Back to Journals » ClinicoEconomics and Outcomes Research » Volume 16
Homologous Recombination Repair Testing Patterns and Outcomes in mCRPC by Alteration Status and Race
Authors Bilen MA, Khilfeh I, Rossi C, Muser E, Morrison L, Hilts A, Diaz L, Lefebvre P, Pilon D, George DJ
Received 16 March 2024
Accepted for publication 27 August 2024
Published 6 September 2024 Volume 2024:16 Pages 657—674
DOI https://doi.org/10.2147/CEOR.S468680
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Samer Hamidi
Mehmet Asim Bilen,1 Ibrahim Khilfeh,2 Carmine Rossi,3 Erik Muser,2 Laura Morrison,3 Annalise Hilts,3 Lilian Diaz,3 Patrick Lefebvre,3 Dominic Pilon,3 Daniel J George4
1Department of Hematology and Medical Oncology, Emory University School of Medicine, Atlanta, GA, USA; 2Janssen Scientific Affairs, LLC, Horsham, PA, USA; 3Analysis Group, Inc., Montréal, QC, Canada; 4Department of Medicine, Duke University Cancer Center, Durham, NC, USA
Correspondence: Carmine Rossi, Analysis Group, Inc., 1190 avenue des Canadiens-de-Montréal, Tour Deloitte, Suite 1500, Montréal, QC, H3B 0G7, Canada, Tel +1 514-871-4233, Email [email protected]
Background: Alterations in DNA damage repair genes in advanced prostate cancer (PC) may impact responses to therapy and clinical outcomes. This study described homologous recombination repair (HRR) testing patterns and clinical outcomes among patients with metastatic castration-resistant prostate cancer (mCRPC) by HRR alteration status and race in the United States (US).
Methods: Clinical data in the nationwide (US-based) Flatiron Health-Foundation Medicine, Inc. (FMI) Metastatic PC Clinico-Genomic Database were evaluated (01/01/2011– 12/31/2022). Patients initiating first-line (1L) mCRPC therapy on or after mCRPC diagnosis were included. Testing patterns, time-to-next treatment, overall survival (OS), and time-to-prostate specific antigen response were described.
Results: Of the 1367 patients with mCRPC and at least one HRR panel test prior to or on the date of 1L mCRPC therapy initiation, 332 (24.3%) were HRR positive (White patients: n = 219 [66.0%]; Black patients: n = 37 [11.1%]) and 1035 (75.7%) were HRR negative (White patients: n = 702 [67.8%]; Black patients: n = 84 [8.1%]). The mean time between first positive test and 1L mCRPC therapy initiation date was 588 days (White patients: 589 days; Black patients: 639 days). Among HRR positive relative to negative patients, trends for faster progression (respective 12-month rate overall: 71.1% and 63.7%; White patients: 72.5% and 64.0%; Black patients: 65.4% and 56.4%), shorter OS (respective 24-month rate overall: 46.8% and 51.9%; White patients: 48.6% and 46.2%; Black patients: 52.8% and 54.1%), and decreased treatment response (respective 12-month rate overall: 24.3% and 37.9%; White patients: 24.5% and 35.2%; Black patients: 17.0% and 43.9%) were observed.
Conclusion: Patients with mCRPC positive for HRR alterations tended to exhibit poorer treatment responses and clinical outcomes than those with a negative status. These findings highlight the importance of timely genetic testing in mCRPC, particularly among Black patients, and the need for improved 1L targeted therapies to address the unmet need in HRR positive mCRPC.
Keywords: burden of illness, electronic health records, homologous recombination repair genes, metastatic castration-resistant prostate cancer, next-generation sequencing testing, precision therapy
Introduction
Prostate cancer (PC) is the most common non-cutaneous cancer diagnosis and the second leading cause of cancer-related deaths among men in the United States (US).1,2 PC is more likely to develop in non-Hispanic Black men, who also exhibit the highest age-adjusted PC-related death rate among races.2 Patients diagnosed with early-stage PC generally have a favorable prognosis, but those with de novo metastatic disease have a dismal 5-year survival rate of 34.1%.2
For many years, androgen deprivation therapy (ADT) monotherapy was considered the standard of care for patients with metastatic and non-metastatic PC.3,4 Although patients may initially respond well to ADT, their disease typically progresses to castration-resistant prostate cancer (CRPC) after two to three years.5,6 Phase 3 trials of androgen-receptor signaling inhibitors (ARSIs) have proven superiority over ADT monotherapy in men with non-metastatic CRPC and metastatic castration-sensitive prostate cancer.7,8 Among men with non-metastatic CRPC treated with ADT monotherapy, approximately 60% develop metastatic castration-resistant prostate cancer (mCRPC) within five years of CRPC diagnosis.9 In the last couple of decades, mCRPC therapies with different mechanisms of action, including ARSIs, taxane-based chemotherapy, immunotherapy, and radiopharmaceuticals have been shown to prolong survival;10–15 however, mCRPC remains incurable, and the attrition rate between first-line (1L) and subsequent-line treatments has been shown to be about 45%,16 urging the search for more effective therapies, particularly in 1L.
With advances in our understanding of the molecular characteristics of mCRPC, recent efforts on mCRPC therapeutic development have focused on precision therapies that target specific gene alterations, particularly those associated with an aggressive disease course and those predictive of treatment responses.4,17,18 For instance, alterations in genes involved in the DNA homologous recombination repair (HRR) pathway in PC have been associated with more advanced disease and shorter cancer-specific survival.19–21 Tumors with HRR alterations are also more susceptible to therapies that impair alternative DNA repair pathways, such as poly ADP-ribose polymerase (PARP) inhibitors,18 and patients with mCRPC harboring HRR alterations treated with PARP inhibitors have shown improved outcomes including radiographic progression-free survival in phase 3 clinical trials compared to enzalutamide or abiraterone acetate,22–25 or in a phase 2 efficacy and safety clinical trial.26
Genetic testing, given its utility in screening, risk assessment, management, and precision treatment for PC, has been integrated into guidelines and recommendations from professional organizations and includes recommendations for next-generation sequencing (NGS) assessment of germline and/or somatic alterations in men at risk of or diagnosed with metastatic PC.27 Notably, genetic studies of PC have largely focused on White patients.28,29 A recent study has highlighted the disparities in genetic testing engagement among African American men, which is concerning as this testing inequality likely reduces access to precision treatment for racial minorities.30
With the expanding guideline recommendations on genetic testing for HRR alterations, there is a need to characterize real-world testing patterns and clinical outcomes among patients with mCRPC to better understand testing trends and differences in disease course by HRR alteration status. This is particularly important for Black patients who have been underrepresented in genetic studies to ensure they are considered for biomarker-targeted therapeutic approaches in clinical practice. This study was conducted to understand NGS testing patterns and positivity rates for HRR alterations in men who have mCRPC, including subgroups of White or Black men, and to understand the unmet need that exists in HRR positive mCRPC as reflected by time-to-next treatment (TTNT), overall survival (OS), and prostate-specific antigen (PSA) response using electronic health record (EHR)-derived data.
Materials and Methods
Data Source
Data from the nationwide (US-based) Flatiron Health Metastatic PC EHR-derived database (hereafter “EHR-derived database”) were used to assess HRR alteration testing rates from 1 January 2013 to 31 December 2022 (see Study Measures and Outcomes: HRR Alteration Testing Rates [EHR-Derived Database] section). The EHR-derived database is a longitudinal database comprising de-identified patient-level structured and unstructured data from ~280 US cancer clinics (~800 sites of care) and curated via technology-enabled abstraction.31,32 The database included a sample of patients with chart-confirmed metastatic PC (International Classification of Diseases, Ninth/Tenth Revision, Clinical Modification [ICD-9-CM: 185.x or ICD-10-CM: C61.x]) with at least two documented clinical visits in the Flatiron Health network, on different days, occurring on or after 1 January 2013. The detailed clinical data extracted from structured EHRs, as well as unstructured data abstracted from physicians’ notes and other documents (through technology-enabled human abstraction and natural language processing, including manual review by a centralized team of clinically trained professionals with quality control measures such as logic checks), contained information on demographics, diagnoses, visits, laboratory tests and vitals, medication administration, medication prescriptions and orders, performance status, and insurance data, and enhanced data elements on PC-related characteristics, including dates of initial/metastatic PC/CRPC diagnoses, lines of therapy (LOTs), PSA measurements, NGS testing dates (excluding results), and mortality (mortality data were obtained from EHR sources as well as through linkages via deterministic matching with the Social Security Death Index and obituary data).
Because the EHR-derived database contains information on NGS testing dates but not the results, data from the nationwide (US-based) Flatiron Health-Foundation Medicine, Inc. (FMI) Metastatic PC Clinico-Genomic Database (hereafter “CGDB”), which contains information on patients with available NGS test results, was used to assess HRR testing patterns, alteration positivity rates, and clinical outcomes from 1 January 2011 to 30 June 2022. The CGDB does not include untested patients; and hence, it could not be used to determine HRR alteration testing rates. Retrospective longitudinal clinical data from the EHR-derived database were linked to genomic data derived from FMI comprehensive genomic profiling (CGP) tests in the CGDB by de-identified, deterministic matching.33 Genomic alterations were identified via CGP of >300 cancer-related genes on FMI’s NGS test and include tumor specimen features (eg, mutation burden, purity), alteration-level details (eg, reference and alternate alleles, allele frequency), and therapeutic recommendations reported to the physician at the time of testing.34–36
The study was considered exempt research under 45 CFR § 46.104(d)(4) as it involved only the secondary use of data that were de-identified in compliance with the Health Insurance Portability and Accountability Act (HIPAA), specifically, 45 CFR § 164.514. The research was conducted according to the principles of the Declaration of Helsinki. Flatiron Health, Inc., and FMI did not participate in data analyses.
Study Design
A retrospective longitudinal cohort study design was used to assess clinical outcomes. The index date was defined as the date of the start of 1L therapy on or after the date of mCRPC diagnosis. The baseline period was the 12 months preceding the index date. The observation period spanned from the index date to the end of clinical activity or data availability (ie, 30 June 2022).
Lines of Therapy
Oncologist-defined, rule-based LOTs (in which a LOT was originally numbered starting from a CRPC diagnosis) were renumbered such that 1L was defined as the line started on or after mCRPC diagnosis. The beginning of a LOT for mCRPC was defined as the date of treatment initiation that was on or after the mCRPC diagnosis date. For the most recent LOT, the LOT end date was defined as the date of last patient-level structured activity or the last day of the month where death was recorded, if observed. For all other LOT, the end date was the day before the start date of the next LOT. Treatments initiated within 28 days of the start of a LOT were considered part of the same LOT. ADT, either in monotherapy or in combination with other advanced PC-related therapies, was not considered as part of a LOT.
Patient Population
Patients from the EHR-derived database and CGDB were included in the study if they met the following inclusion criteria: 1) had a chart-confirmed diagnosis of metastatic PC; 2) had confirmed CRPC based on Flatiron Health’s algorithm incorporating i) physician-reported CRPC in medical chart, ii) observed rising PSA values while on hormone therapy, or iii) physician-documented rising PSA on hormone therapy plus a change in treatment; 3) were ≥18 years of age at mCRPC diagnosis (ie, latter of the date of chart-confirmed metastasis or CRPC); 4) initiated ≥1 LOT on or after mCRPC diagnosis; and 5) had ≥12 months of observation prior to the index date. Patients from the CGDB were additionally required to have ≥1 NGS HRR panel test prior to or on the index date.
For both the EHR-derived database and CGDB, patients were excluded if they used a clinical trial medication as part of 1L therapy for mCRPC.
Patients were classified into the HRR positive cohort or the HRR negative cohort based on testing results observed any time prior to or on the index date for eight out of nine alterations included as screening criteria in the MAGNITUDE trial (NCT03748641; a phase 3, randomized, placebo-controlled trial of niraparib and abiraterone acetate plus prednisone in mCRPC; pathogenic gene alterations evaluated included ATM, BRCA1, BRCA2, BRIP1, CDK12, CHEK2, FANCA, and/or PALB2; HDAC2 testing is not available in FMI data).22
Study Measures and Outcomes
HRR Alteration Testing Rates (EHR-Derived Database)
HRR alteration testing rates were assessed among patients in the EHR-derived database based on all NGS HRR panel tests received prior to or on the date of 1L mCRPC therapy initiation, reported by calendar year of 1L mCRPC therapy initiation (ie, 2013–2022).
HRR Alteration Testing Patterns and Positivity Rates (CGDB)
HRR alteration positivity rates were assessed among patients in the CGDB and defined as the proportion of patients with at least one positive test result for any HRR alteration (ie, HRR positive) among all patients with at least one NGS HRR panel test received prior to or on the date of 1L mCRPC therapy initiation. HRR alteration positivity rates were reported overall and separately for specific alterations and for co-occurring alterations (see Patient Population section).
The following testing patterns were measured among patients with HRR positive results received before 1L mCRPC therapy and were described based on the date the specimen was collected in the CGDB: 1) time from first positive test to the date of 1L mCRPC therapy initiation; 2) metastatic disease at first positive test and time from metastasis to first positive test; 3) castrate-resistant disease at first positive test and time from castrate-resistant disease to first positive test; 4) type of testing used at first positive test (ie, tumor tissue or blood; of note, the first observed specimen collection for a tissue test was on 4 January 2001, and the first observed specimen collection for a liquid test was on 20 June 2016); and 5) type of alteration (ie, somatic, germline, unknown, missing).
HRR alteration positivity rates and testing patterns were also assessed cumulatively over the entire observation period (ie, across patients’ entire observed medical history) to account for repeated testing as well as for cases in which patients received initial NGS HRR alteration testing after the date of 1L mCRPC therapy initiation. Additionally, to understand retesting patterns and the potential value of retesting, the following were described among patients with at least one negative test followed by a subsequent positive test: 1) time between the first and second test; 2) type of testing (ie, tissue or liquid) used for the first and second tests; and 3) disease stage (ie, localized PC, non-metastatic CRPC, metastatic castration-sensitive PC, and mCRPC) at first and second tests.
Clinical Outcomes (CGDB)
Clinical outcomes, including TTNT, OS, and prostate-specific antigen 90 (PSA90) response were assessed among the HRR positive and HRR negative cohorts during the observation period. TTNT was included as a study outcome given it may serve as a proxy for disease progression in databases that do not routinely capture this information.37 PSA90 response was included as a study outcome given its association with long-term clinical benefit in CRPC.38
TTNT was defined as the time from 1L initiation (index date) to the start of second-line (2L) therapy or the use of clinical trial medication.
OS was defined as the time from the index date to the date of death from any cause. Mortality information in the EHR-derived database is presented as the month and year of death. The date of death was imputed as the last date of clinical activity observed during that month. If no clinical activity was observed in the month of death, the death date was imputed as the 15th of the respective month.
PSA90 response was defined as a decline of ≥90% in PSA from the most recent baseline value obtained within 13 weeks prior to and including the date of 1L initiation.
Statistical Analysis
Baseline patient characteristics and HRR alteration testing rates and patterns were described using means, standard deviations, and medians for continuous variables, and frequencies and proportions for categorical variables.
Kaplan-Meier (KM) analysis was used to assess the proportion of patients initiating the next treatment (ie, 2L) and the proportion achieving PSA90, both up to 12 months post-index, as well as the proportion of patients who were alive up to 24 months post-index; the median TTNT, OS, and PSA90 time were also reported, if observed. All time-to-event analyses were censored at the earliest of 1) the date of the first positive HRR alteration (for HRR negative patients only); 2) end of clinical activity; 3) end of data availability (30 June 2022); or 4) 1L therapy end date (PSA90 response only).
All analyses were descriptive (ie, no formal statistical testing or generated p-values) and were not adjusted for potential baseline confounders between the HRR positive and HRR negative cohorts. All results were also stratified by race (ie, White patients or Black patients; data by ethnicity were not available); patients with non-White/non-Black or unknown race were included in the overall HRR positive or negative cohorts. HRR alteration testing rates were also stratified by academic or community-based practice settings.
Results
HRR Alteration Testing Rates
From 2013 to 2022, 30.4% (2628 of 8638) patients included in the EHR-derived database were tested for HRR alterations at any time (White patients: 30.2% [1666 of 5524]; Black patients: 29.4% [252 of 858]). More specifically, 8.9% (767 of 8638) patients included in the EHR-derived database were tested for HRR alterations prior to or on the date of 1L mCRPC therapy initiation (Figure 1). Stratified by race, the HRR alteration testing rate before 1L mCRPC was 9.2% (506 of 5524) among White patients and 7.3% (63 of 858) among Black patients. Stratified by practice setting, the HRR alteration testing rate before 1L mCRPC was 7.8% (574 of 7323) among patients from community-based practices and 14.7% (160 of 1085) among patients from academic-based practices (Supplemental Figure 1).
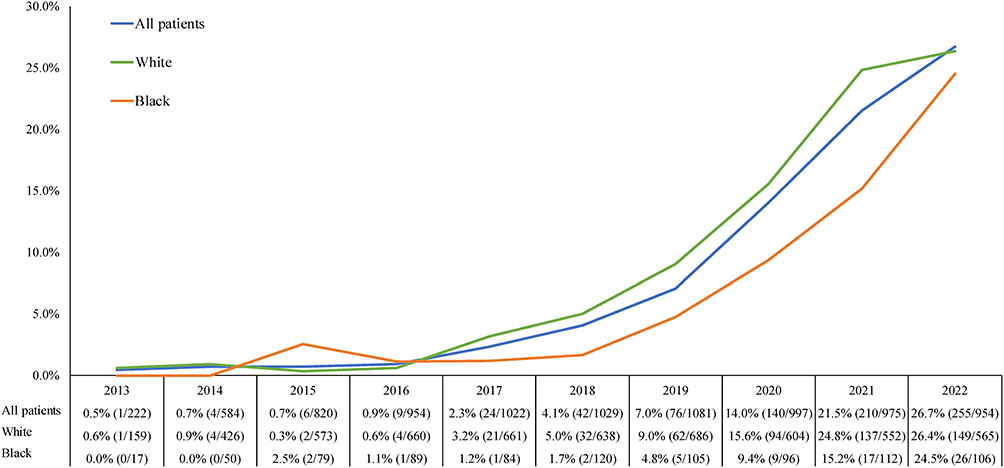 |
Figure 1 Proportion of patients in the EHR-derived database with ≥1 NGS test prior to or on the date of 1L therapy initiation, by calendar yeara,b. Abbreviations: 1L, first-line; EHR, electronic health record; HRR, homologous recombination repair; mCRPC, metastatic castration-resistant prostate cancer; NGS, next-generation sequencing. Notes: aTesting rates are reported based on the calendar year of 1L mCRPC therapy initiation and include all HRR panel tests prior to or on the date of 1L mCRPC therapy initiation. bPatients with non-White/non-Black or unknown race were included in the “all patients” population. |
Over time, HRR alteration testing rates prior to or on the date of 1L mCRPC therapy in the EHR-derived database increased from 0.0% in 2013 to 26.7% in 2022 (White patients: 0.0% to 26.4%; Black patients: 0.0% to 24.5%).
Baseline Characteristics of Patients from the CGDB
A total of 1367 patients with mCRPC and at least one NGS HRR panel test prior to or on the date of 1L mCRPC therapy initiation were included from the CGDB (Figure 2). Of these patients, 332 (24.3%) were HRR positive, among whom 219 (66.0%) were White patients and 37 (11.1%) were Black patients; 1035 (75.7%) were HRR negative, among whom 702 (67.8%) were White patients and 84 (8.1%) were Black patients.
 |
Figure 2 Selection of the study population from the CGDB. Abbreviations: 1L, first-line; CGDB, Clinico-Genomic Database; EHR, Electronic Health Records; HRR, homologous recombination repair; mCRPC, metastatic castration-resistant prostate cancer; NGS, next-generation sequencing. Notes: aContinuous clinical activity was defined as the period from the first to last record in the EHR-derived database observed across all component tables. bPatients with non-White/non-Black or unknown race were included in the overall HRR positive and HRR negative populations. |
Overall, the mean age was 70 years in the HRR positive cohort (White patients: 70 years; Black patients: 68 years) and 71 years in the HRR negative cohort (White patients: 71 years; Black patients 68 years) (Table 1). During the baseline period, most patients in both cohorts were treated at community-based oncology practices (HRR positive: 82.2%; HRR negative: 79.5%). The most frequently used medications as a component of 1L mCRPC therapy were abiraterone acetate (HRR positive: 27.7%; HRR negative: 30.1%), enzalutamide (HRR positive: 25.9%; HRR negative: 30.6%), and docetaxel (HRR positive: 20.5%; HRR negative: 20.3%). Olaparib was used by 12.3% of HRR positive patients.
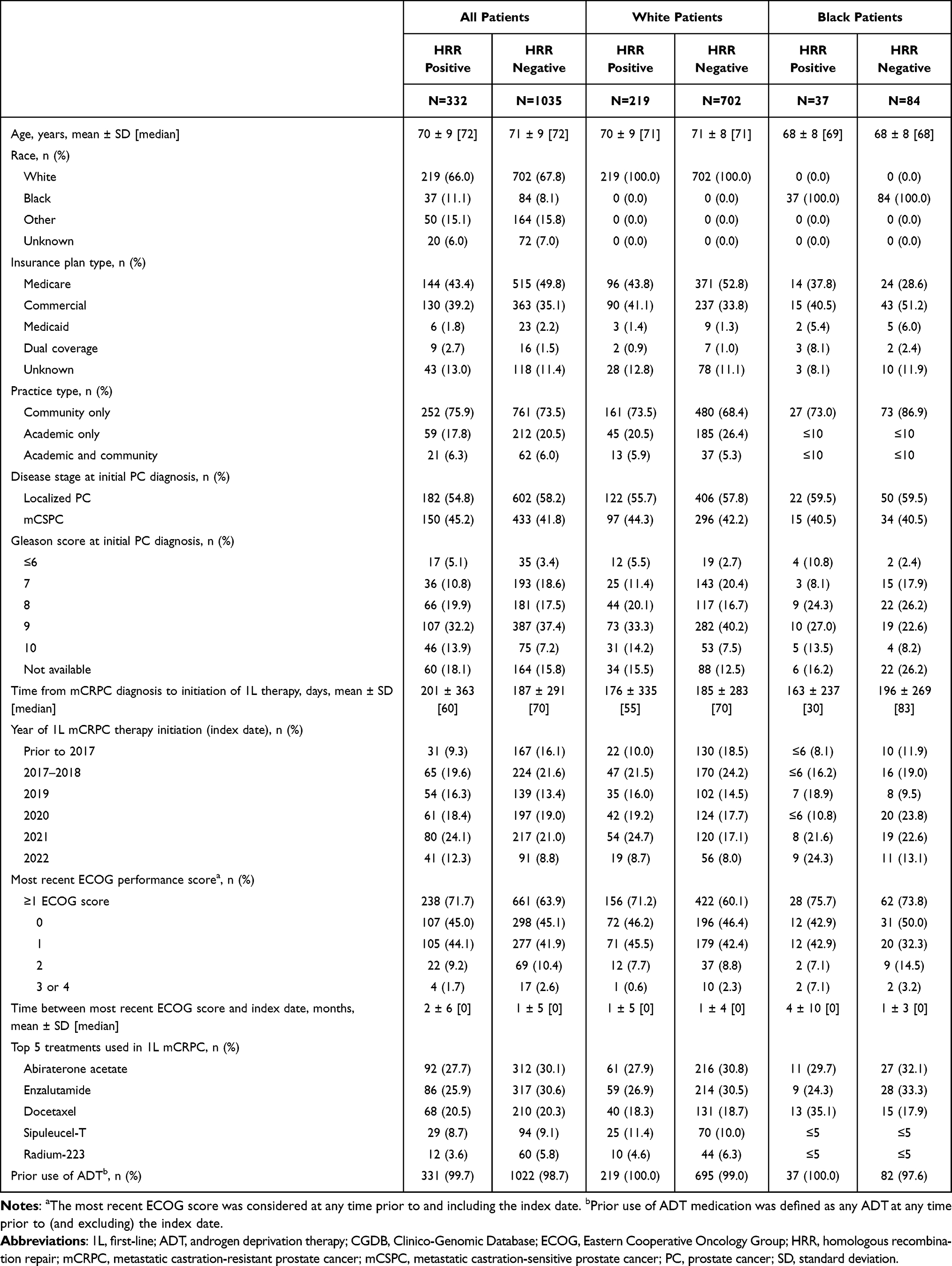 |
Table 1 Baseline Demographic and Clinical Characteristics of Patients from the CGDB |
HRR Alteration Positivity Rates and Testing Patterns Prior to or on the Date of 1L mCRPC
Among patients included in the CGDB, at the time of the first NGS test, 603 (44.1%) patients had metastatic castration-sensitive PC, 394 (28.8%) had localized PC, 332 (24.3%) had mCRPC, and 38 (2.8%) had non-metastatic CRPC. Over time, the proportion of patients with mCRPC at the time of the first NGS test has increased (Supplemental Figure 2). At the time of the first positive NGS HRR panel test, 246 (74.1%) HRR positive patients had metastatic disease and 99 (29.8%) were castrate-resistant (Table 2). Among White patients, the number of HRR positive patients with metastatic and castrate-resistant disease were 164 (74.9%) and 67 (30.6%); and among Black patients, 23 (62.2%) and 8 (21.6%), respectively.
 |
Table 2 HRR Alteration Testing Patterns Evaluated in the CGDB Prior to or on the Date of 1L mCRPC Therapy Initiation |
Tumor tissue testing was the most frequent testing method used among HRR positive patients (overall: 75.6%; White patients: 76.3%; Black patients: 73.0%). Somatic and germline alterations were observed in 97 (29.2%) and 73 (22.0%) of HRR positive patients, respectively (White patients: 25.1% and 26.5%, respectively; Black patients: 56.8% and 2.7%, respectively); the type of alteration was unknown in 50.3% (White patients: 47.5%; Black patients: 45.9%) and missing in 25.0% (White patients: 27.4%; Black patients: 24.3%) of HRR positive patients.
The mean (median) time between first positive test for any HRR alteration and the date of 1L mCRPC therapy initiation among HRR positive patients was 588 (423) days (White patients: 589 [436] days; Black patients: 639 [526] days).
Among the 1367 patients tested prior to or on the date of 1L therapy initiation, 113 (8.3%) had BRCA1/2-positive alterations and 232 (17.0%) had non-BRCA1/2-positive alterations. The distribution of specific HRR alterations was as follows: BRCA2: 7.2%, CDK12: 6.4%, ATM: 6.1%, CHEK2: 3.2%, BRCA1: 1.2%, PALB2: 1.1%, FANCA: 0.9%, and BRIP1: 0.7% (Figure 3). A total of 31 patients (2.3%) had co-occurring HRR alterations, among whom 14 had co-occurring BRCA1/2 alterations, and 17 had non-BRCA1/2 co-occurring alterations (Supplemental Table 1).
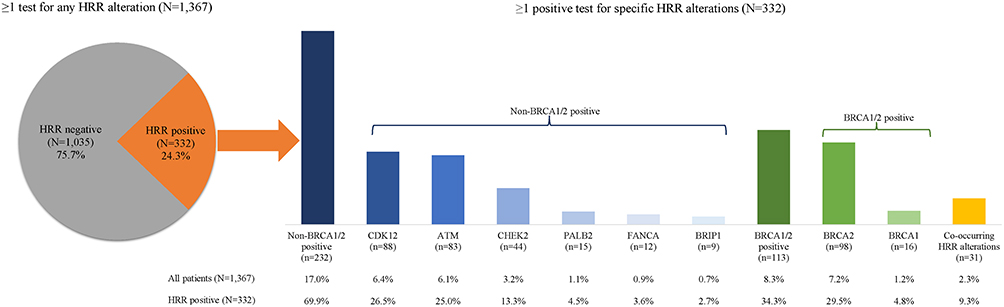 |
Figure 3 HRR alteration positivity rates evaluated in the CGDB prior to or on the date of 1L mCRPC therapy initiationa. Abbreviations: 1L, first-line; CGDB, Clinico-Genomic Database; HRR, homologous recombination repair; mCRPC, metastatic castration-resistant prostate cancer. Note: aHRR alteration positivity rates were not mutually exclusive, as patients could test positive for ≥2 different alterations. |
Stratified by race, the proportions of tested patients with BRCA1/2-positive alterations and non-BRCA1/2-positive alterations were numerically higher in Black patients (11.6% and 21.5%, respectively) than in White patients (7.7% and 17.0%, respectively; Figure 4). Co-occurring HRR alterations were observed in 3.3% of Black patients and 2.4% of White patients (Figure 4 and Supplemental Table 1).
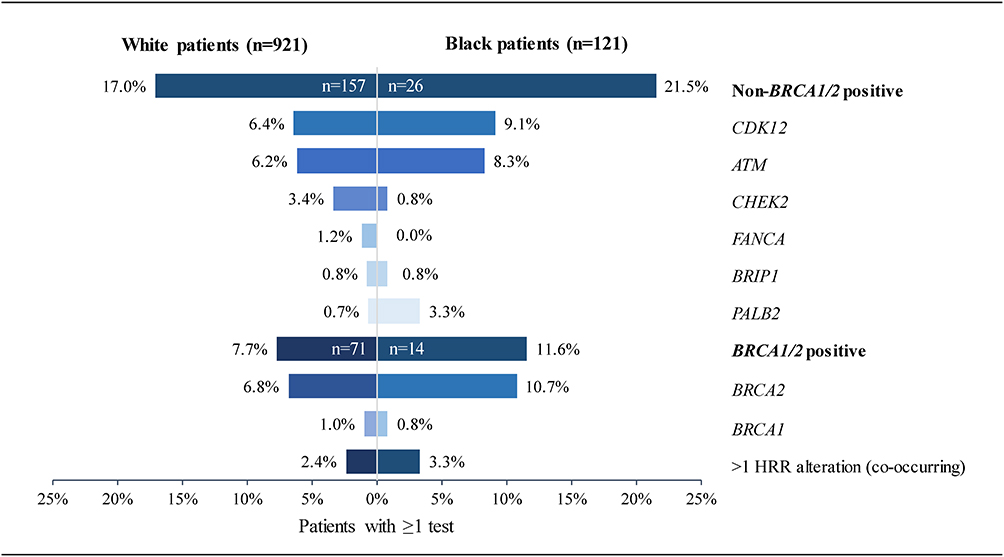 |
Figure 4 HRR alteration positivity rates evaluated in the CGDB prior to or on the date of 1L mCRPC therapy initiation, by racea. Abbreviations: 1L, first-line; CGDB, Clinico-Genomic Database; HRR, homologous recombination repair; mCRPC, metastatic castration-resistant prostate cancer. Note: aHRR alteration positivity rates were not mutually exclusive, as patients could test positive for ≥2 different alterations. |
HRR Alteration Retesting Patterns and Positivity Rates for Patients with More Than One Test Over the Entire Observation Period
A total of 2640 patients with mCRPC received at least one NGS test at any time, including 1739 White patients and 268 Black patients. Overall, 1911 (72.4%) patients had at least one negative test for any HRR alteration (White patients: 72.9%; Black patients: 70.5%); and 197 (7.5%) patients had at least two NGS HRR panel tests (White patients: 7.5%; Black patients: 7.1%) (Table 3).
 |
Table 3 HRR Alteration Retesting Patterns and Positivity Rates Evaluated in the CGDB for Patients with More Than One Test Over the Entire of the Observation Perioda,b |
All the 197 patients with at least two HRR panel tests were observed to have at least one negative test, the mean (median) time between tests was 930 (516) days (White patients: 1024 [597] days; Black patients: 503 [267] days). Out of these 197 retested patients, 27 (13.7%) patients had at least one subsequent positive test for any HRR alteration (White patients: 13.0%; Black patients: 15.8%), 13 (48.1%) had a liquid biopsy on both the first and second tests (White patients: 35.3%; Black patients: 100%). Overall, about half of these patients had mCRPC at the time of the first test (51.9%), and almost all patients had mCRPC at the time of the subsequent positive test (96.3%). The proportion of White patients with mCRPC at the time of first test and at subsequent positive test was 47.1% and 94.1%, respectively; and that of Black patients was 33.3% and 100%, respectively.
Time-to-Next Treatment
Overall, the median TTNT from the start of 1L therapy was 6.8 months for HRR positive patients (White patients: 6.6 months; Black patients: 6.6 months) and 8.1 months for HRR negative patients (White patients: 8.1 months; Black patients: 10.5 months) (Figure 5a and b).
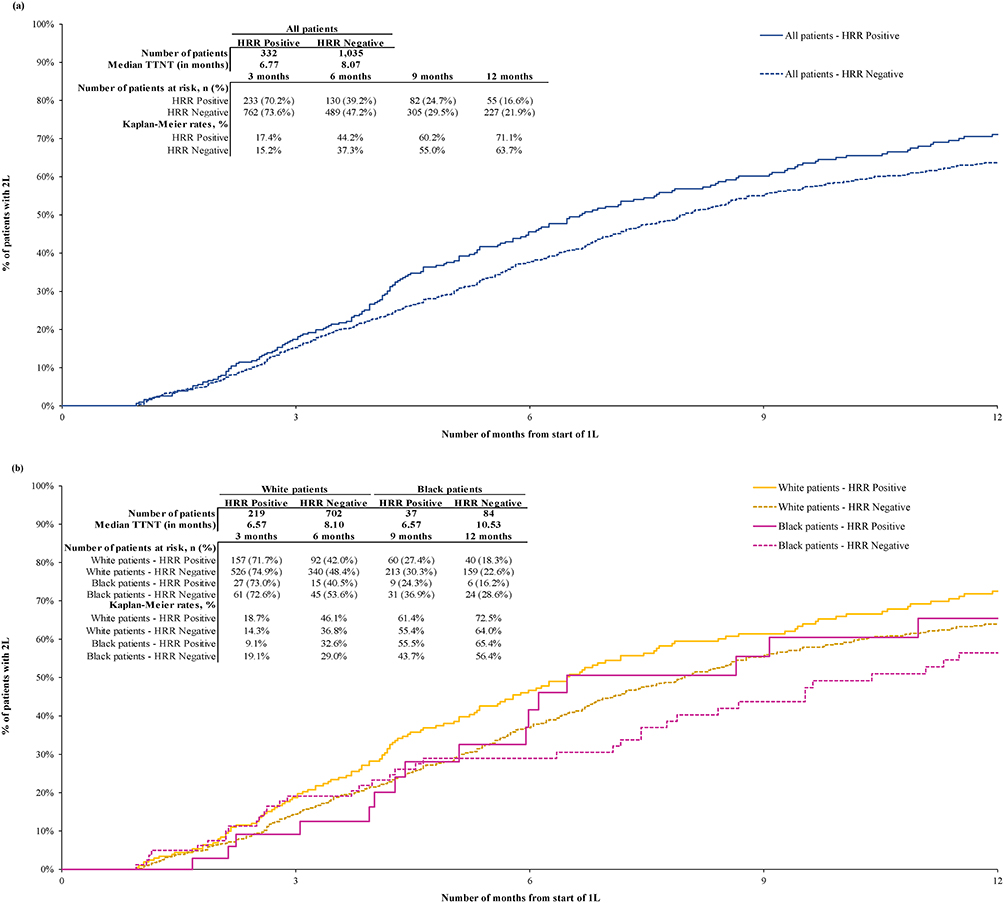 |
Figure 5 Time-to-next-treatment (a) among all patients in 1L and (b) among White and Black patients in 1La,b. Abbreviations: 1L, first-line; 2L, second-line; HRR, homologous recombination repair; TTNT, time-to-next treatment. Notes: aTTNT was defined as the time from 1L start date to 2L start date (including clinical trial medications). bTTNT was censored at the earliest of i) HRR conversion date (negative to positive only), ii) end of clinical activity (including death), or iii) end of data availability. |
The rates of initiation of a subsequent LOT (ie, 2L) among HRR positive and HRR negative patients were 17.4% and 15.2% at 3 months, 44.2% and 37.3% at 6 months, and 71.1% and 63.7% at 12 months, respectively. Stratified by race, the rates of initiation of a subsequent LOT among HRR positive and HRR negative White patients were 18.7% and 14.3% at 3 months, 46.1% and 36.8% at 6 months, and 72.5% and 64.0% at 12 months, respectively; and among HRR positive and HRR negative Black patients were 9.1% and 19.1% at 3 months, 32.6% and 29.0% at 6 months, and 65.4% and 56.4% at 12 months, respectively.
Overall Survival
Overall, the median OS after starting 1L therapy was 23.0 months for HRR positive patients (White patients: 23.7 months; Black patients 21.4 months) and 25.5 months for HRR negative patients (White patients: 26.4 months; Black patients: 26.8 months) (Figure 6a and b).
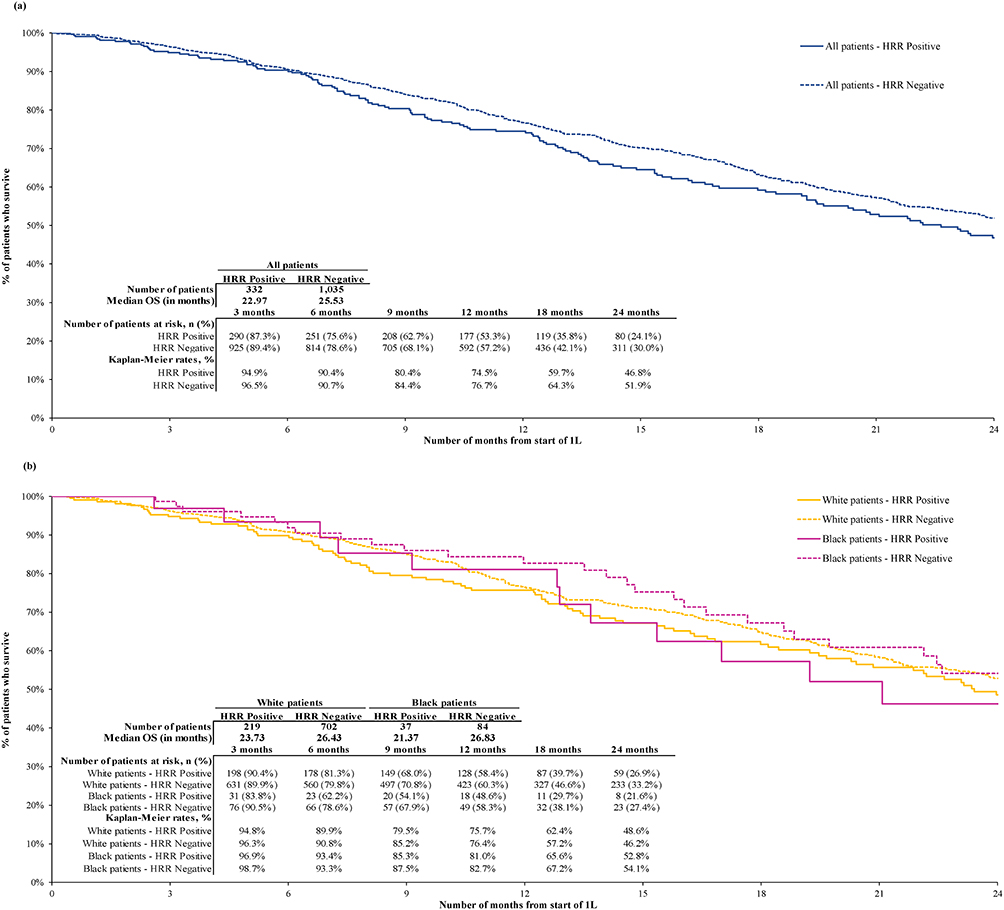 |
Figure 6 Overall survival (a) among all patients in 1L and (b) among White and Black patients in 1La,b. Abbreviations: 1L, first-line; HRR, homologous recombination repair; OS, overall survival. Notes: aOS was defined as the time from 1L start date to the date of death. bOS was censored at the earliest of i) HRR conversion date (negative to positive only), ii) end of clinical activity, or iii) end of data availability. |
OS rates among HRR positive and HRR negative patients were 74.5% and 76.7% at 12 months and 46.8% and 51.9% at 24 months, respectively. Stratified by race, OS rates among HRR positive and HRR negative White patients were 75.7% and 76.4% at 12 months and 48.6% and 46.2% at 24 months, respectively; and among HRR positive and HRR negative Black patients were 81.0% and 82.7% at 12 months and 52.8% and 54.1% at 24 months, respectively.
Time-to-PSA90 Response
The median time-to-PSA90 response was not reached in all cohorts. Overall, PSA90 response rates among HRR positive and HRR negative patients were 12.7% and 15.1% at 3 months, 19.5% and 25.6% at 6 months, and 24.3% and 37.9% at 12 months, respectively (Figure 7a). Among White HRR positive patients, PSA90 response rates were 12.1% at 3 months, 18.7% at 6 months, and 24.5% at 12 months, while PSA90 response rates were 13.6% at 3 months, 23.5% at 6 months, and 35.2% at 12 months for White HRR negative patients (Figure 7b). Among Black HRR positive patients, PSA90 response rates were 17.0% at 3, 6, and 12 months, while PSA90 response rates were 25.6% at 3 months, 37.6% at 6 months, and 43.9% at 12 months for Black HRR negative patients.
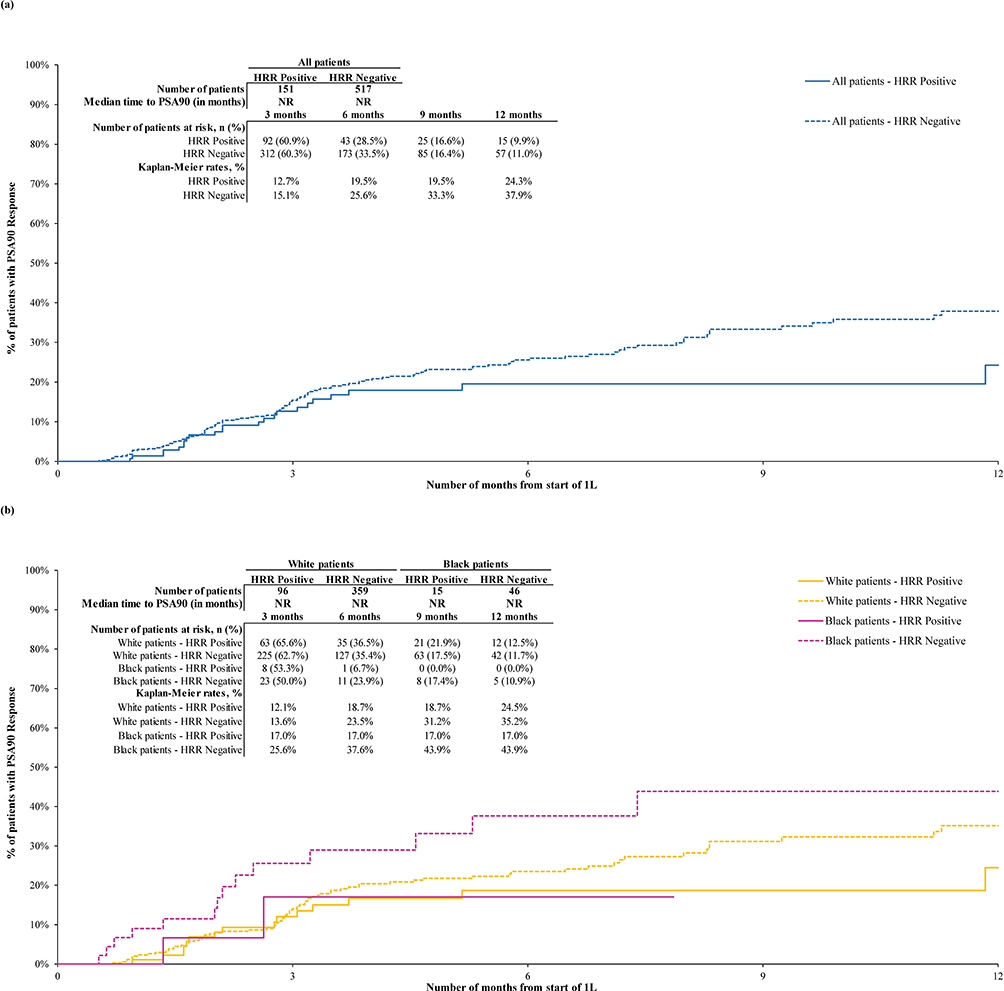 |
Figure 7 Time-to-PSA90 (a) among all patients in and (b) among White and Black patients in 1La,b. Abbreviations: 1L, first-line; 2L, second line; HRR, homologous recombination repair; NR, not reached; PSA, prostate-specific antigen. Notes: aTime-to-PSA90 was defined as the time from 1L start to the first observed decline ≥90% from the latest baseline value obtained no later than 13 weeks prior to or on the index date, evaluated among patients with a latest baseline PSA value obtained no later than 13 weeks prior to or on the index date. bTime-to-PSA90 was censored at the earliest of i) HRR conversion date (negative to positive only) or ii) 1L end date (ie, the earliest of the day before the start of 2L, end of clinical activity [including death], or end of data availability). |
Discussion
This retrospective EHR-based study found that between 2013 and 2022, less than 10% of the patients with mCRPC in the EHR-derived database received NGS HRR alteration testing prior to initiating 1L therapy. In the CGDB cohort, patients largely received ARSIs and taxane-based chemotherapy as 1L mCRPC therapy, likely due to the approval timing of PARP inhibitors for mCRPC in the year 2020 that had limited their availability during the current study period.39,40 Among those in the CGDB cohort, HRR positive patients tended to progress faster to the next treatment and have numerically shorter survival than HRR negative patients. The median OS of approximately 2 years is consistent with prior evidence in mCRPC in the pre-PARP inhibitor era,16,41 reflecting a need for therapeutic interventions that effectively delay progression and prolong survival. In addition, a numerically lower proportion of HRR positive than HRR negative patients achieved a PSA90 response, which may suggest a lack of treatment response or resistance to medications among HRR positive patients, as supported by their numerically shorter TTNT relative to HRR negative patients. Stratified results suggested that trends in poorer clinical outcomes among HRR positive patients were similarly observed in both races, with the differences by HRR alteration status being generally more evident among Black patients.
While NGS HRR alteration testing rates have increased since 2013, potentially due in part to advancement in testing techniques as well as increasing integration of genetic testing in treatment guidelines and insurance policies,4,27,42 they remain low. In 2022, only about 1 in 4 treated patients with mCRPC were tested for HRR alterations, and testing rates generally appeared lower among Black patients than White patients, despite observing a trend toward a higher mutational burden among Black patients in this study. With the expansion of clinical guideline recommendations that advocate for genetic testing in metastatic PC and the multiple precision therapies approved or in the pipeline,27 HRR alteration testing rates may further rise in the coming years. However, additional efforts are needed to address disparities in genetic testing among Black patients. The underlying causes of the disparities are multifactorial and may include lack of access to genetic counseling and education, healthcare system mistrust, and social determinants of health (eg, income, insurance status).43,44 Strategies to reduce racial disparities in genetic testing may help promote equitable and tailored genetic management for all patients with mCRPC.30
The observation of increasing HRR alteration testing rates over time is consistent with a prior US EHR-based study investigating real-world genetic testing patterns in patients with mCRPC, which reported increasing testing rates for all HRR alterations assessed (including ATM, BRCA1/2, CDK12, PALB2, and FANCA) from 2013 to 2018.45 However, in that study, 13% of the patients had a documented genetic test over the study period, which is higher than the 8.9% found in the EHR-derived database in the current study. The apparent discrepancy in testing rate is potentially because the current study focused on HRR alteration testing before 1L mCRPC therapy initiation, and the test must be performed using NGS panels, which were not requirements in the prior study.45
The HRR alteration positivity rate among patients in the CGDB was approximately 25%, which aligns with the prevalence range of germline/somatic HRR alterations in mCRPC reported in previous studies.46,47 It is worth noting that variability in tissue and plasma assays is expected in patients based on sample characteristics, tumor biology, and disease status.27 These variables may sometimes lead to false negative results, potentially contributing to the underestimation of HRR alteration positivity rates. For instance, evaluation of HRR alteration status via circulating tumor DNA in blood can result in a false negative finding if tumor DNA content in blood is below the assay’s detection level,48 and detection of large structural alterations such as homozygous deletions is challenging with plasma assays.49 Tumor tissue testing may also be susceptible to false negative results, as tumor tissue is heterogeneous and different tumor cells within the same tumor, or between metastatic lesions, may show distinct genetic alterations.14 In addition, archival tumor tissue samples are often used when patients develop metastasis as metastatic samples may be inaccessible, particularly for metastasis in bone, which is the most common metastatic site in mCRPC. The quantity and/or quality of archival tumor tissues may lead to invalid test results.46 Therefore, repeated testing may be of value in clinical practice.27 In this study, 13.7% of the retested patients had a subsequent positive test for any HRR alteration after an initial negative test, underscoring the potential value of retesting. It should nonetheless be noted that whether this observation is due to an inadequate initial test or the acquisition of a new somatic alteration cannot be determined.
The current descriptive findings on TTNT, OS, and PSA90 response reflect poorer clinical outcomes among HRR positive patients relative to HRR negative patients with mCRPC. Given the observed differences by HRR alteration status, genetic testing may be useful in identifying patients who may benefit from more targeted approaches to mCRPC treatment. Of note, due to the timing of the current study, most of the patients had received ARSIs and taxane-based chemotherapy for mCRPC. In this context, findings from existing studies on the impact of HRR alterations on clinical outcomes of patients with mCRPC treated with these therapies are conflicting.50–54 It has been suggested that the treatment type and treatment sequence received may have interacted with HRR alteration status and contributed to the discordant findings,55 a phenomenon that warrants further examinations. Importantly, with the introduction of PARP inhibitors to the mCRPC armamentarium in recent years,14 future real-world studies should assess potential differences in clinical outcomes of patients with mCRPC treated with precision therapies in routine clinical practice to provide further insight on the value of genetic testing in delivering personalized care in mCRPC.
Findings of this study should be interpreted considering certain limitations. First, EHR-derived databases may contain inaccuracies or omissions (eg, diagnosis dates, treatment start dates, etc.), although these are expected to be random and impact all patients equally. Second, diagnoses or medical services obtained outside the Flatiron Health network were not captured; additionally, patients selected from the EHR-derived database may not be representative of the entire population of patients with mCRPC in the US, or in non-US settings, which may limit the generalizability of the study. Furthermore, all patients included in the CGDB have sought genetic testing; these patients may be more attentive to their health or have better access to healthcare relative to the general population, which may further impact the generalizability of the study. Third, HRR alteration testing is subject to errors during blood/tissue sampling and laboratory procedures, which may potentially affect the observed positivity rates and testing patterns. Fourth, ADT was not considered in the definition of a LOT and therefore patients who only used ADT in monotherapy after diagnosis of mCRPC were excluded. Fifth, differential censoring could be possible given that patients censored at the time of HRR status switch (ie, change in HRR alteration status from negative to positive) may have different disease profile and clinical outcomes compared to those who maintained a constant HRR status and remained in the study. Sixth, the time-to-PSA response may be subject to measurement error, which may be differential if the prescribing physician’s behavior led to more frequent PSA testing, depending on the choice of patient’s treatment regimen. Seventh, the sequence of treatment received by patients, which was not factored in this study, could influence the incidence of somatic alterations and confound the treatment responses assessed. Lastly, this was a descriptive study with no formal comparisons, significance testing, or adjustments for confounders performed; any differences between cohorts cannot be interpreted as statistically significant.
Conclusions
While NGS HRR alteration testing rates in the US increased from 0.0% in 2013 to 26.7% in 2022, rates remained relatively low with only about 1 in 4 treated patients with mCRPC being tested for HRR alterations in 2022, years after integration of genetic testing into clinical guideline recommendations. Relative to HRR negative patients, those who tested positive for HRR alterations tended to have faster progression from 1L to 2L treatment, shorter survival, and reduced PSA90 response, suggesting a greater unmet treatment need for these patients. In the context of newer precision therapies targeting HRR alteration(s), this study highlights the potential value of genetic testing for patients with mCRPC, particularly for Black patients, who have been underrepresented, and who may have a higher burden of HRR alterations. Observations here further emphasize the increased need for testing and additional precision therapies for earlier use in mCRPC.
Abbreviations
1L, first-line; ADT, androgen deprivation therapy; ARSI, androgen receptor signaling inhibitor; CGDB, Clinico-Genomic Database; CRPC, castration-resistant prostate cancer; EHR, electronic health record; FMI, Foundation Medicine, Inc.; HIPAA, Health Insurance Portability and Accountability Act; HRR, homologous recombination repair; LOT, line of therapy; mCRPC, metastatic castration-resistant prostate cancer; NGS, next-generation sequencing; OS, overall survival; PARP, poly ADP-ribose polymerase; PC, prostate cancer; PSA, prostate-specific antigen; TTNT, time-to-next-treatment; US, United States.
Data Sharing Statement
The data that support the findings of this study have been originated by Flatiron Health, Inc. and Foundation Medicine, Inc. Requests for data sharing by license or by permission for the specific purpose of replicating results in this manuscript can be submitted to [email protected] and [email protected].
Ethical Conduct of Research Statement
The authors declared that the research was conducted according to the principles of the Declaration of Helsinki.
Acknowledgments
Part of the material in this manuscript was presented at the Society of Urologic Oncology 23rd Annual Meeting from November 30-December 2, 2022 in San Diego, CA, USA, the International Prostate Cancer Update from January 22-25, 2023 in Vail, CO, USA; and the ASCO Genitourinary Cancers Symposium from February 16-18, 2023 in San Francisco, CA, USA. Medical writing assistance was provided by Flora Chik, PhD, MWC, an employee of Analysis Group, Inc. and was funded by Janssen Scientific Affairs, LLC.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Janssen Scientific Affairs, LLC.
Disclosure
Mehmet A. Bilen is a professor at Emory University School of Medicine and has acted as a paid consultant for and/or as a member of the advisory boards of Exelixis, Bayer, BMS, Eisai, Pfizer, AstraZeneca, Janssen, Calithera Biosciences, Genomic Health, Nektar, EMD Serono, SeaGen, and Sanofi; and has received grants to his institution from Merck, Xencor, Bayer, Bristol-Myers Squibb, Genentech/Roche, SeaGen, Incyte, Nektar, AstraZeneca, Tricon Pharmaceuticals, Genome & Company, AAA, Peloton Therapeutics, and Pfizer for work performed as outside of the current study. Ibrahim Khilfeh is an employee of Janssen Scientific Affairs, LLC and stockholder of Johnson & Johnson. Erik Muser was an employee of Janssen Scientific Affairs, LLC at the time the study was conducted. Carmine Rossi, Laura Morrison, Annalise Hilts, Lilian Diaz, Patrick Lefebvre, and Dominic Pilon are employees of Analysis Group, Inc., a consulting company that has provided paid consulting services to Janssen Scientific Affairs, LLC, which funded the development and conduct of this study and manuscript. Daniel J. George is a professor at Duke University School of Medicine and reports the following in the past 24 months: has acted in leadership role for Capio Biosciences; has acted as a paid consultant for and/or as a member of the advisory boards of Ambrx, AVEO, Corvus, Eisai, IdeOnocology, Medscape Educ., Nektar, Seattle Genetics, Sumitovant Biopharma, Surface Oncology, UroGPO, WebMD, Bayer, Exelixis, Pfizer, Sanofi, Astellas Pharma, Innocrin Pharma, Bristol Myers Squibb, Genentech, Janssen, Merck Sharp & Dohme, Myovant Sciences, AstraZeneca, Michael J. Hennessy Associates, Constellation Pharmaceuticals, Physicians’ Education Resource, Propella Therapeutics, RevHealth, and xCures; has been a member of the speakers’ bureau of Sanofi, Bayer, and Exelixis; has received honoraria from Sanofi, Bayer, Exelixis, EMD Serono, OncLive, Pfizer, UroToday, Acceleron Pharma, American Association for Cancer Research, Axess Oncology, Janssen Oncology, and Millennium Medical Publishing; has received research funding from Exelixis, Janssen Oncology, Novartis, Pfizer, Astellas Pharma, Bristol Myers Squibb, Acerta Pharma, Bayer, Dendreon, Innocrin Pharma, Calithera Biosciences, and Sanofi/Aventis; and has received other research support (travel, accommodations, expenses) from Bayer, Exelixis, Merck, Pfizer, Sanofi, Janssen Oncology, and UroToday.
References
1. American Cancer Society. Key Statistics for Prostate Cancer. 2023, Available from: https://www.cancer.org/cancer/prostate-cancer/about/key-statistics.html.
2. National Cancer Institute, Surveillance Epidemiology and End Results. Cancer Stat Facts: Prostate Cancer. 2023, https://seer.cancer.gov/statfacts/html/prost.html.
3. Lowrance WT, Breau RH, Chou R, et al. Advanced prostate cancer: AUA/ASTRO/SUO Guideline PART I. J Urol. 2021;205(1):14–21. doi:10.1097/JU.0000000000001375
4. Lowrance WT, Breau RH, Chou R, et al. Advanced prostate cancer: AUA/ASTRO/SUO Guideline PART II. J Urol. 2021;205(1):22–29. doi:10.1097/JU.0000000000001376
5. Shafi AA, Yen AE, Weigel NL. Androgen receptors in hormone-dependent and castration-resistant prostate cancer. Pharmacol Ther. 2013;140(3):223–238. doi:10.1016/j.pharmthera.2013.07.003
6. Karantanos T, Corn PG, Thompson TC. Prostate cancer progression after androgen deprivation therapy: mechanisms of castrate resistance and novel therapeutic approaches. Oncogene. 2013;32(49):5501–5511. doi:10.1038/onc.2013.206
7. Smith MR, Saad F, Chowdhury S, et al. Apalutamide treatment and metastasis-free survival in prostate cancer. N Engl J Med. 2018;378(15):1408–1418. doi:10.1056/NEJMoa1715546
8. Chi KN, Agarwal N, Bjartell A, et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N Engl J Med. 2019;381(1):13–24. doi:10.1056/NEJMoa1903307
9. Moreira DM, Howard LE, Sourbeer KN, et al. Predictors of time to metastasis in castration-resistant prostate cancer. Urology. 2016;96:171–176. doi:10.1016/j.urology.2016.06.011
10. Kantoff PW, Higano CS, Shore ND, et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med. 2010;363(5):411–422. doi:10.1056/NEJMoa1001294
11. Ryan CJ, Smith MR, Fizazi K, et al. Abiraterone acetate plus prednisone versus placebo plus prednisone in chemotherapy-naive men with metastatic castration-resistant prostate cancer (COU-AA-302): final overall survival analysis of a randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol. 2015;16(2):152–160. doi:10.1016/S1470-2045(14)71205-7
12. Scher HI, Fizazi K, Saad F, et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med. 2012;367(13):1187–1197. doi:10.1056/NEJMoa1207506
13. Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004;351(15):1502–1512. doi:10.1056/NEJMoa040720
14. Congregado B, Rivero I, Osman I, Saez C, Medina Lopez R. PARP inhibitors: a new horizon for patients with prostate cancer. Biomedicines. 2022;10(6):1416. doi:10.3390/biomedicines10061416
15. Sanli Y, Simsek DH, Sanli O, Subramaniam RM, Kendi AT. (177)Lu-PSMA therapy in metastatic castration-resistant prostate cancer. Biomedicines. 2021;9(4):430. doi:10.3390/biomedicines9040430
16. Shore ND, Laliberte F, Ionescu-Ittu R, et al. Real-world treatment patterns and overall survival of patients with metastatic castration-resistant prostate cancer in the US prior to PARP Inhibitors. Adv Ther. 2021;38(8):4520–4540. doi:10.1007/s12325-021-01823-6
17. Huang X, Chau CH, Figg WD. Challenges to improved therapeutics for metastatic castrate resistant prostate cancer: from recent successes and failures. J Hematol Oncol. 2012;5(1):35. doi:10.1186/1756-8722-5-35
18. Schweizer MT, Antonarakis ES. Prognostic and therapeutic implications of DNA repair gene mutations in advanced prostate cancer. Clin Adv Hematol Oncol. 2017;15(10):785–795.
19. Leongamornlert D, Saunders E, Dadaev T, et al. Frequent germline deleterious mutations in DNA repair genes in familial prostate cancer cases are associated with advanced disease. Br J Cancer. 2014;110(6):1663–1672. doi:10.1038/bjc.2014.30
20. Pritchard CC, Mateo J, Walsh MF, et al. Inherited DNA-repair gene mutations in men with metastatic prostate cancer. N Engl J Med. 2016;375(5):443–453. doi:10.1056/NEJMoa1603144
21. Castro E, Goh C, Leongamornlert D, et al. Effect of BRCA mutations on metastatic relapse and cause-specific survival after radical treatment for localised prostate cancer. Eur Urol. 2015;68(2):186–193. doi:10.1016/j.eururo.2014.10.022
22. Chi KN, Rathkopf D, Smith MR, et al. Niraparib and Abiraterone acetate for metastatic castration-resistant prostate cancer. J Clin Oncol. 2023;41(18):3339–3351. doi:10.1200/JCO.22.01649
23. de Bono J, Mateo J, Fizazi K, et al. Olaparib for metastatic castration-resistant prostate cancer. N Engl J Med. 2020;382(22):2091–2102. doi:10.1056/NEJMoa1911440
24. Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): a randomised, placebo-controlled, phase 3 trial. Lancet. 2023;402(10398):291–303. doi:10.1016/S0140-6736(23)01055-3
25. Clarke NW, Armstrong AJ, Thiery-Vuillemin A, et al. Abiraterone and olaparib for metastatic castration-resistant prostate cancer. NEJM Evidence. 2022;1(9). doi:10.1056/EVIDoa2200043
26. Abida W, Patnaik A, Campbell D, et al. Rucaparib in men with metastatic castration-resistant prostate cancer harboring a BRCA1 or BRCA2 gene alteration. J Clin Oncol. 2020;38(32):3763–3772. doi:10.1200/JCO.20.01035
27. Giri VN, Morgan TM, Morris DS, Berchuck JE, Hyatt C, Taplin ME. Genetic testing in prostate cancer management: considerations informing primary care. CA Cancer J Clin. 2022;72(4):360–371. doi:10.3322/caac.21720
28. Benafif S, Kote-Jarai Z, Eeles RA, Consortium P. A review of prostate cancer genome-wide association studies (GWAS). Cancer Epidemiol Biomarkers Prev. 2018;27(8):845–857. doi:10.1158/1055-9965.EPI-16-1046
29. Trendowski MR, Sample C, Baird T, et al. Germline variants in DNA damage repair genes and HOXB13 among black patients with early-onset prostate cancer. JCO Precis Oncol. 2022;6(6):e2200460. doi:10.1200/PO.22.00460
30. Giri VN, Hartman R, Pritzlaff M, Horton C, Keith SW. Germline variant spectrum among African American men undergoing prostate cancer germline testing: need for equity in genetic testing. JCO Precis Oncol. 2022;6(6):e2200234. doi:10.1200/PO.22.00234
31. Ma X, Long L, Moon S, Adamson BJS, Baxi SS. Comparison of population characteristics in real-world clinical oncology databases in the US: Flatiron Health, SEER, and NPCR. medRxiv. 2020;20037143. doi:10.1101/2020.03.16.20037143
32. Birnbaum B, Nussbaum N, Seidl-Rathkopf K, et al. Model-assisted cohort selection with bias analysis for generating large-scale cohorts from the EHR for oncology research. arXiv preprint. 2020;2020:1. doi:10.48550/arXiv.2001.09765
33. Singal G, Miller PG, Agarwala V, et al. Association of patient characteristics and tumor genomics with clinical outcomes among patients with non-small cell lung cancer using a clinicogenomic database. JAMA. 2019;321(14):1391–1399. doi:10.1001/jama.2019.3241
34. Agarwala V, Khozin S, Singal G, et al. Real-world evidence in support of precision medicine: clinico-genomic cancer data as a case study. Health Aff (Millwood). 2018;37(5):765–772. doi:10.1377/hlthaff.2017.1579
35. Hess LM, Han Y, Zhu YE, Bhandari NR, Sireci A. Characteristics and outcomes of patients with RET-fusion positive non-small lung cancer in real-world practice in the United States. BMC Cancer. 2021;21(1):28. doi:10.1186/s12885-020-07714-3
36. Woodhouse R, Li M, Hughes J, et al. Clinical and analytical validation of FoundationOne Liquid CDx, a novel 324-gene cfDNA-based comprehensive genomic profiling assay for cancers of solid tumor origin. PLoS One. 2020;15(9):e0237802. doi:10.1371/journal.pone.0237802
37. Walker MS, Herms L, Miller P. Performance of time to discontinuation and time to next treatment as proxy measures of progression-free survival, overall and by treatment group. J Clin Oncol. 2020;38(15 (Supplement):e19135. doi:10.1200/JCO.2020.38.15_suppl.e19135
38. Saad F, Small EJ, Feng FY, et al. Deep prostate-specific antigen response following addition of apalutamide to ongoing androgen deprivation therapy and long-term clinical benefit in SPARTAN. Eur Urol. 2022;81(2):184–192. doi:10.1016/j.eururo.2021.11.020
39. U.S. Food and Drug Administration (FDA). FDA approves olaparib for HRR gene-mutated metastatic castration-resistant prostate cancer. 2020, Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-olaparib-hrr-gene-mutated-metastatic-castration-resistant-prostate-cancer.
40. U.S. Food and Drug Administration (FDA). FDA grants accelerated approval to rucaparib for BRCA-mutated metastatic castration-resistant prostate cancer. 2020, Available from:https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-olaparib-hrr-gene-mutated-metastatic-castration-resistant-prostate-cancer.
41. Freedland SJ, Davis M, Epstein AJ, Arondekar B, Ivanova JI. Overall survival by race and ethnicity among men with metastatic castration-resistant prostate cancer (mCRPC) in the U.S. Medicare population. Journal of Clinical Oncology. 2022;40(28_suppl):144. doi:10.1200/JCO.2022.40.28_suppl.144
42. Szymaniak BM, Facchini LA, Giri VN, et al. Practical considerations and challenges for germline genetic testing in patients with prostate cancer: recommendations from the germline genetics working group of the PCCTC. JCO Oncol Pract. 2020;16(12):811–819. doi:10.1200/OP.20.00431
43. Rogers CR, Rovito MJ, Hussein M, et al. Attitudes toward genomic testing and prostate cancer research among black men. Am J Prev Med. 2018;55(5 Suppl 1):S103–S111. doi:10.1016/j.amepre.2018.05.028
44. Weise N, Shaya J, Javier-Desloges J, Cheng HH, Madlensky L, McKay RR. Disparities in germline testing among racial minorities with prostate cancer. Prostate Cancer Prostatic Dis. 2022;25(3):403–410. doi:10.1038/s41391-021-00469-3
45. Shore N, Ionescu-Ittu R, Yang L, et al. Real-world genetic testing patterns in metastatic castration-resistant prostate cancer. Future Oncol. 2021;17(22):2907–2921. doi:10.2217/fon-2021-0153
46. Scott RJ, Mehta A, Macedo GS, Borisov PS, Kanesvaran R, El Metnawy W. Genetic testing for homologous recombination repair (HRR) in metastatic castration-resistant prostate cancer (mCRPC): challenges and solutions. Oncotarget. 2021;12(16):1600–1614. doi:10.18632/oncotarget.28015
47. Lang SH, Swift SL, White H, Misso K, Kleijnen J, Quek RGW. A systematic review of the prevalence of DNA damage response gene mutations in prostate cancer. Int J Oncol. 2019;55(3):597–616. doi:10.3892/ijo.2019.4842
48. Stejskal P, Goodarzi H, Srovnal J, Hajduch M, van ‘t Veer LJ, Magbanua MJM. Circulating tumor nucleic acids: biology, release mechanisms, and clinical relevance. Mol Cancer. 2023;22(1):15. doi:10.1186/s12943-022-01710-w
49. Chi KN, Barnicle A, Sibilla C, et al. Detection of BRCA1, BRCA2, and ATM alterations in matched tumor tissue and circulating tumor DNA in patients with prostate cancer screened in PROfound. Clin Cancer Res. 2023;29(1):81–91. doi:10.1158/1078-0432.CCR-22-0931
50. Annala M, Struss WJ, Warner EW, et al. Treatment outcomes and tumor loss of heterozygosity in germline DNA repair-deficient prostate cancer. Eur Urol. 2017;72(1):34–42. doi:10.1016/j.eururo.2017.02.023
51. Antonarakis ES, Lu C, Luber B, et al. Germline DNA-repair gene mutations and outcomes in men with metastatic castration-resistant prostate cancer receiving first-line abiraterone and enzalutamide. Eur Urol. 2018;74(2):218–225. doi:10.1016/j.eururo.2018.01.035
52. Carlson AS, Acevedo RI, Lim DM, et al. Impact of mutations in homologous recombination repair genes on treatment outcomes for metastatic castration resistant prostate cancer. PLoS One. 2020;15(9):e0239686. doi:10.1371/journal.pone.0239686
53. Gallagher DJ, Cronin AM, Milowsky MI, et al. Germline BRCA mutation does not prevent response to taxane-based therapy for the treatment of castration-resistant prostate cancer. BJU Int. 2012;109(5):713–719. doi:10.1111/j.1464-410X.2011.10292.x
54. Mateo J, Cheng HH, Beltran H, et al. Clinical outcome of prostate cancer patients with germline DNA repair mutations: retrospective analysis from an international study. Eur Urol. 2018;73(5):687–693. doi:10.1016/j.eururo.2018.01.010
55. Castro E, Romero-Laorden N, Del Pozo A, et al. PROREPAIR-B: a prospective cohort study of the impact of germline DNA repair mutations on the outcomes of patients with metastatic castration-resistant prostate cancer. J Clin Oncol. 2019;37(6):490–503. doi:10.1200/JCO.18.00358
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.