Back to Journals » Risk Management and Healthcare Policy » Volume 18
High-Flow Nasal Oxygen Prolongs Safe Apnea Time in Obstructive Sleep Apnea Patients Undergoing General Anesthesia: A Randomized Controlled Trial
Authors Lei G, Yang S, Wu L, Yin Y, Xi C, Yang Q, Wang G ![]()
Received 18 January 2025
Accepted for publication 8 July 2025
Published 22 July 2025 Volume 2025:18 Pages 2469—2477
DOI https://doi.org/10.2147/RMHP.S518271
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Haiyan Qu
Guiyu Lei,1 Siliu Yang,2 Lili Wu,1 Yue Yin,1 Chunhua Xi,1 Qingwen Yang,3 Guyan Wang1
1Department of Anesthesiology, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Anesthesiology, Beijing Dongcheng Maternal and Child Health Care Hospital, Beijing, People’s Republic of China; 3Department of Otolaryngology Head and Neck Surgery, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Guyan Wang, Department of Anesthesiology, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China, Email [email protected]
Background: Patients with obstructive sleep apnea (OSA) are at high risk for rapid oxygen desaturation during anesthesia induction. Apneic oxygenation with high-flow nasal oxygen (HFNO) has proven effective in prolonging safe apnea time in various patient populations. However, evidence for the efficacy of HFNO in OSA patients remains limited. This study aimed to evaluate whether the use of HFNO during anesthesia induction in OSA patients prolongs safe apnea time.
Methods: In this prospective randomized clinical trial, all participants underwent standardized pre-oxygenation and anesthesia induction. During the apneic period, oxygen was delivered either via HFNO at 60L/min (HFNO group) or with the nasal cannula left in place but disconnected from the oxygen source (control group, no supplemental oxygen). The primary outcome of this study was the time to peripheral oxygen desaturation (SpO2 < 95%) during apneic oxygenation. Secondary outcomes included minimum SpO2, re-oxygenation time, and tcCO2 levels.
Results: The HFNO group demonstrated a significantly prolonged safe apnea time compared to the Control group (18.1 [12.1,18.8] vs 4.2 [2.5,6.3] minutes; p < 0.001). Additionally, minimum SpO2 levels were higher, and re-oxygenation time was shorter in the HFNO group (p < 0.001 for both). Kaplan-Meier survival analysis revealed a substantially reduced risk of desaturation in the HFNO group (hazard ratio: 0.071; 95% CI, 0.021– 0.222; p < 0.001). No serious adverse events were reported.
Conclusion: In this randomized controlled trial, HFNO significantly prolongs safe apnea time and enhances oxygenation during anesthesia induction in OSA patients. These findings highlight the potential of HFNO to improve perioperative airway management and patient safety in this high-risk population.
Keywords: HFNO, OSA, apnea time, difficult airway management, anesthesia induction
Introduction
Difficult airway management remains a persistent challenge in the operating room, particularly in patients with obstructive sleep apnea (OSA), a well-recognized independent risk factor for difficult intubation, difficult mask ventilation, or a combination of both.1–3 Moderate to severe OSA patients face a 3-to 4-fold increased risk of difficult intubation, with approximately 1 in 7 (14.5%) severe OSA patients encountering intubation challenges.4–6 Physiologically, OSA patients exhibit reduced functional residual capacity and increased oxygen consumption, leading to rapid oxygen desaturation during anesthesia induction.7,8 These risks are further compounded by anatomically features such as restrictive cervico-maxillo-mandibular enclosure anatomy, crowded collapsible pharyngeal space, increased oropharyngeal soft tissue. The combination of difficult mask ventilation and rapid desaturation significantly heightens the likelihood of a “cannot intubate, cannot ventilate” scenario, which can result in severe hypoxia, anoxic brain injury, or even mortality. This underscores the critical importance of employing strategies to optimize oxygenation and extend safe apneic time, ensuring sufficient opportunity to secure the airway and achieve a safe and effective intubation process.9,10
Oxygenation with high-flow nasal oxygen (HFNO) has gained popularity within anesthetic practice for its ability to enhance safety in apneic patients since its introduction by Patel and Nouraei in 2015.11 Studies on HFNO in obese patients, who, like OSA patients, belong to high-risk populations, have demonstrated its potential to significantly extend safe apnea time,12–14 offering promise for its application in other challenging patients groups, such as OSA. However, despite those encouraging findings, there is currently no empirical evidence assessing the efficacy of HFNO in OSA patients. Randomized clinical trials evaluating the role of HFNO in OSA patients remain scarce, particularly within the specific perioperative settings which may have the greatest impact.
To date, no randomized controlled trial has evaluated HFNO in OSA patients during anesthesia induction-a phase in which these high-risk patients are particularly prone to rapid desaturation. Addressing this gap, we conducted a single-center randomized controlled study to determine whether HFNO can significantly extend safe apnea time in OSA patients, thereby improving perioperative airway management and patient safety.
Methods
Trial Design and Participants
This single-center, prospective, randomized trial was conducted in the Department of Anesthesiology at Beijing Tongren Hospital in China between April 2022 and July 2024. This study was approved by the Ethics Committee of Tongren Hospital (NO. TREC2021-KY099) and was registered in the Chinese Trials registry (https://www.chictr.org.cn/showproj.html?proj=132805) prior to patient enrollment. Written informed consent was obtained from all participants before enrollment. This study adhered to Declaration of Helsinki principles.
Eligible participants were recruited at a national key otorhinolaryngology clinical center. Participants were included if they were> 18yr of age, American society of anesthesiologists (ASA) physical status of I–III, be diagnosed with OSA, and undergoing elective modified uvulopalatopharyngoplasty. Exclusion criteria included: (1) chronic respiratory diseases; (2) oxygen saturation below 98% while on supplemental oxygen; (3) anticipated difficulty with intubation; (4) uncontrolled hypertension; (5) ischemic cardiomyopathy; (6) congestive heart failure; (7) increased intracranial pressure; (8) uncontrolled gastroesophageal reflux disease; (9) known allergy to anesthetics; or (10) inability to use high-flow devices due to nasopharyngeal blockage.
Participants were randomized into two groups: HFNO (HFNO using Optiflow THRIVETM) or Control (no oxygen delivery). Block randomization with a 1:1 ratio was performed using a computer-generated sequence generation and sealed opaque envelopes.
Preoxygenation for both groups was provided via a face mask with an FiO2 of 1.0 at 10 L/min, with the patient positioned in a 30-degree ramped position. Before induction, tracheostomy trays, cricothyroidotomy equipment, and resuscitation resources were prepared in the operating room. An experienced laryngologist was standby in case of failed intubation or the complete obstruction during induction. One senior anesthetists and an assistant were present throughout the procedure. Anesthesia induction included using opioid, propofol, and rocuronium, with doses selected by the anesthetist, and maintained with intravenous infusions of propofol and remifentanil to maintain a BIS range of 40–60. Systolic blood pressure was maintained within 20% of baseline values. Manual bag-mask ventilation was performed with PEEP adjusted as needed by the anesthetist. Laryngoscopy was conducted using a CMAC videolaryngoscope, with Cormack-Lehane laryngoscopy grades recorded. Patients with difficulty in manual ventilation or a Grade 3 or 4 laryngoscopy view were excluded at this stage. Following successful ventilation, the videolaryngoscope was removed, and the patient was manually ventilated until an end-tidal oxygen level of 90% was achieved. Nasal oxygen therapy was then applied based on group assignment. An oropharyngeal airway was employed to optimize airway patency until the study endpoint was reached.
Intervention
Participants in the HFNO group received oxygen via the Optiflow THRIVE TM system, with settings of 60 L/min flow rate, 100% inspired oxygen fraction, and a temperature of 37°C (Optiflow; Fisher & Paykel Healthcare, Auck- land, New Zealand). Participants in the Control group wore the nasal cannula of the Optiflow THRIVE TM system with identical device settings (flow rate: 60L / min, FiO2:100%, temperature: 37°C). However, the oxygen supply tubing was disconnected at the connection point between the oxygen source and the nasal cannula, ensuring no oxygen delivery.
Outcomes
The primary outcome was safe apnea time, defined as the interval from the cessation of mechanical ventilation (start of apnea) until peripheral oxygen saturation (SpO2) first falls below 95%, or, if desaturation does not occur, until the 18-minute observation limit is reached. The patient remained anesthetized and apneic until one of the following occurred: (1) SpO2 dropped to 95%, (2) tcCO2 exceeded 80 mmHg, (3) arrhythmias or other complications arose, or (4) the maximum observation time of 18 minutes was reached. When the endpoint was reached, the nasal cannula was removed, and the patient was manually bag-mask ventilated until SpO2 reached 98%, followed by intubation performed by attending anesthetists with more than 5 years of airway experience.
Statistical Analysis
The study was powered for the primary outcome. There are few data recommending a certain apnea time in OSA patients under general anesthesia induction. Sample size estimation was based on preliminary data and survival analysis. Using data from a prior study, apnea durations of 261 and 185 seconds were estimated for the HFNO and Control groups, respectively, with an SD of 77 seconds.14 Type I and type II errors of 5% and 20% were used, yielding an estimated sample size of 36 (18 per group). To account for dropout rates, the sample size was increased by 22%, requiring 44 participants. Survival analysis estimated a failure rate of 90% in the Control group and 12% in the HFNO group at 18 minutes.13,15 Adjusted calculations confirmed a total sample size of 44 (Log rank test, Freedman method).
The Shapiro–Wilk test was used to assess the normality of continuous variables. Group characteristics were summarized with means and standard deviations (SD) for normally distributed variables and medians with interquartile ranges (IQR) or 95% confidence intervals (CI) for skewed distributions. Kaplan-Meier curves were used to represent time to desaturation, with comparisons made using the Log rank test. Continuous variables were analyzed with independent t-tests or Mann–Whitney U-tests as appropriate. Among participants desaturating within 18-minute, the Mann–Whitney U-test compared time to desaturation between groups. With statistical significance defined as a two-tailed p-value < 0.05. Data were analyzed using SPSS version 28.
Results
Sixty-three participants were assessed for eligibility, and 44 patients were recruited, randomized, and enrolled in the study. One patient developed anaphylactic shock during induction and was excluded from the analysis. A total of 43 patients were included in the final analysis, with 22 in the HFNO group and 21 in the control group. All participants completed the study (Figure 1). No serious adverse events were reported.
 |
Figure 1 Study flow diagram. Enrollment, randomization, and follow-up of all participants. Abbreviations: HFNO, high-flow nasal oxygen. |
The patient characteristics were comparable between the two groups (Table 1). The study was conducted in a population with obstructive sleep apnea, there was a greater percentage of participants were male (79.1%), due to the sex differences and gender bias in OSA. Men are more likely to present with typical symptoms that align with diagnostic criteria. The majority of patients (90.7%) were diagnosed with moderate or severe OSA, and more than half (55.8%) experienced severe hypoxemia.
 |
Table 1 Subject Characteristics |
The primary and secondary outcomes are summarized in Table 2. Median safe apnea time was 18.1 min [12.1–18.8] in the HFNO group versus 4.2 min [2.5–6.3] in the control group (P< 0.001), although interpretability is limited by heavy right censoring, as nearly half of the HFNO group did not desaturate within 18 minutes. Among the 30 patients who desaturated, time to desaturation was significantly longer in the HFNO group (mean=10.9; SD=4.6 min; n=9) compared to the control group (mean=4.5; SD=2.7 min; n=21), and was statistically significant (independent t test P= 0.009).
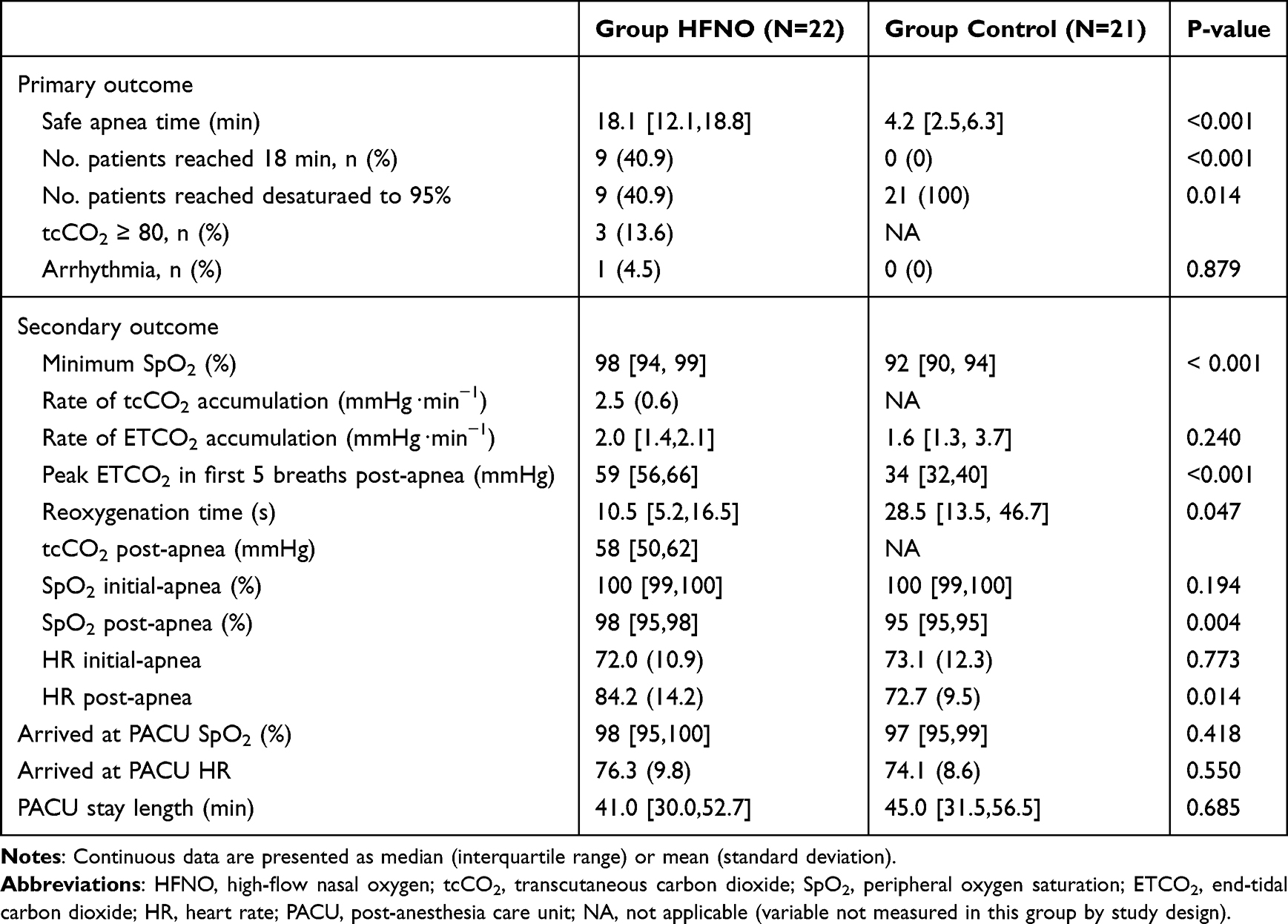 |
Table 2 Primary and Secondary Outcomes |
The Kaplan-Meier survival curves for each group are shown in Figure 2. All (100%) in the control group and 9 patients (40.9%) in the HFNO group desaturated to an SpO2 of 95% within 18 min of apnea. The risk of desaturation was significantly lower in the HFNO group compared to the control group (hazard ratio=0.071; 95% CI, 0.021–0.222; Log rank test P < 0.001).
 |
Figure 2 Kaplan-Meier curve of time to SpO2≤95% for the two study groups. Group HFNO (green line) and Group Control (purple). Hazard ratio comparing Control and HFNO groups, 0.071 (95% confidence interval, 0.021–0.222; log-rank P< 0.001). Number at risk represents number of patients yet to reach SpO2≤95% at a time point of every 2 minutes from the beginning of apnea to a maximum of 18 minutes. Abbreviations: HFNO, high-flow nasal oxygen; SpO2, peripheral oxygen saturation. |
The mean (SD) CO2 accumulation was similar between the two groups (Table 2). The median minimum SpO2 was significantly higher in the HFNO group (Mann–Whitney-U test, P< 0.001), and the median re-oxygenation time was significantly shorter in the HFNO group (Mann–Whitney-U test, P= 0.047).
Discussion
Our results suggest a clear effect of HFNO administered at 60L/min in extending safe apnea time and improving perioperative oxygenation in paralyzed OSA patients. To the author’s knowledge, based on the literature, this presents the first randomized controlled trial examining HFNO as apneic oxygenation in OSA patients during anesthesia induction. The findings contribute significantly to the limited available evidence on this topic, addressing a critical gap in airway management for this high-risk patient group.
HFNO has previously been shown to prolong apnea duration in obese patients, a population at high risk group for difficult airway management.12,14,16–19 Our results extend these findings by demonstrating that HFNO significantly increases safe apnea time in OSA patients, who, beyond sharing reduced functional residual capacity and rapid desaturation risk, also contend with pharyngeal narrowing, soft-tissue collapsibility, and airway collapse under muscle relaxation.1,5,20–22 There distinctions underscore the need for OSA-specific investigations, since evidence derived solely from obese cohorts may not capture the full spectrum of airway dynamics in OSA. By prolonging safe apnea time, HFNO enables uninterrupted intubation even during prolonged procedures and alleviates the pressure on anesthesiologists to achieve rapid intubation by preventing desaturation in anticipated difficult airways. Furthermore, HFNO mitigates the risk of catastrophic outcomes, particularly in challenging airway scenarios such as “cannot intubate, cannot ventilate” situations, thereby enhancing patient safety and providing clinicians with critical time for effective airway management.
In our study, 9 of 22 HFNO recipients (40.9%) maintained stable oxygenation throughout the 18-minute observation period. This proportion is lower than the 88% observed by Schutzer-Weissmann et al’s in obese patients under identical HFNO settings.13 While differences in patient positioning (45°incline versus our 30°ramp) may partially account for this discrepancy, the dominant factor is likely the unique anatomical limitations in OSA, exacerbated by anesthetic muscle relaxation.
Importantly, over 90% of HFNO patients sustained safe oxygenation for at least 10 minutes, a duration sufficient for securing the airway in most clinical scenarios. Conversely, 76% of controls desaturated within 6 minutes, a rate similar to that reported by Guy et al despite their use of 4L/min supplemental oxygen.12 However, our control group did not receive supplemental oxygen, as we aimed to simulate real clinical scenarios where oxygenation is typically paused during intubation. This differs from previous studies,12,13,15,23,24 where face mask is provided, which is impractical during actual intubation. Our results shows the safe apnea time in OSA patients without oxygenation during apnea was 4.2 minutes, which was comparable or litter shorter than that observed in obese patients in former study.14,15 Notably, the BMI of patients in our study was not high, whereas patients in those studies had a higher BMI greater than 40.
In this study, the rate of increase of carbon dioxide was not directly measured to avoid the risks associated with invasive arterial blood gas analysis. Instead, we monitored tcCO2 in the HFNO arm as a safety threshold, terminating observations at 80 mmHg. In the control arm, apneic intervals were too brief for tcCO2 to stabilize or reliably track PaCO2.25 Even if PaCO2 rose by 10 mmHg in the first minute,26 subsequent accumulation is only ~2 mmHg·min−1,27,28 precluding control patients from ever reaching the 70 mmHg safety limit within the observation window. Thus, tcCO2 monitoring could not have provided actionable data in controls and was reserved for the HFNO arm. Emerging AI-driven predictive models may soon enable noninvasive estimation of PaCO2 trends, further enhancing perioperative safety.29
Although the rate of increase in ETCO2 in our study was similar between groups, previous research has demonstrated significant discrepancies between PaCO2 and ETCO2 levels, indicating that ETCO2 is an unreliable indicator of CO2 accumulation following apnea.12 Riva et al27 reported a consistent PaCO2 increase rate of approximately 2 Hg min−1 across various flow rates (0.25–70Lmin−1), comparable to 2.2 Hg min−1 in obese patients.12,13,30 Similarly, Schutzer’s study found no significant difference in PaCO2 increase between HFNO and face mask groups,13 reinforcing that the oxygenation method does not effect CO2 accumulation during apnea. Based on the widely accepted rate of 2 mmHg min−1,27,28 the preset 18-minute apnea time in our study was considered safe.
Limitations of the study include the following. First, it was a small single-center study with a larger proportion of male participants, so results may not be generalizable. Second, arterial blood gas was not analyzed in our study, as it is not a routine measurement taking during surgery and could increase the risk to the risk due to invasive manipulation, carbon dioxide accumulation was unable to be clarified in this study.
In conclusion, apneic oxygenation with HFNO at 60L/min significantly increases safe apnea time and reduces the risk of desaturation in OSA patients during general anesthesia induction. These findings suggest that HFNO is a promising approach to enhance OSA patient safety, further research is needed to confirm its efficacy and guide clinical recommendations.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article or are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Beijing Hospitals Authority Clinical Medicine Development of Special Funding Support (No. ZYLX202103) & Beijing Hospitals Authority’s Ascent Plan (No. DFL20220203). The present study was registered at the Chinese Trials registry (ChiCTR2100050517).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sato S, Hasegawa M, Okuyama M, et al. Mask ventilation during induction of general anesthesia: influences of obstructive sleep apnea. Anesthesiology. 2017;126(1):28–38. doi:10.1097/ALN.0000000000001407
2. Cook TM. Strategies for the prevention of airway complications - a narrative review. Anaesthesia. 2018;73(1):93–111. doi:10.1111/anae.14123
3. Leong SM, Tiwari A, Chung F, et al. Obstructive sleep apnea as a risk factor associated with difficult airway management - A narrative review. J Clin Anesth. 2018;45:63–68. doi:10.1016/j.jclinane.2017.12.024
4. Seet E, Chung F, Wang CY, et al. Association of obstructive sleep apnea with difficult intubation: prospective multicenter observational cohort study. Anesth Analg. 2021;133(1):196–204. doi:10.1213/ANE.0000000000005479
5. Memtsoudis SG, Cozowicz C, Nagappa M, et al. Society of anesthesia and sleep medicine guideline on intraoperative management of adult patients with obstructive sleep apnea. Anesth Analg. 2018;127(4):967–987. doi:10.1213/ANE.0000000000003434
6. Barajas van Langen ME, Meesters MI, Hiensch RJ, et al. Perioperative management of obstructive sleep apnoea: limitations of current guidelines. Br J Anaesth. 2023;131(4):e133–e134. doi:10.1016/j.bja.2023.07.011
7. Seet E, Nagappa M, Wong DT. Airway management in surgical patients with obstructive sleep apnea. Anesth Analg. 2021;132(5):1321–1327. doi:10.1213/ANE.0000000000005298
8. Lv R, Liu X, Zhang Y, et al. Pathophysiological mechanisms and therapeutic approaches in obstructive sleep apnea syndrome. Signal Transduct Target Ther. 2023;8(1):218.
9. Chung SA, Yuan H, Chung F. A systemic review of obstructive sleep apnea and its implications for anesthesiologists. Anesth Analg. 2008;107(5):1543–1563. doi:10.1213/ane.0b013e318187c83a
10. Heard A, Toner AJ, Evans JR, et al. Apneic oxygenation during prolonged laryngoscopy in obese patients: a randomized, controlled trial of buccal RAE tube oxygen administration. Anesth Analg. 2017;124(4):1162–1167. doi:10.1213/ANE.0000000000001564
11. Patel A, Nouraei SA. Transnasal humidified rapid-insufflation ventilatory exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways. Anaesthesia. 2015;70(3):323–329. doi:10.1111/anae.12923
12. Guy L, Christensen R, Dodd B, et al. The effect of transnasal humidified rapid-insufflation ventilator exchange (THRIVE) versus nasal prongs on safe apnoea time in paralysed obese patients: a randomised controlled trial. Br J Anaesth. 2022;128(2):375–381. doi:10.1016/j.bja.2021.10.048
13. Schutzer-Weissmann J, Wojcikiewicz T, Karmali A, et al. Apnoeic oxygenation in morbid obesity: a randomised controlled trial comparing facemask and high-flow nasal oxygen delivery. Br J Anaesth. 2023;130(1):103–110. doi:10.1016/j.bja.2021.12.011
14. Wong DT, Dallaire A, Singh KP, et al. High-flow nasal oxygen improves safe apnea time in morbidly obese patients undergoing general anesthesia. Anesthesia Analg. 2019;129(4):1130–1136. doi:10.1213/ANE.0000000000003966
15. Pierpoint SA, Burke JL. Comparing nasopharyngeal apnoeic oxygenation at 18 l/min to preoxygenation alone in obese patients - A randomised controlled study. J Clin Anesth. 2023;88:111126. doi:10.1016/j.jclinane.2023.111126
16. Hamp T, Prager G, Baron-Stefaniak J, et al. Duration of safe apnea in patients with morbid obesity during passive oxygenation using high-flow nasal insufflation versus regular flow nasal insufflation, a randomized trial. SurgObesRelatDis. 2021;17:347–355.
17. Vourc’h M, Baud G, Feuillet F, et al. High-flow nasal cannulae versus non-invasive ventilation for preoxygenation of obese patients: the PREOPTIPOP randomized trial. EClinicalMedicine. 2019;13:112–119. doi:10.1016/j.eclinm.2019.05.014
18. Jaber S, De Jong A, Schaefer MS, et al. Preoxygenation with standard facemask combining apnoeic oxygenation using high flow nasal cannula versuss standard facemask alone in patients with and without obesity: the OPTIMASK international study. Ann Intensive Care. 2023;13(1):26. doi:10.1186/s13613-023-01124-x
19. Rodriguez M, Ragot S, Coudroy R, et al. Noninvasive ventilation vs. high-flow nasal cannula oxygen for preoxygenation before intubation in patients with obesity: a post hoc analysis of a randomized controlled trial. Ann Intensive Care. 2021;11(1):114. doi:10.1186/s13613-021-00892-8
20. Ceban F, Yan E, Pivetta B, et al. Perioperative adverse events in adult patients with obstructive sleep apnea undergoing ambulatory surgery: an updated systematic review and meta-analysis. J Clin Anesth. 2024;96:111464. doi:10.1016/j.jclinane.2024.111464
21. Cukierman DS, Perez M, Guerra-Londono JJ, et al. Nasal continuous positive pressure versus simple face mask oxygenation for adult obese and obstructive sleep apnea patients undergoing colonoscopy under propofol-based general anesthesia without tracheal intubation: a randomized controlled trial. J Clin Anesth. 2023;89:111196. doi:10.1016/j.jclinane.2023.111196
22. Subramani Y, Singh M, Wong J, et al. Understanding phenotypes of obstructive sleep apnea: applications in anesthesia, surgery, and perioperative medicine. Anesth Analg. 2017;124(1):179–191. doi:10.1213/ANE.0000000000001546
23. Bright MR, Harley WA, Velli G, et al. High-flow nasal cannula for apneic oxygenation in obese patients for elective surgery: a systematic review and meta-analysis. Anesth Analg. 2023;136(3):483–493. doi:10.1213/ANE.0000000000006304
24. Rosen J, Frykholm P, Fors D. High-flow nasal cannula versus face mask for preoxygenation in obese patients: a randomised controlled trial. Acta anaesthesiologica Scandinavica. 2021;65(10):1381–1389. doi:10.1111/aas.13960
25. Eley VA, Guy L, Woods C, et al. Transcutaneous carbon dioxide measurements in anesthetized apneic patients with BMI > 35 kg/m2. J Anesth. 2023;37(6):971–975. doi:10.1007/s00540-023-03263-8
26. Cook TM, Wolf AR, Henderson AJ. Changes in blood-gas tensions during apnoeic oxygenation in paediatric patients. Br J Anaesth. 1998;81(3):338–342. doi:10.1093/bja/81.3.338
27. Riva T, Greif R, Kaiser H, et al. Carbon dioxide changes during high-flow nasal oxygenation in apneic patients: a single-center randomized controlled noninferiority trial. Anesthesiology. 2022;136(1):82–92. doi:10.1097/ALN.0000000000004025
28. Lyons JM, Young O. The effect of high‐flow nasal oxygen flow rate on gas exchange in apnoeic patients. Anesthesia. 2023. doi:10.1111/anae.16200
29. Mira FA, Favier V, Dos Santos Sobreira Nunes H, et al. Chat GPT for the management of obstructive sleep apnea: do we have a polar star? Eur Arch Oto-Rhino-Laryngol. 2024;281(4):2087–2093. doi:10.1007/s00405-023-08270-9
30. Piosik ZM, Dirks J, Rasmussen LS, et al. Exploring the limits of prolonged apnoea with high-flow nasal oxygen: an observational study. Anaesthesia. 2021;76(6):798–804. doi:10.1111/anae.15277
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.