Back to Journals » Vascular Health and Risk Management » Volume 17
Higher Total Physical Activity is Associated with Lower Arterial Stiffness in Swedish, Young Adults: The Cross-Sectional Lifestyle, Biomarkers, and Atherosclerosis Study
Authors Fernberg U ![]() , Fernström M
, Fernström M ![]() , Hurtig-Wennlöf A
, Hurtig-Wennlöf A ![]()
Received 17 December 2020
Accepted for publication 8 March 2021
Published 29 April 2021 Volume 2021:17 Pages 175—185
DOI https://doi.org/10.2147/VHRM.S283211
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Daniel Duprez
Ulrika Fernberg,1 Maria Fernström,2 Anita Hurtig-Wennlöf1,3
1Cardiovascular Research Center, Faculty of Medicine and Health, Örebro University, Örebro, 70182, Sweden; 2Department of Physical Activity and Health, The Swedish School of Sport and Health Sciences, GIH, Stockholm, 11433, Sweden; 3The Biomedical Platform, Department of Natural Science and Biomedicine, School of Health and Welfare, Jönköping University, Jönköping, 55111, Sweden
Correspondence: Ulrika Fernberg
Cardiovascular Research Center, Faculty of Medicine and Health, Örebro University, Fakultetsgatan 1, Örebro, SE 701 82, Sweden
Tel +46 19 30 30 54
Email [email protected]
Purpose: Arterial stiffness describes the rigidity of the arterial walls and is associated with risk factors for cardiovascular disease (CVD). Arterial stiffness predicts future events and mortality, and the predictive value is stronger in younger versus older subjects. The aims of the present study were, firstly, to present data on physical activity (PA) and time spent sedentary, in the population of Swedish, young adults. Secondly, to explore the association between PA and arterial stiffness.
Material and Methods: Self-reported healthy, non-smoking, Swedish, young adults, 18– 25 years old, participated in the cross-sectional Lifestyle, Biomarkers and Atherosclerosis (LBA) study. The daily PA was objectively measured with an accelerometer for 1 week. Of the 834 participants, 658 individuals had valid registrations. The arterial stiffness measures, pulse wave velocity (PWV) and augmentation index (AIx) were measured with applanation tonometry.
Results: Women were on overall more physically active than men, they spent 214 min/day in light PA (LPA) compared to men who spent 202 min/day. Women took significantly more steps per day than men, 7796 vs 7336 steps/day, and spent less time sedentary, 523 min/day, compared to men who spent 547 min/day sedentary. In total, 76% of the individuals spent on average at least 30 minutes per day in the recommended moderate and vigorous PA (MVPA). Lower arterial stiffness was associated with more MVPA and total PA in the total population.
Conclusion: We conclude that in this age group of young, self-reported healthy adults 18– 25 years, it is important to highlight the health-enhancing possibilities of time spent in physical activity on the vascular function, measured as PWV and AIx. It is of high relevance in a public health perspective to expand preventive efforts beyond the high-risk groups and encourage young adults to be physically active.
Keywords: accelerometry, atherosclerosis, healthy population, pulse wave analysis, pulse wave velocity
Introduction
Atherosclerosis is a complex, chronic vessel wall disease that often leads to severe and acute cardiovascular disease (CVD). The atherosclerotic process is slow, starts already in childhood and develops over decades.1,2 Since most of the risk factors for atherosclerosis are preventable,3 it is of great importance to investigate the impact of lifestyle-related factors on arterial stiffness in young adults who are about to create their own habits which could be seen as a part of long-term primary prevention. Arterial stiffness describes the rigidity of the arterial walls.4 Along with healthy ageing there is a progressive stiffening of the elastic arteries, this has been described in several longitudinal studies.5–7 The stiffening of the arteries increases the wave reflection from peripheral points in the arterial tree, leading to increases in ventricular afterload and less diastolic coronary perfusion, resulting in risk of myocardial hypertrophy and ischemia.8 Previous studies have shown that arterial stiffness is associated with the presence of cardiovascular risk factors and atherosclerotic disease in adults.3,8 A meta-analysis also showed that aortic stiffness predicts future events and mortality and the predictive value was stronger in younger versus older subjects, even after accounting for other established risk factors.9
It is well established that physical activity (PA) is protective in the development of atherosclerosis10 and that PA is inversely associated with cardiovascular morbidity, cardiovascular mortality and all-cause mortality.11,12 Regular PA also reduces the risk of several other health outcomes such as hypertension, type 2 diabetes mellitus, obesity, osteoporosis, colon cancer, breast cancer, anxiety, and depression.13 Based on this knowledge, recommendations on physical activity for health have been developed. According to the WHO recommendations for healthy adults, 18–64 years, you promote and maintain good health if you perform aerobic PA at a moderate-intensity level of at least 150 minutes per week.14
Higher levels of physical activity (PA) attenuate the increase in arterial stiffness that occurs with ageing15 and several studies have investigated the association between arterial stiffness and objectively measured PA but the results are conflicting.16–21 In a longitudinal study following individuals from adolescence to the age of 36 years, they showed that performing vigorous physical activity (VPA), but not light-to-moderate physical activity had a beneficial impact on arterial stiffness later in life.20 However, in a systematic review and meta-analysis with different age groups and also patient groups included, it was found that time spent in light and moderate physical activity were associated with lower arterial stiffness while time spent in sedentary was associated with higher arterial stiffness.21 Healthy young adults are underrepresented in the CVD literature compared to different patient groups and since the knowledge about the association between objectively measured PA and arterial stiffness is limited in Swedish young adults, the purposes of the present study were, firstly, to present data on PA and time spent sedentary, in the population of Swedish, young adults, including analyses of sex differences. Secondly, to explore the association between PA and arterial stiffness, in this age group, with respect to confounding variables such as mean arterial pressure (MAP), age, height, and PWV.22
In addition to this purposes, we also wanted to investigate if young adults, earlier classified as being at risk for atherosclerosis and cardiovascular disease23 by using the definition by Wildman,24,25 differed in their PA levels compared to young adults not being at risk.
Materials and Methods
Study Population
Self-reported healthy, non-smoking, Swedish, young adults, 18.0–25.9 years old, participated in the cross-sectional Lifestyle, Biomarkers and Atherosclerosis (LBA) study.26 The study participants were mainly students (94%), with no difference between women and men. The 834 individuals who met the inclusion criteria (ie, 18–25 years, non-smoking, self-reported healthy without chronic diseases) did two visits with approximately 1 week apart, to examine vessel status, biomarkers, and lifestyle factors.23 All individuals had oral and written information about the study and gave their written consent to participate. The study design was approved by the Uppsala Ethics Committee (Dnr: 2014/224) and all procedures were performed in accordance with the ethical standards of the Regional Ethics Committee in Uppsala and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Body Composition
Height, weight, and percentage of body fat were measured with the subject in a fasting state. Height was measured to the nearest 0.5 cm with a fixed stadiometer. Weight was measured, and percentage of body fat was calculated using an impedance body composition analyzer (Tanita BC-418 MA, Tanita Europe B.V., Amsterdam, Netherlands). Body mass index (BMI) (kg/m2) was calculated.
Biomarkers and Definition of Early Risk Factors for Atherosclerosis
Blood samples were collected with the individuals in a fasting state, and venipuncture was performed after a resting period of approximately 20 minutes. High-density lipoprotein cholesterol (HDL-C), triglycerides, and glucose (mmol/L) were analyzed on an Ortho Clinical DiagnosticsTM (Vitros 5.1TM FS; Clinical Chemistry Instruments, Raritan, NJ, USA). Insulin (mU/L) was analyzed on an Architect i2000SR instrument from Abbott (Architect i2000SR, Abbott Park, IL, USA) and high-sensitive C-reactive protein (hs-CRP) (mg/L) was analyzed with the method from Siemens27 (ADVIA 1800 Chemistry System; Upplands Väsby, Sweden). Homeostasis model of assessment of insulin resistance (HOMA-IR) was calculated using Matthews’ equation, insulin (mU/L) × glucose (mmol/L)/22.5.28 Analyses were performed at the accredited clinical chemistry laboratory at Örebro University Hospital, as earlier described.23
The definition by Wildman24,25 was used to classify individuals being at risk for atherosclerosis and CVD. Individuals having two or more of the following characteristics were classified as being at risk according to Wildman’s cut-off values; elevated blood pressure (130/85 mmHg), elevated triglycerides (≥1.70 mmol/L), decreased HDL-C (women <1.30 mmol/L, men <1.04 mmol/L), elevated glucose (≥5.6 mmol/L), insulin resistance (HOMA-IR >2.52), and elevated hs-CRP (>5.07 mg/L).
Physical Activity
The study participant’s daily PA was objectively measured with an accelerometer (ActiGraph, model GT3X+, Pensacola, FL, USA). The intensity (light, moderate, and vigorous PA, see definitions below) and duration of PA, as well as sedentary time,29 were recorded over 1 week. The study participants were instructed to wear the accelerometer on an elastic belt around their waist at their lower back during all waking time, except during water activities.30 The accelerometer data were processed and analyzed with the Actilife software (ActiLife, version 6.13.3, ActiGraph, Pensacola, FL, USA). The accelerometer was initialized with a raw data sampling frequency of 30 Hz, and uniaxial (vertical) analyses with 60-s epoch was used. Non-wear time was defined by an interval of at least 60 consecutive minutes of 0 counts per minute with an allowance for maximum 2 minutes of counts between 0 and 100. Wear-time was defined by subtracting non-wear time from 24 hours31 and the wear-time criteria to be included in the analyses were at least 10 hours of wear-time per day, and at least 4 valid days.30,32
The cut-off points used to define different PA intensity levels were for light-intensity PA (LPA) <2020 counts, for moderate-intensity PA (MPA) 2020–5999 counts, and for vigorous-intensity PA (VPA) >5999 counts per minute. Moderate- and vigorous physical activity (MVPA) were defined as ≥2020 counts without any distinction between MPA and VPA.31 Total PA per day is the sum of LPA and MVPA in minutes per day. Sedentary time was defined as registration time with <100 counts per minute.33 Number of steps was also registered by the accelerometer.
Study participants in the LBA population with valid PA data, who met the MVPA recommendations, were also analysed. Current Swedish national guidelines34 based on the physical activity recommendations from WHO14 recommend at least 150 minutes/week of MVPA. Since not all participants with valid PA data reached 7 days (a week) valid registration, we calculated the average time in MVPA/day by dividing total time in MVPA with the number of valid days. We then categorized the participants accumulating at least 30 minutes per day in MVPA as “reaching 30 minutes MVPA per day” and the participants accumulating less than 30 minutes as “not reaching 30 minutes MVPA per day”. In the same way the study participants with more than 60 minutes in MVPA per day were categorized as “reaching 60 minutes MVPA per day”.
Blood Pressure and Arterial Stiffness Measurements
Brachial blood pressure was measured with an oscillometric, non-invasive blood pressure method, after 10 minutes rest in a supine position, using a digital automated device (Dinamap V100, GE Healthcare, Buckinghamshire, UK) as earlier described.23 The stiffness measurements, PWA and PWV were measured with SphygmoCor (SphygmoCor, AtCor Medical Pty Ltd, Sydney, Australia) as earlier described.35 For PWA, a radial artery tonometry was performed at the subject’s right wrist and the aortic pressure waveform was derived from the radial waveform by a validated transfer function.36 At least three measurements were made on each test subject and an average of AIx_HR75 from three measurements were reported for each subject with a standard deviation (SD) for repeated measurements of ±2. For interpretation, higher value of AIx_HR75 indicates stiffer vessels.
For PWV, carotid and femoral pulse waves were recorded with applanation tonometry with simultaneously electrocardiography (ECG) recording to get the pulse transit time.22 At least three measurements were performed and PWV was calculated using the transit time and the measured distance with an SD of 0.44 m/s for repeated measurements. Distance was measured as a straight line from the sternal to the carotid site, and from the sternal notch to the femoral site via the umbilicus. The length between the sternal notch and the carotid site was subtracted from the length between the sternal notch and the femoral site to get the distance.37 When three measurements were stable within 0.5 m/s between three measurements, the examination was ended and an average of the three measurements was calculated. For interpretation, higher value of PWV indicates stiffer vessels.
Statistical Analyses
Statistical calculations were performed using IBM SPSS Statistics, version 25.0 for Windows (IBM SPSS Statistics 25, IBM Corp, Armonk, New York, USA). The Shapiro–Wilk test was used to check all variables for normal distribution. Descriptive data in normal distributed variables are presented as mean and standard deviation, and skewed variables are presented as median and interquartile range. The natural logarithms of the skewed variables were used when applying unpaired Student t-test for comparing mean differences between the sexes, between individuals with valid data for the accelerometer registration (ie, 4 valid days with at least 10 hours per day) vs excluded individuals, between the individuals reaching 30 minutes MVPA per day vs not reaching 30 minutes MVPA per day, and between time spent in different intensity levels (ie LPA, MPA, VPA, MVPA, and time spent in sedentary (min/day)) in individuals at risk and not at risk, according to Wildman’s risk score. For comparisons of arterial stiffness measurements (ie PWV and AIx_HR75) across the MVPA categories, not reaching 30 minutes MVPA per day, reaching 30 minutes MVPA per day, and reaching 60 minutes MVPA per day, one-way ANOVA with Hochberg’s GT2 post-hoc test was applied. Significance level was set to p<0.05 in all tests.
Simple linear regression was used to study the associations between time spent in different intensity levels and arterial stiffness measurements. Corrections for multiple comparisons were made according to Bonferroni. Based on the number of tests, the Bonferroni correction resulted in the following: Significant level <0.05 required p<0.0025, significant level <0.01 required p<0.0005, and significant level <0.001 required p<0.00005.
Multiple regression analyses were performed with arterial stiffness measurements as dependent variables to explore the effect of PA per day. In addition to PA, confounding variables (age, height, MAP, and PWV) earlier described in the literature as determining factors of arterial stiffness were included in the multiple regression models.22
Results
Of the total population (834 individuals), 828 individuals used and returned their accelerometer. A total of 658 individuals (73% women) who fulfilled the PA wear-time criteria were included in the analyses, see Figure 1. In comparisons between individuals with valid PA data and the individuals excluded because of no valid PA data, the analyses showed that the women with valid PA data had significantly lower BMI (p<0.05) and percentage of body fat (p<0.01) than the excluded women. The men with valid PA data had significantly lower glucose (p<0.05), HOMA-IR (p<0.05), and AIx_HR75 (p<0.05), than the excluded men.
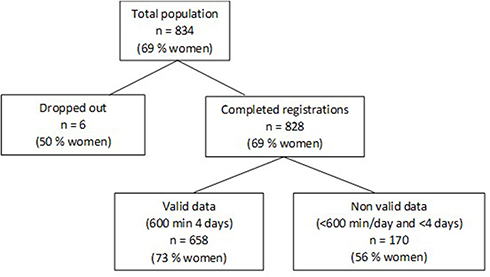 |
Figure 1 Sampling procedure of the physical activity (PA) data in the Lifestyle, Biomarkers, and Atherosclerosis Study. |
Basic characteristics and PA data of the 658 individuals are presented divided into categories, women and men, Table 1. There were significant differences between women and men in all basic characteristics, p<0.01, except for age, triglycerides, HOMA-IR, hs-CRP, and diastolic blood pressure (DBP). Daily median accelerometer wear time was 13.2 h per day in the total population with no significant differences between women and men. Women spent significantly more time per day in LPA (p<0.01) and total PA (p<0.01), were less time sedentary (p<0.001), and took significantly more steps per day (p<0.05), than men. There were no significant differences between women and men in how much time they spent in MPA, VPA, and MVPA per day, Table 1.
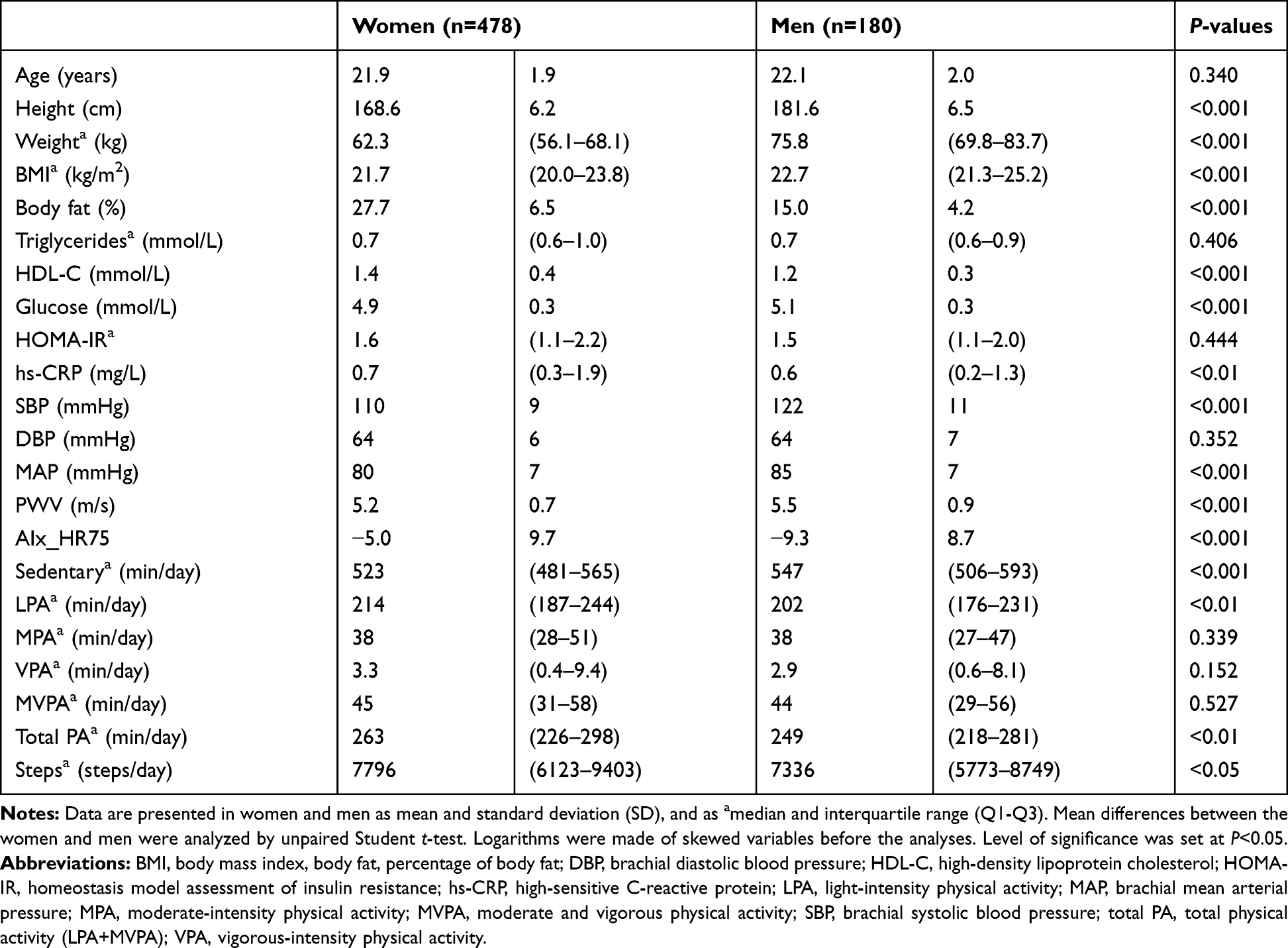 |
Table 1 Basic Characteristics in the Study Participants with Valid Physical Activity (PA) Data |
On average, women and men accumulated 523 (481–565) and 547 (506–593) minutes per day in sedentary time, respectively. That corresponds to approximately 67% and 69%, respectively, in sedentary time of total registration time per day. Women and men accumulated on average 45 (31–58) and 44 (29–56) minutes per day, respectively, in MVPA with large individual variations. Total daily time spent in MVPA varied from 7 to 203 minutes in women and from 4 to 294 minutes in men. In total 76% of the individuals spent on average at least 30 minutes per day in MVPA. There was no significant difference between women and men, 77% of women and 74% of men spent on average at least 30 minutes per day in MVPA.
When comparing subjects at risk and subjects not at risk, according to Wildman’s risk score, subjects at risk had less time spent in LPA (p<0.01) and less time spent in total PA (p<0.01) per day, Table 2. The women reaching 30 minutes MVPA per day had significantly lower AIx_HR75 (p<0.05) compared to women not reaching 30 minutes MVPA per day. The same result was seen in comparison between women reaching 60 minutes MVPA per day compared to women not reaching 30 minutes MVPA per day (p<0,05). No significant differences were seen in men. In total population, the study participants reaching 60 minutes in MVPA per day had significantly lower AIx_HR75 (p<0.05) than the ones not reaching 30 minutes MVPA per day, Figure 2. No significant differences in PWV were seen between the groups.
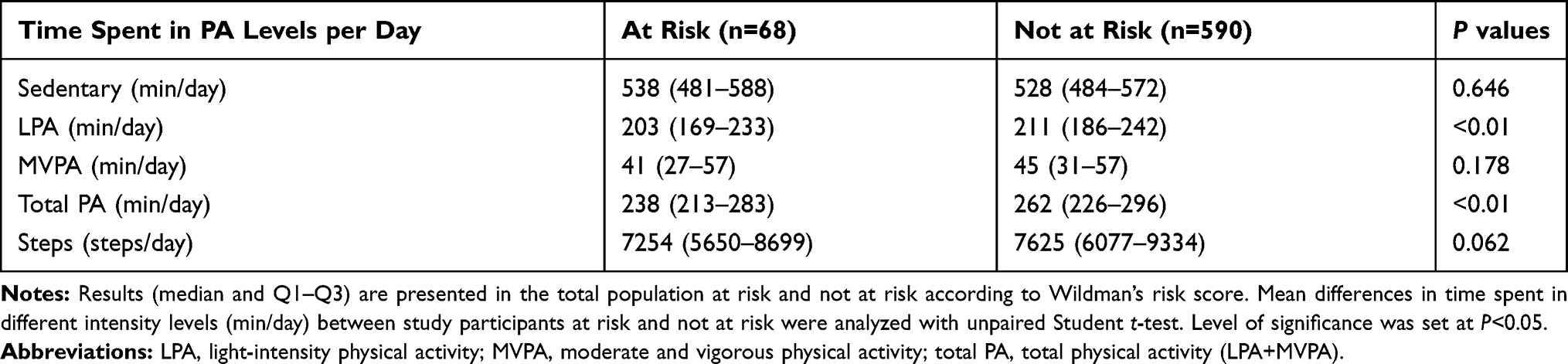 |
Table 2 Distribution of Time Spent in Different Physical Activity Intensity Levels (Min/Day) and Steps per Day, in the Total Population, Divided in the Categories At Risk and Not At Risk According to Wildman’s Risk Score |
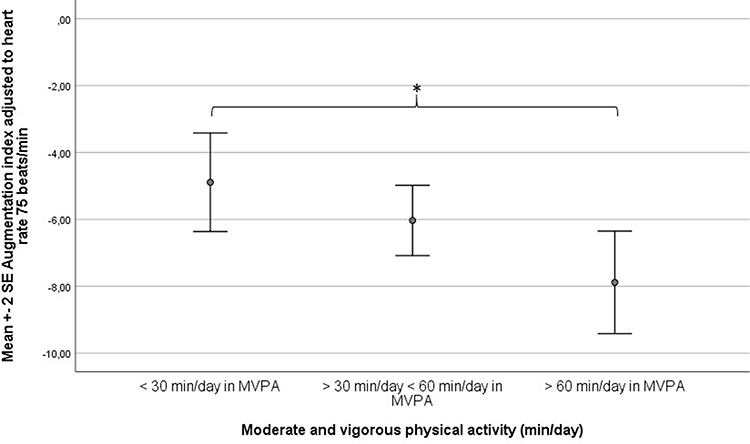 |
Figure 2 AIx_HR75 (Augmentation index adjusted to heart rate 75 beats/min) in the moderate and vigorous physical activity (MVPA) categories not reaching 30 minutes MVPA per day (n=157), reaching 30 minutes MVPA per day (n=353), and reaching 60 minutes MVPA per day (n=144) in total population with valid physical activity data. Study participants who spent <30 minutes per day in MVPA had significantly higher AIx_HR75 than study participants who spent >60 minutes/day in MVPA, *P<0.05. |
Significant inversed associations (standardized β coefficients and P-value) were seen between AIx_HR75 and MVPA (−0.166; p<0.001), total PA (−0.116 p<0.05), and steps (−0.150; p<0.001) per day, in women. In men, a significant inverse association was seen between AIx_HR75 and total PA (−0.153; p<0.05). Significant inversed associations were also seen between PWV and MVPA (−0.104; p<0.05), and PWV and steps (−0.128; p<0.01) per day in women (ie, lower stiffness when more PA). After Bonferroni correction, significant inverse associations were still present between AIx_HR75 and MVPA and between AIx_HR75 and steps per day, in women Table 3.
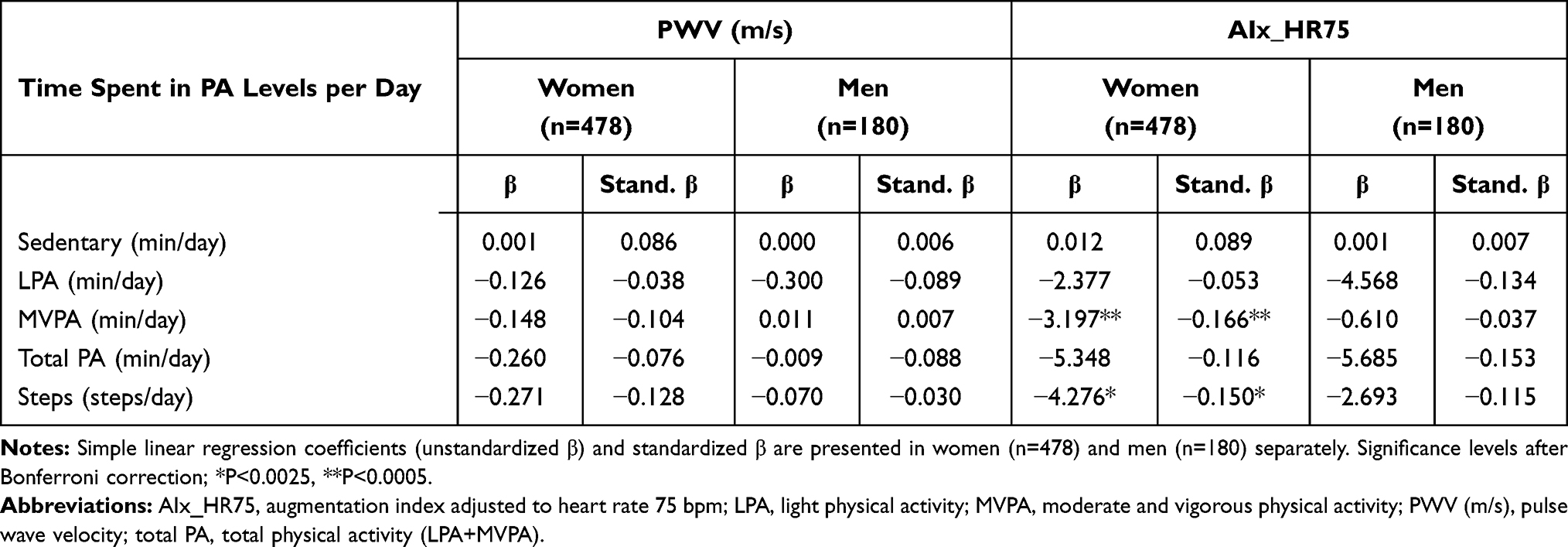 |
Table 3 Simple Linear Regression Coefficients (β) and Standardized β (Stand β) Between Regional Stiffness Measurements as Dependent Variables and Physical Activity Levels as Independent Variables, in Women and Men |
To explore the effect of total PA and MVPA per day on AIx_HR75, after adjustment for confounding variables previously described as determining factors (MAP, Height, Age, PWV), multiple regression analyses were performed. After controlling for confounding variables an inversed association was seen between AIx_HR75 and time spent in total PA per day, in total population (−0.110; p<0.01), and in women (−0.108; p<0.05). No significant association was seen between total PA and AIx_HR75 in men (−0.113; p=0.120). An inversed association was also seen between AIx_HR75 and MVPA, in total population (−0.093; p<0.01), and in women (−0.119; p<0.01), but not in men (−0.042; p=0.552).
Discussion
In the LBA study, women spent less time sedentary (p<0.001) and more time in LPA (p<0.01) in comparison with men. These findings are in line with the findings in another Swedish study, the SCAPIS Pilot Study, which observed that men spent more time sedentary and less time in LPA compared to women.38 However, no significant differences between the sexes were seen in MPA, VPA, or MVPA in the present study. This finding differs from several other studies38–40 where, most commonly, men are reported to be more physical active at a moderate and vigorous level. The LBA study included self-reported healthy, young adults, and many of the women included were well trained and had an interest in health and fitness.23 This could possibly explain why we do not observe the previously reported differences between the sexes in time spent in MVPA. Another explanation can be the decline in cardiorespiratory fitness (CRF) in Swedish adults over the last 20 years. The proportion of individuals with low CRF (estimated maximal oxygen uptake (VO2max) <32 mL/kg/min) almost doubled, from 27% to 46% between 1995 and 2017. The decrease in VO2max was more pronounced in men than in women, and in the youngest age group (18–34 years) compared to the middle (35–49 years) and oldest age group (50–74 years). The finding of no difference in the present study in how much time women and men spend in MVPA is maybe partially explained by the decline in CRF in especially young men. The decline in CRF may indicate a secular trend and can partially be a result of less time spent at higher physical activity intensity levels (MVPA).41
In total, 76% of the individuals spent on average at least 30 minutes per day in MVPA. In an earlier publication from the Swedish SCAPIS pilot Study in 2015,38 75.7% in the age group 50–64 years fulfilled the recommendations of 150 minutes of MVPA per week. These results are in line with the findings in the present study were 77% of the women and 74% of the men spent on average at least 30 minutes per day in MVPA. However, the age groups in the studies differ so comparisons are difficult to do. Data from a national survey in Sweden, the Physical Activity Fact Sheet from 2018,42 presented similar results, 67% in the age group 18–64 years met the PA recommendations of at least 150 minutes of MVPA per week.14 The PA level was assessed subjectively with questionnaire unlike the PA data in the LBA study, and the age group was considerably wider in its range than in the LBA study, so comparisons can be less relevant. However, it is striking to observe that one-fourth (24%) of the young adults with valid PA data in the LBA population did not spend the recommended 30 minutes per day in MVPA. You could expect that you are more physically active as young adult than as middle-aged and should reach a higher level of MVPA per day in younger years. The current PA recommendations14,34,43 are similar for adults from 18 to 64 years which is a quite wide age range. It would be interesting to further explore PA habits in young adults to investigate whether individuals in this age group could receive additional health benefits from more targeted PA recommendations. In Figure 2, we show that the young adults who spend at least 60 minutes per day in MVPA have the lowest AIx_HR75, indicating less stiffer arteries.
The present study showed that the study participants with two or more risk factors categorized as at-risk according to Wildman were less physically active than the study participants not at risk according to Wildman. The findings are supported by the recently published systematic review and harmonized meta-analysis44 with individual data from a large sample (n=36,383). More women than men (72.8%) were included in the sample, like in the LBA study, but the mean age was considerably older, mean age 62.6 years. The meta-analysis showed that higher levels of total physical activity and less time spent sedentary were associated with a reduced risk of premature mortality. This is supported by the findings of the LBA study where we demonstrate that young adults without risk factors for CVD have a higher level of total PA compared to those at risk for future CVD who are less physically active. The meta-analysis showed that all intensities of PA were associated with a reduced risk of mortality, highlighting the fact that all PA is better than time spent sedentary.43 Not only high intensities of PA had beneficial effects for health. The greatest risk reduction for mortality was seen at about 375 min/day in LPA or 24 min/day of MVPA. In addition, a higher risk of death was seen if spending 9.5 hours or more per day sedentary.44
When investigating the relationship between PA and arterial stiffness after adjusting for several confounding variables, inversed associations between AIx_HR75 and total PA and AIx_HR75 and MVPA were significant in total population and in women, but not in men. However, in the association between AIx_HR75 and total PA, the standardized β coefficient in men was similar in magnitude to the standardized β coefficient in women. Failure to observe significant standardized β coefficients for total PA may be due to low statistical power resulting from the lower number of men.
In the LBA study, we could not see any significant positive association between time spent sedentary and arterial stiffness. This has been found in a couple of other studies,17,21 but this was not observed in the LBA study.
Thus, in this age group of young adults, it is important to maintain or strive for more time in physical activity. Physical activity seems to be beneficial for the vascular health as total PA and MVPA are associated with lower arterial stiffness in the total population, and observed especially clear in women.
One important strength of the present study was the large study group with young adults that had their physical activity habits assessed objectively with an accelerometer. This age group can contribute to the detection of early changes affecting the development of CVD and it is important to highlight the benefits of a healthy lifestyle early in life. Although it is a strength that the PA was measured objectively, the accelerometer has some limitations. There is no information on the subjects’ physical activity outside the accelerometer wear time (mean wear time 13.2 hours per day). Other known limitations of accelerometry are the lack of information from water activities, underestimation of activity during weight-bearing activities and biking.
These issues are well-known limitations of the accelerometry methodology. Still, the objective accelerometry is regarded to be superior to self-report or other subjective methods. The shortcomings of accelerometry are to some extent overcome by the large number of subjects. A recent methodological paper concluded that a large sample size is more important than a long observation period within each individual.45
We had valid PA data from 79.5% of the study population who completed their accelerometer registration. Analyses between the individuals with valid PA data and the individuals excluded because of no valid PA data, showed that the women with valid data had lower BMI and percentage of body fat while the men with valid PA data had more beneficial levels of glucose, HOMA-IR, and AIx_HR75, compared to the women and men, respectively, who did not reach the requirement of 600 minutes per day on at least 4 days. Thus, an overrepresentation of healthier individuals, according to the tests in the LBA study, had full PA registrations. This decreases the variability in the data set and decreases the probability in detecting differences. Despite a healthy active cohort, we saw associations between higher levels of PA and lower stiffness.
Another limitation in the present study was that the individuals included in the study were self-reported healthy. We did not include individuals with a chronic disease, but we accepted, eg, individuals with obesity, which is a reversible condition and an important risk factor for CVD. Furthermore, the study has a lower number of male individuals. For unknown reasons, it was much more difficult to recruit men to the study. Finally, one further limitation that needs to be highlighted is the cross-sectional design in the LBA study that prevents us from drawing conclusions in terms of causality.
In summary, the main findings of the present study were that 76% of the Swedish, young adults in the LBA study population spent on average at least 30 minutes in MVPA per day. Young adults without risk factors for CVD had a higher level of total PA compared to the young adults with two or more risk factors for future CVD. Lower arterial stiffness was associated with higher levels of PA.
Conclusion
We conclude that already in this age group of healthy young adults, aged 18–25 years, it is important to highlight the health-enhancing possibilities of PA on the vascular function, measured as PWV and AIx. It is of high relevance in a public health perspective to expand preventive efforts beyond the high-risk groups and encourage young adults to be physically active.
Abbreviations
AIx, augmentation index; AIx_HR75, augmentation index adjusted to heart rate 75 beats per minute; BMI, body mass index; CVD, cardiovascular diseases; DBP, diastolic blood pressure; ECG, electrocardiography; HDL-C, high-density lipoprotein cholesterol; HOMA-IR, homeostasis model of assessment of insulin resistance; Hs-CRP, high-sensitive C-reactive protein; LBA study, lLifestyle, Biomarkers, and Atherosclerosis study; LPA, light physical activity; MAP, mean arterial pressure; MPA, moderate physical activity; MVPA, moderate and vigorous physical activity; PA, physical activity; PWA, pulse wave analysis; PWV, pulse wave velocity; SBP, systolic blood pressure; total PA, total physical activity (LPA+MVPA); VPA, vigorous physical activity.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Informed Consent
The study design was approved by the Uppsala Ethics Committee (Dnr: 2014/224) and all procedures were performed in accordance with the ethical standards of the Regional Ethics Committee in Uppsala and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. All individuals had oral and written information about the study and gave their written consent to participate.
Consent for Publication
Not applicable.
Acknowledgments
The authors wish to thank all the volunteers who participated in the study. We also thank Madelene Lindqvist, Katya Matusevich and Gabriella Eliason who contributed to the collection of data. This work was supported by the Asset Management Arm (AFA) [grant number: 130275]. AFA contributed with financial support. Study design, data collection, analysis of data, and writing the manuscript were done by the authors.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
Funding was provided by Asset Management Arm (AFA) life insurance nr: 130275. AFA contributed with financial support, but study design, data collection, analysis of data, and writing the manuscript were done by the authors.
Disclosure
The manuscript is based on the thesis “Arterial stiffness and risk factors for cardiovascular disease in young adults” by the author Ulrika Fernberg. The authors report no other conflicts of interest in this work.
References
1. Berenson GS, Srinivasan SR, Bao W, Newman WP
2. McGill HC
3. Nichols W, O’Rourke MF, Vlachopoulos C. McDonald’s Blood Flow in Arteries.
4. Mackenzie IS, Wilkinson IB, Cockcroft JR. Assessment of arterial stiffness in clinical practice. QJM. 2002;95(2):67–74. doi:10.1093/qjmed/95.2.67
5. Mitchell GF, Parise H, Benjamin EJ, et al. Changes in arterial stiffness and wave reflection with advancing age in healthy men and women: the Framingham Heart Study. Hypertension. 2004;43(6):1239–1245. doi:10.1161/01.HYP.0000128420.01881.aa
6. Ferreira I, van de Laar RJ, Prins MH, Twisk JW, Stehouwer CD. Carotid stiffness in young adults: a life-course analysis of its early determinants: the Amsterdam Growth and Health Longitudinal Study. Hypertension. 2012;59(1):54–61. doi:10.1161/HYPERTENSIONAHA.110.156109
7. Gepner AD, Korcarz CE, Colangelo LA, et al. Longitudinal effects of a decade of aging on carotid artery stiffness: the multiethnic study of atherosclerosis. Stroke. 2014;45(1):48–53. doi:10.1161/STROKEAHA.113.002649
8. Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J Am Coll Cardiol. 2010;55(13):1318–1327. doi:10.1016/j.jacc.2009.10.061
9. Ben-Shlomo Y, Spears M, Boustred C, et al. Aortic pulse wave velocity improves cardiovascular event prediction: an individual participant meta-analysis of prospective observational data from 17,635 subjects. J Am Coll Cardiol. 2014;63(7):636–646. doi:10.1016/j.jacc.2013.09.063
10. Palmefors H, DuttaRoy S, Rundqvist B, Borjesson M. The effect of physical activity or exercise on key biomarkers in atherosclerosis-a systematic review. Atherosclerosis. 2014;235(1):150–161. doi:10.1016/j.atherosclerosis.2014.04.026
11. Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380(9838):219–229. doi:10.1016/S0140-6736(12)61031-9
12. Nocon M, Hiemann T, Muller-Riemenschneider F, Thalau F, Roll S, Willich SN. Association of physical activity with all-cause and cardiovascular mortality: a systematic review and meta-analysis. Eur J Cardiovasc Prev Rehabil. 2008;15(3):239–246. doi:10.1097/HJR.0b013e3282f55e09
13. Haskell WL, Lee IM, Pate RR, et al. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc. 2007;39(8):1423–1434. doi:10.1249/mss.0b013e3180616b27
14. World Health Organization. Global Recommendations on Physical Activity for Health. World Health Organization; 2010. Available from: http://who.int/dietphysicalactivity/factsheet_recommendations/en/.
15. Seals DR, Desouza CA, Donato AJ, Tanaka H. Habitual exercise and arterial aging. J Appl Physiol. 2008;105(4):1323–1332. doi:10.1152/japplphysiol.90553.2008
16. Edwards NM, Daniels SR, Claytor RP, et al. Physical activity is independently associated with multiple measures of arterial stiffness in adolescents and young adults. Metabolism. 2012;61(6):869–872. doi:10.1016/j.metabol.2011.10.016
17. Horta BL, Schaan BD, Bielemann RM, et al. Objectively measured physical activity and sedentary-time are associated with arterial stiffness in Brazilian young adults. Atherosclerosis. 2015;243(1):148–154. doi:10.1016/j.atherosclerosis.2015.09.005
18. Andersson C, Lyass A, Larson MG, et al. Physical activity measured by accelerometry and its associations with cardiac structure and vascular function in young and middle-aged adults. J Am Heart Assoc. 2015;4(3):e001528. doi:10.1161/JAHA.114.001528
19. Hawkins M, Gabriel KP, Cooper J, Storti KL, Sutton-Tyrrell K, Kriska A. The impact of change in physical activity on change in arterial stiffness in overweight or obese sedentary young adults. Vasc Med. 2014;19(4):257–263. doi:10.1177/1358863X14536630
20. van de Laar RJ, Ferreira I, van Mechelen W, Prins MH, Twisk JW, Stehouwer CD. Lifetime vigorous but not light-to-moderate habitual physical activity impacts favorably on carotid stiffness in young adults: the Amsterdam growth and health longitudinal study. Hypertension. 2010;55(1):33–39. doi:10.1161/HYPERTENSIONAHA.109.138289
21. Germano-Soares AH, Andrade-Lima A, Menêses AL, et al. Association of time spent in physical activities and sedentary behaviors with carotid-femoral pulse wave velocity: a systematic review and meta-analysis. Atherosclerosis. 2018;269:211–218. doi:10.1016/j.atherosclerosis.2018.01.009
22. Laurent S, Cockcroft J, Van Bortel L, et al. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006;27(21):2588–2605. doi:10.1093/eurheartj/ehl254
23. Fernstrom M, Fernberg U, Eliason G, Hurtig-Wennlof A. Aerobic fitness is associated with low cardiovascular disease risk: the impact of lifestyle on early risk factors for atherosclerosis in young healthy Swedish individuals - the Lifestyle, Biomarker, and Atherosclerosis study. Vasc Health Risk Manage. 2017;13:91–99. doi:10.2147/VHRM.S125966
24. Shea JL, King MT, Yi Y, Gulliver W, Sun G. Body fat percentage is associated with cardiometabolic dysregulation in BMI-defined normal weight subjects. Nutr Metab Cardiovasc Dis. 2012;22(9):741–747. doi:10.1016/j.numecd.2010.11.009
25. Wildman RP, Muntner P, Reynolds K, et al. The obese without cardiometabolic risk factor clustering and the normal weight with cardiometabolic risk factor clustering: prevalence and correlates of 2 phenotypes among the US population (NHANES 1999-2004). Arch Intern Med. 2008;168(15):1617–1624. doi:10.1001/archinte.168.15.1617
26. Fernberg U Arterial stiffness and risk factors for cardiovascular disease in young adults. Örebro Universtiy, Repro 10/2019. School of Medical Sciences, Örebro University; 2019.
27. Siemens. Available from: https://www.healthcare.siemens.se/point-of-care/poc-cardiac-topics/cardiac-assays/cardiophase-hscrp.
28. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28(7):412–419. doi:10.1007/BF00280883
29. Pettee gabriel KK, Morrow JR
30. Trost SG, McIver KL, Pate RR. Conducting accelerometer-based activity assessments in field-based research. Med Sci Sports Exerc. 2005;37(11):S531–543. doi:10.1249/01.mss.0000185657.86065.98
31. Troiano RP, Berrigan D, Dodd KW, Masse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008;40(1):181–188. doi:10.1249/mss.0b013e31815a51b3
32. Matthews CE, Hagstromer M, Pober DM, Bowles HR. Best practices for using physical activity monitors in population-based research. Med Sci Sports Exerc. 2012;44(Suppl 1S):S68–76. doi:10.1249/MSS.0b013e3182399e5b
33. Matthews CE, Chen KY, Freedson PS, et al. Amount of time spent in sedentary behaviors in the United States, 2003-2004. Am J Epidemiol. 2008;167(7):875–881. doi:10.1093/aje/kwm390
34. Yrkesföreningar för fysisk aktivitet (YFA) och Svenska Läkaresällskapet. Rekommendationr Om Fysisk Aktivitet För Vuxna. Yrkesföreningar för fysisk aktivitet (YFA); 2011. Available from: http://www.yfa.se/rekommendationer-for-fysisk-aktivitet/.
35. Fernberg U, Fernstrom M, Hurtig-Wennlof A. Arterial stiffness associated to cardiorespiratory fitness and body mass index in young Swedish adults: the Lifestyle, Biomarkers, and Atherosclerosis study. Eur J Prev Cardiol. 2017;24(17):1809–1818. doi:10.1177/2047487317720796
36. Pauca AL, O’Rourke MF, Kon ND. Prospective evaluation of a method for estimating ascending aortic pressure from the radial artery pressure waveform. Hypertension. 2001;38(4):932–937. doi:10.1161/hy1001.096106
37. Weber T, Ammer M, Rammer M, et al. Noninvasive determination of carotid-femoral pulse wave velocity depends critically on assessment of travel distance: a comparison with invasive measurement. J Hypertens. 2009;27(8):1624–1630. doi:10.1097/HJH.0b013e32832cb04e
38. Ekblom-Bak E, Olsson G, Ekblom O, Ekblom B, Bergstrom G, Borjesson M. The daily movement pattern and fulfilment of physical activity recommendations in Swedish middle-aged adults: the SCAPIS pilot study. PLoS One. 2015;10(5):e0126336. doi:10.1371/journal.pone.0126336
39. Ried-Larsen M, Grontved A, Froberg K, Ekelund U, Andersen LB. Physical activity intensity and subclinical atherosclerosis in Danish adolescents: the European Youth Heart Study. Scand J Med Sci Sports. 2013;23(3):e168–177. doi:10.1111/sms.12046
40. Hagstromer M, Oja P, Sjostrom M. Physical activity and inactivity in an adult population assessed by accelerometry. Med Sci Sports Exerc. 2007;39(9):1502–1508. doi:10.1249/mss.0b013e3180a76de5
41. Ekblom-Bak E, Ekblom O, Andersson G, et al. Decline in cardiorespiratory fitness in the Swedish working force between 1995 and 2017. Scand J Med Sci Sports. 2019;29(2):232–239. doi:10.1111/sms.13328
42. World Health Organzation. Sweden Physical Activity Factsheet 2018. Available from: http://www.euro.who.int/en/countries/sweden/data-and-statistics/sweden. 2018.
43. Office of Disease Prevention and Health Promotion. Physical Activity Guidelines for Americans.
44. Ekelund U, Tarp J, Steene-Johannessen J, et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: systematic review and harmonised meta-analysis. BMJ. 2019;366:l4570. doi:10.1136/bmj.l4570
45. Bergman P, Hagströmer M. No one accelerometer-based physical activity data collection protocol can fit all research questions. BMC Med Res Methodol. 2020;20(1):141. doi:10.1186/s12874-020-01026-7
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.