Back to Journals » Integrated Pharmacy Research and Practice » Volume 9
Hospital-Wide Medication Reconciliation Program: Error Identification, Cost-Effectiveness, and Detecting High-Risk Individuals on Admission
Authors Uhlenhopp DJ ![]() , Aguilar O, Dai D, Ghosh A
, Aguilar O, Dai D, Ghosh A ![]() , Shaw M, Mitra C
, Shaw M, Mitra C
Received 29 June 2020
Accepted for publication 22 August 2020
Published 13 October 2020 Volume 2020:9 Pages 195—203
DOI https://doi.org/10.2147/IPRP.S269857
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jonathan Ling
Dustin J Uhlenhopp,1 Oscar Aguilar,2 Dong Dai,3 Arka Ghosh,4 Michael Shaw,1 Chandan Mitra1
1Department of Internal Medicine, MercyOne Des Moines Medical Center, Des Moines, IA 50314, USA; 2Department of Business Administration, Grand View University, Des Moines, IA 50316, USA; 3Department of Mathematics, Iowa State University, Ames, IA 50011, USA; 4Department of Statistics, Iowa State University, Ames, IA 50011, USA
Correspondence: Dustin J Uhlenhopp
MercyOne Des Moines Medical Center, 1111 6 th Avenue, Des Moines, IA 50314, USA
Tel +1 515 643-2261
Fax +1 (515) 643-5802
Email [email protected]
Background: Medication reconciliation (MR) on admission has potential to reduce negative patient outcomes. The objectives of this prospective observational study were to 1) measure the impact a hospital-wide MR program has on home medication error identification at hospital admission, 2) demonstrate cost-effectiveness of this program, and 3) identify risk factors placing individual patients at higher risk for medication discrepancies.
Methods: Technicians obtained medication histories on adult patients admitted to the hospital that managed their own medications. Frequency and type of medication errors were recorded. Cost avoidance estimations were determined based on expected adverse drug event rates. Logistic regression analysis was used to test for associations between medication errors and patient characteristics. Results were considered significant when p-value was less than 0.05.
Results: The study included 817 patients. Technicians recorded a mean of 6.1 medication discrepancies per patient (SD ± 0.4) and took 28.5 minutes (SD ± 1.2 minutes) to complete a medication history. Omission, commission, and dosing/frequency errors occurred in 82%, 59%, and 50% of medication histories, respectively. We estimated cost avoidance of $210.33 per patient with this program. Female gender, age, and high alert/risk medication use were linked to an increase in the likelihood of occurrence of a medication discrepancy.
Conclusion: This study validated the ability of a pharmacy technician to identify errors, demonstrated economic cost-effectiveness, provided new data on time to obtain a BPMH, and further identified factors that contribute to the occurrence of medication discrepancies. Potentially harmful medication discrepancies were identified frequently on admission. With further research, it may be possible to identify those at highest risk for home medication discrepancies upon admission.
Keywords: medication safety, pharmacoeconomics, pharmacy administration, transitions of care, MARQUIS, drug information
Introduction
There is considerable evidence that medication discrepancies can affect patient outcomes.1,3,13 The Joint Commission noted in their 2020 National Patient Safety Goals (NPSG) the importance of reducing negative patient outcomes through medication reconciliation by attempting to identify and resolve medication discrepancies at hospital admission.1 The goal is to minimize discrepancies and thus improve outcomes. Medication reconciliation involves comparing the medications a patient reports taking against what a patient should be taking. This comparison should address duplications, omissions, interactions, medication adherence, and continued need for home medications. It is important for organizations to identify this information to safely prescribe medications while the patient is hospitalized.
This task is often complicated by a variety of factors, such as a patient utilizing multiple pharmacies, medication changes by care specialists, and medication non-adherence. This increases the risk for costly adverse medication errors in hospitalized patients. Some hospitals have begun to employ specialist pharmacy technicians to collect the best possible medication history (BPMH). Previous studies have indicated a positive impact on accuracy with error reductions upward of 88%2–5,22,25,26 but few studies have evaluated hospital-wide coverage from a fully developed program. It has been estimated that 39% of prescription medication history errors have the potential to cause moderate to severe discomfort or deterioration in a patient’s condition.3
Collecting the BPMH can be a challenging task. Ideally, this would detail recent medication changes, medication adherence, and the name, dose, route, and frequency of the medication a patient is currently taking.6 In some cases, a patient will arrive at the hospital with a medication list and/or medication bottles, but there is no guarantee this information is up-to-date or complete. Often, patients and/or their caregiver(s) must rely on recalling medications from memory, which also creates risk for omission and inaccuracies. Verification through an additional source, such as the patient’s pharmacy and/or providers’ office, helps to confirm accuracy and detect discrepancies.6 However, this additional verification may take a considerable amount of time and is not always feasible for the patient’s nurse or physician to complete. This is especially problematic whenever a patient utilizes multiple pharmacies, is cared for by various specialists, and/or takes numerous medications.
Due to the increased opportunity for error and the risk associated with these errors, there is a growing pool of literature on the topic of medication history programs.2–5,22–26 Many of these studies focus on emergency department-based pilot programs or individual departments within a hospital; however, there is little data evaluating these programs in a hospital-wide or institution-wide setting. There is also little data on what specific factors place an individual patient at higher risk for medication error upon admission to a hospital. Additionally, there remains a lack of evidence supporting the cost-effectiveness of medication history programs.23 It is vital that new research consider cost-effectiveness to ensure appropriate resource allocation for medication reconciliation services in order to meet Joint Commission recommendations.
The objectives of this study were to 1) measure to what degree a hospital-wide Medication History Technician (MHT) program identifies errors from home medications, 2) prove the cost-effectiveness of this error reduction on a large scale, and 3) identify risk factors placing individual patients at higher risk for medication discrepancies. We expect our institution will demonstrate similar rates of medication discrepancies of 1.1 to 11.5 medication discrepancies per admission seen in other studies13,14,16,24,25 as well as demonstrate a positive economic impact on our institution. As one of the largest programs of its kind, to our knowledge, a detailed study of the degree of error identification and its financial impact could benefit other healthcare facilities investigating implementation or expansion of pharmacy-led medication history programs.
Methods
Patient Selection
Our MHT program involves two hospitals within our city but the study focused on our 499-bed tertiary care hospital. We enrolled patients 18-years-old or older without any exclusions in gender, ethnic background, or health status that were admitted to our facility to receive medical treatment. Areas of the hospital involved included our critical care units, emergency department, and general medical floors. Within the emergency department, the MHTs completed as many medication histories as possible for patients prior to transfer to an inpatient floor. Direct admissions transferred from other hospitals were also included, provided they did not meet one of the below exclusion criteria.
Patients were recruited over seven weeks from October 2017 to December 2017. Readmission BPMHs were not included in this study if a patient was admitted more than once during the study period.
Exclusion Criteria
Our behavioral health unit and long-term rehabilitation unit were excluded as full medication histories are not completed by MHTs in these units. Pediatric and obstetric units were also excluded from evaluation. Patients that were admitted to the areas covered by the MHTs after a pre-scheduled surgery or catheterization were excluded as a medication history is obtained from staff in those areas prior to their procedure. Additionally, patients admitted from residential facilities that administer medications to the patient were excluded as the design of this study was to capture patients managing their own medications.
Best Possible Medication History Compilation
The BPMH was obtained in accordance with MARQUIS Implementation Manual guidelines via interview of the patient, patient’s caregiver(s), transferring hospital documentation, electronic health record (EHR) review, patient’s pharmacy(ies), and/or provider’s office.6 The process was designed to involve no clinical judgement on behalf of the MHTs. Medication entry was standardized to improve conversion to inpatient orders. Omission, commission, and dose/frequency errors were recorded. Errors were calculated by comparing the final list generated by the MHT against the initial list as provided by the patient. Omission errors were defined as medications the MHT determined the patient should be taking but the patient failed to identify as a medication they are or should be taking. Commission errors were defined as medications the patient reported as taking but the MHT determined the patient should not be taking, was discontinued previously, or the medication was expired. Dose/frequency errors were defined as errors in which the patient misidentified the dosage or how often they should take the medication. Home medications, as it relates to this study, were defined as any medication, both prescription and non-prescription (eg, herbal supplements, over-the-counter medications, vitamins), that a patient reported as taking and included details such as formulation (eg, extended release), dosage, route, and frequency.
A progress note went into the patient chart, listing time of last dose, any medication assistance the patient receives, reports of possible medication nonadherence, and comments regarding use of expired medications. An additional section to the progress note would be added for the use of any high-alert medications, as identified by the Institute for Safe Medication Practices (ISMP);7 these tended to mostly consist of antithrombotic agents, insulin, opioids, warfarin, and sulfonylurea hypoglycemics. The use of any direct oral anticoagulants, factor Xa inhibitors, and direct thrombin inhibitors were incorporated as high-alert medications in the study. The ISMP subsequently included these as high-alert medications in their acute care setting medication list that was released after our study was designed and data had been collected.8
A supervised training program was in place to ensure competency of each technician. Minimum standards for employment in our MHT program included a high school diploma or GED, 3000 hours of pharmacy technician experience, national certification through either the Pharmacy Technician Certification Board or National Healthcare Association, and the technician must have obtained their Pharmacy Technician Certification through the Iowa Board of Pharmacy. Passing scores on 10 direct and 10 indirect observations were required before a technician can operate independently as an MHT. Direct observations consisted of witnessing the trainee physically obtain the BPMH while indirect observations consisted of comparing the individually obtained BPMH by the trainer against the one obtained by the trainee. Quality assurance was performed annually for each technician through a shortened retesting protocol similar to the initial testing process. Our MHT program was an institution-wide entity for approximately two years prior to this study and utilized 17.5 technicians. MHT are staffed in the hospital between the hours of 07:00am to 01:00am all days of the week. Any admissions outside of these hours get added to the MHT’s work docket at 07:00am to ensure timely BPMH completion. All technicians were utilized to obtain the data in this study, and they did not record any data outside their normal scope of work. All technicians received special training on data collection and submission to ensure the data remained accurate and deidentified when transferred to the password-protected SQL database.
Providers at our facility postpone reconciliation until a BPMH is completed by an MHT in alliance with Society of Hospital Medicine recommendations that a BPMH be completed by someone other than the provider placing admission orders to maximize identification of unintentional discrepancies.6
Cost Analysis: Valuation and Cost Avoidance
The hospital’s cost for this intervention was determined by adding the MHT’s wages plus benefits multiplied by the average time required to perform a BPMH. The cost of a medication error in our study was based on the Bates et al study, which reported an estimate of $2595 in post-event costs for all in-hospital adverse drug events in 1996 dollars.9 Using an inflation adjustment ratio of 1.563 from 1996 to 2017 obtained from the US Bureau of Labor Statistics, we calculated the cost of an adverse drug event in 2017 dollars to be $4056. We used a separate Bates et al study,10 which determined harm occurred in 0.9% of all inpatient medication errors, to estimate the total costs of harm. This value was chosen over other studies, such as Boockvar et al,22 which demonstrated higher rates of adverse drug events to ensure a more conservative analysis. This percentage was used to determine the harmful errors per patient and multiplied by cost of an adverse drug event to determine cost avoidance per patient. We then compared the cost of our program against the potential cost avoidance.
Statistical Analysis
Logistic regression was utilized to test for associations between medication errors and patient characteristics including, but not limited to, age, gender, ethnicity/race, primary payor, and high-alert medication. All information collected from patients is included in Table 1. The Akaike Information Criterion27 was applied to develop a reduced model that eliminates variables from Table 1 that were deemed not significant. The likelihood ratio test was then applied to verify the reduced model. Statistical analysis was conducted using open-source software R, version 3.4.3 (R Core Team – 2017).
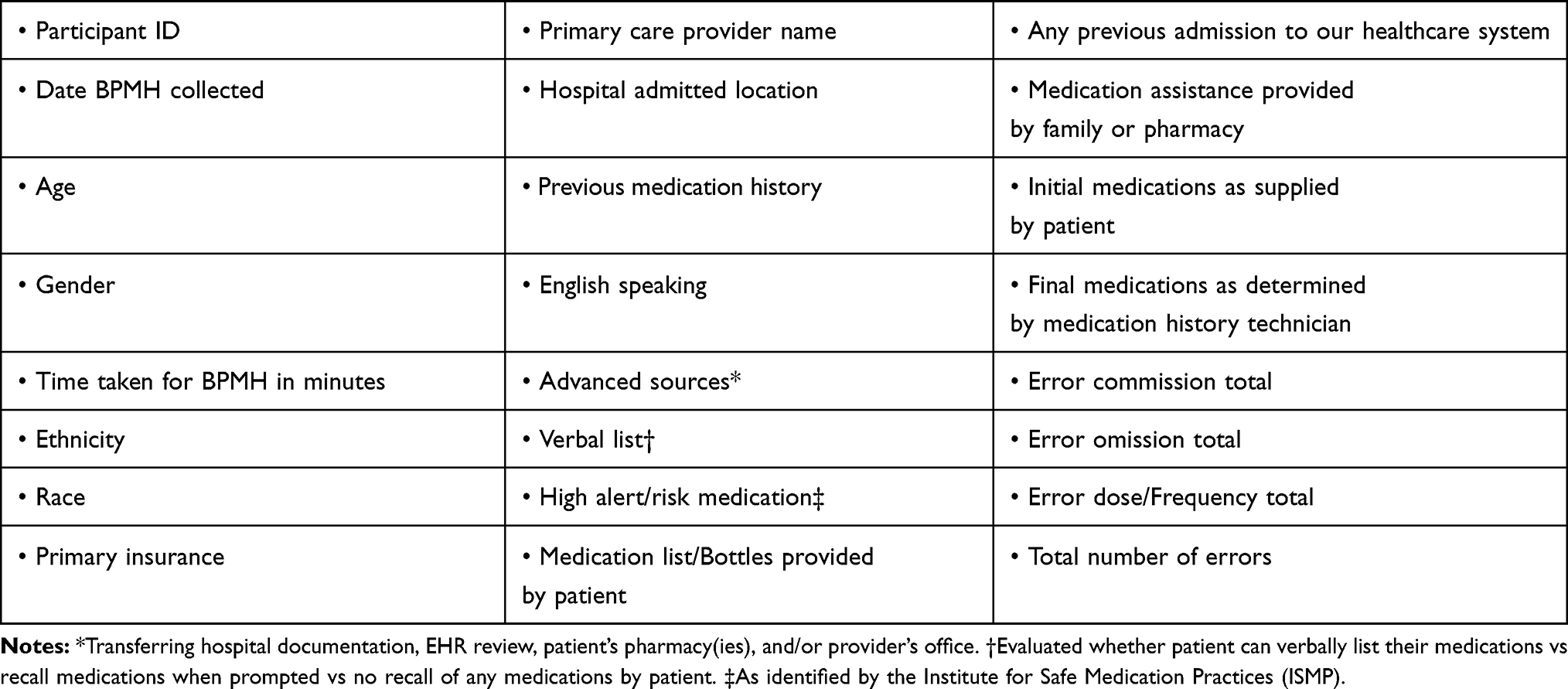 |
Table 1 Data Collected on Patients |
Ethical Considerations
Data from this study were sourced from information routinely collected by the MHTs as part of their medication history procedure. This study primarily focused on increased documentation of a process that is already completed for patients as they are admitted to our institution. Therefore, there was no risk above and beyond the regular MHT workflow. Written informed consent beyond consent to receive treatment was not necessary to obtain a medication history as this is already standard practice at our institution. The procedures were performed in accordance with the Declaration of Helsinki. The MercyOne institutional review board (IRB) approved the study protocol.
Results
We enrolled 817 patients in total. Seventy-four additional BPMHs were excluded due to readmission by a patient within the study period. Patient demographics are presented in Table 2. The mean age was 60 (SD ± 18.9). Our patients were 53% male, 84% white, and 55% received Medicaid or Medicare. High-alert medications were used by 55% of our patients, as identified by the ISMP8; these tended to mostly consist of antithrombotic/anticoagulant agents, insulin, opioids, and sulfonylurea hypoglycemics.
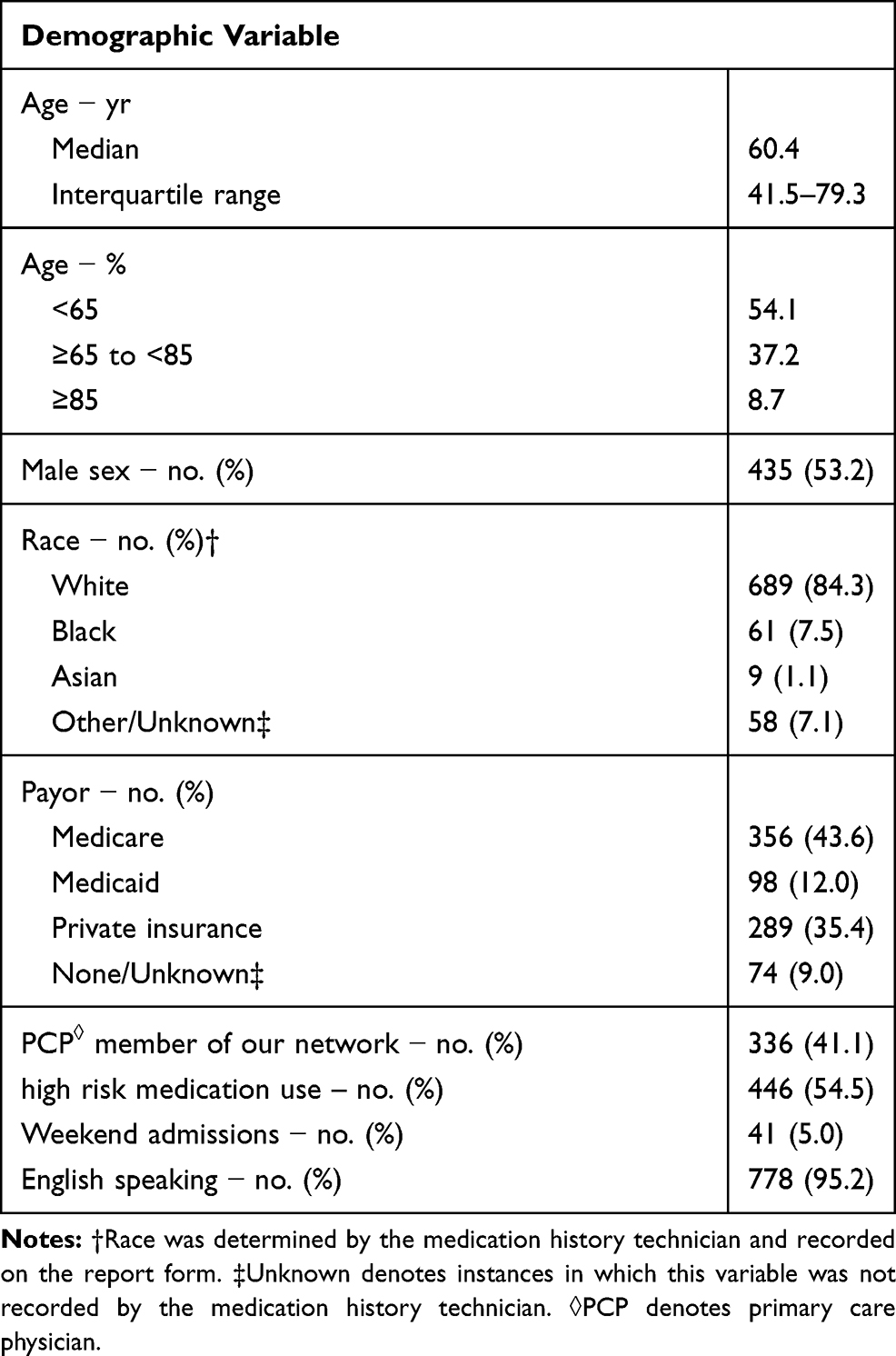 |
Table 2 Characteristics of the 817 Patients |
Prior to implementation of our MHT program, nursing staff within our hospital performed a BPMH <50% of the time spending an average of 5.7 minutes on a medication history (means of 1.2 minutes in the emergency department and 8.0 minutes in other locations). BPMH completion rates improved to 97% at the time of this study. We found that MHTs spent an average of 28.5 minutes (SD ± 1.2 minutes) interviewing, verifying, and documenting. Advanced sources were utilized on 94% of patients. An average of 6.1 potential errors (SD ± 0.4) per patient were identified. Omission of medications on admission was the most common discrepancy in 82% of patients with each patient committing 3.7 errors, on average, of this type (Table 3). Commission errors occurred in 59% of patients with each patient averaging 2.1 errors of this type. Errors in dosing/frequency occurred in 50% of medication histories in our study with each patient averaging 1.1 errors.
 |
Table 3 Error Types with Associated Average Number of Errors per Patient and the Associated Percent of Patients with These Errors in 817 Patients |
Our negative binomial regression reduced model identified female gender (p < 0.001) and high-alert medication use (p < 0.001) as being significant factors that increase the likelihood of the occurrence of a medication discrepancy. These high-alert medications consisted of medications identified by the Institute for Safe Medication Practices as clearly causing substantial patient harm if used in error.7,8 Additional analysis revealed availability of advanced sources to MHTs (p = 0.002) and patient provided medication list/medication bottles (p = 0.034) as significant aides in the technician’s ability to detect a medication discrepancy. Within our observational data we found that if a patient provided their own medication list or brought their medication bottles to the hospital, more errors were identified when compared to those who do not; 7.9 errors (SD ± 5.9) vs 6.3 errors (SD ± 5.0) respectively. Frequently, patients continued to take medications that had been discontinued by a provider previously and these discrepancies were subsequently identified by the MHT. If a patient was able to verbally list their own medications, they tended to have fewer errors when verified against other sources.
Poisson regression demonstrated that age contributes to the total errors made (p < 0.001). Change point detection identified a significant increase in average error at ages 32 and 89 when including both genders (Figure 1). Patients between ages 18–32 made an average of 3.4 errors. Patients between ages 33–89 made an average of 7.2 errors. Patients above age 89 made an average of 10.3 total errors. For male patients, the average error increased at age 44 and 86. Between ages 18–44, the average error made was 3.6 per male patient. Between ages 45–86, the average error made was 6.7 per male patient. Those above age 86 made an average of 10.5 errors. For female patients, the average total error increased at age 32. Female patients between ages 18–32 averaged 4.0 errors. Female patients above age 32 averaged 8.3 errors.
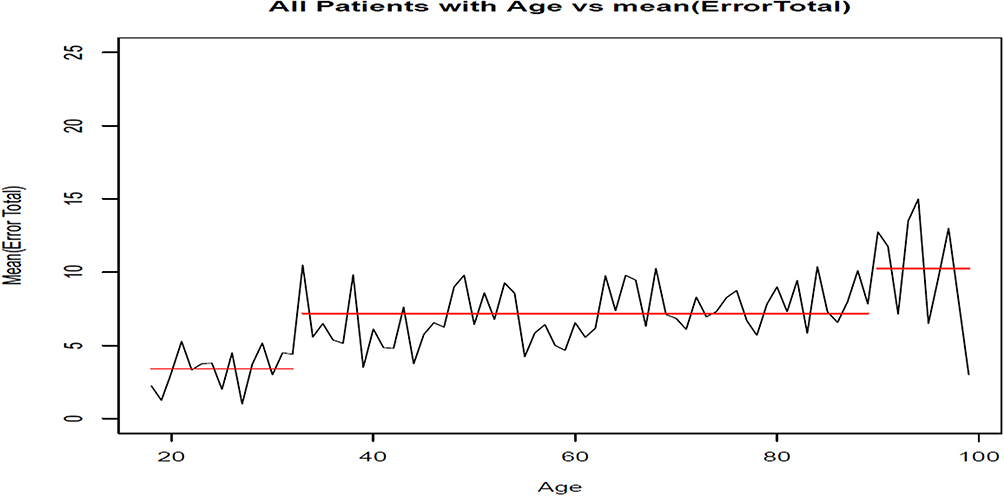 |
Figure 1 Change point detection of age against error total of all 817 patients. For both genders, a significant increase in average error was observed at age 32 and 89. Patients between ages 18–32 made an average of 3.4 errors. Patients between ages 33–89 made an average of 7.2 errors. Patients above age 89 made an average of 10.3 errors. |
The data show that patients coming from outside of our affiliation of Primary Care Providers did not have more errors than our in-network affiliates (mean 7.0 total errors vs 6.8, respectively). Utilizing an unpaired t-test, our data also suggest admission over the weekend has no effect on pre-existing medication errors (p = 0.757); 5.0% of admissions occurred over the weekend during the study. Attempts were made to observe differences in ethnicity, race, and primary language but we felt the homogeneity of our patient population did not allow for meaningful analysis.
There was a significant association with use of high-alert medications by Medicaid (odds ratio, 1.654; 95% CI, 1.041–2.626) or Medicare (odds ratio, 2.105; 95% CI 1.534–2.888) patients when compared to private insurance.
Cost Analysis
MHTs receive $26.00 per hour (benefits included) and they spent 28.5 minutes (SD ± 1.2 minutes) performing a BPMH resulting in a cost for this intervention of $12.37 per patient. Using a $2595 estimate for in-hospital adverse drug event in 1996 and adjusting to 2017 dollars with a US Bureau of Labor Statistics inflation adjustment ratio of 1.563 resulted in an estimated cost of $4056 for an adverse drug event. Assuming 0.9% of all inpatient medication errors lead to harm, the average error per patient of 6.1 is multiplied by 0.9% which results in 0.0549 harmful errors avoided per patient by identifying the medication discrepancies.10 Multiplying the estimated cost of an adverse drug event in 2017 dollar by the number of harmful errors avoided per patient then subtracting the cost of the intervention results in a cost avoidance estimate of $210.33 per patient. This results in greater than $1,600,000 per year in net savings to our 499-bed moderate-sized not-for-profit hospital without consideration for the cost avoidance benefits of our MHT program at our other hospitals within our system.
Discussion
To our knowledge, this prospective observational study of a large institution-wide medication reconciliation program is the largest to date. This study validates the ability of a pharmacy technician to identify medication discrepancies, demonstrates economic cost-effectiveness, provides new data on time to obtain a BPMH, and further identifies factors that contribute to the occurrence and detection of medication discrepancies.
Significant resources are required by health systems to implement and manage MHT programs. It is not sufficient to show effectiveness of error identification. It is important, in resource limited health systems, to demonstrate that such investments constitute value for the organization. It is worth mentioning that this study was originally born out of the requirement from our institution to demonstrate economic viability of our MHT program. To combat potential biases, we purposefully utilized more conservative adverse drug event rates as detailed by Bates et al.10 It should also be noted that not all adverse drug events result in harm. Regardless, the Joint Commission has mandated appropriate resources be allocated for inpatient medication reconciliation as an essential patient safety process. We feel the cost of this intervention, by employing dedicated Medication History Technicians, to be of significant resource utilization benefit while ensuring appropriate error identification. Our institution employs 17.5 MHTs, which we believe reduces the cost of healthcare. Each adverse drug event is estimated to cost approximately $4050. Obtaining a BPMH costs approximately $12 per patient. Thus, preventing one adverse drug event in roughly 330 patients would constitute a “breakeven” point.
Multiple previous studies have shown medication discrepancies to be a common occurrence in tertiary centers with identified unintentional errors on admission ranging from 30% to 70%.1,13–16,24,25,28 It is well established that these errors can lead to significant patient discomfort or clinical deterioration.1,13 Previous studies have consistently shown omission of a medication as the most common error.13,15,28 Our study supports this growing body of literature, as 82% of patients had an omission error, 59% had a commission error, and 50% had an error in dosing or frequency in their medication histories.
Our study demonstrated a higher rate of error identification than seen in most previous studies with a mean of 6.1 total medication discrepancies (SD ± 0.4) per patient. Most previous studies have shown a discrepancies per admission rate of 1.1 to 2.813,14,24,25 though Pippins et al16 demonstrated a rate of 11.5 medication discrepancies per admission. The differences in discrepancies seen between studies are not readily apparent but likely lies in the differing definitions of unintentional discrepancies/errors, age groups evaluated, and ascertainment of adverse drug events between each study. One explanation for our higher medication error may lie in the significant number of advanced sources available to our MHTs when compiling the BPMH. These advanced sources, which were utilized in 94% of the BPMHs, typically included transferring hospital documentation, access to multiple electronic health record systems, patient’s pharmacies, and contacting provider’s offices. Another explanation may include our medication error definitions. For instance, if an MHT determined a patient should be taking 4 different medications, but the patient could only recall one of their medications, this was documented as 3 omission errors.
Increasing age was a significant factor in medication discrepancies, which is consistent with previous studies;11,12,14,17 significant (p < 0.001) rises in error can be seen for all patients at ages 32 and 89 in our study (Figure 1).
Additional significant factors include female gender, high-alert medication use, availability of advanced sources for use by MHTs, history of previous admission, and patient provided medication lists/bottles. The association with gender is not readily clear to the authors. Gender as an influence on medication error is controversial; a previous systematic review found 5 out of 24 studies had an association between gender and frequency of medication error though not every study reported on gender.17 Our data suggest that patients on high-alert medications presenting to our hospital are likely to have more medication discrepancies (Figure 2). The importance of obtaining the BPMH in these patients is especially necessary as these particular errors can be devastating if not discovered.
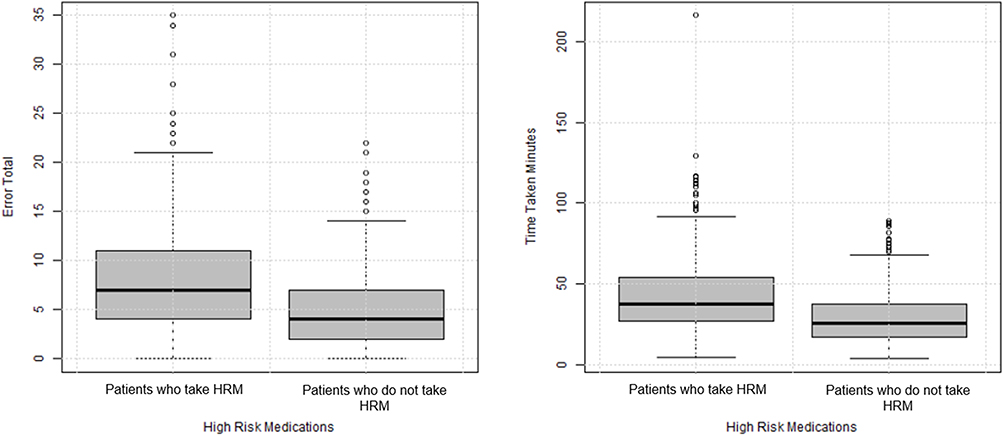 |
Figure 2 Error Total per BPMH against patients taking high alert/risk medications (HRM) and those who do not take HRM. These medications are as identified by the Institute for Safe Medication Practices and include antithrombotic agents, insulin, opioids, sulfonylurea hypoglycemics, and anticoagulants agents. There were 446 patients taking HRM with a mean error total of 8.3. There were 371 patients not taking HRM with a mean error total of 5.2. |
As expected, when patients brought in their own medication list or brought in all their medications at admission, the likelihood of detecting discrepancies was increased. Several from this group of patients had continued taking medications that were discontinued previously and may have played a role in their hospitalization during this study. This was also coupled with the finding that if a patient was able to list all their medications from memory, they tended to have fewer medication discrepancies identified when verifying each group of patients through advanced sources. This may simply be that those who memorized their medications are more involved in their own care or the reason may perhaps be more nuanced. Previous studies demonstrate positive correlations of patient medication knowledge with higher education level, frequent office visits, trust in their primary care provider, and use of fewer medications which were factors not evaluated in this study.18–21 With continued emphasis on medication safety, there should be improved processes in place to encourage patients and caregivers to bring in their medications to aid with admission, as well as improved resources for technicians to better access a patient’s other medication data. Further research in this area could evaluate the effects of disposing of old medications prior to discharge on readmission rates, patient adherence to discharge medication lists, and other adverse events affecting patients after discharge from the hospital.
The time to complete a BPMH in our study should be encouraging, particularly for institutions that treat high percentages of high complexity patients. Our MHTs completed BPMH with a mean time of 28.5 minutes, which aligns with the recommended time frame by the Society of Hospital Medicine of 20–30 minutes.7 It is faster than other trials that used individuals with higher levels of training, such as the pharmacist-led pilot study by Cadman et al,24 were the mean total time was 48.6 minutes (range 2–195 min). Our MHT program was in place for two years at the time of this study suggesting that resource utilization will become more efficient for institutions after their MHT programs have time to develop. Of note, we also noticed that more time was required to perform a BPMH when more errors were identified. This satisfies our anecdotal experiences that more errors identified require more time and effort to document/correct.
There are several limitations to our study. First, our protocol had no control group that allowed for monitoring how many errors existed at baseline. This was a within-subject study. We relied heavily on previous literature that has demonstrated dedicated MHTs can appropriately identify errors when adequately trained.2,4,5,15 We did not attempt to identify that an adverse medication error would have occurred had a BPMH not been completed. We followed Society of Hospital Medicine best practice recommendations that the BPMH be completed by someone other than the admitting provider to maximize identification of unintentional errors.6 Thus, we do not have a comparator group to evaluate whether or not the providers would have identified similar errors. Ideally, future studies will evaluate the potential gravity of discrepancies for the patient if not detected. Second, the anticipated number for the study was originally 1400 over four weeks but zealous recruitment estimates and financial restrictions placed by our institution ended the study at seven weeks with 817 BPMHs completed. We present our study as observational data. Third, attempts were made to observe differences in ethnicity, race, and primary language but the homogeneity of our patient population at our Midwest hospital did not allow for significant analysis of these factors. Fourth, though our MHT program involves multiple hospitals within our institution, this study was only carried out in our largest hospital. Additionally, our study focused solely on admission medication histories/reconciliation so our results may not be generalizable to other levels of transition of care. Finally, our cost estimates and rates for adverse drug events are largely derived from two studies from 1995 to 1997. Adjusting for inflation may not adequately account for the true cost at the time of this study.
In conclusion, this study enforces the importance of performing medication reconciliation and demonstrates the cost-effectiveness of a medication history technician program. It identifies patient age and gender as irreversible risk factors and high-alert medication use as a potentially modifiable risk factor that increases the likelihood of the occurrence of medication discrepancies. History of previous hospitalization to our health system, patient provided medication lists, and availability of advanced sources were identified as independent risk factors for identifying medication discrepancies on admission and highlight the importance of utilizing multiple sources when obtaining the BPMH. This study notes that Medicare and Medicaid patients tend to be on high-alert medications more often than patients on private insurance and that admission on the weekend did not influence discrepancy identification. The most common error was “omission” and occurred in eight of every ten patients on average admitted to the hospital.
Disclosure
The authors report no conflicts of interest for this work.
References
1. The Joint Commission Web site. The Joint Commission National Patient Safety Goals Effective January 2020 Hospital Accreditation Program. https://www.jointcommission.org/-/media/tjc/documents/standards/national-patient-safety-goals/npsg_chapter_hap_jan2020.pdf. Accessed December 14, 2019.
2. Mekonnen AB, McLachlan AJ, Brien JE. Pharmacy-led medication reconciliation programmes at hospital transitions: a systematic review and meta-analysis. J Clin Pharm Ther. 2016;41(2):128–144. doi:10.1111/jcpt.12364
3. Tam VS, Knowles SR, Cornish PL, et al. Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review. CMAJ. 2005;173(3):510–515. doi:10.1503/cmaj.045311
4. Rubin EC, Pisupati R, Nerenberg SF. Utilization of Pharmacy Technicians to Increase the Accuracy of Patient Medication Histories Obtained in the Emergency Department. Hosp Pharm. 2016;51(5):396–404. doi:10.1310/hpj5105-396
5. Smith L, Mosley J, Lott S, et al. Impact of pharmacy-led medication reconciliation on medication errors during transition in the hospital setting. Pharm Pract (Granada). 2015;13(4):634. doi:10.18549/PharmPract.2015.04.634
6. Society of Hospital Medicine Web site. MARQUIS Implementation Manual A Guide for Medication Reconciliation Quality Improvement. http://tools.hospitalmedicine.org/resource_rooms/imp_guides/MARQUIS/Marquis_Manual2011.pdf.; 2011.
7. Institute for Safe Medication Practices Web site. ISMP List of High-Alert Medications in Community/Ambulatory Healthcare. https://www.ismp.org/recommendations/high-alert-medications-community-ambulatory-list; 2011.
8. Institute for Safe Medication Practices Web site. ISMP List of High-Alert Medications in Acute Care Settings. https://www.ismp.org/recommendations/high-alert-medications-acute-list.; 2018.
9. Bates DW, Spell N, Cullen DJ, et al. The costs of adverse drug events in hospitalized patients. Adverse Drug Events Prevention Study Group. JAMA. 1997;277(4):307–311. doi:10.1001/jama.1997.03540280045032
10. Bates DW, Boyle DL, Vander Vliet MB, Schneider J, Leape L. Relationship between medication errors and adverse drug events. J Gen Intern Med. 1995;10(4):199–205. doi:10.1007/BF02600255
11. Kantor ED, Rehm CD, Haas JS, Chan AT, Giovannucci EL. Trends in Prescription Drug Use Among Adults in the United States From 1999–2012. JAMA. 2015;314(17):1818–1831. doi:10.1001/jama.2015.13766
12. Martin CB, Hales CM, Gu Q, Ogden CL. Prescription Drug Use in the United States, 2015–2016. NCHS Data Brief. 2019;334:1–8.
13. Cornish PL, Knowles SR, Marchesano R, et al. Unintended medication discrepancies at the time of hospital admission. Arch Intern Med. 2005;165(4):424–429. doi:10.1001/archinte.165.4.424
14. Van Der Luit CD, De Jong IR, Ebbens MM, et al. Frequency of occurrence of medication discrepancies and associated risk factors in cases of acute hospital admission. Pharm Pract (Granada). 2018;16(4):1301. doi:10.18549/PharmPract.2018.04.1301
15. Feldman LS, Costa LL, Feroli ER, et al. RN‐Pharmacist Medication Reconciliation. J Hosp Med. 2012;5(5):396–401. doi:10.1002/jhm.1921
16. Pippins JR, Gandhi TK, Hamann C, et al. Classifying and predicting errors of inpatient medication reconciliation. J Gen Intern Med. 2008;23(9):1414–1422. doi:10.1007/s11606-008-0687-9
17. Hias J, Van der Linden L, Spriet I, et al. Predictors for unintentional medication reconciliation discrepancies in preadmission medication: a systematic review. Eur J Clin Pharmacol. 2017;73(11):1355–1377. doi:10.1007/s00228-017-2308-1
18. Ramia E, Zeenny RM, Hallit S, Salameh P. Order of Pharmacists Scientific Committee – medication Safety Subcommittee. Assessment of patients’ knowledge and practices regarding their medication use and risks in Lebanon. Int J Clin Pharm. 2017;39(5):1084–1094. doi:10.1007/s11096-017-0517-4
19. Romero-Sanchez J, Garcia-Cardenas V, Abaurre R, Martínez-Martínez F, Garcia-Delgado P. Prevalence and predictors of inadequate patient medication knowledge. J Eval Clin Pract. 2016;22(5):808–815. doi:10.1111/jep.12547
20. AlRuthia Y, Almalag H, Sales I, et al. The relationship between trust in primary care physicians and medication knowledge among diabetic patients. Res Social Adm Pharm. 2019;15(6):656–661. doi:10.1016/j.sapharm.2018.08.004
21. Huang YM, Yang YH, Lin SJ, Chen KC, Kuo CC, Wu FL. Medication knowledge to be improved in participants in community universities in Taiwan: outcome of a nationwide community university program. J Formos Med Assoc. 2015;114(12):1267–1279. doi:10.1016/j.jfma.2014.12.001
22. Boockvar KS, Blum S, Kugler A, et al. Effect of Admission Medication Reconciliation on Adverse Drug Events From Admission Medication Changes. Arch Intern Med. 2011;171(9):860–861. doi:10.1001/archinternmed.2011.163
23. Hammad EA, Bale A, Wright DJ, Bhattacharya D. Pharmacy led medicine reconciliation at hospital: A systematic review of effects and costs. Res Social Adm Pharm. 2017;13(2):300–312. doi:10.1016/j.sapharm.2016.04.007
24. Cadman B, Wright D, Bale A, et al. Pharmacist provided medicines reconciliation within 24 hours of admission and on discharge: a randomised controlled pilot study. BMJ Open. 2017;7(3):e013647. doi:10.1136/bmjopen-2016-013647
25. Beckett RD, Crank CW, Wehmeyer A. Effectiveness and feasibility of pharmacist-led admission medication reconciliation for geriatric patients. J Pharm Pract. 2012;25(2):136–141. doi:10.1177/0897190011422605
26. Choi YJ, Kim H. Effect of pharmacy-led medication reconciliation in emergency departments: A systematic review and meta-analysis. J Clin Pharm Ther. 2019;44(6):932–945. doi:10.1111/jcpt.13019
27. Portet S. A primer on model selection using the Akaike Information Criterion. Infect Dis Model. 2020;5:111–128. doi:10.1016/j.idm.2019.12.010
28. Karaoui LR, Chamoun N, Fakhir J, et al. Impact of pharmacy-led medication reconciliation on admission to internal medicine service: experience in two tertiary care teaching hospitals. BMC Health Serv Res. 2019;19(1):493. doi:10.1186/s12913-019-4323-7
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.