Back to Journals » International Journal of General Medicine » Volume 18
Histopathological Correlation of Cases with Epithelial Cell Abnormality Detected in Cervicovaginal Smear Screenings of Turkish Women and Their Association with HPV Subtypes
Authors Kılıç HÖ, İlhan Çelik Ö ![]()
Received 16 June 2025
Accepted for publication 10 July 2025
Published 14 July 2025 Volume 2025:18 Pages 3871—3879
DOI https://doi.org/10.2147/IJGM.S546538
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Hilal Özlem Kılıç,1,* Özgür İlhan Çelik2,*
1Department of Pathology, Muğla Training and Research Hospital, Muğla, Turkey; 2Department of Pathology, Muğla Sıtkı Koçman University, Faculty of Medicine, Muğla, Turkey
*These authors contributed equally to this work
Correspondence: Özgür İlhan Çelik, Muğla Sıtkı Koçman University, Faculty of Medicine, Department of Pathology, Muğla, 48000, Turkey, Tel +905063058343, Email [email protected]; [email protected]
Background: Cervical cancer is the second most common gynecological malignancy worldwide and one of the leading cause of cancer-related mortality among women. In Turkey, its incidence remains considerably high. Early detection through Pap (Papanicolaou) smear and HPV (Human Papilloma virus) DNA testing plays a vital role in reducing morbidity and mortality.
Objective: This study aims to evaluate the diagnostic concordance between cytological screening methods and definitive histopathological diagnoses, and to identify factors associated with diagnostic discrepancies.
Methods: A retrospective analysis was conducted on 643 cases that received both cytological and histopathological diagnoses. Patient data, including age, HPV-DNA type, presence of endocervical cells, atrophy, and inflammation, were reviewed and compared.
Results: Of the SCC (squamous cell carcinoma) cases, 96.2% were found in the 30– 65 age group HPV positivity and the presence of endocervical cells decreased with age. SCC was three times more frequent in HPV 16/18-positive cases than in other genotypes. A statistically significant inverse relationship was observed between increasing age and diagnostic concordance. HPV negativity was significantly associated with diagnostic discordance, while HPV genotype had no significant effect. Therefore, it would be appropriate to perform HPV screening at regular intervals. So our findings suggest that diagnostic concordance between cytology and histology is influenced by age and HPV status. Since HPV 16/18 positivity significantly increases the risk of SCC, screening strategies should take both age and genotype into consideration. High concordance between cytological screening results and histological diagnosis is very important for the prevention of advanced stage SCC.
Keywords: cervix, cervicovaginal smear, epithelial cell abnormality, HPV
Introduction
Cervical cancer is the 4th most common cancer in women after breast, lung and colorectal cancers and has very serious mortality and morbidity rates. It ranks 18th in our country.1,2 Although cervical cancer is a gynecological cancer that has the privilege of having a screening program and is therefore preventable, its mortality rate is quite high, especially for low and middle-income countries.3 The main risk factor for cervical cancer, which is one of the preventable cancers today, is Human Papillomavirus (HPV) and HPV DNA has been detected in approximately 95% of cases. Persistent HPV infection; the long-term presence of HPV settled in the cervix, is associated with the development of cervical cancer. In addition, the presence of other risk factors in the development of precancerous lesions together with HPV is important. Early onset of sexual activity, having more than one sexual partner, long-term use of contraceptives, sexually transmitted infections, tobacco use and immunosuppression are possible risk factors for cervical cancer.4–12
PAP (Papanicolaou) smear test and HPV DNA genotyping provide great benefits for the prevention and early treatment of cervical cancer. Routine screening programs are widely used worldwide today to identify individuals with risk factors for cervical cancer and to organize appropriate gynecological follow-up for them. Early detection of preinvasive and invasive cervical lesions and early initiation of treatment with the most commonly used PAP smear test have provided significant decreases in morbidity and mortality rates related to cervical neoplasms.3–5,7–10
The etiology of cervical cancer is more distinct compared to other cancers. Approximately 85% of cancer cases caused by HPV are cervical, while the others are vulva, anal, vaginal, penile, oropharyngeal and oral cancers. The presence of HPV is absolutely necessary but not sufficient for cervical cancer. It is important to focus on other risk factors because they increase the likelihood of encountering the virus or accelerate viral resistance to the immune system and the cancer formation period.5–7 Long-term use of oral contraceptives increases the risk of cervical cancer.6–13 It has been shown that the risk of developing cervical carcinoma in situ increases two-fold in oral contraceptive use for more than 5 years. It is estimated that this risk lasts for at least 10 years after stopping use.13–15
In epidemiological studies conducted on cervical cancer and reproductive factors, it has been found that the risk of developing cancer increases with the early age of initiation of sexual activity, the first term pregnancy being at a young age (<17) and having given birth multiple times.13–15 Multiparity is thought to be the underlying cause of this condition because hormonal conditions such as high estrogen and progesterone during pregnancy create susceptibility to HPV.6,15 In addition, family history of cervical cancer, poor hygiene conditions, a diet low in vegetables and fruits, low sociocultural and economic level, immunosuppression, and not routinely screening with PAP test are among the predisposing causes of cervical cancer.13–15 Given the high number of sexually active women and the elevated rates of HPV positivity in our society, as well as the limited accessibility of HPV screening programs in certain areas, conducting similar studies in different regions of the country may be important to support the inclusion of the HPV vaccine in the national routine immunization schedule. So we planned this study to highlight the high prevalence of HPV positivity in our society, its association with cervical cancer, and the significance and necessity of screening methods used for early detection.
Cervical cancer does not occur suddenly but through a multistage carcinogenesis and usually takes years to appear. Precancerous lesions are called cervical intraepithelial neoplasia (CIN) or squamous intraepithelial lesion (SIL). So it is very important to diagnose early precancerous cervical lesions in order to prevent carcinomas and PAP smear test seems to be very appropriate for this purpose.3 Many classifications have been used in the past to classify preneoplastic lesions of the cervix, and over the years the classification has evolved into more understandable but clinically significant subtypes. The Bethesda system was developed in 1988 by the American Cancer Institute in Bethesda, Maryland. The system, revised in 1991, 2001 and 2014, aimed to standardize Pap smear reporting.16,17
HPV types that cause anogenital lesions are divided into 3 groups according to their carcinogenic potential as high-risk carcinogenic types (types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59), possible carcinogenic types (types 26, 53, 66, 67, 68, 70, 73, 82) and low-risk type (types 6, 11, 42, 44, 51,83). The most common types worldwide are HPV types 16 and 18. It is known that the majority of women will be exposed to HPV infection at least once in their lives, and most of these patients will be between the ages of 15 and 25.3–15
In 2012, the American College of Pathologists (CAP) and the American Society for Colposcopy and Cervical Pathology (ASCCP) published a comprehensive reevaluation of the terminology used for HPV and squamous intraepithelial lesions and early invasive cancers in the LAST (Lower Anogenital Squamous Terminology) project to harmonize the terminology used in all lower anogenital regions. The LAST project recommends a two-digit classification of high and low grade, followed by the term “Squamous Intraepithelial Lesion” (SIL). The SIL terminology was developed to use a uniform terminology for diagnosis and is parallel to the Bethesda system used since 1988. Although the term SIL is widely accepted, the term “Cervical Intraepithelial Neoplasia” (CIN) can also be used. The “Low-Grade Squamous Intraepithelial Lesion” (LGSIL) group includes CIN1 lesions, and the “High-Grade Squamous Intraepithelial Lesion” (HGSIL) category includes CIN 2–3 lesions.3,16–18
This study aimed to determine the frequency of cervical neoplasia in our city and its surroundings and to investigate the consistency of PAP smear and biopsy diagnoses. In addition, the factors causing incompatibility were examined.
Materials and Methods
For the study, patients whose Liquid-based PAP smears were evaluated in the Department of Medical Pathology of Muğla Sıtkı Koçman University Education and Research Hospital between January 2015 and December 2023 and had the diagnosis of the epithelial cell abnormality according to the Bethesda System were determined. Among these patients, 643 were suitable for the study as the inclusion criterias were being unvaccinated (HPV vaccine), untreated before and whose biopsy or excision material diagnoses and HPV tests were available in our center and had the diagnosis of the epithelial cell abnormality. The patients whose biopsies were taken and evaluated in other hospitals were excluded. All pathology reports, HPV tests (Studied by Microbiology Department using HPV sign Q24 complete kit- Rotor-Gene and PyroMark Q24 instrument) were evaluated retrospectively.
This study was initiated after the approval of Muğla Sıtkı Koçman University Clinical Research Ethics Committee with the decision number 99 dated 10.10.2023 and our study completely complies with the Declaration of Helsinki. As a general informed consent form is routinely obtained from all patients at the time of hospital admission, the Hospital Ethics Committee does not deem it necessary to obtain additional consent for retrospective studies.
Cervicovaginal smears of 643 patients were prepared with liquid-based cytology method (Sure-path) and stained with Papanicolaou (PAP) stain. All cases were evaluated according to final version of 2014 Bethesda system in terms of adequacy, epithelial cell abnormality, presence of microorganism, inflammation, reactive cellular changes, atrophy and the presence of transformation zone/endocervical cell component. For the adequacy criteria, at least 5000 squamous cells were sought, and for the presence of transformation zone, 10 endocervical or squamous metaplastic cells were sought.17 Hematoxylin-Eosin sections of the colposcopic biopsies and/or resection materials of these patients were evaluated by pathologists with the light microscopes for their histopathological diagnoses. Full concordance is considered as the exact diagnosis. A subsequent histopathological diagnosis of LSIL or SCC in cases with an initial cytological diagnosis of ASC-H, HSIL in cases with ASCUS, LSIL or HSIL in cases with AGC, SCC in cases with HSIL, and HSIL or SCC in cases with LSIL were considered as partial concordance.17 The results of the patients obtained by HPV DNA genotyping PCR test in our hospital’s medical microbiology laboratory and Cancer Early Diagnosis Screening and Education Center (KETEM) were used for the study. All data were obtained from the hospital software using a retrospective scanning method.
All statistical analyses were performed with SPSS version 26.0 software (SPSS, Chicago, IL, USA). Kolmogorov–Smirnov test was used to examine whether the distribution of discrete numerical variables was close to normal. In descriptive statistics related to variables, categorical variables were expressed as number of cases and (%), and discrete numerical variables were expressed as mean ± standard deviation. Student T test was applied to binary groups showing normal distribution on measurement data, and One Way Anova Variance Analysis was applied to three-category groups. Mann Whitney U and Kruskal Wallis Analysis were applied to binary groups not showing normal distribution. Pearson’s χ2 test was used in the analyses of categorical data unless otherwise stated. On the other hand, in 2×2 cross tables, when the expected frequency was between 5 and 25, the continuity-corrected χ2 test was used for examination, and when the expected frequency was below 5 in at least 1/4 of the cases, Fisher’s exact probability test was used for evaluation. As a result of statistical analysis, p<0.05 results were considered statistically significant.
Results
The ages of the 643 cases included in our study group ranged from 19 to 73, with an average age of 46.6±10.7 years. The cases were divided into three age groups as under 30 (24 cases 3.7%), 30–65 (592 cases 92.1%), and over 65 (27 cases 4.2%). The distribution of the cases included in our study group based on their cytological and histological diagnoses are presented in Table 1.
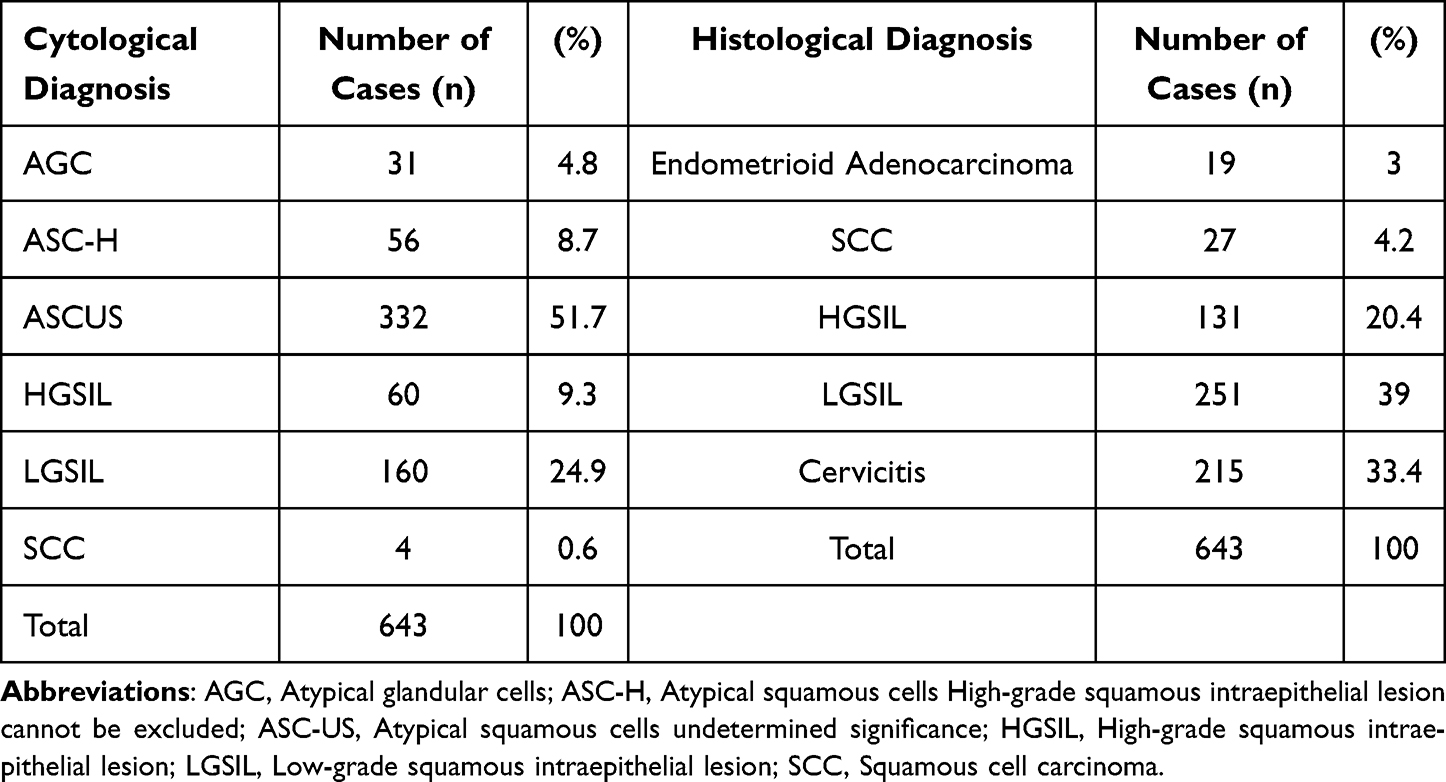 |
Table 1 Distribution of Cases According to Cytological and Histological Diagnosis |
When examined according to age groups, the ASC-H rate in cytology materials was proportionally less common in the 30–65 age group than in other groups. In contrast, the LGSIL rate was statistically significantly more common in this age group than in other groups (p=0.008). Cytological diagnoses of the cases included in our study group according to age groups are shown in Table 2.
 |
Table 2 Cytological Diagnoses of Cases According to Age Groups |
When we look at the histological diagnoses of our cases, almost all of the SCC cases (96.2%) were detected in the 30–65 age group. In the group over 65 years of age, a higher percentage of Endometrioid Adenocarcinoma cases were seen compared to other groups and the results were statistically significant (p=0.023). The age group-histological diagnosis comparison is shown in Table 3.
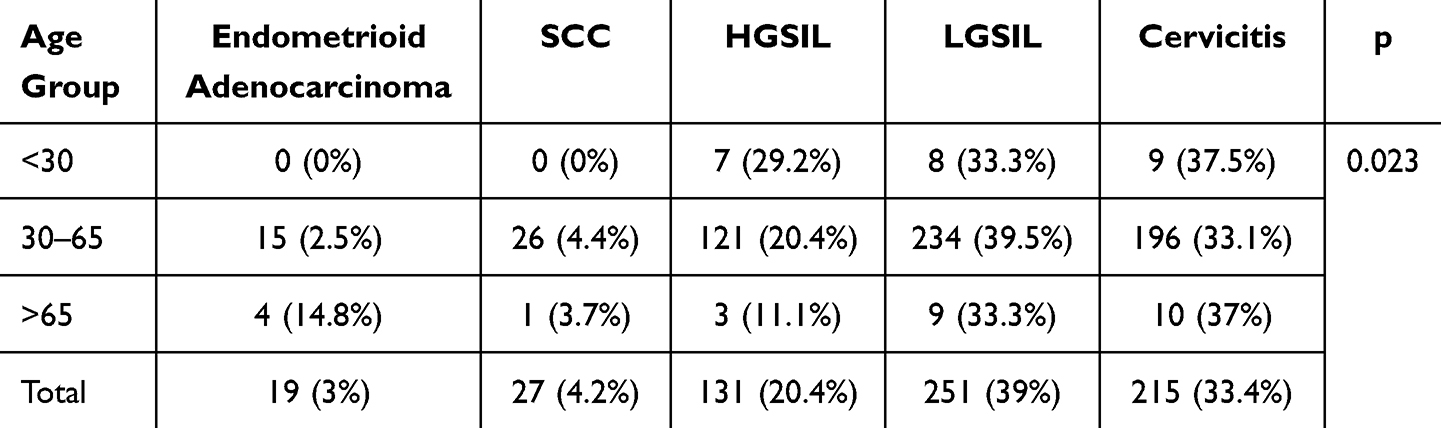 |
Table 3 Histological Diagnoses of Cases According to Age Group |
When non-neoplastic parameters were evaluated in PAP smears, endocervical cells were present in 488 (75.9%) patients, inflammation in 297 (46.2%) patients, and atrophy in 95 (14.8%) patients. The presence of endocervical cells decreased as age increased. The rates were 87.5%, 76.5% and 51.9% for the groups under 30, 30–65 and over 65, respectively, and the results were statistically significant (p=0.005).
When atrophy status was examined according to age groups, the frequency of atrophy increased with age, as expected. The percentages for these three age groups were 0%, 13.7% and 51.9%, respectively, and the results were statistically significant (p<0.001).
When the relationship between HPV positivity and age groups was evaluated, the frequency of HPV positivity was 70.2% in the group under 30 years of age, 54.7% in the 30–65 age group, and 33.3% in those over 65 years. These results indicate that the frequency of HPV positivity increases as age decreases in our case group, and the findings were statistically significant (p=0.023). HPV subtype 16 was positive in 24.6%, HPV subtype 18 was positive in 6.1% and other subtypes were positive in 23.8% of the patients. In 45.6% of the patients HPV was not detected positive. No statistically significant difference was found in the distribution of HPV genotypes according to age groups (p=0.26).
When cytological materials were examined, HGSIL diagnosis was seen more frequent in cases with HPV 16 positivity compared to other genotypes. This result was statistically significant (p=0.002). When histological diagnoses were compared with HPV genotypes, it was found that the incidence of SCC in cases with HPV 16 and HPV 18 positivity were totally 3 times higher than in cases with HPV-other types, and the results were statistically significant (p=0.023). Cytological and histological diagnoses according to HPV genotypes are shown in Table 4.
 |
Table 4 Tissue Diagnoses of Cases According to HPV Genotype Distribution |
The cytological diagnoses of our cases compared with the histological diagnoses are shown in Table 5. Only 4 of the 27 cases with a tissue diagnosis of SCC had previously been diagnosed with SCC cytologically, and these diagnoses are among the most incompatible diagnoses as a group. The concordance rate between the cytological and histological diagnoses of our cases are also evaluated. Full concordance between cytological and histological diagnoses was found in 332 (51.6%) cases, partial concordance was found in 271 (42.1%) cases, and no concordance was found in 40 (6.2%) cases.
 |
Table 5 Comparison of Cytological-Histological Diagnosis |
When the mean ages are examined according to diagnostic concordance, the mean age of patients with no concordance is 50 ± 11.8; the mean age of patients with partial concordance is 47.7 ± 10.3; and the mean age of patients with concordance is 45.2 ± 10.7. As the age decreases, the concordance rate between cytological and histological diagnoses increases, and this relationship is statistically significantly correlated according to the Student t test. The concordance rates of our cases with histological diagnoses according to their individual cytological diagnoses are shown in Table 6. The lowest concordance rate was in patients with cytological diagnosis of ASC-H and LGSIL, and the results were statistically significant (p< 0.001).
 |
Table 6 Histological Diagnosis Concordance According to Cytological Results |
The concordance rates of our cases with cytological diagnoses according to their individual histological diagnoses are shown in Table 7.
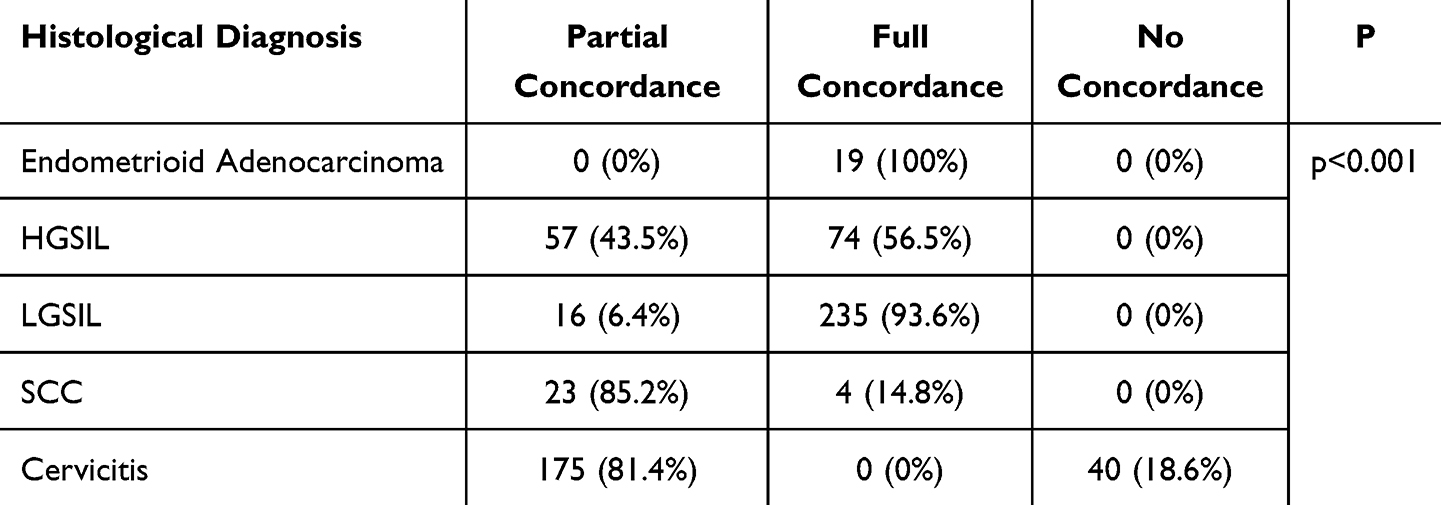 |
Table 7 Cytological Diagnosis Concordance According to Histological Results |
The highest rate of discordance was observed in cases diagnosed histologically with cervicitis. However, since only patients with abnormal cytology results were included in our study, cases with a histological diagnosis of chronic cervicitis were considered discordant unless the cytological diagnosis was ASCUS. Additionally, cases diagnosed with SCC (14.8%) and HSIL (56.5%) also showed relatively low full concordance rates, and the results were statistically significant (p<0.001).
When evaluating the effects of non-neoplastic parameters on the concordance between cytological and histological diagnoses, it was found that the absence of endocervical cells, presence of atrophy and inflammation all had a negative impact on diagnostic concordance (p<0,001).
Discussion
Although the incidence of cervical cancer has decreased with the implementation of effective screening programs, it remains one of the leading causes of cancer-related mortality in women worldwide, with approximately 600,000 new cases reported annually. As a potentially preventable cancer, screening programs and vaccination efforts are of critical importance. The PAP smear test, one of the oldest and most widely used screening tool, plays a key role in detecting premalignant lesions before symptoms arise.1–3 Squamous cell carcinoma accounts for nearly 80% of cervical malignancies, with high-risk HPV types, especially HPV 16 and 18, implicated in the vast majority (90–99%) of SCC cases. In our study, the HPV positivity rate among SCC cases was 78%, slightly lower than in the literature, possibly due to the small number of SCC cases in our cohort (27 cases).
Screening programs play a crucial role in detecting pre-malignant lesions before they become symptomatic. In many countries, women aged 30 to 65 are included in routine screening programs, based on both scientific and economic considerations. The American College of Obstetricians and Gynecologists (ACOG) recommends against HPV DNA testing in women under 30 due to the high rate of transient infections in this age group. Our findings align with this recommendation, as HPV positivity was most prevalent in the under-30 age group (70.8%).19–21 In our study, none of the biopsied cases from the under-30 age group were diagnosed with SCC. However, 33.3% were diagnosed with LGSIL, and 29.2% with HGSIL. According to these results, in our society, where the average age of first sexual intercourse is decreasing, we believe it is necessary to include the under 30 age group in routine screening. Early detection and treatment of premalignant lesions in this group can enhance survival rates and preserve fertility. In the literature, HPV positivity rates vary significantly across different populations, ranging from 3% to 45%. In a study by Beyazıt et al, the HPV DNA positivity rate in Turkey was reported as 45.2%.21–23 In our study, the HPV positivity rate was 55.5%. However, since all the cases we included had cytological atypia, this rate can be considered within the expected range. Indeed, in the literature, HPV positivity rates among cases with cytological atypia range from 52% to 77%. In the study by Yüce et al, this rate was reported as 54.4%, which is very close to our findings.24
Not all HPV types lead to malignancy or premalignant lesions. As has long been established, HPV 16 and HPV 18 are among the highest-risk groups. According to the literature on HPV genotyping, HPV 16 is the most frequently detected type.21 In our study, the most commonly observed HPV type was also HPV 16, with a prevalence of 24.5% among all cases. Although this percentage is relatively high, the frequency is consistent with findings in the literature. In our study, HPV types other than HPV 16 and HPV 18 were not specifically genotyped. This group represents 43.7% of all HPV-positive cases. Due to the lack of specific genotyping, there is a partially incorrect perception that this large group-excluding HPV 16 and 18- consists solely of low-risk HPV types. So our findings demonstrate that among the group with “HPV-other positivity” the rate of HGSIL in histological diagnoses is 23.5%, and the SCC rate is 2.6%. To avoid missing high-grade premalignant or malignant lesions, complete HPV genotyping should be performed at all our medical centers. If this is not feasible, it must be kept in mind that the broad “HPV-other positive” group also includes high-risk genotypes.
All cases included in our study were cytologically atypical. In the literature, among cytological specimens indicating epithelial cell abnormality, the most frequently observed was ASCUS, followed by LGSIL similarly in the study by Yüce et al,24 Hasçiçek et al.25 The cytological findings in our study are consistent with the Turkish literature, suggesting that our case distribution is representative of the Turkish population.
The Pap smear test is widely used in cervical cancer screening due to its ease of application and non-invasive nature. However, cytological findings do not always perfectly correlate with biopsy results. In a study by Anschau et al, the histopathological concordance rate was reported as 90.8%.26 In our study, two categories were established: full concordance and partial concordance. These parameters include diagnoses that do not result in significant clinical management differences. The percentage of cases without significant diagnostic discordance was 93.8%, which aligns with the literature. In the study by Demir et al, the detection rate of pathological lesions in tissue among patients with cytologically detected pathology was 45.5%.27 In our study, however, this rate was 66.6%, which is significantly higher than previously reported in the Turkish literature. This increase may be attributable to the more widespread use of HPV DNA co-testing. More further studies are needed to establish a current rate representative of the Turkish population.27,28
Numerous studies in the literature have examined the concordance between cytology and biopsy from various perspectives. The general approach evaluates the percentage of epithelial lesions detected in biopsies of patients who received a cytological diagnosis. Therefore, cytological diagnoses such as HGSIL, which show more pronounced atypia, are generally more successful, while ambiguous categories like ASCUS are less predictive.27,28 In our study, rather than measuring lesion detection rates, we focused on the one-to-one concordance between cytological and histopathological diagnoses. For this reason, some of the data we present may be new to the Turkish literature. The two largest cytological diagnostic groups that did not correlate with histological biopsy results were AGC (29%) and ASC-H (21.4%). Among cases diagnosed with ASCUS, our detection rate of intraepithelial lesions was 32.5%. In the study by Hasçicek et al, the same rate was reported as 43%. These rates are about 10% lower compared to values reported in the Turkish literature, indicating a lower lesion detection rate per ASCUS diagnosis in our center.25
The highest rate of diagnostic discordance was observed in the group with a histological diagnosis of SCC. Only 14.8% of cases with a biopsy-confirmed SCC had previously been diagnosed as SCC on cytology, most of them had previously been diagnosed as HGSIL and ASC-H. This level of discordance carries significant clinical and therapeutic implications, as the management of SCC differs considerably from that of other intraepithelial lesions. To reduce such discordance, it is essential to diminish the potential technical limitations (eg, interobserver variability, quality of sample fixation), to obtain adequate clinical information, for the pathologist to adopt a meticulous approach when evaluating smears with potential for invasive disease, and to mention any suspicion of invasion in their reports when applicable.
When the PAP smear is combined with HPV DNA testing, its sensitivity increases significantly. However, a large proportion of cases with diagnostic discordance were HPV-negative. While the overall concordance rate between cytology and biopsy was 51.6%, this rate dropped to 37.5% among HPV-negative patients. This finding highlights the need for more detailed cytomorphological evaluation even in HPV-negative patients during co-testing.
In addition to these factors, some non-neoplastic parameters also affect concordance rates. These include the absence of endocervical cells, the presence of atrophy, and chronic inflammation. The concordance rates in these groups were 34.2%, 35.8%, and 43.1%, respectively-all significantly below the average concordance rate of 51.6%. Therefore, in the presence of these suboptimal conditions, more meticulous evaluation and, if necessary, repeat smears are crucial for accurate diagnosis.
Cervical cancer and premalignant lesions vary depending on the region where studies are conducted, the cultural habits of populations, and sample sizes. Our study is single-centered and reflects data from 643 patients who presented to our hospital with various complaints, representing a specific population. The findings are consistent with the broad range of prevalence rates in the literature and highlight the role of cytology and HPV DNA testing in the early detection of cervical lesions. Moreover, individual HPV genotypes were examined and compared with other clinical parameters in our study.23–28
Conclusion
In conclusion, considering the high prevalence of HPV in our country, the inclusion of individuals under the age of 30 in cervical cancer screening programs, wider HPV typing or resampling in atypical cytological results may contribute significantly to improving early diagnosis rates. Early diagnosis and treatment are crucial in preventing carcinoma development and the potentially fatal outcomes that may follow. Therefore, cytology-histology concordance plays a critical role. Our study mainly discusses the parameters that contribute to diagnostic discordance. Among these variables, limitations related to clinicians, pathologists, and technical methodology can be identified and may be prevented by improving sampling protocols, professional training, or complementary use of diagnostic techniques. We had some study limitations; as this was a retrospective study, the specific sample, and the potential influence of bias or misclassification; so future prospective studies addressing these factors are expected to provide further insight and potentially reduce the incidence of SCC in the population.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Global Cancer Observatory. Cancer Today. Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.who.int/media/globocan/factsheets/populations/900-world-fact-sheet.pdf.
2. Global Cancer Observatory. Cancer Today. Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.who.int/media/globocan/factsheets/populations/792-turkiye-fact-sheet.pdf.
3. WHO Classification of Tumours Editorial Board. Tumours of uterine cervix. In: Female Genital Tumours, WHO Classification of Tumours.
4. Small W, Bacon MA, Bajaj A, et al. Cervical cancer: a global health crisis. Cancer. 2017;123(13):2404–2412. doi:10.1002/cncr.30667
5. Harris TG, Kulasingam SL, Kiviat NB, et al. Cigarette smoking, oncogenic human papillomavirus, Ki-67 antigen, and cervical intraepithelial neoplasia. Am J Epidemiol. 2004;159(9):834–842. doi:10.1093/aje/kwh115
6. Hebnes JB, Munk C, Frederiksen K, et al. The role of circumcision, tobacco, and alcohol use in genital human papillomavirus infection among men from Denmark. Int J STD AIDS. 2021;32(11):1028–1035. doi:10.1177/09564624211014727
7. Muñoz-Bello JO, Carrillo-García A, Lizano M. Epidemiology and molecular biology of HPV variants in cervical cancer: the state of the art in Mexico. Int J Mol Sci. 2022;23(15):8566. doi:10.3390/ijms23158566
8. Yuan Y, Cai X, Shen F, et al. HPV post-infection microenvironment and cervical cancer. Cancer Lett. 2021;497:243–253. doi:10.1016/j.canlet.2020.10.034
9. Wójcik L, Samulak D, Makowska M, et al. The role of human papillomavirus in cervical cancer. Int J Cancer Clin Res. 2019;6:125. doi:10.23937/2378-3419/1410125
10. Dunne EF, Nielson CM, Stone KM, et al. Prevalence of HPV infection among men: a systematic review of the literature. J Infect Dis. 2006;194(8):1044–1057. doi:10.1086/507432
11. Appleby P, Beral V, Berrington de Gonzále A, et al. Carcinoma of the cervix and tobacco smoking: collaborative reanalysis of individual data on 13,541 women with carcinoma of the cervix and 23,017 women without carcinoma of the cervix from 23 epidemiological studies. Int J Cancer. 2006;118(6):1481–1495. PMID: 16206285. doi:10.1002/ijc.21493
12. García-Closas R, Castellsagué X, Bosch X, et al. The role of diet and nutrition in cervical carcinogenesis: a review of recent evidence. Int J Cancer. 2005;117(4):629–637. doi:10.1002/ijc.21193
13. Chelimo C, Wouldes TA, Cameron LD, et al. Risk factors for and prevention of human papillomaviruses (HPV), genital warts and cervical cancer. J Infect. 2013;66(3):207–217. doi:10.1016/j.jinf.2012.10.024
14. Tao L, Han L, Li X, et al. Prevalence and risk factors for cervical neoplasia: a cervical cancer screening program in Beijing. BMC Public Health. 2014;14:1185. doi:10.1186/1471-2458-14-1185
15. International Collaboration of Epidemiological Studies of Cervical Cancer. Cervical carcinoma and reproductive factors: collaborative reanalysis of individual data on 16,563 women with cervical carcinoma and 33,542 women without cervical carcinoma from 25 epidemiological studies. Int J Cancer. 2006;119(5):1108–1124. doi:10.1002/ijc.21953
16. Nayar R, Wilbur DC, editor. The Bethesda System for Reporting Cervical Cytology.
17. Pangarkar MA. The Bethesda System for reporting cervical cytology. Cytojournal. 2022;19:28. doi:10.25259/CMAS_03_07_2021
18. Darragh TM, Colgan TJ, Cox JT, et al. The lower anogenital squamous terminology standardization project for HPV-associated lesions: background and consensus recommendations from the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology. Int J Gynecol Pathol. 2013;32(1):76–115. doi:10.1097/PGP.0b013e31826916c7
19. Curry SJ, Krist AH, Owens DK; US Preventive Services Task Force, et al. Screening for cervical cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2018;320(7):674–686. doi:10.1001/jama.2018.10897
20. Aydoğdu SGM, Özsoy Ü. Serviks kanseri ve HPV. Androl Bul. 2018;20(1):25–29. doi:10.24898/tandro.2018.62533
21. Forman D, de Martel C, Lacey CJ, et al. Global burden of human papillomavirus and related diseases. Vaccine. 2012;30(5):F12–F23. doi:10.1016/j.vaccine.2012.07.055
22. Li W, Liu LL, Luo ZZ, et al. Associations of sexually transmitted infections and bacterial vaginosis with abnormal cervical cytology: a cross-sectional survey with 9090 community women in China. PLoS One. 2020;15(3):e0230712. doi:10.1371/journal.pone.0230712
23. Beyazit F, Sılan F, Gencer M, et al. The prevelance of human papillomavirus (HPV) genotypes detected by PCR in women with normal and abnormal cervico-vaginal cytology. Ginekol Pol. 2018;89(2):62–67. doi:10.5603/GP.a2018.0011
24. Yuce K, Pinar A, Salman MC, et al. Detection and genotyping of cervical HPV with simultaneous cervical cytology in Turkish women: a hospital-based study. Arch Gynecol Obstet. 2012;286(1):203–208. doi:10.1007/s00404-012-2280-z
25. Hasçiçek SÖ, Oğuzsoy T, Eken KG, et al. Comparison of liquid-based cytology cervical smears with histopathological findings. J Clin Anal Med. 2018;9(5):359–362. doi:10.4328/JCAM.5763
26. Anschau F, Guimarães Gonçalves MA. Discordance between cytology and biopsy histology of the cervix: what to consider and what to do. Acta Cytol. 2011;55(2):158–162. doi:10.1159/000320911
27. Demir F, Erten R, Aras I, et al. Correlation of cervical smear cytology and histopathology findings from Van Yüzüncü Yıl University Dursun Odabaş Medical Center in Turkey. Eastern J Med. 2020;25(2):305–311. doi:10.5505/ejm.2020.01886
28. Atılgan R, Artaş G, Kaplan S, et al. Comparison of histopathological results of thinprep and conventional cervicovaginal smears. Firat Med J. 2015;20(1):19–24.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.