Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Hope-Enhancing Interventions in Schizophrenia Survivors: A Snyder’s Hope Theory–Based Scoping Review
Authors Widianti E ![]() , Suryani S
, Suryani S ![]() , Sunjaya DK
, Sunjaya DK ![]() , Iskandar S
, Iskandar S
Received 11 February 2026
Accepted for publication 8 May 2026
Published 15 May 2026 Volume 2026:19 602913
DOI https://doi.org/10.2147/JMDH.S602913
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tilakavati Karupaiah
Efri Widianti,1 Suryani Suryani,2 Deni Kurniadi Sunjaya,3 Shelly Iskandar4
1Doctoral Study Program, Faculty of Medicine, Universitas Padjadjaran, Bandung, Indonesia; 2Department of Mental Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, Indonesia; 3Department of Public Health, Faculty of Medicine, Universitas Padjadjaran, Bandung, Indonesia; 4Department of Psychiatry, Faculty of Medicine, Universitas Padjadjaran, Bandung, Indonesia
Correspondence: Efri Widianti, Doctoral Study Program, Faculty of Medicine, Universitas Padjadjaran, Bandung, Indonesia, Email [email protected]
Background: Hope is the fundamental to the recovery process in people with schizophrenia. Hope provides motivation to continue living a challenging life. Therefore, interventions to support people with schizophrenia to foster and maintain hope during the recovery process are important.
Purpose: This study aims to describe interventions to foster and increase hope in survivors of schizophrenia.
Methods: This study used a scoping review method, and the selection of articles using the databases Science Direct, EBSCO, SAGE, PubMed, Scopus, Springer Link. The keywords used were schizophrenia, hope, and interventions. The article search protocol used PRISMA Extension for Scoping Review, using the terms “schizophrenia OR psychosis OR psychotic disorder” AND “hope OR hopefulness OR meaning of hope” AND “interventions OR treatments OR programs”. The selected studies were based on original research, used quantitative approaches (RCT and pre-experimental), focused on interventions to foster and or increase hope in survivors of Schizophrenia, and published in January 2014-June 2025).
Results: Fourteen articles that met the criteria were found in the study. This study identified 14 interventions that can increase hope in patients with schizophrenia, including Mandala Art Therapy, Mindfulness Therapy, Positive Psychotherapy for Psychosis (PPP), Mixed-mode Mindfulness-Based Cognitive Therapy (M-MBCT), Social Recovery Therapy (SRT), Educational Music Therapy, Narrative Enhancement and Cognitive Therapy (NECT), Abriged Illness Management and Recovery Program (AIMR), and Positive Psychology Expressive Writing (PPEW), Hope Instillation, psychoeducation, Empowerment intervention, Mindfulness Based Stress Reduction (MBSR) and The Needs-Tailored Recovery Program.
Conclusion: There are 14 interventions that can increase hope in patients with schizophrenia. These interventions are inseparable from the three components of hope theory, namely goals, pathway thinking, and agency thinking.
Keywords: hope, interventions, psychosis, schizophrenia
Introduction
Schizophrenia is a severe mental disorder with frequent relapse.1 People living with Schizophrenia experience distortions in perception, thoughts, speech, emotions, behavior and self-concept.2 In 2022, approximately 24 million people aged 20 years and above were living with schizophrenia worldwide.3 In Indonesia, there was a prevalence of 7 per 1000 households with a family member with schizophrenia mental disorder in 2018. This means that out of 1000 households, there are 7 households that have a family member with schizophrenia mental disorder.4 Despite the smaller proportion of schizophrenia found in anxiety and depressive disorders, Global Burden of Disease data in 2019 indicate that it contributes disproportionately to severe disability schizophrenia has the highest proportion of mental health problems that result in severe disability. As a consequence, the treatment of schizophrenia is a current concern of mental health services around the world.3
People with Schizophrenia can encounter several challenges and barriers in the recovery process.5 The disorders suffered by people with schizophrenia can cause dysfunction in perceptual, motor, and emotional aspects, causing people with schizophrenia to withdraw from social interactions to avoid stigma.6 Thus, daily life activities such as making friends, going to school or work, getting married and having offspring can be disrupted.7 This may lead to loss of hope and feelings of hopelessness in people with Schizophrenia.8,9 Hopelessness will contribute to a person with Schizophrenia experiencing decreased self-esteem, increased suicide rates, and discontinuation of treatment.10,11 However, people living with schizophrenia may also experience meaningful improvement and live fulfilling lives.12,13 Bellack’s findings suggest that many individuals with schizophrenia can experience significant improvements in symptoms, functioning, and quality of life.10 However, recovery in schizophrenia should not be understood solely as clinical improvement or symptom reduction. Contemporary perspectives increasingly conceptualize recovery as a multidimensional and personal process that may include functional improvement, identity reconstruction, social connectedness, empowerment, and the pursuit of a meaningful life despite ongoing mental health challenges. These findings therefore suggest that recovery is possible, though it is best understood as a complex and individualized journey rather than a singular clinical outcome.14,15
Hope is widely recognized as a central component of this broader recovery process.16 Beyond being an individual psychological resource, hope may also be shaped by interpersonal relationships, spirituality, cultural context, social inclusion, and structural opportunities.17 In schizophrenia recovery, hope has been described as both an internal source of motivation and a relational process nurtured through connection with others and supportive environments. In people living with Schizophrenia, according to Deegan, hope is a flame to be a light in the darkness of despair experienced during the recovery process.15 Meanwhile, according to Noh, et al18 Hope in individuals with schizophrenia is an aspiration to achieve a life with happiness, meaning, future optimism, and enthusiasm for life, so hope can prevent helplessness and increase motivation in schizophrenia survivors. In line with that, one influential framework for understanding hope is Snyder’s Hope Theory, which conceptualizes hope through goals, agency, and pathways. Snyder explains that hope is a belief that a person can find pathways to achieve goals and has the motivation (agency) to use these pathways.19 While this framework offers a useful structure for understanding goal-directed cognition, its primarily individualistic and goal-oriented orientation may not fully capture the broader emotional, relational, cultural, and structural dimensions of hope relevant to schizophrenia recovery across diverse contexts. Therefore, Snyder’s framework may serve as one useful interpretive lens, while broader perspectives remain necessary to understand hope in lived recovery experiences.15,17
Based on previous studies, sources of hope in individuals with schizophrenia may come from their immediate social environment, such as friends, family, and health professionals.20 Health workers have an important role in facilitating the growth of hope in individuals with schizophrenia.21 The role of health workers in the recovery process is to collaborate and have closeness with survivors, helping individuals with schizophrenia to realize changes in themselves as a result of mental disorders, then directing their lives positively.22 Health workers can foster hope in individuals with schizophrenia through various interventions. Various forms of interventions conducted by health workers have been shown to be effective in increasing hope, as shown in various previous studies. Importantly, these interventions are not always explicitly based on hope theory. Some interventions, such as Cognitive Behavioral Therapy (CBT) and other psychosocial approaches, may incorporate elements of hope as part of broader therapeutic processes, even when hope is not the primary theoretical foundation. However, there is still limited evidence synthesizing whether previous reviews have specifically examined hope-enhancing interventions in schizophrenia, particularly across different theoretical approaches. Therefore, considering the many findings in various studies regarding the effectiveness of interventions in increasing hope in schizophrenia survivors, a scoping review was conducted as an effort to identify, summarize, and map the various forms of interventions that have been used. This review aims to explore the most relevant interventions that can be optimized in professional practice by health workers, especially in supporting the recovery process through strengthening hope as a crucial component in the recovery of schizophrenia survivors.
Methods
Study Design
This study used a scoping review research design. A scoping review is a research method to clarify the working definition and conceptual boundaries of a topic or concept that is still developing. The steps in this study were identification of the research topic, identification of literature relevant to the search strategy using keywords and inclusion criteria, sorting of articles, data extraction, and data analysis. The search strategy in this study used the PRISMA Extension for Scoping Reviews (PRISMA-ScR) to select articles that discussed interventions to foster and increase hope in schizophrenia survivors.
Research Question
The objective of this review is to describe interventions in fostering and enhancing hope among schizophrenia survivors. The initial research question that guided the literature search was: “What interventions do schizophrenia survivors use to build and maintain hope for recovery?”
Eligibility Criteria and Study Selection
The search strategy in this study used the PRISMA Extension for Scoping Reviews (PRISMA-ScR) to select articles discussing interventions to foster and increase hope in schizophrenia survivors (Figure 1). The inclusion criteria for article selection were studies involving participants diagnosed with schizophrenia or schizophrenia-spectrum disorders, published in English, available in full text, focused on interventions aimed at increasing hope, and designed as primary studies (randomized controlled trials or quasi-experimental studies) published between 2014 and 2025. To enhance search sensitivity, broader psychosis-related terms (eg, psychosis, psychotic disorder) were included during the database search; however, final study selection was restricted to studies specifically involving schizophrenia or schizophrenia-spectrum populations. Studies primarily involving participants with other psychiatric diagnoses (eg, bipolar disorder or non-schizophrenia psychotic disorders) without clearly identifiable schizophrenia-specific findings were excluded.
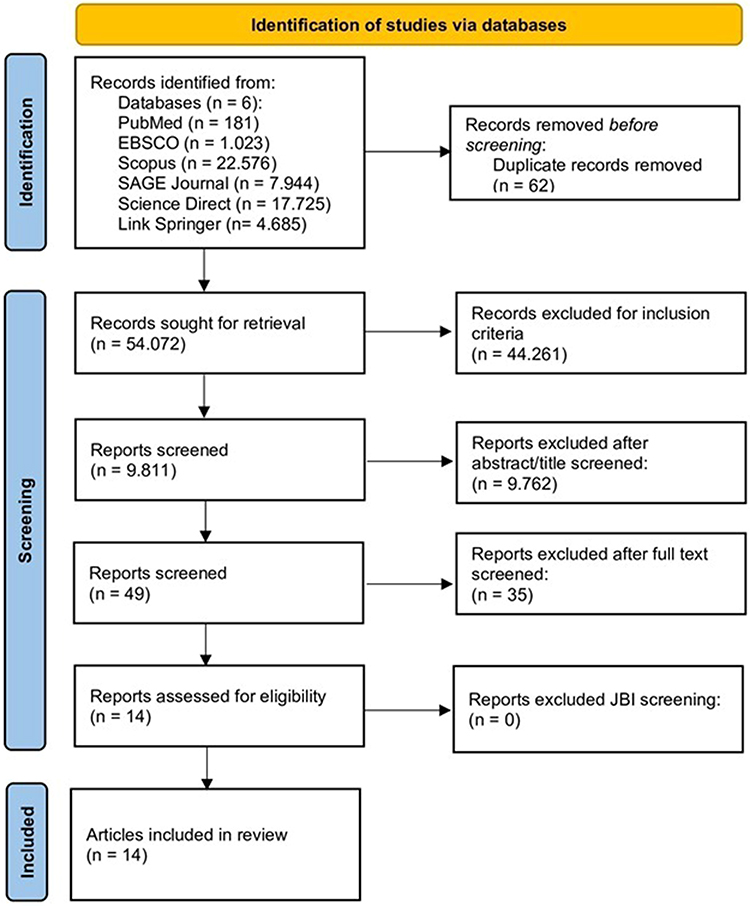 |
Figure 1 PRISMA Flow Diagram. Notes: PRISMA figure adapted from Page MJ. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. |
Search Strategy
This study uses the Population, Concept, Context (PCC) framework as a basis for identifying problems and developing review questions. The literature search uses the Science Direct, EBSCO, SAGE, PubMed, Scopus, and Link Springer databases and search engines. The keywords used were in English: “schizophrenia OR psychosis OR psychotic disorder” AND “hope OR hopefulness OR meaning of hope” AND “intervention OR treatments OR program”. To maximize search sensitivity, broader terms such as “psychosis” and “psychotic disorder” were included alongside “schizophrenia”. However, study selection was guided by predefined eligibility criteria that prioritized studies specifically involving individuals diagnosed with schizophrenia or schizophrenia-spectrum disorders. Studies focusing primarily on other psychotic conditions (eg, bipolar disorder with psychotic features) were excluded unless findings specific to schizophrenia participants could be clearly identified.
Data Extraction
Data extraction in this study used tables to group similar extracted data to answer the research objectives. The articles obtained were then written in an extraction table containing information on the author, year, objective, sample, research method, intervention, research results and hope measurement.
Quality Assessment
At this stage, articles were selected based on their quality. Quality assessment was conducted using the Joanna Briggs Institute (JBI) instrument. The authors used articles with a quality score above 75% for this study. All authors double-checked to ensure that the articles obtained were in line with the research objectives.
Data Analysis
Data analysis used a descriptive approach, beginning with data classification, followed by the author writing the research results from the articles that had been reviewed. Data analysis grouped the types of interventions that can foster and increase hope in schizophrenia survivors.
Results
Selection Process
The search process began with database identification of relevant articles, followed by duplicate removal. A total of 9811 records were identified through the initial search process. After title and abstract screening based on predefined inclusion and exclusion criteria, 49 articles were retained for further assessment. Full-text review resulted in 14 eligible studies describing interventions aimed at improving hope among people living with schizophrenia. Methodological quality was then assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist appropriate to each study design. The JBI tool evaluates study quality across domains such as participant selection, methodological rigor, control of confounding factors, reliability of outcome measurement, and appropriateness of statistical analysis. Studies scoring ≥75% were categorized as high quality, 50–74% as moderate quality, and <50% as low quality. The appraisal followed standardized JBI guidance for critical evaluation of methodological quality.23 All 14 included studies achieved scores above 75% and were therefore classified as high quality. The detailed results of the methodological quality assessment are presented in Table 1.
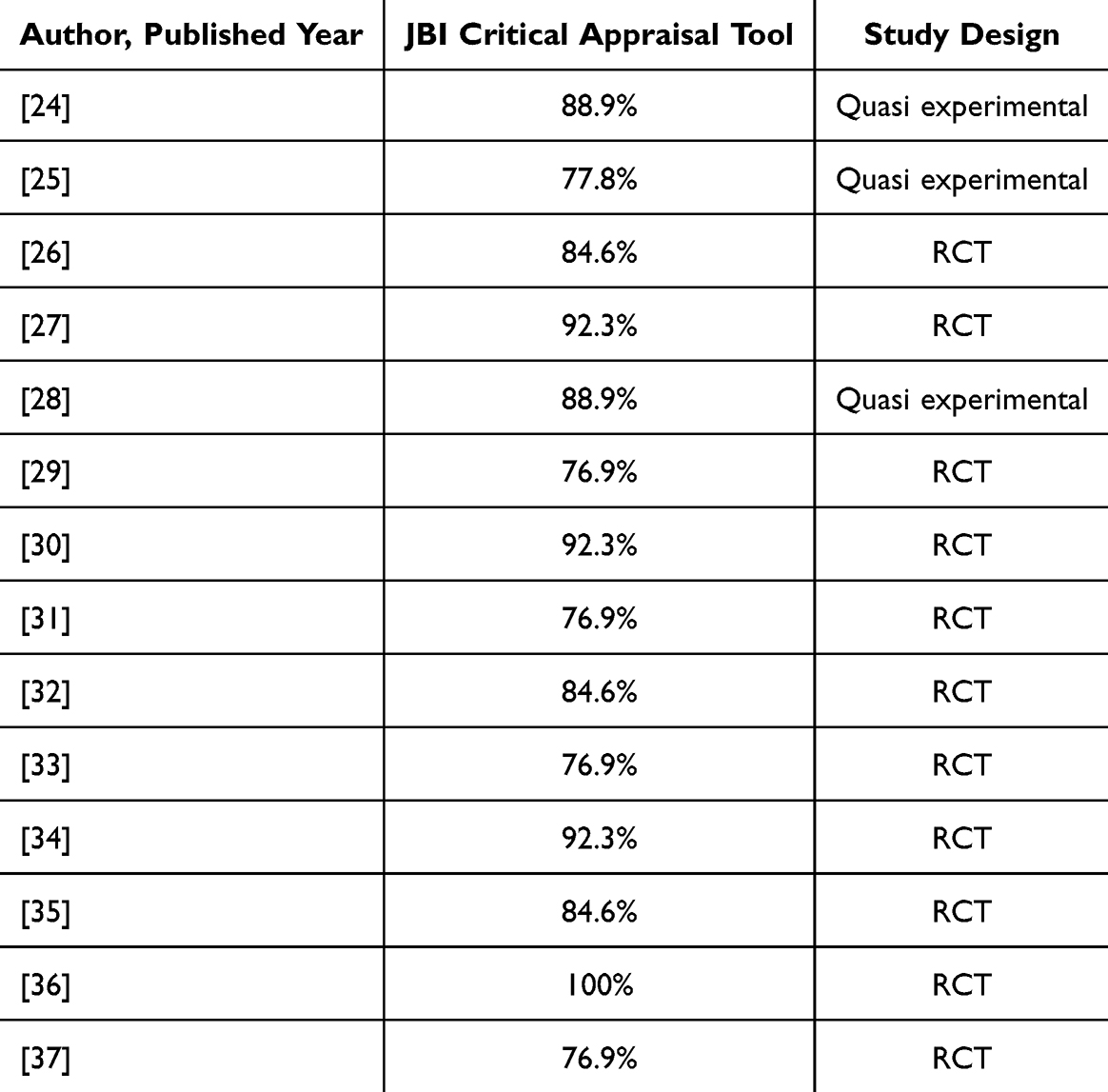 |
Table 1 JBI Critical Appraisal Tool |
Characteristic of Included Studies
Fourteen articles on interventions to improve hope in schizophrenia patients were classified based on the location of the research, namely in clinical settings and community settings. For clinical settings, the interventions conducted were Mandala Art Therapy, Mindfulness Therapy, Positive Psychotherapy for Psychosis (PPP), Mixed-mode Mindfulness-Based Cognitive Therapy (M-MBCT), Social Recovery Therapy (SRT), Educational Music Therapy, Narrative Enhancement and Cognitive Therapy (NECT), Abridged Illness Management and Recovery Program (AIMR), and Positive Psychology Expressive Writing (PPEW), while for community settings, the interventions are Hope Instillation, psychoeducation, Empowerment intervention, Mindfulness Based Stress Reduction (MBSR), and The Needs-Tailored Recovery Program. The sample in this study ranged from 28 to 600 participants, with most participants being adults. The research was conducted in Turkey, Korea, China, Indonesia, Taiwan, Hong Kong, Chicago, Saudi Arabia, and the United States (Table 2).
 |
Table 2 Extraction Data |
Setting Intervention
Clinical Setting Interventions
There are several types of interventions to foster and increase hope in schizophrenia survivors in clinical settings, including Mandala Art Therapy, Mindfulness Therapy, Positive Psychotherapy for Psychosis (PPP), Mixed-mode Mindfulness -Based Cognitive Therapy (M-MBCT), Social Recovery Therapy (SRT), Educational Music Therapy, Narrative Enhancement and Cognitive Therapy (NECT), Abridged Illness Management and Recovery Program (AIMR), and Positive Psychology Expressive Writing (PPEW). Most of the intervention activities involved a high level of collaboration with several professionals (nurses, psychologists, therapists). These interventions in a clinical setting, carried out in psychiatric wards, proved to be effective in fostering and increasing hope among schizophrenia survivors.
Although these interventions contribute to increasing hope, not all are explicitly grounded in Snyder’s Hope Theory. Instead, they are based on diverse theoretical frameworks, including cognitive behavioral therapy (CBT), mindfulness-based approaches, positive psychology, expressive therapies, and recovery-oriented models. Nevertheless, these interventions still incorporate core elements of hope, such as goal-setting, pathway development, and motivational enhancement.
The Mandala Art Therapy intervention program has 8 sessions: Sessions 1 and 2 for self-understanding, sessions 3 and 4 for understanding others, sessions 5 and 6 for self-expression, session 7 for internal integration, and session 8 for closure and post-testing, in which sessions 2 and 7 the intervention group patients were given the freedom to draw, color, and listen to music for meditation. The therapy was conducted for approximately 2 weeks. Another intervention that combines art to increase hope during recovery is Educational Music Therapy, which consists of 42 sessions during the program, each lasting about 45 minutes. All sessions are group sessions and have been structured. Participants were divided into two groups to receive different interventions, namely Lyric Analysis and Song Writing sessions. In the Lyric Analysis session, participants played songs, analyzed lyrics related to hope, and engaged in dialogue about how the lyrics reflected aspects of the path to hope. Meanwhile, in the Song Writing session, patients wrote songs about their hopes for recovery, but they began by brainstorming ideas about why they wanted to recover. Common ideas included family, friends, health, career aspirations, and happiness. The first verse focuses on “why they want recovery” (motivation) and the second verse focuses on “how to recover”.
Mandala Art Therapy and Educational Music Therapy are primarily grounded in expressive and creative therapy approaches, which emphasize emotional expression, self-awareness, and meaning-making. Although they do not explicitly use hope theory, these interventions foster hope by helping individuals explore personal goals, express emotions, and develop adaptive coping pathways.
Next, Mindfulness Therapy was provided for 2 weeks, with participants receiving 2 mindfulness therapy sessions of 30 minutes each. The intervention included relaxation or calming techniques, deep breathing, self-awareness of time, place, and why they were in the hospital, self-compassion to reduce negative judgment of themselves and acceptance of their condition, and belief that God would take away their illness. Unlike other mindfulness interventions, Mixed-mode Mindfulness-Based Cognitive Therapy (M-MBCT) combines face-to-face group interventions and self-directed interventions. This intervention also incorporates an additional approach combining cognitive therapy (CBT). The intervention was administered over a total of 8 weeks. Group therapy activities include body scans, mindfulness breathing, mindfulness yoga, sitting meditation, ABC theory of emotions, exercises in accepting negative emotions, and discussions on how mindfulness can be applied in daily life. Meanwhile, the independent intervention uses audio and video recordings containing guidance on meditation, yoga, body scans, and awareness of thoughts and emotions.
Mindfulness Therapy and M-MBCT are based on mindfulness-based and cognitive behavioral frameworks. These approaches primarily target emotional regulation, awareness, and acceptance. While not directly derived from hope theory, they contribute to hope enhancement by strengthening agency (through increased self-regulation and acceptance) and supporting adaptive cognitive pathways in managing challenges.
Social Recovery Therapy (SRT) intervention is a new form of Cognitive Behavioral Therapy (CBT) that focuses on individual values and goals, identifies problems and obstacles that hinder their achievement, and then encourages hope for meaningful behavioral change. The approach begins with the formulation of social recovery from an individual perspective. Similar to SRT, Narrative Enhancement and Cognitive Therapy (NECT) is a CBT intervention with a structured group-based approach. However, the goal of this intervention is to address the impact of self-stigma. The NECT intervention is structured, consisting of 20 sessions guided by two facilitators. In each meeting, participants read material from the manual, complete exercises and reflective questions, share their answers and experiences, and discuss related personal views and experiences.
SRT and NECT are rooted in cognitive behavioral therapy (CBT). These interventions focus on restructuring maladaptive thoughts, addressing self-stigma, and promoting behavioral activation. Through these mechanisms, they indirectly enhance hope by facilitating goal clarification, identifying barriers, and developing realistic pathways toward recovery.
There are interventions that involve positive psychology principles by exploring positive experiences and practicing positive thinking. These interventions are PPP and PPEW. Positive Psychotherapy for Psychosis (PPP) is a positive psychology-based group therapy program. This intervention is designed to improve the well-being of patients with psychosis. The program consists of 13 sessions over 7 weeks (two sessions per week). The sessions include exercises in positive responding, savoring good experiences, recognizing and utilizing personal strengths, finding positive meaning in negative experiences, and developing attitudes of gratitude and forgiveness. Meanwhile, the Positive Psychology Expressive Writing (PPEW) intervention is conducted over 2 weeks. The PPEW intervention covers six themes: coping with trauma, focusing on strengths, exploring positive things, learning to be grateful, appreciating happiness, and renewing hope. The stages of activity in the session are that participants listen to six audio lectures that provide positive psychology knowledge about the six themes. Participants are instructed to write without worrying about grammar, punctuation, or length, but must stay on topic and try not to stop randomly and to feel sincerely. The writing time lasts about 20–30 minutes. This program is conducted by six nurses and two psychiatrists.
PPP and PPEW are grounded in positive psychology, which emphasizes strengths, positive emotions, and meaning-making. These interventions foster hope by enhancing agency through positive affect, gratitude, and self-reflection, while also supporting goal orientation and future optimism, even though they are not exclusively based on Snyder’s framework.
There are also interventions that focus on recovery, improving understanding of the disease and health services, and developing personal plans for recovery. These interventions are AIMR, or the Abridged Illness Management and Recovery Program (AIMR). In this study, participants were divided into two groups: a control group that underwent conventional occupational therapy, and an experimental group that underwent conventional occupational therapy plus 10 AIMR sessions. The AIMR material covered seven main topics, namely: (1) recovery strategies, (2) understanding schizophrenia, (3) medication, (4) social support, (5) relapse prevention, (6) mental health services, and (7) the recovery journey.
AIMR is based on a recovery-oriented model and illness self-management framework. This intervention emphasizes practical strategies, psychoeducation, and relapse prevention. Although not explicitly framed within hope theory, AIMR supports pathway thinking through structured recovery planning and strengthens agency through increased knowledge and self-efficacy.
Community Setting Interventions
Interventions in community settings to increase hope among schizophrenia survivors include Hope Instillation, psychoeducation, Empowerment Intervention, Mindfulness Based Stress Reduction (MBSR), and The Needs-Tailored Recovery Program.
The Hope Instillation intervention was researched in Community Mental Health Care (CMHC) and consisted of 16 sessions, namely 1) Preparation; 2) The meaning and nature of hope; 3) Exploration of sources of hope; 4) Decision-making support; 5) Improving social relationships; 6) Life review (reminiscence therapy); 7) Strengthening coping; 8) Cognitive restructuring; 9) Improving self-esteem; 10) Managing disturbances; 11) Improving sleep quality; 12) Mood management; 13) Anger control; 14) Expanding boundaries; 15) Exploring potential; and 16) Evaluation. These 16 sessions are conducted over 8 weeks, with 2 sessions per week and a duration of 40–50 minutes per session. Similar to hope instillation, the needs-tailored recovery program intervention is also a community-based intervention that focuses on the overall recovery process. The program runs for six months with home visits every two weeks (a total of approximately 12 visits, each lasting ±50 minutes). The process begins with building an empathetic and supportive therapeutic relationship, followed by an integrated needs assessment to identify the patient’s priority issues. Based on the assessment results, nurses and patients work together to develop personal recovery goals and provide empowerment interventions covering seven aspects: disease management, crisis management, personal recovery, daily life management, family support, social participation, and connection with community resources.
Hope Instillation is one of the few interventions explicitly grounded in hope theory, as it directly targets goal setting, pathway development, and agency enhancement. In contrast, other community-based interventions such as psychoeducation, empowerment intervention, MBSR, and the Needs-Tailored Recovery Program are based on psychoeducational, empowerment, mindfulness, and recovery-oriented frameworks.
Further, for psychoeducation conducted at Community Mental Health Care (CMHC), interventions were provided twice a week for six weeks. The intervention group consisted of 10–11 people per group for each session, and the intervention consisted of six sessions. 1) Empathizing with patients by listening to their perceptions of health, recovery, and hopes, 2) Reviewing patients’ perceptions of stigma and side effects on their future relationships, expectations, treatment, and benefits of treatment, etc, 3) Giving patients the initiative for each treatment received, 4) Observation and collection of evidence to initiate change, 5) Discussion of patients’ experiences and decisions about future planning, summarizing patients’ success in doing their homework, 6) Explanation of the concept of future goals, sources of support for achieving goals, and others. The empowerment intervention is also a structured psychoeducation program. This program aims to increase the self-confidence, self-control, and independence of schizophrenia patients in their daily lives. The program consists of six sessions over six weeks, delivered in the form of short face-to-face meetings (20–30 minutes) combined with the use of educational booklets. The topics covered include a basic understanding of schizophrenia and stigma, an introduction to the strengths and weaknesses in the recovery process, life challenges and the role of family, communication skills and self-care, the importance of treatment compliance, and crisis management strategies.
Conducted at Community Mental Health Care (CMHC) were provided over 8 weeks and 8 sessions, while other studies provided interventions over 2 weeks and 2 sessions. The mindfulness intervention provided includes relaxation or calming techniques, deep breathing, self-awareness of time, place, and why they are in the hospital, self-compassion to reduce negative judgment of oneself and acceptance of one’s condition, and belief that God will take away their illness. In addition, patients are also given homework and booklets for additional education.
These interventions, although not always explicitly derived from Snyder’s Hope Theory, still incorporate key elements of hope. Psychoeducation and empowerment interventions strengthen agency through increased knowledge, self-confidence, and autonomy. The Needs-Tailored Recovery Program emphasizes goal-setting and individualized recovery planning, while MBSR enhances emotional regulation and acceptance, contributing to agency and adaptive coping pathways.
Hope Theory
The author analyzes interventions based on Snyder’s Expectancy Theory, which explains that expectations are formed from three main components, namely goal, pathway thinking, and agency thinking. These interventions include Mandala Art Therapy, Mindfulness Therapy, Positive Psychotherapy for Psychosis (PPP), Mixed-Mode Mindfulness-Based Cognitive Therapy (M-MBCT), Social Recovery Therapy (SRT), Educational Music Therapy, Narrative Enhancement and Cognitive Therapy (NECT), Abriged Illness Management and Recovery Program (AIMR), Positive Psychology Expressive Writing (PPEW), Hope Instillation, psychoeducation, Empowerment Intervention, Mindfulness-Based Stress Reduction (MBSR), and The Needs-Tailored Recovery Program. The classification of these interventions based on the components of hope theory is presented in Table 3.
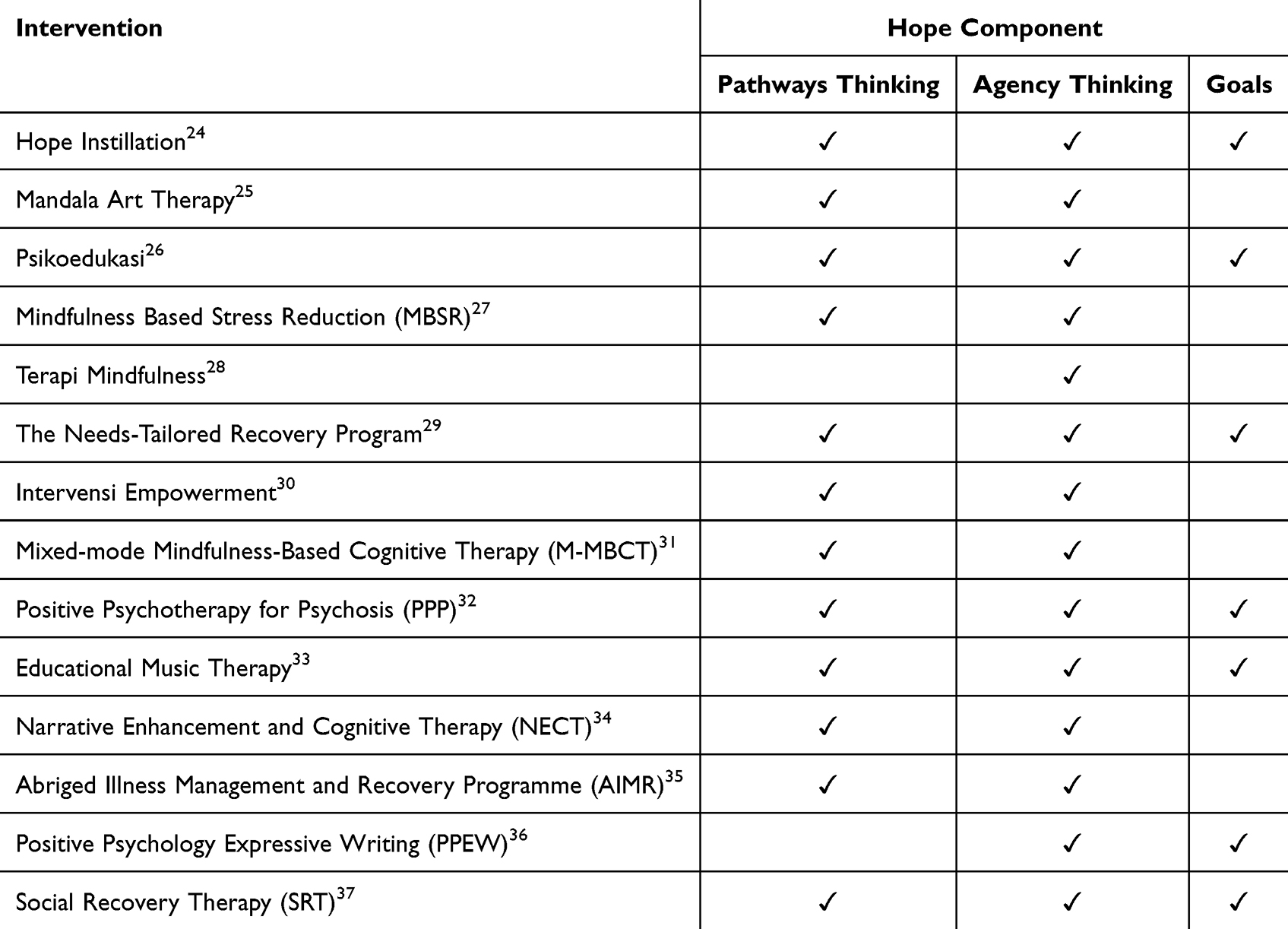 |
Table 3 Classification of Interventions Based on the Components of Hope Theory |
The goals component refers to determining what objectives an individual aims to achieve. These goals should be specific, realistic, and meaningful, thereby providing patients with a clear sense of direction. Interventions that enhance the goals component include Hope Installation, Psychoeducation, The Needs-Tailored Recovery Program, Positive Psychotherapy for Psychosis (PPP), Educational Music Therapy, Positive Psychology Expressive Writing (PPEW), and Social Recovery Therapy (SRT). For example, Hope Instillation and Psychoeducation explicitly incorporate structured sessions focused on goal-setting, where participants are guided to identify personal life goals and formulate both short-term and long-term plans. Similarly, interventions such as PPP and SRT facilitate goal clarification by encouraging individuals to define meaningful roles, daily activities, and future aspirations within their recovery process. The goals component of hope is essential in the recovery process, as it provides direction, motivation, and renewed hope for individuals with schizophrenia.
The pathways component refers to an individual’s ability to design realistic strategies or routes to achieve goals and overcome obstacles. Nearly all interventions reviewed contribute to strengthening the pathways component among survivors. These include Mandala Art Therapy, Mixed-Mode Mindfulness-Based Cognitive Therapy (M-MBCT), Abridged Illness Management and Recovery Program (AIMR), Educational Music Therapy, Positive Psychotherapy for Psychosis (PPP), Social Recovery Therapy (SRT), Narrative Enhancement and Cognitive Therapy (NECT), Hope Instillation, Empowerment Intervention, Mindfulness-Based Stress Reduction (MBSR), The Needs-Tailored Recovery Program, and Psychoeducation. These interventions differ in how pathway thinking is operationalized. For instance, AIMR and Psychoeducation emphasize structured problem-solving, relapse prevention planning, and illness self-management strategies. M-MBCT and MBSR focus on developing cognitive and emotional regulation strategies that help individuals manage barriers and remain adaptive in pursuing goals. Meanwhile, SRT and NECT support individuals in reconstructing personal narratives and identifying alternative pathways for social and functional recovery. These interventions equip survivors with the knowledge and practical skills necessary to build diverse and effective recovery pathways, such as strategies for symptom management, stress and emotion regulation, communication and social support development, medication management, self-care, and relapse prevention. Thus, these interventions play a significant role in strengthening the strategic aspect (pathways) by enhancing individuals’ capacity to plan and navigate their recovery process.
The agency component refers to an individual’s capacity to sustain motivation, self-confidence, and internal drive in pursuing meaningful goals. Interventions that develop the agency component include Hope Instillation, Mandala Art Therapy, Psychoeducation, Mindfulness-Based Stress Reduction (MBSR), Mindfulness Therapy, The Needs-Tailored Recovery Program, Empowerment Intervention, Mixed-Mode Mindfulness-Based Cognitive Therapy (M-MBCT), Positive Psychotherapy for Psychosis (PPP), Educational Music Therapy, Narrative Enhancement and Cognitive Therapy (NECT), Abridged Illness Management and Recovery Program (AIMR), Positive Psychology Expressive Writing (PPEW), and Social Recovery Therapy (SRT). Interventions targeting agency demonstrate variation in their approaches to enhancing motivation. For example, PPEW strengthens agency through reflective writing focused on gratitude, hope, and positive future orientation, while Mandala Art Therapy and Educational Music Therapy enhance emotional engagement and self-expression. Empowerment Intervention and The Needs-Tailored Recovery Program emphasize self-efficacy, autonomy, and personal control, whereas mindfulness-based interventions (MBSR, M-MBCT) support awareness and acceptance, which indirectly strengthen motivation and persistence. Interventions targeting agency primarily focus on enhancing motivation and cultivating positive emotions. This is achieved through activities such as expressive writing on themes of gratitude, happiness, and hope; strengthening the sense of self and resilience; engaging in art-based or music-based activities; practicing mindfulness; and participating in psychoeducational sessions.
Discussion
This scoping review identified fourteen interventions that have an impact on fostering and increasing hope in survivors of schizophrenia. These results are important given that people with Schizophrenia often experience loss of hope and hopelessness.1 Feelings of hopelessness in people living with schizophrenia may contribute to adverse outcomes such as treatment discontinuation and suicidal behavior, which can negatively affect the recovery process.13,14 These interventions can be integrated into mental health practice or can be redeveloped more comprehensively to aid the recovery process of people with Schizophrenia by increasing hope.
Hope is generally defined simply as a positive expectation for goal achievement, or as a belief about future possibilities.38 The role of hope is essential during the recovery process by increasing motivation and preventing feelings of hopelessness and pessimism from arising. In addition, hope also contributes to positive life energy and provides the confidence needed to achieve goals.39 The recognized and most comprehensive expectancy theory is Synder’s Expectancy Theory. In this theory, Snyder, Irving, and Anderson,40 Hope is a positive motivation based on the belief in the ability to achieve success obtained interactively starting with the individual’s ability to set the desired goal (goal), then develop plans and strategies (pathways) and motivation (agency) or energy directed at achieving goals. Thus, hope consists of three core components, which are goal, method/strategy (pathways), and agency.19
Snyder argues in hope theory that the essence of human behavior is directed towards achieving a desired goal. Thus, goals are the most fundamental cognitive component of hope theory.41 The goals provide a target sequence for action. Goals vary in temporal framework, there are short-term and long-term goals. Goals must have sufficient value to warrant sustained conscious thought about the goal to be achieved. In a hopeful person, the process and means of achieving the goal are as important as the goal itself.
Hope is not just optimism, hope requires strategies and active actions (pathways) to achieve the possibility. People who have hope in pursuing certain goals require logical pathway thinking. The pathway thinking process will be different for high-hope and low-hope people. For low-hope people, the pathway thinking is less sophisticated, and the resulting pathway is not well articulated, while high-hope people can adapt a more effective pathway quickly.19,42 Then to get to the goal also requires encouragement or motivation. The motivation component in expectancy theory is known as agency thinking. Agency thinking involves the psychological energy to initiate and continue thinking about all stages of pursuing a goal. Agency thinking will also help in providing motivation in finding alternative strategies in the presence of obstacles.43
In principle, the three components of Hope Theory provide the greatest benefit when they are integrated and applied synergistically. This is evident in the Positive Psychology Expressive Writing (PPEW) intervention, which reflects two core components of Snyder’s Hope Theory, namely agency and goals. The agency component is manifested through reflective and personal writing processes that focus on facing trauma, exploring positive aspects of life, cultivating gratitude and happiness, and renewing hope. These activities assist individuals in reconstructing their life experiences in a more adaptive manner, enabling them to regain a sense of control, enhance self-efficacy, and reduce hopelessness through the development of a more positive and meaningful self-narrative.
Meanwhile, pathways within PPEW emerge in the form of cognitive routes, specifically new ways of thinking that help individuals reinterpret past experiences as sources of learning and identify alternative approaches to coping with life challenges. These findings suggest that PPEW plays a crucial role in building a foundation of hope through the restoration of internal psychological processes, which may subsequently support the development of more concrete recovery goals and strategies.
Similarly, mindfulness-based interventions primarily strengthen hope through the agency component by targeting individuals’ internal processes. Practices such as mindfulness awareness, self-compassion, and acceptance help individuals with schizophrenia enhance emotional regulation and regain a sense of control over their responses to life experiences. Although mindfulness interventions do not directly target goal setting or explicit recovery planning, the reinforcement of agency provides an essential psychological foundation for the later development of goals and pathways in the recovery process.
As individuals’ internal capacities increase, several interventions begin to integrate the strengthening of agency with the development of pathways. Mandala Art Therapy, for instance, enhances motivation to move away from negative emotional states (agency) through creative expression such as mandala coloring, while simultaneously providing strategies for managing negative emotions and improving self-understanding and interpersonal awareness. Another intervention, Modified Mindfulness-Based Cognitive Therapy (M-MBCT), offers structured strategies (pathways) for regulating thoughts and emotions, promoting self-care through mindfulness practices, and fostering motivation and energy to act (agency) via emotional acceptance and sustained mindfulness practice.
In addition, empowerment-based interventions demonstrate a dominant role in strengthening agency by helping individuals recognize their personal strengths and capabilities, enhance self-confidence, and build the belief that they can make autonomous decisions. Reductions in self-stigma and improvements in self-worth further reinforce internal motivation during recovery. Empowerment interventions also support the development of pathways through skills training and increased social participation, enabling individuals to access relevant resources and support systems while identifying adaptive ways to manage life challenges.
Further evidence of hope enhancement through the integration of agency and pathways is found in Narrative Enhancement and Cognitive Therapy (NECT). This intervention employs cognitive restructuring and the development of more adaptive self-narratives to reduce self-stigma and hopelessness. These processes simultaneously open cognitive pathways by offering alternative ways of interpreting life experiences and confronting recovery-related challenges. By fostering new self-narratives, NECT not only strengthens internal motivation but also provides sustainable cognitive routes that help individuals maintain hope over time.
Similarly, the Abridged Illness Management and Recovery Program (AIMR) emphasizes the operational development of pathways through illness management education, medication understanding, and relapse prevention strategies, thereby offering concrete routes toward stability and recovery. Active participation in AIMR learning processes further strengthens agency by enhancing individuals’ sense of competence and engagement. These findings indicate that AIMR supports hope formation by combining internal motivation with practical recovery steps, enabling individuals to sustain hope in a structured and everyday context.
Another intervention encompassing both agency and pathways is Mindfulness-Based Stress Reduction (MBSR). Through education and mindful awareness of illness, stress management skills, and reflection on personal progress, MBSR enhances motivation, positive emotional states, and self-confidence (agency). Additionally, the intervention provides practical techniques for cultivating calmness and coping with difficult situations through breathing exercises, body scans, and meditation practices, thereby strengthening recovery pathways.
Despite the wide range of interventions designed to support recovery in individuals with schizophrenia, not all interventions comprehensively address the three components of Hope Theory. Among the fourteen interventions identified in this scoping review, only a subset, namely Hope Instillation, psychoeducation, the Needs-Tailored Recovery Program, Positive Psychotherapy for Psychosis (PPP), Educational Music Therapy, and Social Recovery Therapy (SRT), were found to address all three components of hope. These interventions are holistic and comprehensive in nature, as they not only assist individuals in defining recovery goals, but also provide pathways to achieve these goals while strengthening agency through enhanced motivation and self-belief, both of which are essential for sustained recovery.
Overall, this scoping review highlights that a range of interventions may strengthen hope among people living with schizophrenia by supporting goal development, motivational capacity, and the identification of meaningful recovery pathways. These elements can contribute to personal recovery, well-being, and the pursuit of a meaningful life. While Snyder’s Hope Theory offers a valuable framework for understanding hope through goals, agency, and pathways, this model primarily emphasizes individual cognitive processes and may not fully capture the broader relational, social, spiritual, cultural, and systemic dimensions of hope identified in schizophrenia recovery. Findings from this review suggest that hope is also shaped by interpersonal support, community belonging, spirituality, and access to supportive care. Therefore, fostering hope in schizophrenia recovery may require broader, person-centered, and contextually responsive approaches beyond exclusively individualistic frameworks.
In addition, although this review identified a wide range of psychosocial and therapeutic interventions, no fully developed digital-based interventions specifically targeting hope enhancement in schizophrenia were found within the included studies. This may indicate that digital interventions in this area are still emerging. Recent developments, such as Hope4Schizophrenia, suggest that technology-based interventions are being explored to support recovery and enhance hope, although they remain in early stages of development and evaluation. Therefore, digital interventions represent a promising area for future research, particularly in improving accessibility, scalability, and personalization of hope-enhancing strategies for individuals with schizophrenia.
Future research should continue to explore culturally sensitive and recovery-oriented conceptualizations of hope to better inform mental health interventions and practice.
Limitation
This scoping review describes interventions to foster and increase hope in people living with schizophrenia. The use of broader psychosis-related search terms may have increased initial heterogeneity; however, this strategy was intended to maximize comprehensiveness while eligibility criteria maintained diagnostic specificity. The results of this review highlight the need for further research and the importance of considering the specific needs and characteristics of the population when designing and implementing interventions for people living with schizophrenia. However, this scoping review still has several limitations that must be acknowledged. These limitations include the fact that the interventions in this study were mostly conducted in developed countries, with few conducted in developing countries. Another limitation is that not all studies focused solely on patients with schizophrenia. There were several studies whose research subjects are people with mental disorders, including schizophrenia. In addition, this scoping review did not consider studies published in languages other than English, thus limiting the findings of articles written in other languages.
Implication to Practice
This study has several implications for nursing practice in improving the hope of schizophrenia survivors. First, this study has implications for nursing practice. Nurses can collaborate with psychologists, psychiatrists, therapists, and other health professionals to implement interventions to improve hope in schizophrenia survivors. Survivors are taught to listen to themselves and take responsibility for their lives so that they can build and maintain hope in their recovery.
This review has implications for further research, particularly in nursing practice, suggesting that hope should be the main focus of recovery-oriented interventions. A person who has positive hope in the recovery process will have higher psychological well-being. A person with high psychological well-being will be able to accept their condition, establish positive relationships with others, be autonomous, be able to control the conditions around them, have goals and meaning in life, and continue to grow personally.
Conclusion
The conclusion of this study shows that there are 14 articles from six databases that discuss interventions to increase hope in patients with schizophrenia. These interventions include Mandala Art Therapy, Mindfulness Therapy, Positive Psychotherapy for Psychosis (PPP), Mixed-mode Mindfulness-Based Cognitive Therapy (M-MBCT), Social Recovery Therapy (SRT), Educational Music Therapy, Narrative Enhancement and Cognitive Therapy (NECT), Abridged Illness Management and Recovery Program (AIMR), Positive Psychology Expressive Writing (PPEW), Hope Instillation, psychoeducation, Empowerment Intervention, Mindfulness-Based Stress Reduction (MBSR), and The Needs-Tailored Recovery Program. Although they use different approaches, the interventions found in this scoping review are inseparable from the three components of hope theory, namely goals, pathway thinking, and agency thinking.
This finding highlights that hope can be enhanced through a variety of intervention approaches, including those not explicitly grounded in hope theory, but which incorporate elements of goal-setting, strategic planning, and motivational enhancement. From a practical perspective, health professionals can integrate these components into routine mental health care to support recovery-oriented practice, particularly by fostering goal clarity, strengthening problem-solving pathways, and enhancing patient motivation.
For future research, further studies are needed to explore the comparative effectiveness of different intervention models, including culturally adapted and digital-based interventions, as well as to examine how various theoretical approaches contribute to enhancing hope in diverse populations of individuals with schizophrenia.
Acknowledgments
The author would like to thank the research team who have contributed to the completion of this research and also thank our institution for supporting the implementation of this research.
Funding
This research was conducted with the support of Universitas Padjadjaran.
Disclosure
The authors declare that there is no conflict of interest in this research.
References
1. Samuelsen SS, Moljord IEO, Eriksen L. Re-establishing and preserving hope of recovery through user participation in patients with a severe mental disorder: the self-referral-to-inpatient-treatment project. Nurs Open. 2016;3(4):222–16. doi:10.1002/nop2.59
2. Tandon R, Gaebel W, Barch DM, et al. Definition and description of schizophrenia in the DSM-5. Schizophr Res. 2013;150(1):3–10. doi:10.1016/j.schres.2013.05.028
3. Evaluation I for HM and. World mental health report: transforming mental health for all. World Health Organization; 2022.
4. KEMENTERIAN. Laporan Riskesdas 2018 Nasional.pdf. Lembaga Penerbit Balitbangkes. 2018:hal156. Available from: https://repository.badankebijakan.kemkes.go.id/id/eprint/3514/1/LaporanRiskesdas2018Nasional.pdf.
5. Jääskeläinen E, Juola P, Hirvonen N, et al. A systematic review and meta-analysis of recovery in schizophrenia. Schizophr Bull. 2013;39(6):1296–1306. doi:10.1093/schbul/sbs130
6. Dziwota E, Stepulak MZ, Włoszczak-Szubzda A, Olajossy M. Social functioning and the quality of life of patients diagnosed with schizophrenia. Ann Agric Environ Med. 2018;25(1):50–55. doi:10.5604/12321966.1233566
7. Townsend MC, Morgan KI. Psychiatric Mental Health Nursing: Concepts of Care in Evidence-Based Practice.
8. Lysaker PH, Salyers MP, Tsai J, Spurrier LY, Davis LW. Clinical and psychological correlates of two domains of hopelessness in schizophrenia. J Rehabil Res Dev. 2008;45(6):911. doi:10.1682/JRRD.2007.07.0108
9. Ridgway P. Restorying psychiatric disability: learning from first person recovery narratives. Psychiatr Rehabil J. 2001;24(4):335. doi:10.1037/h0095071
10. Lysaker PH, Clements CA, Wright DE, Evans J, Marks KA. Neurocognitive correlates of helplessness, hopelessness, and well-being in schizophrenia. J Nerv Ment Dis. 2001;189(7):457–462. doi:10.1097/00005053-200107000-00007
11. Lysaker PH, Roe D, Yanos PT. Toward understanding the insight paradox: internalized stigma moderates the association between insight and social functioning, hope, and self-esteem among people with schizophrenia spectrum disorders. Schizophr Bull. 2007;33(1):192–199. doi:10.1093/schbul/sbl016
12. Bellack AS. Scientific and consumer models of recovery in schizophrenia: concordance, contrasts, and implications. Schizophr Bull. 2006;32(3):432–442. doi:10.1093/schbul/sbj044
13. Lysaker PH, Roe D, Buck KD. Recovery and wellness amidst schizophrenia: definitions, evidence, and the implications for clinical practice. J Am Psychiatr Nurses Assoc. 2010;16(1):36–42. doi:10.1177/1078390309353943
14. Leamy M, Bird V, Le Boutillier C, Williams J, Slade M. Conceptual framework for personal recovery in mental health: systematic review and narrative synthesis. Br J Psychiatry. 2011;199(6):445–452. doi:10.1192/bjp.bp.110.083733
15. Deegan PE. Recovery the lived experience. Pyschosoc Rehalb J. 1998;11(4):11–19.
16. Andresen R, Oades L, Caputi P. The experience of recovery from schizophrenia: towards an empirically validated stage model. Aust N Z J Psychiatry. 2003;37(5):586–594. doi:10.1046/j.1440-1614.2003.01234.x
17. Soundy A, Stubbs B, Roskell C, Williams SE, Fox A, Vancampfort D. Identifying the facilitators and processes which influence recovery in individuals with schizophrenia: a systematic review and thematic synthesis. J Ment Health. 2015;24(2):103–110. doi:10.3109/09638237.2014.998811
18. Noh C, Choe K, Yang B. Hope from the perspective of people with schizophrenia (Korea). Arch Psychiatr Nurs. 2008;22(2):69–77. doi:10.1016/j.apnu.2007.10.002
19. Snyder CR. TARGET ARTICLE: hope theory: rainbows in the mind. Psychol Inq. 2002;13(4):249–275. doi:10.1207/S15327965PLI1304_01
20. Schrank B, Bird V, Rudnick A, Slade M. Determinants, self-management strategies and interventions for hope in people with mental disorders: systematic search and narrative review. Soc Sci Med. 2012;74(4):554–564. doi:10.1016/j.socscimed.2011.11.008
21. Kylmä J, Juvakka T, Nikkonen M, Korhonen T, Isohanni M. Hope and schizophrenia: an integrative review. J Psychiatr Ment Health Nurs. 2006;13(6):651–664. doi:10.1111/j.1365-2850.2006.01012.x
22. Çam O, Yalçıner N. Mental illness and recovery. J Psychiatr Nurs. 2018;9(1):55–60.
23. Joanna Briggs Institute. JBI manual for evidence synthesis. 2020. Available from: https://jbi-global-wiki.refined.site/space/MANUAL.
24. Öztürk Z, Şahin Altun Ö. The effect of nursing interventions to instill hope on the internalized stigma, hope, and quality of life levels in patients with schizophrenia. Perspect Psychiatr Care. 2022;58(1):364–373. doi:10.1111/ppc.12800
25. Kim H, Kim S, Choe K, Kim JS. Effects of mandala art therapy on subjective well-being, resilience, and hope in psychiatric inpatients. Arch Psychiatr Nurs. 2018;32(2):167–173. doi:10.1016/j.apnu.2017.08.008
26. Harmanci P, Budak FK. The effect of psychoeducation based on motivational interview techniques on medication adherence, hope, and psychological well-being in Schizophrenia patients. Clin Nurs Res. 2022;31(2):202–216. doi:10.1177/10547738211046438
27. Özdemir AA, Kavak Budak F. The effects of mindfulness-based stress reduction training on hope, psychological well-being, and functional recovery in patients with schizophrenia. Clin Nurs Res. 2022;31(2):183–193. doi:10.1177/10547738211039069
28. Astuti HWY, Agustin M, Sari SP, Wijayanti DY, Sarjana W, Locsin RC. Effects of mindfulness on stimulating hope and recovery among people with schizophrenia. Nurse Media J Nurs. 2020;10(2):119–129. doi:10.14710/nmjn.v10i2.28775
29. Liu WI, Hsieh WL, Lai CT, Liu CC, Tai YM, Liu CY. Effectiveness of a needs-tailored nurse-led recovery program for community-dwelling people with schizophrenia: a cluster-randomized controlled trial. BMC Nurs. 2024;23(1):329. doi:10.1186/s12912-024-01986-x
30. Hasan A, Musleh M. The impact of an empowerment intervention on people with schizophrenia: results of a randomized controlled trial. Int J Soc Psychiatry. 2017;63(3):212–223. doi:10.1177/0020764017693652
31. Dai J, Sun D, Li B, et al. Mixed-Mode Mindfulness-based cognitive therapy for psychological resilience, Self Esteem and Stigma of patients with schizophrenia: a randomized controlled trial. BMC Psychiatr. 2024;24:1–10.
32. Wai CMH, Lau B, Leung J, et al. Positive psychotherapy for psychosis in Hong Kong: a randomized controlled trial. Schizophr Res. 2022;240:175–183. doi:10.1016/j.schres.2021.12.044
33. Silverman MJ. Effects of educational music therapy on state hope for recovery in acute care mental health inpatients: a cluster-randomized effectiveness study. Front Psychol. 2016;7:1569. doi:10.3389/fpsyg.2016.01569
34. Yanos PT, Lysaker PH, Silverstein SM, et al. A randomized-controlled trial of treatment for self-stigma among persons diagnosed with schizophrenia-spectrum disorders. Soc Psychiatry Psychiatr Epidemiol. 2019;54(11):1363–1378. doi:10.1007/s00127-019-01702-0
35. Wong RHK, Wing Cheong Au R, Wai Lan C, et al. A randomized controlled trial on the effectiveness of the abridged illness management and recovery program for people with schizophrenia spectrum disorders. Hong Kong J Occup Ther. 2023;36(2):118–127. doi:10.1177/15691861231204904
36. Tang MW, Cheng Y, Zhang YH, Liu SJ. Effect of a positive psychology expressive writing on stigma, hope, coping style, and quality of life in hospitalized female patients with Schizophrenia: a randomized, controlled trial. Perspect Psychiatr Care. 2023;2023(1):1577352. doi:10.1155/2023/1577352
37. Fowler D, Hodgekins J, French P. Social recovery therapy in improving activity and social outcomes in early psychosis: current evidence and longer term outcomes. Schizophr Res. 2019;203:99–104. doi:10.1016/j.schres.2017.10.006
38. Gum A, Snyder CR. Coping with terminal illness: the role of hopeful thinking. J Palliat Med. 2002;5(6):883–894. doi:10.1089/10966210260499078
39. Coşkun E, Şahin Altun Ö. The relationship between the hope levels of patients with schizophrenia and functional recovery. Arch Psychiatr Nurs. 2018;32(1):98–102. doi:10.1016/j.apnu.2017.10.006
40. Snyder CR, Irving LM, Anderson JR. Hope and health. Handbook Soc Clin Psychol. 1991;162:285–305.
41. Snyder CR. Conceptualizing, measuring, and nurturing hope. J Counseling Develop. 1995;73(3):355–360. doi:10.1002/j.1556-6676.1995.tb01764.x
42. Woodbury J. Advising with a strong assessment component helps students achieve their educational goals. NACADA J. 1999;19(2):10–17. doi:10.12930/0271-9517-19.2.10
43. Snyder CR. The Psychology of Hope: You Can Get There From Here. Simon and Schuster; 1994.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.