Back to Journals » Clinical Ophthalmology » Volume 11
Higher order optical aberrations and visual acuity in a randomized controlled trial comparing transepithelial versus epithelium-off corneal crosslinking for progressive keratoconus
Authors Godefrooij DA, El Kandoussi M, Soeters N, Wisse RP ![]()
Received 11 April 2017
Accepted for publication 3 June 2017
Published 30 October 2017 Volume 2017:11 Pages 1931—1936
DOI https://doi.org/10.2147/OPTH.S139358
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Daniel A Godefrooij, Mustapha El Kandoussi, Nienke Soeters, Robert PL Wisse
Utrecht Cornea Research Group, Department of Ophthalmology, University Medical Center Utrecht, Utrecht, the Netherlands
Purpose: The purpose of this study was to compare the effects of transepithelial crosslinking (trans-CXL) versus epithelium-off crosslinking (epi-off CXL) for progressive keratoconus with respect to the development of higher order aberrations (HOAs) and their effects on visual acuity.
Materials and methods: A total of 61 patients were randomized and examined preoperatively and 1, 3, 6, and 12 months postoperatively in an academic referral center. Total corneal HOAs were compared between the two treatment groups using mixed linear modeling. Types of HOAs (coma, trefoil, and spherical aberration) that differed between groups were entered in a multivariable analysis to test their effect on uncorrected distance visual acuity (UDVA) and corrected distance visual acuity (CDVA).
Results: The epi-off CXL group had more flattening in maximal keratometry compared to the trans-CXL group (P=0.02). UDVA did not differ significantly between the groups (P=0.59); however, CDVA was significantly more improved in the trans-CXL group (P=0.02). Horizontal trefoil improved more in the epi-off group compared to the trans-CXL group (P=0.04), whereas the other HOAs were virtually unchanged in both groups. Differences in changes in HOAs between the two groups had no effect on either UCVA (P=0.76) or CDVA (P=0.96).
Conclusion: Although HOAs are clinically relevant determinants of vision quality in keratoconus patients, the change in total HOAs post treatment did not differ between the trans-CXL and epi-off CXL groups. Only horizontal trefoil differed significantly post treatment between the trans-CXL and epi-off CXL groups. However, this difference did not independently affect either UDVA or CDVA. Trans-CXL provides no benefit over epi-off CXL regarding visual relevant HOAs.
Keywords: keratoconus, crosslinking, epithelium off, epithelium on, transepithelial, higher order aberrations, HOAs
Introduction
Keratoconus is a disorder of the cornea characterized by changes in corneal collagen structure and progressive stromal thinning. The etiology of this thinning has been studied extensively and is believed to arise from a multifactorial interplay between genetic susceptibility, environmental factors, and chronic low-grade inflammation.1 The resulting decrease in the cornea’s mechanical stability leads to progressive ectasia, which in turn can lead to myopia, irregular astigmatism, higher order aberrations (HOAs), and – eventually – corneal scarring, all of which can result in a marked decrease in vision quality.2,3
Corneal collagen crosslinking (CXL) can be performed in order to stabilize the progression of keratoconus and prevent the need for corneal transplantation.4,5 The standard CXL treatment includes removal of the epithelium (ie, epithelium-off crosslinking [epi-off CXL]), followed by the application of riboflavin and ultraviolet (UV)-A irradiation.4 However, removing the epithelium causes significant postoperative pain and discomfort that can last several days, and it increases the risk of developing postoperative complications such as bacterial keratitis.6,7
Unlike epi-off CXL, transepithelial crosslinking (trans-CXL) does not require removal of the epithelium, thereby reducing postoperative pain and decreasing the risk of postoperative infection.8 However, because riboflavin does not readily penetrate the intact epithelium, various techniques have been developed to promote the absorption of riboflavin by the corneal stroma. The clinical effects of trans-CXL on corneal curvature have been studied in several studies; however, the results are inconsistent – two randomized controlled trials (RCTs) concluded that trans-CXL was less effective at treating progression of corneal ectasia compared to epi-off CXL, whereas another RCT concluded that the effects were similar between treatment groups.9–11 Interestingly, all three trials found significantly higher improvement in visual acuity in the trans-CXL group. We hypothesized that this improvement may be due to differences in the development of HOAs, as trans-CXL does not cause complications due to wound repair or long-lasting epithelial remodeling, both of which occur in epi-off CXL as a result of epithelial abrasion.
To test this hypothesis, we used data collected from a previously published RCT11 in order to investigate the effects of trans-CXL and epi-off CXL on HOAs, and we examined their effects on visual acuity.
Materials and methods
Dataset and study design
Data were derived from an RCT in which trans-CXL and epi-off CXL were performed to treat progressive keratoconus; this trial was conducted at the University Medical Center Utrecht in the Netherlands.11 Adult patients who were diagnosed with progressive keratoconus and were candidates for CXL were enrolled from May 30, 2011 through September 4, 2013. Trans-CXL was performed with Ricrolin TE solution (consisting of riboflavin 0.1% eye drops with dextran T500 15 mg and EDTA; Sooft Italia, Montegiorgio, Italy). Epi-off CXL was performed in accordance with the Dresden protocol, using 0.1% riboflavin with 20% dextran (Medio Cross, Burlington, MA, USA). Riboflavin soaking time (30 min) and UV irradiation (3 mW/cm2 for 30 min) were identical between the treatment groups. Detailed information regarding the inclusion criteria and surgical procedures has been published previously.11 The study was approved and monitored by the University Medical Center Utrecht Ethics Review Board (reference number NL29961) and registered at ClinicalTrials.gov (identification number NCT02349165). All procedures were conducted in accordance with the ethical standards established by the Declaration of Helsinki and local laws regarding privacy and research in human subjects. Written informed consent was obtained from all patients prior to their participation.
Assessment of corneal optical aberrations
Patients were examined preoperatively and 1, 3, 6, and 12 months postoperatively. At each visit, measurements included manifest refraction, uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), and Scheimpflug corneal tomography (Pentacam HR; Oculus, Wetzlar, Germany). In the event that the tomogram did not reach the minimum quality criterion of 90%, tomography was repeated up to three times and the best scan was used to assess HOAs. Patients who wore contact lenses were instructed to discontinue use at least 1 week (for scleral and soft contact lenses) or 2 weeks (for hybrid and rigid gas-permeable lenses) prior to each examination.11 Corneal optical aberrations were measured at each visit using the Pentacam device, which measures anterior and posterior corneal elevations over the central 6.0 mm and calculates HOAs from these elevation data. The software program reports aberrations at the anterior and posterior surfaces, as well as for the total cornea. Total corneal aberrations were used as the outcome parameter in this study because this outcome is most relevant to patients. The Pentacam software subdivides this outcome into the following two composite values: total corneal lower order aberrations (LOAs) and total corneal HOAs. Normalized coefficients were expressed in microns of wavefront error (in root mean square) and labeled with International Organization for Standardization (ISO)-standardized double index Zernike symbols. HOAs were reported with their Zernike weight coefficient, as the polynomial coefficient is considered to be invariant. Total corneal HOAs were calculated based on the third- to eigth-order aberrations. The following LOA subtypes were reported in detail: defocus  , vertical astigmatism
, vertical astigmatism  , and horizontal astigmatism
, and horizontal astigmatism  . HOA subtypes were reported in detail for horizontal coma and vertical coma (
. HOA subtypes were reported in detail for horizontal coma and vertical coma ( and
and  , respectively), horizontal trefoil and vertical trefoil (
, respectively), horizontal trefoil and vertical trefoil ( and
and  , respectively), and spherical aberration
, respectively), and spherical aberration  .
.
Statistical analysis
Visual acuity was converted to the logarithm of the minimal angle of resolution (logMAR). Baseline measurements were compared between the two groups using an independent samples t-test. Normality of baseline measurements was assessed using a Q–Q plot. Because both positive and negative HOAs can impair visual acuity, we used absolute values for all HOAs. We used a linear mixed model with generalized estimating equations correction to analyze trends over time, and outcomes were corrected for baseline values. HOAs that differed significantly between the two treatment groups were entered in a multivariable analysis with treatment as an interaction term and visual acuity as the outcome, while correcting for changes in LOAs. Uncorrected visual acuity and corrected visual acuity were analyzed separately. Except where indicated otherwise, data are reported as mean ± standard deviation. Differences with a P-value <0.05 were considered as statistically significant. All statistical analyses were performed using SPSS version 21.0 (IBM Corporation, Armonk, NY, USA).
Results
Baseline characteristics
Sixty-one eyes of 61 patients (47 men and 14 women) with progressive keratoconus were included in this randomized clinical trial. These 61 patients were randomly assigned to either the epi-off CXL group (n=26) or the trans-CXL group (n=35). Baseline characteristics were similar between the two treatment groups apart from a lower spherical equivalent and logMAR UDVA in the trans-CXL group (Table 1).
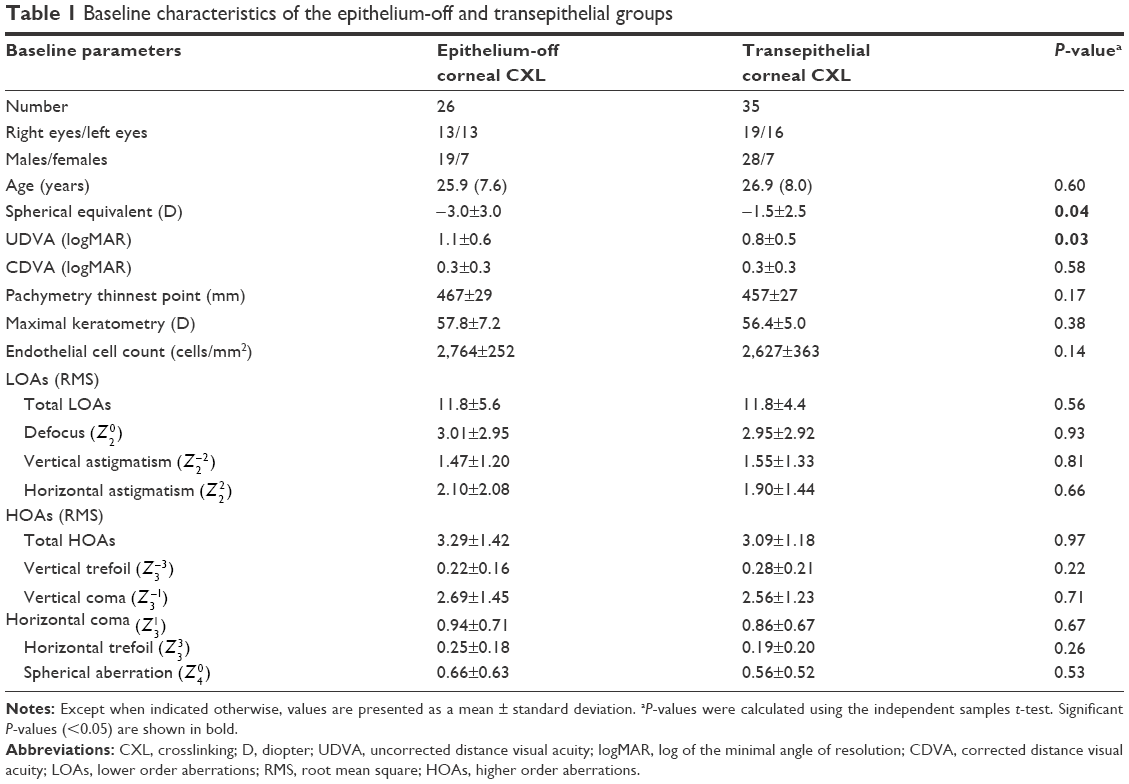 | Table 1 Baseline characteristics of the epithelium-off and transepithelial groups |
Follow-up and adverse events
A total of four patients (6% of patients, two patients in each group) were lost to follow-up at the last follow-up visit. Two of these patients moved abroad, one patient received follow-up care at another hospital, and one patient was retreated with epi-off CXL 10 months after the initial trans-CXL treatment. At the 1-, 3-, and 6-month visit, data were missing from zero (0%), two (3%), and four (6%) patients, respectively. No adverse events were reported in the trans-CXL group; in contrast, four patients in the epi-off CXL group (15% of patients) developed an adverse event: one patient developed herpes simplex keratitis, one patient had a sterile infiltrate, and two patients had delayed epithelial healing.11
Clinical outcomes
The clinical outcomes in the trans-CXL and epi-off CXL groups 1, 3, 6, and 12 months post treatment are summarized in Table 2. The two groups differed significantly with respect to both maximal keratometry (P=0.02) and corneal thickness (P<0.001). The two groups did not differ significantly with respect to their change in UCVA (P=0.59). In contrast, CDVA differed significantly between the two groups (P=0.02), with the trans-CXL group having a larger improvement compared to the epi-off CXL group. Complete details regarding the clinical outcomes of this trial have been published.11
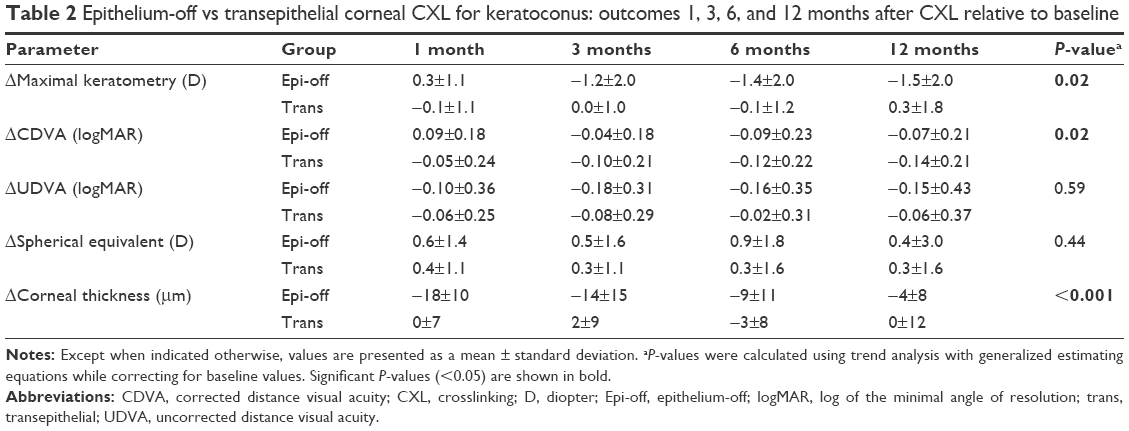 | Table 2 Epithelium-off vs transepithelial corneal CXL for keratoconus: outcomes 1, 3, 6, and 12 months after CXL relative to baseline |
HOAs
Table 3 summarizes the change in optical aberrations in the two treatment groups. Only horizontal trefoil differed significantly between the two groups (P=0.04), with a larger improvement in the epi-off CXL group. We found no significant difference between the treatment groups with respect to total LOAs (P=0.41) or total HOAs (P=0.98).
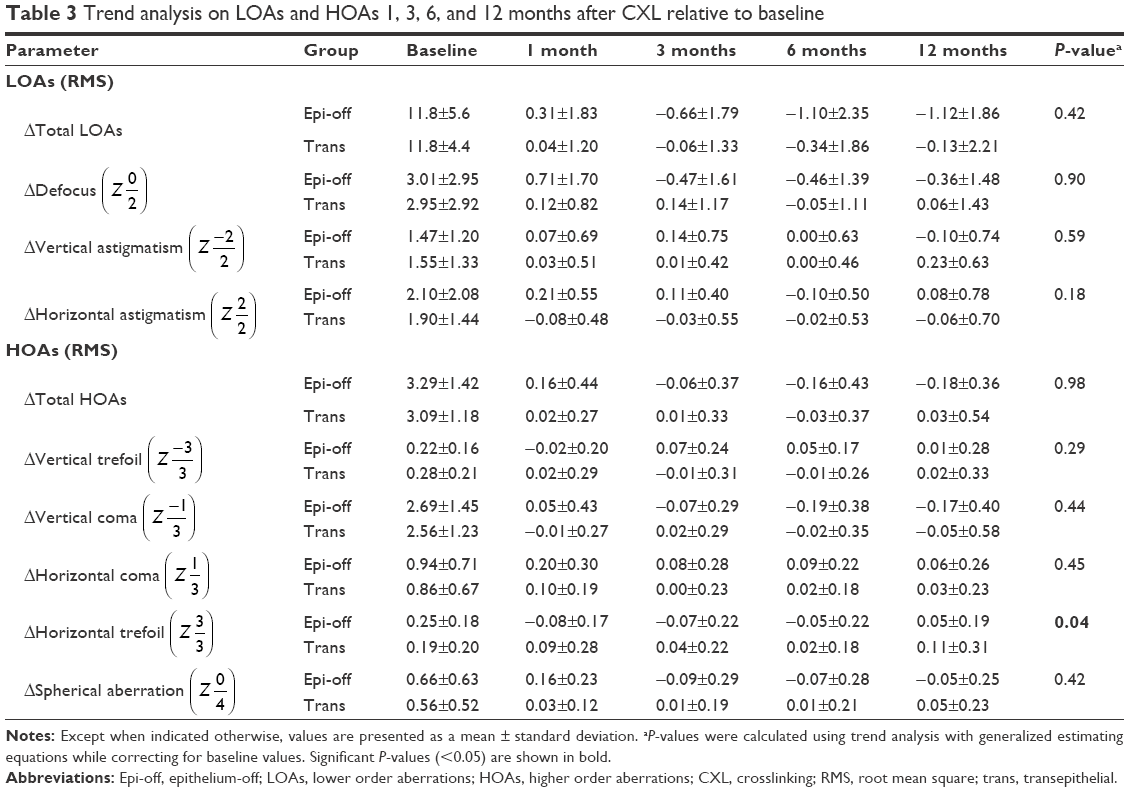 | Table 3 Trend analysis on LOAs and HOAs 1, 3, 6, and 12 months after CXL relative to baseline |
Relationship between visual acuity and horizontal trefoil
Our analysis revealed that the difference in horizontal trefoil between the two treatment groups did not independently affect either UDVA (P=0.76) or CDVA (P=0.96). Similar results were obtained when we corrected for the change in LOAs (P=0.75 and P=0.84 for UDVA and CDVA, respectively).
Discussion
Changes in HOAs do not differ between patients who undergo trans-CXL and patients who undergo epithelial-off CXL; only horizontal trefoil differed significantly between the groups. Moreover, we found no independent relationship between the change in horizontal trefoil and visual acuity outcome. Therefore, we conclude that no clinically relevant differences exist between treatment groups with respect to the effect of treatment on HOAs.
A major strength of this study is our use of data obtained from a randomized clinical trial, which provided the best setting to compare treatment effects without confounding factors. In addition, all measurements and refractions were performed by one senior optometrist with extensive experience in keratoconus care. Moreover, the follow-up rate was high, with 57 out of 61 patients completing the follow-up course. In this study, we focused on the HOA subtypes that are most relevant to clinical practice (ie, coma, trefoil, and spherical aberrations). We also performed our analyses using total corneal HOAs and anterior HOAs only, with nearly identical results. Finally, the clinical results of our RCT are consistent with other results comparing trans-CXL and epi-off CXL.2,17,18
A limitation of this study is the use of a Scheimpflug-based device, which calculates Zernike coefficients and HOAs based on anterior and posterior elevation maps, rather than using a wavefront device that directly measures optical aberrations. On the other hand, the use of a Scheimpflug-based device could also be considered as a strength because its repeatability in keratoconus patients has been proven to be superior compared to the Placido topographer and the Javal keratometer.19 Another limitation of this study is that whole-eye optical aberrations were not measured during this RCT. Optical aberrations within the eye (ie, internal aberrations) can compensate for corneal aberrations, particularly in healthy eyes.12–14 An additional limitation of this study is that only high-contrast visual acuity was tested in this RCT. Previous studies found that low-contrast visual acuity testing can be more sensitive when measuring the effect of HOAs on visual acuity.15,16 To the best of our knowledge, the effect of HOAs on low-contrast visual acuity following CXL has never been studied.
An auxiliary limitation to this study is the baseline imbalance between the two treatment groups with a lower spherical equivalent and logMAR UDVA in the trans-CXL group. However, the applied trend analysis is relatively robust for baseline imbalances (because it is focused at relative differences and corrected for baseline values), and both LOAs and HOAs were equally distributed between the treatment groups. Therefore, we think that our conclusions are not affected by this baseline imbalance.
In this study, only horizontal trefoil differed significantly between the two treatment groups. Optical disturbances caused by a slight haze after CXL in the epi-off CXL group might be the pathophysiological explanation because the difference between the treatment groups was largest 1 month after treatment. Another explanation for the difference in horizontal trefoil could be that this finding is a type I error, because the difference between the two groups was relatively small and fluctuating over time. Furthermore, there was no difference in total HOAs between the treatment groups (P=0.98) and there was no biological substrate that would explain a difference in only this specific HOA subtype.20 Moreover, if any type of multiple testing correction was applied, the difference in horizontal trefoil would become insignificant. Vinciguerra et al21 and Caporossi et al22 reported that total HOAs and/or HOA subtypes improved following trans-CXL or epi-off CXL; however, neither group studied the relationship between HOAs and visual acuity. Studies by Greenstein et al23 and Ghanem et al24 found significant reductions in coma, spherical, and trefoil aberrations that were not correlated with an improvement in visual acuity. On the other hand, our research group previously reported that changes in horizontal coma have an effect on UCVA following epi-off CXL.25
Three RCTs studying trans-CXL versus epi-off CXL found significant improvement in visual acuity in the trans-CXL group.9–11 This improvement in visual acuity in the trans-CXL group could be related to a decrease in HOAs. Alternatively, it could be due to the reduced need for wound repair compared to epi-off CXL. However, neither of these possibilities is supported by the results of our study.
Conclusion
Our randomized clinical trial detected no clinically relevant difference between patients who received trans-CXL and epi-off CXL with respect to HOAs and the effect of HOAs on visual acuity. Specifically, only horizontal trefoil differed significantly between treatment groups but did not affect visual acuity outcomes. Based on these results, we conclude that trans-CXL provides no benefit over epi-off CXL regarding the effect on visual relevant HOAs.
Acknowledgment
Daniel Godefrooij and Robert Wisse are supported by unrestricted grants from the Dr F.P. Fischer Foundation, facilitated by the Foundation Friends from the UMC Utrecht.
Disclosure
The authors report no conflicts of interest in this work.
References
Wisse RP, Kuiper JJ, Gans R, Imhof S, Radstake TR, Van der Lelij A. Cytokine expression in keratoconus and its corneal microenvironment: a systematic review. Ocul Surf. 2015;13(4):272–283. | ||
Meiri Z, Keren S, Shenhav L, Varssano D. Efficacy of corneal collagen cross-linking for the treatment of keratoconus: a systematic review and meta-analysis. Cornea. 2016;35(3):417–428. | ||
Rabinowitz Y. Keratoconus. Surv Ophthalmol. 1998;42(4):297–319. | ||
Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-A-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135(5):620–627. | ||
Godefrooij DA, Gans R, Imhof SM, Wisse RPL. Nationwide reduction in the number of corneal transplantations for keratoconus following the implementation of cross-linking. Acta Ophthalmol. 2016;94(7):675–678. | ||
Ghanem VC, Ghanem RC, de Oliveira R. Postoperative pain after corneal collagen cross-linking. Cornea. 2013;32(1):20–24. | ||
Koller T, Mrochen M, Seiler T. Complication and failure rates after corneal crosslinking. J Cataract Refract Surg. 2009;35(8):1358–1362. | ||
Chan E, Snibson GR. Current status of corneal collagen cross-linking for keratoconus: a review. Clin Exp Optom. 2013;96(2):155–164. | ||
Bikbova G, Bikbov M. Standard corneal collagen crosslinking versus transepithelial iontophoresis-assisted corneal crosslinking, 24 months follow-up: randomized control trial. Acta Ophthalmol. 2016;94(7):e600–e606. | ||
Nawaz S, Gupta S, Gogia V, Sasikala NK, Panda A. Trans-epithelial versus conventional corneal collagen crosslinking: a randomized trial in keratoconus. Oman J Ophthalmol. 2015;8(1):9–13. | ||
Soeters N, Wisse RP, Godefrooij DA, Imhof SM, Tahzib NG. Transepithelial versus epithelium-off corneal cross-linking for the treatment of progressive keratoconus: a randomized controlled trial. Am J Ophthalmol. 2015;159(5):821–828. | ||
Wang L, Santaella RM, Booth M, Koch DD. Higher-order aberrations from the internal optics of the eye. J Cataract Refract Surg. 2005;31(8):1512–1519. | ||
Artal P, Berrio E, Guirao A, Piers P. Contribution of the cornea and internal surfaces to the change of ocular aberrations with age. J Opt Soc Am A Opt Image Sci Vis. 2002;19(1):137–143. | ||
Artal P, Guirao A, Berrio E, Williams DR. Compensation of corneal aberrations by the internal optics of the eyes. J Vis. 2001;1(1):1–8. | ||
Pepose JS, Applegate RA. Making sense out of wavefront sensing. Am J Ophthalmol. 2005;139(2):335–343. | ||
Pesudovs K, Marsack J, Donnelly W, Thibos LN, Applegate RA. Measuring visual acuity – mesopic or photopic conditions, and high or low contrast letters? J Refract Surg. 2004;20(5):S508–S514. | ||
Al Fayez MF, Alfayez S, Alfayez Y. Transepithelial versus epithelium-off corneal collagen cross-linking for progressive keratoconus: a prospective randomized controlled trial. Cornea. 2015;34(suppl 10):53–56. | ||
Gatzioufas Z, Raiskup F, O’Brart D, Spoerl E, Panos GD, Hafezi F. Transepithelial corneal cross-linking using an enhanced riboflavin solution. J Refract Surg. 2016;32(6):372–377. | ||
Hashemi H, Yekta A, Khabazkhoob M. Effect of keratoconus grades on repeatability of keratometry readings: comparison of 5 devices. J Cataract Refract Surg. 2015;41(5):1065–1072. | ||
Ioannidis JP. Why most published research findings are false. PLoS Med. 2005;2(8):e124. | ||
Vinciguerra R, Romano MR, Camesasca FI, et al. Corneal cross-linking as a treatment for keratoconus: four-year morphologic and clinical outcomes with respect to patient age. Ophthalmology. 2013;120(5):908–916. | ||
Caporossi A, Mazzotta C, Baiocchi S, Caporossi T. Long-term results of riboflavin ultraviolet a corneal collagen cross-linking for keratoconus in Italy: the Siena eye cross study. Am J Ophthalmol. 2010;149(4):585–593. | ||
Greenstein SA, Fry KL, Hersh MJ, Hersh PS. Higher-order aberrations after corneal collagen crosslinking for keratoconus and corneal ectasia. J Cataract Refract Surg. 2012;38(2):292–302. | ||
Ghanem RC, Santhiago MR, Berti T, Netto MV, Ghanem VC. Topographic, corneal wavefront, and refractive outcomes 2 years after collagen crosslinking for progressive keratoconus. Cornea. 2014;33(1):43–48. | ||
Wisse RPL, Gadiot S, Soeters N, Godefrooij DA, Imhof SM, van der Lelij A. Higher-order aberrations one year after corneal crosslinking for keratoconus and their independent effect on visual acuity. J Cataract Refract Surg. 2016;42(7):1046–1052. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.