Back to Archived Journals » Open Access Journal of Sports Medicine » Volume 16
Hip Microinstability: Current Concepts in Diagnosis, Surgical Management, and Outcomes A Narrative Review
Authors Villegas Meza AD ![]() , Nocek M
, Nocek M ![]() , Felan NA, Speshock A, Bolia IK, Philippon MJ
, Felan NA, Speshock A, Bolia IK, Philippon MJ ![]()
Received 13 September 2025
Accepted for publication 23 December 2025
Published 31 December 2025 Volume 2025:16 Pages 205—221
DOI https://doi.org/10.2147/OAJSM.S505874
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Andreas Imhoff
Alan D Villegas Meza,1 Michael Nocek,1 Nicholas A Felan,1 Alyson Speshock,1 Ioanna K Bolia,1,2 Marc J Philippon1,3
1The Center for Outcomes-Based Orthopaedic Research, The Steadman Philippon Research Institute, Vail, CO, USA; 2Department of Orthopaedic Surgery, University of Southern California, Los Angeles, CA, USA; 3The Steadman Clinic, Vail, CO, USA
Correspondence: Marc J Philippon, The Steadman Clinic and The Steadman Philippon Research Institute, 181 W. Meadow Drive, Suite 1000, Vail, CO, 81657, USA, Tel +1(970) 283-8091, Email [email protected]
Background: Hip microinstability—subtle, symptomatic femoral head translation without dislocation—compromises the labral suction seal and accelerates chondrolabral wear. Clinical overlap with femoroacetabular impingement syndrome (FAIS) and borderline dysplasia delays recognition.
Purpose: To synthesize contemporary evidence on definitions, diagnosis, imaging, management, and outcomes in hip microinstability and to propose a phenotype-guided framework grounded in the labrum-capsule-ligamentum teres (LT) stability continuum.
Study Design: Narrative review.
Methods: Peer-reviewed literature (2000– 2025) focusing on biomechanical investigations, comparative cohorts, meta-analyses, and consensus statements on microinstability, hip capsular management, borderline dysplasia, and LT pathology.
Results: A four-pillar diagnostic approach improves accuracy. The Abduction-Hyperextension-External Rotation (AB-HEER) and Hyperextension-External Rotation (HEER) tests provide the highest single-test accuracy among exam maneuvers, whereas the prone instability test offers high specificity to rule in. The femoroepiphyseal acetabular roof (FEAR) index aids in risk stratification for borderline dysplasia but is position-sensitive. Arthroscopy with labral preservation and complete hip capsular closure improves patient-reported outcomes (PROs) and survivorship relative to non-closure. Iatrogenic cam over-resection can precipitate microinstability; femoral head-neck remplissage is a revision option to restore contour and sealing mechanics. In borderline dysplasia, both arthroscopy and periacetabular osteotomy (PAO) improve PROs when selection is phenotype-guided; PAO trends toward lower total hip arthroplasty (THA) conversion when undercoverage is the primary driver. Early postoperative circumduction is associated with lower rates of adhesion-related reoperation. Return-to-sport (RTS) decisions are criteria-based rather than time-based across successful programs.
Conclusion: A seal-first, close-second strategy, situated within a stability continuum, underpins contemporary care. Standardized definitions, objective laxity metrics, multicenter registries, and microinstability-specific rehabilitation/RTS batteries are needed to refine indications and improve durability; evidence specific to labral augmentation in microinstability remains limited.
Clinical Relevance: Precise phenotyping and capsular stewardship reduce the risk of revision hip arthroscopy and conversion to total hip arthroplasty, inform sport-specific counseling, and align with joint-preservation goals in young, active patients.
Level of Evidence: V (Narrative Review).
Plain Language Summary: Hip microinstability refers to the hip being slightly too loose to maintain the ball of the joint centered during everyday movement or sports. It can cause pain in the front or side of the hip, feelings of the hip giving way, and a clicking sensation. It is more common in athletes and in people with mild undercoverage of the hip socket (sometimes referred to as borderline dysplasia), generalized joint looseness, or differences in the twist of the thigh or pelvis. This review explains how clinicians can recognize microinstability, how to ensure consistency in X-rays and scans across clinics, and how to determine the best course of action between rehabilitation and surgery. Diagnosis combines a careful history, a focused exam that looks for positions that reproduce symptoms, and standardized imaging. Most people start with targeted exercises to strengthen and coordinate the muscles that center the hip. When symptoms persist and imaging reveals treatable issues, surgery can repair the labrum (the seal around the socket) and tighten the joint lining with precision. If the socket does not cover the ball sufficiently, a realignment operation may be considered, sometimes in conjunction with surgery. Across published studies, many patients experience improvement and return to activity; however, results vary depending on anatomy and sport, and overtightening of the hip capsule can lead to stiffness. A clear, step-by-step pathway from assessment to treatment helps patients receive the right care at the right time while setting realistic expectations for recovery and return to sport.
Keywords: Hip arthroscopy, labral repair, Hip capsule, femoroacetabular impingement, microinstability, sports medicine
Introduction
Hip microinstability is characterized by excessive femoral head translation within the physiologic range of motion (ROM), resulting in pain, apprehension, and dysfunction without frank subluxation or dislocation.1–3 The concept was refined through descriptions of capsular laxity testing (eg, the dial test) and the observation that capsulotomy destabilizes, whereas capsular closure or plication restores near-native hip kinematics.4–9 Since 2013, the literature has evolved from technique reports to the biomechanical quantification of suction seal mechanics and capsular tensioning, as well as comparative outcomes demonstrating the value of routine capsular closure.10–14 Microinstability is particularly relevant in sports that require an extreme and prolonged ROM (eg, ballet, gymnastics, figure skating, hockey), where repetitive extension, external rotation, and abduction stress the anterior capsulolabral complex, potentially leading to central femoral head chondromalacia.15–17
Methods
This narrative review was conducted in accordance with the SANRA (Scale for the Assessment of Narrative Review Articles) guidelines to ensure methodological rigor and transparency. A comprehensive search was performed in PubMed/MEDLINE, Embase, and the Web of Science databases from January 2000 to June 2025. The search strategy included combinations of the following terms: hip, instability, microinstability, labrum, capsule, capsular plication, borderline dysplasia, and periacetabular osteotomy. Reference lists of key articles and prior reviews were also screened to identify additional studies.
Eligible studies included clinical or biomechanical investigations that described the diagnosis, imaging assessment, management, or outcomes of patients with hip microinstability with no language restriction. Both nonoperative and operative management strategies were included, with a focus on arthroscopic and realignment techniques. Studies focusing on conditions unrelated to instability (such as advanced osteoarthritis or femoroacetabular impingement syndrome [FAIS] without instability features) were excluded from the analysis.
Two reviewers (A.V.M. and M.K.) independently screened titles and abstracts, followed by full-text evaluation for eligibility. Disagreements were resolved through open discussion and a consensus-based approach. Data extracted included study design, population characteristics, diagnostic criteria, interventions, outcomes, and follow-up duration. No formal risk-of-bias tool was applied, given the narrative design; study limitations and heterogeneity were recorded and used to temper recommendations in accordance with SANRA guidance.
Definitions and Pathophysiology
Hip Instability Versus Microinstability
Gross instability of the hip denotes pathological translation with clinical subluxation or dislocation (often traumatic).1,2 Microinstability refers to excessive femoral translation of the head upon the acetabulum within physiologic ROM, producing pain, apprehension, and dysfunction without frank subluxation or dislocation.3,9,18–20 Static radiographs may appear normal, and contributions often include both osseous and soft tissue.
Position- and posture-dependent femoral head translation in native hips appears to occur on the order of sub-millimeter to low single-digit millimeters. Emerging unpublished cadaveric work from the senior author’s group, using a 6-degrees-of-freedom robotic platform, suggests that native translation magnitudes are position-dependent and in the low single-digit millimeter range, and that experimentally reducing capsular restraint increases both excursion and decentration; taken together with published in-vivo and cadaveric series, these observations support the view that no single numerical threshold defines microinstability across positions.4,6,7,21 Reported mean excursions in native conditions are typically ~0.3–2.0 mm, with higher transient maxima during provocative maneuvers, while isolated capsulotomy or selective ligament release increases excursion by approximately 1–4 mm, depending on the structure released and the hip posture.22 These magnitudes, although small in absolute terms, are biomechanically meaningful.22
Contact-pressure mapping and computational modelling demonstrate systematic shifts in contact location and peak pressures with changes in flexion and rotation (cadaveric mean pressures commonly reported 1.5–4.4 MPa), indicating that modest translations and altered rotational restraint can meaningfully redistribute load across the acetabular rim and articular cartilage.23 In practical terms, such load redistribution offers a mechanistic link to activity-related pain and progressive chondrolabral injury in susceptible morphologies.23
Mechanistically, capsular ligaments provide the primary rotational and translational restraints across most of the arc of motion, with the labrum and ligamentum teres serving as secondary stabilizers.24 The relative contribution of the ligamentum teres increases in positions of high flexion with adduction and external rotation, which helps explain the position-dependent increases in excursion observed following capsular injury or insufficiency.24 This ligament-angle relationship aligns with clinical observations of apprehension and giving-way in provocative positions, underscoring the rationale for measured capsular management and labral seal restoration in surgical treatment algorithms.24
Osseous Contributions
The hip’s ball-and-socket geometry provides passive containment; loss of coverage or unfavorable femoral version reduces the contact area that resists translation, especially at terminal motion.25,26 Osseous patterns associated with microinstability include acetabular undercoverage (low lateral center-edge angle [LCEA], elevated Tönnis angle), borderline dysplasia of the hip (BDH) with concerning femoro-epiphyseal acetabular roof (FEAR) index values, and femoral version mismatch (excess femoral antetorsion or acetabular retro/anteversion).27,28 These patterns alter load distribution and can accelerate chondrolabral injury.25,29 Selected FAIS morphologies may drive posterior translation at end range and, when combined with capsular laxity or undercoverage, contribute to microinstability.24,30,31 Surgical treatment of FAIS carries an iatrogenic risk: over-resection during cam decompression reduces head-neck offset and can disrupt labral suction mechanics.32,33 A femoral head-neck remplissage using iliotibial (IT) band allograft is a viable revision strategy to restore contour and re-establish the seal when over-resection is present (Grading of Recommendations, Assessment, Development, and Evaluation[GRADE]: Very low; level of evidence [LOE]: IV).10,32
Soft-Tissue Contributors
Hip Capsule
The capsule comprises the zona orbicularis (ZO) and three principal ligaments: the iliofemoral ligament (IFL), pubofemoral ligament (PFL), and ischiofemoral ligament (ISFL).24,34,35 Collectively, they resist distraction, rotation, and translation in position-specific ways.24,35–37 The IFL is the dominant anterior restraint, limiting extension and external rotation (ER); the PFL contributes restraint in abduction and ER; the ISFL primarily limits internal rotation (IR), particularly in flexion.24,31,35,36 The ZO forms a sling around the femoral neck, providing support for distraction resistance.34,35 Disruption—whether from arthroscopic capsulotomy, generalized hyperlaxity, or repetitive end-range loading in sport—can permit pathologic micromotion and symptoms consistent with microinstability.4–6,8,38
Ligamentum Teres
The ligamentum teres (LT) augments stability by resisting distraction and constraining rotation at high flexion angles.39,40 Although the LT’s contribution to microinstability is adjunctive rather than primary, LT pathology is observed frequently in athletes who perform extreme ROM.41 Addressing LT lesions in the context of optimized capsulolabral management leads to symptomatic improvement.42,43
Labrum
The acetabular labrum attaches to the rim, deepens the socket, and maintains the negative-pressure-suction effect that stabilizes the femoral head.31,34,44 The labrum also contributes to joint homeostasis by promoting lubrication.31,44 A primary role of the labrum is uniform pressure distribution, which protects the underlying cartilage.31,44 Labral injury or detachment compromises these functions and can manifest as microinstability.24,31,45 Restoration of labral sealing mechanics through repair or reconstruction is central to joint preservation.45,46
Hip Muscle Strength
Periarticular muscles act as dynamic stabilizers, compressing, steering, and controlling the joint.34 Key contributors include the deep external rotators (quadratus femoris, obturator internus/externus, superior/inferior gemelli), gluteus minimus/medius, and the iliocapsularis, which tensions the anterior capsule.34 Weakness, atrophy, or delayed activation of these muscles has been associated with impaired dynamic containment and modest increases in femoral-head translation at terminal ranges, thereby contributing to secondary microinstability. In conditions such as developmental dysplasia of the hip (DDH), atrophy or dysfunction can diminish compressive stability and exacerbate symptoms of microinstability.25,47
Diagnosis
History and Physical Examination
Diagnosing microinstability is challenging and benefits from a consistent, multi-pillar approach.2,18 Patients often report apprehension or giving way in extension, ER, and pain during rotational or end-range tasks.2,3,18 Particular attention is warranted for athletes who require prolonged hyperextension.3,18,48 A prior hip surgery is an additional clue when postoperative milestones are delayed with persistent pain, reflecting possible iatrogenic capsular defects or loss of the suction seal.11,32,49 Generalized ligamentous laxity (Beighton score) heightens suspicion.50,51
Distinguishing pathologic microinstability from nonpathologic generalized hypermobility requires a combined quantitative assessment rather than reliance on an isolated Beighton value.51,52 A Beighton score compatible with generalized hypermobility (commonly ≥4 in adults) increases the pretest probability but does not establish symptomatic microinstability.50,51 Integrate Beighton with dynamic and instrumented measures when available: (1) examination under anesthesia with axial distraction measurements (traction/distraction sensors or goniometric translation) to quantify excessive femoral head translation, (2) ultrasound-assisted axial distraction to visualize translation in real time in selected centers, and (3) diagnostic stress imaging to complement static radiographs in ambiguous cases.47,52,53 In combination, these elements help differentiate systemic laxity from focal loss of capsular or suction-seal function, strengthening a working case definition for symptomatic microinstability. (Recommendation: Conditional; GRADE: Low; LOE: III–V). A history of subjective instability remains an essential diagnostic element, particularly when corroborated by objective findings.3,25,52
A standardized sequence reduces guarding and improves reproducibility: gait and single-leg- stance → passive log-roll (capsular laxity) → Abduction-Hyperextension-External Rotation Test (AB-HEER) → Hyperextension-External Rotation (HEER) → prone instability, with contralateral comparison and localization of anterior apprehension.18,52 Examination under anesthesia often unmasks laxity.47,52,53 The senior author additionally uses axial distraction, with and without ultrasound, as an adjunct to confirm excessive translation in patients with normal femoral torsion.5,52,53 Patterns of cartilage damage often reflect femoral head micromotion, which may be sport-specific (“motions at risk”) or patient-specific, reinforcing integration of sport history and physical findings during assessment.2,25,54
Test Performance and Interpretation
The AB-HEER test shows the highest single-test accuracy (sensitivity, 80.6%; specificity, 89.4%).19,55 HEER is slightly lower (sensitivity 71.0%, specificity 85.1%) but is a reliable adjunct.19 The prone instability test has limited sensitivity (33.9%) but very high specificity (97.9%), making it a strong rule-in maneuver.2,18,19 The dial test identifies excessive ER without a firm endpoint; interpretation should be integrated with the Beighton score to avoid false positives in generalized hyperlaxity.18,19,47,53
Interobserver reproducibility for provocative tests varies with examiner training, standardized positioning, and case mix. AB-HEER and HEER demonstrate the highest reported diagnostic accuracy in single-center series; however, reproducibility metrics differ between studies.2,18,19,55 Trained examiners using a standardized sequence achieve moderate to substantial agreement, whereas novice performance is less consistent.2,18,19,55 Prone instability and dial tests are more operator-dependent (prone: low sensitivity, high specificity) and are best used as adjuncts rather than stand-alone screens.2,18,19,53 To reduce variability, we recommend a standardized, stepwise examination sequence and formal examiner training, with the examiner’s level documented in the record (Recommendation: Conditional; GRADE: Low; LOE: III). These clinical tests should be applied within a multi-pillar diagnostic strategy (history, imaging, intraoperative confirmation) rather than as single-test decision tools (Recommendation: Conditional; GRADE: Low; LOE: III). Table 1 summarizes test characteristics for patient counseling.
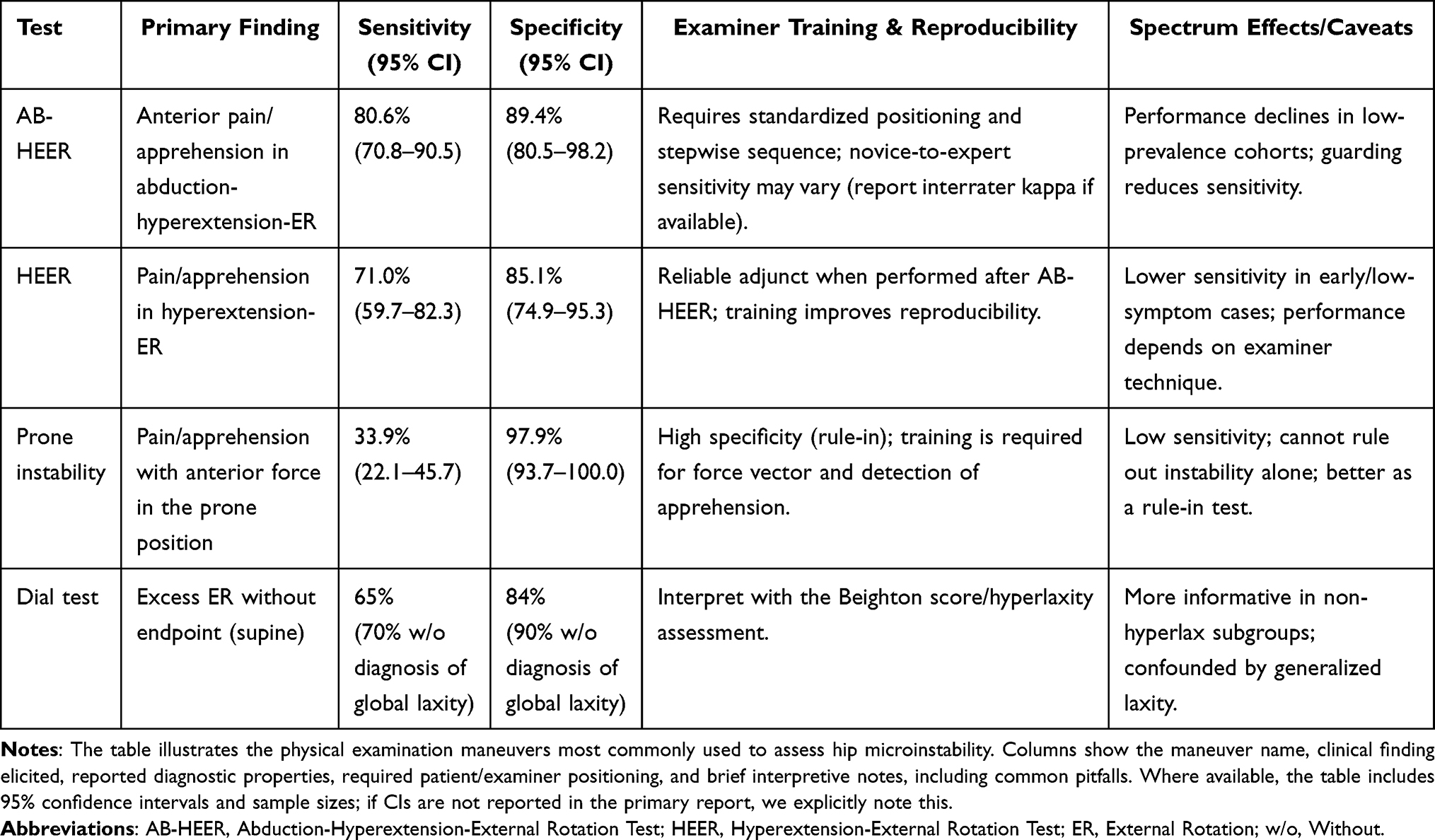 |
Table 1 Physical Examination Maneuvers for Microinstability |
Pragmatic Diagnostic Algorithm
We integrate four pillars with explicit thresholds and documentation, rather than a numeric score:
- History: activity-linked apprehension/giving-way in extension/external rotation with functional limitation; document generalized laxity (modified Beighton).50,51
- Physical examination: standardized sequence (gait, single-leg stance, log roll, AB-HEER, HEER, prone instability, dial) with contralateral comparison; interpret positive tests in combination.2,18,19,47,53,55
- Imaging: posture-standardized AP pelvis and false-profile for LCEA/Tönnis/Anterior Center Edge Angle (ACEA)/FEAR, with cross-sectional imaging when values are within ≤5° of thresholds; record pelvic tilt/rotation and limb position.28,56–58
- Intraoperative verification (when surgery is indicated): suction-seal assessment, drive-through sign, capsular redundancy/deficiency, and ease of distraction; apply a test–treat–retest workflow after labral repair and after capsular plication.21,30,59
Microinstability is probable when there is a characteristic history, plus at least two reproducible positive provocative tests and posture-standardized imaging consistent with under-containment or labral/capsular compromise, or when intraoperative loss of suction seal/drive-through sign corroborates symptoms. Otherwise classify as possible, prioritize nonoperative care, and pursue targeted reassessment (examination under anesthesia or ultrasound-assisted axial distraction may be used selectively to quantify translation)(Recommendation: Conditional; GRADE: Low; LOE: III–V).5,47,56–58
Emerging dynamic modalities, such as stress- or position-dependent magnetic resonance imaging (MRI) and three-dimensional functional computed tomography (CT), may quantify posture- and load-related changes in coverage and femoral head translation, complementing static indices. These applications are promising but remain investigational and warrant prospective validation with standardized acquisition protocols.34,47
Imaging: Indices, Positioning, and Consequences
Radiographs (anteroposterior [AP] pelvis and false-profile-views) allow LCEA, Tönnis angle, ACEA, and FEAR calculations.28,56,60–62 FEAR is helpful in borderline dysplasia (LCEA ≤25°) but is sensitive to pelvic tilt and limb position; document positioning and avoid single-value decisions.28,57,62 CT quantifies femoral and acetabular version.52,56,58 MRI and magnetic resonance arthrography (MRA) help evaluate structures that are poorly visualized on radiographs and CT, including the capsule, labrum, and LT, and can further assess articular cartilage.34,47 In dysplastic ranges, radiographs may underestimate coverage relative to CT; it is essential to recognize method-dependent measurement shifts.56 When the radiographic LCEA or Tönnis angle is within ≤5° of a classification threshold (eg, LCEA 18–25° borderline range), obtain cross-sectional imaging and document patient positioning (pelvic tilt/rotation), as AP radiographs can underestimate lateral coverage.56–58 This approach avoids misclassification and inappropriate selection of arthroscopy versus reorientation (GRADE: Low; LOE: III).56–58 Table 2 details thresholds, caveats, and clinical use.
 |
Table 2 Radiographic Indices and Clinical Use |
Intraoperative Confirmation and Phenotyping
Arthroscopy enables direct assessment of the suction seal, drive-through sign, focal capsular redundancy/deficiency, LT status, and ease of distraction.49,52 A test–treat–retest workflow—rechecking the seal after labral repair and again after capsular plication—aligns technical choices with observed function.21,30,52 Synthesizing intraoperative findings with history, examination, and imaging supports phenotype classification—coverage-dominant, torsion-dominant, or capsular-dominant-—which then guides the choice among arthroscopy, periacetabular osteotomy (PAO), staged/hybrid strategies, and adjunctive procedures (version correction, LT treatment).25,59
Management
Nonoperative Care
All patients with suspected microinstability should begin with nonoperative care consistent with FAIS/dysplasia pathways.2,48,63 First-line treatment includes targeted physical therapy and symptom or disability-guided activity modification.2,63 Emphasis typically includes: (1) strengthening hip abductors and deep external rotators; (2) anterior chain control to limit extension-ER stress; (3) lumbopelvic stability and kinetic-chain-mechanics; and (4) graded exposure to end-range tasks.48,63–65 Image-guided intra-articular injection can aid diagnosis and provide short-term relief.25 Targeted deep-rotator focus: because the deep external rotators act as dynamic joint-centers, rehabilitation should prioritize restoring compressive motor control (early low-load isometrics/closed-chain drills), progress to external-rotation strengthening at functional angles, and finish with neuromuscular re-education to reestablish timely activation and reduce secondary femoral-head translation.3 Protocols remain heterogeneous; microinstability-specific regimens require prospective validation. Progression should be criteria-based (apprehension-free ROM, strength symmetry, task tolerance), not time-based.16,64,65 Patients are often reassessed after 6–8 weeks; persistent symptoms may warrant discussion of surgical options.48,52,63
Surgical Management & Outcomes
Hip microinstability is rarely the sole indication for surgery.26,49 Hip preservation procedures typically occur in the setting of concomitant FAIS, borderline dysplasia, or symptomatic hyperlaxity.25,51
Bone—Containment, Iatrogenesis, and Outcomes
Bony architecture contributes to passive containment and influences the risk-benefit calculation for resective procedures.66,67 Resection for cam or pincer morphology is calibrated to relieve conflict while guarding against destabilization in instability-dominant phenotypes.68,69 Excessive cam resection can induce microinstability; case series and technique reports describe femoral head-neck soft-tissue remplissage as a salvage maneuver to re-establish contour and sealing mechanics.32,33,70 Current evidence is limited and early (single-center case series/technical notes, short follow-up, and no robust comparators), so its use should be conditional rather than routine (GRADE very low; Level IV).32,33,70 Candidate profiles include revision hips with documented over-resection and intraoperative suction-seal failure, focal head–neck contour defects amenable to soft-tissue filling, and absence of advanced chondral loss or substantial undercoverage that would favor bony reconstruction or arthroplasty.32,33,70 Early reports describe symptomatic improvement and favorable patient-reported outcomes (PROs) after remplissage; however, available data are largely limited to single-center case series and technical notes, with limited follow-up and no high-quality comparative trials.32,33,70 Outcomes data on revision rates, sport-specific performance, and total hip arthroplasty (THA) conversion remain sparse.32,33,70 In addition, studies of primary FAIS correction in patients with borderline instability show variable survivorship and THA-conversion rates across cohorts, and surgeon/institutional factors (including case volume and selection thresholds) modify observed outcomes, which argues for caution in making blanket procedural recommendations without larger, multicenter, and disease-specific cohorts.69,71,72
Hip Capsule—Components, Stewardship, and Outcomes
The hip capsule (IFL, PFL, ISFL; ZO) provides bulk restraint to rotation and translation, contributing to the suction seal.24,35 Because arthroscopic capsulotomy compromises these restraints, contemporary protocols advocate re-establishing capsular continuity with complete hip capsular repair/closure or plication (Expert consensus; GRADE quality: Very low; Evidence level: V).8,21,31 Comparative pooled reviews and meta-analyses of predominantly observational cohorts report overall superior patient-reported outcomes and improved survivorship with complete capsular closure versus non-closure, but these syntheses combine heterogeneous single-center series, retrospective matched cohorts, and differing definitions of closure, producing variable effect sizes and limited causal inference (Comparative data; GRADE quality: Low; Evidence level: III–IV [retrospective matched cohorts/case series]).11,13,73,74 Some multicenter datasets and adjusted analyses reveal smaller or non-significant differences for specific endpoints (including THA conversion) after accounting for patient factors and surgeon volume, suggesting that capsular management is one of several interdependent variables influencing outcomes, rather than a universally decisive intervention.75
Observational series consistently implicate incomplete capsular closure or capsular deficiency in reoperation among younger, hyperlax, or revision patients, supporting a risk-stratified approach to capsule stewardship (Comparative data + expert synthesis; GRADE quality: Low; Evidence level: III–IV).14,30 Short- to mid-term THA conversion is uncommon, and several series report lower THA conversion rates after capsular repair/closure compared to non-repair, although findings vary by cohort and follow-up duration.11,12,72,76
In high-level athletic cohorts, complete capsular closure has been associated with a faster time to criteria-based return to play and a higher return rate compared with non-closure in single-center studies.15–17 Reported overall return-to-sport (RTS) rates after arthroscopy with repair/capsule closure commonly range from 70% to 90%, with 50% to 70% returning to the same competitive level in pooled and systematic reviews, recognizing wide heterogeneity across studies.15,16,77,78
While complete capsular closure after hip arthroscopy generally restores axial distraction resistance and is associated with improved clinical outcomes, excessive capsular tension or aggressive plication may alter physiologic kinematics and predispose patients to postoperative stiffness or capsulorrhaphy-related morbidity.79 Cadaveric and clinical reports demonstrate that different suture techniques and degrees of imbrication variably change joint laxity and range of motion, with some plication constructs producing measurable reductions in external rotation and end-range motion.80 Case series and technique reviews also document that overtightening can contribute to adhesive-like capsular stiffness and reduced functional ROM.4,68,81 Therefore, intraoperative calibration of capsular tension—aiming to reconstitute near-native distraction resistance and rotational freedom rather than maximal tautness—is recommended.4,68,81 Passive rotation testing should be performed after repair and compared with the native or contralateral baseline, and objective adjuncts (traction-force logs, calibrated suture tensioners, intraoperative fluoroscopic measurements) should be incorporated to reduce the risk of over-constraint.4,68,81
The incremental value of routine, complete closure in non-hyperlax, non-dysplastic FAIS remains mixed: some cohorts show similar PROs and RTS to selective closure when stability is otherwise addressed, whereas others report modest reductions in failure or revision with complete closure and/or plication.12–14,82,83 Taken together, the balance of evidence favors closure where feasible and in at-risk hips, but equipoise persists in clearly nondysplastic, non-hyperlax FAIS; effect sizes are small and technique-dependent (closure versus imbrication, suture configuration, rehabilitation protocol).68,84
Labrum—Implications, Repair, Reconstruction, and Augmentation
The labrum is a fibrocartilaginous ring that deepens the socket and maintains the suction seal; loss of this seal increases micromotion and pain.8,44 The primary surgical goal in instability-leaning phenotypes is to restore sealing mechanics: repair when tissue is viable, augment when tissue is thin or hypoplastic, and reconstruct when tears are irreparable, rim work is minimized to preserve coverage.45,85
Across comparative cohorts, labral preservation outperforms debridement on PROs, with lower reoperation rates.45,46,85,86 A multicenter series with a follow-up of> 10 years in selected cohorts with borderline dysplasia reports sustained benefit when sealing mechanics are restored.69,71,87
Augmentation (eg, IT band allograft) is increasingly used for insufficient labral tissue and has shown encouraging PRO gains and sealing restoration in early cohorts; however, microinstability-specific data are limited. Observational series suggest favorable short- to mid-term PROs and RTS after augmentation in carefully selected patients; however, comparative data versus repair are heterogeneous and technique-dependent, and universally accepted thickness thresholds are lacking.88–92 MRI millimetric cut-points and arthroscopic grading vary across studies.93,94 Augmentation can restore the seal and reduce the retear risk in low-volume labra; however, repair may suffice when tissue quality is adequate.91,95,96 Equipoise remains, and trials with predefined thickness criteria and core outcome sets are needed.89,94,97,98
Ligamentum Teres—Function, Indications, and Outcomes
The LT provides measurable end-range rotational restraint and contributes to distraction resistance, particularly in high flexion/adduction/external-rotation positions.39,40 Debridement may relieve symptoms from partial or degenerative tears; LT reconstruction (auto/allograft) is reserved for refractory instability after labral and capsular optimization.42
Systematic reviews and ≥ 2-year series report short-term improvements in PROs, with reoperation rates of approximately 10–20% and limited long-term survivorship data.42,99 LT reconstruction better serves as an adjunct rather than a primary stabilizing procedure.43,100 RTS following LT reconstruction is inconsistent and commonly reported to be around 40–60% in available series.43,100 Given variable outcomes and lower-level evidence, LT reconstruction is best viewed as an adjunctive procedure rather than a stand-alone stabilizer.
Biomechanically, LT contribution is modulated by structural morphology (length, cross-sectional area, and insertional integrity) and by the status of the capsulolabral complex.39,40 Shorter or thicker LTs tend to demonstrate greater stiffness and higher load-to-failure, whereas attenuated ligaments engage later and tolerate lower loads, predisposing to earlier terminal rotation.39,40 For these reasons, LT reconstruction is most rational when (1) labral seal and capsular function have been optimized but symptomatic end-range rotational laxity persists, (2) imaging or arthroscopy documents marked LT attenuation or partial absence, and (3) intraoperative testing shows persistent excess terminal rotation or drive-through despite repair and plication.42,43 Routine primary LT reconstruction is not supported by high-level evidence; morphology-informed selection (MRI/arthroscopic measurement of LT length and cross-sectional area (CSA) plus quantitative intraoperative rotation testing) strengthens mechanistic justification and should be incorporated into future comparative studies.
Borderline Dysplasia—Arthroscopy Versus Periacetabular Osteotomy, Selection, and Outcomes
For hips with LCEA 18–25°, both arthroscopy (labral preservation with meticulous hip capsular plication) and PAO can improve outcomes when selection is phenotype-guided (GRADE: Low; LOE: III).59,101–103 Arthroscopy is suitable for impingement-dominant patterns with manageable coverage, whereas PAO is favored when undercoverage and instability predominate (eg, positive FEAR, elevated Tönnis angle, symptomatic laxity) or when significant version abnormalities exist—often in a staged or combined fashion.29,87,104,105
Propensity-matched cohorts with ≥ 5-year follow-up report comparable PROs when selection is appropriate, but PAO tends to yield lower THA conversion, where undercoverage is the root cause. Arthroscopy often provides faster early functional recovery but carries a higher likelihood of revision if residual instability or undercoverage is not corrected.59,102,106 Given heterogeneity in cohort definitions, imaging metrics, and sequencing, prospective comparative studies that stratify borderline hips by LCEA and version, report standardized torsion metrics (CT/3D imaging), and compare arthroscopy, PAO, and staged/combined strategies with mid- to long-term survivorship and revision endpoints are required to refine selection algorithms.
Rehabilitation, Return to Sport, and Global Synthesis
Rehabilitation
Rehabilitation translates structural restoration into functional readiness and should prioritize early motion, progressive load restoration, and objective criteria-based progression. Early postoperative circumduction—initiated as passive motion in the immediate postoperative period (recovery room/first 24–48 hours) and progressed to active-assisted circumduction during the first 2–4 weeks, is recommended to reduce intra-articular adhesions after hip arthroscopy.15,16,64,65,107 In a large series examining adhesions as an outcome, symptomatic adhesions accounted for approximately 4.8% of revisions. The omission of an early circumduction protocol in the immediate postoperative period was associated with a fourfold increase in adhesion rate in that cohort.107,108 Because most clinically relevant adhesions manifest in the early postoperative months, clinicians should document initiation timing and frequency of circumduction (passive in Post Anesthesia Care Unit → several daily active-assisted sets during weeks 1–4) as part of routine rehabilitation to reduce the risk of adhesions and the need for early re-intervention.15,16,107,108
Progression through phases of rehabilitation should be anchored to objective, apprehension-free, and symmetric measures of range of motion and strength, rather than fixed calendar milestones.16,64,65 We recommend a multi-domain, criteria-based battery to inform RTS decisions that explicitly incorporates psychological readiness, objective neuromuscular function, and a simple neurocognitive/dual-task assessment.
Recommended RTS Battery (Provisional; Pragmatic)
- Psychological readiness: Hip-Return to Sport after Injury scale (Hip-RSI) with provisional operational cut-point ≥90/100 indicating high readiness (interpret in clinical context).64,65
- Strength and power: Limb symmetry index (LSI) ≥90% on objective strength testing (hand-held dynamometry) and hop tests.16
- Balance/motor control: Y-Balance anterior-reach interlimb asymmetry <4 cm (or normalized composite reach ≥94% when using limb-length normalization).54
- Dual-task assessment: Dual-task cost (DTC) on an agility or hop task: DTC (%) = ((single-task − dual-task) / single-task) × 100; provisional threshold DTC ≤10%. Values greater than 10% suggest a meaningful decrement and warrant targeted neuromotor and neurocognitive training.64
The Hip-RSI is validated in hip arthroscopy cohorts and correlates with RTS level; a provisional operational cut-point of ≥90/100 indicates high psychological readiness, but this must be interpreted in the broader clinical context.64,65 Psychological readiness should be combined with pragmatic functional thresholds: (1) LSI ≥90% for hop tests and for objective strength testing (hand-held dynamometry); (2) Y-Balance anterior-reach interlimb asymmetry <4 cm (or normalized composite reach ≥94% when using limb-length normalization); and (3) satisfactory performance across a composite battery of hop, strength, and balance tests before initiating sport-specific progression.54,65
Operational rule for activity-specific clearance (rule-in checklist): Hip-RSI ≥90/100 + LSI ≥90% on strength and hop tests + Y-Balance anterior asymmetry <4 cm + DTC ≤10%. If any element is unmet, continue targeted rehabilitation (psychological support, neuromuscular retraining, dual-task drills, and graded sport-specific exposure) and reassess. Document examiner level (fellow/attending vs trainee), baseline measures, and sport classification (cutting/contact vs flexibility/endurance vs asymmetric/overhead) to personalize thresholds. These cut-points are pragmatic and conditional, operationalizing criterion-based clearance but reflecting a largely observational evidence base (GRADE: Low; LOE: III–V).54,64,65
Return-to-Sport
RTS definitions vary; clearance is best based on objective criteria and tailored to the demands of the sport, particularly for activities that load extension and ER at end range.15,16 Pooled estimates from systematic reviews and meta-analyses report an overall RTS rate after hip arthroscopy of approximately 84.6% (95% CI, 80.4–88.8), with a mean time to return of around 7.4 months. Pooled estimates for return to the same competitive level are lower and more variable.15–17,54 Sex and sports categories significantly alter these probabilities. In one collegiate cohort, female athletes returned at higher rates than males (female, 93% vs male, 82%; odds ratio [OR], 2.8; 95% CI, 1.00–7.82), although pooled analyses report inconsistent sex effects, reflecting low certainty and cohort dependence.17,109,110 Sport-type effects are directionally consistent: flexibility/technical athletes (dancers, gymnasts) and some endurance athletes commonly demonstrate the highest any-sport RTS (pooled series reporting 94.8% in flexibility athletes), whereas cutting and contact sports show lower same-level return rates and longer timelines (mean times to RTS in cutting sports reported 8.5 ± 1.9 months in select series).54,77
After PAO, RTS typically occurs later (approximately 9–12 months) and at lower rates (approximately 60–80%), reflecting the magnitude of structural correction and recovery.102,111 Clinicians should provide sport- and sex-specific counseling, emphasize criterion-based functional clearance rather than calendar time, discuss cartilage status and psychological readiness as major modifiers, and frame expectations as conditional, given the predominantly observational evidence base.15,16,112
Synthesis
Sustained improvement depends on reconstituting labral sealing mechanics, re-establishing capsular tension with complete closure or plication, and calibrating bony correction to the presenting phenotype.11,12,45 When labral preservation is combined with complete capsular closure, revision and THA conversion rates are generally lowest—particularly in impingement-dominant- morphologies.11,14,113 Arthroscopy with repair/closure tends to yield the highest and earliest RTS; PAO offers structural stability and lower THA conversion when undercoverage is primary, albeit with slower return; revision strategies such as remplissage or LT reconstruction show more modest RTS and uncertain durability.15,32,43,100,102 A summary of outcome comparison by procedure is provided in Table 3.
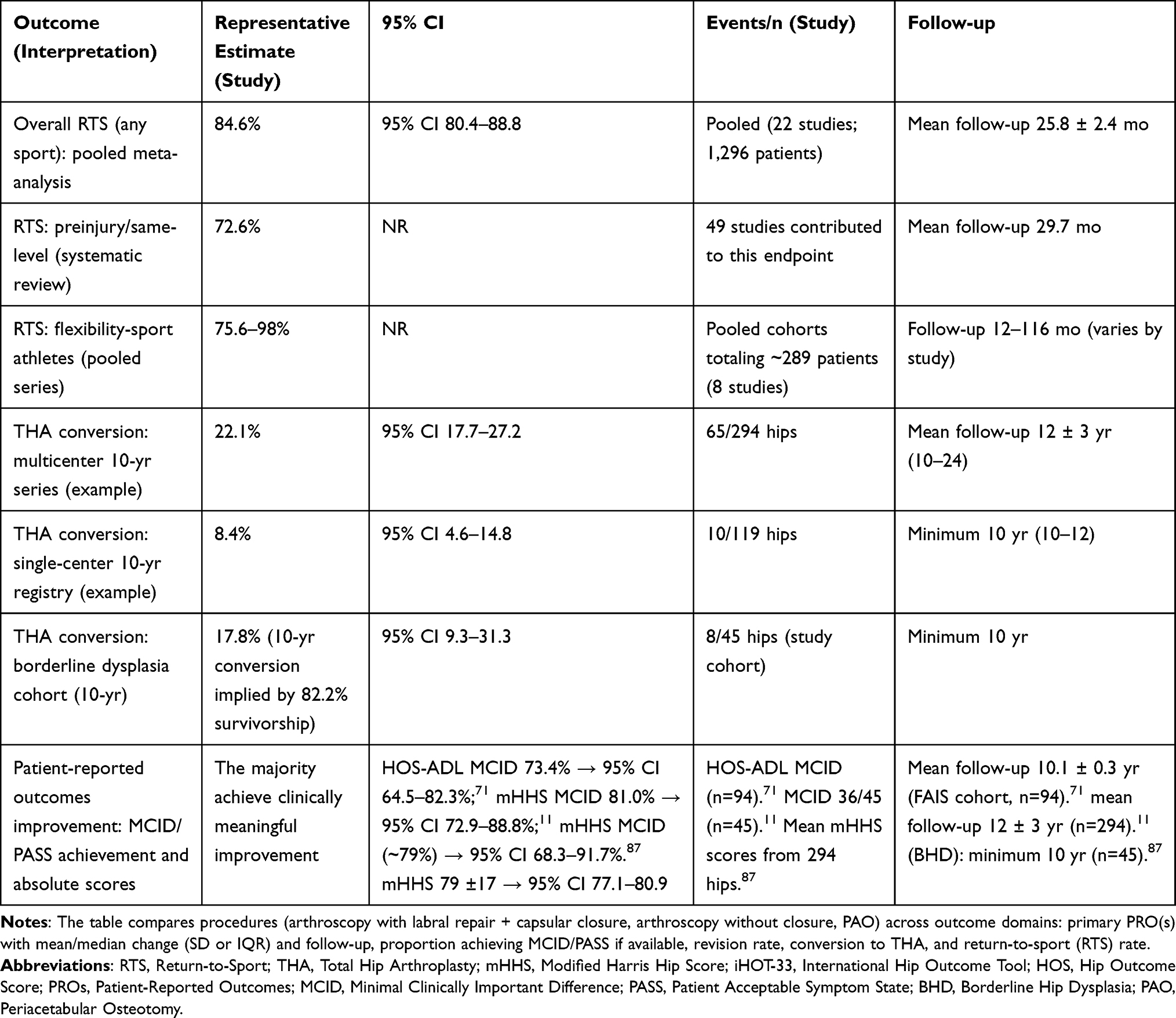 |
Table 3 Outcomes Overview |
Clinical decision-making should therefore prioritize phenotype-matching interventions, transparent documentation of imaging positioning and torsion metrics, intraoperative functional testing (such as suction-seal, drive-through, and ease of distraction), and standardized, criteria-based rehabilitation pathways. These elements will reduce practice variation and improve the interpretability of outcome data across centers.
Limitations of the Evidence
The current evidence is dominated by retrospective or matched cohort studies.2,102 Randomized controlled trials are rare, given the need for equipoise and the requirement for crossover.2 Without RCTs, outcomes are easily influenced by surgeon preference, heterogeneous rehabilitation protocols, and selection bias.2,102 Imaging-derived indexes/values such as FEAR are sensitive to pelvic and limb position and display variable reproducibility.28,34,62,114 Microinstability-specific PRO instruments are scarce, and sex- and sport-stratified RTS reporting is inconsistent.17,64,65 These limitations underscore the need for multicenter prospective registries with standardized imaging protocols, explicit operative reporting (including capsular construct and tensioning), and standardized rehabilitation pathways.59,111,115
Future Directions and Research Agenda
A coordinated research agenda should couple a precise taxonomy with pragmatic study designs.2,115 This can be achieved by taking a multi-step approach.2 First, replace binary labels with a phenotype-based lexicon (coverage, torsion, and capsular-dominant) and adopt uniform failure endpoints—revision arthroscopy, PAO conversion, THA, and failure to achieve the minimal clinically important difference (MCID)/patient acceptable symptomatic state (PASS)—to reduce heterogeneity and enable aggregation.66 Second, develop objective laxity metrics: instrumented examination and standardized axial-stress testing under anesthesia, position-controlled FEAR (or corrected FEAR), and dynamic imaging (stress MRI/functional CT) to bridge static indices and symptomatic translation.34,47,62,114 Third, prioritize comparative effectiveness at scale: multicenter registries with common data elements and propensity methods to clarify the incremental value of complete versus partial closure, suture number/vector, and labral reconstruction versus augmentation/repair in instability-dominant phenotypes, and to refine indications for arthroscopy versus PAO in borderline dysplasia.11,12,59,102 Fourth, prevent iatrogenesis: delineate safe cam resection envelopes in instability-prone hips and evaluate indications and durability for femoral head–neck remplissage after over-resection-, including sport-specific functional metrics sensitive to end-range ER/extension demands.32,33,70
Fifth, define LT reconstruction candidacy and durability (graft choice, fixation, interaction with capsular plication, survivorship beyond mid-term, and sport-specific performance).42,43,99,100 Sixth, advance rehabilitation science: create microinstability-specific rehabilitation algorithms and criteria based on RTS batteries with sex/sport/level stratification; test early circumduction and controlled early motion for adhesion mitigation without compromising stability.16,64,65 Lastly, address equity and sex differences by prospectively reporting outcomes by sex, hyperlaxity spectrum (eg, Ehlers–Danlos syndrome), sport, and competitive level to enable individualized counseling and reduce disparities.17,25 A targeted gap exists in the role of dynamic stabilizers (eg, gluteus medius/minimus, iliocapsularis) in microinstability; mechanistic and interventional work is needed.35
Conclusion
Hip microinstability lies between physiologic laxity and frank instability and often coexists with FAIS or borderline dysplasia.1,25 Accurate diagnosis emerges from the convergence of history, examination, imaging, and intraoperative assessment, rather than relying on any single test.2,18,52 Contemporary surgical care centers on the labrum-capsule-LT stability continuum, focusing on restoring the suction seal, re-establishing capsular restraint with complete closure or plication, and correcting bony morphology judiciously within a phenotype-guided algorithm (GRADE: Very low; LOE: V–III).12,42,45 Rehabilitation should be criteria-based, with early motion strategies (eg, circumduction) to limit adhesions.16,63 Many athletes return to sport after arthroscopy with repair/closure, although the same-level return rate is variable and slower after PAO; revision strategies yield lower return rates.15,17 Future progress hinges on standard definitions, objective laxity measurement, multicenter comparative-effectiveness- research, and rehabilitation trials tailored to microinstability—with specific attention to the unanswered role of dynamic stabilizers and the durability of LT reconstruction and femoral head-neck remplissage.16,53,59,66,115
Disclosure
Dr Marc Philippon reports research supports from National Institute of Health, National Institute of Arthritis and Musculoskeletal and Skin Disease, National Institute of Aging, US Department of Defense, Smith + Nephew, Inc, Ossur, Arthrex, Siemens; shareholder of Arthrosurface, MIS, Vail Valley Medical Center, Vail MSO Holdings LLC, Effrx, MJP Innovations, Inc, Olatec, iBalance, Stryker, Trimble, Grocery Outlet, 3M, Bristol Myers Squibb, Pfizer, AbbVie, AbbVie, Johnson & Johnson; personal fees from NICE Recovery Systems, hospitality payments from HydroCision, ownership of MJP Innovations, LLC, investor of Manna Tree Partners, outside the submitted work. In addition, Dr Marc Philippon has a patent US 20210046123 A1 pending to Steadman Philippon Research Institute; royalties from Bledsoe, ConMed Linvatec, DJO, Arthrosurface, Slack Inc., Elsevier, Smith + Nephew, Inc; and Board Member of Vail Health Services, Vail Valley Surgery Center-Governing, ISHA, Orthopedics Today; advisory for AJSM; editorial co-chairman for Steadman Philippon Research Institute. The authors report no other conflicts of interest in this work.
References
1. Boykin RE, Anz AW, Bushnell BD, Kocher MS, Stubbs AJ, Philippon MJ. Hip instability. J Am Acad Orthop Surg. 2011;19(6):340–349. doi:10.5435/00124635-201106000-00004
2. Cohen D, Jean PO, Patel M, et al. Hip microinstability diagnosis and management: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2023;31(1):16–32. doi:10.1007/s00167-022-06976-7
3. Curtis DM, Murray IR, Money AJ, Pullen WM, Safran MR. Hip microinstability: understanding a newly defined hip pathology in young athletes. Arthroscopy. 2022;38(2):211–213. doi:10.1016/j.arthro.2021.12.001
4. Philippon MJ, Trindade CAC, Goldsmith MT, et al. Biomechanical assessment of hip capsular repair and reconstruction procedures using a 6 degrees of freedom robotic system. Am J Sports Med. 2017;45(8):1745–1754. doi:10.1177/0363546517697956
5. Khair MM, Grzybowski JS, Kuhns BD, Wuerz TH, Shewman E, Nho SJ. The effect of capsulotomy and capsular repair on hip distraction: a cadaveric investigation. Arthroscopy. 2017;33(3):559–565. doi:10.1016/j.arthro.2016.09.019
6. Abrams GD, Hart MA, Takami K, et al. biomechanical evaluation of capsulotomy, capsulectomy, and capsular repair on hip rotation. Arthroscopy. 2015;31(8):1511–1517. doi:10.1016/j.arthro.2015.02.031
7. Wuerz TH, Song SH, Grzybowski JS, et al. Capsulotomy size affects hip joint kinematic stability. Arthroscopy. 2016;32(8):1571–1580. doi:10.1016/j.arthro.2016.01.049
8. Jimenez AE, Owens JS, Shapira J, et al. Hip capsular management in patients with femoroacetabular impingement or microinstability: a systematic review of biomechanical studies. Arthroscopy. 2021;37(8):2642–2654. doi:10.1016/j.arthro.2021.04.004
9. Philippon MJ. The role of arthroscopic thermal capsulorrhaphy in the hip. Clin Sports Med. 2001;20(4):817–830. doi:10.1016/S0278-5919(05)70287-8
10. Hoffer AJ, Beel W, KCG N, Degen RM. The contribution of soft tissue and bony stabilizers to the hip suction seal: a systematic review of biomechanical studies. Am J Sports Med. 2024;52(10):2657–2666. doi:10.1177/03635465231208193
11. Boos AM, Wang AS, Lamba A, et al. Long-term outcomes of primary hip arthroscopy: multicenter analysis at minimum 10-year follow-up with attention to labral and capsular management. Am J Sports Med. 2024;52(5):1144–1152. doi:10.1177/03635465241234937
12. Carbone AD, Prabhavalkar O, Chishti Z, Curley AJ, Parsa A, Domb BG. Hip capsular repair results in improved patient-reported outcomes and survivorship: a systematic review of the literature. Arthroscopy. 2023;39(2):488–497. doi:10.1016/j.arthro.2022.11.013
13. Phillips MK, Abouhaif T, Waters TL, et al. Routine capsular closure outperforms incomplete capsular closure after hip arthroscopy: a meta-analysis and expected-value decision analysis. Arthroscopy. 2025;41(7):2551–2564.e2554. doi:10.1016/j.arthro.2024.11.080
14. Beck EC, Nwachukwu BU, Chahla J, Clapp IM, Jan K, Nho SJ. Complete capsular closure provides higher rates of clinically significant outcome improvement and higher survivorship versus partial closure after hip arthroscopy at minimum 5-year follow-up. Arthroscopy. 2021;37(6):1833–1842. doi:10.1016/j.arthro.2021.01.035
15. O’Connor M, Minkara AA, Westermann RW, Rosneck J, Lynch TS. Return to play after hip arthroscopy: a systematic review and meta-analysis. Am J Sports Med. 2018;46(11):2780–2788. doi:10.1177/0363546518759731
16. Davey MS, Hurley ET, Davey MG, et al. Criteria for return to play after hip arthroscopy in the treatment of femoroacetabular impingement: a systematic review. Am J Sports Med. 2022;50(12):3417–3424. doi:10.1177/03635465211038959
17. Nishimura H, Comfort S, Brown J, et al. Females have higher return-to-sport rate than males among collegiate athletes after hip arthroscopy for femoroacetabular impingement due to the difference in the type of sports, type of impingement, and prevalence of severe cartilage damage. Arthroscopy. 2025;41(7):2320–2329. doi:10.1016/j.arthro.2024.10.016
18. Khanduja V, Darby N, O’Donnell J, Bonin N, Safran MR. Diagnosing Hip Microinstability: an international consensus study using the Delphi methodology. Knee Surg Sports Traumatol Arthrosc. 2023;31(1):40–49. doi:10.1007/s00167-022-06933-4
19. Reiman MP, Décary S, Mathew B, Reiman CK. Accuracy of clinical and imaging tests for the diagnosis of hip dysplasia and instability: a systematic review. J Orthop Sports Phys Ther. 2019;49(2):87–97. doi:10.2519/jospt.2019.8476
20. Bolia I, Chahla J, Locks R, Briggs K, Philippon MJ. Microinstability of the Hip: a previously unrecognized pathology. Muscles Ligaments Tendons J. 2016;6(3):354–360. doi:10.32098/mltj.03.2016.11
21. Chahla J, Mikula JD, Schon JM, et al. Hip capsular closure: a biomechanical analysis of failure torque. Am J Sports Med. 2017;45(2):434–439. doi:10.1177/0363546516666353
22. Sakai S, Kutsuna T, Kono K, Kinoshita T, Mashima N, Takao M. Femoral head translation in borderline and definite dysplastic hips during weight‐bearing: 2D/3D image registration analysis. J. Exp. Orthop. 2023;10(1). doi:10.1186/s40634-023-00707-8
23. Dantas P, Gonçalves RS, Grenho A, et al. Hip joint contact pressure and force: a scoping review of in vivo and cadaver studies. Bone & Joint Res. 2023;12(12):712–721. doi:10.1302/2046-3758.1212.BJR-2022-0461.R2
24. van Arkel RJ, Amis AA, Cobb JP, Jeffers JR. The capsular ligaments provide more Hip rotational restraint than the acetabular labrum and the ligamentum teres: an experimental study. Bone Joint J. 2015;97–b(4):484–491.
25. Kraeutler MJ, Safran MR, Scillia AJ, Ayeni OR, Garabekyan T, Mei-Dan O. A contemporary look at the evaluation and treatment of adult borderline and frank hip dysplasia. Am J Sports Med. 2020;48(9):2314–2323. doi:10.1177/0363546519881411
26. Nepple JJ. Editorial commentary: at the intersection of borderline dysplasia and femoroacetabular impingement-which way should we turn? Arthroscopy. 2020;36(4):1185–1188. doi:10.1016/j.arthro.2020.01.023
27. Cohen D, Ifabiyi M, Mathewson G, et al. The radiographic femoroepiphyseal acetabular roof index is a reliable and reproducible diagnostic tool in patients undergoing hip-preservation surgery: a systematic review. Arthroscopy. 2023;39(4):1074–1087.e1071. doi:10.1016/j.arthro.2022.11.041
28. Jud L, Neopoulos G, Dimitriou D, Zingg PO. Femoro-epiphyseal acetabular roof index values on anteroposterior pelvic radiographs significantly increase with hip adduction and decrease with abduction. Arthroscopy. 2024;40(8):2197–2203. doi:10.1016/j.arthro.2023.12.013
29. Shah A, Kay J, Memon M, et al. Clinical and radiographic predictors of failed Hip arthroscopy in the management of dysplasia: a systematic review and proposal for classification. Knee Surg Sports Traumatol Arthrosc. 2020;28(4):1296–1310. doi:10.1007/s00167-019-05416-3
30. Huntley SR, Villegas Meza AD, Nocek MJ, Philippon MJ. Hip arthroscopy and the capsule: why repair remains central to my approach. Arthroscopy. 2025;41:4542–4543. doi:10.1016/j.arthro.2025.07.033
31. Myers CA, Register BC, Lertwanich P, et al. Role of the acetabular labrum and the iliofemoral ligament in Hip stability: an in vitro biplane fluoroscopy study. Am J Sports Med. 2011;39:85s–91s. doi:10.1177/0363546511412161
32. Ruzbarsky JJ, Noorzad A, Felan NA, Philippon MJ. Revision hip arthroscopy terrible triad: capsular deficiency, labral deficiency, and femoral over-resection. Arthroscopy. 2025;41(2):164–165. doi:10.1016/j.arthro.2024.11.001
33. Hatakeyama A, Utsunomiya H, Nishikino S, et al. Predictors of poor clinical outcome after arthroscopic labral preservation, capsular plication, and cam osteoplasty in the setting of borderline hip dysplasia. Am J Sports Med. 2018;46(1):135–143. doi:10.1177/0363546517730583
34. Flores DV, Foster RCB, Sampaio ML, Rakhra KS. Hip capsulolabral complex: anatomy, disease, mri features, and postoperative appearance. Radiographics. 2024;44(2):e230144. doi:10.1148/rg.230144
35. van Arkel RJ, Amis AA, Jeffers JR. The envelope of passive motion allowed by the capsular ligaments of the Hip. J Biomech. 2015;48(14):3803–3809. doi:10.1016/j.jbiomech.2015.09.002
36. Martin HD, Khoury AN, Schröder R, et al. Contribution of the pubofemoral ligament to hip stability: a biomechanical study. Arthroscopy. 2017;33(2):305–313. doi:10.1016/j.arthro.2016.07.025
37. Burkhart TA, Baha P, Blokker A, et al. Hip capsular strain varies between ligaments dependent on both hip position- and applied rotational force. Knee Surg Sports Traumatol Arthrosc. 2020;28(10):3393–3399. doi:10.1007/s00167-020-06035-z
38. Weber AE, Neal WH, Mayer EN, et al. Vertical extension of the t-capsulotomy incision in hip arthroscopic surgery does not affect the force required for hip distraction: effect of capsulotomy size, type, and subsequent repair. Am J Sports Med. 2018;46(13):3127–3133. doi:10.1177/0363546518800710
39. Martin HD, Hatem MA, Kivlan BR, Martin RL. Function of the ligamentum teres in limiting Hip rotation: a cadaveric study. Arthroscopy. 2014;30(9):1085–1091. doi:10.1016/j.arthro.2014.04.087
40. Jo S, Hooke AW, An KN, Trousdale RT, Sierra RJ. Contribution of the ligamentum teres to hip stability in the presence of an intact capsule: a cadaveric study. Arthroscopy. 2018;34(5):1480–1487. doi:10.1016/j.arthro.2017.12.002
41. Wu JY, Li W, Xu LY, Zheng G, Chen XD, Shen C. Ligamentum teres tears and increased combined anteversion are associated with hip microinstability in patients with borderline dysplasia. Arthroscopy. 2024;40(3):745–751. doi:10.1016/j.arthro.2023.06.041
42. de SD, Phillips M, Philippon MJ, Letkemann S, Simunovic N, Ayeni OR. Ligamentum teres injuries of the Hip: a systematic review examining surgical indications, treatment options, and outcomes. Arthroscopy. 2014;30(12):1634–1641. doi:10.1016/j.arthro.2014.06.007
43. Shapira J, Yelton MJ, Rosinsky PJ, et al. ligamentum teres reconstruction may lead to improvement in outcomes following a secondary hip arthroscopy for symptomatic microinstability: a systematic review. Arthroscopy. 2021;37(6):1811–1819.e1811. doi:10.1016/j.arthro.2021.01.022
44. Bsat S, Frei H, Beaulé PE. The acetabular labrum: a review of its function. Bone Joint J. 2016;98(6):730–735. doi:10.1302/0301-620X.98B6.37099
45. Cooper JD, Dekker TJ, Ruzbarsky JJ, Pierpoint LA, Soares RW, Philippon MJ. Autograft versus allograft: the evidence in hip labral reconstruction and augmentation. Am J Sports Med. 2021;49(13):3575–3581. doi:10.1177/03635465211042633
46. Larson CM, Dean RS, McGaver RS, Seiffert KJ, Giveans MR. Arthroscopic debridement versus refixation of the acetabular labrum associated with femoroacetabular impingement: updated mean 7-year follow-up. Am J Sports Med. 2022;50(3):731–738. doi:10.1177/03635465211067818
47. Guimarães JB, Arruda PHC, Cerezal L, et al. Hip microinstability: new concepts and comprehensive imaging evaluation. Radiographics. 2025;45(7):e240134. doi:10.1148/rg.240134
48. Seijas R, Barastegui D, López-de-Celis C, et al. Preoperative risk factors in Hip arthroscopy. Knee Surg Sports Traumatol Arthrosc. 2021;29(5):1502–1509. doi:10.1007/s00167-021-06484-0
49. Domb BG, Philippon MJ, Giordano BD. Arthroscopic capsulotomy, capsular repair, and capsular plication of the Hip: relation to atraumatic instability. Arthroscopy. 2013;29(1):162–173. doi:10.1016/j.arthro.2012.04.057
50. Devitt BM, Harrington C. Editorial commentary: patients with thin hip capsules, capsular redundancy, capsular defects, hypermobility, dysplasia, and female patients are at increased risk of hip instability. Arthroscopy. 2022;38(12):3141–3142. doi:10.1016/j.arthro.2022.06.013
51. Saadat AA, Lall AC, Battaglia MR, Mohr MR, Maldonado DR, Domb BG. Prevalence of generalized ligamentous laxity in patients undergoing hip arthroscopy: a prospective study of patients’ clinical presentation, physical examination, intraoperative findings, and surgical procedures. Am J Sports Med. 2019;47(4):885–893. doi:10.1177/0363546518825246
52. Safran MR, Murray IR, Andrade AJ, et al. Criteria for the operating room confirmation of the diagnosis of hip instability: the results of an international expert consensus conference. Arthroscopy. 2022;38(10):2837–2849.e2832. doi:10.1016/j.arthro.2022.03.027
53. Parvaresh KC. Editorial commentary: axial stress examination under anesthesia provides a highly reliable test for measurement of hip distraction. Arthroscopy. 2022;38(5):1478–1479. doi:10.1016/j.arthro.2021.12.016
54. Bolia IK, Ihn H, Kang HP, et al. Cutting, impingement, contact, endurance, flexibility, and asymmetric/overhead sports: is there a difference in return-to-sport rate after arthroscopic femoroacetabular impingement surgery? A systematic review and meta-analysis. Am J Sports Med. 2021;49(5):1363–1371. doi:10.1177/0363546520950441
55. Maslowski E, Sullivan W, Forster Harwood J, et al. The diagnostic validity of Hip provocation maneuvers to detect intra-articular hip pathology. Pm r. 2010;2(3):174–181. doi:10.1016/j.pmrj.2010.01.014
56. Nerys-Figueroa J, Kahana-Rojkind AH, Parsa A, Walsh EG, Lambers F, Domb BG. Radiographs underestimate lateral center-edge angle and tönnis angle measurements compared to computed tomography scan in assessment of borderline and frank acetabular dysplasia. Arthroscopy. 2025;41(7):2343–2350. doi:10.1016/j.arthro.2024.10.038
57. Andronic O, Germann C, Jud L, et al. How useful are indirect radiographic measurements of Hip instability in borderline hip dysplasia? An MRI-based comparison to a healthy cohort. Int Orthop. 2024;48(8):2007–2015. doi:10.1007/s00264-024-06202-8
58. Graesser EA, Schwabe MT, Clohisy JC, Nepple JJ. Defining the borderline dysplastic hip: high variability in acetabular coverage and femoral morphology on low-dose computed tomography. Am J Sports Med. 2023;51(10):2551–2558. doi:10.1177/03635465231184395
59. Andronic O, Chaharbakhshi EO, Zingg PO, et al. No difference in patient-reported outcomes for periacetabular osteotomy and hip arthroscopy with capsular plication in the setting of borderline hip dysplasia: a propensity-matched multicenter study with minimum 5-year follow-up. Arthroscopy. 2024;40(3):754–762. doi:10.1016/j.arthro.2023.06.045
60. Delaunay S, Dussault RG, Kaplan PA, Alford BA. Radiographic measurements of dysplastic adult hips. Skeletal Radiol. 1997;26(2):75–81. doi:10.1007/s002560050197
61. Anderson LA, Gililland J, Pelt C, Linford S, Stoddard GJ, Peters CL. Center edge angle measurement for Hip preservation surgery: technique and caveats. Orthopedics. 2011;34(2):86. doi:10.3928/01477447-20101221-17
62. Batailler C, Weidner J, Wyatt M, Pfluger D, Beck M. Is the Femoro-Epiphyseal Acetabular Roof (FEAR) index on MRI a relevant predictive factor of instability in a borderline dysplastic Hip? Bone Joint J. 2019;101(12):1578–1584. doi:10.1302/0301-620X.101B12.BJJ-2019-0502.R1
63. Nho S, Rasio J. Editorial commentary: rehabilitation after hip arthroscopy-bear in mind the bearing of weight. Arthroscopy. 2020;36(1):165–166. doi:10.1016/j.arthro.2019.10.015
64. Wörner T, Thorborg K, Webster KE, Stålman A, Eek F. Psychological readiness is related to return to sport following Hip arthroscopy and can be assessed by the Hip-Return to Sport after Injury scale (Hip-RSI). Knee Surg Sports Traumatol Arthrosc. 2021;29(5):1353–1361. doi:10.1007/s00167-020-06157-4
65. Jones DM, Webster KE, Crossley KM, et al. Psychometric properties of the hip-return to sport after injury scale (short form) for evaluating psychological readiness to return to sports after arthroscopic hip surgery. Am J Sports Med. 2020;48(2):376–384. doi:10.1177/0363546519888644
66. Wilkin GP, Ibrahim MM, Smit KM, Beaulé PE. A contemporary definition of hip dysplasia and structural instability: toward a comprehensive classification for acetabular dysplasia. J Arthroplasty. 2017;32(9s):S20–s27. doi:10.1016/j.arth.2017.02.067
67. Stetzelberger VM, Moosmann AM, Zheng G, Schwab JM, Steppacher SD, Tannast M. Does the rule of thirds adequately detect deficient and excessive acetabular coverage? Clin Orthop Relat Res. 2021;479(5):974–987. doi:10.1097/CORR.0000000000001598
68. Beck EC, Suppauksorn S, Nho SJ. The role of comprehensive capsular management in hip arthroscopy for the treatment of femoroacetabular impingement syndrome. Arthroscopy. 2020;36(1):9–11. doi:10.1016/j.arthro.2019.10.028
69. Carton P, Filan D, Mullins K. Survivorship rate and clinical outcomes 10 years after arthroscopic correction of symptomatic femoroacetabular impingement. Am J Sports Med. 2022;50(1):19–29. doi:10.1177/03635465211055485
70. Maldonado DR, Perets I, Mu BH, et al. Arthroscopic capsular plication in patients with labral tears and borderline dysplasia of the hip: analysis of risk factors for failure. Am J Sports Med. 2018;46(14):3446–3453. doi:10.1177/0363546518808033
71. Allahabadi S, Chapman RS, Fenn TW, Brusalis CM, Kaplan DJ, Nho SJ. Hip arthroscopic surgery with chondrolabral refixation, osteochondroplasty, and routine capsular closure for femoroacetabular impingement syndrome: clinical outcomes at a minimum 10-year follow-up. Am J Sports Med. 2024;52(1):24–33. doi:10.1177/03635465231212663
72. Ruzbarsky JJ, Seiter MN, Soares R, Pierpoint L, Briggs K, Philippon MJ. Lower center edge angle and bioipolar cartilage lesions are associated with conversion to hip arthroplasty within 2 years following hip arthroscopy: a matched cohort analysis. Arthroscopy. 2022;38(5):1480–1485. doi:10.1016/j.arthro.2021.09.025
73. Bolia IK, Fagotti L, Briggs KK, Philippon MJ. Midterm outcomes following repair of capsulotomy versus nonrepair in patients undergoing hip arthroscopy for femoroacetabular impingement with labral repair. Arthroscopy. 2019;35(6):1828–1834. doi:10.1016/j.arthro.2019.01.033
74. Looney AM, McCann JA, Connolly PT, Comfort SM, Curley AJ, Postma WF. Routine capsular closure with hip arthroscopic surgery results in superior outcomes: a systematic review and meta-analysis. Am J Sports Med. 2022;50(7):2007–2022. doi:10.1177/03635465211023508
75. Kaplan JD, Fenn WT, Jan K, Nho JS. Capsular repair is associated with lower revision rates yet similar clinical outcomes and arthroplasty conversion 5 years after hip arthroscopy: a systematic review. Arthroscopy. 2023;39(8):1882–1891.e1881. doi:10.1016/j.arthro.2023.04.016
76. Hassebrock DJ, Makovicka LJ, Chhabra A, et al. Hip arthroscopy in the high-level athlete: does capsular closure make a difference? Am J Sports Med. 2020;48(10):2465–2470. doi:10.1177/0363546520936255
77. Yacovelli S, Parvizi J. Return to sports after joint preservation hip surgery. Orthop Clin North Am. 2020;51(4):427–439. doi:10.1016/j.ocl.2020.06.001
78. Ifabiyi M, Patel M, Cohen D, Simunovic N, Ayeni RO. Return-to-sport rates after hip arthroscopy for femoroacetabular impingement syndrome in flexibility sports athletes: a systematic review. Sports Health. 2024;16(6):982–990. doi:10.1177/19417381231217503
79. Dasari SP, Kasson LB, Condon JJ, et al. Systematic review and meta-analysis of studies comparing complete capsular closure against unrepaired hip capsules during hip arthroscopy. Orthop J Sports Med. 2023;11(10):23259671231197435. doi:10.1177/23259671231197435
80. Murata Y, Pierpoint L, DeClercq M, et al. Cotyloid fossa coverage percentages may be associated with alpha angle, labral tear, and clinical outcomes in patients with femoroacetabular impingement. Am J Sports Med. 2022;50(1):50–57. doi:10.1177/03635465211056958
81. O’Neill DC, Tomasevich KM, Mortensen AJ, Featherall J, Ohlsen SM, Aoki SK. Capsular repair during hip arthroscopy demonstrates restoration of axial distraction resistance in an in vivo intraoperative testing model. J Bone Joint Surg Am. 2021;103(21):1977–1985. doi:10.2106/JBJS.20.01932
82. Filan D, Mullins K, Carton P. Similar rates of survivorship and marginal clinical impact of routine interportal capsular repair versus no repair at 5 years after arthroscopic correction of femoroacetabular impingement. Arthroscopy. 2025;41:4529–4541. doi:10.1016/j.arthro.2025.04.034
83. Pepic L, Markes RA, Soriano KJK, Flores ES, Zhang LA. No difference in 2-year outcomes for non-hypermobile femoroacetabular impingement syndrome patients undergoing hip arthroscopy with and without closure of periportal capsulotomy. arthroscopy. J Arthroscopy Related Surg. 2025;41(8):2844–2852.e2841. doi:10.1016/j.arthro.2024.12.027
84. Ortiz-Declet V, Mu B, Chen AW, et al. Should the capsule be repaired or plicated after hip arthroscopy for labral tears associated with femoroacetabular impingement or instability? A systematic review. Arthroscopy. 2018;34(1):303–318. doi:10.1016/j.arthro.2017.06.030
85. Jackson TJ. Editorial commentary: indications for acetabular labral debridement versus repair and reconstruction: there is still a role for selective labral debridement. Arthroscopy. 2024;40(2):341–342. doi:10.1016/j.arthro.2023.06.051
86. Haddad B, Konan S, Haddad FS. Debridement versus re-attachment of acetabular labral tears: a review of the literature and quantitative analysis. Bone Joint J. 2014;96(1):24–30. doi:10.1302/0301-620X.96B1.32425
87. Domb BG, Owens JS, Glein RM, Jimenez AE, Maldonado DR. Borderline dysplasia after primary hip arthroscopy with capsular plication and labral preservation: ten-year survivorship and patient-reported outcomes. J Bone Joint Surg Am. 2023;105(9):687–699. doi:10.2106/JBJS.22.00340
88. Soares RW, Ruzbarsky JJ, Arner JW, Comfort SM, Briggs KK, Philippon MJ. Midterm outcomes after hip labral augmentation in revision hip arthroscopy. Am J Sports Med. 2022;50(5):1299–1305. doi:10.1177/03635465221080162
89. Lee MS, Fong S, Lee AY, et al. Patients undergoing revision hip arthroscopy with labral reconstruction or augmentation demonstrate favorable patient reported outcomes: a systematic review. Arthroscopy. 2024;40(6):1923–1937. doi:10.1016/j.arthro.2023.11.027
90. Philippon MJ, Bolia IK, Locks R, Briggs KK. Labral preservation: outcomes following labrum augmentation versus labrum reconstruction. Arthroscopy. 2018;34(9):2604–2611. doi:10.1016/j.arthro.2018.04.021
91. Bodendorfer BM, Alter TD, Carreira DS, et al. Multicenter outcomes after primary hip arthroscopy: a comparative analysis of two-year outcomes after labral repair, segmental labral reconstruction, or circumferential labral reconstruction. Arthroscopy. 2022;38(2):352–361. doi:10.1016/j.arthro.2021.05.013
92. Jimenez AE, Monahan PF, Owens JS, et al. Return to sports and minimum 2-year outcomes of primary arthroscopic hip labral reconstruction for irreparable tears in high-level athletes with a propensity-matched benchmarking against a labral repair control group. Am J Sports Med. 2021;49(12):3261–3269. doi:10.1177/03635465211032593
93. Morgan P, Crawford A, Marette S, et al. Using a simplified version of a common surgical grading scale for acetabular labral tears improves the utility of preoperative Hip MRI for femoroacetabular impingement. Skeletal Radiol. 2020;49(12):1987–1994. doi:10.1007/s00256-020-03495-9
94. Youm T. Editorial commentary: measure labral height using magnetic resonance imaging prior to hip arthroscopy: a diminutive labrum should be reconstructed with a graft to restore the suction seal. Arthroscopy. 2025;41:3982–3984. doi:10.1016/j.arthro.2025.05.009
95. Maldonado DR, Ouyang VW, Owens JS, et al. labral tear management in patients aged 40 years and older undergoing primary hip arthroscopy: a propensity-matched case-control study with minimum 2-year follow-up. Am J Sports Med. 2021;49(14):3925–3936. doi:10.1177/03635465211046915
96. Maldonado DR, Monahan PF, Domb BG. Restoration of labral function in primary hip arthroscopy from labral repair to labral reconstruction. arthroscopy. J Arthroscopy Related Surg. 2021;37(10):3013–3015. doi:10.1016/j.arthro.2021.08.003
97. Zhang AL. Editorial commentary: arthroscopic treatment for diminutive hip labral size: go big or go home? Arthroscopy. 2021;37(1):108–110. doi:10.1016/j.arthro.2020.09.040
98. Khalil LS, Lynch TS. Editorial commentary: surgeons planning hip labral arthroscopic repair should have a backup plan of labral reconstruction or augmentation based on intraoperative labral degeneration, hypoplasia, or ossification. Arthroscopy. 2022;38(9):2669–2671. doi:10.1016/j.arthro.2022.04.001
99. Hartigan DE, Hegedus CE. Editorial commentary: ligamentum teres reconstruction may improve hip stability but has high revision rates: fad or restoration of function? Arthroscopy. 2021;37(6):1820–1821. doi:10.1016/j.arthro.2021.02.037
100. Rosinsky PJ, Annin S, Maldonado DR, et al. Arthroscopic ligamentum teres reconstruction: minimum 2-year patient-reported outcomes with subanalysis of patients with ehlers-danlos syndrome. Arthroscopy. 2020;36(8):2170–2182. doi:10.1016/j.arthro.2020.04.028
101. Nepple JJ, Parilla FW, Pashos GE, Clohisy JC. Outcomes of periacetabular osteotomy for borderline acetabular dysplasia. J Bone Joint Surg Am. 2023;105(2):137–144. doi:10.2106/JBJS.22.00491
102. Kuhns BD, Becker N, Strok MJ, O’Brien EJ, Hassan M, Domb BG. Patient-reported outcomes after periacetabular osteotomy versus hip arthroscopy for borderline acetabular dysplasia are both favorable: a systematic review. Arthroscopy. 2025;41(8):3079–3093.e3072. doi:10.1016/j.arthro.2024.11.090
103. McClincy MP, Wylie JD, Kim YJ, Millis MB, Novais EN. Periacetabular osteotomy improves pain and function in patients with lateral center-edge angle between 18° and 25°, but are these hips really borderline dysplastic? Clin Orthop Relat Res. 2019;477(5):1145–1153. doi:10.1097/CORR.0000000000000516
104. Adler KL, Giordano BD. The utility of hip arthroscopy in the setting of acetabular dysplasia: a systematic review. Arthroscopy. 2019;35(1):237–248. doi:10.1016/j.arthro.2018.07.048
105. Edelstein AI, Nepple JJ, Abu-Amer W, Pascual-Garrido C, Goss CW, Clohisy JC. What mid-term patient-reported outcome measure scores, reoperations, and complications are associated with concurrent hip arthroscopy and periacetabular osteotomy to treat dysplasia with associated intraarticular abnormalities? Clin Orthop Relat Res. 2021;479(5):1068–1077. doi:10.1097/CORR.0000000000001599
106. Foissey C, Abid H, Martinot P, Cazor A, Thaunat M. Predictive radiological parameters of failure following surgical management of femoroacetabular impingement associated with borderline acetabular dysplasia. Orthop Traumatol Surg Res. 2023;109(4):103349. doi:10.1016/j.otsr.2022.103349
107. Willimon SC, Briggs KK, Philippon MJ. Intra-articular adhesions following Hip arthroscopy: a risk factor analysis. Knee Surg Sports Traumatol Arthrosc. 2014;22(4):822–825. doi:10.1007/s00167-013-2728-0
108. Ruzbarsky JJ, Comfort SM, Martin MD, Briggs KK, Philippon MJ. Outcomes for treatment of capsulolabral adhesions with a capsular spacer during revision hip arthroscopy. Am J Sports Med. 2023;51(2):487–493. doi:10.1177/03635465221145704
109. King GM, Klij VP, Hoak F, et al. Are women less likely to return to sport compared to men following hip arthroscopy. a systematic review and meta-analysis. J Orthop Sports Phys Ther. 2025;55(3):193–205. doi:10.2519/jospt.2025.12813
110. Walsh GE, Wallace AI, Becker N, Flynn M, Domb A, Quesada-Jimenez R. With proper surgical indications, sex-based differences in pathology do not impact hip arthroscopy outcomes or complications: a systematic review. Arthroscopy. 2025;41(8):3094–3112. doi:10.1016/j.arthro.2024.12.031
111. Clohisy JC, Ackerman J, Baca G, et al. Patient-reported outcomes of periacetabular osteotomy from the prospective ANCHOR cohort study. J Bone Joint Surg Am. 2017;99(1):33–41. doi:10.2106/JBJS.15.00798
112. Leopold JV, Szarek A, Hipfl C, Bärtl S, Perka C, Hardt S. Outcomes and return-to-sports rates in patients with borderline hip dysplasia after periacetabular osteotomy: a case series with 5-year follow-up. Am J Sports Med. 2024;52(2):383–389. doi:10.1177/03635465231217736
113. Domb BG, Chaharbakhshi EO, Perets I, Walsh JP, Yuen LC, Ashberg LJ. Patient-reported outcomes of capsular repair versus capsulotomy in patients undergoing hip arthroscopy: minimum 5-year follow-up-a matched comparison study. Arthroscopy. 2018;34(3):853–863.e851. doi:10.1016/j.arthro.2017.10.019
114. Wyatt M, Weidner J, Pfluger D, Beck M. The Femoro-Epiphyseal Acetabular Roof (FEAR) index: a new measurement associated with instability in borderline hip dysplasia? Clin Orthop Relat Res. 2017;475(3):861–869. doi:10.1007/s11999-016-5137-0
115. Kuhns BD, Becker N, Patel D, Shah PP, Domb BG. Significant heterogeneity in existing literature limits both indication and outcome comparability between studies involving periacetabular osteotomy for acetabular dysplasia with or without arthroscopy despite improvement for both: a systematic review. Arthroscopy. 2025;41:4858–4873. doi:10.1016/j.arthro.2025.06.030
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence of Hip Pain in Elite Badminton Players: Observational Study
Denis S, Rose C, Ramos-Pascual S, Le Garrec S, Van Rooij F, Saffarini M, Nogier A
Open Access Journal of Sports Medicine 2025, 16:79-87
Published Date: 23 July 2025