Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
High Serum FABP4 Levels are Negatively Associated with the Reversion from Prediabetes to Normal Glucose Tolerance: A 2-Year Retrospective Cohort Community Study
Authors Gu M, Lin Y, Gai X, Wei X, Lu C, Wang Y, Ding X, Peng Y, Ma Y
Received 22 May 2022
Accepted for publication 20 July 2022
Published 28 July 2022 Volume 2022:15 Pages 2217—2225
DOI https://doi.org/10.2147/DMSO.S374912
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Mingyu Gu,1,2,* Yi Lin,2,* Xianying Gai,3,* Xiaohui Wei,2 Chunhua Lu,4 Yufan Wang,2 Xiaoying Ding,2,* Yongde Peng,1,2 Yuhang Ma2
1Department of Endocrinology and Metabolism, Shanghai General Hospital of Nanjing Medical University, Shanghai, 200080, People’s Republic of China; 2Department of Endocrinology and Metabolism, Shanghai General Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200080, People’s Republic of China; 3Department of Endocrinology, Shanghai Sijing Hospital, Shanghai, 201601, People’s Republic of China; 4Community Health Service Center of Sijing, Shanghai, 201601, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yongde Peng, Department of Endocrinology and Metabolism, Shanghai General Hospital of Nanjing Medical University, 100 Haining Road, Shanghai, 200080, People’s Republic of China, Email [email protected] Yuhang Ma, Department of Endocrinology and Metabolism, Shanghai General Hospital, Shanghai Jiao Tong University School of Medicine, 100 Haining Road, Shanghai, 200080, People’s Republic of China, Email [email protected]
Objective: To explore the relationship between the level of fatty acid-binding protein 4 (FABP4) and reversion from prediabetes to normal glucose tolerance (NGT).
Methods: A two-year retrospective cohort study was conducted on 398 participants with complete information. These 398 participants were divided into an NGT group and an abnormal glucose metabolism (AGM) group after 2 years of follow-up. The baseline level of FABP4 was determined, and the role of FABP4 in predicting reversion from prediabetes to NGT was investigated using an unconditional logistic regression model.
Results: Over the two-year follow-up period, 37.4% (149/398) of the participants reverted from prediabetes to NGT. The participants with AGM had a higher baseline level of FABP4 than those with NGT. The baseline level of FABP4 was significantly negatively correlated with reversion from prediabetes to NGT. After adjusting for age, sex, body mass index and waist-to-hip ratio, the level of fasting blood glucose (FBG) [odds ratio (OR) 0.336, 95% confidence interval (CI) (0.196– 0.576)], 2-h post-challenge blood glucose (2hBG) [OR 0.697, 95% CI (0.581– 0.837)], and FABP4 [OR 0.960, 95% CI (0.928– 0.993)] at baseline were significant independent predictors of reversion from prediabetes to NGT. The area under the curve (AUC) value of the receiver operating characteristic curve for FABP4 was 0.605 (95% CI: 0.546– 0.665), and the AUC for FABP4 combined with FBG and 2hBG was 0.716 (95% CI: 0.663– 0.769).
Conclusion: A higher baseline level of FABP4 was positively correlated with an adverse profile of diabetes risk factors and negatively correlated with reversion from prediabetes to NGT. FABP4, FBG and 2hBG were predictors of reversion from prediabetes to NGT.
Keywords: fatty acid-binding protein 4, FABP4, prediabetes, normal glucose tolerance, abnormal glucose metabolism
Introduction
The prevalence of diabetes in China has increased rapidly over the years, causing a serious socioeconomic burden. Research has shown that the prevalence of diabetes and prediabetes in Chinese adults over 18 years of age has reached 12.8% and 35.2%, respectively.1 Prediabetes is one of the risk factors for diabetes.2 Previous studies have shown that the annual rate of progression from prediabetes to diabetes is 5%-10%, and 70% of individuals with prediabetes will eventually develop diabetes.3–5 Lifestyle interventions can effectively delay progression from prediabetes to diabetes, and individuals with prediabetes who revert to normoglycemia have a reduced risk of diabetes.6,7 However, the pathogenesis of progression from prediabetes to diabetes has not been fully clarified, and therapeutic targets remain to be identified within this mechanism.
Fatty acid-binding protein (FABP) is a member of the intracellular lipid-binding protein superfamily. FABP plays an important role in the uptake, transport and metabolic regulation of long-chain fatty acids.8 FABP4 (also known as A-FABP or aP2) is mainly found in adipose tissue and macrophages and plays an important role in regulating metabolism and inflammatory responses.9,10 The serum level of FABP4 has been found to be a predictor of the incidence of type 2 diabetes,11 gestational diabetes mellitus,12 metabolic disorder–associated fatty liver disease (MAFLD)13 and metabolic syndrome.14 Moreover, the level of FABP4 is associated with insulin resistance and insulin secretion.15 Whether serum FABP4 levels are associated with reversion from prediabetes to normal glucose tolerance (NGT) is a question that remains to be further investigated.
In this study, we explored the relationship between the baseline level of FABP4 and reversion from prediabetes to NGT using data from a cohort of individuals with prediabetes in a community in Shanghai over a 2-year follow-up period.
Methods
Participants and Ethical Approval
This study was part of an epidemiologic study that took place in the countryside of Shanghai, China. A total of 5569 individuals over 40 years of age participated in the survey from July 2012 to March 2013 (baseline visits) and from July 2014 to March 2015 (2-year follow-up visits). At baseline and the 2-year follow-up, all participants underwent standardized interviews, physical examinations, and a standard 75-g oral glucose tolerance test (OGTT) or steamed bread meal test depending on whether they had diabetes.
A total of 1213 local residents were defined as having prediabetes after undergoing a standard 75-g OGTT at baseline. We randomly selected 404 participants for this study through random number table Ultimately, 398 participants with complete information were enrolled. After two years of follow-up, 37.4% (149/398) of the participants reverted from prediabetes to NGT. Additionally, 14.1% (56/398) of the participants developed diabetes, and 48.5% (193/398) of the participants remained prediabetic. We combined participants with prediabetes and diabetes into the abnormal glucose metabolism (AGM) group (Figure 1).
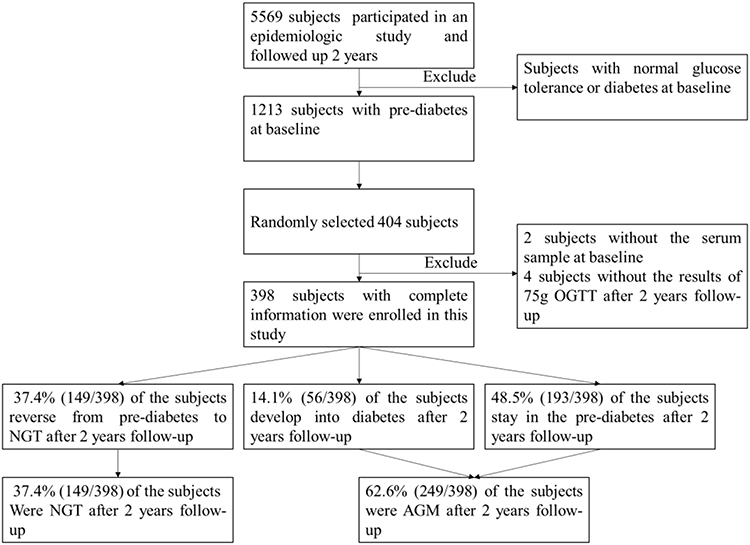 |
Figure 1 Flow chart of study participant enrollment. Abbreviations: OGTT, oral glucose tolerance test; NGT, normal glucose tolerance; AGM, abnormal glucose metabolism. |
The study followed the principles in the Declaration of Helsinki. The study protocol was approved by the Committee on Human Research at Shanghai General Hospital, Shanghai Jiao Tong University School of Medicine. Written informed consent was obtained from each participant.
Data Collection
Physical Examinations
Physical examinations were performed with participants in a fasted state. Blood pressure was measured thrice consecutively in each participant after at least 15 minutes of rest in a seated position, and the average of the three measurements was recorded. Height, weight, waist circumference (WC) and hip circumference (HC) were measured while the participants were standing. Each participant’s body mass index (BMI) and waist-to-hip ratio (WHR) were calculated after the data were collected.
Laboratory Tests
Venous blood samples were collected from all participants in the morning after they had fasted overnight for at least 10 h. The baseline serum FABP4 level was determined using a validated enzyme-linked immunosorbent assay (ELISA) kit (R&D Systems, Inc. Catalog Number DFBP40). Plasma glucose concentrations, total cholesterol (TC), low-density lipoprotein cholesterol (LDL), high-density lipoprotein cholesterol (HDL), and triglycerides (TG) were measured enzymatically using an automatic biochemical analyzer (BECKMAN COULTER AU5800). Insulin concentrations was detected by automatic immunoluminescence analyzer (Abbott ARCHITECT i2000SR). Glycosylated hemoglobin (HbA1c) was detected by glycosylated hemoglobin analyzer (ARKRAY, ADAMS A1C HA-8180).
The homeostasis model assessment (HOMA) was used to estimate insulin resistance (HOMA-IR) and β-cell function (HOMA-β) as follows: HOMA-IR=[fasting insulin (μU/mL)×fasting glucose (mmol/L)]/22.5 and HOMA-β=[20×fasting insulin (μU/mL)]/[fasting glucose (mmol/L)–3.5].16
Diagnostic Criteria
According to the World Health Organization (WHO) criteria,17 1) NGT is defined as fasting blood glucose (FBG) < 6.1 mmol/L and 2-hour blood glucose after a 75-g glucose challenge (2hBG) < 7.8 mmol/L; 2) prediabetes is defined as impaired fasting glucose (IFG) and impaired glucose tolerance (IGT), where IFG is defined as FBG 6.1–6.9 mmol/L and 2hBG<7.8 mmol/L, while IGT is defined as FBG<7.0 mmol/L and 2hBG<11.1 mmol/L; and 3) diabetes is defined as FBG ≥7.0 mmol/L, 2hBG≥11.1 mmol/L, or a history of diabetes.
Statistical Analysis
Analyses were performed with SPSS version 22.0 (Chicago, IL, USA). Data were tested for normality; if they did not follow the normal distribution, they were logarithmically transformed for statistical analysis as needed. Continuous data with a normal distribution are presented as the mean±standard deviation (SD) and were compared using independent-sample t-tests. Nonnormally distributed continuous data are presented as the median (interquartile range, IQR). Categorical variables were compared using the chi-square test. Correlations between FABP4 and anthropometric and biochemical variables were analyzed by Pearson’s or Spearman correlation. An unconditional logistic regression model was used to identify baseline variables that were independent predictors of reversion from prediabetes to NGT. The predictive ability of independent predictors and their combinations was assessed using the area under the curve (AUC) value of the receiver operating characteristic (ROC). All P values were 2-tailed, and a P value < 0.05 was considered statistically significant.
Results
Comparison of Clinical Parameters Between Participants with NGT and Those with AGM at Baseline and the 2-Year Follow-Up
As shown in Table 1, compared to participants with NGT, participants with AGM had increased WC, glycated hemoglobin (HbA1c), FBG, 2hPG and FABP4 at baseline (all P<0.01). There were no significant differences in age, sex, systolic blood pressure (SBP), diastolic blood pressure (DBP), BMI, WHR, HOMA-IR, HOMA-β, TC, TG, LDL, HDL, or TG/HDL between participants with AGM and those with NGT at baseline. At the 2-year follow-up, participants with AGM had higher BMI, WC, WHR, HbA1c, FBG, 2hBG, TG, TC and TG/HDL than participants with NGT (all P<0.01).
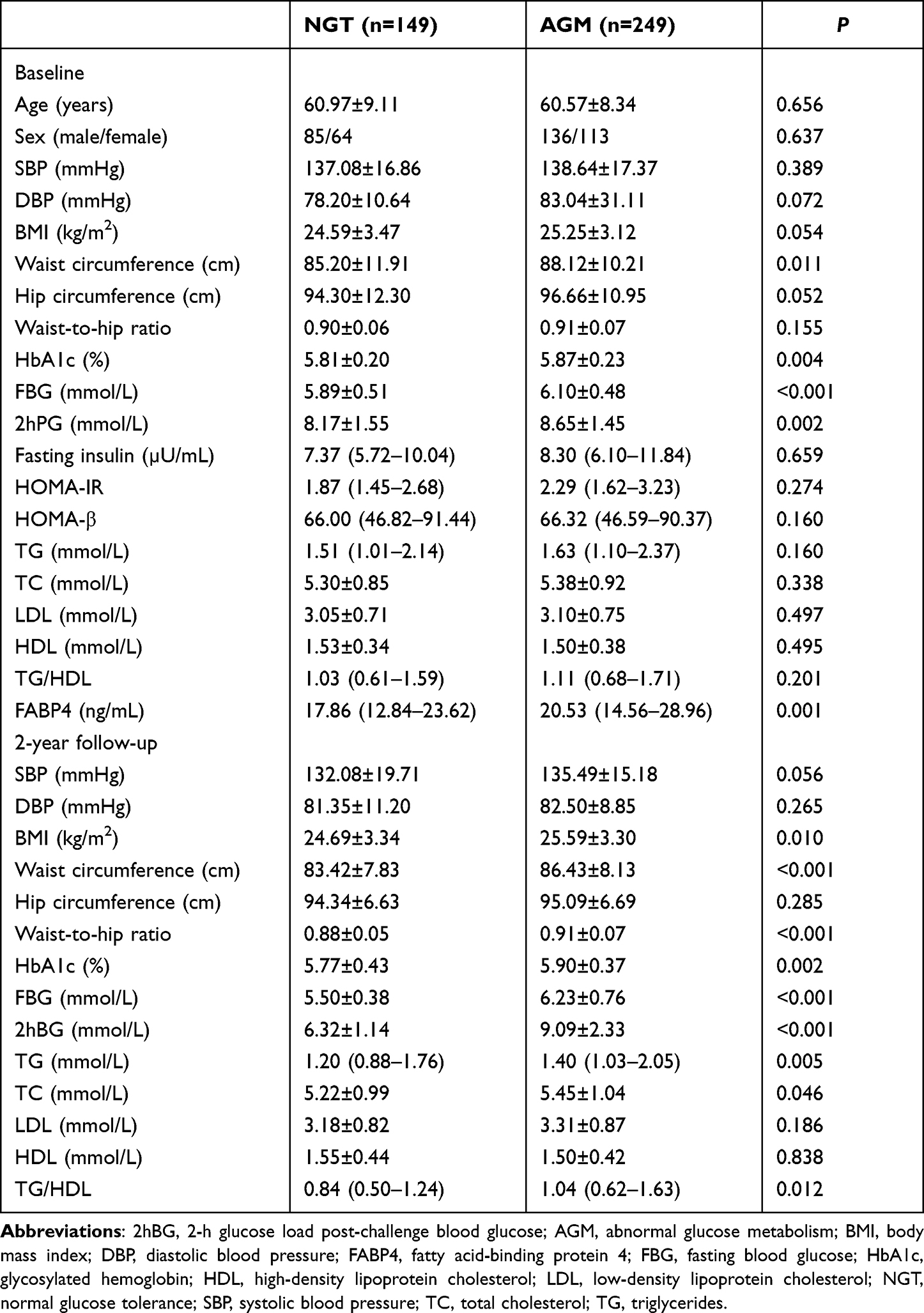 |
Table 1 Clinical Parameters of Participants with Normal Glucose Tolerance and Abnormal Glucose Metabolism at Baseline and the 2-Year Follow-Up |
Correlations Between the Level of FABP4 at Baseline and the Clinical Parameters of the Participants at the 2-Year Follow-Up
We found that the baseline level of FABP4 was significantly negatively correlated with reversion from prediabetes to NGT and positively correlated with age, BMI, WC, HC, 2hBG, TG, TC and LDL at the 2-year follow-up (all P<0.01, Table 2).
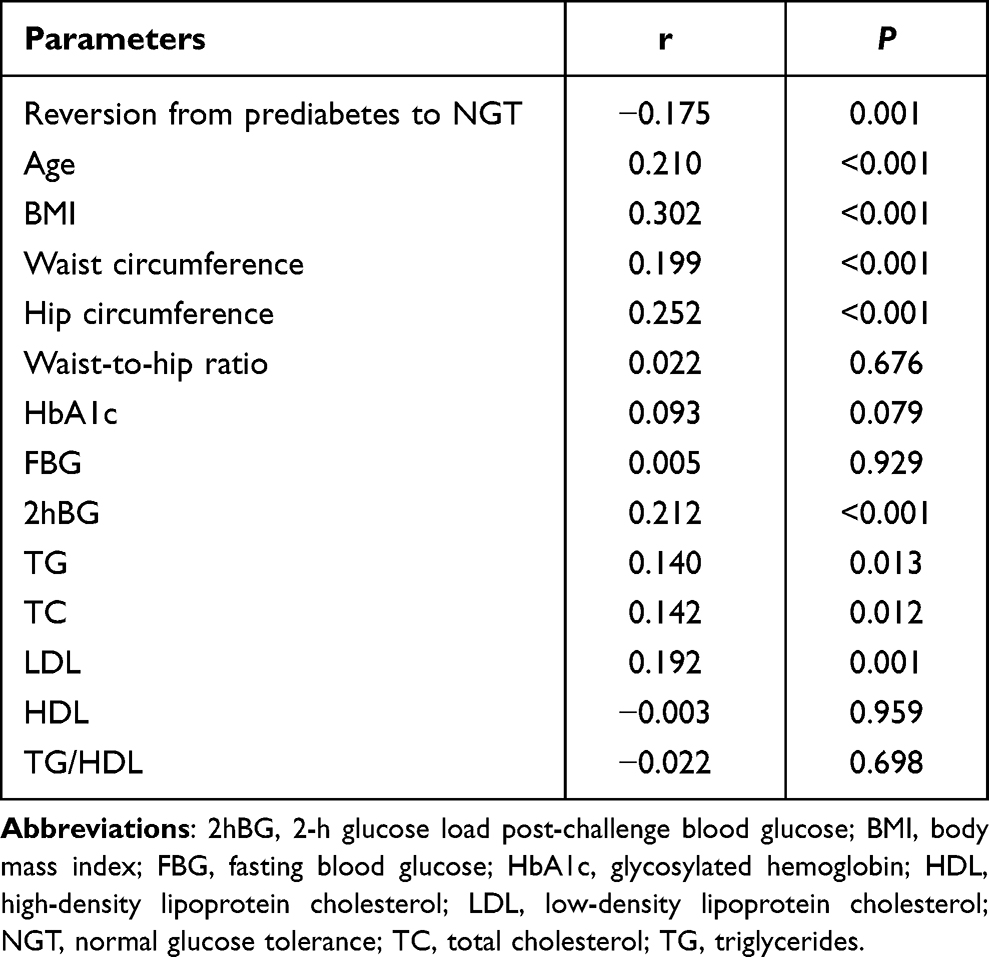 |
Table 2 Correlations Between FABP4 Levels and the Clinical Parameters of Participants at the End of the Follow-Up Period |
Baseline Variables Predicting Reversion from Prediabetes to NGT
Baseline variables that were significantly different between participants with NGT and those with AGM after 2 years of follow-up (shown in Table 1) were analyzed by logistic regression analysis to determine the predictors associated with reversion from prediabetes to NGT. We found that the levels of FBG [odds ratio (OR) 0.322, 95% confidence interval (CI) (0.188–0.549)], 2hBG [OR 0.699, 95% CI (0.584–0.837)] and FABP4 [OR 0.958, 95% CI (0.931–0.985)] at baseline were significant independent predictors of reversion from prediabetes to NGT. After adjusting for age, sex, BMI and WHR, the levels of FBG [OR 0.336, 95% CI (0.196–0.576)], 2hBG [OR 0.697, 95% CI (0.581–0.837)] and FABP4 [OR 0.960, 95% CI (0.928–0.993)] at baseline were also significant independent predictors of reversion from prediabetes to NGT (Table 3).
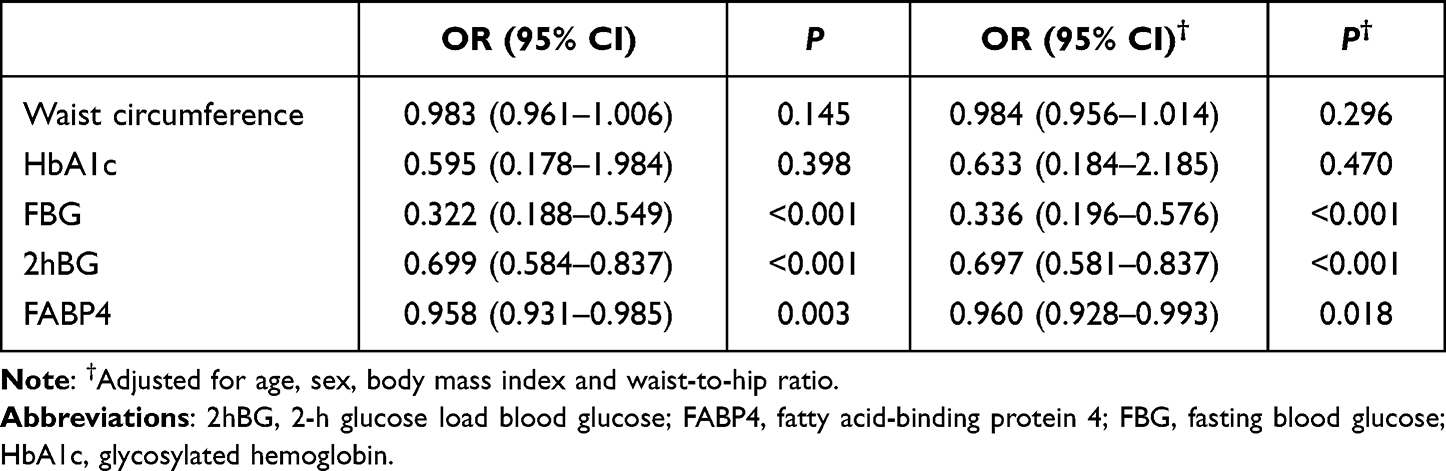 |
Table 3 The Baseline Variables That Predict Reversion from Prediabetes to Normal Glucose Tolerance |
ROC Curve Analysis for the Predictors of Reversion from Prediabetes to NGT
ROC curve analysis was conducted to determine and compare the utility of FBG, 2hBG, FABP4 and their combinations in predicting reversion from prediabetes to NGT. The ROC curve demonstrated that FBG, 2hBG and FABP4 can differentiate between NGT and AGM at a cut-off ≤5.82mmol/L, ≤9,19mmol/L and ≤25.37ng/mL, respectively (Table 4). The AUCs of FBG, 2hBG and FABP4 were 0.629 (95% CI: 0.569–0.6889), 0.601 (95% CI: 0.541–0.662), and 0.605 (95% CI: 0.546–0.665), respectively. However, combining these variables improved their predictive performance; the combination of all three variables had the greatest AUC [0.716 (95% CI: 0.663–0.769)] (Figure 2).
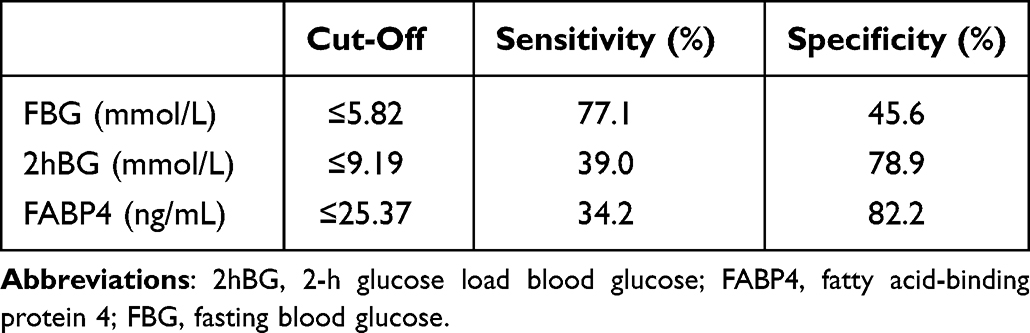 |
Table 4 Cut off Value of FBG, 2hBG and FABP4 in Predict Reversion from Prediabetes to Normal Glucose Tolerance |
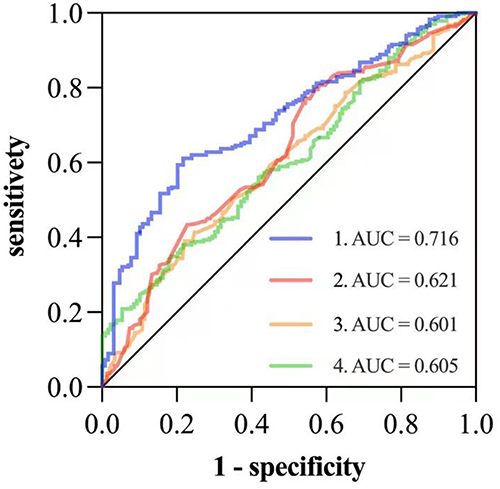 |
Figure 2 Receiver operating characteristic (ROC) curves of baseline FBG (Line 2), baseline 2hPG (Line 3), baseline FABP4 (Line 4), and a combination of the three (Line 1) for predicting reversion from prediabetes to normal glucose tolerance. |
Discussion
This study enrolled 398 participants with prediabetes. After 2 years of follow-up, 37.4% of the participants reverted from prediabetes to NGT, and 14.1% of the participants developed diabetes. The annual progression rate from prediabetes to diabetes was 7.05% in our study. Previous studies have shown that prediabetes progresses to diabetes at an annual rate of 5–10%.3–5 Our findings were similar to those of previous studies, which suggests that the participants were representative of the general population.
Many factors have been found to be involved in progression from prediabetes to diabetes. Obesity is a major risk factor for chronic diseases, including type 2 diabetes mellitus (T2DM). BMI, WC and WHR are useful in assessing obesity.18 We found a higher baseline WC in the AGM group than in the NGT group after 2 years of follow-up. In Chinese adults, the treatment of participants with BMI≥28 to maintain WC under 85 cm for men or 80 cm for women could prevent the clustering of risk factors related to chronic diseases.19 Therefore, controlling the increase in WC in prediabetes patients may be helpful in preventing diabetes.
Insulin resistance and β-cell dysfunction are both important in the pathogenesis of diabetes mellitus. In this study, the baseline HOMA-IR was 2.29 (1.62–3.23) in participants with AGM and 1.87 (1.45–2.68) in participants with NGT. The baseline HOMA-β was 66.32 (46.59–90.37) in the AGM group and 66.00 (46.82–91.44) in the NGT group. Although no significant difference was found in HOMA-IR or HOMA-β between the AGM group and the NGT group, an increasing trend in HOMA-IR was observed in the AGM group. According to data from the China Cardiometabolic Disease and Cancer Cohort Study Group, approximately 24.4% (95% CI, 23.6–25.2) of incident diabetes cases could be attributed to insulin resistance, and 12.4% (95% CI, 11.2–13.7) could be attributed to β-cell dysfunction.20 Insulin resistance showed a stronger association with incident diabetes than β-cell dysfunction showed; thus, it is important to improve insulin resistance in order to reduce progression from prediabetes to diabetes.
FBG and 2hBG were also important risk factors for developing diabetes.21 Prediabetic participants with both IFG and IGT were more likely to develop diabetes than those with isolated IFG or isolated IGT.5,22 Consistent with previous studies, the current study showed that baseline levels of FBG and 2hBG were higher in participants with AGM than in those with NGT. The baseline levels of FBG [OR 0.336, 95% CI (0.196–0.576)] and 2hBG [OR 0.697, 95% CI (0.581–0.837)] were significant independent predictors of reversion from prediabetes to NGT.
FABP4 plays an important role in regulating energy metabolism.9 The mechanism by which this protein regulates glucose homeostasis is not yet fully understood. The involvement of FABP4 in the pathogenesis of insulin resistance might be mediated by the inhibition of PPARγ.23 FABP4-deficient mice had better glucose tolerance and were more insulin sensitive than wild-type mice.24,25 In humans, increased FABP4 levels are reportedly associated with many diseases, such as insulin resistance, T2DM, fatty liver disease and atherosclerosis.11,14,26–28 FABP4 has also been reported to be correlated with an adverse profile of diabetes risk factors.29 Increased serum FABP4 levels were found to be closely associated with insulin resistance and elevated fasting and post-challenge glucagon levels in T2DM.30 In this study, we also found that the baseline level of FABP4 was higher in participants with AGM than in those with NGT, and the baseline level of FABP4 was positively correlated with age, BMI, WC, 2hBG, TG, TC and LDL at the 2-year follow-up. Furthermore, we found that high baseline FABP4 [OR 0.960, 95% CI (0.928–0.993)] was not conducive to reversion from prediabetes to NGT.
ROC curve analysis was used to compare the accuracy of FABP4, FBG, 2hPG and their combinations as predictors of reversion from prediabetes to NGT. The AUC for FABP4 was 0.605 (95% CI: 0.546–0.665), similar to those of FBG and 2hBG. Nevertheless, the AUC was 0.716 (95% CI: 0.663–0.769) when FABP4 was combined with FBG and 2hBG. Due to the implications of FABP4 in various diseases, FABP4 has become a promising target for the treatment of metabolic dysfunction.31,32 Our results suggested that FABP4 inhibitors, if developed in the future, might be able not only to treat diabetes but also to prevent it.
Our study has several limitations. First, we combined participants with prediabetes and those with diabetes into the AGM group because of the small sample size. Second, the 2-year follow-up period was not sufficiently long. Third, the effects of lifestyle differences were not evaluated in this study.
In conclusion, our study showed a high baseline level of FABP4 in participants with AGM after 2 years of follow-up. The high baseline level of FABP4 was positively correlated with an adverse profile of diabetes risk factors and was negatively correlated with reversion from prediabetes to NGT. Moreover, the combination of FABP4, FBG and 2hBG was the best predictor of reversion from prediabetes to NGT. Therefore, it may be possible to prevent diabetes by decreasing FABP4 levels.
Acknowledgments
The authors acknowledge the contributions of all the participants.
Funding
The study was supported by the NSFC (81870596, 81870594); a Clinical Research Plan of the SHDC [No. SHDC2020CR1016B]; the Shanghai Jiao Tong University Research Funding for Medical and Engineering Interdisciplinary Projects (YG2019GD05); a Multicenter Clinical Research Project of Shanghai Jiao Tong University School of Medicine (DLY201824); a third-round cooperation project of the Songjiang District Municipal Health Commission (0702N18003); a Shanghai General Hospital Clinical Research Innovation Team Project (CTCCR-2018A02); and a new round of the Medical Key Discipline Construction Program in Songjiang District (ZK2019B02).
Disclosure
The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
1. Li Y, Teng D, Shi X, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ. 2020;369:m997. doi:10.1136/bmj.m997
2. Tabák AG, Herder C, Rathmann W, Brunner EJ, Kivimäki M. Prediabetes: a high-risk state for diabetes development. Lancet. 2012;379(9833):2279–2290. doi:10.1016/S0140-6736(12)60283-9
3. Gerstein HC, Santaguida P, Raina P, et al. Annual incidence and relative risk of diabetes in people with various categories of dysglycemia: a systematic overview and meta-analysis of prospective studies. Diabetes Res Clin Pract. 2007;78(3):305–312. doi:10.1016/j.diabres.2007.05.004
4. Hostalek U. Global epidemiology of prediabetes - present and future perspectives. Clin Diabetes Endocrinol. 2019;5(1):5. doi:10.1186/s40842-019-0080-0
5. Li N, Lu C, Ma Y, et al. Factors associated with progression of different prediabetic status to Diabetes: a Community-based cohort study. Diabetes Res Clin Pract. 2022;184:109193. doi:10.1016/j.diabres.2022.109193
6. Diabetes Prevention Program Research Group. Long-term effects of lifestyle intervention or metformin on diabetes development and microvascular complications over 15-year follow-up: the Diabetes Prevention Program Outcomes Study. Lancet Diabetes Endocrinol. 2015;3(11):866–875. doi:10.1016/S2213-8587(15)00291-0
7. Gong Q, Gregg EW, Wang J, et al. Long-term effects of a randomised trial of a 6-year lifestyle intervention in impaired glucose tolerance on diabetes-related microvascular complications: the China Da Qing Diabetes Prevention Outcome Study. Diabetologia. 2011;54(2):300–307. doi:10.1007/s00125-010-1948-9
8. Haunerland NH, Spener F. Fatty acid-binding proteins–insights from genetic manipulations. Prog Lipid Res. 2004;43(4):328–349. doi:10.1016/j.plipres.2004.05.001
9. Li B, Hao J, Zeng J, Sauter ER. SnapShot: FABP Functions. Cell. 2020;182(4):1066–1066. doi:10.1016/j.cell.2020.07.027
10. Jin J, Hao J, Yi Y, Sauter E, Li B. Regulation of macrophage functions by FABP-mediated inflammatory and metabolic pathways. Biochim Biophys Acta Mol Cell Biol Lipids. 2021;1866(8):158964. doi:10.1016/j.bbalip.2021.158964
11. Tso AW, Xu A, Sham PC, et al. Serum adipocyte fatty acid binding protein as a new biomarker predicting the development of type 2 diabetes: a 10-year prospective study in a Chinese cohort. Diabetes Care. 2007;30(10):2667–2672. doi:10.2337/dc07-0413
12. Ning H, Tao H, Weng Z, Zhao X. Plasma fatty acid-binding protein 4 (FABP4) as a novel biomarker to predict gestational diabetes mellitus. Acta Diabetol. 2018;55(10):1089. doi:10.1007/s00592-016-0867-8
13. Tanaka M, Takahashi S, Higashiura Y, et al. Circulating level of fatty acid-binding protein 4 is an independent predictor of metabolic dysfunction-associated fatty liver disease in middle-aged and elderly individuals. J Diabetes Investig. 2021;2021. doi:10.1111/jdi.13735
14. Xu A, Tso AW, Cheung BM, et al. Circulating adipocyte-fatty acid binding protein levels predict the development of the metabolic syndrome: a 5-year prospective study. Circulation. 2007;115(12):1537–1543. doi:10.1161/CIRCULATIONAHA.106.647503
15. Nakamura R, Okura T, Fujioka Y, et al. Serum fatty acid-binding protein 4 (FABP4) concentration is associated with insulin resistance in peripheral tissues, A clinical study. PLoS One. 2017;12(6):e0179737. doi:10.1371/journal.pone.0179737
16. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28(7):412–419. doi:10.1007/BF00280883
17. Colman PG, Thomas DW, Zimmet PZ, Welborn TA, Garcia-Webb P, Moore MP. New classification and criteria for diagnosis of diabetes mellitus. The Australasian working party on diagnostic criteria for diabetes mellitus. N Z Med J. 1999;112(1086):139–141.
18. Alberti KG, Zimmet P, Shaw J; IDF Epidemiology Task Force Consensus Group. The metabolic syndrome–a new worldwide definition. Lancet. 2005;366(9491):1059–1062. doi:10.1016/S0140-6736(05)67402-8
19. Zhou BF; Cooperative Meta-Analysis Group of the Working Group on Obesity in China. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults–study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomed Environ Sci. 2002;15(1):83–96.
20. Wang T, Lu J, Shi L, et al. Association of insulin resistance and β-cell dysfunction with incident diabetes among adults in China: a nationwide, population-based, prospective cohort study. Lancet Diabetes Endocrinol. 2020;8(2):115–124. doi:10.1016/S2213-8587(19)30425-5
21. de Vegt F, Dekker JM, Jager A, et al. Relation of impaired fasting and postload glucose with incident type 2 diabetes in a Dutch population: the Hoorn Study. JAMA. 2001;285(16):2109–2113. doi:10.1001/jama.285.16.2109
22. Bozorgmanesh M, Hadaegh F, Azizi F. A simple clinical model predicted diabetes progression among prediabetic individuals. Diabetes Res Clin Pract. 2012;97(2):e34–e36. doi:10.1016/j.diabres.2012.04.018
23. Cabia B, Andrade S, Carreira MC, Casanueva FF, Crujeiras AB. A role for novel adipose tissue-secreted factors in obesity-related carcinogenesis. Obes Rev. 2016;17(4):361–376. doi:10.1111/obr.12377
24. Boord JB, Maeda K, Makowski L, et al. Combined adipocyte-macrophage fatty acid-binding protein deficiency improves metabolism, atherosclerosis, and survival in apolipoprotein E-deficient mice. Circulation. 2004;110(11):1492–1498. doi:10.1161/01.CIR.0000141735.13202.B6
25. Uysal KT, Scheja L, Wiesbrock SM, Bonner-Weir S, Hotamisligil GS. Improved glucose and lipid metabolism in genetically obese mice lacking aP2. Endocrinology. 2000;141(9):3388–3396. doi:10.1210/endo.141.9.7637
26. Xu A, Wang Y, Xu JY, et al. Adipocyte fatty acid-binding protein is a plasma biomarker closely associated with obesity and metabolic syndrome. Clin Chem. 2006;52(3):405–413. doi:10.1373/clinchem.2005.062463
27. Li S, Bi P, Zhao W, et al. Prognostic utility of fatty acid-binding protein 4 in patients with type 2 diabetes and acute ischemic stroke. Neurotox Res. 2018;33(2):309–315. doi:10.1007/s12640-017-9792-z
28. Trojnar M, Patro-Małysza J, Kimber-Trojnar Ż, Leszczyńska-Gorzelak B, Mosiewicz J. Associations between fatty acid-binding protein 4⁻a proinflammatory adipokine and insulin resistance, gestational and type 2 diabetes mellitus. Cells. 2019;8(3):227. doi:10.3390/cells8030227
29. Liu G, Ding M, Chiuve SE, et al. Plasma levels of fatty acid-binding protein 4, retinol-binding protein 4, high-molecular-weight adiponectin, and cardiovascular mortality among men with type 2 diabetes: a 22-year prospective study. Arterioscler Thromb Vasc Biol. 2016;36(11):2259–2267. doi:10.1161/ATVBAHA.116.308320
30. Wang H, Cao J, Su JB, et al. Serum fatty acid-binding protein 4 levels and responses of pancreatic islet β-cells and α-cells in patients with type 2 diabetes. Diabetol Metab Syndr. 2021;13(1):70. doi:10.1186/s13098-021-00690-z
31. Li HL, Wu X, Xu A, Rl Hoo. A-FABP in metabolic diseases and the therapeutic implications: an update. Int J Mol Sci. 2021;22(17):9386. doi:10.3390/ijms22179386
32. Burak MF, Inouye KE, White A, et al. Development of a therapeutic monoclonal antibody that targets secreted fatty acid-binding protein aP2 to treat type 2 diabetes. Sci Transl Med. 2015;7(319):319ra205. doi:10.1126/scitranslmed.aac6336
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.