Back to Journals » Patient Preference and Adherence » Volume 17
Hopelessness in Patients with Early-Stage Relapsing-Remitting Multiple Sclerosis
Authors Sainz de la Maza S, Maurino J ![]() , Castillo-Triviño T, Borges M
, Castillo-Triviño T, Borges M ![]() , Sebastián Torres B, Sotoca J, Alonso Torres AM, Caminero AB, Borrega L, Sánchez-Menoyo JL
, Sebastián Torres B, Sotoca J, Alonso Torres AM, Caminero AB, Borrega L, Sánchez-Menoyo JL ![]() , Barrero-Hernández FJ
, Barrero-Hernández FJ ![]() , Calles C, Brieva L, Blasco MR, Dotor García-Soto J, Rodríguez-Regal A, Navarro-Cantó L, Agüera-Morales E, Garcés M, Carmona O
, Calles C, Brieva L, Blasco MR, Dotor García-Soto J, Rodríguez-Regal A, Navarro-Cantó L, Agüera-Morales E, Garcés M, Carmona O ![]() , Gabaldón-Torres L, Forero L
, Gabaldón-Torres L, Forero L ![]() , Hervás M, Gómez-Ballesteros R
, Hervás M, Gómez-Ballesteros R ![]()
Received 4 March 2023
Accepted for publication 25 May 2023
Published 14 June 2023 Volume 2023:17 Pages 1431—1439
DOI https://doi.org/10.2147/PPA.S411069
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Susana Sainz de la Maza,1 Jorge Maurino,2 Tamara Castillo-Triviño,3 Mónica Borges,4 Berta Sebastián Torres,5 Javier Sotoca,6 Ana María Alonso Torres,7 Ana B Caminero,8 Laura Borrega,9 José L Sánchez-Menoyo,10 Francisco J Barrero-Hernández,11 Carmen Calles,12 Luis Brieva,13 María Rosario Blasco,14 Julio Dotor García-Soto,4 Ana Rodríguez-Regal,15 Laura Navarro-Cantó,16 Eduardo Agüera-Morales,17 Moisés Garcés,18 Olga Carmona,19 Laura Gabaldón-Torres,20 Lucía Forero,21 Mariona Hervás,22 Rocío Gómez-Ballesteros2
1Department of Neurology, Hospital Universitario Ramón y Cajal, Madrid, Spain; 2Medical Department, Roche Farma, Madrid, Spain; 3Department of Neurology, Hospital Universitario Donostia, San Sebastián, Spain; 4Department of Neurology, Hospital Universitario Virgen Macarena, Sevilla, Spain; 5Department of Neurology, Hospital Universitario Miguel Servet, Zaragoza, Spain; 6Department of Neurology, Hospital Universitari Vall d´Hebrón, Barcelona, Spain; 7Department of Neurology, Hospital Regional Universitario de Málaga, Málaga, Spain; 8Department of Neurology, Complejo Asistencial de Ávila, Ávila, Spain; 9Department of Neurology, Hospital Universitario Fundación Alcorcón, Alcorcón, Spain; 10Department of Neurology, Hospital de Galdakao-Usansolo, Galdakao, Spain; 11Department of Neurology, Hospital Universitario Clínico San Cecilio, Granada, Spain; 12Department of Neurology, Hospital Universitari Son Espases, Palma de Mallorca, Spain; 13Department of Neurology, Hospital Universitari Arnau de Vilanova, Lleida, Spain; 14Department of Neurology, Hospital Universitario Puerta de Hierro, Madrid, Spain; 15Department of Neurology, Complexo Hospitalario Universitario de Pontevedra, Pontevedra, Spain; 16Department of Neurology, Hospital General Universitario de Elche, Elche, Spain; 17Department of Neurology, Hospital Universitario Reina Sofía, Córdoba, Spain; 18Department of Neurology, Hospital Clínico Universitario Lozano Blesa, Zaragoza, Spain; 19Department of Neurology, Fundació Salut Empordà, Figueres, Spain; 20Department of Neurology, Hospital Francesc de Borja, Gandía, Spain; 21Department of Neurology, Hospital Universitario Puerta del Mar, Cádiz, Spain; 22Department of Neurology, Consorci Corporació Sanitària Parc Taulí, Sabadell, Spain
Correspondence: Jorge Maurino, Medical Department, Roche Farma, Ribera del Loira, 50, Madrid, 28042, Spain, Tel +34 913 24 81 00, Email [email protected]
Background: Hopelessness is a risk factor for depression and suicide. There is little information on this phenomenon among patients with relapsing-remitting multiple sclerosis (RRMS), one of the most common causes of disability and loss of autonomy in young adults. The aim of this study was to assess state hopelessness and its associated factors in early-stage RRMS.
Methods: A multicenter, non-interventional study was conducted. Adult patients with a diagnosis of RRMS, a disease duration ≤ 3 years, and an Expanded Disability Status Scale (EDSS) score of 0– 5.5 were included. The State-Trait Hopelessness Scale (STHS) was used to measure patients´ hopelessness. A battery of patient-reported and clinician-rated measurements was used to assess clinical status. A multivariate logistic regression analysis was conducted to determine the association between patients’ characteristics and state hopelessness.
Results: A total of 189 patients were included. Mean age (standard deviation-SD) was 36.1 (9.4) years and 71.4% were female. Median disease duration (interquartile range-IQR) was 1.4 (0.7, 2.1) years. Symptom severity and disability were low with a median EDSS (IQR) score of 1.0 (0, 2.0). A proportion of 65.6% (n=124) of patients reported moderate-to-severe hopelessness. Hopelessness was associated with older age (p=0.035), depressive symptoms (p=< 0.001), a threatening illness perception (p=0.001), and psychological and cognitive barriers to workplace performance (p=0.029) in the multivariate analysis after adjustment for confounders.
Conclusion: Hopelessness was a common phenomenon in early-stage RRMS, even in a population with low physical disability. Identifying factors associated with hopelessness may be critical for implementing preventive strategies helping patients to adapt to the new situation and cope with the disease in the long term.
Keywords: relapsing-remitting multiple sclerosis, hopelessness, depressive symptoms, workplace difficulties, suicide
Introduction
Hopelessness is a psychological construct defined as negative expectations characterized by the feeling that one lacks control over events in the future and is a known risk factor for depression and suicide behavior.1,2 Hopelessness can either represent a personality trait or a state in response to negative events. It is a phenomenon associated with poor outcome that has been studied in the general population and in patients with several medical conditions, including cancer and ischemic heart disease.3–5
Multiple sclerosis (MS) is a chronic autoimmune neurological disease that causes disability and poor quality of life mainly in active people between 20 and 40 years of age.6,7 Most patients have a relapsing-remitting form of the disease (RRMS), characterized by attacks or relapses of sensorial symptoms, weakness, vision and gait problems followed by periods of stability with recovery that may be complete or incomplete.6,8 The uncertainty of the long-term trajectory of the disease, the frequency and severity of residual symptoms, and the lack of curative treatments provide a context for the development of hopelessness, anxiety and mood disorders among MS patients.7,9–12 The risk of suicide is almost two times higher in patients with MS than in the general population, especially at the time of diagnosis.10 However, there is limited information about the phenomenon of hopelessness in patients with a recent diagnosis of MS.13,14 As a modifiable risk factor in suicidal behavior, the aim of this study was to assess the presence of state hopelessness and its associated factors in early-stage RRMS.
Methods
A non-interventional, cross-sectional study was conducted at 21 hospital-based MS Care Units in Spain. We recruited adult patients with a diagnosis of RRMS (2017 revised McDonald criteria), a disease duration no longer than 3 years, and an Expanded Disability Status Scale (EDSS) score from 0 to 5.5 in the context of their routine follow-up visits.15,16 Patients were invited to participate in the study by their treating neurologists in the context of their regular follow-up visits.
This study was reviewed and approved by the ethical review board of the Hospital Universitari Arnau de Vilanova (Lleida, Spain) and performed in accordance with the 1964 Helsinki Declaration and its later amendments. All participants provided a written informed consent.
Measures
The State-Trait Hopelessness Scale (STHS) was used to measured patients´ hopelessness.17 The STHS is a validated, self-rated instrument to differentiate trait (13 items) and state (10 items) hopelessness in research and clinical practice. Each subscale is measured on a 4-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree). Higher scores indicate higher levels of hopelessness.17 A cut-off score ≥1.8 was used to define the presence of moderate-to-severe trait and state hopelessness.5 We focused on state rather than trait hopelessness, as this can be addressed by short-term interventions that could be implemented in the multidisciplinary setting of MS Care Units.
Table 1 shows details of patient-reported and clinician-rated outcome measures administered. The SymptoMScreen (SyMS), 5-item Modified Fatigue Impact Scale (MFIS-5), a pain visual analog scale, Hospital Anxiety and Depression Scale (HADS), Multiple Sclerosis Impact Scale (MSIS-29), Brief-Illness Perception Questionnaire (B-IPQ), Stigma Scale for Chronic Illness (SSCI-8), 5-item Perceived Deficit Questionnaire (PDQ-5) and Multiple Sclerosis Work Difficulties Questionnaire (MSWDQ-23) were used to assess patients´ perception of symptom severity, fatigue, pain, mood and anxiety, health-related quality of life, illness representation, perception of stigma, cognition, and work-related problems, respectively.18–25 The EDSS, Symbol Digit Modalities Test (SDMT), 9-Hole Peg Test (9-HPT), and Timed 25-Foot Walk (T25-FW) were administered by clinicians to assess disability, cognition, hand dexterity, and gait, respectively.16,26–28 Questionnaires were administered through an electronic tablet and completed online at the hospital.
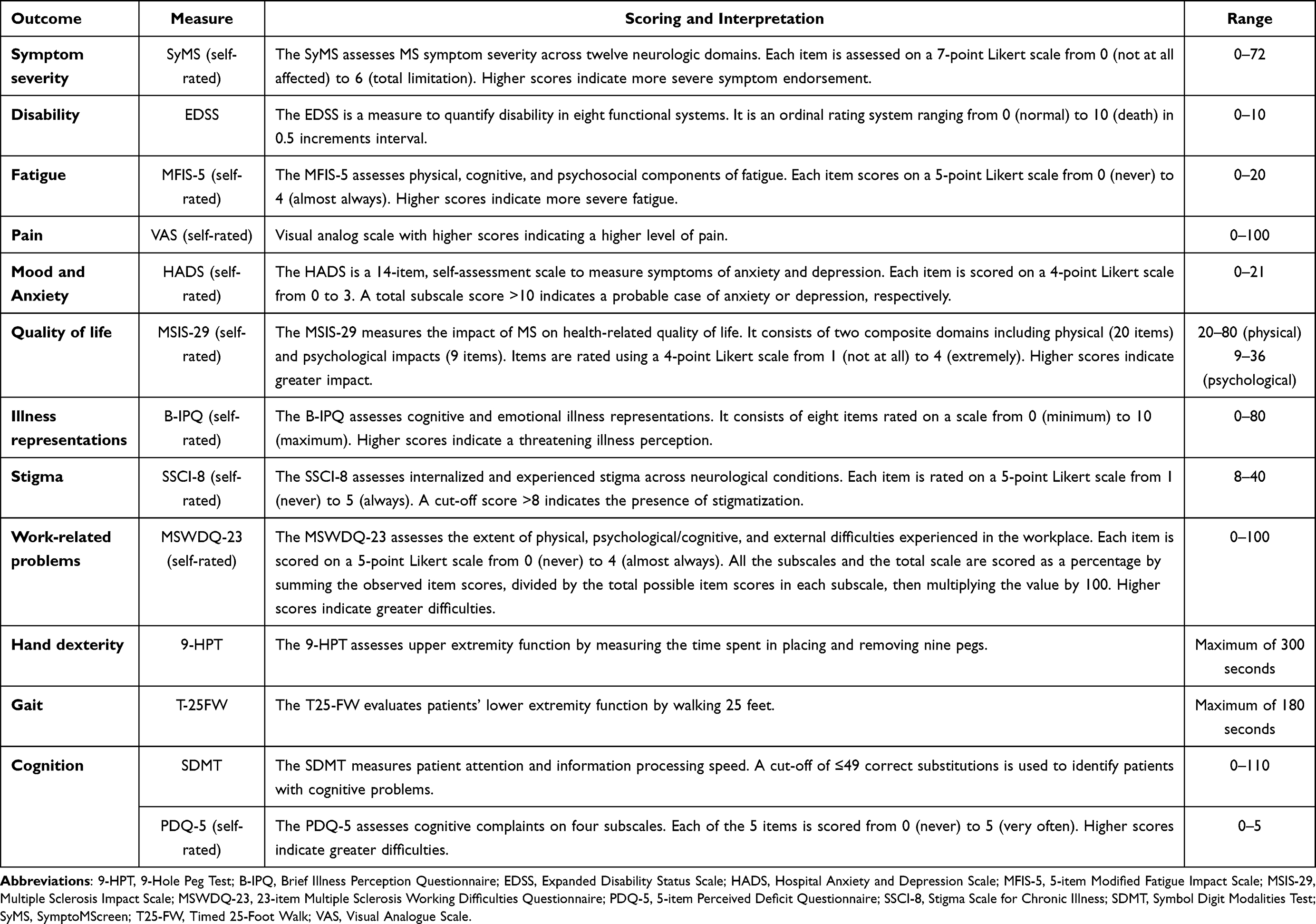 |
Table 1 Outcome Measures |
Statistical Analysis
Demographic and clinical characteristics were summarized using frequencies (percentages) and mean (standard deviation) or median (interquartile range) as appropriate. P-values <0.05 were considered statistically significant.
A multivariate logistic regression analysis was conducted to assess the association between state hopelessness (STHS state score) and demographic, clinical characteristics, and patients’ perspectives. Bivariate analyses were performed using logistic regression, taking the STHS state score as the dependent variable and each study variable as the independent variable. The multivariate analysis included those variables that were significant (p-value <0.10) in the previous analysis as the independent variables. These variables were further selected through stepwise regression using the Akaike information criterion (AIC), which chooses the model with the best quality as the final model.
Results
A total of 189 patients were included in the study. The mean age (SD) was 36.1 (9.4) years and 71.4% were female. The median disease duration (IQR) was 1.4 (0.7, 2.1) years and the median EDSS score was 1.0 (0, 2.0). Patients perceived low symptom severity, with fatigue, sensory symptoms and anxiety being the most affected dimensions. A proportion of 65.6% (n=124) of patients reported moderate-to-severe state hopelessness. Forty-seven (24.9%) and thirteen (6.9%) patients had anxiety and depressive symptoms, respectively. Sociodemographic and clinical characteristics of the sample are shown in Table 2.
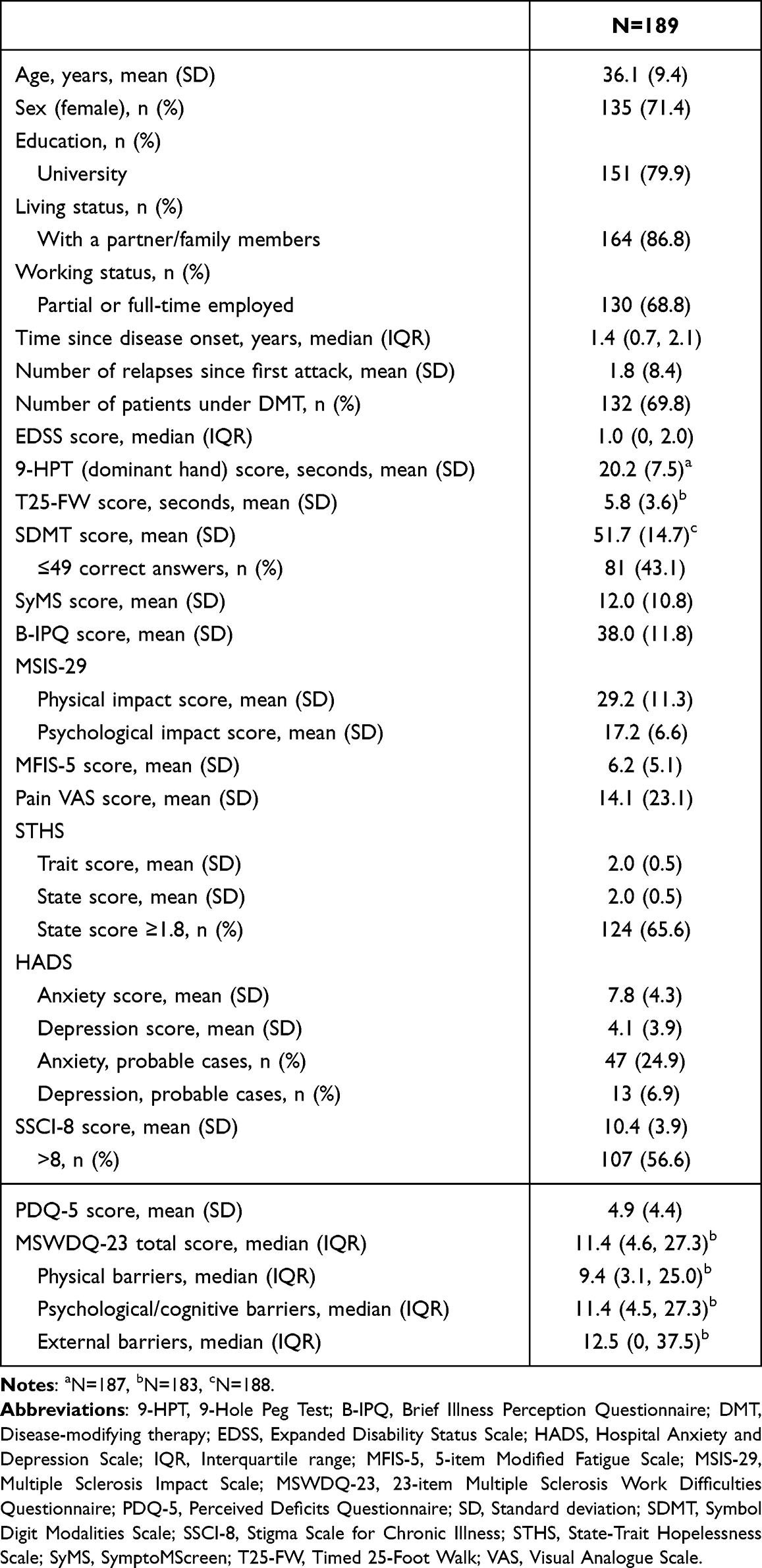 |
Table 2 Sociodemographic and Clinical Characteristics |
Multivariate analysis showed that older age (OR=1.05, 95% CI 1.00–1.10; p=0.035), depressive symptoms (OR=1.80, 95% CI 1.40–2.40; p=<0.001), a threatening illness perception (OR=1.10, 95% CI 1.04–1.20; p=0.001), and the presence of psychological and cognitive barriers to workplace performance (OR=1.06, 95% CI 1.01–1.11; p=0.029) were predictors of moderate-to-severe state hopelessness. Bivariate and multivariate analysis are shown in Table 3.
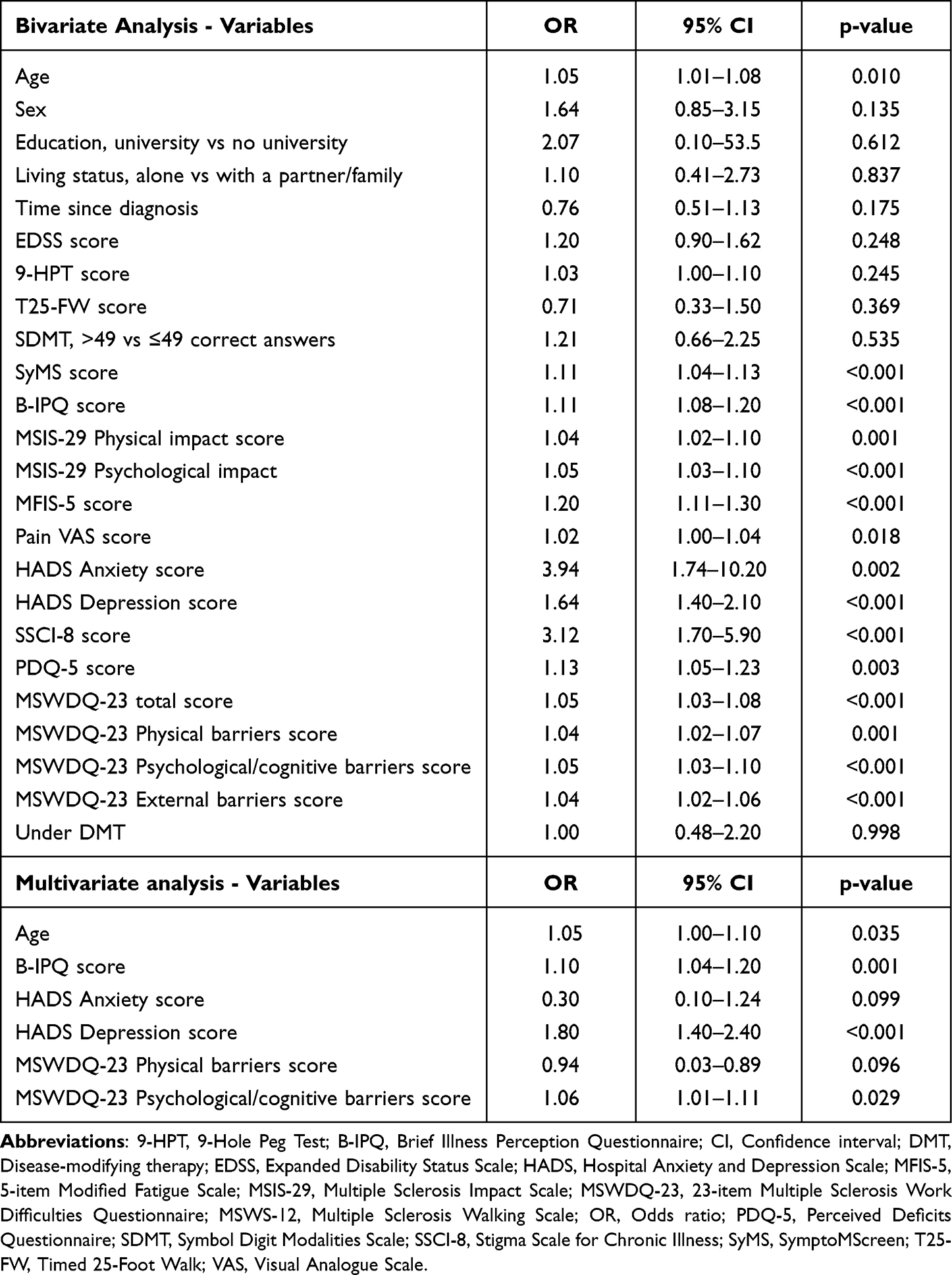 |
Table 3 Bivariate and Multivariate Logistic Regression Analysis |
Discussion
The impact of being diagnosed early in life with a chronic disease without curative treatment and an uncertain prognosis has a negative impact on most MS patients.9,29 Problems already common in the early phase of the disease such as fatigue, depressive symptoms, cognitive difficulties, and motor impairments together with the fear of disability progression affect patients’ quality of life and decision-making ability.9,29–31 Functional impairment and productivity loss already occur at a low level of physical disability.7 The pooled suicide rate ratio at diagnosis was 2.12 (95% CI 1.84–2.46) in a meta-analysis of 16 studies focused on suicide and multiple sclerosis.10
Hopelessness has traditionally been considered one of the risk factors for suicide.32 This type of negative perception was found in 23% of cancer patients and 27–52% of patients with ischemic heart disease during their hospitalization.33,34 However, no previous studies analyzed hopelessness in MS patients at early stages of the disease. In our study, hopelessness was a common phenomenon in a sample of patients with early-stage RRMS with low physical disability. Hopelessness was significantly associated with older age, a threatening illness perception, depressive symptoms, and perceived psychological and cognitive problems affecting the ability to work.
Patients’ beliefs and expectations about a disease influence their emotional reactions and coping resources, and have been associated with quality of life and treatment adherence.35 MS patients’ perspectives and preferences are dynamic and may change along the disease trajectory following clinical events and contextual factors.36–38 In a recent systematic review, Luca et al found that MS patients´ illness perceptions predicted physical, psychological, functioning, and disease management outcomes.39 High emotional impact, illness attribution to psychological causes, number of symptoms, and functional limitations due to MS were associated with worse outcomes. Poor self-perception of physical condition in MS patients was associated with negative beliefs about treatment efficacy and poor adherence.31,40 In addition, the self-perception of cognitive difficulties predicted presenteeism and unemployment since diagnosis.41
Interestingly, all of the impacted symptom domains that were associated in our study with hopelessness were identified from patient-reported assessment instruments (PROs), including the B-IPQ, HADS, and MSWDQ-23. These findings may support the complementary usefulness of including PROs in addition to routine neurological examination.42,43
Our study has some limitations. First, a selection bias may have influenced the prevalence of hopelessness as more motivated or cooperative patients may have chosen to participate in the study. Second, the study population may not be representative of the full spectrum of patients with early-stage RRMS as we only included patients with mild-to-moderate disability (EDSS score ≤ 5.5). Third, the cross-sectional study design limits the ability to establish causal relationships between the factors assessed and hopelessness. Another limitation is the lack of information collected on different factors known to be related to hopelessness, such as the perception of social support or disease knowledge.44,45
Conclusion
Hopelessness was a common phenomenon in an early-stage RRMS population. Early identification of factors associated with hopelessness in patients with RRMS may enable multidisciplinary teams to conduct a comprehensive approach aimed at training patients to understand their disease, prevent and manage mood disorders, and undertake early cognitive rehabilitation. Further studies with a longitudinal design are needed to understand the whole spectrum of mechanisms involved in hopelessness and MS.
Acknowledgments
The authors are most grateful to all patients, neurologists, and nurses participating in the study. This manuscript has not been previously published and is not under consideration elsewhere. The abstract of this paper was presented at the 38th Congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS) and the 75th American Academy (AAN) Annual Meeting as poster presentations with interim findings (ePoster EPO844; Amsterdam, Netherlands; October 26-28, 2022 and Poster P13-3.006; Boston, USA; Neurology. 2023;100 (17 Supplement 2) https://doi.org/10.1212/WNL.0000000000203496).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Roche Medical Department, Spain (ML42064). The funding source had no role in the design, analysis and interpretation of the data, review or approval of the manuscript, and decision to submit for publication.
Disclosure
Susana Sainz de la Maza received payment for lecturing or travel expenses from Merck, Biogen, Sanofi- Genzyme, Roche, and Novartis. Ana María Alonso Torres received compensation for consulting services from Biogen, BMS, Sanofi, Roche, Janssen and Novartis; and speaking honoraria from Biogen, BMS, Sanofi, Roche, Janssen, Merck, Almirall and Novartis. Ana B Caminero received courses and honoraria for her participation as speaker/meeting moderator/symposia organizer from Alter, Almirall, Bayer, Bial, Biogen, Bristol-Myers-Squibb, Lilly, Merck, Mylan, Novartis, Roche, Sanofi-Genzyme, Teva and UCB; and support to attend scientific meetings from Biogen, Bial, Merck-Serono, Novartis, Roche, Sanofi-Genzyme and Teva. Laura Borrega received compensation for consulting services, speaking honoraria and support to attend scientific meetings from Bayer, Celgene, Biogen, Genzyme, Merck, Novartis, Roche, Almirall and Teva. José L Sánchez-Menoyo received support to attend scientific meetings from Novartis, Merck, and Biogen; speaking honoraria from Biogen, Novartis, Sanofi, Merck, Almirall, Bayer and Teva; and participated in clinical trials from Biogen, Merck, and Roche. Francisco J Barrero-Hernández received compensation for consulting services and speaking honoraria from Almirall, Biogen, Genzyme, Merck, Novartis, Roche, Sanofi and Teva. Carmen Calles received compensation for consulting services, speaking honoraria and support to attend scientific meetings and courses from Merck, Teva, Sanofi-Genzyme, Novartis, Biogen, Roche, and Bristol-Myers-Squibb. Julio Dotor García-Soto received compensation for consulting services and speaking honoraria from Biogen, Novartis, Merck, UCB, Sanofi-Genzyme, Roche, Almirall and Teva. Laura Navarro-Cantó received compensations from Sanofi-Genzyme, Merk, Biogen and Roche. Eduardo Agüera-Morales received speaking honoraria from Roche, Novartis, Merck, Sanofi and Biogen. Moisés Garcés has received speaking honoraria from Biogen, Sanofi, Almirall and Novartis. Laura Gabaldón-Torres received speaking honoraria from Biogen, Novartis, Merck, Bayer, Sanofi-Genzyme, Almirall, Roche and Teva. Mariona Hervás participated in observational studies and received compensation for consulting services and speaking honoraria from Roche, Merck, Sanofi, Biogen, Novartis and Bayer. Jorge Maurino and Rocío Gómez-Ballesteros are employees of Roche Farma Spain. Tamara Castillo-Triviño reports personal fees from Almirall, Biogen, Bristol Myers Squibb, Janssen, Merck, Novartis, Roche, and Sanofi-Genzyme, outside the submitted work. The rest of the authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Balsamo M, Carlucci L, Innamorati M, et al. Further insights into the beck hopelessness scale (BHS): unidimensionality among psychiatric inpatients. Front Psychiatry. 2020;11:727. doi:10.3389/fpsyt.2020.00727
2. McMillan D, Gilbody S, Beresford E, et al. Can we predict suicide and non-fatal self-harm with the Beck Hopelessness Scale? A meta-analysis. Psychol Med. 2007;37(6):769–778. doi:10.1017/S0033291706009664
3. Assari S, Lankarani MM. Depressive symptoms are associated with more hopelessness among white than black older adults. Front Public Health. 2016;4:82. doi:10.3389/fpubh.2016.00082
4. Luo J, Li L, Reangsing C, et al. Effects of psychotherapy on hope/hopelessness in adults with cancer: a systematic review and meta-analysis. Int J Behav Med. 2022;29(6):691–704. doi:10.1007/s12529-021-10051-9
5. Dunn SL, DeVon HA, Buursma MP, et al. Reliability and validity of the state-trait hopelessness scale in patients with heart disease and moderate to severe hopelessness. J Cardiovasc Nurs. 2020;35(2):126–130. doi:10.1097/JCN.0000000000000647
6. McGinley MP, Goldschmidt CH, Rae-Grant AD. Diagnosis and treatment of multiple sclerosis: a review. JAMA. 2021;325(8):765–779. doi:10.1001/jama.2020.26858
7. Maurino J, Martínez-Ginés ML, García-Domínguez JM, et al. Workplace difficulties, health-related quality of life, and perception of stigma from the perspective of patients with multiple sclerosis. Mult Scler Relat Disord. 2020;41:102046. doi:10.1016/j.msard.2020.102046
8. Pitt D, Lo CH, Gauthier SA, et al. Toward precision phenotyping of multiple sclerosis. Neurol Neuroimm Neuroinfl. 2022;9(6):e200025. doi:10.1212/NXI.0000000000200025
9. Nielsen J, Saliger J, Montag C, et al. Facing the unknown: fear of progression could be a relevant psychological risk factor for depressive mood states among patients with multiple sclerosis. Psychother Psychosom. 2018;87(3):190–192. doi:10.1159/000487329
10. Shen Q, Lu H, Xie D, Wang H, Zhao Q, Xu Y. Association between suicide and multiple sclerosis: an updated meta-analysis. Mult Scler Relat Disord. 2019;34:83–90. doi:10.1016/j.msard.2019.06.012
11. Alejos M, Vázquez-Bourgon J, Santurtún M, Riancho J, Santurtún A. Do patients diagnosed with a neurological disease present increased risk of suicide? Neurologia. 2023;38(1):41–46. doi:10.1016/j.nrleng.2020.03.005
12. Shin JS, Kwon YN, Choi Y, et al. Comparison of psychiatric disturbances in patients with multiple sclerosis and neuromyelitis optica. Medicine. 2019;98(38):e17184. doi:10.1097/MD.0000000000017184
13. Patten SB, Metz LM. Hopelessness ratings in relapsing-remitting and secondary progressive multiple sclerosis. Int J Psychiatry Med. 2002;32(2):155–165. doi:10.2190/2G2N-WE19-NM47-JNY8
14. Luca M, Chisari MG, D’Amico E, et al. Hopelessness in multiple sclerosis: psychological and organic correlates. J Psych Psych Dis. 2019;3:241–244. doi:10.26502/jppd.2572-519X0078
15. Thompson AJ, Banwell BL, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018;17(2):162–173. doi:10.1016/S1474-4422(17)30470-2
16. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. 1983;33(11):1444–1452. doi:10.1212/WNL.33.11.1444
17. Dunn SL, Olamijulo GB, Fuglseth HL, et al. The state-trait hopelessness scale: development and testing. West J Nurs Res. 2014;36(4):552–570. doi:10.1177/0193945913507634
18. Meca-Lallana J, Maurino J, Hernández-Pérez MÁ, et al. Psychometric properties of the symptom screen questionnaire in a mild disability population of patients with relapsing-remitting multiple sclerosis: quantifying the patient’s perspective. Neurol Ther. 2020;9(1):173–179. doi:10.1007/s40120-020-00176-6
19. Meca-Lallana V, Brañas-Pampillón M, Higueras Y, et al. Assessing fatigue in multiple sclerosis: psychometric properties of the five-item Modified Fatigue Impact Scale (MFIS-5). Mult Scler J Exp Transl Clin. 2019;5(4):2055217319887987. doi:10.1177/2055217319887987
20. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
21. Hobart J, Lamping D, Fitzpatrick R, et al. The multiple sclerosis impact scale (MSIS-29): a new patient-based outcome measure. Brain. 2001;124(Pt 5):962–973. doi:10.1093/brain/124.5.962
22. Basu S, Poole J. The brief illness perception questionnaire. Occup Med. 2016;66(5):419–420. doi:10.1093/occmed/kqv203
23. Ballesteros J, Martínez-Ginés ML, García-Domínguez JM, et al. Assessing stigma in multiple sclerosis: psychometric properties of the eight-item stigma scale for chronic illness (SSCI-8). Int J MS Care. 2019;21(5):195–199. doi:10.7224/1537-2073.2018-053
24. Sullivan MJ, Edgley K, Dehoux E. A survey of multiple sclerosis: i. Perceived cognitive problems and compensatory strategy use. Canadian. J Rehabil. 1990;4(2):99–105.
25. Honan CA, Brown RF, Hine DW. The multiple sclerosis work difficulties questionnaire (MSWDQ): development of a shortened scale. Disabil Rehabil. 2014;36(8):635–641. doi:10.3109/09638288.2013.805258
26. López-Góngora M, Querol L, Escartín A. A one-year follow-up study of the symbol digit modalities test (SDMT) and the PACED AUDITORY SERIAL ADDITION TEst (PASAT) in relapsing-remitting multiple sclerosis: an appraisal of comparative longitudinal sensitivity. BMC Neurol. 2015;15:40. doi:10.1186/s12883-015-0296-2
27. Feys P, Lamers I, Francis G, et al. The Nine-Hole Peg Test as a manual dexterity performance measure for multiple sclerosis. Mult Scler. 2017;23(5):711–720. doi:10.1177/1352458517690824
28. Goldman MD, Motl RW, Scagnelli J, Pula JH, Sosnoff JJ, Cadavid D. Clinically meaningful performance benchmarks in MS: timed 25-foot walk and the real world. Neurology. 2013;81(21):1856–1863. doi:10.1212/01.wnl.0000436065.97642.d2
29. Thrue C, Riemenschneider M, Hvid LG, et al. Time matters: early-phase multiple sclerosis is accompanied by considerable impairments across multiple domains. Mult Scler. 2021;27(10):1477–1485. doi:10.1177/1352458520936231
30. Cattaneo D, Gervasoni E, Anastasi D, et al. Prevalence and patterns of subclinical motor and cognitive impairments in non-disabled individuals with early multiple sclerosis: a multicenter cross-sectional study. Ann Phys Rehabil Med. 2022;65(1):101491. doi:10.1016/j.rehab.2021.101491
31. Saposnik G, Sotoca J, Sempere ÁP, et al. Therapeutic status quo in patients with relapsing-remitting multiple sclerosis: a sign of poor self-perception of their clinical status? Mult Scler Relat Disord. 2020;45:102354. doi:10.1016/j.msard.2020.102354
32. Klonsky ED, Saffer BY, Bryan CJ. Ideation-to-action theories of suicide: a conceptual and empirical update. Curr Opin Psychol. 2018;22:38–43. doi:10.1016/j.copsyc.2017.07.020
33. Meggiolaro E, Berardi MA, Andritsch E, et al. Cancer patients’ emotional distress, coping styles and perception of doctor-patient interaction in European cancer settings. Palliat Support Care. 2016;14:204–211. doi:10.1017/S1478951515000760
34. Dunn SL, Corser W, Stommel M, et al. Hopelessness and depression in the early recovery period after hospitalization for acute coronary syndrome. J Cardiopulm Rehabil. 2006;26:152–159. doi:10.1097/00008483-200605000-00007
35. Hagger MS, Orbell S. The common sense model of illness self-regulation: a conceptual review and proposed extended model. Health Psychol Rev. 2022;16(3):347–377. doi:10.1080/17437199.2021.1878050
36. Eskyte I, Manzano A, Pepper G, et al. Understanding treatment decisions from the perspective of people with relapsing remitting multiple Sclerosis: a critical interpretive synthesis. Mult Scler Relat Disord. 2019;27:370–377. doi:10.1016/j.msard.2018.11.016
37. Różycka J. How I see is how I feel. Identification of illness perception schema and its association with adaptation outcomes in multiple sclerosis - a 5-year prospective study. PLoS One. 2021;16(10):e0258740. doi:10.1371/journal.pone.0258740
38. Sinnakaruppan I, Macdonald K, McCafferty A, et al. An exploration of the relationship between perception of control, physical disability, optimism, self-efficacy and hopelessness in multiple sclerosis. Int J Rehabil Res. 2010;33:26–33. doi:10.1097/MRR.0b013e32832e6b16
39. Luca M, Eccles F, Perez Algorta G, et al. Illness perceptions and outcome in multiple sclerosis: a systematic review of the literature. Mult Scler Relat Disord. 2022;67:104180. doi:10.1016/j.msard.2022.104180
40. Wilski M, Kocur P, Górny M, et al. Perception of multiple sclerosis impact and treatment efficacy beliefs: mediating effect of patient’s illness and self-appraisals. J Pain Symptom Manage. 2019;58(3):437–444. doi:10.1016/j.jpainsymman.2019.06.013
41. Honan CA, Brown RF, Batchelor J. Perceived cognitive difficulties and cognitive test performance as predictors of employment outcomes in people with multiple sclerosis. J Int Neuropsychol Soc. 2015;21(2):156–168. doi:10.1017/S1355617715000053
42. McGinley MP, Lapin B. The value of patient-reported outcome measures for multiple sclerosis. Mult Scler. 2022;28(10):1489–1490. doi:10.1177/13524585221111675
43. Zaratin P, Vermersch P, Amato MP, et al. The agenda of the global patient reported outcomes for multiple sclerosis (PROMS) initiative: progresses and open questions. Mult Scler Relat Disord. 2022;61:103757. doi:10.1016/j.msard.2022.103757
44. Buursma MP, Tintle NL, Boven E, et al. Lack of perceived social support in patients with ischemic heart disease is associated with hopelessness. Arch Psychiatr Nurs. 2020;34(2):14–16. doi:10.1016/j.apnu.2019.12.001
45. Claflin SB, Bessing B, van der Mei I, et al. Gains in multiple sclerosis knowledge following completion of the understanding multiple sclerosis online course are maintained six months after course completion. Mult Scler Relat Disord. 2022;67:104085. doi:10.1016/j.msard.2022.104085
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.