≥80% of patients with AF should be treated with an anticoagulant, contraindications taken into account. There are data indicating an undertreatment, primarily and paradoxically most obvious among those with the highest risk of stroke.13,19,20 In a Swedish report from 2013, only 58% of AF patients received anticoagulation treatment.21
Goals of the investigation
The aim of this study was to investigate the prevalence of atrial fibrillation among hospitalized frail elderly patients, their use of anticoagulation and their 12-month outcomes with a focus on the composite outcome of stroke and/or clinically relevant bleeding.
Patients and methods
Study design and setting
This was a clinical observational study. It was conducted within the project “Is the treatment of frail elderly patients effective in an elderly care unit (TREEE)” at the NU county hospital group in the Västra Götaland region in Sweden between March 2013 and July 2015. The TREEE study was registered at the Swedish National Database of Research and Development, identifier 113021 (http://www.researchweb.org/is/vgr/project/113021) November 4, 2012, and approved by the Independent Ethics Committee at the Sahlgrenska University Hospital in Gothenburg, Sweden (registration number 883-12, 20121212).
Selection of participants
The selection of patients and data collection for TREEE has been previously described.22 In total, 419 patients were included, 408 of whom could be evaluated. Inclusion criteria were age ≥75 years, need of hospital care, and frailty according to the validated Frail Elderly Support Research (FRESH) group screening instrument,23 see “Measurements section”. Exclusion criteria included acute need of care at an organ-specific unit, eg, patients with an acute myocardial infarction or a stroke. All patients provided written informed consent to participate.
Measurements
Clinical and demographic characteristics
The following data were collected from patients, medical records and registers during the index care episode and at the 12-month follow-up: age, gender, housing, strokes/transitory ischemic attacks (TIAs), bleeding, falls, fractures, hypertension, vascular disease, diabetes mellitus, renal function, heart failure, other comorbidities, laboratory parameters, electrocardiogram (ECG) and X-ray examination results, medications, numbers of in-hospital care days, rehospitalizations, and mortality. Data regarding anticoagulation therapy were extracted from the specific files for anticoagulation treatment in the medical records. Activities of daily living (ADL) independence/dependence was assessed using the ADL Staircase.24 The risk of malnutrition was assessed through the Mini Nutritional Assessment – short form (MNA-SF).25 The patient’s total burden of morbidity was measured by the Charlson Comorbidity Index.26
Atrial fibrillation
A cardiologist judged the ECGs regarding the sub-classification of AF, ie, paroxysmal, persistent or permanent AF.
Frailty
Two or more of the following criteria in the FRESH screening instrument implies frailty: tiredness from a short walk, general fatigue, frequent falls/anticipation of falls, dependence in shopping, and three or more visits to the emergency ward during the last 12 months.23
CHA2DS2-VASc score
The CHA2DS2-VASc score evaluates ischemic stroke risk in patients with atrial fibrillation.17,18,27 This acronym denotes the following: congestive heart failure, hypertension, age ≥ 75 years, diabetes mellitus, prior stroke/TIA, vascular disease, age 65–74 years, sex category (female). The higher the CHA2DS2-VASc score, the higher the annual stroke risk.
Contraindication to anticoagulation
If a responsible physician had judged and documented that a patient had a contraindication to anticoagulation, this assessment was accepted.
Stroke/TIA
Stroke was diagnosed on the basis clinical symptoms and signs of stroke, including cerebral computed tomography, and reported in the patient’s medical record. TIA was diagnosed on the basis neurological symptoms and signs which disappeared within 24 hours.
Bleeding
Bleeding was defined as any clinically relevant bleeding, intra- or extracranial, and reported in the patient’s medical record.
Statistical analysis
Clinically relevant outcomes in comparing AF patients with and without anticoagulation therapy were the composite of ischemic stroke and/or bleeding within 12 months, which was considered as primary outcome in the analysis, ischemic stroke/TIA, mortality, bleeding and hospital care consumption.
Descriptive data are presented as number (percent) or mean (SD). Fisher’s exact test and Mann–Whitney U test were used for group comparisons regarding dichotomous and ordered/continuous variables, respectively. Kaplan–Meier estimates were used to assess cumulative incidence of outcomes and the log rank test was used for testing of difference between the two groups. For multivariable adjustment of potential confounders, defined as those variables (characteristics of AF patients) with a p < 0.20 for association with the composite outcome, Cox proportional hazards model was used. These potential confounders included chronic heart failure, malignancy, anemia and acute heart failure.
The p-values below 0.05 was regarded as statistically significant. SAS version 9.4 and SPSS version 22.0 for Windows were used for the statistical analysis.
Results
Baseline characteristics of AF- vs non-AF patients
Of 408 evaluable patients, 190 (46.6%) had a diagnosis of AF reported at the index care episode, while 218 patients (53.4%) had not (Figure 1). Baseline characteristics for both groups are presented in Table 1. In unadjusted analysis, the groups did not differ significantly in terms of age, gender, total morbidity burden, ADL, frailty score, living in residential care, own living with home help services, most of the studied diagnoses and duration of index hospital stay. These data also indicate that disabilities, ie, dependence or difficulty carrying out personal or instrumental ADL, were common, and both groups were also heavily affected by diseases, particularly cardiovascular disease. Differences between the groups were that the AF patients had a significantly higher baseline prevalence of hypertension and chronic heart failure compared to non-AF patients (both p < 0.001), had higher CHA2DS2-VASc scores (p = 0.003) and more often acute heart failure at index hospitalization (p < 0.001). Permanent AF was the most frequent type of AF (n = 115; 60.5%), the second most frequent type was paroxysmal AF (n = 69; 36.3%).
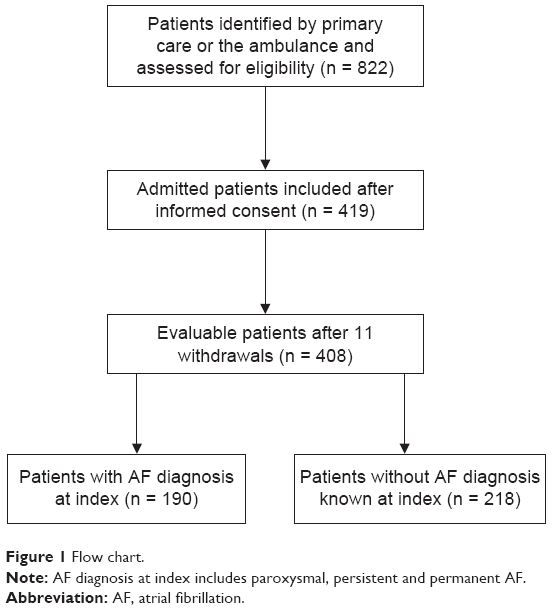 | Figure 1 Flow chart. |
 | Table 1 Baseline clinical and demographic characteristics of patients with AF diagnosis (n = 190) and patients without AF diagnosis (n = 218), reported during the index care episode, unadjusted analysis |
Baseline characteristics of AF-patients with or without anticoagulation
Baseline clinical and demographic characteristics of AF patients with (n = 119) and without anticoagulation (n = 71), as reported during the index care episode, are presented in Table 2. The following anticoagulation medications were used (n [%]): VKAs (warfarin) (95 [79.8]), LMWH (5 [4.2]), apixaban (16 [13.4]), dabigatran (1 [0.84]) and rivaroxaban (2 [1.7]). The groups did not differ significantly in terms of total morbidity burden, frailty score, most of the diagnoses studied, own living with home help services, CHA2DS2-VASc scores and duration of index hospital stay. The group of AF patients without anticoagulation were significantly older, more often females and more often in residential care. Furthermore, they had significantly worse MNA and ADL scores.
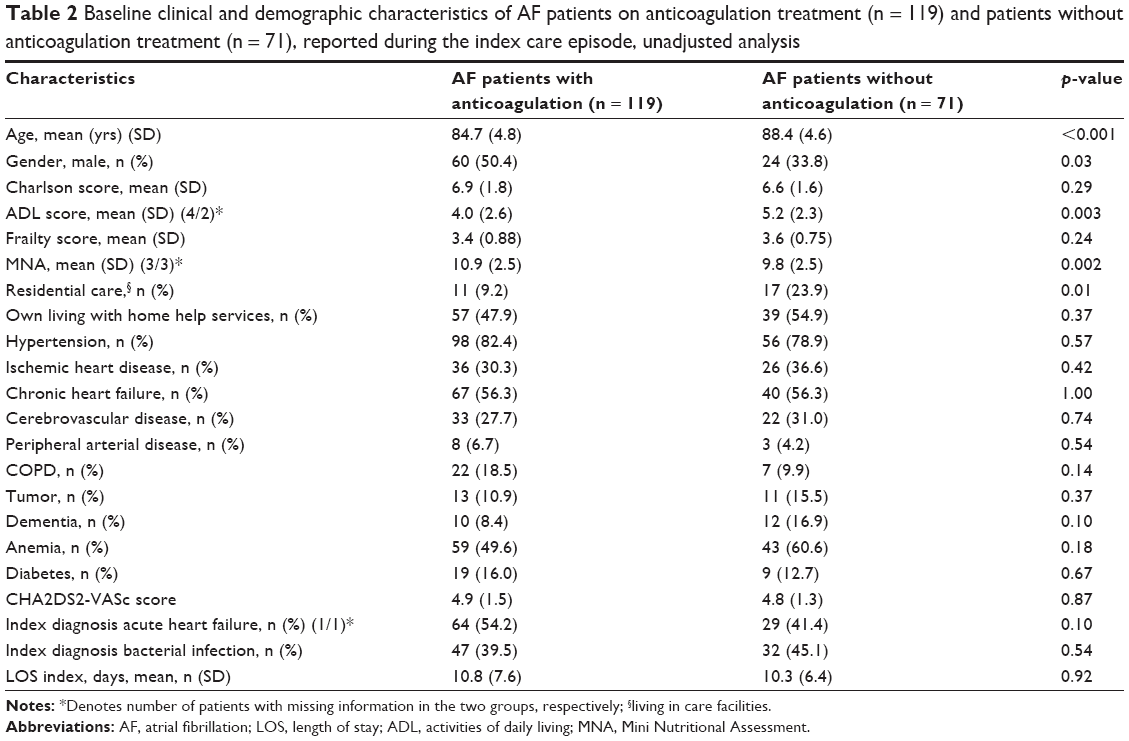 | Table 2 Baseline clinical and demographic characteristics of AF patients on anticoagulation treatment (n = 119) and patients without anticoagulation treatment (n = 71), reported during the index care episode, unadjusted analysis |
The distribution of CHA2DS2-VASc score in patients receiving anticoagulation and patients not receiving anticoagulation is shown in Figure 2. Both groups follow a normal distribution regarding scoring.
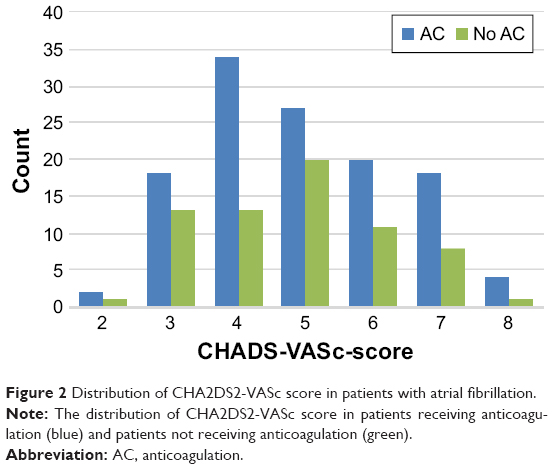 | Figure 2 Distribution of CHA2DS2-VASc score in patients with atrial fibrillation. |
Of the 71 patients without anticoagulation, 40 (56%) had a documented contraindication, while 31 (44%) had no reported contraindication. The most commonly stated contraindications in the medical records were: anemia, prior bleeding or bleeding disorder (9 cases); high age and decline in general condition (7 cases), high risk of falling (6 cases), dementia (5 cases), patient is unwilling to receive treatment (3 cases), other conditions or combinations of the listed conditions (10 cases).
Outcomes during 12 months’ follow-up of AF patients with or without anticoagulation
In univariate analysis, there were significantly more events among AF patients without anticoagulation regarding the composite outcome of ischemic stroke and/or bleeding (HR 3.65, 95% CI = 1.70–7.86; p < 0.001), as well as ischemic stroke (p = 0.02) and bleeding (p = 0.005) separately. There were no statistically significant differences between the groups regarding mortality, stroke/TIA, falls, fractures rehospitalizations or number of hospital days (Table 3).
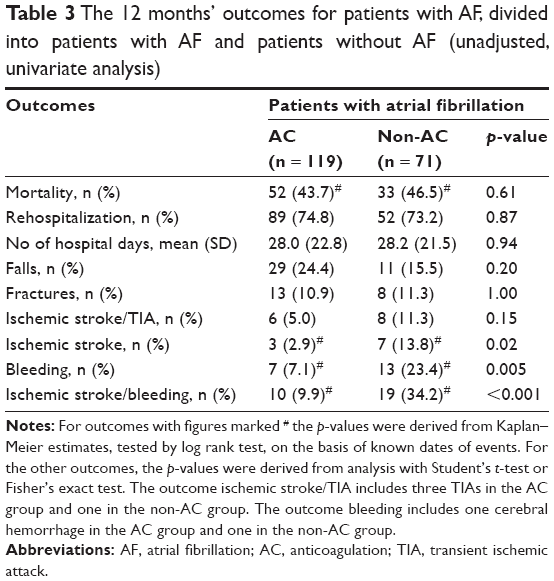 | Table 3 The 12 months’ outcomes for patients with AF, divided into patients with AF and patients without AF (unadjusted, univariate analysis) |
Four factors were identified as potential confounders regarding the composite outcome. These were chronic as well as acute heart failure, malignancy and anemia. When adjusting for these factors in Cox regression analysis, there were still significantly more composite outcome events among AF patients without anticoagulation than those with (HR 4.54, 95% CI = 1.83–11.25; p = 0.001).
Discussion
In this study, the prevalence of AF in a hospitalized frail elderly population was 47%. Among patients with AF, 63% were prescribed anticoagulation therapy. The group of AF patients without anticoagulation were older, more often females and more often in residential care, and they had worse MNA and ADL scores. In adjusted analyzes, the composite risk of ischemic stroke and/or bleeding was significantly higher in AF patients without anticoagulation than in patients with anticoagulation.
This study shows a high prevalence of AF in a hospitalized frail elderly population, higher than the previously published 38% in frail elderly patients.12 Our study included only acutely hospitalized frail elderly patients. The prevalence of AF in a frail elderly population in general is probably lower, as AF is a common cause of hospitalization, and as other acute conditions may trigger AF. Permanent AF was the most frequent type. This is in line with the results from a previous study, which found that about half of AF patients ≥80 years old had the permanent type.28
AF patients had a higher prevalence of hypertension and chronic heart failure, and higher CHA2DS2-VASc scores and more often acute heart failure at index hospitalization than patients without AF. These findings were not surprising, since there are causal relationships between these conditions.
About 63% of the AF patients were prescribed anticoagulants. Although lower than the recommended percentage level in Sweden of ≥80%, this proportion is slightly higher compared to Swedish data from 2013 when only 58% of AF patients received anticoagulation treatment.21 Furthermore, our study’s proportion of 63% is clearly higher than that in another recent study on elderly frail patients, showing a treatment rate of merely 17%.12 Possible explanations for the difference might be varying adherence to guidelines and different population characteristics. Other surveys report a treatment rate of up to 70%–80% in elderly patients in general, both frail and non-frail included.28,29
AF patients without anticoagulation treatment were older, more often females and more often in residential care, and they had worse MNA and ADL scores. However, notably, they did not differ from AF patients with anticoagulation in terms of CHA2DS2-VASc scores.
A total of 56% of the AF patients without anticoagulation had a documented contraindication in the medical records. We did not evaluate the contraindications stated in the hospital records in a structured way, ie, if the physician had judged that a patient had a contraindication we accepted that assessment. However, the validity of some of the contraindications can be discussed. Seven patients with high age and bad general condition reported contraindication for anticoagulation. It has been concluded that elderly patients benefit from anticoagulants unless they have a contraindication not including chronological age. Thus, it is not appropriate to exclude a patient from anticoagulation therapy with reference merely to age itself.29,30 In this study, if the AF patients not receiving anticoagulants and without documented contraindication should have been prescribed anticoagulation, the treatment level would have reached the recommended target level of 80% of all AF patients.
A previous publication reports an underuse of anticoagulation therapy in patients with the highest stroke risk.31 However, in our study there was no apparent difference in the CHA2DS2-VASc score distribution between AF patients with and without stroke prophylaxis. Both groups follow a normal distribution regarding scoring. One possible explanation is the very high mean age in this study.
There were significantly more events among AF patients without anticoagulation regarding clinically relevant bleeding, ischemic stroke and the composite outcome of ischemic stroke and/or bleeding. From a clinical point of view, these are highly relevant outcomes. It is essential to notice that bleeding events were more frequent in AF patients without anticoagulation therapy. This might reflect background characteristics of the patients in the two groups, ie, a higher perceived baseline bleeding risk in patients not receiving anticoagulants.
One strength of our study is that it included very frail elderly patients with a large morbidity burden, patients who usually are excluded from most clinical trials. Further, we studied clinically relevant outcomes, including ischemic stroke and/or important bleeding, with an appropriate follow-up period of 1 year. We performed different types of regression analyses, all with similar results, which indicate robust results. It is also a strength that the study included an analysis of documented contraindications, implying a balanced perspective of benefit and risk.
The study was based on secondary analyses of the TREEE study data, which might be considered a weakness, although studies on medications were outlined in the original study protocol. The study sample was mid-sized, and a larger number of patients would have strengthened the results. Twelve months is a relatively limited follow-up period for the events investigated in this study, and this study might have been underpowered to detect these event differences. On the other hand, considering the age and frailty of the population, a longer follow-up might have been very difficult to perform. Further, an even broader approach regarding drug therapy could be valuable in future research.32,33 We were not able to specifically investigate the effects of possible drug interactions. The contraindications judged and documented by the responsible physician were accepted. This resembles the decision-making in real-life health care. We lack 12-month data on the incidence of dementia or cognitive decline during the follow-up period. Although the associations between AF, anticoagulation and dementia is important to study,34,35 12 months might have been a too short follow-up period.
These frail elderly patients are rarely included in studies. It is important to continue research on these patients to be able to treat them in an effective and safe manner. This study shows a relatively high prevalence of stroke prophylaxis among frail elderly patients with atrial fibrillation compared to previous reports. Appropriately powered studies regarding anticoagulation treatment for frail elderly AF patients are needed in the future to evaluate if this represents a consistent trend. There are indications that CHA2DS2-VASc can be used to evaluate the risk of ischemic stroke/TIA and thromboembolism even in patients without AF.36 Similar analyses on frail patients without AF would be of interest. Furthermore, there is a need for long-term follow-up studies in order to appropriately address the association between AF, anticoagulation and dementia for very frail elderly patients.
Conclusion
This study showed a high prevalence of AF among frail elderly patients, and that many of these patients did not receive anticoagulation even if contraindications were not obvious. In adjusted analyses, the composite risk of ischemic stroke and/or bleeding was significantly higher among AF patients without anticoagulation compared with patients with anticoagulation. These results may be of interest to physicians who treat frail elderly patients, and of value in their clinical evaluation of AF patients for anticoagulation therapy.
Acknowledgments
This study was funded by grants from the Healthcare sub-committee, Region Västra Götaland; Department of Research and Development, NU Hospital Group; and the Fyrbodal Research and Development Council, Region Västra Götaland, Sweden.
Disclosure
Dr Björn W Karlson is an employee of AstraZeneca. The other authors report no conflicts of interest in this work.
References
World Health Organization (WHO). Fact sheet: Ageing and health 2015. Available from: http://www.who.int/mediacentre/factsheets/fs404/en/. Accessed September 17, 2017. | ||
Bergman H, Ferrucci L, Guralnik J, et al. Frailty: an emerging research and clinical paradigm. Issues and controversies. J Gerontol A: Biol Sci Med Sci. 2007;62(7):731–737. | ||
Morley JE, Vellas B, van Kan GA, et al. Frailty consensus: a call to action. J Am Med Direct Assoc. 2013;14(6):392–397. | ||
Chen X, Mao G, Leng SX. Frailty syndrome: an overview. Clin Interv Aging. 2014;9:433–441. | ||
Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A: Biol Sci Med Sci. 2001;56:146–156. | ||
Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173(5):489–495. | ||
Clegg A, Young J, Iliffe S, et al. Frailty in elderly people. Lancet. 2013;381(9868):752–762. | ||
Afilalo J, Alexander KP, Mack MJ, et al. Frailty assessment in the cardiovascular care of older adults. J Am Coll Cardiol. 2014;63(8):747–762. | ||
Woodard J, Gladman J, Conroy S. Frail older people at the interface. Age Ageing. 2010;39(S1):i36. | ||
Edmans J, Bradshaw L, Gladman J, et al. The Identification of Seniors at Risk (ISAR) score to predict clinical outcomes and health service costs in older people discharged from UK acute medical units. Age Ageing. 2013;42(6):747–753. | ||
Ekerstad N, Bylin K, Karlson BW. Early re-hospitalizations of frail elderly patients – the role of medications: clinical, prospective, observational trial. Drug Healthc Patient Saf. 2017;9:77–88. | ||
O’Caoimh R, Igras E, Ramesh A, Power B, O’Connor K, Liston R. Assessing the appropriateness of oral anticoagulation for atrial fibrillation in advanced frailty: use of stroke and bleeding risk-prediction models. J Frailty Aging. 2017;6(1):46–52. | ||
Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Rev Esp Cardiol (English Ed). 2017;70(1):50. | ||
Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22(8):983–988. | ||
Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383(9921):955–962. | ||
The Swedish National Board of Health and Welfare. National guidelines for cardiac healthcare. Scientific base for the anticoagulation treatment of atrial fibrillation. Supplement. 2015. Available from: https://www.socialstyrelsen.se/SiteCollectionDocuments/nr-stroke-antikoagulantia-2015-vetenskapligt-underlag.pdf. Accessed September 2017. | ||
Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA. 2001;285(22):2864–2870. | ||
Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137(2):263–272. | ||
Kakkar AK, Mueller I, Bassand JP, et al. Risk profiles and antithrombotic treatment of patients newly diagnosed with atrial fibrillation at risk of stroke: perspectives from the international, observational, prospective GARFIELD registry. PLoS One. 2013;8(5):e63479. | ||
Vallakati A, Lewis WR. Underuse of anticoagulation in patients with atrial fibrillation. Postgrad Med. 2016;128(2):191–200. | ||
The Swedish National Board of Health and Welfare. Target levels for cardiac care and stroke care 2014. Available from: https://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/19363/2014-2-19.pdf. Accessed September 2017. | ||
Ekerstad N, Karlson BW, Dahlin Ivanoff S, et al. Is the acute care of frail elderly patients in a comprehensive geriatric assessment unit superior to conventional acute medical care? Clin Interv Aging. 2017;12:1–9. | ||
Eklund K, Wilhelmsson K, Landahl S, Ivanoff Dahlin S. Screening for frailty among older emergency department visitors: Validation of the new FRESH-screening instrument. BMC Emerg Med. 2016;16(1):27. | ||
Sonn U, Asberg KH. Assessment of activities of daily living in the elderly. A study of a population of 76-year-olds in Gotherburg, Sweden. Scand J Rehabil Med. 1991:23:193–202. | ||
Rubenstein LZ, Stuck AE, Siu AL, Wieland D. Impacts of geriatric evaluation and management programs on defined outcomes: overview of the evidence. J Am Geriatr Soc. 1991;39(9 Pt 2):8S–16S; discussion 17S–18S. | ||
Charlson M, Pompei P, Ales K, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. | ||
Friberg L, Rosenqvist M, Lip GY. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182,678 patients with atrial fibrillation: the Swedish Atrial Fibrillation cohort study. Eur Heart J. 2012;33(12):1500–1510. | ||
Hanon O, Vidal JS, Le Heuzey JY, et al. Oral anticoagulant use in octogenarian European patients with atrial fibrillation: a subanalysis of PREFER in AF. Int J Cardiol. 2017;232:98–104. | ||
Poli D, Antonucci E, Testa S, et al. Bleeding risk in very old patients on vitamin K antagonist treatment: results of a prospective collaborative study on elderly patients followed by Italian Centres for Anticoagulation. Circulation. 2011;124(7):824–829. | ||
Mant J, Hobbs FD, Fletcher K, et al. Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study, BAFTA): a randomised controlled trial. Lancet. 2007;370(9586):493–503. | ||
Swedish Council on Health Technology Assessment (SBU) 2011. Atrial fibrillation; prevalence and risk of stroke. 2011 Available from: http://www.sbu.se/contentassets/0a28a5ac104d4f329ad8f839d19ca6f9/formaksflimmer_forekomst_risk_for_stroke.pdf. Accessed September 17, 2017. | ||
Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161–167. | ||
Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. Adverse drug events occurring following hospital discharge. J Gen Intern Med. 2005;20(4):317–323. | ||
Cacciatore F, Testa G, Langellotto A, et al. Role of ventricular response on dementia in cognitively impaired elderly subjects with atrial fibrillation: a 10-year study. Dement Geriatr Cogn Disord. 2012;34(3–4):143–148. | ||
Moffitt P, Lane DA, Park H, O’Connell J, Quinn TJ. Thromboprophylaxis in atrial fibrillation and association with cognitive decline: systematic review. Age Ageing. 2016;45(6):767–775. | ||
Liu FD, Shen XL, Zhao R, et al. Predictive role of CHADS2 and CHA2DS2-VASc scores on stroke and thromboembolism in patients without atrial fibrillation: a meta-analysis. Ann Med. 2016;48(5):367–375. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.