Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Home Phototherapy Improves Access to Dermatologic Care: A Novel Stakeholder Alliance to Facilitate Its Implementation
Authors Bawany F, Ryan Wolff J, Ritchlin CT, Tausk F ![]()
Received 1 March 2023
Accepted for publication 27 April 2023
Published 2 May 2023 Volume 2023:16 Pages 1175—1180
DOI https://doi.org/10.2147/CCID.S408323
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Fatima Bawany,1 Julie Ryan Wolff,1 Christopher T Ritchlin,2 Francisco Tausk1,2
1Department of Dermatology, University of Rochester Medical Center, Rochester, NY, USA; 2Department of Medicine, University of Rochester Medical Center, Rochester, NY, USA
Correspondence: Francisco Tausk, Department of Dermatology, University of Rochester Medical Center, 601 Elmwood Ave., Box 697, Rochester, NY, 14642, USA, Email [email protected]
Introduction
Phototherapy is a standard treatment for dermatologic diseases such as psoriasis in patients with moderate to severe disease. Compared with alternative systemic therapies such as biologics, it has fewer side effects and costs, with comparable efficacy.1 However, it often requires in-office treatments two to three times a week, resulting in a substantial patient burden, such as the inability to attend during office hours, lengthy travel times to the medical office, and a significant financial burden resulting from the high cost of treatment co-pays, that in the case of most commercial insurers, is equal to that of a physician specialist visit.
Home phototherapy can reduce many barriers to care. This study determined disease, quality-of-life, and treatment satisfaction outcomes from a home phototherapy program at our academic center involving all stakeholders’ alliance (insurance carrier, instrument manufacturer, health providers, and hospital pharmacy).
Methods
We developed a home phototherapy program in conjunction with a major insurance carrier, the device manufacturer (Daavlin, Bryan, Ohio), and the hospital pharmacy.
Home Phototherapy Methods
- Patients are seen at the dermatology clinic of the University of Rochester Medical Center, and the healthcare provider makes the determination to consider phototherapy based on the clinical assessment and disease characteristics.
- Initial presentation of this procedure to the subject, and if in agreement to proceed, we educate the patient on benefits, goals, and expectations of this treatment, including expected time to improvement. We review possible side effects, such as burns, the need to reduce doses if they develop pinkness in the skin, and the instructions to contact us in case of adverse effects. If the face is not affected, they are instructed to place a pillowcase over it, always in the same position. If the face is to be exposed, we stress the requirement to wear goggles provided by the pharmacy. Time is allotted for any patient questions.
- Following the education session, patients sign a consent form with detailed instructions and information that can be reviewed at home.
- We then determine the phototherapy unit to be ordered. Either a 6-foot stand-up unit for the entire body (Series 7) or a flat panel (Series 1) for hands/feet treatment. The electronic order is placed to the pharmacy after determining the ideal starting dose based on Fitzpatrick skin type ranging from 125 mJ/cm2 for skin type I to 400 mJ/cm2 for skin type VI, conveying this to the pharmacy and instructing an escalating dose of 10% each session (2 or 3 sessions per week and never two consecutive days).
- Dedicated pharmacy personnel educated on phototherapy contact the insurance carrier and delivers and install the phototherapy unit in the patient’s home. The insurer charges a 0–20% one-time copay and the total cost is markedly reduced due to bulk-purchasing by the pharmacy.
- Upon delivery, the pharmacist reviews the operating instructions, dosing, and side effects with the patient. The subject is provided with an app (Daavlin) to calculate escalating doses and a document to log in every treatment and possible adverse effects. Patients are provided protection goggles, and males are given straps to cover their genitals.
- Two days later, the pharmacist contacts the patient via telephone to review any problems, and this is repeated two weeks later and subsequently monthly.
- The patients are scheduled to follow up with their dermatologist three months after initiating the home phototherapy.
Study Methods
In this cross-sectional cohort study (01/2019–02/2021, IRB approved 10/12/2020), patients were eligible if they met the following criteria: >18 years old, prescribed home phototherapy for a dermatologic disease, and able to give informed consent in English (telephone questionnaire only). This study complies with the declaration of Helsinki.
Demographics and disease courses were determined using medical records. A 12-question telephone survey ascertained device use, Perceived Global Impression of Severity,2 quality-of-life (Skindex-mini),3 and treatment satisfaction. Subgroup analyses were performed using Chi-square tests and Fisher’s exact tests for categorical data and unpaired t-tests for continuous data.
Results
Table 1 summarizes patient demographics. The most common diseases were psoriasis and AD. Almost all patients (96.8%, n=61) received narrow-band ultraviolet B phototherapy. The survey response rate was 68% (n=43), and the sample was representative of the population.
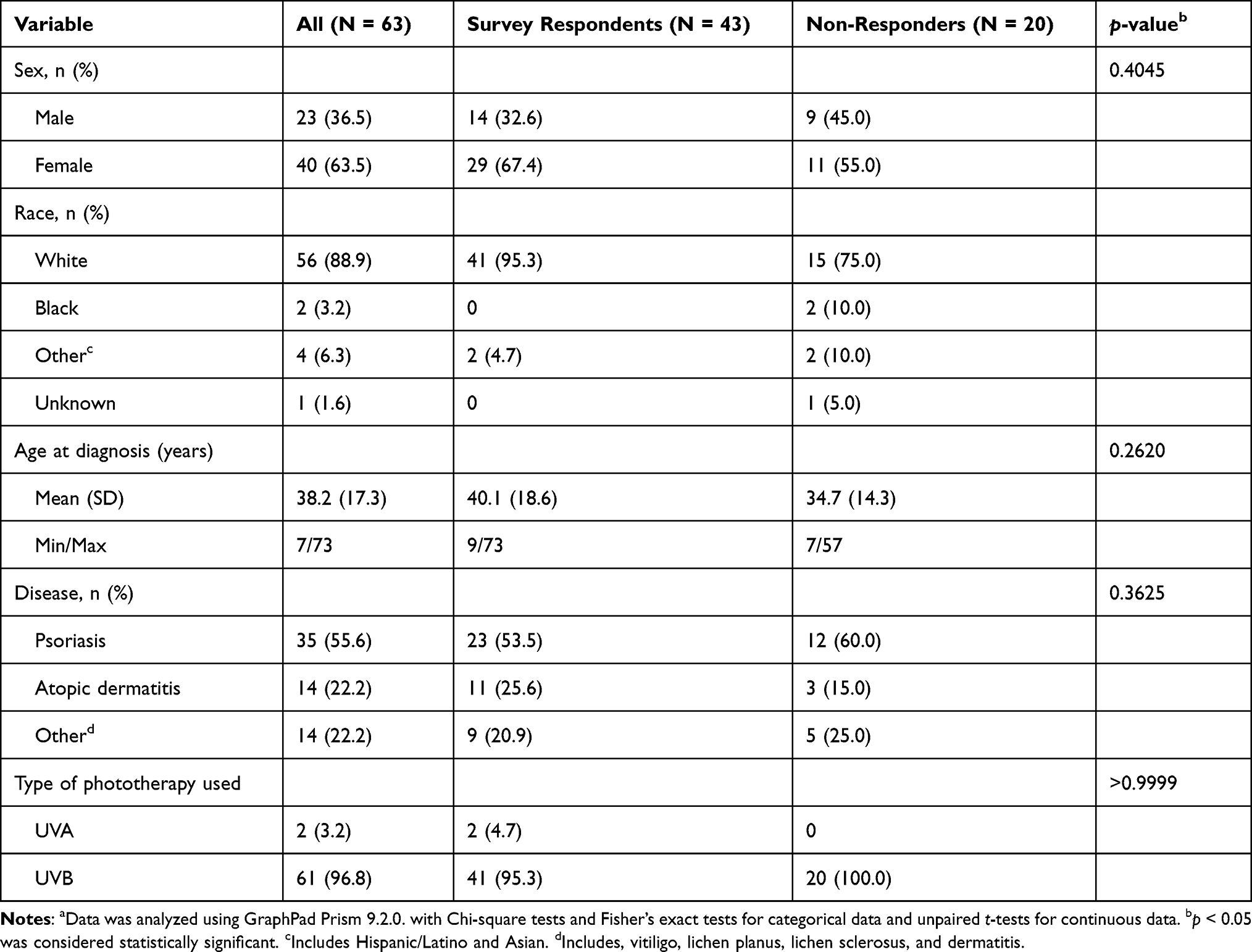 |
Table 1 Demographics and Clinical Features of Study Cohorta |
Table 2 describes the clinical features and questionnaire responses of the survey sample. Nearly 90% of patients endorsed improvement with phototherapy. Sixteen patients (37.2%) had used their device for >1 year. Five patients (11.6%) had not improved despite phototherapy (psoriasis n=2, AD n=2, lichen sclerosus n=1). Of them, only the patient with lichen sclerosus had used the device for >1 year. Of the remaining four patients, two experienced difficulties using the device, and one experienced side effects (n=1).
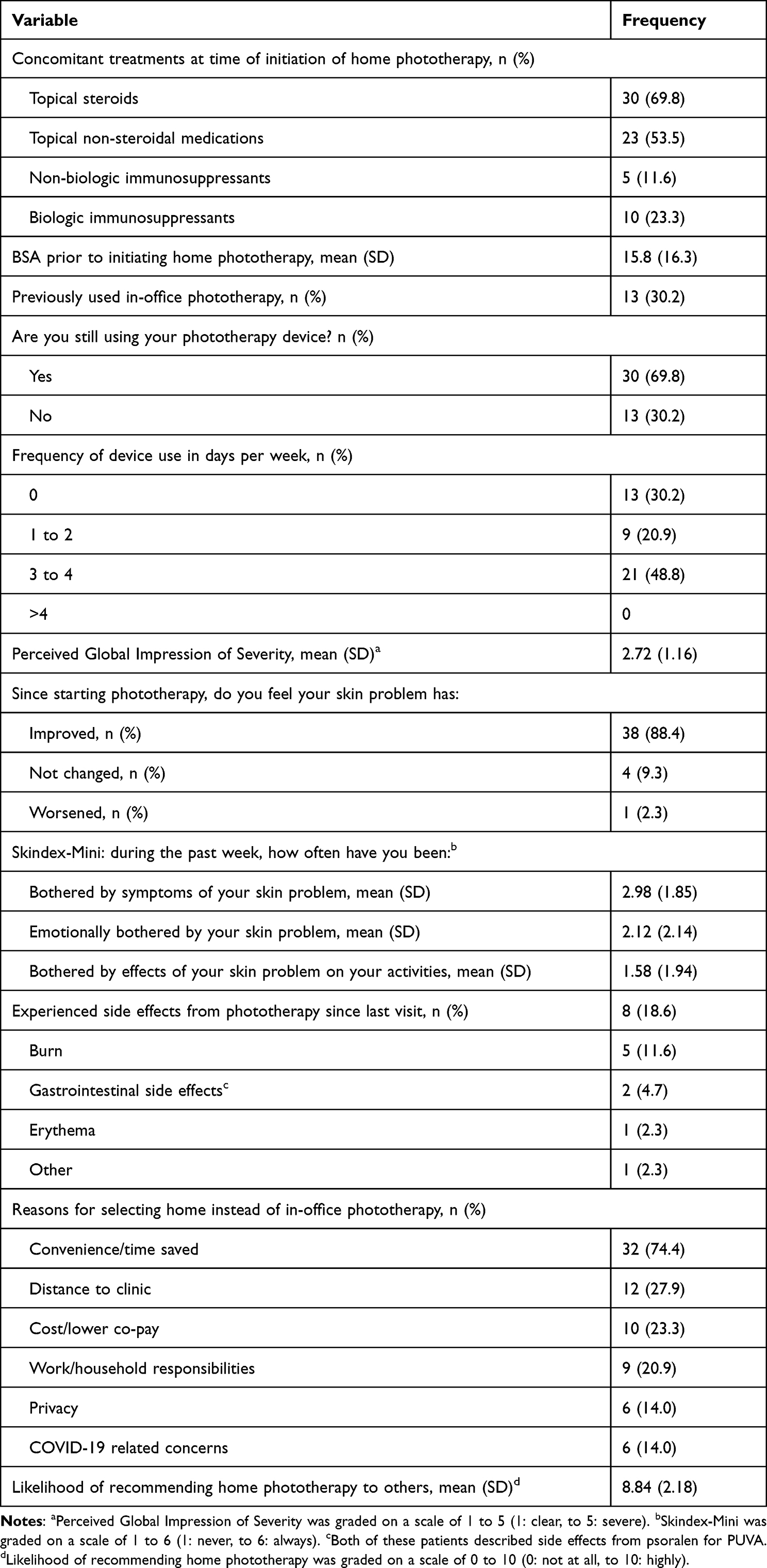 |
Table 2 Disease Course and Experiences of Survey Respondents (N = 43) |
All subjects preferred home treatment to in-office treatment due to the reduced time, travel, and financial burden. Most patients preferred home phototherapy to biologics (74.4%, n=32), primarily due to concerns about biologic side effects (40.6%, n=13). Those who were undecided perceived both treatments as efficacious (100%, n=10).
A minority of patients endorsed difficulties using the device (13.9%, n=6) or side effects (18.6%, n=8). Thirteen patients (30.2%) were no longer using their device; common reasons for discontinuation were disease clearance (n=4), treatment dissatisfaction (n=3), difficulties using the device (n=2), and inability to adhere to the regimen (n=2).
Discussion
Our data reaffirms that home phototherapy is efficacious and reduces patient burden.4 Our compliance and clinic follow-up rates were reassuring. However, several patients reported side effects or difficulties using their devices despite in-person and telephone follow-ups, suggesting that improvements can be made in monitoring. Study limitations were the relatively small sample size, retrospective design, and racially homogenous population.
In-office phototherapy can be burdensome to patients and staff due to the numerous appointments, transportation, co-pays, staffing, and equipment.5 However, home units often have limited or complex insurance coverage. In one study, less than half of patients filled their prescriptions for home phototherapy due to high out-of-pocket costs.6 In our program, the expense to the insurer was the device cost. In contrast, the cost of biologic medications is approximately $60,000–$70,000/year (data.medicaid.gov). This, along with the possible side effects of biologics, yields a strong argument for expanding home phototherapy services in lieu of or prior to trialing biologics. A study performed in 20187 reported that the 3-year cost of biologics at that time ranged between $109,066 and $180,718; newer ones, such as risankizumab, carry a wholesale acquisition cost of $236,815 (https://www.skyrizi.com/psoriasis-psoriatic-arthritis/cost-and-savings), compared to a 3-year cost of home phototherapy between $700 and $2400. Paradoxically, most insurance carriers systematically reject home phototherapy, favoring the utilization of biologics in spite of the fact that home phototherapy would result in substantial savings.
Conclusion
We have developed a home phototherapy program that is effective, safe, and economical for insurers and patients, and believe that this successful program should be replicated by other medical institutions and encourage insurance carriers to include home phototherapy in their covered plans. A large-scale, pragmatic, longitudinal study is currently being funded by PCORI comparing patient outcomes between home phototherapy and in-office phototherapy (https://www.pcori.org/research-results/2017/comparing-home-versus-clinic-based-phototherapy-treatment-psoriasis-lite-study).
Ethics and Consent
Informed consent was obtained from all patients who participated in the questionnaire.
This study was approved by the University of Rochester Medical Center IRB.
Acknowledgment
The abstract of this paper was presented at the 2022 Annual Meeting of the American Academy of Dermatology as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in the J Am Acad Dermatol, 2022, Vol 87(3), pAB65
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Almutawa F, Alnomair N, Wang Y, Hamzavi I, Lim HW. Systematic review of UV-based therapy for psoriasis. Am J Clin Dermatol. 2013;14(2):87–109. doi:10.1007/s40257-013-0015-y
2. Newton L, DeLozier AM, Griffiths PC, et al. Exploring content and psychometric validity of newly developed assessment tools for itch and skin pain in atopic dermatitis. J Patient Rep Outcomes. 2019;3(1):42. doi:10.1186/s41687-019-0128-z
3. Swerlick RA, Zhang C, Patel A, Chren MM, Chen S. The Skindex-Mini: a streamlined quality of life measurement tool suitable for routine use in clinic. J Am Acad Dermatol. 2021;85(2):510–512. doi:10.1016/j.jaad.2018.12.035
4. Koek MB, Buskens E, van Weelden H, Steegmans PH, Bruijnzeel-Koomen CA, Sigurdsson V. Home versus outpatient ultraviolet B phototherapy for mild to severe psoriasis: pragmatic multicentre randomised controlled non-inferiority trial (Pluto study). BMJ. 2009;338:b1542. doi:10.1136/bmj.b1542
5. Click J, Alabaster A, Postlethwaite D, Lide W. Effect of availability of at-home phototherapy on the use of systemic medications for psoriasis. Photodermatol Photoimmunol Photomed. 2017;33(6):345–346. doi:10.1111/phpp.12349
6. Yentzer BA, Feldman SR. Trends in home phototherapy adoption in the US: monetary disincentives are only the tip of the iceberg. J Dermatolog Treat. 2011;22(1):27–30. doi:10.3109/09546630903440080
7. Hyde K, Cardwell L, Stotts R, Feldman SR. Psoriasis treatment cost comparison: biologics versus home phototherapy. Am J Pharm Benefits. 2018;10(1):18–21.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psoriasis on Lesions of Vitiligo: A Case Report
Wang L, Zhang B
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2005-2007
Published Date: 4 August 2023
Development of Predictive Models for NB-UVB Treatment Efficacy and Safety in Psoriasis
Yu Y, Li B, Wang Y, Qu Z, Wang X, Jiang Y, Zhong X, Chen Y, Huang D, Bi X, Lu J, Ding Y, Gong Y, Gu J, Zhang X, Shi Y
Psoriasis: Targets and Therapy 2026, 16:609637
Published Date: 25 May 2026