Back to Journals » Clinical Epidemiology » Volume 15
High Perceived Stress and Low Self-Efficacy are Associated with Functional Somatic Disorders: The DanFunD Study
Authors Petersen MW ![]() , Carstensen TBW
, Carstensen TBW ![]() , Frostholm L, Wellnitz KB
, Frostholm L, Wellnitz KB ![]() , Ørnbøl E, Jørgensen T
, Ørnbøl E, Jørgensen T ![]() , Eplov LF
, Eplov LF ![]() , Dantoft TM
, Dantoft TM ![]() , Fink P
, Fink P ![]()
Received 1 December 2022
Accepted for publication 16 March 2023
Published 27 March 2023 Volume 2023:15 Pages 407—419
DOI https://doi.org/10.2147/CLEP.S399914
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Irene Petersen
Marie Weinreich Petersen,1,2 Tina Birgitte Wisbech Carstensen,1,2 Lisbeth Frostholm,1,2 Kaare Bro Wellnitz,1,2 Eva Ørnbøl,1,2 Torben Jørgensen,3,4 Lene Falgaard Eplov,5 Thomas Meinertz Dantoft,3 Per Fink1,2
1Research Clinic for Functional Disorders and Psychosomatics, Aarhus University Hospital, Aarhus, Denmark; 2Department of Clinical Medicine, University of Aarhus, Aarhus, Denmark; 3Center for Clinical Research and Prevention, Bispebjerg/Frederiksberg Hospital, Frederiksberg, Capital Region, Denmark; 4Department of Public Health, Faculty of Medical Sciences, Copenhagen University, Copenhagen, Denmark; 5Copenhagen Research Center for Mental Health – CORE, Mental Health Centre Copenhagen, Copenhagen, Capital Region, Denmark
Correspondence: Marie Weinreich Petersen, Research Clinic for Functional Disorders and Psychosomatics, Aarhus University Hospital, Palle Juul-Jensens Boulevard 11, Aarhus, 8200, Denmark, Tel +45 7846 4310, Email [email protected]
Objective: Several psychological factors have been proposed to be associated with functional somatic disorders (FSD) including functional somatic syndromes, such as irritable bowel, chronic widespread pain, and chronic fatigue. However, large randomly selected population-based studies of this association are sparse. This study aimed to investigate the association between FSD and perceived stress and self-efficacy, respectively, and to investigate if FSD differed from severe physical diseases on these aspects.
Methods: This cross-sectional study included a random sample of the adult Danish population (n = 9656). FSD were established using self-reported questionnaires and diagnostic interviews. Perceived stress was measured with Cohen’s Perceived Stress Scale and self-efficacy with the General Self-Efficacy Scale. Data were analysed with generalized linear models and linear regression models.
Results: FSD were associated with higher perceived stress and lower self-efficacy, especially for the multi-organ and the general symptoms/fatigue FSD types and for chronic fatigue. However, controlling for the personality trait neuroticism altered the associations with self-efficacy so it became insignificant. The analysis did not support an important interaction between perceived stress and self-efficacy on the likelihood of having FSD. Individuals with FSD presented levels of perceived stress that were not equal, ie higher, to those in individuals with severe physical diseases.
Conclusion: FSD were positively associated with perceived stress and negatively associated with self-efficacy. Our study may point to stress being part of the symptomatology of FSD. This underlines the severity of having FSD and stresses the relevance of the resilience theory in the understanding of the condition.
Keywords: functional somatic disorders, functional somatic syndromes, perceived stress, self-efficacy, irritable bowel syndrome, fibromyalgia, chronic fatigue syndrome, population-based
Introduction
Functional somatic disorders (FSD) are common conditions characterized by patterns of persisting physical symptoms that cannot be better explained by other physical or mental conditions.1 FSD is a unifying diagnosis; in this paper operationalized as Bodily Distress Syndrome (BDS), which includes functional somatic syndromes (FSS) such as irritable bowel, chronic widespread pain, and chronic fatigue.2 Patients with severe cases of FSD are severely impaired and emotionally distressed and have an excessive use of healthcare services in terms of repeated hospitalizations, medical investigations, and fruitless treatment attempts.1,3,4 The etiology of FSD is considered multifactorial5–9 and in a previous study, we have shown that higher scores on neuroticism and experiencing a higher number of adverse life events were strongly associated with FSD.10 Furthermore, high levels of stress and low self-efficacy have been suggested to be associated with FSD.1,11
According to the transactional model of stress and coping by Lazarus and Folkman,12 perceived stress is
a particular relationship between the person and the environment that is appraised by the person as taxing or exceeding his or her resources and endangering his or her well-being.
Hence, stress is both dependent on the cognitive evaluation (ie, appraisal) on whether given situations may be harmful, and also the subjective assessment of the resources and abilities of the individual to control this situation (ie, coping/self-efficacy).
The relationship between levels of stress and the importance of self-efficacy for disease outcome, distress, and quality of life has been established for a range of somatic diagnoses including cardiovascular disease,13,14 stroke,15 HIV/AIDS,14 cancer,14,16 and rheumatic disease.17 In addition, high levels of stress have been proposed to predispose FSD18,19 and multiple somatic symptoms,20 and in clinical studies, low self-efficacy has been proposed to be associated with fibromyalgia,21 whiplash-associated disorders,22 and chronic fatigue syndrome.23 The relationship between stress, self-efficacy and disease may be biologically explained by the shifts between homeostasis and allostasis: Over a life course, events are constantly perceived and determined in the brain as threatening together with an individual’s behavioral and psychological responses which optimally creates adaptive and survival promoting processes (allostasis). These processes are mediated by hormones, such as cortisol and adrenalin, but they also include components such as the autonomic nervous system and pro- and anti-inflammatory cytokines. However, when dysregulated, these mediators can lead to allostatic load, which may give rise to pathology.24
As health care professionals often have limited knowledge of FSD,1 patients are often misdiagnosed and may be met with mistrust and doubt by health care professionals, the social welfare system, and friends and relatives.25,26 This may cause more insecurity, possibly leading to reduced self-efficacy in patients with FSD compared with patients diagnosed with conventionally defined physical diseases.
So far, most studies into stress and self-efficacy have been carried out in selected patient samples, and general population-based studies including a large randomly obtained sample investigating the stress/resource balance in FSD are lacking.
The present study included a large random sample from the adult Danish population and aimed to investigate the association between FSD and perceived stress and self-efficacy, respectively, and to compare the level of perceived stress and self-efficacy between individuals with FSD, healthy individuals, and individuals with a severe physical disease.
We hypothesized that 1) FSD are associated with higher levels of perceived stress and lower levels of self-efficacy, respectively; 2) the level of perceived stress is higher in individuals with FSD than in healthy individuals but equivalent to individuals with a severe physical disease as well as individuals with a severe physical disease and FSD; and 3) the level of self-efficacy is lower in individuals with FSD than in healthy individuals and individuals with a severe physical disease but equivalent to the level in individuals with a severe physical disease and FSD.
Methods
Study Population
The present study included data from the Danish Study of Functional Disorders (DanFunD) baseline cohort, gathered between years 2011 and 2015.27 Participants were randomly drawn from the Danish Civil Registration system.28 The exclusion criteria were: not born in Denmark, not being a Danish citizen, and pregnancy.
The DanFunD baseline cohort comprises a total of 9656 (33.7% of the invited participants) men and women aged 18–76 years born in Denmark and living in the Western part of greater Copenhagen. All participants completed questionnaires about physical symptoms and psychological factors, among others. A stratified subsample (n = 2450) including every tenth participant and all participants with high symptom scores on the DanFunD baseline symptom questionnaires were invited to participate in a diagnostic interview (the Research Interview for Functional somatic Disorders (RIFD)), performed by trained family physicians;29 1590 (64.9%) participants accepted and participated in the interview.
The study complies with the Declaration of Helsinki. It was approved by the Ethical Committee of the Capital Region (H-3-2011-081, H-3-2012-015), and all participants gave written informed consent prior to study commencement.
Functional Somatic Disorders
For the primary operationalization of FSD, the unifying diagnostic construct of Bodily Distress Syndrome was used.1,30,31 It presents with four symptom clusters: a cardiopulmonary cluster, a gastrointestinal cluster, a musculoskeletal cluster, and a general symptoms/fatigue cluster. The patients are subdivided into two subgroups: a single-organ subgroup (ie, patients with symptoms from one or two of the symptom clusters), and a multi-organ subgroup (ie, patients with symptoms from at least three of the symptom clusters).31 The diagnostic construct has been validated and confirmed in several clinical and population-based studies and has been shown to encompass a range of functional somatic syndromes, such as irritable bowel, chronic widespread pain, and chronic fatigue.32–35
In this paper, we present data using both the FSD diagnosis and three commonly used FSS diagnoses: irritable bowel,36 chronic widespread pain,37 and chronic fatigue.38 Due to overlap between these three syndromes,2 the “pure” types of each syndrome, ie, individuals with only one of the three syndromes were included in an additional analysis.
Assessment of Functional Somatic Disorders
Cases with FSD were identified by the self-reported Bodily Distress Syndrome Checklist,31 including bothersome symptoms within the last 12 months. Additionally, a stratified subsample of participants with a clinical diagnosis of FSD was identified with the Research Interview for functional somatic disorders (RIFD), developed to be used as a second phase tool after a respondent’s self-report in symptom questionnaires.29 The RIFD interviews were performed by three trained primary care physicians over the telephone. The physicians assessed whether a specific symptom pattern was due to an FSD rather than another physical or mental condition. The RIFD interview has shown good criterion validity for identifying individuals with FSD.29
Cases with irritable bowel,36 chronic widespread pain,37 and chronic fatigue38 were identified with self-reported validated symptom questionnaires including bothersome symptoms within the last 12 months. Cases with “pure” types of each syndrome were identified with the same self-reported symptom questionnaires and defined as individuals who only fulfilled one of the three syndrome criteria.
Primary Measures
Perceived Stress
Perceived stress was measured with the Cohen’s Perceived Stress Scale that assesses the extent to which an individual finds his/her life to be unpredictable, uncontrollable, and overloaded.39,40 The scale consists of 10 items each rated on a five-point rating scale from “never” to “very often”. An example of an item could be: “How often have you found that you could not cope with all the things that you had to do?”. The sum score ranges from 0 to 40, where a higher score indicates a higher level of perceived stress.
Self-Efficacy
Self-efficacy was measured with the General Self-Efficacy Scale (GSE),41 a questionnaire assessing people’s beliefs in their capabilities to perform a specific action required to attain a desired outcome. A typical item in the scale is “Thanks to my resourcefulness, I can handle unforeseen situations”. The scale consists of 10 items rated on a four-point rating scale from “not at all true” to “exactly true”. A sum score is calculated, and higher scores indicate higher degree of self-efficacy. In the present study, the sum score ranged from 0 to 30.
Severe Physical Disease
Individuals with a severe physical disease was identified with a predefined 22-item list that covered lifetime diagnoses of physical diseases (“Has a doctor ever told you that you have/had…”) etc. Within this list, five severe diagnoses (cancer, myocardial infarction, other heart disease, obstructive pulmonary disease, and stroke) were operationalized as severe physical diseases.
Secondary Measures
Social Status
Subjective social status was measured with one item asking the participants to rate their own social status on a scale from 1 to 10; with 1 being the lowest and 10 being the highest status in society.42
Neuroticism
Neuroticism was measured with the Danish version of the short-form NEO Personality Inventory (NEO-PI-Rsf),43,44 an instrument used to measure the five personality domains: neuroticism, extraversion, openness, agreeableness, and conscientiousness. The NEO-PI-Rsf includes 60 self-descriptive statements, such as “I often feel tense and jittery”. Each statement is rated with a five-point rating scale from “strongly disagree” to “strongly agree”. For the domain neuroticism, a sum score of 12 items, ranging from 12 to 60, is calculated, and higher scores indicate higher neuroticism.
Accumulated Number of Adverse Life Events
The accumulated number of adverse life events was measured with the Danish version of the Cumulative Lifetime Adversity Measure (CLAM).45 The CLAM is used to examine exposure to lifetime adversity by asking the respondents whether they have experienced 37 different adverse life events including the possibility to add an additional unnamed life event. An example of an item could be “Have you suffered from a serious illness”, which is answered “yes” or “no”. For a positive answer to an event, a sum score is calculated by adding age time points and age ranges by simply counting age time points and age ranges (ie, an age range counted for one event and an age time point counted for one event. The sum score ranges from 0 to 130, with a higher score indicating a higher number of adversities.
Statistical Analyses
All analyses were performed in Stata 17.0 for Windows (StataCorp LLC, College Station, USA).46 Descriptive statistics were presented as medians and interquartile ranges (IQRs) due to non-normal distribution of the continuous variables. Categorical variables were presented as frequencies with percentages.
For the testing of hypothesis 1, a number of generalized linear models were conducted including FSD as a dichotomous dependent variable (yes/no) and perceived stress and self-efficacy, respectively, as the primary independent continuous variable. Preferably, generalized linear models with binomial family and log link were conducted but in case of convergence problems, generalized linear models with family Poisson and log link with robust error were performed.47 Potential confounders included in the analyses were identified using directed acyclic graphs (DAGs) constructed in the browser-based program DAGitty Version 3.0.48 For hypothesis 1, four models were built, each adjusting for a varying number of prioritized confounders in order to be able to explore the impact of each possible confounder: Model 1 was adjusted for sex, age, and social status; model 2 was adjusted for sex, age, social status, and neuroticism; model 3 was adjusted for sex, age, social status, neuroticism, and accumulated number of adverse life events; and model 4 was adjusted for sex, age, social status, neuroticism, accumulated number of adverse life events, and self-efficacy or perceived stress. Linearity of each independent variable was checked by expanding the model with natural cubic splines. Associations were reported as prevalence ratios (PR) with 95% confidence intervals (CI).49 In an exploratory analysis, a moderation analysis including an interaction term between perceived stress and self-efficacy to the generalized linear models number 1 was performed.
For the testing of hypotheses 2 and 3, two linear regression analyses were performed. Perceived stress and self-efficacy constituted the continuous dependent variables, and case status constituted the four-level categorical independent variable: The first category (reference) constituted individuals with FSD but no comorbid severe physical disease (FSD only); the second category constituted individuals without FSD or any severe physical disease (healthy); the third category constituted individuals with a severe physical disease but no FSD (PhyDis); the fourth category constituted individuals having both FSD and a comorbid severe physical disease (FSD + PhyDis).
In the analyses of equivalence, equivalence in perceived stress was defined as a difference smaller than ± 5 on Cohen's Perceived Stress Scale and equivalence in self-efficacy was defined as a difference smaller than ± 2 on the General Self-Efficacy Scale. These cut-offs were pragmatically based on the sparse available literature40 and the theory of equivalence testing.50 The conclusions on difference and equivalence were based on 90% CI.51,52
Results
Characteristics of Study Participants
The median age of the 9656 participants that completed the self-reported symptom questionnaires was 54 years (IQR = 44–64) and 5203 (53.9%) were women. The median score on perceived stress was 10.0 (IQR = 6–14) and the median score on self-efficacy was 21 (IQR = 18–25).
The median age of the stratified subsample of 1590 participants who participated in the diagnostic research interview was 54 years (IQR = 44–63) and 942 (59.3%) were women. The median score on perceived stress was 12 (IQR = 7–17) and the median score on self-efficacy was 21 (IQR = 17–25). More characteristics of the study participants are displayed in Table 1.
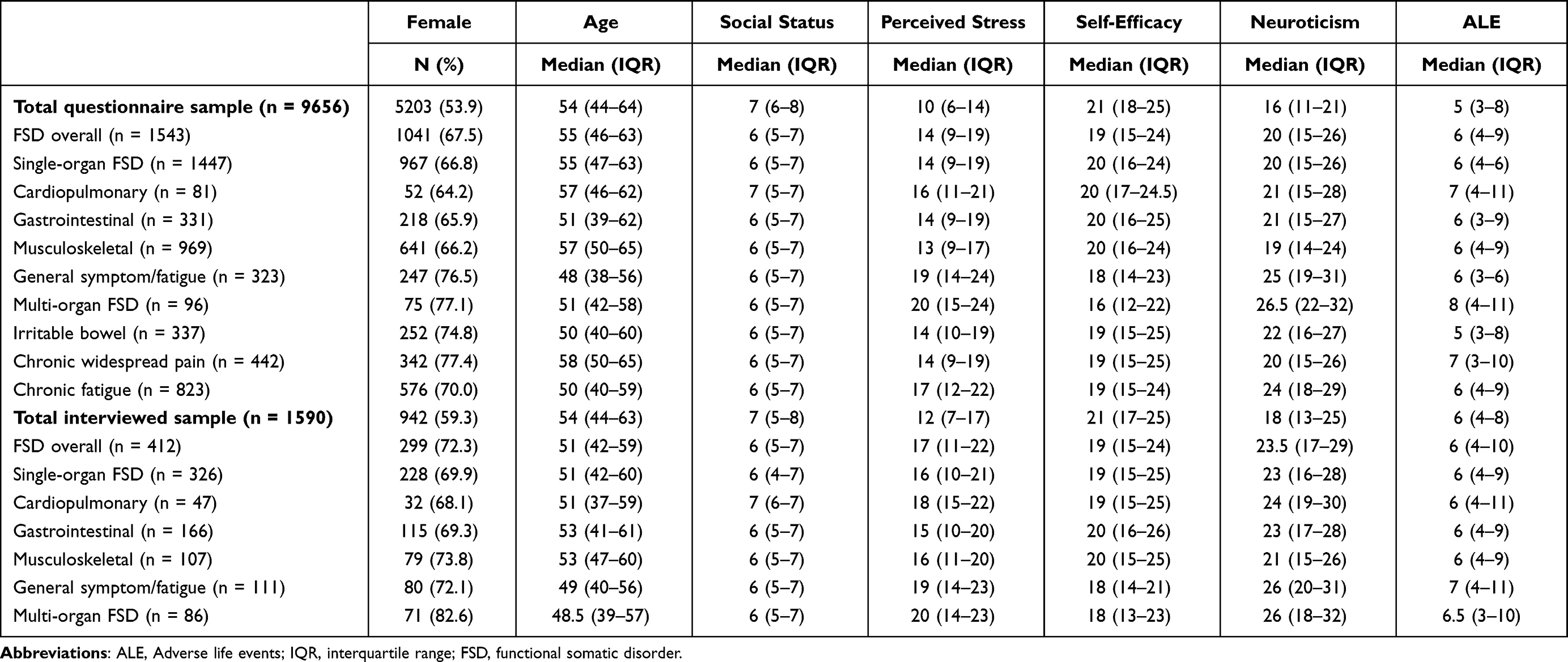 |
Table 1 Characteristics of the Study Participants |
Perceived Stress and Functional Somatic Disorders
Positive associations were found between perceived stress and FSD: a higher level of perceived stress was associated with higher likelihood of FSD (Table 2 and Table 3). Eg when comparing two participants who differed with only one point on the Cohen’s Perceived Stress Scale, ranging from 0 to 40, the participant with the highest score was 9% (95% CI: 8–9%) more likely to have overall FSD, 20% (95% CI: 16–24%) more likely to have questionnaire-defined FSD multi-organ type, and 13% (95% CI: 12–14%) more likely to have questionnaire-defined chronic fatigue (Table 2). Associations remained throughout models 1–4, but they were reduced in model 2 with additional adjustment for neuroticism. Further adjustment for adverse life events and self-efficacy in model 3 and 4, respectively, did not change the size of association compared to model 2 (Table A1).
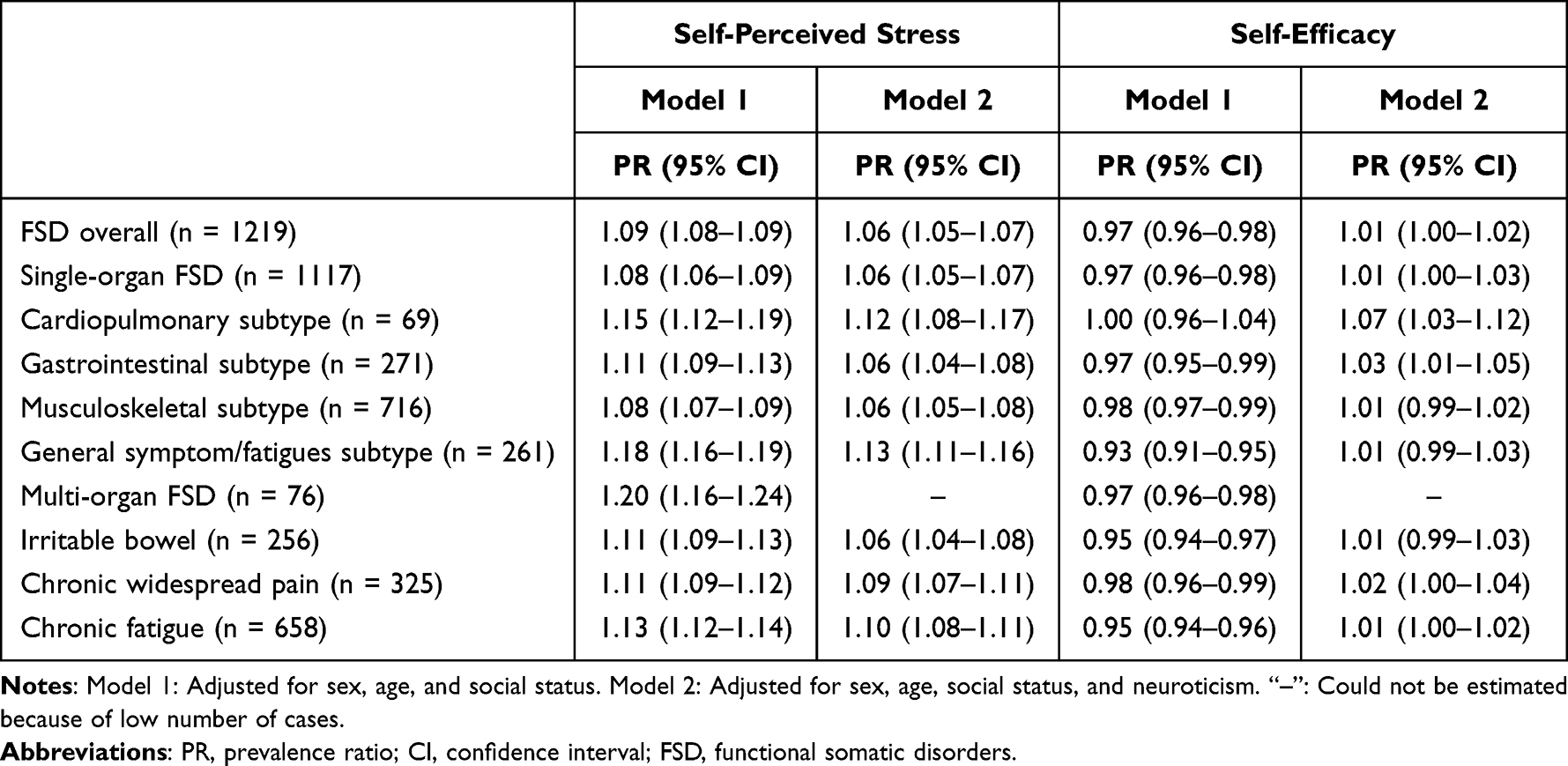 |
Table 2 Association Between Questionnaire-Defined Functional Somatic Disorders and Functional Somatic Syndromes, Perceived Stress and Self-Efficacy |
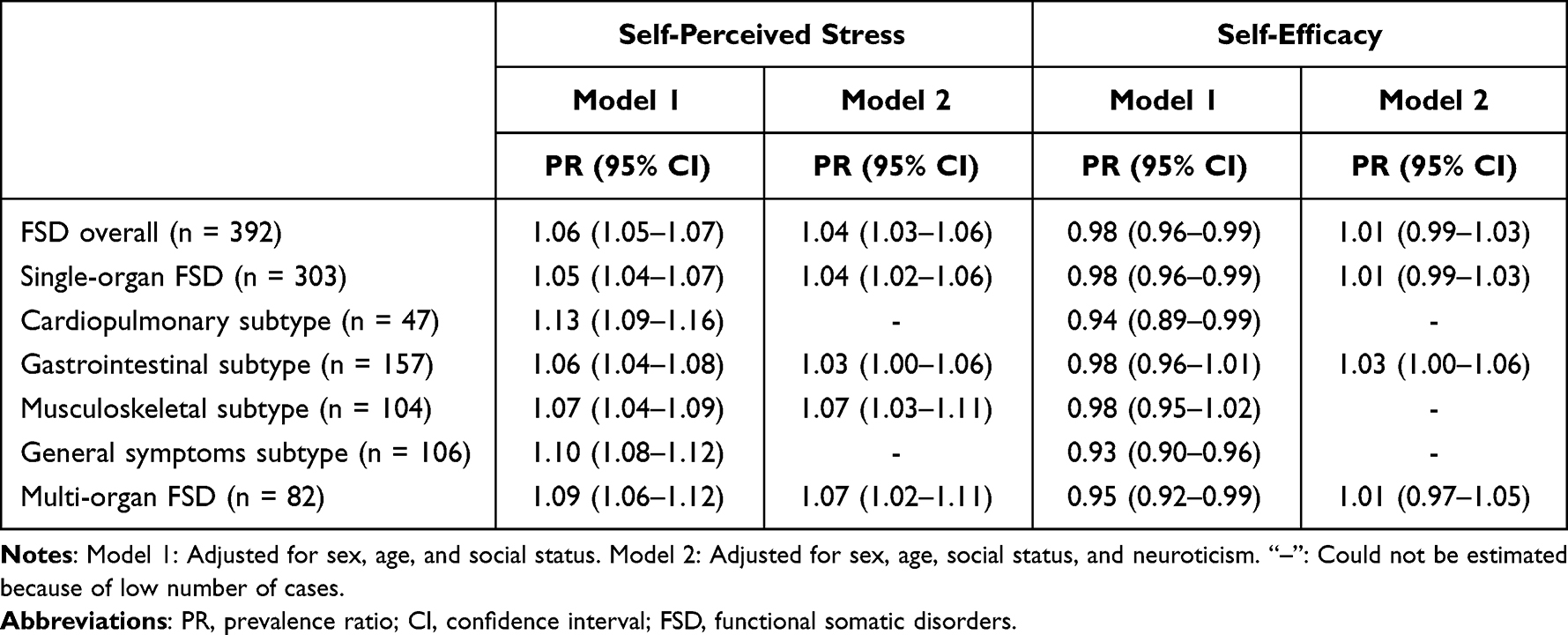 |
Table 3 Association Between Clinical Interview-Established Functional Somatic Disorders, Perceived Stress and Self-Efficacy |
For individuals with FSD established by the diagnostic interview, the same pattern was seen throughout all four models (Table 3). When comparing two participants who differed with only one point on the Cohen’s Perceived Stress Scale, ranging from 0 to 40, the participant with the highest score was 6% (95% CI: 5–7%) more likely to have overall FSD and 13% (95% CI: 9–16%) more likely to have the cardiopulmonary single-organ FSD type. Also here, the associations were reduced in model 2 (Table 3) with further adjustment for neuroticism, while additional adjustment for adverse life events and self-efficacy in model 3 and 4, respectively, did not change the size of association compared to model 2 (Table A2).
Examining the pure types of questionnaire-defined irritable bowel, chronic widespread pain, and chronic fatigue did not alter the above results (Table A3).
Self-Efficacy and Functional Somatic Disorders
Apart from the questionnaire-defined cardiopulmonary single-organ FSD subtype (Table 2) and the gastrointestinal and musculoskeletal FSD subtypes established by the diagnostic interview (Table 3), small but negative associations were found between self-efficacy and FSD in model 1, after adjusting for sex, age, and social status. Hence, a higher level of self-efficacy was associated with lower likelihood of having FSD in 14 out of 17 analyses.
Comparing two participants who differed with only one point on the General Self-Efficacy Scale, ranging from 0 to 30, the participant with the highest score was 7% (95% CI: 5–9%) less likely to have questionnaire-defined general symptoms/fatigue subtypes of FSD (Table 2). However, with further adjustment for neuroticism in model 2, the associations changed to a small positive association for the cardiopulmonary and gastrointestinal subtypes, whereas precision estimates for the associations for the other diagnoses changed to include 1. Further adjustment for adverse life events in model 3 and perceived stress in model 4 did not deviate from the results from model 2 (Table A1).
For individuals with FSD established by the diagnostic interview, the largest negative association was with the general symptoms subtype of FSD and multi-organ FSD in model 1 after adjusting for sex, age, and social status (Table 3). Hence, comparing two participants who differed with only one point on the General Self-Efficacy Scale, ranging from 0 to 30, the participant with the highest score was 7% (95% CI: 4–10%) less likely to have general symptoms/fatigue sub type of FSD and 5% (95% CI: 1–8%) less likely to have the multi-organ type of FSD. With further adjustment in model 2, the same pattern was seen as for the questionnaire-defined FSD cases: the associations changed and for most diagnoses, the precision estimates for the associations changed to include 1. For those delimitations with a sufficient number of cases to allow further adjustment, no differences in size of associations were found after adjusting for adverse life events and perceived stress in model 3 and 4, respectively (Table A2).
Looking into the pure types of irritable bowel, chronic widespread pain, and chronic fatigue did not alter the above results (Table A4).
For only some of the questionnaire-based FSD delimitations (overall FSD, single- and multi-organ type of FSD, the musculoskeletal and general symptoms subtypes of FSD, chronic fatigue, and the pure type of chronic fatigue) the analysis supported an interaction between perceived stress and self-efficacy on the likelihood of having FSD. However, as the size estimate was 0.1%, it was negligible.
Functional Somatic Disorders vs Severe Physical Disease
Both for questionnaire-defined FSD cases and individuals with FSD established by the diagnostic interview, the level of perceived stress was higher (90% CI for the difference did not contain 0) compared with healthy individuals and equivalent (90% CI for the difference was completely within the equivalence bounds ± 5 on the Cohen’s Perceived Stress Scale) to individuals with a severe physical disease and an FSD (Figure 1A, Table S5) as hypothesized. However, we could not support the hypothesis of equivalence in perceived stress between individuals with FSD and individuals with a severe physical disease (as the latter had 90% CI’s overlapping with −5) (Figure 1A, Table A5).
Both for questionnaire-defined FSD cases and individuals with FSD established by the diagnostic interview, the level of self-efficacy was lower (90% CI for the difference did not contain 0) compared with healthy individuals and individuals with severe physical disease as hypothesized (Figure 1B, Table A5). The hypothesis of equivalence (90% CI for the difference was completely within the equivalence bounds ± 2 on the General Self-efficacy Scale) between individuals with FSD and individuals with a severe physical disease and an FSD was supported for questionnaire-defined cases, however, not for individuals with FSD established with the diagnostic interview where the latter had 90% CI’s overlapping with −2 (Figure 1B, Table A5).
 |
Figure 1 Difference in self-perceived stress and self-efficacy between FSD and other disease groups. Abbreviations: FSD, functional somatic disorder, operationalized as Bodily Distress Syndrome; PhyDis, physical disease only; FSD+PhyDis, functional somatic disorder and physical disease; Ref., reference; Solid lines, questionnaire-defined cases; Dashed lines, interview-established cases. |
For the three FSS (irritable bowel, chronic widespread pain, and chronic fatigue), the hypotheses of lower perceived stress (90% CI for the difference did not contain 0) in healthy individuals and equivalent perceived stress (90% CI for the difference was completely within the equivalence bounds ± 5 on the Cohen’s Perceived Stress Scale) in individuals with severe physical disease and FSS were supported (Figure 1A, Table A6). However, the hypothesis of equivalence between individuals with FSS and individuals with severe physical disease could not be supported (as the latter had 90% CI’s lower than −5). As hypothesized, individuals with FSS had lower self-efficacy (90% CI for the difference did not contain 0) than healthy individuals and individuals with a severe physical disease, and equivalent self-efficacy (90% CI for the difference was completely within the equivalence bounds ± 2 on the General Self-efficacy Scale) as individuals with a severe physical disease and an FSS (Figure 1A, Table A6).
Discussion
In the present study, we found higher perceived stress and lower self-efficacy to be associated with FSD, especially for the multi-organ FSD type, the general symptoms/fatigue subtype, and chronic fatigue. However, after adjusting for neuroticism, the association with self-efficacy became non-significant for most of the diagnoses. Furthermore, our analysis did not support an important interaction between perceived stress and self-efficacy on the likelihood of having FSD.
Our study supports other studies showing stress to be associated with FSS,18,19 functional somatic symptoms,53,54 chronic fatigue syndrome,55 fibromyalgia,56,57 irritable bowel syndrome,58 and functional dyspepsia.59
Generally, we found that perceived stress was higher in individuals with FSD than in healthy individuals; however, we could not support the hypothesis of equivalence in perceived stress between individuals with FSD and individuals with a severe physical disease, as the latter had lower perceived stress. However, compared to individuals with severe physical disease and an FSD, we found equivalent levels of perceived stress. The literature on how to define a cut-off for evaluating equivalence is very sparse. Hence, it was necessary to base the definition on the knowledge that was available at the given time. However, it may be questioned if our 5-point cut-off may have been too high. Our results point towards equal or higher perceived stress in individuals with FSD compared with individuals with a severe physical disease, which may often be life threatening or at least have a heavy impact on their life quality. This underlines the severity of FSD, being a condition which – whether it is a risk factor for developing or a consequence of having FSD – presents with great stress for the patient. A review and meta-analysis by Berezowski et al60 supports this severity of FSD by stating that individuals suffering from FSS show at least the same, if not worse outcomes compared with individuals suffering from well-defined biomedical conditions.
Higher self-efficacy has been shown to be associated with less pain and less impairment and to predict the outcome in fibromyalgia patients.61,62 Furthermore, it has been shown to reduce functional impairment and contribute to higher general health in chronic widespread pain and chronic fatigue patients.63 In the current study, our hypotheses of lower self-efficacy in individuals with FSD compared with healthy individuals and individuals with a severe physical diagnosis was supported. Also, our data supported the hypothesis of equivalence (defined as a difference smaller than ±2 on the General Self-Efficacy Scale) comparing questionnaire-based FSD cases with individuals with a severe physical diagnosis and FSD.
Although our results showed lower self-efficacy to be associated with FSD, the association became insignificant after adjusting for neuroticism. Hence, it may be that there is an association between FSD and self-efficacy because of the confounding effect of neuroticism. Studies on this subject within the field of FSD are sparse and within other fields, results are contradicting: Population-based studies have found the association between low self-efficacy and self-reported depression to remain after adjustment for neuroticism,64 whereas the association with self-evaluated anxiety became insignificant.65 In a previous study, we found strong associations between FSD and higher neuroticism,10 and neuroticism has generally shown to be strongly associated with psychopathology and associated outcomes.66 Hence, the importance of neuroticism for disease development and disease outcome is not surprising.
Our study supports the understanding of FSD as being a “multi-system stress” or stress-related condition, which may be understood as dysregulated neural and systemic processes in shifts between homeostasis and allostasis, which may lead to allostatic overload. This is also a common explanation that clinicians give to their patients when explaining the illness mechanisms behind these conditions.67 Moreover, the relationship between stress and resilience and its important role for disease outcome has been exploited in the treatment of FSD patients including stress reduction and stress management in combination with other psychological interventions.68–71 Given the cross-sectional design of the current study, we cannot conclude on whether stress is a risk factor for developing FSD or it is a consequence of having FSD. However, our finding that individuals with FSD had non-equivalent perceived stress compared with individuals with a severe physical disease, but equivalent perceived stress compared with individuals with a severe physical disease and an FSD may point to stress being part of the symptomatology of FSD rather than being a consequence per se.
Strengths and Limitations
The inclusion of a large random sample from the general population with an almost equal distribution of women and men is a major strength of the current study. Also, many definitions of FSD have been proposed, and the current study used more than one definition to capture the diverse nature of FSD as both mono- and multi-systemic conditions.1 Another strength is the use of different methods for assessing FSD: The use of self-reported questionnaires is a convenient and cost-effective method, ensuring the possibility of investigating a large data material, and the diagnostic interviews performed by trained family physicians enabled us to investigate on clinically verified cases of FSD.
Some limitations also need to be addressed: First, an important limitation of the study is the response rate of 33.7% for the questionnaire sample and 64.9% for the interviewed sample caused by invited participants who declined to participate. Hence, although the risk of selection bias in this study was markedly reduced compared to clinical studies as participants were randomly drawn from the general population, we cannot rule it out completely. Unfortunately, it was not possible to statistically account for this non-response by eg post-survey weighting. However, a non-responder analysis indicated that selection bias did not seem to influence noticeably on social parameters, hence, it may be reasonable to believe that non-response did not influence on the psychological parameters included in the current study either.72 Second, even though potential confounders were identified by thoroughly made DAGs and we made a prioritized list of confounders to be adjusted for in several steps of analyses, it was not possible to take into account for all confounders in all analyses because of a too low number of cases in some of the dependent variables. This especially accounted analyses on the multi-organ type of FSD and for the diagnoses established by the diagnostic interview. Therefore, we cannot rule out possible confounding effect on the estimates from some of these analyses. Third, all measures for the current study were self-reported. Hence, recall bias and measurement error in terms of operator error, ie reading or understanding a question or scale incorrectly, might have occurred. However, as all included measures are well respected and often used questionnaires, we believe that any possible operator error would be random. Fourth, as the current study is cross-sectional, we cannot conclude on the direction of causality. Hence, we may propose that higher stress and lower self-efficacy contribute to the development of FSD, but we also have to consider a reverse causality where being ill with an FSD cause higher stress and lower self-efficacy for the patient. In order to conclude on these aspects, longitudinal studies are needed.
Conclusion
FSD were associated with higher perceived stress and lower self-efficacy, but the analysis did not support an important interaction between these two on the likelihood of having FSD. Individuals with FSD had lower self-efficacy but non-equivalent levels of perceived stress compared with individuals with a severe physical disease, which may point to stress being part of the symptomatology of FSD. Our study underlines the severity of FSD and justifies the incorporation of resilience theory in the understanding of FSD etiology and patient management.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, MWP, upon reasonable request.
Ethics Statement
The study complies with the Declaration of Helsinki. It was approved by the Ethical Committee of the Capital Region (H-3-2011-081, H-3-2012-015), and all participants gave written informed consent prior to study commencement.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the Lundbeck Foundation [grant number R155-2013-14070] and TrygFonden [grant number 7-11-0213 and grant number 153171].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Burton C, Fink P, Henningsen P, Lowe B, Rief W. Functional somatic disorders: discussion paper for a new common classification for research and clinical use. BMC Med. 2020;18(1):34. doi:10.1186/s12916-020-1505-4
2. Petersen MW, Schröder A, Jørgensen T, et al. Irritable bowel, chronic widespread pain, chronic fatigue and related syndromes are prevalent and highly overlapping in the general population: DanFunD. Sci Rep. 2020;10(1):3273. doi:10.1038/s41598-020-60318-6
3. Fink P. Funktionelle lidelser - fysiske symptomer og sygdomme uden kendt kropslig årsag.
4. Rask MT, Ørnbøl E, Rosendal M, Fink P. Long-term outcome of bodily distress syndrome in primary care: a follow-up study on health care costs, work disability, and self-rated health. Psychosom Med. 2016. doi:10.1097/PSY.0000000000000405
5. Henningsen P, Zipfel S, Herzog W. Management of functional somatic syndromes. Lancet. 2007;369(9565):946–955. doi:10.1016/S0140-6736(07)60159-7
6. Fink P, Schröder A. One single diagnosis, bodily distress syndrome, succeeded to capture 10 diagnostic categories of functional somatic syndromes and somatoform disorders. J Psychosom Res. 2010;68(5):415–426. doi:10.1016/j.jpsychores.2010.02.004
7. Schröder A, Sharpe M, Fink P. Medically unexplained symptom management. Lancet Psychiatry. 2015;2(7):587–588. doi:10.1016/S2215-0366(15)00233-3
8. Wessely S, Nimnuan C, Sharpe M. Functional somatic syndromes: one or many? Lancet. 1999;354(9182):936–939. doi:10.1016/S0140-6736(98)08320-2
9. Yunus MB. Fibromyalgia and overlapping disorders: the unifying concept of central sensitivity syndromes. Semin Arthritis Rheum. 2007;36(6):339–356. doi:10.1016/j.semarthrit.2006.12.009
10. Petersen MW, Carstensen TBW, Frostholm L, et al. Neuroticism and adverse life events are important determinants in functional somatic disorders: the DanFunD study. Sci Rep. 2022;12(1):19604. doi:10.1038/s41598-022-24213-6
11. Henningsen P, Gundel H, Kop WJ, et al. Persistent physical symptoms as perceptual dysregulation: a neuropsychobehavioral model and its clinical implications. Psychosom Med. 2018;80(5):422–431. doi:10.1097/PSY.0000000000000588
12. Lazarus RSFS. Stress, Appraisal, and Coping. Springer Publishing Company; 1984.
13. Banik A, Schwarzer R, Knoll N, Czekierda K, Luszczynska A. Self-efficacy and quality of life among people with cardiovascular diseases: a meta-analysis. Rehabil Psychol. 2018;63(2):295. doi:10.1037/rep0000199
14. Cohen S, Janicki-Deverts D, Miller GE. Psychological stress and disease. JAMA. 2007;298(14):1685–1687. doi:10.1001/jama.298.14.1685
15. Korpershoek C, Van der Bijl J, Hafsteinsdóttir TB. Self‐efficacy and its influence on recovery of patients with stroke: a systematic review. J Adv Nurs. 2011;67(9):1876–1894. doi:10.1111/j.1365-2648.2011.05659.x
16. Chirico A, Lucidi F, Merluzzi T, et al. A meta-analytic review of the relationship of cancer coping self-efficacy with distress and quality of life. Oncotarget. 2017;8(22):36800–36811. doi:10.18632/oncotarget.15758
17. Mineva K, Petrova B. Psychosocial factors associated with chronic disease self-efficacy in patients with rheumatic diseases. Trakia J Sci. 2017;15(3):233.
18. Nater M, Fischer S, Ehlert U. Stress as a pathophysiological factor in functional somatic syndromes. Curr Psychiatry Rev. 2011;7(2):152–169. doi:10.2174/157340011796391184
19. Fischer S, Lemmer G, Gollwitzer M, Nater UM, Dekel S. Stress and resilience in functional somatic syndromes--a structural equation modeling approach. PLoS One. 2014;9(11):e111214. doi:10.1371/journal.pone.0111214
20. Creed F. The predictors of somatic symptoms in a population sample: the Lifelines cohort study. Psychosom Med. 9900. doi:10.1097/psy.0000000000001101
21. Galvez-Sánchez CM, Duschek S, Reyes del paso GA. Psychological impact of fibromyalgia: current perspectives. Psychol Res Behav Manag. 2019;12:117–127. doi:10.2147/PRBM.S178240
22. Williamson E, Williams M, Gates S, Lamb SE. A systematic literature review of psychological factors and the development of late whiplash syndrome. PAIN. 2008;135(1):20–30. doi:10.1016/j.pain.2007.04.035
23. Knoop H, Prins JB, Moss-Morris R, Bleijenberg G. The central role of cognitive processes in the perpetuation of chronic fatigue syndrome. J Psychosom Res. 2010;68(5):489–494. doi:10.1016/j.jpsychores.2010.01.022
24. McEwen BS. Allostasis and the epigenetics of brain and body health over the life course: the brain on stress. JAMA Psychiatry. 2017;74(6):551–552. doi:10.1001/jamapsychiatry.2017.0270
25. Fink P. Syndromes of bodily distress or functional somatic syndromes - Where are we heading. Lecture on the occasion of receiving the Alison Creed award 2017. J Psychosom Res. 2017;97:127–130. doi:10.1016/j.jpsychores.2017.04.012
26. Drossman DA. From pretending to truly being OK: a journey from illness to health with postinfection irritable bowel syndrome: the provider’s perspective. Gastroenterol. 2018;155(6):1664–1665. doi:10.1053/j.gastro.2018.11.002
27. Dantoft TM, Ebstrup JF, Linneberg A, et al. Cohort description: the Danish study of functional disorders. Clin Epidemiol. 2017;9:127–139. doi:10.2147/CLEP.S129335
28. Pedersen CB. The Danish civil registration system. Scand J Public Health. 2011;39(7Suppl):22–25. doi:10.1177/1403494810387965
29. Petersen MW, Schröder A, Jørgensen T, et al. RIFD - A brief clinical research interview for functional somatic disorders and health anxiety. J Psychosom Res. 2019;122:104–111. doi:10.1016/j.jpsychores.2019.04.001
30. Fink P, Toft T, Hansen MS, Ørnbøl E, Olesen F. Symptoms and syndromes of bodily distress: an exploratory study of 978 internal medical, neurological, and primary care patients. Psychosom Med. 2007;69(1):30–39. doi:10.1097/PSY.0b013e31802e46eb
31. Budtz-Lilly A, Fink P, Ørnbøl E, et al. A new questionnaire to identify bodily distress in primary care: the ‘BDS checklist’. J Psychosom Res. 2015;78(6):536–545. doi:10.1016/j.jpsychores.2015.03.006
32. Petersen MW, Schröder A, Jørgensen T, et al. The unifying diagnostic construct of bodily distress syndrome (BDS) was confirmed in the general population. J Psychosom Res. 2019;128:109868. doi:10.1016/j.jpsychores.2019.109868
33. Hauser W, Constanze Hausteiner W, Henningsen P, Brahler E, Schmalbach B, Wolfe F. Prevalence and overlap of somatic symptom disorder, bodily distress syndrome and fibromyalgia syndrome in the German general population: a cross sectional study. J Psychosom Res. 2020;133:110111. doi:10.1016/j.jpsychores.2020.110111
34. Schmalbach B, Roenneberg C, Hausteiner-Wiehle C, et al. Validation of the German version of the bodily distress syndrome 25 checklist in a representative German population sample. J Psychosom Res. 2020;132:109991. doi:10.1016/j.jpsychores.2020.109991
35. Wertenbruch-Rocke T, Hüsing P, Löwe B, Toussaint A. Application and validation of the bodily distress syndrome checklist in a psychosomatic outpatient sample. Gen Hosp Psychiatry. 2021;69:104–110. doi:10.1016/j.genhosppsych.2020.12.005
36. Kay L, Jørgensen T. Redefining abdominal syndromes. Results of a population-based study. Scand J Gastroenterol. 1996;31(5):469–475. doi:10.3109/00365529609006767
37. White KP, Harth M, Speechley M, Ostbye T. Testing an instrument to screen for fibromyalgia syndrome in general population studies: the London Fibromyalgia Epidemiology Study Screening Questionnaire. J Rheumatol. 1999;26(4):880–884.
38. Chalder T, Berelowitz G, Pawlikowska T, et al. Development of a fatigue scale. J Psychosom Res. 1993;37(2):147–153. doi:10.1016/0022-3999(93)90081-P
39. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–396. doi:10.2307/2136404
40. Eskildsen A, Dalgaard VL, Nielsen KJ, et al. Cross-cultural adaptation and validation of the Danish consensus version of the 10-item Perceived Stress Scale. Scand J Work Environ Health. 2015;41(5):486–490. doi:10.5271/sjweh.3510
41. Luszczynska A, Scholz U, Schwarzer R. The general self-efficacy scale: multicultural validation studies. J Psychol. 2005;139(5):439–457. doi:10.3200/jrlp.139.5.439-457
42. Singh-Manoux A, Adler NE, Marmot MG. Subjective social status: its determinants and its association with measures of ill-health in the Whitehall II study. Soc Sci Med. 2003;56(6):1321–1333. doi:10.1016/s0277-9536(02)00131-4
43. Hansen HM, Mortensen EL. Dokumentation for den danske udgave af NEO PI-R og NEO PI-R Kort Version. NEO PI-R Manual - Klinisk. Hogrefe Psykologisk Forlag A/S; 2004.
44. Costa PJ, McCrae R. Revised NEO Personality Inventory (NEO-PI-R) and NEO Five-Factor Inventory (NEO-FFI) Professional Manual. Odessa, FL: Psychological Assessment Ressources; 1992.
45. Carstensen TBW, Ørnbøl E, Fink P, et al. Adverse life events in the general population - a validation of the cumulative lifetime adversity measure. Eur J Psychotraumatol. 2020;11(1):1717824. doi:10.1080/20008198.2020.1717824
46. StataCorp. Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC; 2021.
47. Barros AJ, Hirakata VN. Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol. 2003;3:21. doi:10.1186/1471-2288-3-21
48. Textor J, van der Zander B, Gilthorpe MS, Liskiewicz M, Ellison GT. Robust causal inference using directed acyclic graphs: the R package ‘dagitty’. Int J Epidemiol. 2016;45(6):1887–1894. doi:10.1093/ije/dyw341
49. Greenland S. Interpretation and choice of effect measures in epidemiologic analyses. Am J Epidemiol. 1987;125(5):761–768. doi:10.1093/oxfordjournals.aje.a114593
50. Ramert A, Westphal E. Equivalence testing. STAT COE-Report-12-2020; 2020.
51. Dixon PM, Saint-Maurice PF, Kim Y, Hibbing P, Bai Y, Welk GJ. A primer on the use of equivalence testing for evaluating measurement agreement. Med Sci Sports Exerc. 2018;50(4):837–845. doi:10.1249/mss.0000000000001481
52. Walker E, Nowacki AS. Understanding equivalence and noninferiority testing. J Gen Intern Med. 2011;26(2):192–196. doi:10.1007/s11606-010-1513-8
53. van Gils A, Burton C, Bos EH, Janssens KA, Schoevers RA, Rosmalen JG. Individual variation in temporal relationships between stress and functional somatic symptoms. J Psychosom Res. 2014;77(1):34–39. doi:10.1016/j.jpsychores.2014.04.006
54. Deary V, Chalder T, Sharpe M. The cognitive behavioural model of medically unexplained symptoms: a theoretical and empirical review. Clin Psychol Rev. 2007;27(7):781–797. doi:10.1016/j.cpr.2007.07.002
55. Nater UM, Maloney E, Heim C, Reeves WC. Cumulative life stress in chronic fatigue syndrome. Psychiatry Res. 2011;189(2):318–320. doi:10.1016/j.psychres.2011.07.015
56. Murray JTL, Murray CE, Daniels MH. Stress and family relationship functioning as indicators of the severity of fibromyalgia symptoms: a regression analysis. Stress Health. 2007;23(1):3–8. doi:10.1002/smi.1102
57. Van Houdenhove B, Egle U, Luyten P. The role of life stress in fibromyalgia. Curr Rheumatol Rep. 2005;7(5):365–370. doi:10.1007/s11926-005-0021-z
58. Mayer EA, Naliboff BD, Chang L, Coutinho SVV. Stress and irritable bowel syndrome. Am J Physiol Gastrointest Liver Physiol. 2001;280(4):G519–24. doi:10.1152/ajpgi.2001.280.4.G519
59. Klaassen T, Vork L, Smeets FGM, et al. The interplay between stress and fullness in patients with functional dyspepsia and healthy controls: an exploratory experience sampling method study. Psychosom Med. 2022;84(3):306–312. doi:10.1097/psy.0000000000001012
60. Berezowski L, Ludwig L, Martin A, Löwe B, Shedden-Mora MC. Early psychological interventions for somatic symptom disorder and functional somatic syndromes: a systematic review and meta-analysis. Psychosom Med. 2022;84(3):325–338. doi:10.1097/psy.0000000000001011
61. Buckelew SP, Murray SE, Hewett JE, Johnson J, Huyser B. Self-efficacy, pain, and physical activity among fibromyalgia subjects. Arthritis Care Res. 1995;8(1):43–50. doi:10.1002/art.1790080110
62. Buckelew SP, Huyser B, Hewett JE, et al. Self-efficacy predicting outcome among fibromyalgia subjects. Arthritis Care Res. 1996;9(2):97–104. doi:10.1002/1529-0131(199604)9:2<97::
63. Smith WR, Strachan ED, Buchwald D. Coping, self-efficacy and psychiatric history in patients with both chronic widespread pain and chronic fatigue. Gen Hosp Psychiatry. 2009;31(4):347–352. doi:10.1016/j.genhosppsych.2009.03.012
64. Bonsaksen T, Grimholt TK, Skogstad L, et al. Self-diagnosed depression in the Norwegian general population – associations with neuroticism, extraversion, optimism, and general self-efficacy. BMC Public Health. 2018;18(1):1076. doi:10.1186/s12889-018-5990-8
65. Bonsaksen T, Heir T, Ekeberg Ø, et al. Self-evaluated anxiety in the Norwegian population: prevalence and associated factors. Arch Public Health. 2019;77:10. doi:10.1186/s13690-019-0338-0
66. Ormel J, Rosmalen J, Farmer A. Neuroticism: a non-informative marker of vulnerability to psychopathology. Soc Psychiatry Psychiatr Epidemiol. 2004;39(11):906–912. doi:10.1007/s00127-004-0873-y
67. Saunders CT, Rask H, Pedersen MT, Rask H, Burton C, Frostholm L. The ways we explain functional somatic symptoms. Under preparation; 2022.
68. Fjorback LO, Arendt M, Ørnbøl E, et al. Mindfulness therapy for somatization disorder and functional somatic syndromes: randomized trial with one-year follow-up. J Psychosom Res. 2013;74(1):31–40. doi:10.1016/j.jpsychores.2012.09.006
69. Schröder A, Rehfeldt E, Ørnbøl E, Sharpe M, Licht RW, Fink P. Cognitive-behavioural group treatment for a range of functional somatic syndromes: randomised trial. Br J Psychiatry. 2012;200(6):499–507. doi:10.1192/bjp.bp.111.098681
70. Pedersen HF, Agger JL, Frosthom L, et al. Acceptance and Commitment group Therapy for patients with multiple functional somatic syndromes: a three-armed trial comparing ACT in a brief and extended version with enhanced care. Psychol Med. 2018:1–10. doi:10.1017/S0033291718001666
71. Rief W, Burton C, Frostholm L, et al. Core outcome domains for clinical trials on somatic symptom disorder, bodily distress disorder, and functional somatic syndromes: European network on somatic symptom disorders recommendations. Psychosom Med. 2017;79(9):1008–1015. doi:10.1097/psy.0000000000000502
72. Schovsbo SU, Dantoft TM, Thuesen BH, et al. Social position and functional somatic disorders: the DanFunD study. Scand J Public Health. 2021:14034948211056752. doi:10.1177/14034948211056752
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.