Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
HIV Prevalence and Associated Factors in Key Groups and General Population Treated at a Health Care Institution in Colombia in 2019: A Cross-Sectional Study
Authors Cardona-Arias JA ![]() , Cataño Correa JC, Higuita-Gutiérrez LF
, Cataño Correa JC, Higuita-Gutiérrez LF
Received 24 April 2020
Accepted for publication 16 July 2020
Published 25 August 2020 Volume 2020:12 Pages 381—391
DOI https://doi.org/10.2147/HIV.S259792
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Jaiberth Antonio Cardona-Arias,1 Juan Carlos Cataño Correa,2 Luis Felipe Higuita-Gutiérrez1,3
1School of Microbiology, University of Antioquia, Medellín, Antioquia, Colombia; 2Internal Medicine Infectious Diseases Section, University of Antioquia, Medellín, Antioquia, Colombia; 3Faculty of Medicine, Cooperative University of Colombia, Medellín, Antioquia, Colombia
Correspondence: Jaiberth Antonio Cardona-Arias
School of Microbiology, University of Antioquia, Calle 70 No. 52– 51, Bloque No. 5, Oficina 103, Medellín, Colombia
Tel/ Fax +57 2195486
Email [email protected]
Background: Research conducted on the prevalence of HIV/AIDS and its associated factors among key groups in Colombia is scarce. The few available studies show heterogeneity in their results and increasing trends of infection. This study analyses the prevalence of HIV and associated factors in key groups served at a health care institution in Colombia in 2019.
Methods: We performed a cross-sectional study with the sample comprised of 5771 subjects from the general population, the LGBTI community, sex workers, people who inject drugs and prisoners. The diagnosis was based on a fourth-generation ELISA. Variables related to sociodemographics, healthcare, sexual risk factors and biological measures of infected subjects were analysed. Prevalence and odds ratios were calculated with 95% confidence intervals, and logistic regression models were performed to identify confounding variables and interactions between independent variables using SPSS 25.0.
Results: The prevalence of HIV was 0.27% among the general population, 0.53% among sex workers, 0.66% among the homeless, 2.44% among transgender persons, 2.44% among prisoners, 5.36% among men who have sex with men and 7.92% among injection drug users. The explanatory model showed higher prevalence among men, those with higher education levels, those with no health coverage, those who have sex with people from key groups and those with sexually transmitted infections, with some interactions between the latter variables.
Conclusion: A high prevalence of infection was found in the key groups, while the main explanatory factors for high infection rates were identified. The data show that national and global goals related to controlling HIV have not been achieved mainly in groups that are at a higher risk of obtaining and transmitting it and, paradoxically, also that are excluded from the national health coverage.
Keywords: HIV/AIDS, prevalence, risk factors, Colombia, vulnerable groups
Introduction
The human immunodeficiency virus (HIV) affects the immune system’s functionality; at its advanced phase, it leads to acquired immune deficiency syndrome (AIDS), with a high risk of infection, cancer and other comorbidities that can cause death.1–3 The World Health Organization (WHO) reported 38 million infected persons, with 1.7 million incident cases in 2018; and 32 million deaths (770,000 in 2018) with decreased of 45% between 2000 and 2018, in countries that have invested in the prevention, diagnosis, treatment, co-infection control and care from interdisciplinary health teams. The main risk factors are unprotected anal or vaginal intercourse; sexually transmitted infections (STIs); shared use of injectable materials or accidents with sharp objects and blood transfusions or tissue transplants.1,2
The highest occurrence was seen in key groups such as men who have sex with men (MSM), injection drug users, persons deprived of liberty, transgender persons, sex workers and groups with social and economic vulnerability such as young or people with problems accessing health care services.1,2 Comparative studies on the prevalence of HIV in key groups (this was corroborated by several searches on PubMed, SciELO and ScienceDirect using the terms prevalence, HIV, transgenders, MSM, prison, sex workers and homeless) are few, heterogeneous and mostly correspond to national surveys or official reports.
Studies with MSMs have reported prevalence of 3.5% and 50.5%, with risk factors as high number of sexual partners, sex without condoms, drug use and other STIs.4–6 Among sex workers, the prevalence has been 5% - 70%, with a high co-infection of syphilis (5%), chlamydia (8%) and gonorrhoea (2%).7,8 In persons deprived of liberty have been reported prevalence as low as 0.47% or 2–10 times higher than the general population.9,10 In homeless was 17%, with heavy alcohol and injection drug use.11
In Colombia were notified 14,474 HIV cases in 2018 and an increase of 16.4% in 2019, with a rate of 28.1 per 100,000 inhabitants. HIV diagnosis is higher among people aged 25–34 years old (37.1% of the total reported cases), 15–24 years old (24.8%), men (81.4%) and in mixed-race (only 1.2% of cases) in Afro-descendants and 4.3% in indigenous. The 91% of new cases are asymptomatic (AIDS in 9%), the primary infections are wasting syndrome (337 cases), oesophageal candidiasis (287 cases) and pulmonary tuberculosis (228 cases). Among the key groups, the most significant are MSMs (6%), homeless people (1.4%), deprived of liberty (1.1%), transgender persons (1.0%) and injection drug users (0.4%).12,13
There are very few Colombian publications on HIV prevalence (as can be demonstrated by applying this syntax in SciELO (ab:(vih)) AND in:(“col”) AND type:(“research-article”) and the following in PubMed (prevalence HIV[Title/Abstract]) AND Colombia)). The following prevalence indicators stand out in the extant research: among 7.5 million inhabitants in Bogotá was 19 per 100,000 inhabitants, higher in men and people aged 20–34 years old;14 0.2% (N= 5386) and 1.8% (N=5851), among general population from Medellín, with a statistical association by sex (higher in men) and age (higher in those aged 40 years or older);15,16 0.07% among 1,385 women with symptoms of vaginal infection;17 11.0% among 336 MSMs from Bucaramanga;18 7.8% and 16.2% among homeless people in Medellín;19,20 11% among 100 prisoners in Barranquilla, associated with the use of hallucinogens and unprotected sex21 and among 1464 injection drug users the prevalence was 1.9% in Pereira, 2.2% in Cali, 2.7% in Armenia, 3.0% in Bogotá, 3.8% in Medellín and 6.7% in Cúcuta.22
Few studies based in Colombia provide evidence with regard to prevalence of HIV in the key groups; furthermore, there is heterogeneity in the infection’s magnitude and its associated factors. Increasing trends of the occurrence of HIV are a proxy of the ineffectiveness of prevention programmes because the number of screenings has not increased significantly, and comparative studies in key populations, among others, remain absent. This panorama is grave when considering the assertion by the WHO that “insufficient provision of HIV-related services to key population groups … [that] threatens global progress in the response to HIV” because such populations present a higher risk of acquiring and transmitting the infection. Paradoxically, they are excluded from national health coverage plans, laws and health policies.23
Therefore, this research study aimed to analyse the prevalence of HIV and associated factors among key groups served by a health care provider (HCP) in Colombia in 2019.
Methods
Study Type and Population
We conducted a descriptive cross-sectional study with 5771 participants, who were screened for HIV at the Infectious Diseases Foundation of Antioquia (FAI, for its acronym in Spanish) between July and December 2019. This population includes a group of people from the general population (who declared a heterosexual orientation, to differentiate them from the other study groups) in order to have a comparison group, and individuals from key groups such as LGBTI persons, sex workers, injectable drug users and those deprived of liberty. Because the entire (institutional) population was used, the concept of sampling does not apply. People of any gender and age who voluntarily attended the HCP or participated in its external campaigns for HIV screening were eligible to participate in the study. Subjects who did not provide informed consent (n=8) and samples that did not meet the pre-analytical conditions for laboratory processing were excluded (lipemic serum n = 2 and lysate n = 1).
The FAI external campaigns were carried out in prisons, areas with a concentration of sex workers, areas with high homosexual socialisation and care centres for homeless people. For each campaign, a standardised field study was conducted by the FAI, which included communication about incentives for participation by a performing arts team and a group of healthcare professionals (one doctor, two nurses and four assistants) who provided clinical and microbiological information to those interested. For the general population group, the invitation to participate in the study was made in educational institutions, companies and factories, supplying the data from the laboratory in which the samples were processed, in order that each subject could attend voluntarily, and guarantying your privacy and confidentiality.
Information Gathering
Four instruments were used to gather primary information: first, a survey with sociodemographic variables; second, a survey on healthcare services, clinical characteristics and risk factors; third, a screening test was applied for the entire population and positive cases were confirmed and fourth, measures were taken of the viral load, CD4/CD8 lymphocyte count, presence of co-infections and other comorbidities, antiretroviral therapy and other variables related to providing healthcare services for subjects who tested positive, in accordance with the Colombian guide to care for patients with HIV.24
The screening test used was SD BIOLINE HIV1-/2, which is a qualitative rapid detection test in serum, plasma or whole blood of antibodies IgG, IgM and IgA, against recombinant antigens gp41 and p24 specific to HIV-1 including subtype O and gp36 for HIV-2. Alere DetermineTM was used to confirm the diagnosis of HIV-1/2 Ag/Ab combo, an immune-chromatography for the qualitative detection of the p24 antigen and HIV 1–2 antibodies. To calculate the prevalence, all subjects who screened positive after confirmation tests were defined as positive.
Bias Control
Selection bias was controlled by applying the eligibility criteria. Information biases were controlled on three levels. The following aspects were standardised: researcher addressing each study subject, filling the informed consent form and doctors filling the sociodemographic and clinical information; the subjects were motivated to complete the field study and pre- and post-test counselling, and the instrument applied surveys with validity in terms of appearance and content (validated by HCP doctors and epidemiologists and subjects of the screened groups). The screening test has a sensitivity and specificity of 99%, and the confirmatory test has a sensitivity of 100% and specificity of 99.7%.
Statistical Analysis
The categorical variables were described with frequency. Overall HIV prevalence was calculated with a 95% confidence interval. The association between HIV prevalence and sociodemographic and clinical characteristics was determined using Pearson’s chi-squared test. The strength of the association was determined using prevalence ratios (PR) with the Katz method and odds ratios (OR) with the Woolf method, both with 95% confidence intervals. In the event of polytomous variables, dummies were constructed using the lowest prevalence as the reference group. Possible overestimation of the strength of association was determined using the formula [(OR-PR)/(OR-1)], considering values less than 0.1 as low (because of a low-incidence infection).
To identify the confounding factors, multivariate models were performed using logistic regression, requiring a confounder to meet three characteristics: having a statistical relationship with the event, an association with another independent variable and not being an intermediate step on the causal horizon. The presence of interaction was also evaluated using logistic multivariate models, in which the independent variables (eg, variables A, B, C and D) were introduced with the interaction factors for each one (eg, A*B, A*C and A*D) with the following formula:
Y = β0 + β1X1 + β2X2 + β3X3 + βnXn + β1(X1*X2) + β1(X1*X3) + β1(X1*Xn).
The goodness of fit of the logistic models was determined using the Wald and Hosmer-Lemeshow statistic (p > 0.05). The analyses were carried out in SPSS 25.0, with a significance of 0.05.
Ethical Statement
The study abides by the guidelines of the Declaration of Helsinki and Resolution 8430 of the Colombian Ministry of Health, which designates this study as having greater than minimum risk. The study was endorsed by the scientific committee of the HCP and Cooperative University (code INV2790), and the HCP guaranteed follow-up treatment for positive cases. The WHO guidelines for HIV detection were adhered to, that is, informed consent, confidentiality, counselling, ensuring that the results are correct and connected to health services for assistance, treatment and other needs.
Results
About half of the participants corresponded to the general population. Among the risk groups, the highest percentages were that of MSMs and homeless people. The majority were residents of one of the three main cities of Colombia (ie, Medellín, Cali or Bogotá); 58.1% were men; 34.8% were young (21–30 years); 47.9% were married or in a common-law marriage and 57.9% had no formal education (Table 1). The (self-reported) ethnic groups were Afro-descendant (0.6%, n = 36); mixed-race (42.4%, n = 2449) and white (56.9%, n = 3286).
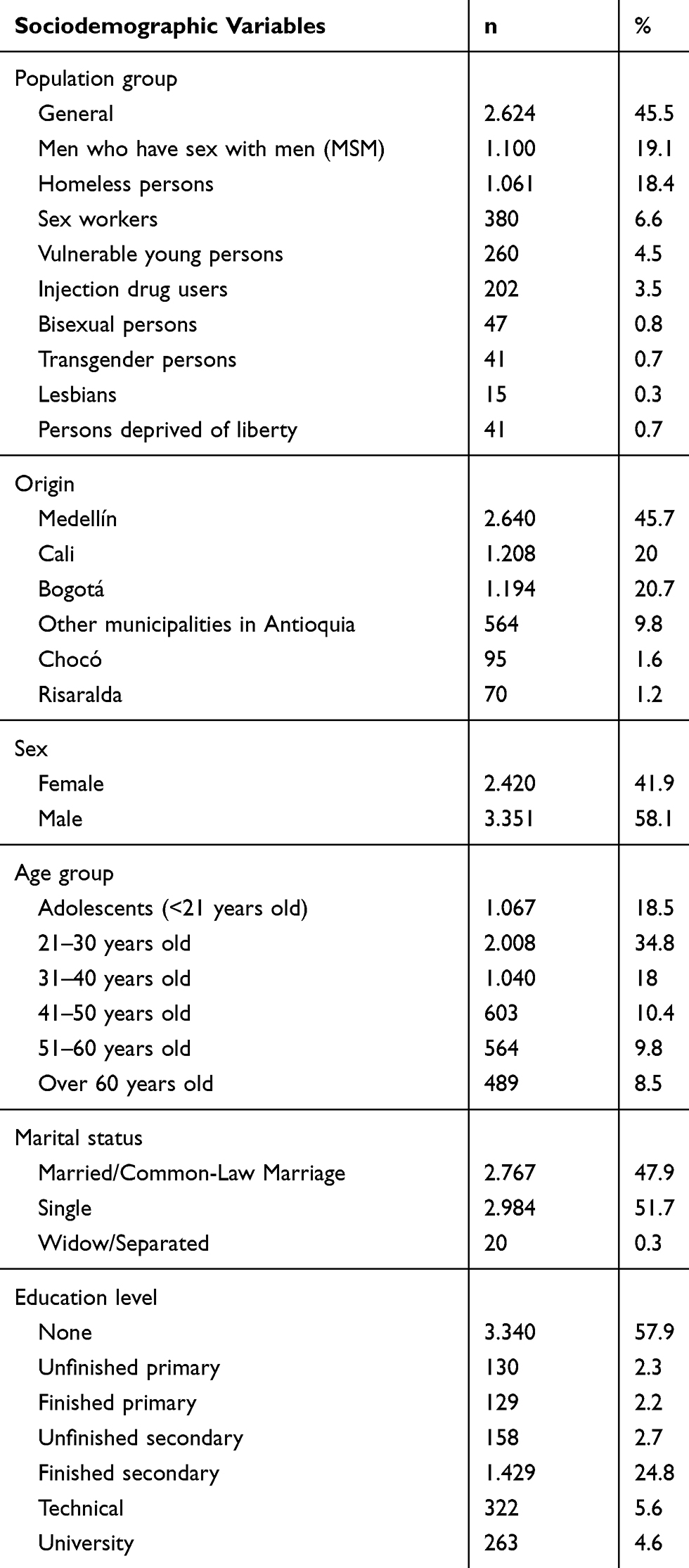 |
Table 1 Sociodemographic Description of the Study Population |
With regard to health coverage, more than half the study population (51.3%) is part of the contributory healthcare system. With regard to perceived health, 18.9% use medications, and 16.4% reported that they were sick in the last month. Only 17.1% donated blood, and 11.0% were hospitalised. In addition, there was a high percentage of participants with risk factors for contracting HIV, such as hallucinogen use in their last sexual relationship (41.0%), a new sexual partner in the last few months (38.3%) and sexual relationships with people with STIs (6.6%), among others (Table 2).
 |
Table 2 Description of Health Characteristics and HIV Risk in the Study Population |
The HIV prevalence was 1.7% (95% CI, 1.3–2.0); among the 96 cases of HIV, 36 (0.6%) had a co-infection with another STI. The prevalence of HIV–HBV co-infection was 0.14% (95% CI, 0.03–0.24), HIV–HCV 0.34% (95% CI, 0.19–0.51) and HIV–Treponema pallidum 0.28% (95% CI, 0.13–0.42); 7 cases (0.12%) presented with a HIV–HBV–HCV co-infection and 1 with HIV-HCV-Treponema pallidum. Timely healthcare (ie, additional examinations and care by health professionals) was provided in less than 30% of the cases detected. 90.6% were in stage 1 according to their CD4/CD8 lymphocyte count. The majority reported symptoms in the last month such as diarrhoea (77.1%), spots (77.1%) or swollen glands (53.1%). 27.1% had previous STIs, and the main STI among the positive subjects and their sexual partners was gonorrhoea (Table 3).
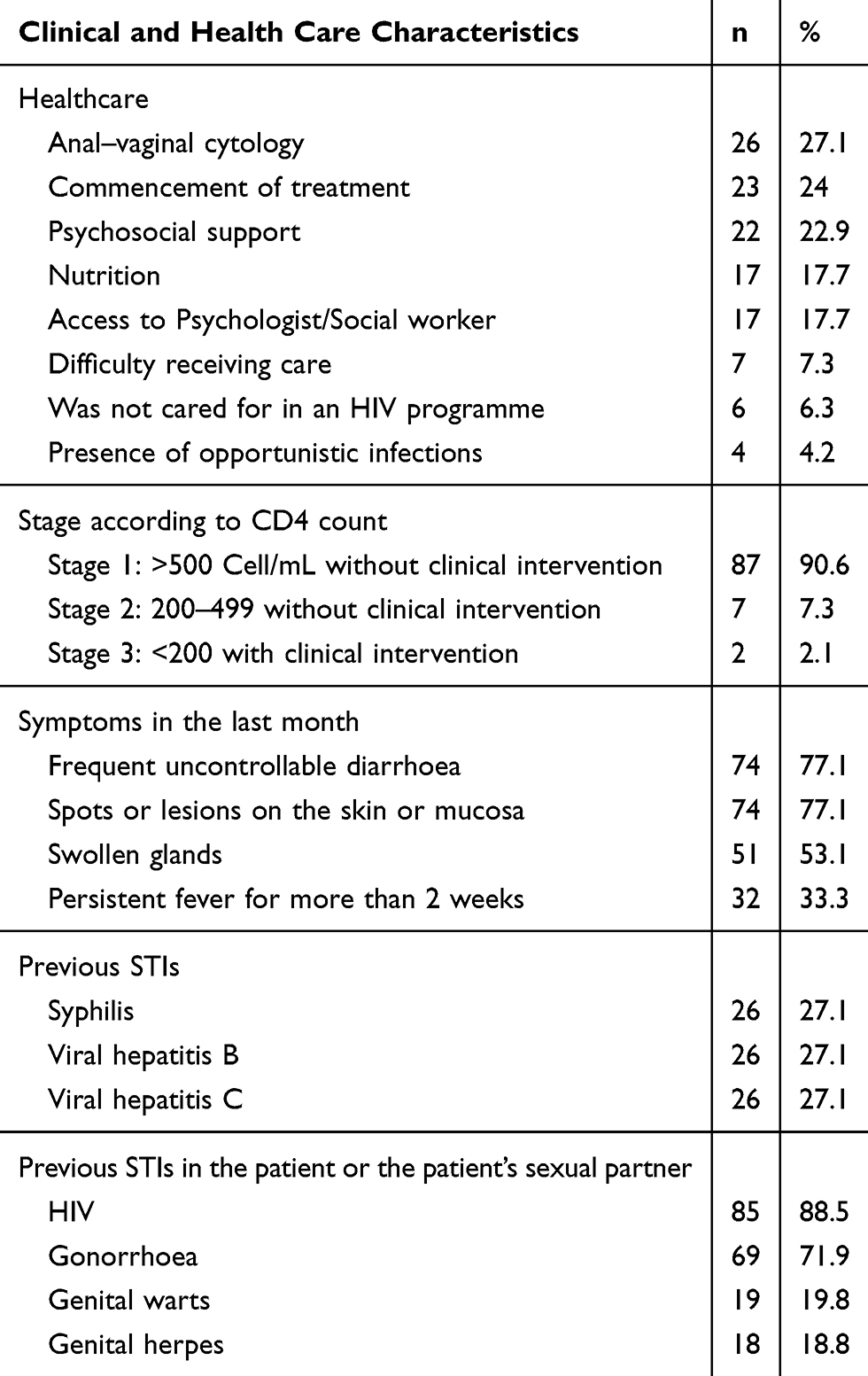 |
Table 3 Clinical and Health Care Characteristics of Positive Subjects (n = 96) |
The following were among the reasons for not seeking timely medical care: being a migrant patient from Venezuela, not having healthcare coverage at a health promoting entity, change of health promoting entity or city, health promoting entity’s administrative problems in verifying medical history data or the patient’s refusal to be referred to a HCP. Opportunistic infections of tuberculosis and toxoplasmosis were recorded.
The prevalence of HIV was statistically associated with the type of population (Chi2 p < 0.001), city of origin (Chi2 p < 0.001), sex (Chi2 p < 0.001), age group (Chi2 p < 0.001), marital status (Chi2 p = 0.006), self-reported ethnicity (Chi2 p = 0.018) and education level (Chi2 p = 0.002). Table 4 shows the specific prevalence of each subgroup (the denominator is the total number of subjects included in a category of the independent variable, for example in the sex, it corresponds to the proportion of positives between the total of men and women, separately), which was higher among injection drug users (7.92%), MSMs (5.36%), people aged 31–40 years (2.88), single people (2.18%) and university students (3.04%). The groups with the highest association are also shown, and the absence of issues related to overestimation is demonstrated (Table 4).
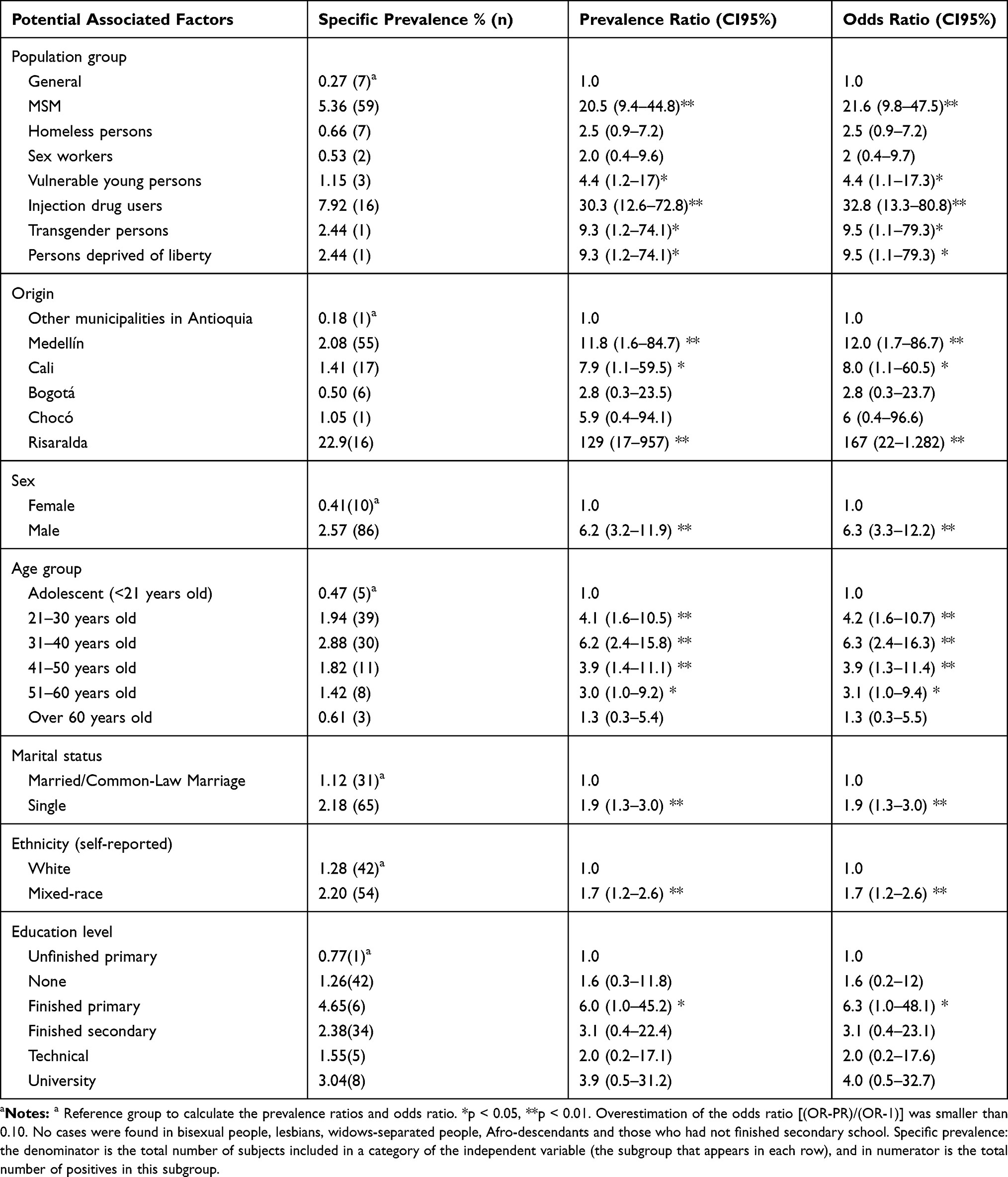 |
Table 4 Specific HIV Prevalence According to Sociodemographic Characteristics in the Study Population |
The prevalence of HIV/AIDS among people without healthcare coverage was 3.7 times that found among those in the contributory system. Furthermore, it was 5.3 times in those who identified a risky sexual relationship, 1.5 times for those who used hallucinogens in their last sexual relationship, 6.4 for those who had sex with key populations and 4.7 for those who had sex with people who had STIs compared with those who did not report these behaviours (Table 5).
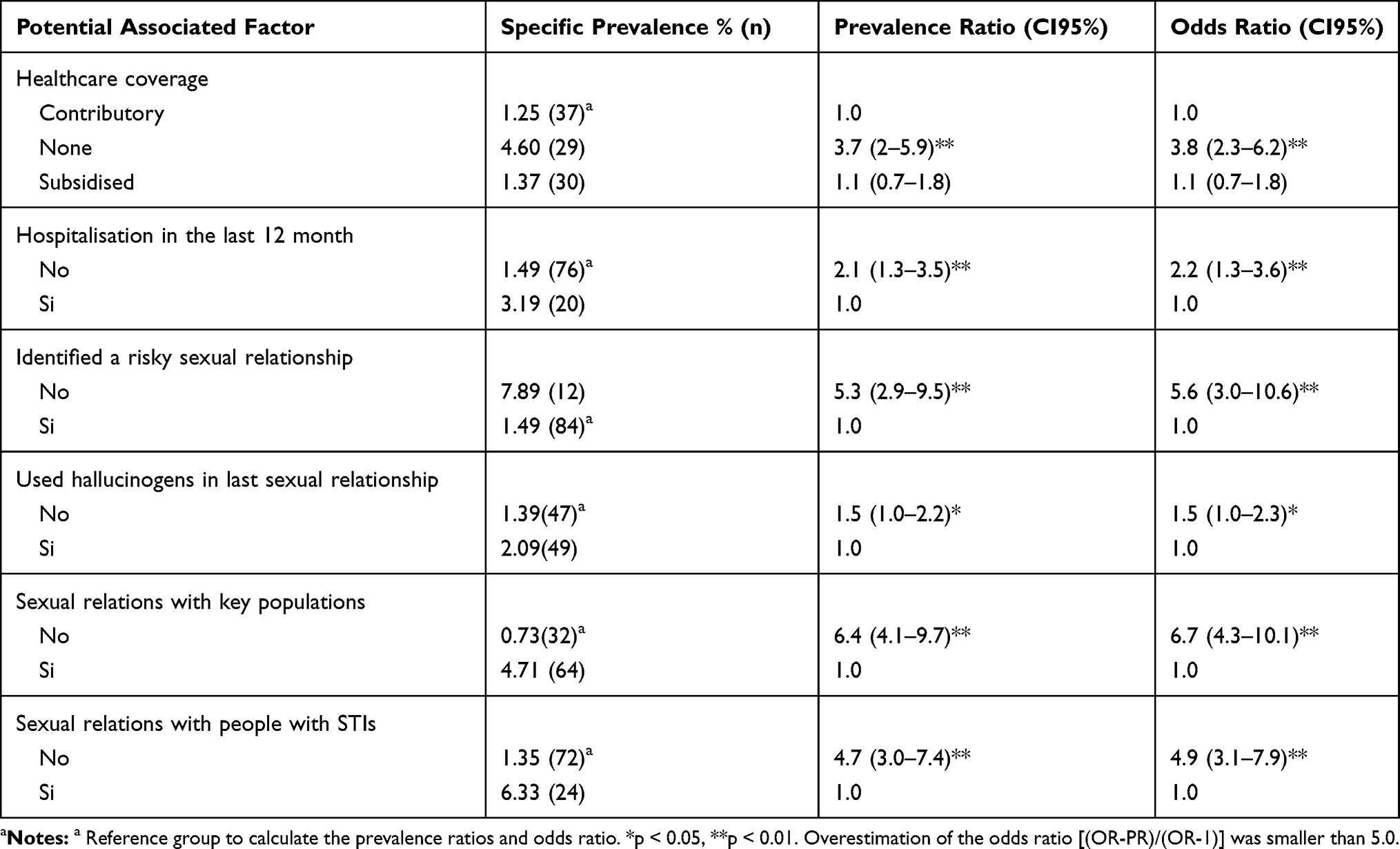 |
Table 5 Specific HIV Prevalence According to Health Characteristics and HIV Risk Factors in the Study Population |
HIV prevalence was not associated with other health variables or HIV risk factors, such as drug use in the last month (Chi2 p = 0.754), previous treatments for HTN (Chi2 p = 0.665), mental disorder (Chi2 p = 0.445) or others; having previously donated blood (Chi2 p = 0.864); having received a blood transfusion or organ or tissue transplant (Chi2 p = 0.367); having a new sexual partner in the last 6 months (Chi2 p = 0.372); engaging in sexual relations in exchange for psychoactive drugs or money (Chi2 p = 0.615); piercings in the last 12 months (Chi2 p = 0.516); deprivation of liberty (own or sexual partner’s) in the last 12 months (Chi2 p = 0.864) or biohazard accident in the last 12 months (Chi2 p = 0.615).
Among the bivariate associations described, those related to previous hospitalisation, city of origin, age, marital status, ethnicity and use of hallucinogens in the last sexual relationship resulted in a confounding effect.
The following variables explain the prevalence of HIV/AIDS in this population: belonging to a key group, sex, formal education, healthcare coverage, identifying a risky sexual relationship and having sexual relations with key groups or people with an STI diagnosis. Among these variables, an interaction (increase in HIV prevalence) was found between belonging to a key group and sex, education level and having sexual relations with subjects from key groups; interaction was also found between sex and having sexual relations with key groups (Table 6).
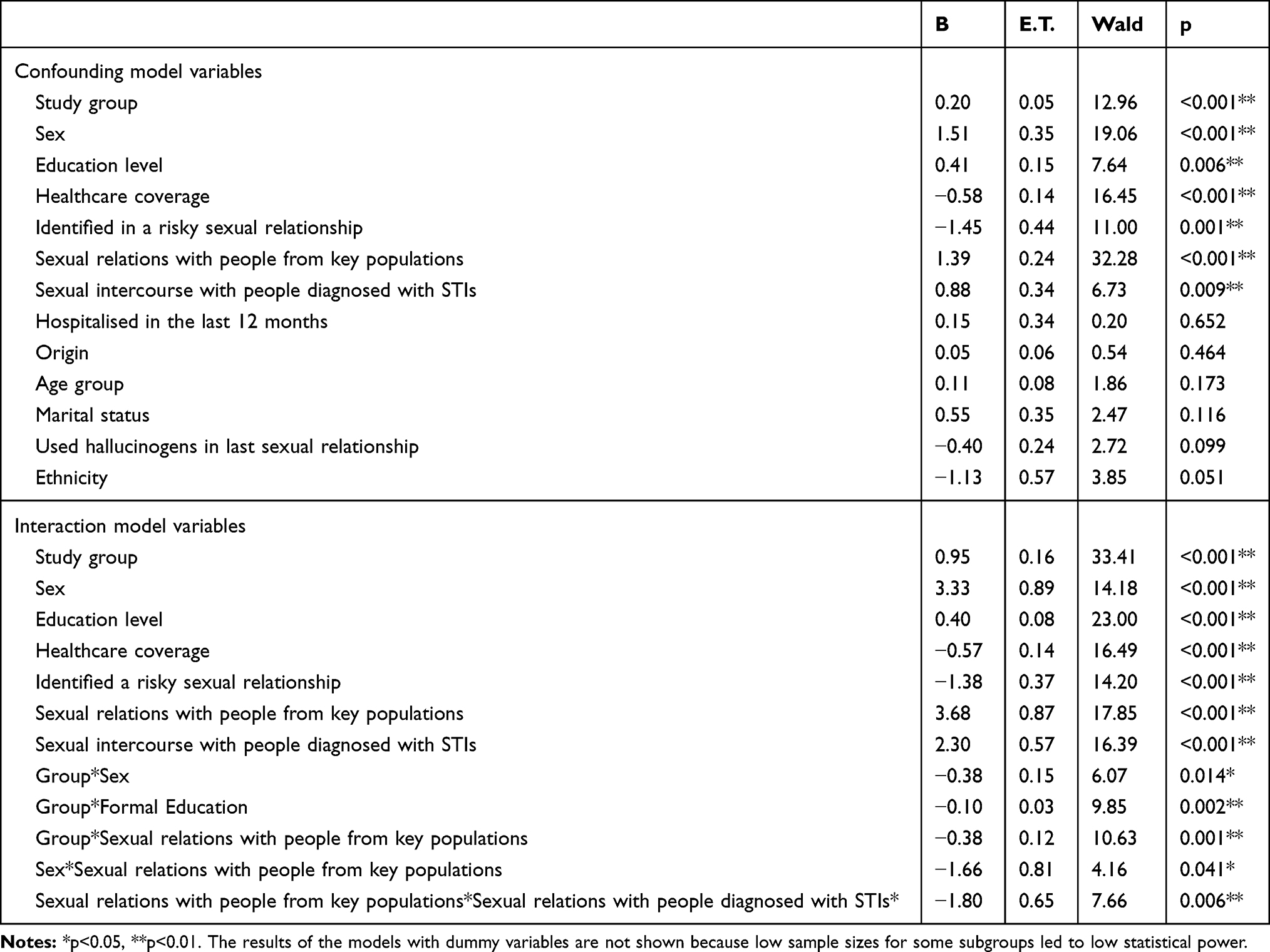 |
Table 6 Evaluation of the Effect Modification Using Multivariate Logistic Regression: Identification of Associations with Confounding and Interaction of Variables |
The main interactions are described below; the prevalence ratios of each subgroup are shown compared to people in the general population:
- For MSMs: 5.5 (95% CI, 1.8–16.7) with no formal education, 27.7 (95% CI, 3.4–227) in subjects who did not finish primary school, 106 (95% CI, 15–778) in those who finished secondary school and 6.8 (95% CI, 3.4–13.7) in those with sexual relations with key groups
- For homeless people: 3.5 (95% CI, 1.0–11.8) in those without a formal education
- For sex workers: 8.5 (95% CI, 1.0–93) in women
- For injection drug users: 131 (95% CI, 14–1233) in women, 14.1 (95% CI, 5.4–36.7) in men, 33.6 (95% CI, 11.3–100) in subjects without a formal education and 69 (95% CI, 5–1038) in those who finished secondary education
- For transgender people: 102 (95% CI, 7–1560) in women
- For prisoners: 22.4 (95% CI, 1.4–350) in those who finished secondary education
Discussion
This research study is one of the first to compare the prevalence of HIV/AIDS in the key groups defined by WHO and adopt in infection control policies in Colombia. An infection rate of 0.27% was found in the general population, 0.53% in sex workers, 0.66% in homeless people, 2.44% in transgender persons, 2.44% in prisoners, 5.36% in MSMs and 7.92% in injection drug users. Potential explanatory factors include sex, education level, type of health coverage and sexual relations with people from key groups or with STIs. This information is highly relevant to evaluate indirectly the institutional efforts to control infection; analyse behaviour in groups seldom studied in the country and identify subgroups with the greatest need for epidemiological monitoring, health care and risk of HIV/AIDS transmission.
The prevalence of HIV in the subgroup of the general population was higher in the present study than in others, such as in the case of Brazil (11–18 cases per 100,000 inhabitants)25 or in the case of Colombian studies, for example, in Bogotá (19 per 100,000 inhabitants).14 Among 5386 people from the general population who visited a Medellín clinical laboratory, it was 0.2%;15 among 5851 healthy people from an HCP in Medellín, it was 1.8%.16 It is also higher among healthy subjects found in blood banks, such as the case of a study in Bucaramanga that reported a prevalence of 0.16% among 3758 donors.26 However, in Colombia, lower prevalence than that reported in the present study has also been found among the general population group. For example, in Medellín, a publication with 65,535 donors reported 0.0%,27 and in Rionegro-Antioquia, a study with 15,461 donors reported 0.04%.28 This heterogeneity in the general prevalence is far from the consistency found in specific prevalences, given that these studies report a statistical association between sex (higher among men) and age (higher among young adults)14–16,25–28 among people who appear to be healthy. These findings present two direct implications. First, the epidemiological characteristics of each population indicate the need to increase studies in each city to gather evidence that demonstrates the achievement of or delay in meeting national and international goals to control the epidemic. Second, the consistent association between age and sex shows the need to increase diagnostic, preventive and therapeutic efforts among men and younger adults (25–40 years old), given that they present the highest specific prevalence and constitute groups at high risk of transmission.
Among the key groups, the lowest prevalence among those infected was found in sex workers (0.53%) and homeless people (0.66%). This is much lesser than the results found in studies in the international sphere, which report 5%–70% prevalence for the first group7,8 and 16%–28% for populations similar to homeless people in countries such as Ukraine11 or 7.8%–16.2% in other studies with homeless people in Medellín, Colombia.19,20
These results lead to the development of three hypotheses. First, the low prevalence found among these groups is an indirect indicator of the effectiveness of preventive actions focused on them. The institutions responsible for intervention could evaluate this hypothesis with studies that establish causal relationships with their programmes, and thus, these interventions could be replicated in other contexts. Second, the discrepancy with previous research accounts for the variability present among countries, within each country and over time; that is, it reflects the impossibility of extrapolating results and the need for constant monitoring with screening tests in these population groups. Third, the low prevalence in highly exposed groups may be mediated by immunological mechanisms that have given rise to HIV-1-exposed seronegative (HESN). Subsequent studies should address these immunological mechanisms in this population.
With regard to other key groups, the evidence found in this study and past research is highly heterogeneous, indicating the need to improve knowledge of group-specific epidemiological profiles. The present study found a prevalence of 2.44% among prisoners, unlike international studies that indicate rates as low as 0.47% or studies that indicate that HIV and other STIs are 2–10 times higher in this population compared to the general population.9,10 In contrast, national evidence reports 11% infection rates in prisoners from Barranquilla, Colombia.21 The differences between studies can be attributed to methodological issues related to sample size calculation, sampling or the diagnostic performance of the test used. Beyond the magnitude of the difference, in Colombia there is consistency in results, indicating that the prevalence of HIV in prison population is much higher than that in the general population. Therefore, governments need to deploy strategies to guarantee the right to health and medical care to this population, with measures that include providing access to condoms, disposable syringes and needles, health education and ensuring care for infected people. In this respect, it is important to understand that the prison population has the same health rights as the general population and that their lives and health are related to that of the general population in many ways.
The prevalence of HIV among MSMs in the present study was 5.36%; among 575 MSMs from the Netherlands, it was 3.5%;4 among 2303 MSMs from Germany, 50.5%5 and in Colombia, a study with 336 MSMs from Bucaramanga reported 11% prevalence.18 Despite the differences in HIV occurrence, all studies report very high prevalence in this population, thus corroborating the need to join efforts to screen MSMs for infection. In terms of preventive actions, it is necessary to review those that are being implemented because they are not as effective as expected. Actions such as including MSMs in planning policies in the fight against AIDS, addressing homophobia, discrimination and stigma regarding sexual preferences and protecting MSMs from human rights abuses and sexual violence are essential aspects in resolving inaccessible or poorly focused programmes.
A HIV prevalence of 2.44% was found among transgender persons, there is no history of research with this group in Colombia. Among injection drug users, this study found 7.92% to be infected. Internationally, data as low as 0.7% have been reported for this group, while in Colombia the figures have ranged between 1.9% and 6.7%.22 This finding highlights the importance of incorporating the WHO’s recommendations, which include educational health interventions, access to condoms, prevention of sexual violence, drug addiction treatment, prevention of transmission due to tattoos and piercings, prophylactic medications and prevention and treatment of STIs.30
WHO recommendations for key groups emphasise the need to work with these groups, including using antiretrovirals as a prophylactic method; this practice could reduce incidence by 20–25%. This has been supported by evidence showing how the probability of contracting HIV/AIDS is 14 times higher among sex workers, 19 times higher among MSMs, 50 times higher among transsexual women and 50 times higher among injection drug users compared to the general population. In addition, global analyses indicate that problems related to accessing healthcare services persist in these groups. There are no services that meet their needs; they are discriminated groups and in many cases, these populations are stigmatised or socially excluded, which is a major obstacle in achieving the goals of fighting the epidemic.23 This vulnerability is exacerbated among this study’s population; in addition to the inherent risk of belonging to a key group, those infected in this population faced deficiencies in care. The present study identified other explanatory factors of the infection, such as education level, type of health coverage and having sexual relations with people from key groups and those with STIs. Interactions among these demonstrate the complexity of the situation and the need for intersectoral, interdisciplinary and inter-institutional actions.
Limitations of this research study include the temporary bias of cross-sectional studies (not being able to establish whether associated variables preceded the infection), low sample size in some key groups (that affects the possibilities of extrapolation of the result), and low statistical power of some comparisons, especially multivariate ones. In this last limitation, it is worth specifying that, despite the fact that the primary outcome was HIV prevalence, statistical associations were explored in order to generate hypotheses for subsequent studies, identifying related variables or groups with a higher occurrence; however, some bivariate and multivariate statistics, mainly in the comparison with the smaller sample size groups, could have power problems (to report as non-significant, some statistical associations that do exist but require a higher n).
Consistent with these limitations and the previous discussion, it is recommended to improve the application of clinical practice guidelines for all those infected and the efforts to screen sexual partners in key groups, decrease treatment times and connect infected patients with care programmes. In addition, the recruitment strategies of the subjects of the key groups must be improved through active surveillance (that the interdisciplinary health team goes to their daily workplaces), motivational campaigns for screening by peers, active members of their groups or non-governmental organizations with experience in the field work with these populations.
Conclusion
A high prevalence of infection was found in the key groups, and the main explanatory factors for high infection rates were identified. This shows the need to increase health efforts for prevention, diagnosis and treatment of cases, mainly in groups that are at a higher risk of contracting and transmitting it while, at the same time, being excluded from national health coverage.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Organización Mundial de Salud (OMS). VIH/SIDA. Datos y cifras. Consultado marzo 2020.2020. Available from: https://www.who.int/es/news-room/fact-sheets/detail/hiv-aids.
2. Organización Mundial de Salud (OMS). Estrategia mundial del sector de la salud contra el VIH, 2016-2021. Hacia el Fin del SIDA. Ginebra: OMS; 2016.
3. Deeks SG, Overbaugh J, Phillips A, Buchbinder S. HIV infection. Nat Rev Dis Primers. 2015;1:15035. doi:10.1038/nrdp.2015.35
4. Woestenberg PJ, van Benthem BHB, Bogaards JA, et al. HPV infections among young MSM visiting sexual health centers in the Netherlands: opportunities for targeted HPV vaccination. Vaccine. 2020;38:3321–3329. doi:10.1016/j.vaccine.2020.03.002
5. Jansen K, Steffen G, Potthoff A, et al. STI in times of PrEP: high prevalence of chlamydia, gonorrhea, and mycoplasma at different anatomic sites in men who have sex with men in Germany. BMC Infect Dis. 2020;20:110. doi:10.1186/s12879-020-4831-4
6. Kusnan A, Alifariki O, Asriati BIMC, et al. Risk factors for HIV incidence in MSM (male sex man) communities in province of southeast Sulawesi. Enferm Clin. 2020;30(Suppl 2):80–83. doi:10.1016/j.enfcli.2019.07.037
7. Almeida N, Melo M, Soares I, Carvalho H. Screening of human immunodeficiency virus and other sexually transmitted infections in a group of sex workers in indoor settings in the Porto metropolitan area. Acta Med Port. 2020;33(3):166–173. doi:10.20344/amp.11687
8. Owen BN, Giroux M, Matse S, et al. Prevalence and correlates of anal intercourse among female sex workers in eSwatini. PLoS One. 2020;15:e0228849. doi:10.1371/journal.pone.0228849
9. Hernández-Vásquez A, Huarez B. HIV in prison: results from a national prison census in Peru. Int J STD AIDS. 2018;29:203–205. doi:10.1177/0956462417744372
10. Organización Mundial de la Salud (OMS), Oficina de Naciones Unidas contra la Droga y el delito (UNODC), ONUSIDA. Interventions to address HIV in prisons. Evidence for action technical papers. Ginebra, OMS, 2007. Available from: http://www.who.int/hiv/pub/prisons/e4a_prisons/en/index.html.
11. Hosseinnataj A, Bahrampour A, Baneshi MR, et al. Correlates of alcohol consumption and drug injection among homeless youth: a case study in the Southeast of Iran. Addict Health. 2019;11:207–215. doi:10.22122/ahj.v11i4.245
12. Instituto Nacional de Salud. Gobierno de Colombia. Comportamiento del VIH/SIDA. Consultado marzo 2020; 2018. Available from https://www.ins.gov.co/buscador-eventos/BoletinEpidemiologico/2018%20Bolet%C3%ADn%20epidemiol%C3%B3gico%20semana%2047.pdf.
13. Instituto Nacional de Salud. Gobierno de Colombia. Comportamiento Del VIH/SIDA 2019. Consultado marzo 2020; 2018. Available from https://www.ins.gov.co/buscador-eventos/BoletinEpidemiologico/2019_Boletin_epidemiologico_semana_47.pdf.
14. Velásquez J, Contreras L, Contreras C, Martínez N, Chaparro J, Sarmiento C. Prevalencia de infección por VIH en Bogotá, D.C., Colombia, en 2012. Caracterización por localidades. Rev Fac Med. 2016;64:609–613. doi:10.15446/revfacmed.v64n4.54148
15. Callejas-Rojo F, Serna-Quintana G, Cardona-Arias JA. Frecuencia de reactividad a la prueba VDRL y de positividad para Chlamydia spp, VIH y virus de la hepatitis B y C en una institución prestadora de servicios de la salud de Medellín, 2015. CES Med. 2017;31:27–37. doi:10.21615/cesmedicina.31.1.3
16. Cardona-Arias J, Álvarez-Flórez C, Gil-Ruiz G. Prevalencia de VIH G-RG/Sida en Medellín y evaluación del desempeño de la prueba presuntiva, 2006-2012. Rev salud publ. 2013;15:888–903.
17. Ángel-Müller E, Rodríguez A, Núñez-Forero LM, et al. Prevalencia y factores asociados a la infección Por C. trachomatis, N. gonorrheae, T. vaginalis, C. albicans, sífilis, VIH y vaginosis bacteriana en mujeres con síntomas de infección vaginal en tres sitios de atención de Bogotá, Colombia, 2010. Rev Colomb Obstet Ginecol. 2012;63:14–24. doi:10.18597/rcog.199
18. Rodríguez L, Moreno L, Bautista J, et al. Revalencia de infección por VIH/SIDA en hombres que tienen sexo con hombres en Bucaramanga, Colombia. Rev Univ Ind Santander Salud. 2009;41:135–141.
19. Berbesí D, Segura-Cardona Á, Caicedo B, Cardona-Arango D. Prevalencia y factores asociados al VIH en habitante de calle de la ciudad de Medellín Colombia. Rev Fac Nac Salud Pública. 2015;33:181–191. doi:10.17533/udea.rfnsp.v33n2a07
20. Berbesi D, Agudelo A, Segura A, Montoya L. VIH en habitantes de calle de Medellín. Rev Fac Nac Salud Publ. 2012;30:310–315.
21. Gaviria García G, Lastre Amell G, Trejos A. Prevalencia del VIH y conductas de riesgo en internos de un centro carcelario del distrito de Barranquilla (Colombia). Salud. Barranquilla. 2015;31:25–35.
22. Berbesi-Fernández D, Segura-Cardona AM, Montoya-Vélez L, López-Ramírez E. Situación de VIH en usuarios de drogas inyectables en Colombia. Infectio. 2016;20:70–76. doi:10.1016/j.infect.2015.07.004
23. Organización Mundial de la Salud. La OMS advierte de que las personas con más riesgo de contraer la infección por el VIH no están recibiendo los servicios de salud que necesitan. Consultado marzo 2020; 2014. Available from https://www.who.int/mediacentre/news/releases/2014/key-populations-to-hiv/es/.
24. Ministerio de Salud y Protección Social. República de Colombia. Guía de Práctica Clínica basada en la evidencia científica para la atención de la infección por VIH/Sida en adolescentes (con 13 años de edad o más) y adultos. Consultado marzo 2020; 2014. Available from http://gpc.minsalud.gov.co/gpc_sites/Repositorio/Otros_conv/GPC_VIH_adolescentes/GPC_Comple_VIHADULTOS_web.pdf.
25. Dartora WJ, Propp Ânflor É, Ribeiro Pavão da Silveira L. Prevalência do HIV no Brasil 2005-2015: dados do Sistema Único de Saúde. Rev Cuid. 2017;8:1919–1928. doi:10.15649/cuidarte.v8i3.462
26. Daza N, Sánchez M, Vanegas T, Ortega I. Prevalencia de infecciones en donantes de sangre en la Universidad Industrial de Santander versus parques de la ciudad de Bucaramanga, 2014. Med UIS. 2016;29:55–60.
27. Bedoya JA, Cortés Márquez MM, Cardona Arias JA. Seroprevalence of markers of transfusion transmissible infections in blood bank in Colombia. Rev Saúde Publ. 2012;46(6):950–959. doi:10.1590/S0034-89102012000600004
28. Giraldo-Valencia EC, Morales-Gallo ME, Maya-Guerrero MA, Rendón-Castrillón LE, Cardona-Arias JA. Prevalencia de marcadores de infecciones transmisibles y su relación con variables domográficas en un banco de sangre Antioquia-Colombia 2010–2013. Rev CES Med. 2015;29:59–74.
29. Hickman M, Hope V, Coleman B, et al. Assessing IDU prevalence and health consequences (HCV, overdose and drug-related mortality) in a primary care trust: implications for public health action. J Public Health (Oxf). 2009;31:374–382. doi:10.1093/pubmed/fdp067,
30. OMS. UNODC, ONUSIDA.. Prevención, tratamiento y atención del VIH en las cárceles y otros lugares de reclusión: Conjunto completo de intervenciones. Consultado marzo 2020. Ginebra: OMS; 2007. Available from: https://www.who.int/hiv/pub/prisons/prison_comp_pack_sp.pdf?ua=1.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.