")
Back to Journals » Substance Abuse and Rehabilitation » Volume 13
History of Delirium Tremens in AUD Patients in Treatment: Relationship to AUD Severity and Other Factors
Authors Bramness JG , Pandey S , Moe JS, Toft H , Lien L, Bolstad I
Received 23 February 2022
Accepted for publication 22 August 2022
Published 13 September 2022 Volume 2022:13 Pages 65—72
DOI https://doi.org/10.2147/SAR.S361810
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Justinn Cochran
Jørgen G Bramness,1– 3 Susmita Pandey,1 Jenny Skumsnes Moe,1,3 Helge Toft,1,4 Lars Lien,1,4 Ingeborg Bolstad1,4
1Norwegian National Advisory Unit on Concurrent Substance Abuse and Mental Health Disorders, Innlandet Hospital Trust, Brumunddal, Norway; 2Norwegian Institute of Public Health, Department of Alcohol, Tobacco and Drugs, Oslo, Norway; 3Institute Clinical of Medicine, UiT – The Arctic University of Norway, Tromsø, Norway; 4Department of Health Studies, Inland Norway University of Applied Sciences, Elverum, Norway
Correspondence: Jørgen G Bramness, Norwegian Institute of Public Health, P.O.Box 222, Oslo, 0213, Norway, Email [email protected]
Introduction: Delirium tremens (DT) occurs after stopping prolonged, high alcohol intake and may be life-threatening if untreated. We need to know about clinical correlates of DT in order to provide the best clinical care.
Methods: At admission to inpatient treatment a cohort of 114 alcohol use disorder (AUD) patients were interviewed and examined concerning psychiatric diagnosis and symptoms, trauma experiences and alcohol related measures and if they had experienced DT.
Results: Twenty-four percent of the patients reported a life-time experience of DT. These patients were predominantly males and had lower educational level. More of the patients in the DT than the non-DT group reported at least one suicide attempt, were diagnosed with PTSD, and dropped out of treatment. Also, having parents with alcohol problems was more common among these patients, and they reported a longer duration of problematic drinking and a higher number of drinks needed to feel an effect of drinking. In the multivariable adjusted analysis only a diagnosis of PTSD (OR=5.71; 95% confidence interval (CI): 1.34– 24.31) and duration of problematic drinking with a 6% increase in risk for every year (OR=1.06; 95% CI: 1.01– 1.11) remained significant risk factors for having DT experience.
Discussion and conclusion: Having experienced DT was more prevalent in the current investigation than in earlier studies. Patients that had experienced DT seemed to have more serious AUD, especially signified by a longer duration of drinking. These patients seemed to have many clinical disadvantages including more drop-out and higher suicide rate. PTSD could be a risk factor for DT but may also follow the DT experience.
Keywords: alcohol use disorder, delirium tremens, treatment, PTSD
Introduction
Delirium tremens (DT) is a life-threatening condition directly caused by cessation of particularly high and prolonged alcohol consumption. It occurs most often in people with alcohol use disorder (AUD), with prevalence estimates ranging from 5 to 12%.1–4 Untreated, DT has a mortality rate of up to 35%,5 while correct treatment can reduce mortality to close to zero.6
Biologically, DT can be viewed as an organic withdrawal psychosis, occurring 2–4 days after last alcohol intake.7 Chronic alcohol consumption most probably influences GABA-receptors and causes an imbalance between inhibitory GABAergic signaling and excitatory glutamatergic signaling.8 GABAergic activity may be downregulated while glutamate activity is upregulated. When alcohol use is stopped, a new imbalance with glutamatergic upregulation and hyperexcitability may occur. This leads to hyperactivation of the autonomic nervous system, alterations in sleep/wake regulation and alterations to the limbic system.9 Clinically, early signs of DT are similar to alcohol withdrawal syndrome, which manifests as sweating, hypertension, tachycardia, tremor, insomnia and anxiety.9,10 If inadequately treated, DT can manifest as a state of confusion with predominantly complex visual hallucinations, risk of cardiac arrhythmias and generalized seizures.9,11 Treatment aims to increase the inhibitory GABAergic activity by means of high doses of benzodiazepines, in addition to rehydration and vitamin supplements and in some cases barbiturates, beta-blockers, antipsychotics, or antiepileptic drugs.12 The condition should be monitored, and treatment guided using the validated Clinical Institute Withdrawal Assessment for Alcohol (CIWA-A).7,13
Early detection of signs of alcohol withdrawal is crucial for prevention of DT. In addition to the clinical presentation, presence of other risk factors can facilitate early treatment. Heavy alcohol use constitutes a risk factor for DT, and higher prevalence estimates have been found in samples with higher severity of dependence.7 In the acute setting, other anamnestic risk factors for DT include a history of detoxification, prior history of seizures, presence of concurrent illness, older age, and social marginalization.10,14–16 Clinical risk factors include signs of withdrawal, reduced platelet count, reduced serum potassium and structural brain lesions.10 There is however little existing research on other characteristics of people who have experienced DT, particularly from the recent decade. Research that has been conducted, indicate increased mortality among people who have experienced DT, and in particular worsening prognosis with repeated DT episodes. These negative outcomes, maybe except for cognitive impairment, have however in some studies been explained by other underlying factors,17–19 but these studies have been conducted in intensive care unit patients and patients with dementia. Thus, knowledge about DT survivors is still limited, and there is still a need to identify clinical characteristics of these patients in order to promote health and facilitate treatment.
The present study explores factors related to history of DT among patients in long-term inpatient AUD treatment. The aim of the study was to investigate aspects of background and current mental health condition in patients with a history of DT compared to those without.
Materials and Methods
Study Participants
Data were collected in three rehabilitation clinics in the Eastern region of Norway from January 2018 to August 2019. The material has been described in a previous publication.20 The clinics offer long-term residential treatment stays (>30 days) for people with substance use disorders (SUD), where the majority have a diagnosis of AUD. People were considered for inclusion in the study if they were not in an unsuitable condition to participate in the study, as assessed by the clinical staff, due to severe somatic illness, psychosis, cognitive impairment, or inability to speak a Scandinavian language. Of the 366 patients who were admitted to treatment in the clinics during our inclusion period, 224 (61%) were considered eligible for participation in this study. Only patients who had current AUD as diagnosed according to International Classification of Diseases 10th Revision (ICD-10) were eligible participants for the current study of which 114 (51%) signed informed written consent and were enrolled in the study. At baseline data collection the patients had been in treatment for a median 7 days (1st, 3rd quartile: Interquartile range, (IQR): 5–12 days) and reported abstinence from alcohol during the last 19 (IQR 12–30) days. Patients who discontinued the treatment program and left the clinic before planned discharge were regarded as dropped out as opposed to patients who completed their stay or were still in treatment at six months follow-up. The study was approved by the Norwegian Regional Ethics Committee and complied with the Helsinki declaration before data collection commenced (ID no: 21505/2017/1314).
Measures
Baseline data collection consisted of an interview, clinical examination, and administration of psychometric questionnaires. Selected modules of the Mini International Neuropsychiatric Interview (M.I.N.I.) version 6.0 were conducted by trained staff, while all other information was collected using self-report forms. The interview and self-report forms were administered at the clinics where the patients were staying. For the current study we included data on sex, age, and level of education. Level of education for this study was dichotomized into those with university degree (bachelor or master) or not.
Mental Health Measures
The M.I.N.I. was used to diagnose AUD, as well as lifetime depressive disorder and post-traumatic stress disorder (PTSD).
The level of depressive symptoms was measured using the Beck depression Inventory 2 (BDI-II).21,22 This self-report questionnaire consists of 21 questions asking the respondents how they have been feeling the preceding two weeks, with responses given on a 4-point Likert scale. Responses are summed up into a total score ranging from 0–63, where higher score indicates higher level of depressive symptoms. Patients were also asked if they ever had attempted suicide.
Exposure to trauma was measured using a structured self-report form with five questions which have been previously used in a study of psychiatric inpatients.23 The first three questions asked whether the person had experienced the following in his or her childhood: sexual assaults (1), physical abuse (2) and other traumatic event that has subsequently caused significant problems (3). The last two questions dealt with experiences in adulthood: sexual assault or physical abuse (4) and other traumatic event that has subsequently caused significant problems (5). For each item, the response alternatives were: 0) “No”, 1) “Yes, once” or 2) “Yes, several times”. Dichotomous variables (“No”/”Yes”, once or several times”) for childhood and adulthood trauma, respectively, were constructed. The patients were advised that they could speak to a psychologist at the clinic in case the questions evoked negative emotions.
Sleep Measure
Subjective sleep quality was measured by the Sleep Condition Indicator (SCI).24 The SCI consists of 8 items with response alternatives ranging from 0 to 4, where 0 indicates a poor state, whereas 4 indicates no/little problems giving a range of sum scores from 0–32 where higher score indicates better sleep. A cut-off of 16 had been set, below which a sleep problem is considered to be present.
Alcohol Related Measures
Severity of alcohol dependence was examined using the Severity of Dependence Scale (SDS). The SDS was originally constructed to measure dependency on illicit drugs,25 but has later shown to also be a reliable and valid measure of alcohol dependence.26 It consists of five items that target subjective aspects of dependence during the preceding year, such as “Did you think your alcohol use was out of control?” and “Did you wish you could stop drinking?” The response alternatives range from 0) “Never” to 3) “Always” for each question. The responses are summed up into a total score ranging from 0–15, where higher score indicates more severe dependence.
Subjective effects of alcohol were measured at baseline by the instrument Self-Rating of the Effects of alcohol (SRE), a twelve item questionnaire asking how many units a person had to drink to feel any effect, produce dizziness or slurred speech, be associated with a stumbling gait or to had fallen asleep at three points in time.27 These times are when first starting to drink (SRE early), during the last period when drinking at least once a month (SRE lately) and in periods of heavy drinking (SRE heavy). A SRE score was generated by summing the number of drinks required for each effect and dividing it by the number of reported effects for each of the three times indicated, resulting in three composite scores “SRE early”, “SRE heavy” or “SRE lately”.27,28
Patients were further asked if they had experienced parental drinking problems, their age of alcohol debut, their estimated duration of problematic drinking and if they had experienced DT, and if so, how many times. For the present study we divided the patient group into those who had or had not experienced DT.
Missing Data
For some analyses (life-time suicide attempt, PTSD, parental drinking problems, age of first drink, duration of problematic drinking) there were no missing data. For some variables, the persons with missing data were excluded. These were (number of total N included in parenthesis): educational level (N=87), life-time depressive disorder (N=112), childhood trauma (N=86), and adult trauma (N=86), and SDS (N=87). For some data imputations of missing values were done. For BDI-II mean values from the answered questions were imputed if 17 or more of the 21 questions were answered (N=67). For SCI mean values from the answered questions were imputed if 6 or more of the 8 questions were answered (N=83). For SRE mean values from the answered questions were imputed if 3 or more of the 4 questions were answered (N=66).
Statistical Analyses
Bivariate analyses were used to assess the relationship between those who had or had not experienced DT. Chi-squared tests or Fisher’s exact tests were used to compare categorical variables, while Mann–Whitney U tests were used to compare continuous variables due to the data being non-normally distributed. For multivariable analysis binary logistic regression was employed to assess associations between various predictors and experience of DT. The variables that were found to be related to DT were adjusted for the relevant background variables. Exact p-values were given, but p-values below 0.050 were considered significant. SPSS version 23.0 for Windows was used to perform the statistical analyses.
Results
Of the 114 AUD patients, 27 (24%) had experienced DT. Median time of occurrence was 3 years before admission, ranging from 25 years to less than one year before admission.
The patients who had experienced DT were predominantly men and less often had university education (Table 1). There was no age difference between the DT and non-DT patients. There were no differences in the current depressive symptom level (BDI-II) nor life-time depression, but the occurrence of history of suicide attempt was higher among DT patients (44 vs 22%; p=0.023). Further, PTSD was more common among DT patients (33 vs 12%; p=0.016) while there was no difference in reported experience of traumatic event between the groups. DT patients did not differ from the other patients concerning sleep quality. Analysis indicated that DT patients were more likely to drop out of treatment during the first 6 weeks (46 vs 26%; p=0.050).
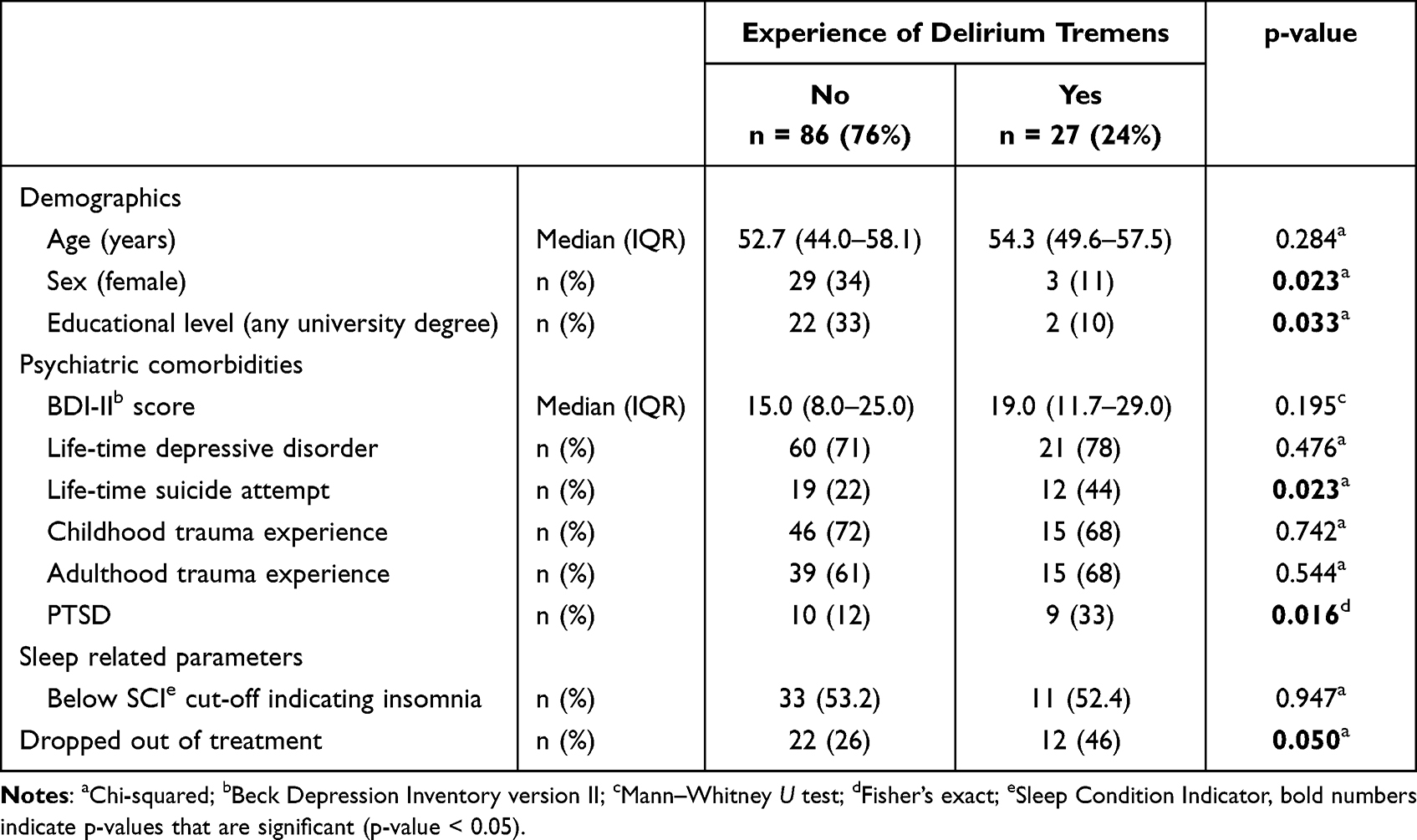 |
Table 1 Background Characteristics, Health Related Measures and Psychological Measures for AUD Patients That Had or Had Not Experienced Delirium Tremens |
Having parents with alcohol problems was more common among DT patients (70 vs 49%; p=0.050) (Table 2). They reported lower age of drinking initiation (p=0.046) and longer duration of problematic drinking (22 vs 11 years; p<0.001). The DT patients reported a higher SRE score both during heavy drinking periods (p=0.025) and recent drinking episodes (p=0.006), but the groups did not differ in their score on SDS. Supplementary analysis showed that males, and at a trend level, participants with lower education reported longer duration of problematic drinking (p=0.001 and p=0.079, respectively) and higher number of drinks required to feel intoxicated during heavy drinking episodes (p=0.026 and p=0.007, respectively) (data not shown in table). Furthermore, across all patients, duration of problematic drinking was correlated to SDS (Spearman’s rho=0.304, p=0.004).
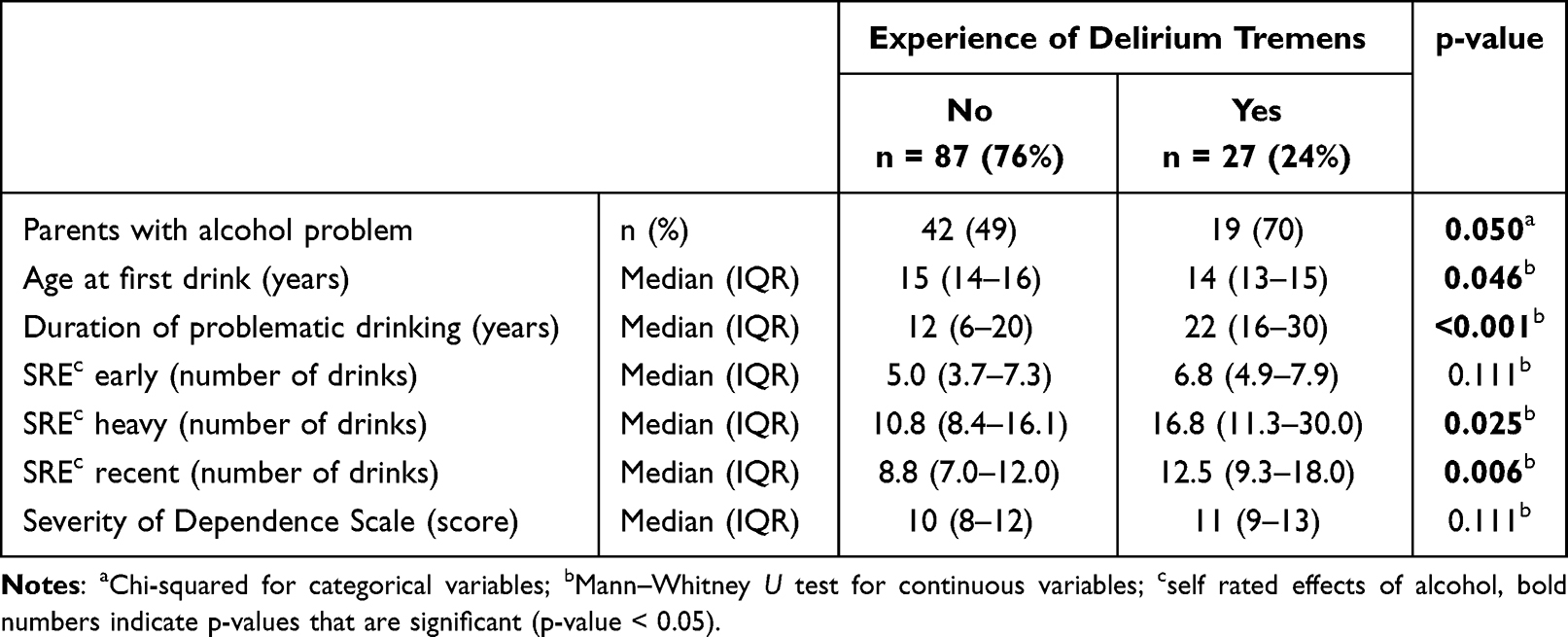 |
Table 2 Alcohol Related Measures of the AUD Patients That Had or Had Not Experienced Delirium Tremens |
In the multivariable analysis (Table 3) we adjusted the clinical measures for the two background variables related to DT: sex and educational level. Patients with PTSD more often reported having experienced DT (OR 5.71; 95% CI 1.34–24.31). There was also a relationship between DT and drinking duration (1.06; 1.01–1.11), indicating a 6% increase in risk of having experienced DT for every extra year of drinking.
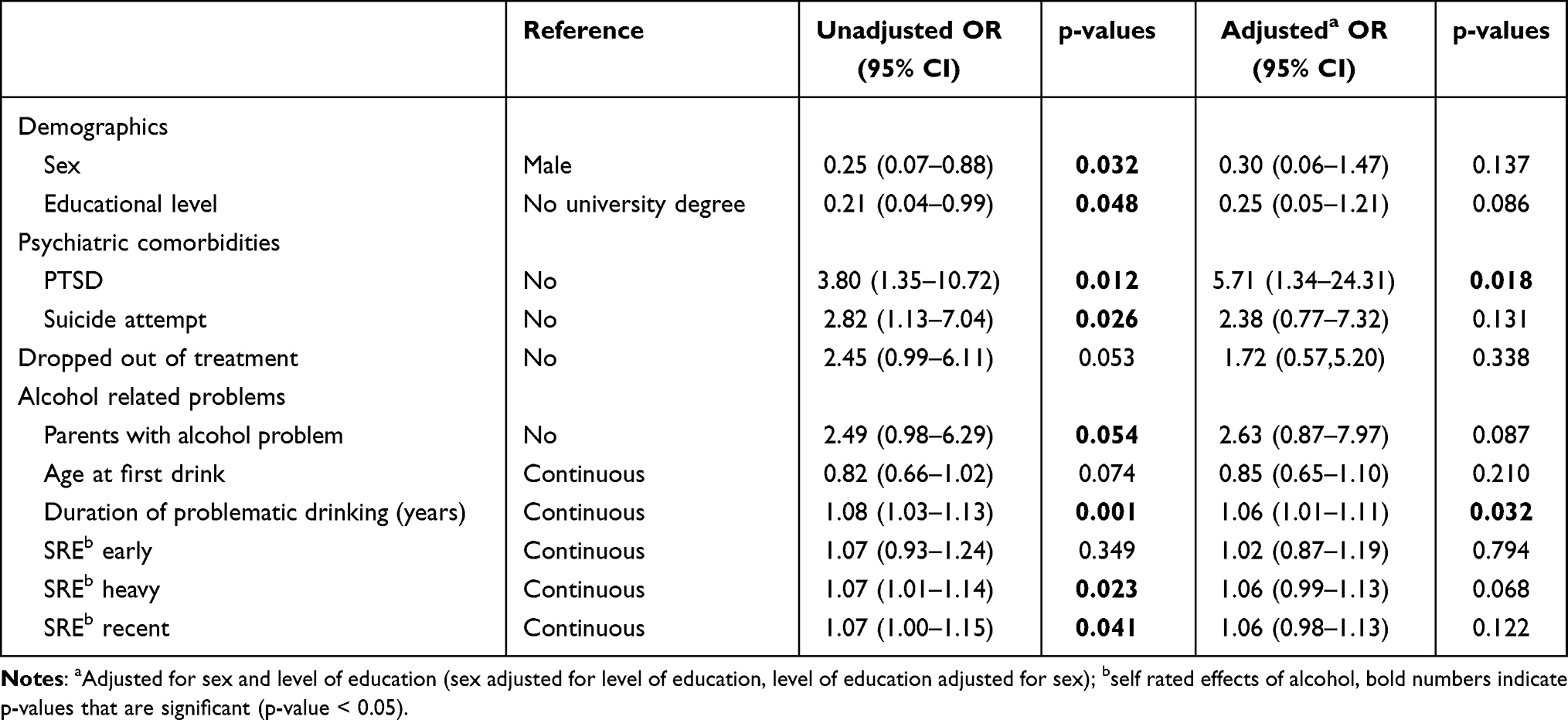 |
Table 3 Logistic Regression of Variables Related to Delirium Tremens Among the Treated AUD Patients in the Study (N=114) |
Discussion
In the present study we found that one in four AUD patients in treatment had experienced delirium tremens (DT). Among males and among those with lower education there were more patients who had experienced DT. Several other factors seemed to be related to DT (lifetime suicide attempt, dropping out of treatment, parental drinking problems, subjective effects of alcohol, duration of problematic drinking and having PTSD), but only duration of problematic drinking and having PTSD remained associated with DT in adjusted analyses.
As many as 24% of the patients in the study reported having experienced DT, higher than shown in previous studies reporting from 5 to 12%.2–4,29 It has been estimated that treatment for AUD in Norway only captures about 5–7% of those with AUD30 and it is reasonable to believe that people in treatment have the most severe conditions with a higher severity of dependence and thus a higher prevalence of DT could be observed.7 Regardless, this high prevalence among in-patients is important clinical information as history of DT is a risk factor for subsequent DT.31
There were more male patients and patients with low educational level that had experienced DT. This is in line with previous studies showing that males are more at risk for DT, maybe due to more intense drinking.32 Other studies correcting for level of drinking fail to find a sex effect.7 Also in the present study, low educational level and male sex may be less important than other clinical features as these background variables were related to duration of problematic drinking and self-reported effects of alcohol.
The relationship between DT and severity of AUD is further underlined by the observed relationship between DT and duration of problematic drinking. Longer experience of heavy drinking means longer exposure time, which could also represent an indirect measure of severity of drinking. In bivariate analyses, duration of problematic drinking was indeed related to severity of dependence (SDS). In other bivariate analyses both parental drinking and how much alcohol the person could take (SRE) were also related to DT, indicating that patients with more severe AUD were most at risk of DT.7 In the present study patients with DT experience reported 12–16 units of alcohol being required to produce an effect, which is lower than the 20 units reported among DT in a Danish study,32 possibly related to higher population-level of alcohol consumption in Denmark than in Norway.
We found that one in three DT patients had a comorbid diagnosis of PTSD. Too little is known about delirium tremens and its relationship with PTSD,33 but some studies show that PTSD may follow DT,34,35 but also that PTSD could be a risk factor for DT.36 As both trauma and DT in the current study are identified as past life experiences, we do not know the order of these events. However, patients do not have current DT but are diagnosed with current PTSD, which could indicate some support to PTSD following DT, however without any claims of causality.
DT patients in the present study did not report worse sleep quality than those not having experienced DT. We know from other sources that grave disease, like DT, may be accompanied with disturbances in the circadian rhythm.37 However, more than half the patients in both the DT and non-DT groups reported poor sleep in the present study, which is in line with other studies showing poor sleep following heavy alcohol use.38
In addition to PTSD, one of the best known adverse events following DT is cognitive deterioration,18 at least in the already impaired.19 Our study is limited in investigating this as it did not include measures of cognitive function. Other limitations to the current study include retrospective self-report of DT and other elements, even if PTSD and major depression was diagnosed by trained staff. The relatively limited number of observations may also have rendered the investigation underpowered to detect some aspects of the DT patients, which could also influence lack of statistical significance for some of the variables after adjustments for sex and educational level.
Conclusion
In the present study delirium tremens (DT) had been experienced by one in four AUD patients. A history of DT was associated with having a diagnosis of PTSD and the duration of problematic drinking. Identifying factors associated with DT may be important in both clinically and preventive perspectives, and larger and prospective studies are warranted to further map risk factors for DT.
Funding
The study was partially funded by a research grant from the Norwegian Research Council (reference: 251140) and partially by internal funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Glass IB. Alcoholic hallucinosis: a psychiatric enigma–1. The development of an idea. Br J Addict. 1989;84(1):29–41. doi:10.1111/j.1360-0443.1989.tb00549.x
2. Moore DT, Fuehrlein BS, Rosenheck RA. Delirium tremens and alcohol withdrawal nationally in the Veterans Health Administration. Am J Addict. 2017;26(7):722–730. doi:10.1111/ajad.12603
3. Schuckit MA, Tipp JE, Reich T, Hesselbrock VM, Bucholz KK. The histories of withdrawal convulsions and delirium tremens in 1648 alcohol dependent subjects. Addiction. 1995;90(10):1335–1347. doi:10.1046/j.1360-0443.1995.901013355.x
4. Schuckit MA. Recognition and management of withdrawal delirium (delirium tremens). N Engl J Med. 2014;371(22):2109–2113. doi:10.1056/NEJMra1407298
5. Khan A, Levy P, DeHorn S, Miller W, Compton S. Predictors of mortality in patients with delirium tremens. Acad Emerg Med. 2008;15(8):788–790. doi:10.1111/j.1553-2712.2008.00187.x
6. Mainerova B, Prasko J, Latalova K, et al. Alcohol withdrawal delirium - diagnosis, course and treatment. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2015;159(1):44–52. doi:10.5507/bp.2013.089
7. Grover S, Ghosh A. Delirium tremens: assessment and management. J Clin Exp Hepatol. 2018;8(4):460–470. doi:10.1016/j.jceh.2018.04.012
8. Rao PSS, Bell RL, Engleman EA, Sari Y. Targeting glutamate uptake to treat alcohol use disorders Review. Front Neurosci. 2015;9(144). doi:10.3389/fnins.2015.00144
9. Fouarge E, Maquet P. Conséquences neurologiques centrales et périphériques de l’alcoolisme. [Neurological consequences of alcoholism]. Rev Med Liege. 2019;74(5–6):310–313. French.
10. Gortney JS, Raub JN, Patel P, Kokoska L, Hannawa M, Argyris A. Alcohol withdrawal syndrome in medical patients. J Clevel Clin Med. 2016;83(1):67–79. doi:10.3949/ccjm.83a.14061
11. Jesse S, Bråthen G, Ferrara M, et al. Alcohol withdrawal syndrome: mechanisms, manifestations, and management. Acta Neurol Scand. 2017;135(1):4–16. doi:10.1111/ane.12671
12. Mirijello A, D’Angelo C, Ferrulli A, et al. Identification and management of alcohol withdrawal syndrome. Drugs. 2015;75(4):353–365. doi:10.1007/s40265-015-0358-1
13. Sullivan JT, Sykora K, Schneiderman J, Naranjo CA, Sellers EM. Assessment of alcohol withdrawal: the revised clinical institute withdrawal assessment for alcohol scale (CIWA-Ar). Br J Addict. 1989;84(11):1353–1357. doi:10.1111/j.1360-0443.1989.tb00737.x
14. Rahman A, Paul M. Delirium Tremens. In: StatPearls [Internet]. StatPearls Publishing; 2021.
15. Wright T, Myrick H, Henderson S, Peters H, Malcolm R. Risk factors for delirium tremens: a retrospective chart review. Am J Addict. 2006;15(3):213–219. doi:10.1080/10550490600625798
16. Ferguson JA, Suelzer CJ, Eckert GJ, Zhou XH, Dittus RS. Risk factors for delirium tremens development. J Gen Intern Med. 1996;11(7):410–414. doi:10.1007/bf02600188
17. Nordström G, Berglund M. Delirium tremens: a prospective long-term follow-up study. J Stud Alcohol. 1988;49(2):178–185. doi:10.15288/jsa.1988.49.178
18. Wolters AE, van Dijk D, Pasma W, et al. Long-term outcome of delirium during intensive care unit stay in survivors of critical illness: a prospective cohort study. Critical Care. 2014;18(3):R125–R125. doi:10.1186/cc13929
19. Gross AL, Jones RN, Habtemariam DA, et al. Delirium and long-term cognitive trajectory among persons with dementia. Arch Intern Med. 2012;172(17):1324–1331. doi:10.1001/archinternmed.2012.3203
20. Bolstad I, Lien L, Bramness JG. ADHD symptoms as risk factor for PTSD in inpatients treated for alcohol use disorder. Psychiatry Res. 2021;300:113904. doi:10.1016/j.psychres.2021.113904
21. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561–571. doi:10.1001/archpsyc.1961.01710120031004
22. McPherson A, Martin CR. A narrative review of the Beck Depression Inventory (BDI) and implications for its use in an alcohol-dependent population. J Psychiatr Ment Health Nurs. 2010;17(1):19–30. doi:10.1111/j.1365-2850.2009.01469.x
23. Toft H, Neupane SP, Bramness JG, Tilden T, Wampold BE, Lien L. The effect of trauma and alcohol on the relationship between level of cytokines and depression among patients entering psychiatric treatment. BMC Psychiatry. 2018;18(1):95. doi:10.1186/s12888-018-1677-z
24. Espie CA, Kyle SD, Hames P, Gardani M, Fleming L, Cape J. The Sleep Condition Indicator: a clinical screening tool to evaluate insomnia disorder. BMJ Open. 2014;4(3):e004183. doi:10.1136/bmjopen-2013-004183
25. Gossop M, Best D, Marsden J, Strang J. Test-retest reliability of the Severity of Dependence Scale. Addiction. 1997;92(3):353. doi:10.1111/j.1360-0443.1997.tb03205.x
26. Gossop M, Marsden J, Stewart D. Dual dependence: assessment of dependence upon alcohol and illicit drugs, and the relationship of alcohol dependence among drug misusers to patterns of drinking, illicit drug use and health problems. Addiction. 2002;97(2):169–178. doi:10.1046/j.1360-0443.2002.00028.x
27. Schuckit MA, Smith TL, Tipp JE. The Self-Rating of the Effects of alcohol (SRE) form as a retrospective measure of the risk for alcoholism. Addiction. 1997;92(8):979–988. doi:10.1111/j.1360-0443.1997.tb02977.x
28. Schuckit MA, Tipp JE, Smith TL, Wiesbeck GA, Kalmijn J. The relationship between Self-Rating of the Effects of alcohol and alcohol challenge results in ninety-eight young men. J Stud Alcohol. 1997;58(4):397–404. doi:10.15288/jsa.1997.58.397
29. Glass IB. Alcoholic hallucinosis: a psychiatric enigma–2. Follow-up studies. Br J Addict. 1989;84(2):151–164. doi:10.1111/j.1360-0443.1989.tb00564.x
30. Torvik FA, Ystrom E, Gustavson K, et al. Diagnostic and genetic overlap of three common mental disorders in structured interviews and health registries. Acta Psychiatr Scand. 2018;137(1):54–64. doi:10.1111/acps.12829
31. Wood E, Albarqouni L, Tkachuk S, et al. Will this hospitalized patient develop severe alcohol withdrawal syndrome?: the rational clinical examination systematic review. JAMA. 2018;320(8):825–833. doi:10.1001/jama.2018.10574
32. Sørensen HJ, Holst C, Knop J, Mortensen EL, Tolstrup JS, Becker U. Alcohol and delirium tremens: effects of average number of drinks per day and beverage type. Acta Psychiatr Scand. 2019;139(6):518–525. doi:10.1111/acps.13006
33. Langan C, Sarode DP, Russ TC, Shenkin SD, Carson A, Maclullich AMJ. Psychiatric symptomatology after delirium: a systematic review. Psychogeriatrics. 2017;17(5):327–335. doi:10.1111/psyg.12240
34. Grover S, Sahoo S, Chakrabarti S, Avasthi A. Post-traumatic stress disorder (PTSD) related symptoms following an experience of delirium. J Psychosom Res. 2019;123:109725. doi:10.1016/j.jpsychores.2019.05.003
35. Bolton C, Thilges S, Lane C, Lowe J, Mumby P. Post-traumatic stress disorder following acute delirium. J Clin Psychol Med Settings. 2021;28(1):31–39. doi:10.1007/s10880-019-09689-1
36. Ali S, Patel M, Jabeen S, et al. Insight into delirium. Innov Clin Neurosci. 2011;8(10):25–34.
37. Pisani MA, D’Ambrosio C. Sleep and delirium in adults who are critically ill: a contemporary review. Chest. 2020;157(4):977–984. doi:10.1016/j.chest.2019.12.003
38. Chakravorty S, Chaudhary NS, Brower KJ. Alcohol dependence and its relationship with insomnia and other sleep disorders. Alcohol Clin Exp Res. 2016;40(11):2271–2282. doi:10.1111/acer.13217
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.