Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
HIV Testing Uptake Among Ethiopian Rural Men: Evidence from 2016 Ethiopian Demography and Health Survey Data
Authors Asresie MB ![]() , Worku GT, Bekele YA
, Worku GT, Bekele YA
Received 6 March 2023
Accepted for publication 29 April 2023
Published 3 May 2023 Volume 2023:15 Pages 225—234
DOI https://doi.org/10.2147/HIV.S409152
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Melash Belachew Asresie,1,* Getasew Tadesse Worku,2,* Yibeltal Alemu Bekele1,*
1Department of Reproductive Health and Population Studies, School of Public Health, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia; 2Department of Health Economics and Health Service Management, School of Public Health, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia
*These authors contributed equally to this work
Correspondence: Melash Belachew Asresie, P.box:79, Tel +251920774471, Email [email protected]
Background: Human immunodeficiency virus (HIV) testing coverage among men remains low in Ethiopia; the problem of limited HIV testing coverage is worst in rural areas. Therefore, this study aims to identify factors associated with HIV testing uptake among rural men in Ethiopia.
Methods: Data from 10,187 rural men was extracted from the 2016 Ethiopian Demography and Health Survey. All analyses were performed using the complex sample analysis procedure to account for the multistage sampling. Bivariable and multivariable regression analyses were performed to identify factors associated with HIV testing uptake. Statistical significance was defined as a 95% Confidence Interval (CI) with a p-value of less than 0.05.
Results: Overall, only 40.3% of rural men have ever been tested for HIV. Being aged 31– 44 years (Adjusted Odds Ratio (AOR) =1.12, 95% CI [1.01– 1.42]), living in developed regions (AOR=1.43, 95% CI [1.09– 1.88]), engaging in non-agricultural activities (AOR = 1.27, 95% CI [1.05– 1.52]), being Muslim (AOR = 2.07; 95% CI [1.67– 2.67]), having comprehensive knowledge about HIV (AOR =1.31, 95% CI [1.12– 1.54]), being from a medium (AOR = 0.56, 95% CI [0.47– 0.93]) and rich (AOR = 0.80, 95% CI [0.56– 0.80]) households, attending primary (AOR = 0.21, 95% CI [0.16– 0.28]) and secondary (AOR = 0.35, 95% CI [0.25– 0.35]) school, having their first sexual experience at the age of 17 or younger (AOR = 0.26, 95% CI [0.19– 0.93]), having discriminatory attitudes towards HIV patients (AOR = 0.67, 95% CI: 0.47– 0.93) and having no health insurance coverage (AOR = 0.54, 95% CI [0.42– 0.69]) were significantly associated with HIV testing uptake.
Conclusion: HIV testing uptake among rural men was low. Strengthening awareness programmes on HIV and HIV testing, integrating HIV testing with all other healthcare, strengthening partner accompany and HIV testing during pregnancy and delivery, and providing home-based HIV testing may increase HIV testing uptake.
Keywords: HIV, testing, rural, men, determinants, Ethiopia
Plain Language Summary
Ethiopia is located in eastern Africa and has the second-largest population in the African continent. HIV testing coverage among men is poor and a key concern in low-income countries, particularly in East Africa. Men have generally lesser access to HIV testing than women since it is not part of their routine care. Unlike for women, HIV testing is routinely offered during antenatal contact and delivery care. The problems are deeply ingrained in rural men; they have limited access to HIV testing services. Their use of HIV tests may have a greater impact on enhancing HIV testing among both men and women. However, the factors and determinants of HIV testing among rural men have received little attention. Therefore, this study aimed to identify factors associated with HIV testing among rural men in Ethiopia using nationally representative 2016 Ethiopian Demographic and Health Survey data. The result of this study revealed that about 40% of rural men have ever been tested for HIV. The multivariable analysis showed that those who were living in developed regions, engaging in non-agricultural activities, being Muslims, and having comprehensive knowledge about HIV were more likely to be tested for HIV. On the contrary, men who were from better economic status (medium and rich households), literate (attending primary and secondary school), those who had their first sexual experience at the age of 17 or younger, having discriminatory attitudes towards HIV patients, and having no health insurance coverage were less likely to be tested for HIV. Therefore, strengthening awareness-building programmes about HIV and HIV testing services, and providing home-based HIV testing as well as strengthening integration with other healthcare services may increase HIV testing uptake.
Background
Despite enormous effort and commitment, the Human Immunodeficiency Virus (HIV) continues to be a global health burden, affecting 34–35.5 million people globally.1 The greater burden of HIV is carried by the Sub-Saharan African region, which is home to only 12% of the world’s population but is home to 66.6% of people living with HIV (PLWH) and 70% of newly infected cases.1–4 Ethiopia is one of the Sub-Saharan African countries with the highest HIV prevalence, estimated to be between 0.9 and 1.1%.3,5 The HIV epidemic in Ethiopia varies by gender and place of residence. HIV prevalence in men is 0.6%, while it is 1.2% in women. HIV prevalence in urban areas is 2.9%, while it is 0.4% in rural areas.4 HIV testing helps to know the HIV status of an individual with the aim of prevention, care, and treatment.3,6 It is a key component of HIV prevention and care methods.5,6 It allows individuals to know their HIV status, which allows them to seek preventive and curative care. Even if countries initiate different policies and programs to expand HIV testing, they cannot reach their target due to a shortage of supply, high test-related costs, lack of awareness in the community, and high levels of stigma and discrimination,1,6 indicating that continuous monitoring and studies are imperative to provide trustworthy data for policymakers to adopt area- and culture-based initiatives. Given the critical necessity of testing and identifying individuals living with HIV is paramount toto reaching UNAIDS’ ambitious 90–90-90 targets: 90% of PLHIV knowing their status, 90% of PLHIV knowing their status being on treatment, and 90% of PLHIV on the treatment being virally suppressed.6
The basic idea behind this 90–90-90 goal is that if more people are aware of their HIV status, they can reduce HIV transmission, and thereby, HIV-related morbidity and mortality can also be reduced by taking timely and proper treatment and precautions. Although, according to the 2014 Ethiopian service provision assessment report, with recognition of variations across regions and residents, about 45% of private health facilities, 94% of health centers, and 98% of hospitals provided HIV counseling and testing (HCT) services.7 Furthermore, only two-thirds (67%) of people knew their HIV/AIDS serostatus.8 Despite the efforts of all stakeholders, the availability and accessibility of HIV tests are rapidly expanding around the world, particularly in Sub-Saharan African countries, but the number of people tested remains below the required level. In 2017, around 25% of the world’s population did not know their HIV status, and 9.4 million PLWH were unaware of their serostatus, with just about 17% of men tested.9,10
Since men are frequently the head of the household and make the majority of decisions, their use of HIV tests may have a greater impact on expanding HIV testing among both men and women.9,11 Because of a lack of information, males with HIV continue to participate in risky sexual activities, increasing the risk of HIV transmission to women. More often than not, PLWHs who are unaware of their serostatus do not seek healthcare until the disease becomes worse.11 This delay in seeking care, particularly HIV testing, increases the amount of mortality and morbidity.11
National studies in Ethiopia suggest that people are more aware of HIV/AIDS and want to test, although their overall understanding is still limited.8 To combat the spread of HIV/AIDS, a separate HIV/AIDS strategy was developed in 1998, with a strong emphasis on voluntary HIV testing and counseling.12 It has also committed to worldwide HIV prevention targets of 90–90-90.2,6 The Health Sector Transformation Plan II (HSTP II) also aims to reduce new HIV infections by half by 2020, from 0.03% to 0.01%, and to end HIV-related public health problems by 2030.4 In Ethiopia, the trend of new infection rates decreased by 81% between 1995 and 2002, and by 36% between 2002 and 2008. However, the annual incidence rate has risen by 10% since 2008.2 The disparity in the incidence of new HIV infection also existed in Ethiopia, the highest prevalence in 2016 found Gambella region was 5%.13
Studies conducted in different countries on HIV testing uptake indicate that men’s age,3,5,9,13–16 education status,6,9,13,16,17 region of residence,16 marital status,9,13,14,16,18 employment status,18 occupation,13,16 wealth status of the family,5,13,16 sex experience,3 number of lifetime sex partner,13,16 condom usage,13,16 age at first sex,16 perceiver risk of HIV,15 level of knowledge about HIV,15 stigma15 and having insurance coverage16 were associated with HIV testing.
Generally, men have lesser access than women since HIV testing is not part of their routine care. Unlike for women, HIV testing is routinely offered during antenatal contact and delivery care. Men need to actively seek testing. The problems are deeply ingrained in rural men; they have limited access to HIV and other health services, even though health equity is at the top of the global agenda. The Ethiopian Demographic and Health Survey (EDHS) results showed that rural men are unaware of HIV. However, data are scarce on the determinants of HIV testing uptake among rural men. Hence, identifying factors associated with HIV testing uptake is crucial for formulating policies and strategies to increase HIV testing uptake in Ethiopia to achieving the sustainable development goal of “health for all”. Therefore, this study aimed to identify factors associated with HIV testing among rural men in Ethiopia using nationally representative data.
Materials and Methods
Data Source
We used the 2016 Ethiopian Demographic Health Survey (EDHS) data, which is administrated across nine regions and two cities. Ethiopia is located in the eastern part of the African continent and has the second-largest population in Africa continent and 12th-largest population in the world.
Study Design and Sampling Technique
The EDHS is a national, regional, and residential-representative cross-sectional community-based survey. Data was collected through a two-stage stratified cluster sampling technique from January 18, 2016, to June 27, 2016. Each region in the EDHS was stratified into urban and rural areas, yielding 21 sampling strata. In the first stage, a total of 645 enumeration areas (202 in urban areas and 443 in rural areas) were independently selected based on the 2007 Ethiopia population and housing census. In the second stage, a fixed number of 28 households per cluster were selected with an equal probability of systematic selection from the newly created household listing. All men aged 15 to 59 years who were either permanent residents of the selected households or stayed in the selected households the night before the survey were eligible for the study.19
Study Population and Sample Size
The study participants for this study were rural men aged 15 to 59 years. A total of weighted 10,187 rural residence men were included in the analysis.19
Measurements
Outcome Variable
The outcome variable for this study was HIV testing. It was measured by a single direct question asking whether the respondent had ever been tested for HIV or not (the response was Yes /No).
Independent Variables
Based on their availability in EDHS data sets and the literature, the following variables were chosen as independent variables for this study: age at the time of interview (≥30, 31–44, and > 45), wealth status (poor, medium, and rich), and the region in which they currently reside have been recorded as emerging (Afar, Benshangul Gumuz, Somalia, and Gambela) and developed (Tigray, Amhara, Oromia, and South nationality people of the region, Addis Abeba, Harari, and Dire Dawa), marital status (single and married/in-union), an education level (no education, primary, and secondary or above), occupation (non-agriculture and agriculture), religion (others (protestant, catholic and other), orthodox, and Muslim), health insurance coverage (no and yes), age at first sex (<17, 18–24, and >25). Comprehensive knowledge of HIV (limited and enough), and discriminatory attitudes towards HIV patients (Yes / No) were also included. The poor wealth index category was created by combining poorer and poorest, and the rich wealth index category was created by combining richer and richest. Respondents were considered to have comprehensive HIV knowledge if they knew four or more of the seven HIV-related knowledge items (knowing that consistent condom use and having one uninfected faithful partner can reduce the risk of contracting HIV, knowing that a healthy-looking person can have HIV, knowing that HIV cannot be transmitted by mosquito bites or supernatural means, knowing that one cannot become infected by sharing food with an HIV-positive person and rejecting the two most common local misconceptions about HIV transmission). Discriminatory attitudes towards HIV patients was constructed based on the two questions: “Should children living with HIV be able to attend school with children who do not have HIV?” and “Would you buy fresh vegetables from a shopkeeper or vendor if you knew that this person had HIV? If they answered “No” to one or both questions, it was assumed that they “have a discriminatory attitude towards HIV.” This study excluded two important variables that are never heard about, HIV/AIDS and STI, from the model because about 97% of respondents were committed.
Statistical Analysis
Descriptive statistics were computed for each independent variable and were presented in terms of frequency and percentage. To adjust disproportionate sampling and non-response, sample weight was used. We also used the “svyset” command to handle the effect of the complex sample survey in EDHS. Chi-square tests were carried out to assess whether the categories of the variables differed in respect of the outcome variable. Bivariate and multivariate logistic regression analyses were performed to examine the independent association between HIV testing uptake and independent variables. All statistically significant variables p<0.25 at bivariate analysis were retained at multivariate analysis to account for confounding. A 95% confidence interval was used to declare statistical significance in the multivariate analysis with a p-value of less than 0.05. Multi-collinearity for predictor variables with a variance inflation factor of less than ten was checked before multivariable logistic regression analysis was performed. The goodness of fit of the final model was tested by the Hosmer-Lemeshow statistic. All analyses were performed using SPSS version 23.
Ethical Approval and Consent to Participate
We used the EDHS 2016 secondary data for this study. We requested that the Demographic and Health Survey program allow us to use DHS data for this study online. Then, we acquired permission from the Inner-City Fund (ICF) International Ethical Review Board (IRB) to download and utilize the survey dataset for this work (Ethical approval number, AuthLetter 167269). The data set was not shared with or passed on to other organizations, and it was kept confidential. The primary data were gathered following the national ethical procedures. Written consent was obtained from each participant before the collection of data. Consent was obtained from the legal guardians of the minors participating in the study before the data collection. Identification, such as a name, was not recorded to maintain confidentiality.
Results
Socio-Demographic and Other Characteristics of Respondents
A total of 10,187 rural men were recruited for this analysis. The mean age of the participants was 31 years old with Standard Deviation (SD)± 12. As Table 1 shows, about 41% of men were from poor households and half of the men (51.2%) attended primary education, followed by no education (35.6%). About 96% of men live in developed regions, and 57.8% of those men were married during the survey. Close to half (41.6%) of respondents were Orthodox religious followers, followed by Muslims and others at 33.9% and 24.6%, respectively. By working status, the majority (79.2%) of men were engaged in the agriculture sector. About 44% of men start sexual debuts at the age of 18–24, and two-thirds (67.8%) of men had no comprehensive knowledge about HIV. The majority of the respondents (92.2%) have discriminatory attitudes toward HIV patients (Table 1).
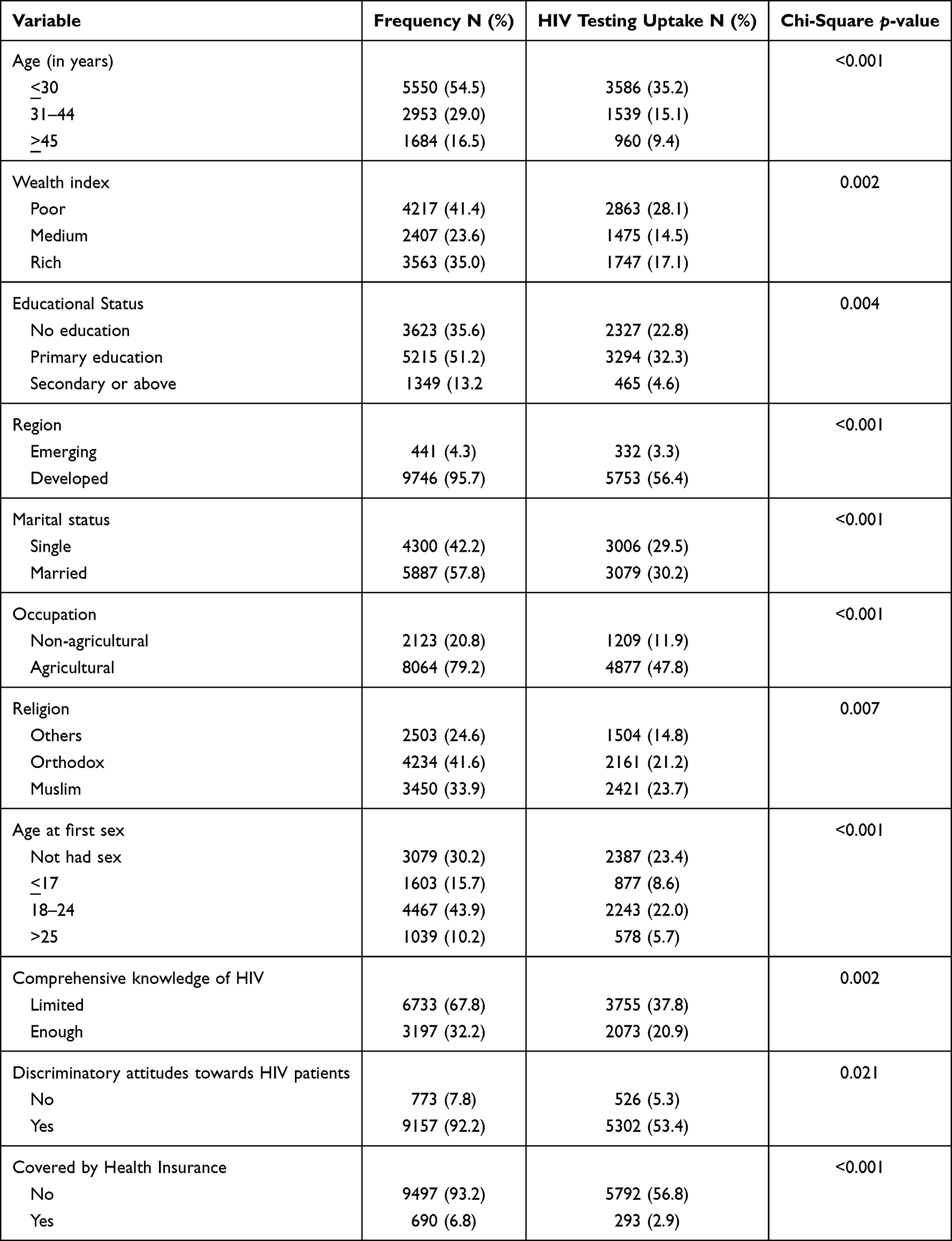 |
Table 1 Socio-Demographic Characteristics of Rural Men and HIV Testing Uptake by Their Characteristics in Ethiopia, Based on EDHS 2016 (N=10,187) |
HIV Testing Uptake Among Rural Men
About 40.3% (95% CI: 37.8–42.8%) of rural had ever been tested for HIV. The proportion of HIV tests differed by age. According to Table 1, 35.2% of the youngest rural men (<30 years) had ever been tested for HIV, while only 9.4% of the oldest men (> 45 years old) had ever been tested for HIV (p <0.001). A third (28.1%) of men from poor households had ever tested for HIV, as compared to 17.1% of men from rich households (p = 0.001). About 56.4% of men from the developed region and only 3.3% of men from the emerging region had ever tested for HIV (p<0.001). The chi-square test result showed HIV testing uptake was associated with all variables included in this model at a P-value <0.05 (Table 1).
Factors Associated with HIV Testing
Table 2 indicates that the age of men, wealth status, education status, region, marital status, religion, age at first sexual debut, comprehensive knowledge about HIV, discriminatory attitudes towards HIV patients, and health insurance coverage were significantly associated with HIV testing in both bivariable and multivariable binary logistic regression analysis at p-values of 0.25 and 0.05, respectively. The odds of being ever tested for HIV among men aged 31–44 years was 1.12 (AOR =1.12; (95% CI; 1.01, 1.42) times higher compared to men aged 45 years or above. Men from medium and rich households were 44.0% (AOR = 0.56; 95% CI; 0.47, 0.67) and 33.0% (AOR = 0.67; 95% CI: 0.56, 0.67), respectively, less likely to be ever tested for HIV compared to men from poor households. Men who attended primary and secondary education were 79.0% (AOR = 0.21; 95% CI; 0.16, 0.28) and 44.0% (AOR = 0.31; 95% CI; 0.25, 0.35)) less likely to be tested for HIV, respectively, compared to men who did not attend formal education. Men who live in the developed region were 1.43 times more likely to be tested for HIV compared to men living in the emerging region (AOR 1.43; (95% CI; 1.09, 1.88)). The odds of being ever tested for HIV among men whose occupation was non-agricultural were 1.27 times higher compared to men whose occupation was in the agricultural sector (AOR 1.27; (95% CI; 1.05, 1.52)). Muslim men had higher odds of HIV testing compared to other religious followers (AOR = 2.07; 95% CI; 1.67, 2.67). Men who started their sexual debut at the age of seventeen years or younger were less likely to be tested for HIV compared to their counterparts (AOR = 0.26; 95% CI; 0.19, 0.36). Men who had a comprehensive knowledge of HIV were 1.31 times more likely to be tested for HIV compared to their counterparts (AOR = 1.31; 95% CI; 1.12, 1.54) (Table 2).
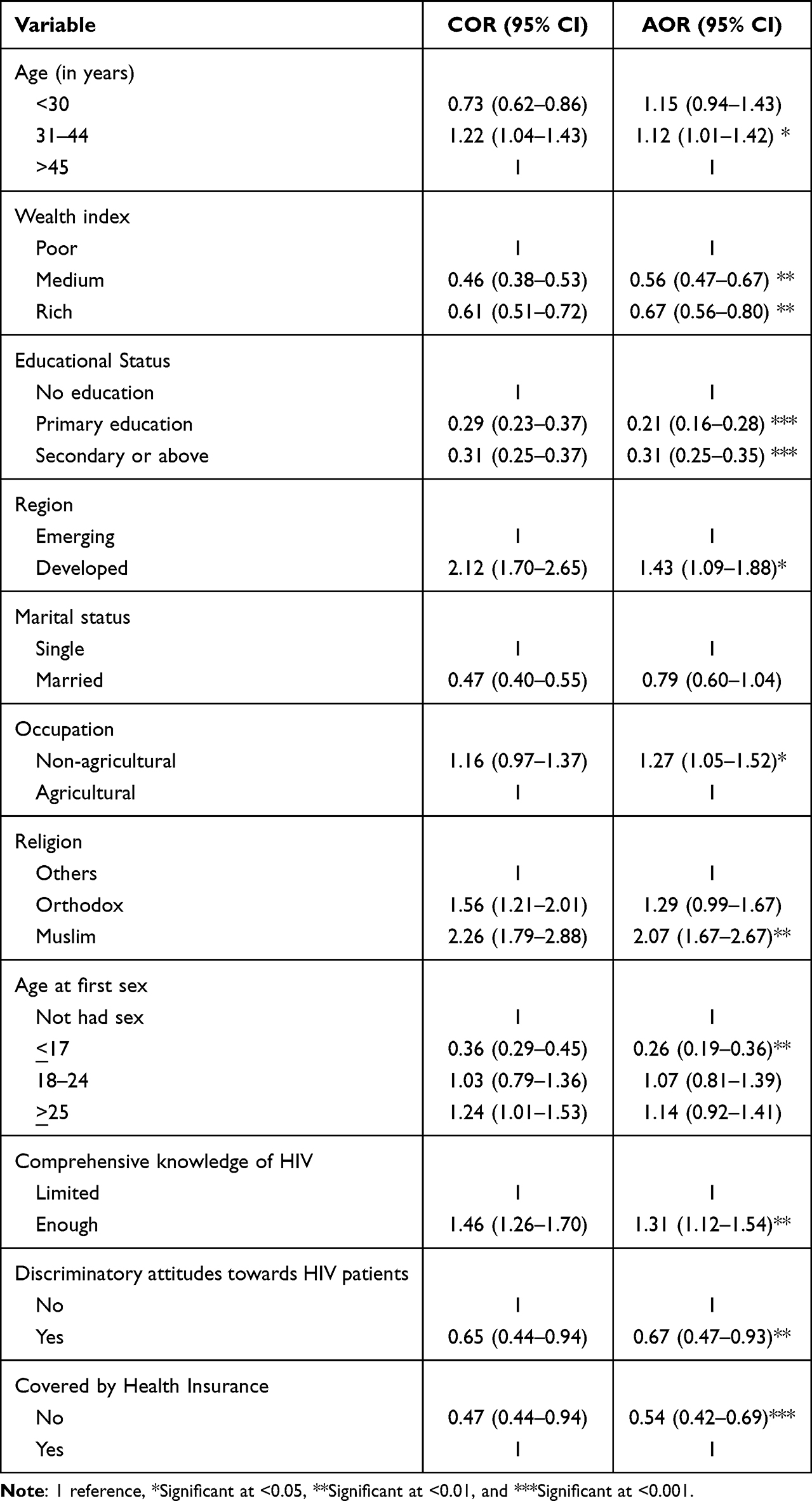 |
Table 2 Factors Associated with HIV Testing Among Rural Men in Ethiopia, Based on EDHS 2016 |
Discussion
The objective of this study was to assess the prevalence and determinants of HIV testing uptake among rural men residents. In Ethiopia, more than 80% of the people reside in a rural setting, having such type of study is paramount for policymakers and program managers to design appropriate and cost effect strategies to enhance HIV-related knowledge and testing uptake as well as minimize HIV transmission by targeting vulnerable groups. It is also crucial to achieving a universal agenda of access to healthcare services for all people and the three 90s agenda by 2030.
Despite governmental and nongovernmental efforts in the last three decades, only 40.3% of rural men were ever tested for HIV in Ethiopia, indicating that Ethiopia will fail to achieve the three 90s global and national targets (90% of PLHIV know their status, 90% of PLHIV knowing their status would be on treatment, and 90% of PLHIV on treatment would be virally suppressed) unless current conditions are changed. If we do not achieve our first 90, we will fall the second and third 90 to achieve. The present finding, however, was higher than the studies conducted in other sub-Saharan countries such as Nigeria, South Africa, and Ghana, the tested prevalence ranged from 14%-22.6%.2,11,15 The possible justification for this may be different among countries in terms of providing HIV testing services through campaigns, integrating HIV services with other routine healthcare services, and making HIV testing available at all health facilities. Besides, variations in cultural attitudes and lifestyles, differences in service quality, and HIV awareness could all be factors for differences in HIV testing service uptake among nations.1 The Ethiopian government is working hard to address the issue, launching a separate HIV/AIDS policy from the national health policy and attempting to provide HIV testing services in nearly all health facilities. Ethiopia also offers free HIV testing, mass mobilization, and HIV awareness programs to the general public. However, the HIV testing rate in rural men was lower than the national rate of HIV testing, at 67%.8 The possible explanation for the urban-rural disparity in HIV testing uptake in Ethiopia is that health facilities are concentrated in urban areas, an outreach of HIV testing services to rural areas may have been particularly scant, and shortages of HIV kits are common in rural settings. Another possible justification for poor HIV testing uptake in rural areas might be attributable to a lack of media exposure, low education, and economic status. Knowledge of HIV transmission is critical for preventing HIV infection and seeking HIV testing. This is especially true for young individuals, who are generally at higher risk due to shorter relationships with more partners or other dangerous activities. Multivariable logistic regression analysis findings showed that socio-demographic and behavioral-related factors influence the use of HIV testing services among Ethiopian rural men. The result revealed that age at interview time, wealth status, education status, region, marital status, religion, age at first sexual debut, comprehensive knowledge about HIV, discriminatory attitude towards HIV patients, and health insurance coverage were significantly associated with HIV testing uptake.
This study showed that adults (31–44 years) had higher odds of being tested for HIV compared to older adults (≥45 years). This finding was consistent with studies undertaken in Burkina Faso, Rwanda, and Cambodia.1,10,16 The reason could be that most men in this age group are fully engaged in sexual relationships or recently married which may provide an opportunity to discuss and get HIV-related information from their sexual partners as well as other sources, boosting the likelihood of HIV testing. In developing countries such as Ethiopia, delaying marriage has lately grown, while having multiple sexual partners is widespread.20 This unsafe sexual conduct may have forced them to be tested for HIV. Furthermore, older men may have a lower perceived need for HIV testing since they are in union.1 Furthermore, fear of HIV stigma may discourage older adult married men in Ethiopia from getting tested for HIV. However, the findings contradicted those of studies conducted in Haiti, South Africa, and Malawi.16,18,21 The disparities could be attributable to differences in government policy, programs, and dedication as well as the sociocultural difference across the nations. Malawian culture, for example, encourages early sexual conduct, which may indirectly motivate people to visit health facilities for HIV counselling and testing.
Surprisingly, this study showed that rural men who attended primary and secondary education were less likely to be tested for HIV. This finding was consistent with studies conducted in the Democratic Republic of Congo, Rwanda, and Congo Kinshasa,1 but not consistent with other studies conducted in other African countries.1,2,14,17,18 HIV testing uptake inequality by education status may be related to HIV/ADIS-related information, access to testing centers, and risky sexual activities. People with more education may be more exposed to HIV-related information and better equipped to make informed decisions about HIV testing than their counterparts. However, this study’s results contradict this expectation. The possible reason might be that educated people living in rural areas believe they do not need the test because they are aware of HIV prevention and can deal with it. Another reason could be that they were aware of the severity and stigma associated with HIV, which led them to refuse to use it.
In this study, rural men from rich households were less likely to be tested for HIV. The result was contradicted by studies conducted in Burkina Faso,11 Nigeria,3 and Cambodia.14 The reason may be due to that their fear of being stigmatized and the loss of their prestige in society if, they are positive.
The findings of this study revealed that rural men living in the developed region had a higher likelihood of being tested for HIV than those living in the country’s emerging regions. The inequality of HIV testing uptake by region was supported by previous studies done in Mozambique and Malawi.16,22 This is because the developed region’s health infrastructure is more advanced than that of the developing region. It enables easier access to the service and enhances their health-seeking behavior. The other reason may be that cultural differences across the region are attributed to regional HIV testing uptake inequality.
This study also identified that rural men engaged in the non-agricultural economic sector were more likely to be tested for HIV as compared to their counterparts. The result was in line with a study conducted in Cambodia.14 This might be since the non-agricultural sector’s engaged segment of the population will have better exposure to media.
According to the findings of this study, rural Muslim men are more likely to be tested for HIV as compared to other religious followers. The finding was supported by a study conducted in Malawi16 but contradicted a study done in Nigeria.15 The discrepancy might be because, unlike in other Muslim-dominated countries in Ethiopia, they are easily accessible to modern education and awareness creation, which gives them freedom of choice, and they are not marginalized from any socio-economic activities.
Rural men who were 17 years old or younger at the time of their first sex debut had fewer odds of ever testing for HIV than those who had not had a sex debut at the same age. This may be due to a lack of awareness about the test and HIV, fear of testing due to their age, or because sex at this age is prohibited by the community. This result was the opposite of the study conducted in Malawi. This might be due to Malawian culture’s allowing early sexual debut, which makes them free to decide to test. Having comprehensive knowledge about HIV would be key to taking a testing decision, but men’s knowledge did not extend from 50%.3,5
This study indicated that rural men who had comprehensive knowledge of HIV had a higher probability of being tested for HIV than those who had not. The result was consistent with studies conducted in Burkina Faso and Nigeria.10,17 This might be because knowledge makes everyone rational, which helps decision-makers to make better choices. Society’s stigmatic attitude will protect individuals from testing for HIV. This study also shows that rural men who were having discriminatory attitudes towards HIV-positive people were less likely to be tested. This might be due to a fear of societal marginalization and exclusion from participating in socio-economic activities if they have got HIV. The result was consistent with the study conducted in many African countries.3,18,23
Rural men who had health insurance coverage were more likely to be tested for HIV than their counterparts. It was in line with a study conducted in Malawi.18 This could be because, even if HIV testing were free, having health insurance packages boosts confidence and health-seeking behavior; they may receive HIV testing services while seeking other healthcare services.
The data for this study comes from a large, nationally representative survey. This finding revealed the HIV testing uptake among rural men as well as the factors contributing to HIV testing uptake. This will help the policymakers ensure more equitable provision of HIV testing services to rural men in Ethiopia by focusing on the identified factors. Some important variables are, however, missing from this analysis because they were not collected at the primary source.
Conclusion
Despite a greater commitment from several stakeholders and a wide variety of service availability and accessibility, this study found that the prevalence of HIV testing among rural men was relatively low. This study indicates that the wealth status of the household, the age of the respondents, their religion, the region where they live, their age at first sex, health insurance coverage, comprehensive knowledge about HIV, and discriminatory attitudes towards HIV patients were associated with HIV testing. So, the concerned bodies could be strategic and design their plan with consideration of the above important variables to improve HIV testing and achieve the universal target of 90–90-90. Therefore, strengthening awareness-building programmes about HIV and HIV testing may increase HIV testing uptake among rural men. This study also emphasizes the importance of strengthening the integration of HIV testing into all men’s health care services, strengthening partner accompanying and HIV testing during pregnancy and delivery care, and providing home-based HIV testing, all of which may be useful in increasing HIV testing uptake in rural Ethiopia.
Data Sharing Statement
The authors used the 2016 EDHS data for this analysis. Since the dataset is publicly available, interested researchers can access it by using the link: https://dhsprogram.com/data.
Acknowledgments
The demographic health survey program should be acknowledged for giving the data set according to our request.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Staveteig S, Wang S, Head SK, Bradley SE, Nybro E. Demographic Patterns of HIV Testing Uptake in Sub-Saharan Africa. MD: ICF International Calverton; 2013.
2. Girum T, Wasie A, Worku A. Trend of HIV/AIDS for the last 26 years and predicting achievement of the 90–90-90 HIV prevention targets by 2020 in Ethiopia: a time series analysis. BMC Infect Dis. 2018;18(1):1–10. doi:10.1186/s12879-018-3214-6
3. Ibrahim M, Ipadeola O, Adebayo S, Fatusi A. Socio-demographic determinants of HIV counseling and testing uptake among young people in Nigeria. Int J Prev Treat. 2013;2(3):23–31.
4. Federal Minster Of Health. HIV Prevention in Ethiopia National Road Map 2018–2020. FHAPaC Office; 2018.
5. Djan D. Factors affecting the attitude of young people towards HIV testing uptake in rural Ghana. J HIV Retro Virus. 2018;4:10–15. doi:10.21767/2471-9676.100045
6. UNAIDS. Aids JUNPo: 90–90-90: An Ambitious Treatment Target to Help End the AIDS Epidemic. Geneva: UNAIDS; 2014.
7. Deribew A, Biadgilign S, Berhanu D, et al. Capacity of health facilities for diagnosis and treatment of HIV/AIDS in Ethiopia. BMC Health Serv Res. 2018;18:1–8. doi:10.1186/s12913-018-3347-8
8. Deribew A, Biadgilign S, Deribe K, et al. The burden of HIV/AIDS in Ethiopia from 1990 to 2016: evidence from the global burden of diseases 2016 study. Ethiop J Health Sci. 2019;29:1.
9. Belato DT, Mekiso AB, Begashaw B. Male partners involvement in prevention of mother-to-child transmission of HIV services in Southern Central Ethiopia: in case of Lemo District, Hadiya Zone. AIDS Res Treat. 2017;2017:1–8. doi:10.1155/2017/8617540
10. Lakhe NA, Diallo Mbaye K, Sylla K, Ndour CT. HIV screening in men and women in Senegal: coverage and associated factors; analysis of the 2017 demographic and health survey. BMC Infect Dis. 2020;20:1–12. doi:10.1186/s12879-019-4717-5
11. De Allegri M, Agier I, Tiendrebeogo J, et al. Factors affecting the uptake of HIV testing among men: a mixed-methods study in rural Burkina Faso. PLoS One. 2015;10(7):e0130216. doi:10.1371/journal.pone.0130216
12. FMOH. Policy on HIV/AIDS of the federal democratic government of Ethiopia; 1980. Available from: https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---ilo_aids/documents/legaldocument/wcms_125382.pdf.
13. Kibret GD, Ferede A, Leshargie CT, Wagnew F, Ketema DB, Alebel A. Trends and spatial distributions of HIV prevalence in Ethiopia. Infect Dis Poverty. 2019;8(1):1–9. doi:10.1186/s40249-019-0594-9
14. Narin P, Yamamoto E, Saw YM, et al. Factors associated with HIV testing among the general male population in Cambodia: a secondary data analysis of the demographic health survey in 2005, 2010, and 2014. PLoS One. 2019;14(7):e0219820. doi:10.1371/journal.pone.0219820
15. Lépine A, Terris-Prestholt F, Vickerman P. Determinants of HIV testing among Nigerian couples: a multilevel modelling approach. Health Policy Plan. 2015;30(5):579–592. doi:10.1093/heapol/czu036
16. Mandiwa C, Namondwe B. Uptake and correlates of HIV testing among men in Malawi: evidence from a national population–based household survey. BMC Health Serv Res. 2019;19:1–8. doi:10.1186/s12913-019-4031-3
17. Magala I, Tapati D, Nalubega R. Factors affecting utilization of HIV care services among men in TASO Masaka, Uganda: an exploratory study. J Clin Microbiol Infect Dis. 2018;2(1):9–11.
18. Peltzer K, Matseke G. Determinants of HIV testing among young people aged 18–24 years in South Africa. Afr Health Sci. 2013;13(4):1012–1020. doi:10.4314/ahs.v13i4.22
19. Csa I. Central Statistical Agency (CSA)[Ethiopia] and ICF. Addis Ababa: Ethiopia Demographic and Health Survey, Central Statistical Agency; 2016.
20. Liga AD, Jabir YN, Wobse BA, Bacha RH. Predictors of multiple sexual partners among men in Ethiopia: a multilevel analysis. Ethiop J Health Sci. 2022;32(4):689–698. doi:10.4314/ejhs.v32i4.4
21. Conserve DF, Iwelunmor J, Whembolua G-L, Sofolahan-Oladeinde Y, Teti M, Surkan PJ. Factors associated with HIV testing among men in Haiti: results from the 2012 demographic and health survey. Am J Mens Health. 2017;11(5):1322–1330. doi:10.1177/1557988316635247
22. Agha S. Factors associated with HIV testing and condom use in Mozambique: implications for programs. Reprod Health. 2012;9(1):1–9. doi:10.1186/1742-4755-9-20
23. Obermeyer CM, Neuman M, Hardon A, et al. Socio‐economic determinants of HIV testing and counselling: a comparative study in four A frican countries. Trop Med Int Health. 2013;18(9):1110–1118. doi:10.1111/tmi.12155
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Determinants of Asthma Attack Among Adult Asthmatic Patients Attending at Public Hospitals of West Shoa Zone, Oromia Regional State, Ethiopia, 2021: Case–Control Study
Megersa S, Chala G, Fikremariam K
Journal of Asthma and Allergy 2022, 15:1143-1154
Published Date: 24 August 2022
Association Between Overweight/Obesity and ART Drug Regimen Among Adult HIV Patients in Gamo Zone Public Health Facilities Southern Ethiopia
Belete NK, Assefa DT, Gadore TF, Teshale MY, Tariku EZ
HIV/AIDS - Research and Palliative Care 2023, 15:349-360
Published Date: 15 June 2023
Determinants of in-Hospital Mortality Among Patients with Acute Coronary Syndrome at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia: unmatched Case Control Study
Admas HA, Altaye KD, Ayalew DG, Mesfin N, Adane A, Tadesse Abebe M, Abegaz SH, Alemu GS, Legese GL
Research Reports in Clinical Cardiology 2024, 15:17-31
Published Date: 21 May 2024
Factors Associated with HIV Testing Uptake in Cameroon: Data from the 2018 Cameroon Demographic and Health Survey
Buh Nkum C, Nanfak A, Guenou E, Fri Kami R, Murhabazi Bashombwa A, Tchio-Nighie KH, Nangue C, Ateudjieu J
HIV/AIDS - Research and Palliative Care 2025, 17:9-17
Published Date: 22 January 2025