Back to Journals » Risk Management and Healthcare Policy » Volume 18
HIV and HCV Screening, and Pre-Exposure Prophylaxis Among Managed Care Beneficiaries with Substance Use Disorders: A Cross-Sectional Study from a Single State
Authors Austin S ![]() , Zhang Y, Venkat D, Fisk SN, Madden M, Cuevas E, Edwards A, Qu H
, Zhang Y, Venkat D, Fisk SN, Madden M, Cuevas E, Edwards A, Qu H ![]()
Received 21 June 2025
Accepted for publication 22 November 2025
Published 17 December 2025 Volume 2025:18 Pages 3889—3899
DOI https://doi.org/10.2147/RMHP.S545358
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mecit Can Emre Simsekler
Shamly Austin,1 Yuan Zhang,2 Divya Venkat,3 Stuart N Fisk,4 Michael Madden,5 Elizabeth Cuevas,3 Anita Edwards,5 Haiyan Qu6
1Research & Development, Highmark Wholecare, Pittsburgh, PA, 15222, USA; 2Population Health Analytics, Highmark Wholecare, Pittsburgh, PA, 15222, USA; 3Center for Inclusion Health, Allegheny Health Network, Pittsburgh, PA, 15212, USA; 4Office of Behavioral Health, Allegheny County Department of Human Services, Pittsburgh, PA, 15222, USA; 5Medical Management, Highmark Wholecare, Pittsburgh, PA, 15222, USA; 6Department of Health Services Administration, University of Alabama at Birmingham, Birmingham, AL, 35294, USA
Correspondence: Shamly Austin, Research & Development, Highmark Wholecare, 501 Penn Ave, Pittsburgh, PA, 15222, USA, Email [email protected]
Purpose: Screening for HIV and Hepatitis C (HCV) is critical in caring for individuals with substance use disorders (SUD). This is particularly relevant in identifying prescribing habits for Pre-Exposure Prophylaxis (PrEP). The objectives were to examine HIV and HCV screening rates, and PrEP prescription among managed care beneficiaries with SUD and without an HIV diagnosis and determine the factors associated with the screenings and PrEP prescriptions.
Methods: We conducted a retrospective cross-sectional analysis (January–December 2021) of managed care claims for beneficiaries who visited either urban primary care clinics or emergency departments affiliated with an academic medical center. Sample included 2381 Medicaid and dually eligible for Medicare and Medicaid managed care beneficiaries with SUD, continuously enrolled for 12 months, 21 years or older, and without an HIV diagnosis. Substances included in the analysis were alcohol, opioid, cocaine, cannabis, and other psychoactive drugs. Univariate descriptive statistics and multivariable logistic models were used to address the objectives. Rates of HIV and HCV screening, and PrEP prescriptions were examined. Outcome variables for multivariable logistic regression were whether beneficiaries had HIV screening, HCV screening, and PrEP prescription. The predictors were age, gender, race, primary language, area of residence, insurance type, chronic conditions, tobacco use, polysubstance use, number of providers seen, primary care physician seen, emergency department visits, hospitalizations, and annual cost of care.
Results: About 22% of beneficiaries had HIV or HCV screening; PrEP prescriptions were non-existent in this sample. About 83% visited their primary care physician (PCP). The predictors of HIV and HCV screenings include gender, area of residence, polysubstance use disorder, PCP visits, and hospitalizations.
Conclusion: Results indicate low HIV and HCV screening rates and no PrEP prescriptions among the managed care population with SUD. Specifically, beneficiaries with rural residence, females, and Medicaid beneficiaries need targeted interventions and missed opportunities exist at PCP offices.
Keywords: substance use disorder, HIV screening, HCV screening, pre-exposure prophylaxis, managed care, Medicaid, dually eligible for Medicare and Medicaid
Introduction
Substance use disorders (SUD), HIV, and HCV (Hepatitis C) are intricately linked. According to the National Survey on Drug Use and Health, about 16.8% of the US population, ages 12 years and older had SUD in 2023.1 SUD can impact behaviors such as needle sharing and condomless sex that may increase the probability of acquiring HIV and HCV, and transmission to others.2 Moreover, about 14% and 40% of individuals are unaware of their HIV and HCV positive status, respectively.3,4
One of the strategies to reduce HIV and HCV incidence is to implement screenings and prescribe Pre-Exposure Prophylaxis (PrEP) for HIV prevention among individuals with SUDs. For HCV, no effective pre-exposure or post-exposure prophylaxis is available, but harm reduction education can be effective, and curative antiviral therapy is available.3 The United States Preventive Services Task Force (USPSTF) recommends at least one HIV and HCV screening annually or more frequent screenings for high-risk groups.5,6 These guidelines also recommend PrEP for persons who inject drugs (PWID) and have high-risk sexual behavior.7 The guidelines do not consider persons with a history of drug use but who are not PWID as high-risk. The use of PrEP reduces HIV risk by 74% for PWID and 99% for people with high-risk sexual behaviors.7,8 However, despite the guidelines, screening and PrEP prescribing rates are low in the SUD population. Although the number of SUD treatment facilities increased from 2017 to 2020, the proportion of facilities offering HIV and HCV screening did not increase during this period. Only half of the SUD treatment facilities offered the screenings9 and 36% of individuals were prescribed PrEP among people with PrEP indications.10
In Pennsylvania, access to HIV and HCV screenings and PrEP prescription for Medicaid beneficiaries is covered by the Office of Medical Assistance through managed care. Medicaid is the single largest payer for SUD and HIV treatment.11,12 Managed care organizations (MCOs) are now the dominant form of delivery system for Medicaid.13 Hence, MCOs are well positioned to support population health strategies to reduce HIV and HCV incidence in Medicaid beneficiaries. The Pennsylvania state Medical Assistance and the Medicaid MCOs do not require prior authorization for PrEP prescription14,15 and HCV treatment.16 Despite the coverage, the screenings and PrEP prescription rates are low. This could be attributed to lack of beneficiaries’ awareness about the availability of services, lower risk perception, mistrust and negative patient-provider communication, and structural inequities such as housing instability, poverty, and incarceration.10 Early detection of HIV and HCV reduces associated morbidity and mortality and decreases transmission to others.17,18 Increasing screening rates in SUD treatment facilities could identify HIV and HCV positive individuals earlier and improve their linkage to appropriate care. Hence, the objective of the study is twofold. First, to estimate HIV and HCV screening rates and PrEP prescription rates among Medicaid and dually eligible for Medicare and Medicaid managed care beneficiaries with SUDs but without an HIV diagnosis. Second, to examine the factors associated with HIV and HCV screenings and PrEP prescription in this population.
One of the widely used theoretical frameworks to examine individuals’ health care access and utilization is the Behavioral Model of Health Care Utilization.19,20 According to this model, beneficiaries’ HIV and HCV screening behaviors can be explained by three groups of factors: predisposing factors (eg, socio-demographics), enabling factors (eg, access-related conditions that facilitate or hinder the use of health services), and need-related factors (eg, perceived or evaluated health needs) that motivate service use. We hypothesize that factors associated with beneficiaries’ HIV and HCV screening and PrEP prescription are similarly related to their predisposing factors (eg, age, sex), enabling factors (eg, rural residence), and need-related factors (eg, comorbidities). The SUDs included in study are alcohol, opioid, cocaine, cannabis, and other psychoactive drugs. Although there are differences in risk based on mode of intake, the intoxication of any of these substances is high risk for HIV and HCV.
Materials and Methods
Data Source and Sample
We conducted a retrospective cross-sectional analysis of administrative claims data merged with the enrollment files from an MCO located in southwestern Pennsylvania that provides coverage in 93% of the 67 counties. The merged data had information on beneficiaries’ health conditions, medication, health care utilization, and costs along with socio-demographics. The sample included beneficiaries who were enrolled in Medicaid or were dually eligible for Medicare and Medicaid with an SUD diagnosis, those who were 21 years or older without an HIV diagnosis. The study included only adult managed care beneficiaries and excluded pediatric population ages newborn to 20 years old. Ages under 21 years old are considered as pediatric population in Pennsylvania Medicaid. The beneficiaries included in the study were continuously enrolled for 12 months in an MCO between January and December of 2021 and accessed care at any of the three high volume primary care practices or four emergency departments (ED) of an academic medical system that had addiction medicine specialists. This time frame was chosen as the high-risk group included in this study are required to be screened at least once annually.5,6 The overall sample size was 2381 beneficiaries with SUD but without an HIV diagnosis.
Variables and Measurements
Rates of HIV and HCV screening, and PrEP prescriptions were examined. The outcome variables were measured as dichotomous variables – whether beneficiaries had an HIV screening (screened/not screened), HCV screening (screened/not screened), and PrEP prescription (yes/no). The PrEP prescriptions included in the analysis were descovy (emtricitabine and tenofovir alafenamide), truvada (emtricitabine and tenofovir disoproxil fumarate), and apretude (cabotegravir). Please see Table 1 for international classification of diseases (ICD)-10 codes, current procedural terminology (CPT) codes, and national drug code (NDC) for PrEP. Based on the Behavioral Model of Health Care Utilization, the predisposing factors included in the model were age, gender, and race/ethnicity. The enabling factors were primary language, rural/urban area of residence, and type of public insurance. The need-related factors included in the model were number of comorbidities, number of substances used, tobacco smoker status, number of providers seen, had a primary care physician (PCP) visit, number of ED visits, hospitalizations, and total cost of care during the year.
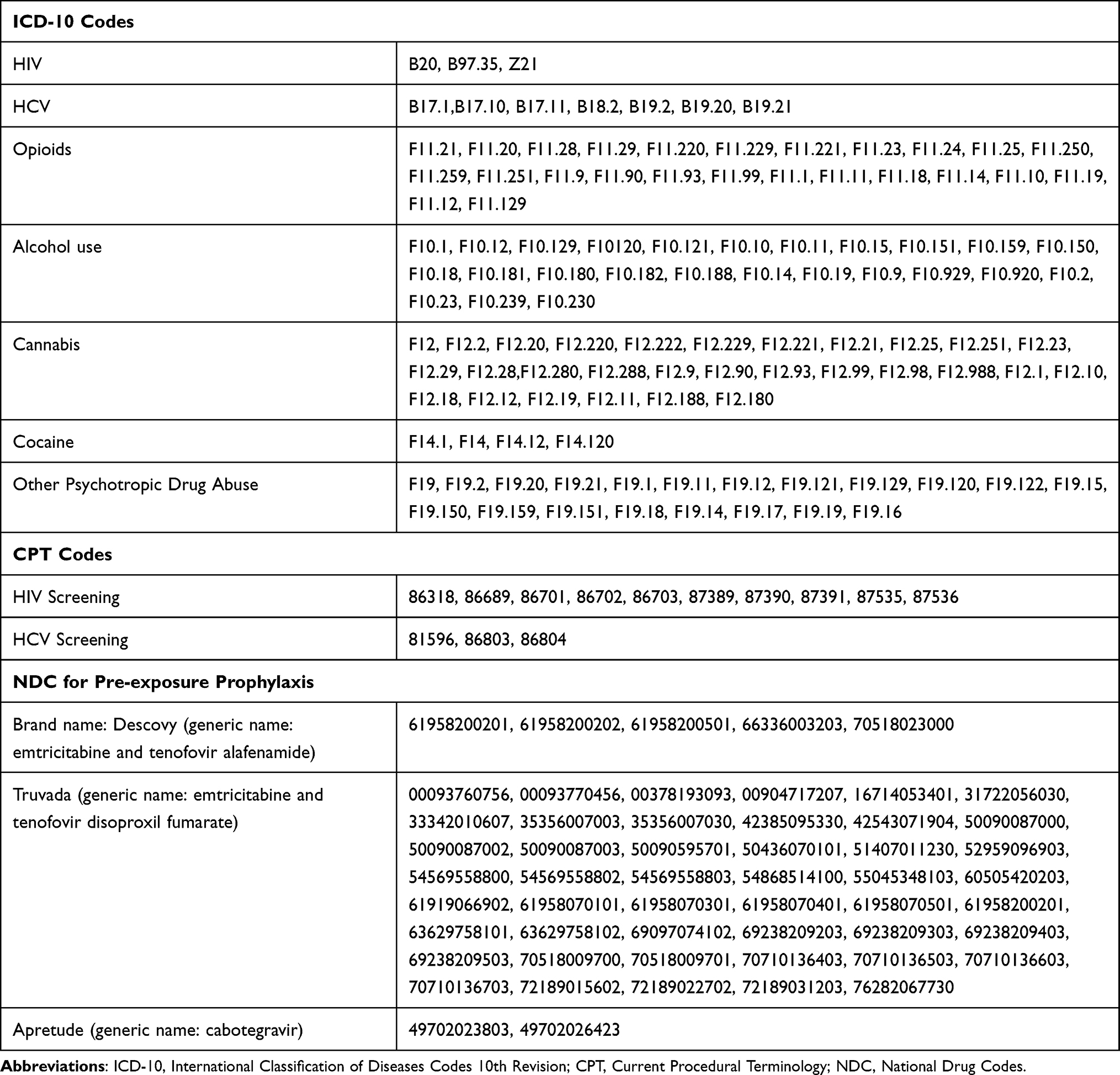 |
Table 1 Diagnosis, Procedural and Drug Codes Used in the Study for Substance Use Disorders, HIV and HCV Screenings and Pre-Exposure Prophylaxis Drug |
Age was categorized into three groups (ie, 21–44 years, 45–64 years, and ≥ 65 years). Both males and females were included in the analyses. Beneficiaries’ race/ethnicity was categorized as White, Black, Hispanic, and “other” racial/ethnic group. The “other” racial/ethnic group consists of Native Americans, Alaskan Natives, Asians, Pacific Islanders, and Hawaiian Natives. Primary language was categorized as English, Spanish, and others. Area of residence was categorized as rural and urban based on the definition from the Center for Rural Pennsylvania. Beneficiaries’ counties were classified as rural if its population density was fewer than 291 people per square mile; otherwise, it was considered urban.21 Beneficiaries enrolled in Medicaid and dually eligible for Medicare and Medicaid public health insurance were included. Co-morbid health conditions were identified by using ICD-10 codes. Co-morbidities included asthma, diabetes, obesity, coronary artery disease, stroke, chronic obstructive pulmonary disease, chronic kidney disease, cancer, hepatitis C, gonorrhea, syphilis, chlamydia, anxiety, depression, bipolar disorder, schizophrenia, and severe mental illness. The number of co-morbidities ranged from none to 17. Tobacco smoking behavior was measured as yes/no. Polysubstance use was categorized as beneficiaries on one substance and others who were on multiple substances (≥ 2). Number of unique providers seen was categorized as none, 1, 2, and ≥3. Although providers are careful in prescribing schedule I drugs, individuals with multiple providers are more likely to obtain concurrent prescription opioids.22,23 Beneficiaries’ PCP visits were defined as encounters with providers in family medicine and general internal medicine specialty working in the primary care settings. PCP visits were categorized as a binary variable (yes/no). Emergency Department visits were defined as any ED encounter that did not include an observation stay and did not result in hospitalization. Hospitalizations were defined as inpatient stays lasting 24 hours or longer. Both ED visits and hospitalizations were analyzed as count variables in the study. The total cost of care includes annual cost incurred on beneficiaries’ health care utilization and prescription drugs.
Statistical Analysis
Analyses included univariate statistics to examine HIV and HCV screening rates, PrEP prescription rates, and sociodemographic characteristics of the managed care beneficiaries. Multivariable logistic regression was used to examine the factors associated with HIV and HCV screening. Factors associated with PrEP prescription were not examined as we did not find any beneficiaries with the prescription in our data. We used IBM SPSS Statistics Version 30 for data management and analysis. The data accessed complied with data protection and privacy regulations. The Allegheny Health Network Research Institute Institutional Review Board (FWA # 000015120) reviewed the study and provided it with an exempt status for the project as it was deemed a quality improvement project. Quality improvement projects aim to improve performance of institutional practices in relation to an established standard and are considered an integral part of normal health care operations.
Results
Table 2 shows descriptive characteristics of the overall sample and by screening status of beneficiaries. The types of SUDs found in the overall sample were opioid (51.2%), cannabis (35.4%), alcohol (32.8%), other psychoactive drugs (10.6%), and cocaine (>1%). Polysubstance use was found among 23% of beneficiaries. Beneficiaries’ average age was 43 years. About 58% were females, 31% were Black, 15% resided in rural areas, and 83% had a PCP visit. More than half of those screened had opioid use disorder. Nearly three-fourth of the screened beneficiaries belonged to 21–44 years of age group and 82% of the beneficiaries who were not screened had seen a PCP (Table 2).
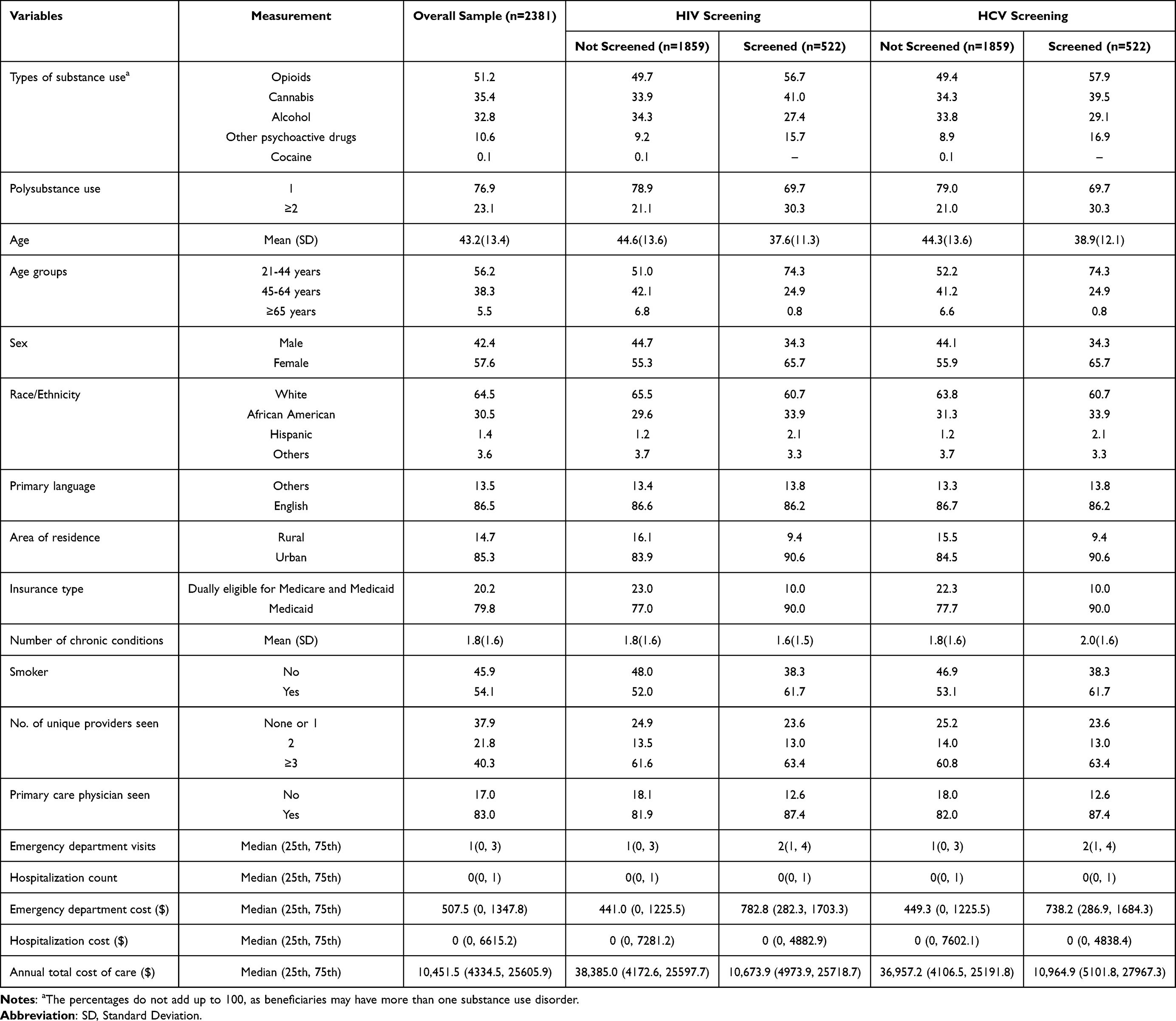 |
Table 2 Descriptive Characteristics of the Overall Sample and by Screening Status Among Managed Care Beneficiaries with Substance Use Disorders |
Prevalence of HIV and HCV screening were 22% (n=522) and none in our data had PrEP prescriptions. Results from multivariable logistic regression indicated females (AOR: 0.69; 95% CI: 0.56–0.86), rural beneficiaries (AOR: 0.57; 95% CI: 0.40–0.79), Medicaid enrollees (AOR: 0.67; 95% CI: 0.47–0.98), and beneficiaries with higher number of hospitalizations (AOR: 0.87; 95% CI: 0.78–0.97) were less likely to receive HIV screening compared with their comparators. Beneficiaries who had PCP visit (AOR: 2.00; 95% CI: 1.44–2.76), and those with higher number of ED visits (AOR: 1.03; 95% CI: 1.01–1.05) were more likely to receive HIV screening compared with their comparators (Figure 1).
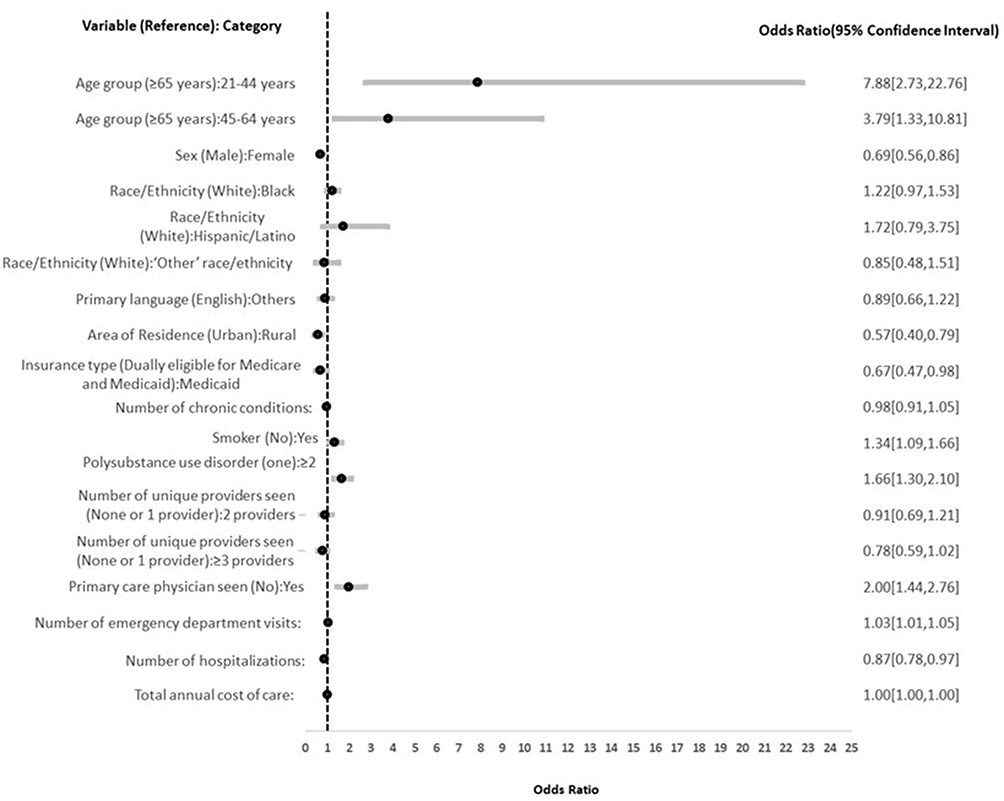 |
Figure 1 Results from Multivariable Logistic Regression Indicating Factors Associated with HIV Screening among Medicaid and Dually Eligible Managed Care Beneficiaries with Substance Use Disorders and Without a HIV diagnosis. |
Similar to the results from HIV screening, females (AOR: 0.75; 95% CI: 0.61–0.93) and rural beneficiaries (AOR: 0.68; 95% CI: 0.50–0.93) were less likely to receive HCV screening; while those who had a PCP visit (AOR: 1.71; 95% CI: 1.25–2.35), and with higher number of ED visits (AOR: 1.03; 95% CI: 1.02–1.06) were more likely to receive HCV screening compared with their comparators (Figure 2).
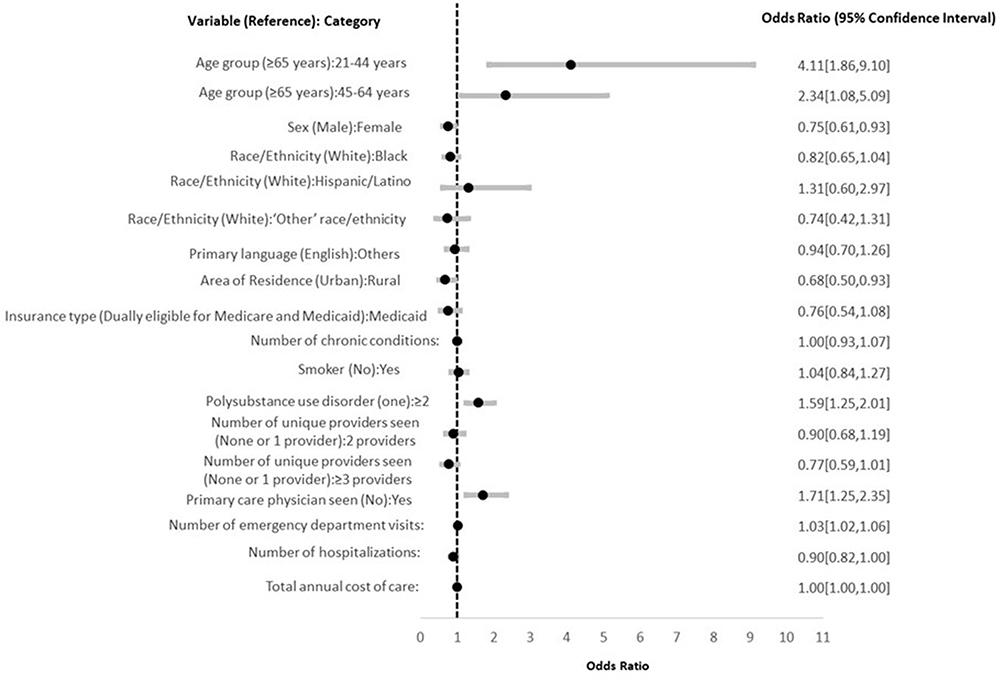 |
Figure 2 Results from Multivariable Logistic Regression Indicating Factors Associated with HCV Screening among Medicaid and Dually Eligible Managed Care Beneficiaries with Substance Use Disorders and Without a HIV diagnosis. |
Discussion
In this cross-sectional analysis, we found an increasing need for HIV and HCV screening and PrEP prescriptions among managed care beneficiaries with SUD and without an HIV diagnosis. One of the key findings from the study is that despite the clinical practice guidelines,5–7 HIV and HCV screening rates were low, and PrEP prescriptions were non-existent in our sample of beneficiaries with SUD. In addition, 17% of beneficiaries with SUD had an HCV diagnosis and about 23% had polysubstance use disorders which further underscores the need to improve HIV and HCV screening rates and PrEP prescriptions among beneficiaries with SUD. Similar to our results, very low PrEP prescription rates (0.1%) were found in a commercially insured population of persons with opioid and/or other SUD.24 The low HIV and HCV screening rates may be associated with the lack of availability of screening in SUD treatment facilities.9,25 In 2020, only half of the SUD treatment facilities in the US offered HIV and HCV screening.9 The lack of availability of an on-site laboratory may also contribute to SUD treatment facilities’ inability to screen individuals for HIV and HCV.25 Rapid testing assays for HIV and HCV screening has the potential to address the barriers faced by SUD treatment facilities as they do not need a laboratory and can be completed in 20 minutes, allowing testing and result notification in the same visit.25,26 In a randomized trial, on-site bundled rapid HIV and HCV screenings in SUD treatment facilities increased awareness of HIV and HCV infection among people with SUD.27
Second, although our results indicate beneficiaries who had higher number of ED visits or saw their PCP were more likely to be screened for HIV and HCV, the screening rates were low. We believe there exists missed opportunities at the provider level to offer the screenings and PrEP prescriptions. Studies have suggested lack of time, training, funding for testing, and capacity to treat or knowledge of referrals among providers as some of the reasons for not screening.28,29 Although the reasons for not prescribing PrEP are limited, we assume the USPSTF guidelines on PrEP prescriptions specifically identifies PWID and those with high-risk sexual behavior, and not persons with drug use who are not PWID.5 This may be a contributing factor for limited PrEP prescription by health care providers. Future studies should focus on providers’ perspectives on barriers and facilitators to PrEP prescription. Further, HIV infection spread among persons with drug use who are not PWID is overlooked.30–32 Although PWID continue to account for majority of HIV infections, studies have observed infection rates to be similar among persons with drug use who are PWID and not-PWID.30–32 Explanations for this include mixing of the two populations, sharing pipes, and inhalers to use drugs, and high-risk sexual behavior between PWID and persons with drug use who are not PWID.31 Hence, PWID and persons with drug use who are not PWID should be equally targeted for HIV and HCV screening and PrEP prescription. Moreover, it is imperative to bundle HIV and HCV screening services and offer opt out testing policy at SUD treatment facilities to reduce stigma surrounding HIV, and to ensure early screening, diagnosis, and linkage to care for both conditions.25,33 The opt out approach for HIV and HCV screenings in an ED setting allowed for stigma-free screenings.34 Evidence from a syringe service program showed bundled HIV and HCV testing increased screening rates by 42% after implementation of an opt out testing policy.35 Some of the facilitators for HIV and HCV screening are implementing standardized written protocols, bundled on-site testing, and identification of a testing champion in health care settings.33
Third, we observed disparities in screenings by beneficiaries’ area of residence, gender, and type of public health insurance. Beneficiaries residing in rural areas lack treatment availability and linkage to care and often travel to urban clinics to obtain care. About 15% of the beneficiaries who accessed care at our study clinics and EDs had rural residence, and we found that rural beneficiaries were less likely to be screened for HIV and HCV compared with their urban comparators. Although, our analysis indicated (not shown here) that a higher percentage of rural beneficiaries (87%) had a PCP visit than urban beneficiaries (82.4%), reasons for disparities in screenings by area of residence are unknown. We also observed that women were less likely to receive HIV and HCV screenings than men. This is in contrary to the expectation that women have higher health care services utilization.36,37 One of the explanations might be stigma associated with the screenings or lower risk perception.38 The opt out screening approach reduces stigma associated with the screenings. When routine opt out screenings were provided in health care settings (hospital outpatient clinics, EDs, and inpatient services and community health centers) more women received screenings than men.38 Further, Medicaid beneficiaries were less likely to be screened than dually eligible beneficiaries. A 2016–2019 study of Medicaid beneficiaries with opioid use disorder from 11 US states indicated that although the screenings increased over the three years from 20% to 25% for HIV and 22% to 27% for HCV, yet the majority were not tested.39 In addition, lower risk perception, lack of continuity of care, and provider bias may be other factors that may influence lower screenings among beneficiaries.40,41 Stigma exists among health care providers towards individuals with specific health conditions such as SUD and HIV, and the degree of stigma varies based on membership in marginalized groups, which contributes to lack of HIV and HCV screening in these populations.41,42 Future studies should address stigma among healthcare providers to improve patient engagement and retention in care.41 We also observed that beneficiaries with higher number of hospitalizations were less likely to get HIV screening; however, association between hospitalizations and HCV screenings were not significant. Hospital stays may be an ideal opportunity to screen and establish linkage to outpatient care for beneficiaries high-risk for HIV and HCV.43
Limitations
Our study has certain limitations. First, in our sample of beneficiaries with SUD, we did not have information on their sexual orientation, gender identity, and injection drug usage. As studies show that prevalence of HIV and HCV is higher in these sub-populations,44,45 and excluding these variables in our analytical model may have biased the results. Second, we did not account for counts of PCP visits and provider specialty in the analysis. Differences may exist between beneficiaries who had one PCP visit versus those with repeated visits and by provider specialty. Third, in Pennsylvania, Medicaid, behavioral health benefits are carved out. The beneficiaries in our sample are from a physical health MCO. The lack of data on beneficiaries’ behavioral health care utilization may have underestimated our results on the screenings. Fourth, the study was conducted using data from a single MCO in one U.S. state, therefore the findings may not be generalizable to Medicaid or dually eligible managed care populations in other states. Fifth, PrEP prescription uptake is slow. The cross-sectional design of the study limits us to capture the prescriptions in this sample beyond the study year. Sixth, beneficiaries may have received screenings from public health department or other facilities not in network with the MCO. Hence, our screening rates may be underreported.
Conclusions
The low HIV and HCV screening rates and no PrEP prescription indicate the need for targeted interventions in our sample of Medicaid and dually eligible for Medicare and Medicaid managed care beneficiaries with SUD. Specifically, rural beneficiaries, females, and Medicaid beneficiaries attending urban clinics and ED of the health care system need attention. Missed opportunities exist at PCP offices to screen high-risk beneficiaries for both HIV and HCV. Strategies to improve screening rates and PrEP prescription include opt out bundled HIV and HCV screening in PCP offices, use of mobile medical vans, provider- and member- level education, and value-based contracting models. Future studies should examine the above strategies for their effectiveness in improving the screening rates and PrEP prescription. The study also has implications for national guidelines to work towards encouraging screenings and PrEP prescription in people with SUDs who are not injection drug users.
Acknowledgment
The study was presented at the 2023 American College of Preventive Medicine Annual Meeting, New Orleans March 20-23.
Disclosure
Shamly Austin, Yuan Zhang, Michael Madden, and Anita Edwards are employees of Highmark Wholecare, a Managed Care Organization where the study was conducted. The authors report no other conflicts of interest in this work.
References
1. U.S. Department of Health & Human Services. Highlights for the 2023 national survey on drug use and health. Available from: https://www.samhsa.gov/data/sites/default/files/NSDUH%202023%20Annual%20Release/2023-nsduh-main-highlights.pdf.
2. NIH Office of AIDS Research. HIV and substance use. Available from: https://hivinfo.nih.gov/understanding-hiv/fact-sheets/hiv-and-substance-use.
3. Centers for Disease Control and Prevention. HIV testing, treatment, prevention not reaching enough Americans. Available from: https://archive.cdc.gov/www_cdc_gov/media/releases/2019/p1203-hiv-testing-treatment-prevention.html.
4. U.S. Department of Health & Human Services. Hepatitis C basic information. Available from: https://www.hhs.gov/hepatitis/learn-about-viral-hepatitis/hepatitis-c-basics/index.html.
5. Owens DK, Davidson KW, Krist AH, et al. Screening for HIV infection: US preventive services task force recommendation statement. JAMA. 2019;321(23):2326–2336. doi:10.1001/jama.2019.6587
6. Owens DK, Davidson KW, Krist AH, et al. Screening for hepatitis C virus infection in adolescents and adults: US preventive services task force recommendation statement. JAMA. 2020;323(10):970–975. doi:10.1001/jama.2020.1123
7. Owens DK, Davidson KW, Krist AH, et al. PreExposure Prophylaxis for the prevention of HIV infection: US Preventive Services Task Force recommendation statement. JAMA. 2019;321(22):2203–2213. doi:10.1001/jama.2019.6390
8. NIH Office of AIDS Research. Pre-exposure prophylaxis (PrEP). Available from: https://hivinfo.nih.gov/understanding-hiv/fact-sheets/pre-exposure-prophylaxis-prep.
9. Patel EU, Genberg BL, Zhu X, Krawczyk N, Mehta SH, Tobian AAR. HIV and hepatitis C virus testing and treatment services in specialty treatment facilities that offer medication for opioid use disorder in the US. JAMA. 2022;327(8):776–778. doi:10.1001/jama.2022.0293
10. McCoy K, Mantell JE, Deiss R, et al. PreP awareness and demand creation: overlooked populations and opportunities to move forward. J Acquir Immune Defic Syndr. 2025;98(5S):e170–e180. doi:10.1097/QAI.0000000000003626
11. Dawson L, Kates J, Roberts T, Chidambaram P. Medicaid and people with HIV. Available from: https://www.kff.org/hivaids/issue-brief/medicaid-and-people-with-hiv/.
12. Saunders H. A look at substance use disorders (SUD) among Medicaid enrollees. Available from: https://www.kff.org/medicaid/issue-brief/a-look-at-substance-use-disorders-sud-among-medicaid-enrollees/.
13. Hinton E, Raphael J. 10 things to know about medicaid managed care. Available from: https://www.kff.org/medicaid/issue-brief/10-things-to-know-about-medicaid-managed-care/.
14. Kaiser Family Foundation. Medicaid coverage of HIV testing and PrEP. Available from: https://www.kff.org/hivaids/state-indicator/hiv-testing/.
15. Pennsylvania Department of Health. Insurance department highlights importance of HIV PrEP medication for HIV prevention, coverage under the affordable care. Available from: https://pacast.com/m?p=22398.
16. Pennsylvania Department of Health. Pennsylvania medical assistance removes prior authorization requirement for preferred hepatitis C virus (HCV) direct acting antivirals. Available from: https://www.health.pa.gov/topics/Documents/HAN/2023-710-07-26-ADV-HepC.pdf.
17. Miller MH, Dillon JF. Early diagnosis improves outcomes in hepatitis C. Practitioner. 2015;259(1787):25–27.
18. National Institute of Allergy and Infectious Diseases (NIAID). Early HIV diagnosis and treatment important for better long-term health outcomes. Available from: https://www.nih.gov/news-events/news-releases/early-hiv-diagnosis-treatment-important-better-long-term-health-outcomes.
19. Aday LA, Andersen RM. Models of Health Care Utilization and Behavior.
20. Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav. 1995;36(1):1–10.
21. The Center for Rural Pennsylvania. Rural urban definitions. Available from: http://www.rural.palegislature.us/demographics_rural_urban.html.
22. Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC clinical practice guideline for prescribing opioids for pain - United States, 2022. MMWR Recomm Rep. 2022;7:1–95.
23. Jena AB, Goldman D, Weaver L, Karaca-Mandic P. Opioid prescribing by multiple providers in medicare: retrospective observational study of insurance claims. BMJ. 2014;348:g1393. doi:10.1136/bmj.g1393
24. Streed CG, Morgan JR, Gai MJ, Larochelle MR, Paasche-Orlow MK, Taylor JL. Prevalence of HIV PreExposure prophylaxis prescribing among persons with commercial insurance and likely injection drug use. JAMA. 2022;5:e2221346.
25. Frimpong JA, D’Aunno T, Perlman DC, et al. On-site bundled rapid HIV/HCV testing in substance use disorder treatment programs: study protocol for a hybrid design randomized controlled trial. Trials. 2016;17(1):117. doi:10.1186/s13063-016-1225-4
26. Assoumou SA, Paniagua SM, Linas BP, et al. Rapid versus laboratory-based testing for HIV and hepatitis C at a drug detoxification treatment center: a randomized trial. J Infect Dis. 2020;222(Supplement_5):S376–S383. doi:10.1093/infdis/jiaa162
27. Frimpong JA, Shiu-Yee K, Tross S, et al. Bundling rapid human immunodeficiency virus and hepatitis C virus testing to increase receipt of test results: a randomized trial. Med Care. 2020;58(5):445–452. doi:10.1097/MLR.0000000000001311
28. D’Aunno T, Pollack HA, Jiang L, Metsch LR, Friedmann PD. HIV testing in the Nation’s opioid treatment programs, 2005–2011: the role of state regulations. Health Serv Res. 2014;49(1):230–248. doi:10.1111/1475-6773.12094
29. Hernández D, Feaster DJ, Gooden L, et al. Self-reported HIV and HCV screening rates and serostatus among substance abuse treatment patients. AIDS Behav. 2016;20(1):204–214. doi:10.1007/s10461-015-1074-2
30. Strathdee SA, Sherman SG. The role of sexual transmission of HIV infection among injection and non-injection drug users. J Urban Health. 2003;80(90003):iii7–iii14. doi:10.1093/jurban/jtg078
31. Strathdee SA, Stockman JK. Epidemiology of HIV among injecting and non-injecting drug users: current trends and implications for interventions. Curr HIV/AIDS Rep. 2010;7(2):99–106. doi:10.1007/s11904-010-0043-7
32. Des Jarlais DC, Arasteh K, Perlis T, et al. Convergence of HIV seroprevalence among injecting and non-injecting drug users in New York City. AIDS. 2007;21(2):231–235. doi:10.1097/QAD.0b013e3280114a15
33. Brooks R, Wegener M, Freeman B, et al. Improving HIV and HCV testing in substance use disorder programs (SUDs) that provide medications for opiate use disorder (MOUD): role of addressing barriers and implementing universal and site-specific approaches. Health Promot Pract. 2023;24(5):1018–1028. doi:10.1177/15248399231169791
34. Lyon C. Routine opt-out screening is key to understanding and identifying HIV/HCV incidence. J Healthc Sci Humanit. 2021;11:101–106.
35. Bartholomew TS, Tookes HE, Serota DP, Behrends CN, Forrest DW, Feaster DJ. Impact of routine opt-out HIV/HCV screening on testing uptake at a syringe services program: an interrupted time series analysis. Int J Drug Policy. 2020;84:102875. doi:10.1016/j.drugpo.2020.102875
36. Bertakis KD, Azari R, Helms LJ, Callahan EJ, Robbins JA. Gender differences in the utilization of health care services. J Fam Pract. 2000;49(2):147–152.
37. Lassman D, Hartman M, Washington B, Andrews K, Catlin A. US health spending trends by age and gender: selected years 2002-10. Health Aff. 2014;33(5):815–822. doi:10.1377/hlthaff.2013.1224
38. Almirol EA, McNulty MC, Schmitt J, et al. Gender differences in HIV testing, diagnosis, and linkage to care in healthcare settings: identifying African American women with HIV in Chicago. AIDS Patient Care STDs. 2018;32(10):399–407. doi:10.1089/apc.2018.0066
39. Ahrens K, Sharbaugh M, Jarlenski MP, et al. Prevalence of testing for human immunodeficiency virus, hepatitis B virus, and hepatitis C virus among Medicaid enrollees treated with medications for opioid use disorder in 11 states, 2016-2019. Clin Infect Dis. 2023;76(10):1793–1801. doi:10.1093/cid/ciac981
40. Schafer KR, Albrecht H, Dillingham R, et al. The continuum of HIV care in rural communities in the United States and Canada: what is known and future research directions. J Acquir Immune Defic Syndr. 2017;75(1):35–44. doi:10.1097/QAI.0000000000001329
41. Surratt HL, Otachi JK, McLouth CJ, Vundi N. Healthcare stigma and HIV risk among rural people who inject drugs. Drug Alcohol Depend. 2021;226:108878. doi:10.1016/j.drugalcdep.2021.108878
42. Madden EF. Intervention stigma: how medication-assisted treatment marginalizes patients and providers. Soc Sci Med. 2019;232:324–331. doi:10.1016/j.socscimed.2019.05.027
43. Nurutdinova D, Ramachandran S, Kadam S, Mojica V, Mullen M, Baney M. Linkage to HIV outpatient care following an inpatient stay. Open Forum Infect Dis. 2017;4(suppl_1):S419. doi:10.1093/ofid/ofx163.1050
44. Kerridge BT, Pickering RP, Saha TD, et al. Prevalence, sociodemographic correlates and DSM-5 substance use disorders and other psychiatric disorders among sexual minorities in the United States. Drug Alcohol Depend. 2017;170:82–92. doi:10.1016/j.drugalcdep.2016.10.038
45. National Survey on Drug Use and Health. Lesbian, gay, and bisexual behavioral health: results from the 2021 and 2022 national surveys on drug use and health. Available from: https://www.drugsandalcohol.ie/38998/1/LGB_Brief_Final_06_07_23.pdf.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluating the Effect of COVID-19 on Outpatient Opioid Utilization Among Health First Colorado Members and a National Non-Medicaid Cohort: An Interrupted Time Series Analysis
Anderson HD, Patterson VP, Wright G, Rawlings JE, Moore GD, Leonard J, Page RL II
Therapeutics and Clinical Risk Management 2023, 19:745-753
Published Date: 18 September 2023