Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
High Levels of D-Dimer are Associated with Poor Hospitalization Outcome of Spontaneous Intraparenchymal Haemorrhage
Received 23 February 2022
Accepted for publication 18 May 2022
Published 30 May 2022 Volume 2022:18 Pages 1079—1086
DOI https://doi.org/10.2147/NDT.S362331
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jun Chen
Xuguang Chen,* Shengyi Shi,* Lan Hu
Department of Emergency, Ruijin Hospital, Shanghai Jiao Tong University School of Medical, Shanghai, 201800, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lan Hu, Department of Emergency, Ruijin Hospital, Shanghai Jiao Tong University School of Medical, Shanghai, 201800, People’s Republic of China, Tel +86 181-2126-3197, Email [email protected]
Objective: To investigate whether D-dimer levels and changes in D-dimer levels can be used as effective indexes to evaluate the risk of death among intraparenchymal haemorrhage (IPH) patients.
Methods: A retrospective cohort study of 732 patients with IPH was conducted at an academic medical centre. The risk factors for adverse hospitalization outcomes were analysed, and logistic multivariate analysis was performed. Patients were divided into supratentorial, brainstem and cerebellum groups. According to whether intraventricular haematoma (IVH) and subarachnoid haematoma (SAH) co-occurred, the supratentorial group was divided into simple haematoma, combined IVH, combined SAH and combined IVH+SAH subgroups. The relationship between D-dimer levels and hospitalization outcome in each group/ subgroup was analysed.
Results: Compared with survivors, the plasma D-dimer level of the nonsurvivors on the second day after admission was significantly higher (2.52 ± 3.89 μg/mL vs 0.77 ± 2.31 μg/mL, P = 0.032), and the difference in plasma D-dimer levels between the second day after admission and admission significantly increased (1.77 ± 3.70 μg/mL vs 0.26 ± 2.80 μg/mL, P = 0.049), and a D-dimer level on day 2 > 0.58 μg/mL was an independent risk factor for mortality among IPH patients (OR 3.114, 95% CI: 1.007). In the supratentorial group and the IVH subgroup, the level of D-dimer on day 2 was significantly higher among nonsurvivors than among survivors (2.18 ± 2.13 μg/mL vs 0.65 ± 1.04 μg/mL, P = 0.011; 2.45 ± 2.31 μg/mL vs 0.91 ± 1.26 μg/mL, P = 0.028, respectively).
Conclusion: The increase in plasma D-dimer levels on day 2 is related to poor hospitalization outcomes of patients with IPH, and this correlation may exist only among patients with both IVH and IPH.
Keywords: intraparenchymal hemorrhage, D-dimer, hospitalization outcomes
Introduction
Spontaneous intraparenchymal haemorrhage (IPH) accounts for 6.5% to 19.6% of stroke cases; however, the highest mortality rate is 36.3% at 30 days, and the one-year survival rate is approximately 40%.1,2 At present, although there are many treatments for IPH, effective treatments are lacking. Therefore, early and accurate assessment of the death risk is very important for improving prognosis. Previous studies have found that local brain injury caused by IPH can cause systemic coagulation activation and fibrinolytic hyperfunction.3,4 However, activation of coagulation and hyperfibrinolysis may lead to an increase in haematoma volume and expansion of the haematoma in the ventricle, increasing the risk of IPH-related death. Therefore, the purpose of this study was to investigate whether the D-dimer level and changes in D-dimer levels can be used as effective indexes for evaluating the risk of death among patients with IPH.
Patients and Methods
Patients
IPH patients who visited the emergency department of Ruijin Hospital affiliated with Shanghai Jiao Tong University School of Medicine from May 1, 2017, to December 31, 2021, were selected as the research subjects. The inclusion criteria were ① a diagnosis of IPH in accordance with the guidelines;5 ② age > 18 years old; ③ first onset of IPH; and ④ plasma D-dimer data at the time of admission and on the second day following admission. The exclusion criteria were ① intracerebral haemorrhage caused by abnormal coagulation; ② haemorrhage after infarction; ③ complication with thrombosis; or ④ complication with trauma. The research was carried out according to the Helsinki Declaration and was approved by the Ethics Committee of Ruijin Hospital affiliated with Shanghai Jiao Tong University School of Medicine. According to the location of bleeding, patients were divided into a supratentorial group, brainstem group and cerebellum group. According to whether intraventricular haematoma (IVH) and subarachnoid haematoma (SAH) co-occurred, the supratentorial group was divided into a simple haematoma subgroup, combined IVH subgroup, combined SAH subgroup and combined IVH+SAH subgroup. Patients were divided into a nonsurvival group and a survival group according to whether they died during hospitalization.
Data Acquisition
The collected data included demographic and clinical characteristics, such as age, sex, bleeding location, systolic blood pressure (SBP), diastolic blood pressure (DBP), Glasgow Coma Scale (GCS) score, Graeb scale scores at admission, and whether surgery was performed, and laboratory data, including plasma d-dimer (D-dimer admission), glucose (Glu), calcium (Ca), creatinine (Cr), glutamic-pyruvic transaminase (GPT), cardiac troponin I (cTnI), and C-reactive protein (CRP) levels, white blood cell count (WBC), platelet count (PLT), and international normalized ratio (INR) on admission; plasma D-dimer levels (D-dimer day 2) on the second day after admission; and the calculation of the change in D-dimer levels after admission (ΔD-dimer = D-dimer day 2 - D-dimer admission).
All patients were examined by CT with a thickness of 5 mm within 1 hour after admission. A deviation of the midline structure from the line of the median bone ridge of the frontal parietal bone by more than 5 mm is regarded as midline displacement. The bleeding sites of patients with IPH are classified as the supratentorial region, brain stem and cerebellum. The haematoma volume (V) of the brain parenchyma was calculated, that is, V=a×b×c×1/2, where a is the largest bleeding diameter, b is the largest diameter perpendicular to a in the same plane, and c is the number of bleeding planes. The volume of ventricular haemorrhage was scored by the Graeb scale score.
Statistical Analysis
Statistical Package for Social Science (SPSS) version 23.0 (IBM Corp., Armonk, NY) and GraphPad Prism 9 (GraphPad Software Inc.) were used for data processing. Qualitative data are expressed as frequencies (percentages), and the chi-square test or Fisher’s exact test was used to compare the differences between groups as appropriate. The Kolmogorov–Smirnov test was conducted to assess the data distribution of quantitative variables. The quantitative data conforming to a normal distribution are expressed as x±s, and an independent sample t-test was used to compare data between groups. Quantitative data that did not conform to a normal distribution are expressed as M (Q1, Q3), and the Mann–Whitney U-test was used for comparisons between groups. The area under the curve (AUC) and 95% CI generated by the analysis of the receiver operating characteristic (ROC) curve were used to evaluate the predictive value. A stepwise logistic regression model, including important variables from univariate analysis (P<0.05), was used to identify independent risk factors for in-hospital death and reported as the odds ratio (OR) and 95% confidence interval (CI) showing the correlation. Spearman correlation between the different variables was calculated. A P value<0.05 indicates that the difference was statistically significant.
Results
Patient Characteristics
A total of 732 patients with IPH were included in this study, and after exclusion of 39 patients with primary intrinsic haemorrhagic disease (PIVH), 27 patients with trauma, 9 patients with cerebral haemorrhage caused by abnormal blood coagulation, 4 patients with postinfarction haemorrhage, 11 patients with thrombosis, and 21 patients with missing data, 621 eligible patients remained (Figure 1). The average age of the patients was 60.1 (15.3) years, and there were 443 males and 178 females. There were 542, 45 and 34 patients with haemorrhage in the supratentorial region, brainstem and cerebellum, respectively. There were 349 patients in the simple haematoma subgroup, 155 patients in the combined IVH subgroup, 62 patients in the combined SAH subgroup and 55 patients in the combined IVH and SAH subgroup. Thirty-six percent of the patients had supratentorial IPH combined with IVH, 20% had supratentorial IPH combined with SAH, 19% had infectious IPH (including the brainstem and cerebellum) combined with IVH, 14% had infectious IPH combined with SAH, and the proportion of supratentorial IPH combined with IVH was significantly higher than that of infectious IPH (x2= 8.893, p=0.003). The median GCS score of all patients was 12 (10, 14), and the average haematoma volume of patients with IPH was 19.1±24.1 mL. The median Graeb scale score of all IPH patients with IVH was 4 (2, 6). Ninety-two patients received surgical treatment, and 81 patients died during hospitalization.
 |
Figure 1 The enrollment strategies of the study. Abbreviations: IPH, intraparenchymal hemorrhage; PIVH, primary intraventricular hemorrhage. |
Analysis of Risk Factors for In-Hospital Mortality
The overall in-hospital mortality rate was 13%. In univariate analysis, age (P=0.030), GCS score (P=0.000), midline deviation (P=0.000), haematoma expansion (P=0.013), haematoma volume (P=0.000), D-dimer day 2 (P=0.032), and WBC count (P=0.030) were related to in-hospital death, but D-dimer admission was not related to in-hospital death (P=0.275) (Table 1).
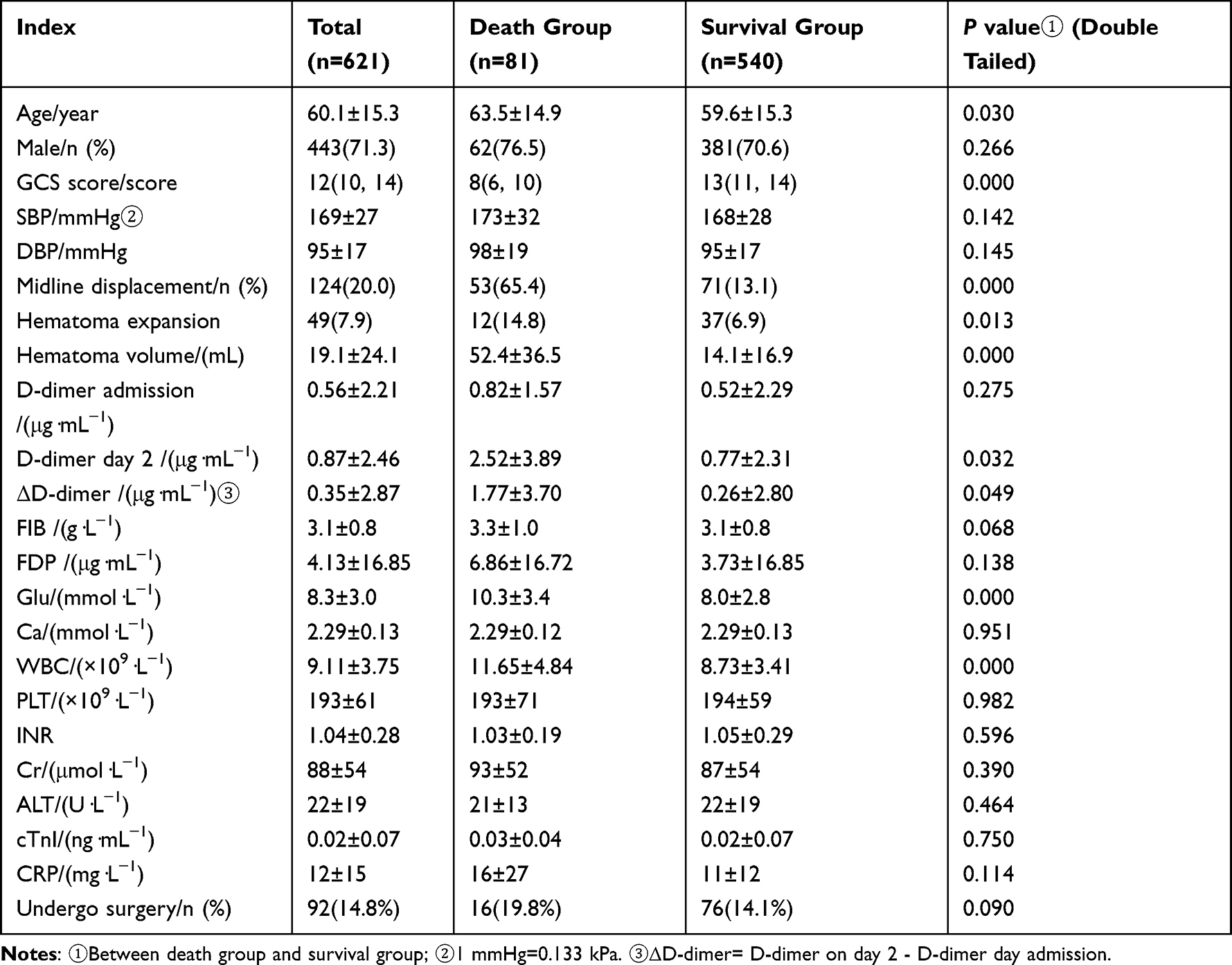 |
Table 1 Baseline Clinical Features of IPH |
The ROC curve showed that the accuracy of D-dimer day 2 and ΔD-dimer in predicting in-hospital death due to IPH was similar (AUC: 0.76 vs 0.75) but lower than that of both the GCS score (AUC=0.83, 95% CI 0.79~0.89) and haematoma volume (AUC = 0.83, 95% CI 0.77~0) However, it was higher than that of the age (AUC=0.58, 95% CI 0.51~0.64), Glu (AUC=0.65, 95% CI 0.59~0.72) and WBC count (AUC=0.69, 95% CI 0.63~0.76) (Figure 2).
 |
Figure 2 ROC curves for risk factors for in-hospital death in IPH. Abbreviations: GCS, Glasgow Coma Scale; WBC, white blood cell count. |
The ROC cut-off value for univariate prediction of in-hospital death was obtained, and in-hospital death was used as the dependent variable. Midline deviation, haematoma expansion, D-dimer day 2>0.58 μg/mL, GCS score, age, blood glucose > 8.8 mmol/L, WBC count>8.76×109/L, and haematoma volume were included as independent variables in multivariate logistic regression analysis. The results showed that haematoma volume, GCS score, haematoma expansion and D-dimer day 2>0.58 μg/mL were independent risk factors for in-hospital death among IPH patients, but midline deviation, age, blood glucose > 8.8 mmol/L, and WBC count>8.76×109/L showed no correlation with in-hospital death (Figure 3).
 |
Figure 3 Multifactorial analysis of risk factors for In-hospital death of IPH. |
Spearman correlation analysis showed that there was a significant correlation between D-dimer day 2 and haematoma volume (r=0.151, p=0.001), age (r=0.350, p=0.000), GCS score (r= −0.149, p=0.001), and grade (R = 0.350, p = 0.001). The level of D-dimer on day 2 in patients with midline deviation was higher than that in patients without a midline deviation (1.20±1.61 μg/mL vs 0.81±2.59 μg/mL), but the difference was not statistically significant (P=0.205). The level of D-dimer day 2 in patients with haematoma expansion was higher than that in patients without haematoma expansion (1.46±3.18 μg/mL vs 0.81±2.37 μg/mL), but the difference was not statistically significant (P=0.214).
Grouping Analysis of the Correlation Between D-Dimer Level on Day 2 and Hospitalization Outcome
The differences in D-dimer levels on day 2 between hospitalized survivors and nonsurviving patients in the supratentorial group, brainstem group and cerebellar group were analysed. The results showed that the level of D-dimer day 2 in hospitalized patients who died in the supratentorial group was significantly higher than that in survivors (2.18±2.13 μg/mL, 0.65±1.04 μg/mL, P = 0.011). In the brainstem group and cerebellum group, although the level of D-dimer day 2 in hospitalized nonsurvivors (1.60±2.67 μg/mL, 1.76±2.31 μg/mL) was higher than that in survivors (0.55±0.74 μg/mL, 0.50±0.54 μg/mL), the difference was not statistically significant (P>0.05) (Figure 4).
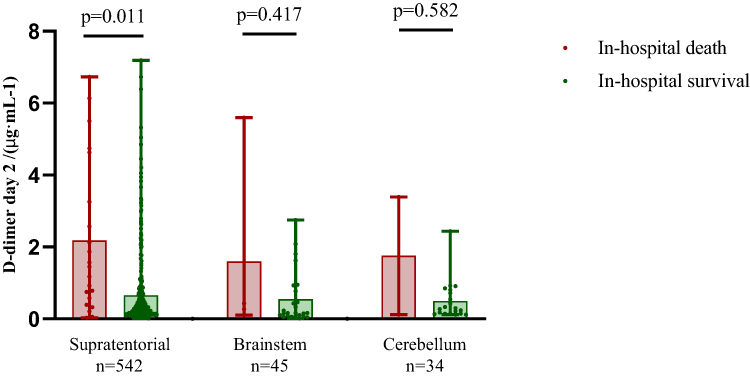 |
Figure 4 Comparison of D-dimer on day 2 levels between in-hospital death and survival groups among IPH patients at different sites. The data presented are M (Q1, Q3) showing all the data points. |
The levels of D-dimer day 2 in the simple haematoma subgroup, combined IVH subgroup, combined SAH subgroup and combined IVH+SAH subgroup were analysed. The results showed that in the combined IVH subgroup, the level of D-dimer day 2 in hospitalized nonsurvivors was 2.45±2.31 μg/mL, which was significantly higher than that in survivors (0.91±1.26 μ g/mL, P = 0.028), while the levels of D-dimer day 2 in patients in the simple haematoma, combined SAH subgroup and combined IVH+SAH subgroups (1.58±2.96 μg/mL, 2.36±1.67 μg/mL, 2.12±2.29 μg/mL) were higher than those of the surviving patients in these groups (0.42±0.56 μg/mL, 1.16±1.78 μg/mL, 0.90±1.04 μg/mL), but the differences were not statistically significant (P>0.05) (Figure 5).
 |
Figure 5 Comparison of D-dimer on day 2 levels in hospital deaths and survivors in different subgroups. The data presented are M (Q1, Q3) showing all the data points. |
Discussion
The activation of the coagulation system after IPH was discovered in the very early phase. In 2001, some studies found that the thrombin-antithrombin complex, plasmin-antifibrinolytic complex and D-dimer levels in the blood of patients with IPH were significantly higher than normal,4 and another study found that blood clots formed more quickly and were stronger in patients with IPH than in healthy people by thromboelastography and that they had shorter R and delta values at baseline.6 Plasma D-dimer levels, as a good index for measuring the activity of the systemic fibrinolytic system, has attracted increasing attention in patients with IPH. Meta-analysis shows that the level of D-dimer in patients with IPH is higher than that in healthy people.7 Another population-based case–control study found that a high plasma level of D-dimer predicted an increased risk of IPH in the future.8 Delgado P et al found that the increase in D-dimer levels in patients with IPH was related to the early deterioration of neurological function.9 It has also been found that the increase in D-dimer levels at admission is related to an adverse neurological prognosis and death 90 days after IPH.10,11 Although our study also found that the level of D-dimer at admission for IPH patients with poor hospitalization outcomes was higher than that of those with good hospitalization outcomes, there was no significant correlation between the level of D-dimer at admission and hospitalization outcomes, the increase in D-dimer levels and Δ D-dimer on the second day after admission significantly increased the risk of in-hospital death among of IPH patients, and a D-dimer day 2 level>0.58 μg/mL was an independent risk factor for in-hospital death of IPH patients. The D-dimer level on the second day following onset can be used to evaluate the hospitalization outcome of IPH.
Interestingly, through further analysis, we found that although the level of D-dimer on day 2 in patients with poor hospitalization outcomes was higher than that in patients with good hospitalization outcomes, regardless of the bleeding site of IPH or whether IPH was combined with IVH or SAH, the level of D-dimer on day 2 was significantly correlated with hospitalization outcomes only in patients with supratentorial IPH or IPH combined with IVH. Because the proportion of supratentorial IPH combined with IVH is obviously higher than that of infratentorial IPH, and D-dimer day 2 is related to grade, it seems that the correlation between D-dimer day 2 and the hospitalization outcome of IPH is related to combination with IVH. IVH is known to be an important clinical factor that increases the mortality rate of IPH. Reducing the volume of intraventricular blood can reduce the volume of haematoma in brain parenchyma.12,13 The coagulation cascade reaction is one of the important mechanisms. After blood enters the ventricle, the coagulation and fibrinolysis systems are activated, and thrombin induces astrocyte proliferation and destroys the blood–brain barrier, causing vascular oedema. After fibrinogen is converted into fibrin, the blood clot that is formed will hinder the circulation of cerebrospinal fluid, and fibrinogen that is released into the ventricle can induce a strong inflammatory reaction. Microglia are activated by CD11b/CD18 receptors, causing brain injury.14,15 Therefore, we speculate that the D-dimer level on day 2 may be related to poor hospitalization outcomes by reflecting the degree of obstacles in the coagulation and fibrinolysis pathways caused by IVH. Within the few hours from onset to admission, IVH does not have enough time or capacity to cause noticeable changes in the coagulation and fibrinolysis systems. Unfortunately, we could not assess whether the increase in ventricular haemorrhage was related to Δ D-dimer synchronization. Delgado P indicated that a possible explanation for the correlation mechanism between D-dimer and adverse outcomes is that abnormal coagulation and fibrinolysis may lead to an increase in ICH volume and early haematoma growth.9 Our research also found that the D-dimer day 2 level had a weak correlation with haematoma volume, but this hypothesis is hard to explain because D-dimer day 2 has no obvious correlation with haematoma expansion. In addition, we noticed that the D-dimer day 2 level was also related to age and GCS score. Although the correlation was not high, it suggested that D-dimer day 2 might be related to the severity of the disease. The correlation mechanism between D-dimer day 2 and adverse hospitalization outcomes may need to be explained by the pathophysiological mechanism of D-dimer in IPH. We also acknowledge that our study has some limitations. Our study did not better eliminate the effect of surgical operation on D-dimer, although only the second D-dimer report of 31 (5%) patients was obtained after surgical operation. Further studies with a prospective and multicenter trial are needed to confirm our findings.
In summary, our study found that the level of plasma D-dimer day 2 or the increase in ΔD-dimer was related to adverse hospitalization outcomes of IPH and that a level of D-dimer day 2>0.58 μg/mL was an independent risk factor for adverse hospitalization outcomes of IPH. However, the value of D-dimer day 2 in evaluating the hospitalization outcome of IPH may be applicable only to patients with IVH.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gross BA, Jankowitz BT, Friedlander RM. Cerebral intraparenchymal hemorrhage: a review. JAMA. 2019;321(13):1295–1303. doi:10.1001/jama.2019.2413
2. Pinho J, Costa AS, Araújo JM, Amorim JM, Ferreira C. Intracerebral hemorrhage outcome: a comprehensive update. J Neurol Sci. 2019;398:54–66. doi:10.1016/j.jns.2019.01.013
3. Lauridsen SV, Hvas AM, Sandgaard E, et al. Coagulation profile after spontaneous intracerebral hemorrhage: a cohort study. J Stroke Cerebrovasc Dis. 2018;27(11):2951–2961. doi:10.1016/j.jstrokecerebrovasdis.2018.06.022
4. Fujii Y, Takeuchi S, Harada A, Abe H, Sasaki O, Tanaka R. Hemostatic activation in spontaneous intracerebral hemorrhage. Stroke. 2001;32(4):883–890. doi:10.1161/01.STR.32.4.883
5. Sacco RL, Kasner SE, Broderick JP, et al. An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44(7):2064–2089. doi:10.1161/STR.0b013e318296aeca
6. Kawano-Castillo J, Ward E, Elliott A, et al. Thrombelastography detects possible coagulation disturbance in patients with intracerebral hemorrhage with hematoma enlargement. Stroke. 2014;45(3):683–688. doi:10.1161/STROKEAHA.113.003826
7. Zhou Z, Liang Y, Zhang X, et al. Plasma D-Dimer concentrations and risk of intracerebral hemorrhage: a systematic review and meta-analysis. Front Neurol. 2018;9:1114. doi:10.3389/fneur.2018.01114
8. Johansson K, Jansson JH, Johansson L, Wiklund PG, Nilsson TK, Lind M. D-Dimer is associated with first-ever intracerebral hemorrhage. Stroke. 2018;49(9):2034–2039. doi:10.1161/STROKEAHA.118.021751
9. Delgado P, Alvarez-Sabín J, Abilleira S, et al. Plasma d-dimer predicts poor outcome after acute intracerebral hemorrhage. Neurology. 2006;67(1):94–98. doi:10.1212/01.wnl.0000223349.97278.e0
10. Hu X, Fang Y, Ye F, et al. Effects of plasma D-dimer levels on early mortality and long-term functional outcome after spontaneous intracerebral hemorrhage. J Clin Neurosci. 2014;21(8):1364–1367. doi:10.1016/j.jocn.2013.11.030
11. Zhou Q, Zhang D, Chen X, et al. Plasma D-dimer predicts poor outcome and mortality after spontaneous intracerebral hemorrhage. Brain Behav. 2021;11(1):462–468. doi:10.1002/brb3.1946
12. Hanley DF. Intraventricular hemorrhage: severity factor and treatment target in spontaneous intracerebral hemorrhage. Stroke. 2009;40(4):1533–1538. doi:10.1161/STROKEAHA.108.535419
13. Witsch J, Roh DJ, Avadhani R, et al. Association between intraventricular alteplase use and parenchymal hematoma volume in patients with spontaneous intracerebral hemorrhage and intraventricular hemorrhage. JAMA Netw Open. 2021;4(12):e2135773. doi:10.1001/jamanetworkopen.2021.35773
14. Wilkinson DA, Pandey AS, Thompson BG, Keep RF, Hua Y, Xi G. Injury mechanisms in acute intracerebral hemorrhage. Neuropharmacology. 2018;134:240–248. doi:10.1016/j.neuropharm.2017.09.033
15. Garton T, Hua Y, Xiang J, Xi G, Keep RF. Challenges for intraventricular hemorrhage research and emerging therapeutic targets. Expert Opin Ther Targets. 2017;21(12):1111–1122. doi:10.1080/14728222.2017.1397628
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.