Back to Journals » Clinical Interventions in Aging » Volume 16
High Sensory Responsiveness in Older Adults is Associated with Walking Outside but Not Inside: Proof of Concept Study
Authors Agmon M, Bar-Shalita T, Kizony R
Received 31 May 2021
Accepted for publication 12 August 2021
Published 14 September 2021 Volume 2021:16 Pages 1651—1657
DOI https://doi.org/10.2147/CIA.S322728
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Maayan Agmon,1 Tami Bar-Shalita,2 Rachel Kizony3,4
1The Cheryl Spencer Department of Nursing, Faculty of Social Welfare and Health Sciences, University of Haifa, Haifa, Israel; 2Department of Occupational Therapy, The Faculty of Medicine, Tel-Aviv University, Tel-Aviv, Israel; 3Department of Occupational Therapy, Faculty of Social Welfare & Health Sciences University of Haifa, Haifa, Israel; 4Department of Occupational Therapy, Sheba Medical Center, Tel Hashomer, Ramat Gan, Israel
Correspondence: Maayan Agmon
The Cheryl Spencer Department of Nursing, Faculty of Social Welfare and Health Sciences, University of Haifa, Haifa, Israel
Tel +972-48240364
Fax +972 4 8249753
Email [email protected]
Background and Purpose: Reduced mobility and a higher risk of falls among older adults are related to aging-associated sensory alteration. Sensory responsiveness (SR) has been found to be strongly correlated with postural control in studies on young adults in stimulating environments; however, SR has not been studied in the context of mobility among older adults, despite its potential to enhance fall risks. The aim of the current study is to characterize the associations between SR and gait under single and dual-task (ST, DT) conditions inside and outside the laboratory.
Methods: Twenty-six community-dwelling older adults (age 70.3 ± 4.6 years, 65.4% women) participated in this cross-sectional study. Gait variables were measured using the APDM system under single and dual task conditions, in a quiet corridor inside and in an ecological (outside) environment. SR was evaluated using the SR questionnaire and cognition was assessed with the Trail-Making Test and the Montreal Cognitive Assessment.
Results: SR was negatively associated with gait speed during ST (rs = − 0.491, p < 0.05) and DT (rs = − 0.528, p < 0.01) outside and with ST gait speed inside (rs = − 0.528, p < 0.01). SR was positively associated with gait variability under DT (rs = 0.41, p < 0.05) and with DT cost (rs = 0.44, p < 0.05) only outside.
Conclusion: SR may play an important role in understanding mobility deterioration throughout the aging process, especially outside, illuminating the importance of SR evaluation among older adults during mobility assessment. Therefore, accounting for SR in gait research may contribute to a better understanding of mobility decline throughout the aging process.
Keywords: sensory responsiveness, gait, dual-task, falls, mobility, sensory processing
Introduction
Mobility is considered a marker for successful aging1 and is the sixth vital sign in geroscience.2 Thirty-five percent of adults aged 70 and above suffer from gait abnormalities3 that lead to higher fall incidence4 and 30–40% of older adults experience at least one fall each year, with half experiencing recurrent falls.5–7 Therefore, one of today’s major public health challenges is to identify risk factors for gait deterioration in the older population3,8 in order to minimize its burden and adverse consequences and to enable early prevention.9
Gait, a central aspect of mobility, relies on a delicate equilibrium between executive and automatic control.10 This equilibrium can be observed using the dual-task (DT) paradigm,11 in which performance of a task alone (termed single task, ST; eg, walking) is compared to performance of the same task while concurrently performing another task (termed dual task, DT; eg, walking while solving a math problem). The difference between ST and DT performance, termed dual task cost (DTC), can illustrate how attention is divided between the tasks and the amount of cognitive resources devoted to and required for task execution. The aging process negatively affects DT gait performance due to reduction in attention, motor, executive functions, and sensory processing.10 In recent years, deterioration in DT gait has come to be considered an early and sensitive marker for many age-associated conditions, including Parkinson’s disease, Alzheimer’s disease,12 cognitive decline,13 and falls.14 Moreover, DT performance can differentiate between older adults with and without fear of falling that is associated with functional decline.15
Effective and safe gait performance is required for correct integration and processing of sensory information in order to adjust one’s motor and attentional responses to constantly changing sensory input and to filter out irrelevant stimuli. This ability is termed sensory responsiveness (SR),16,17 and includes regulating the degree, type, and/or intensity of sensory stimulation across one or several sensory systems essential for both performing everyday activities18–21 and maintaining quality of life.22,23 SR can affect gait via direct and indirect pathways: directly through its guidance and feedback for gait execution24,25 and indirectly through its effects on cognition, especially executive function and attentional control.26–28 Attentional abilities, integrated with sensory input from various systems,29,30 are necessary to adequately adapt postural control to constantly changing environmental and task demands, particularly in DT situations.26
SR varies among individuals;31 adults with high sensory responsiveness (HSR) indicate that coping with daily activities may be overwhelming and distracting, leading to low social participation,16,22 and quality of life among various populations e.g.32. and affective disorders.33 Moreover, as HSR may elicit performance difficulties in new and/or overstimulating environments and transitions (eg, between situations or environments),20,34 it can pose a challenge even for walking in everyday situations. The aging process affects all sensory systems (eg, vision, hearing, proprioception, vestibular) and even more dramatically alters integration among systems.35,36 People with HSR may be more severely affected by the aging associated sensory decline than those with normal sensory responsiveness; these differences may manifest especially in situations requiring multitasking, such as walking in a busy mall, running errands, or crossing a street with obstacles while talking on the phone.10,37 During these “real life” situations, adequate multi-sensory integration and processing are critical and the effect of HSR is more expressed,20 similar to the effect of dual-task, which is more pronounced in real-life situations.38 Despite the plethora of studies regarding relationships between sensory processing and motor performance in childhood,39 and the link between sensory and motor systems in the aging process (highly expressed during daily functioning40), the impact of SR on gait among older adults, especially in stimulating real-life situations, has yet to be studied.
Thus, the aim of the current study is to characterize the associations between SR and gait, under conditions of ST and DT with a cognitive task, inside (in a quiet corridor) and outside, among community-dwelling older adults. We hypothesize that the link between SR and gait will be stronger during DT than during ST conditions, and will be more pronounced outside than in a quiet corridor inside.
Methods
Study Sample
Sample size was calculated with G*Power for one tailed moderate (0.5) correlation, power of 0.80 and alpha level of 0.05 for a total sample size of 23. A convenience sample of 26 community-dwelling older adults (65.4% women) participated in this cross-sectional proof of concept study. They were recruited via advertisements in their communities. Inclusion criteria were (1) age 60 or older; (2) ability to walk independently; (3) ability to speak, understand, and read the local language [MASK]; and (4) independence in basic and instrumental activities of daily living (eg, dressing, shopping). Exclusion criteria were (1) the presence of a neurologic diagnosis, such as a stroke, Parkinson’s disease, Alzheimer’s disease, or multiple sclerosis; (2) severe orthopedic restrictions such as acute back pain, recent fractures, or a total hip replacement; and (3) significant hearing or vision loss.
Measures
Gait Inside and Outside in Real-Life Conditions
The participants were asked to walk on a 10-meter path in a quiet corridor inside and on a flat path of the same length outside for one minute each. Walking tasks were administrated in a random order. The number of people in the vicinity of the outdoor path was documented to ensure similarity between conditions and among participants. Gait performance under the conditions of ST and DT (with the cognitive task, see below) was evaluated using the Mobility Lab system (APDM, http://www.apdm.com), which consists of three small wireless OPAL movement sensors affixed to the participant’s legs and waist. The APDM system has been shown to be sensitive and reliable.41 Gait parameters including gait speed, stride length, and stride time, were collected. DT costs (DTCs) for gait speed and the cognitive task were calculated using the common equation [(ST – DT)/ST*100]; higher scores represent a higher cost due to dual-tasking.42
Cognitive Task
Continuous subtraction by 3 from a random number between 100 and 250 for one minute was used to evaluate the effect of cognitive load on gait performance. This task requires internal mental processing and enabling standardization and comparison between studies.41 This task was administered as an ST (while sitting) and as a DT (with gait, see above) and the number of correct responses was recorded.
Sensory Responsiveness
The Sensory Responsiveness Questionnaire Intensity Scale (SRQ-IS)43 is a 58-item self-report questionnaire that assesses responses to daily sensations in order to evaluate sensory responsiveness in adults.43,44 For this study, we used the SRQ-Aversive sub-score, which is calculated as the mean of 32 items; higher scores indicate higher sensory responsiveness.43 The SRQ-IS presents daily scenarios, each involving one sensory stimulus in one modality, including auditory, visual, gustatory, olfactory, vestibular, and somatosensory stimuli (excluding pain) (eg, “It bothers me the way new clothes feel”). The participant rates the intensity of their response using a 5-point scale (1 = not at all; 5 = very much).
Additional Measures
Information about participants’ age, gender, education, chronic disease(s) (eg, diabetes and high blood pressure), weekly frequency of physical activity (eg walking, swimming), and inclusion/exclusion criteria was collected with a self-report questionnaire. Cognitive status was assessed using the Montreal Cognitive Assessment (MoCA),45 which screens for cognitive abilities in seven domains (eg, executive functions and memory), with scores ranging from 0 to 30. In addition, executive skills were evaluated with the Trail Making Test–B (TMT–B). The test measures complex visual scanning and cognitive flexibility.46
Procedure
Participants were asked to walk forward at a comfortable speed for one minute on a flat ten-meter stretch of (1) an otherwise-empty corridor inside, and (2) a paved flat outdoor path in a crowded area outside that had a relatively constant noise level and number of people around during the day, but without people crossing the specific path. In each setting, participants performed two walking tasks: one with (DT) and one without (ST) the cognitive subtraction task. The cognitive task was also performed while sitting as an ST. The order of the inside/outside and ST/DT trials was randomized. The personal data questionnaires and cognitive assessments were administered inside.
Data Analysis
Data were analyzed with IBM-SPSS version 25. Pearson correlations were performed with data that were normally distributed (SRQ-Aversive score, MoCA, gait speed, stride length, stride time, cognitive task responses) and Spearman’s rho was calculated for variables that were not normally distributed (variability of gait speed, stride length, and stride time; DTCs), according to the Shapiro–Wilk test. The alpha level was set at 0.05.
Results
Participants’ characteristics are presented in Table 1. Participants were mostly women, highly educated, with ages ranging between 62 and 81 years. Eleven (42.3%) participants were retired. Twenty-one (80.1%) at least twice a week reported doing physical activity at least three times per week. MOCA scores presented a large range with 57.69% in the range of mild cognitive impairment and 34.61% with intact cognition according to the 26-score cutoff. The SRQ scores indicated that most of the participants were within the normal range of SR with 7 (26.9%) participants presenting HSR.
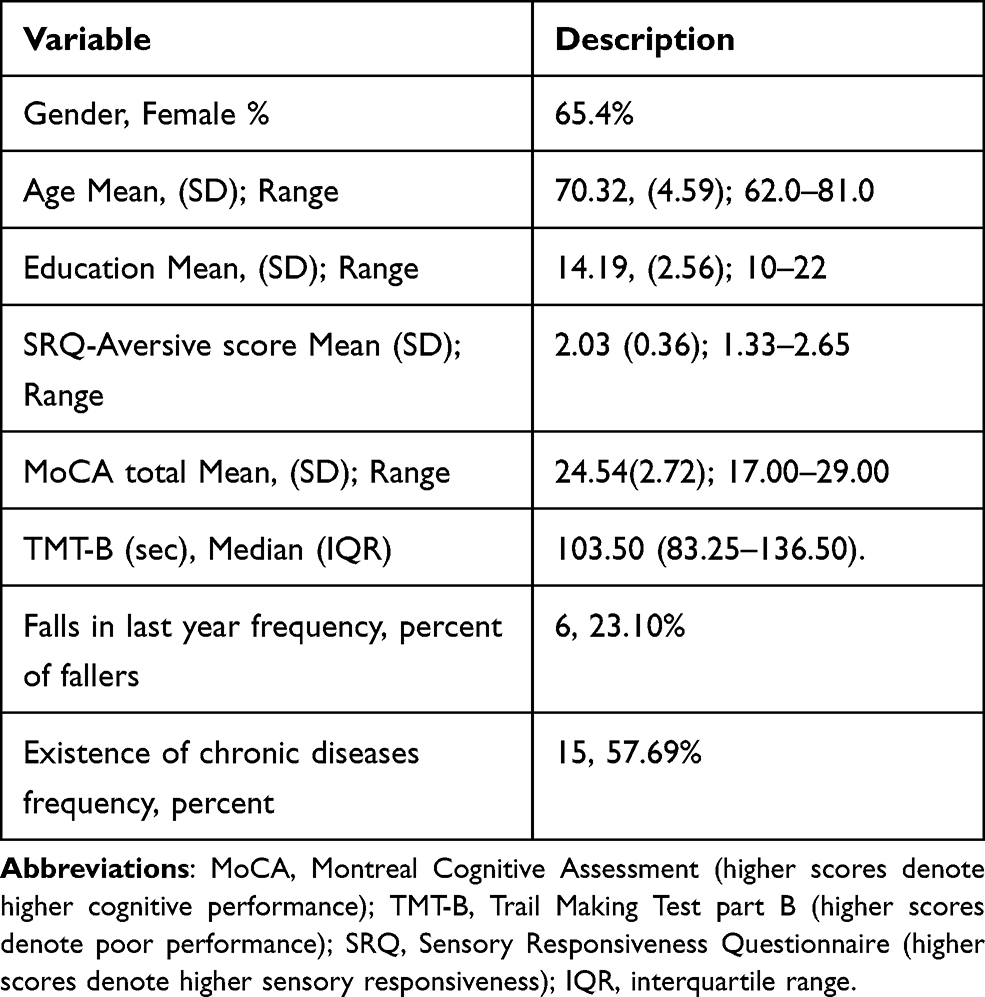 |
Table 1 Sample Characteristics (N=26) |
Descriptive statistics for gait and cognitive parameters during gait as well as ST, DT, DTCs inside and outside are presented in Table 2. Correlations are presented in Table 3, showing that the SRQ-Aversive sub-score was significantly correlated with gait parameters mainly outside indicating that higher SR is associated with low performance during ST or DT.
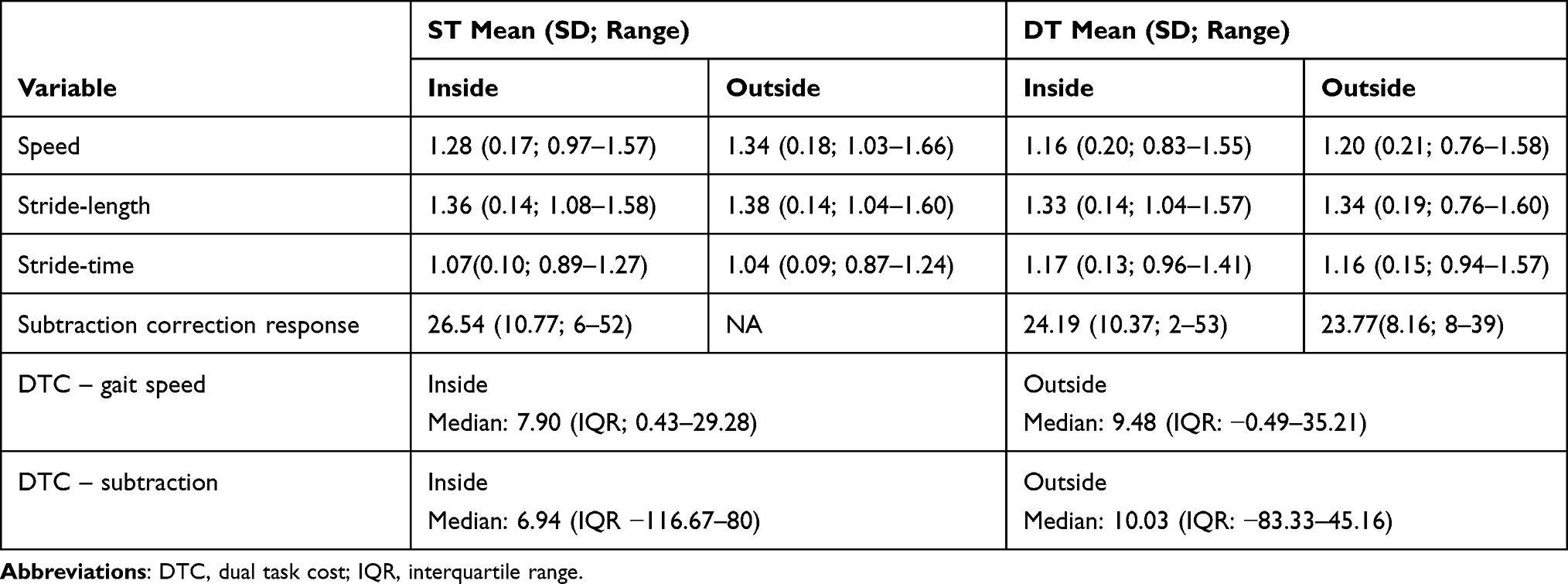 |
Table 2 Descriptive of Gait Associated Variables Under ST, DT Conditions Inside and Outside |
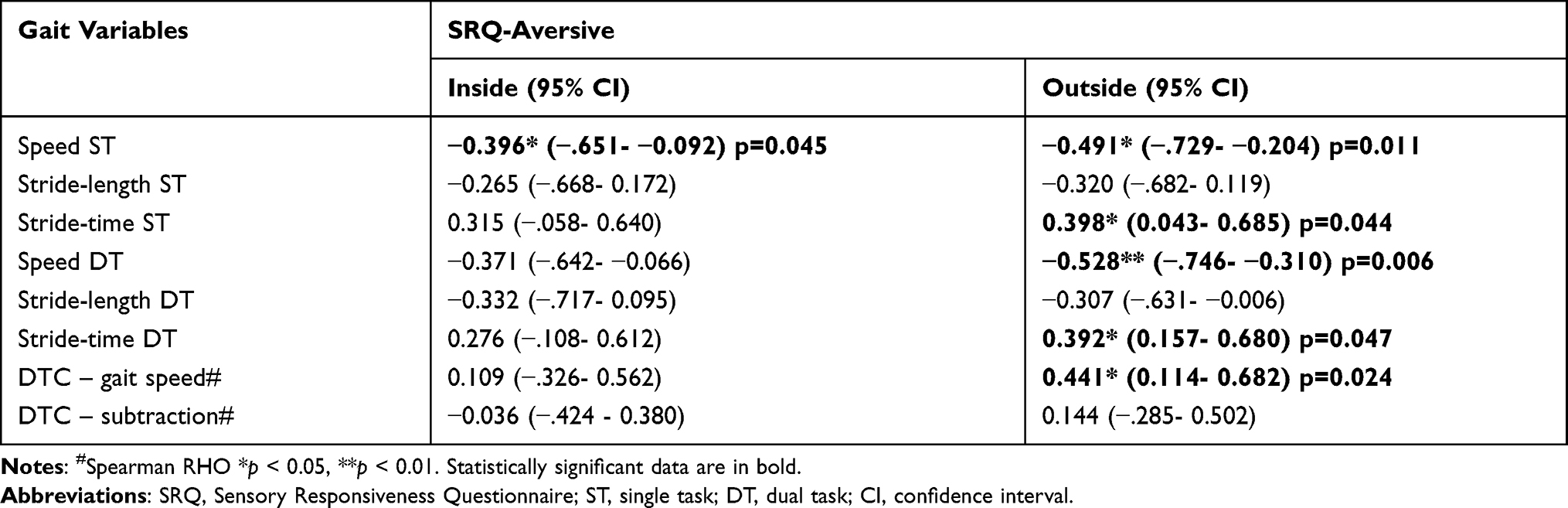 |
Table 3 Correlations Between Gait Variables, SRQ-Aversive Score Inside and Outside the Lab |
No significant correlations were found between the SRQ-Aversive sub-score and performance of the cognitive (subtraction) task inside or outside as a ST or a DT and DTC. No significant correlations were found between the MoCA, TMT-B and the gait parameters inside or outside or with the SRQ-Aversive sub-score.
Discussion
Our findings revealed that the association between SR and gait is more pronounced outside in a real-life condition than in a quiet corridor inside. Namely, outside, HSR was associated with worse gait performance, expressed as lower gait speed and longer stride time during both ST and DT and higher gait speed DTC. However, inside, SR was associated only with decreased ST gait speed. These findings are in line with previous studies demonstrating a greater effect of HSR in real-life conditions compared to a controlled laboratory setting.24,34 Our findings that HSR interferes with sensory motor tasks in older adults, resulting in worsened performance in complicated situations, contribute to the current understanding of both sensory integration and gait performance34,47 throughout the aging process.
Our findings also suggest that older adults with HSR do not have sufficient available cognitive resources to cope with the multisensory information26 that characterizes real environments, which adds cognitive load to the task of gait. Indeed, more cognitive resources are required to cope with sensory triggers evoked by environmental stimuli among adults with HSR.16 The constant need to control their high responsiveness may pose an additional attentional load, especially when the level of environmental stimuli increases; thus, high SR may be more pronounced in a real environment than in a laboratory setting as well as in a crowded environment than in a quiet one.
Surprisingly, in the current study, cognitive and executive functions were not related to DT performance. These findings are similar to those of Krasovsky et al,38 unlike previous studies that showed a positive association between DT gait performance and executive functions.48 This discrepancy can be explained by the characteristics of the current study sample, which included community-dwelling, high-functioning older adults. Indeed, older adults that are more physically fit, tend to suffer less from DT decrement compared with their less active counterparts.49 Nevertheless, the discrepancy between different studies demonstrates the importance of further exploration of factors associated with gait performance among older adults including HSR, revealed by our study, as a possible underlying factor that may explain mobility deterioration among older adults, which to date has been neglected in studies of older adults’ mobility. Thus, evaluating SR in older adults may improve early diagnosis and inform strategies to reduce mobility deterioration and prevent the vicious cycle of associated functional decline.
Limitations and Future Directions
Our sample is relatively small and included high-functioning older adults which limit our ability to generalize the findings to different sub-groups of older adults with various levels of function and disabilities. Moreover, other variables that may affect the association between SR and gait were not addressed, including medical conditions such as diabetes mellitus and impairment of uni-sensory functions such as tactile sensation. Similarly, we did not consider emotional factors such as depression, anxiety and fear of falling that may affect gait performance and may interact with sensory modulation. Future studies should recruit a larger heterogeneous sample across the aging spectrum, with various health conditions while accounting for emotional statues and apply neuroimaging techniques to further explore the underlying brain mechanisms and the relationship between SR and gait.
Conclusions
To the best of our knowledge, this is the first study to investigate the association between SR and gait performance inside (indoors) and outside in real-life conditions among community-dwelling older adults. We established a significant link between HSR and mobility in an ecological setting (ie, in a natural environment with concurrent cognitive demand) in community-dwelling older adults. The impact of SR is significantly enhanced in ecological conditions and when higher cognitive demands are required. These results stress the importance of considering SR characteristics across the lifespan and specifically during gait evaluation. Considering ones’ sensory profile can guide the implementation of an early and more effective tools within fall prevention interventions such as training outside the laboratory within crowded environments or using virtual reality during a training session to improve coping mechanisms with challenged environment. In this vein, it is particularly important to assess gait in natural settings that are part of older adults’ real-life conditions such as parks and malls. Our findings indicate the potential for developing personally tailored fall-prevention interventions that consider the individual’s SR profile in ecological environments, which could reduce the burden of falls in the aging population.
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki.
The study was approved by the Institutional Review Board of the University of Haifa, #685/14, and written informed consent was obtained from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors declare that they have no conflicts of interest.
References
1. Teater B, Chonody JM. How do older adults define successful aging? A scoping review. Int J Aging Human Develop. 2020;91(4):599–625.
2. Fritz S, Lusardi M. White paper:“walking speed: the sixth vital sign”. J Geriatric Phys Ther. 2009;32(2):2–5.
3. Verghese J, LeValley A, Hall CB, Katz MJ, Ambrose AF, Lipton RB. Epidemiology of gait disorders in community‐residing older adults. J Am Geriatr Soc. 2006;54(2):255–261.
4. Verghese J, Holtzer R, Oh-Park M, Derby CA, Lipton RB, Wang C. Inflammatory markers and gait speed decline in older adults. J Gerontol Ser A. 2011;66(10):1083–1089.
5. Stevens JA, Corso PS, Finkelstein EA, Miller TR. The costs of fatal and non-fatal falls among older adults. Injury Prev. 2006;12(5):290–295.
6. Davis JC, Robertson MC, Ashe MC, Liu-Ambrose T, Khan KM, Marra CA. International comparison of cost of falls in older adults living in the community: a systematic review. Osteoporosis Int. 2010;21(8):1295–1306.
7. Hausdorff JM, Rios DA, Edelberg HK. Gait variability and fall risk in community-living older adults: a 1-year prospective study. Arch Phys Med Rehabil. 2001;82(8):1050–1056.
8. Rantakokko M, Mänty M, Rantanen T. Mobility decline in old age. Exerc Sport Sci Rev. 2013;41(1):19–25.
9. Rosso AL, Studenski SA, Chen WG, et al. Aging, the central nervous system, and mobility. J Gerontol Ser A. 2013;68(11):1379–1386.
10. Clark DJ, Rose DK, Ring SA, Porges EC. Utilization of central nervous system resources for preparation and performance of complex walking tasks in older adults. Front Aging Neurosci. 2014;6:217.
11. Verhaeghen P, Steitz DW, Sliwinski MJ, Cerella J. Aging and dual-task performance: a meta-analysis. Psychol Aging. 2003;18(3):443.
12. Belghali M, Chastan N, Davenne D, Decker LM. Improving dual-task walking paradigms to detect prodromal Parkinson’s and Alzheimer’s diseases. Front Neurol. 2017;8:207.
13. Beauchet O, Launay CP, Sekhon H, et al. Association of increased gait variability while dual tasking and cognitive decline: results from a prospective longitudinal cohort pilot study. Geroscience. 2017;39(4):439–445.
14. Menant JC, Schoene D, Sarofim M, Lord SR. Single and dual task tests of gait speed are equivalent in the prediction of falls in older people: a systematic review and meta-analysis. Ageing Res Rev. 2014;16:83–104.
15. Brustio PR, Magistro D, Zecca M, Liubicich ME, Rabaglietti E. Fear of falling and activities of daily living function: mediation effect of dual-task ability. Aging Ment Health. 2018;22(6):856–861.
16. Kinnealey M, Oliver B, Wilbarger P. A phenomenological study of sensory defensiveness in adults. Am J Occup Ther. 1995;49(5):444–451.
17. Ahn RR, Miller LJ, Milberger S, McIntosh DN. Prevalence of parents’ perceptions of sensory processing disorders among kindergarten children. Am J Occup Ther. 2004;58(3):287–293.
18. Zero To Three. Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood: Revised Edition (DC: 0-3R). Zero to Three Press. Washington, DC; 2005.
19. Association AP, Organizations AoP. Psychodynamic Diagnostic Manual (PDM). Interdisciplinary Council On; 2006.
20. Miller LJ, Anzalone ME, Lane SJ, Cermak SA, Osten ET. Concept evolution in sensory integration: a proposed nosology for diagnosis. Am J Occup Ther. 2007;61(2):135–140.
21. Dunn W, Little L, Dean E, Robertson S, Evans B. The state of the science on sensory factors and their impact on daily life for children: a scoping review. OTJR. 2016;36(2_suppl):3S–26S.
22. Kinnealey M, Koenig KP, Smith S. Relationships between sensory modulation and social supports and health-related quality of life. Am J Occup Ther. 2011;65(3):320–327.
23. Bar-Shalita T, Deutsch L, Honigman L, Weissman-Fogel I. Ecological aspects of pain in sensory modulation disorder. Res Dev Disabil. 2015;45:157–167.
24. James K, Miller LJ, Schaaf R, Nielsen DM, Schoen SA. Phenotypes within sensory modulation dysfunction. Compr Psychiatry. 2011;52(6):715–724.
25. Pearson KG. Generating the walking gait: role of sensory feedback. In: Progress in Brain Research. Vol. 143. Elsevier; 2004:123–129. doi:10.1016/S0079-6123(03)43012-4
26. Shumway-Cook A, Woollacott M. Attentional demands and postural control: the effect of sensory context. J Gerontol Biol Sci Med Sci. 2000;55(1):M10.
27. Redfern MS, Chambers AJ, Jennings JR, Furman JM. Sensory and motoric influences on attention dynamics during standing balance recovery in young and older adults. Exp Brain Res. 2017;235(8):2523–2531.
28. Engel-Yeger B, Rosenblum S. Executive dysfunctions mediate between altered sensory processing and daily activity performance in older adults. BMC Geriatr. 2021;21(1):1–10.
29. Takakusaki K. Functional neuroanatomy for posture and gait control. J Movement Disord. 2017;10(1):1.
30. Koziol LF, Budding DE, Chidekel D. Sensory integration, sensory processing, and sensory modulation disorders: putative functional neuroanatomic underpinnings. Cerebellum. 2011;10(4):770–792.
31. Engel-Yeger B, Dunn W. The relationship between sensory processing difficulties and anxiety level of healthy adults. Br J Occup Ther. 2011;74(5):210–216.
32. Serafini G, Gonda X, Pompili M, Rihmer Z, Amore M, Engel-Yeger B. The relationship between sensory processing patterns, alexithymia, traumatic childhood experiences, and quality of life among patients with unipolar and bipolar disorders. Child Abuse Negl. 2016;62:39–50.
33. Engel-Yeger B, Muzio C, Rinosi G, et al. Extreme sensory processing patterns and their relation with clinical conditions among individuals with major affective disorders. Psychiatry Res. 2016;236:112–118.
34. Dunn W. The sensations of everyday life: empirical, theoretical, and pragmatic considerations. Am J Occup Ther. 2001;55(6):608–620.
35. Freiherr J, Lundström JN, Habel U, Reetz K. Multisensory integration mechanisms during aging. Front Hum Neurosci. 2013;7:863.
36. de Dieuleveult AL, Siemonsma PC, van Erp JB, Brouwer A-M. Effects of aging in multisensory integration: a systematic review. Front Aging Neurosci. 2017;9:80.
37. Woollacott M, Shumway-Cook A. Attention and the control of posture and gait: a review of an emerging area of research. Gait Posture. 2002;16(1):1–14.
38. Krasovsky T, Weiss PL, Kizony R. Older adults pay an additional cost when texting and walking: effects of age, environment, and use of mixed reality on dual-task performance. Phys Ther. 2018;98(7):549–559.
39. Niutanen U, Harra T, Lano A, Metsäranta M. Systematic review of sensory processing in preterm children reveals abnormal sensory modulation, somatosensory processing and sensory‐based motor processing. Acta Paediatrica. 2020;109(1):45–55.
40. Paraskevoudi N, Balcı F, Vatakis A. “Walking” through the sensory, cognitive, and temporal degradations of healthy aging. Ann N Y Acad Sci. 2018;1426(1):72–92.
41. Al-Yahya E, Dawes H, Smith L, Dennis A, Howells K, Cockburn J. Cognitive motor interference while walking: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2011;35(3):715–728.
42. McIsaac TL, Lamberg EM, Muratori LM. Building a framework for a dual task taxonomy. Biomed Res Int. 2015;2015:591475. doi:10.1155/2015/591475
43. Bar-Shalita T, Seltzer Z, Vatine -J-J, Yochman A, Parush S. Development and psychometric properties of the Sensory Responsiveness Questionnaire (SRQ). Disabil Rehabil. 2009;31(3):189–201.
44. Bar-Shalita T, Yarnitsky JJV, Parush S, Weissman-Fogel I. Atypical central pain processing in sensory modulation disorder: absence of temporal summation and higher after-sensation. Exp Brain Res. 2014;232(2):587–595.
45. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. Int J Geriatr Psychiatry. 2005;53(4):695–699.
46. Reitan RM. Relationships between measures of brain functions and general intelligence. J Clin Psychol. 1985;41(2):245–253.
47. Dunn W. Supporting children to participate successfully in everyday life by using sensory processing knowledge. Infants Young Child. 2007;20(2):84–101.
48. Rollman GB. The Need for Ecological Validity in Studies of Pain and Ethnicity. LWW; 2005.
49. Petrigna L, Pajaujiene S, Iacona GM, et al. The execution of the grooved pegboard test in a dual-task situation: a pilot study. Heliyon. 2020;6(8):e04678.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.