Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
High-Flow Nasal Cannula Oxygen Therapy in Perioperative Respiratory Care: Application and Prospects
Authors Chen J ![]() , Hu X, Han D, Liu Y, Chen D, Chen S
, Hu X, Han D, Liu Y, Chen D, Chen S ![]() , Chen Y
, Chen Y ![]() , Wu J
, Wu J ![]()
Received 25 October 2025
Accepted for publication 8 January 2026
Published 22 January 2026 Volume 2026:19 576767
DOI https://doi.org/10.2147/JMDH.S576767
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Jing Chen, Xinyue Hu, Dong Han, Yuwei Liu, Danqi Chen, Shuangyun Chen, Yuwei Chen, Jing Wu
Department of Anesthesiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Hubei Province, Wuhan, People’s Republic of China
Correspondence: Jing Wu, Department of Anesthesiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Hubei Province, Wuhan, People’s Republic of China, Tel +86 27 13995650750, Fax +86 27 85351618, Email [email protected]
Abstract: High-flow nasal cannula (HFNC) oxygen therapy is an oxygen delivery technique that provides warmed and humidified high-flow oxygen through a non-sealing nasal cannula. With multiple physiological advantages, HFNC had been increasingly used in perioperative respiratory management. Evidence indicates that HFNC significantly reduces the incidence of hypoxemia and decreases procedural interruptions during procedural sedation. As an updated HFNC technique, transnasal humidified rapid-insufflation ventilatory exchange (THRIVE) had been proved to extend the safe apneic time and promote safety during laryngoscopic examination and endotracheal intubation. In tubeless pharyngeal surgery, it effectively balances the dilemma between a clear surgical field and adequate intraoperative oxygenation. In the postoperative recovery period, HFNC helps to reduce the incidence of postoperative hypoxemia and other postoperative pulmonary complications, and decreases the need for reintubation. HFNC demonstrates broad potential in perioperative respiratory care. However, current evidence is limited by the heterogeneity of oxygen protocols and inconsistent results among studies, especially for high-risk patients. The efficacy of HFNC is difficult to predict, which may lead to intubation delay and limits the application of HFNC. Future research should focus on optimizing clinical application strategies for HFNC, developing reliable efficacy prediction models, and validating these findings through large-sample, multicenter randomized controlled trials to advance perioperative respiratory management toward greater effectiveness and safety.
Keywords: oxygen therapy, hypoxemia, airway management, intubation, anesthesia
Introduction
High-flow nasal cannula (HFNC) oxygen therapy is a non-invasive respiratory support method which continuously supplies warmed and humidified oxygen at high flow via a non-sealing nasal cannula.1 Before delivery, the gas is conditioned to ensure a constant inspired oxygen concentration (FiO2) (21–100%), stable temperature (31–37°C), near-saturated humidity (approximately 100% relative humidity), and high flow rates (up to 80 L/min or higher). HFNC was initially used as an adjunctive oxygen therapy for patients with respiratory failure2 or bronchitis,3 and subsequently applied to patients with mechanical ventilation, demonstrating effective oxygenation support during endotracheal intubation1 and post-extubation sequential treatment.4
In perioperative respiratory management, however, there remains an unmet need for a technique that provides reliable oxygenation without compromising procedures or patient comfort. Standard nasal cannulas, which are frequently employed during procedural sedation and postoperative recovery, are often constrained by their upper limits of oxygen fraction and flow, posing risks of hypoxemia and other complications for patients.5 While facemasks or non-invasive ventilation (NIV) can achieve better oxygenation, they are often unsuitable for concurrent use during gastroscopic laryngoscopy or tracheal intubation. In addition, tight facemasks bring issues such as poor patient tolerance, skin injury, impaired communication, and hindered airway secretion clearance.6 HFNC could overcome these limitations and provide effective oxygenation at the same time. Besides, its unique capacity for effective apneic oxygenation allows its application during laryngoscopy, tracheal intubation, and even brief tubeless laryngopharyngeal surgery, ensuring effective oxygenation without interrupting the procedure.7,8 HFNC has thus emerged as a promising solution for perioperative respiratory management.
Recently, the applications of HFNC have rapidly expanded into various perioperative scenarios. Moreover, recent high-quality multicenter trials have further elucidated its efficacy in these settings.9–11 This ongoing expansion, coupled with the publication of new evidence9,12 and evolving indications, necessitates an updated synthesis of current knowledge to guide clinical practice. Therefore, this study aims to summarize the current evidence regarding the perioperative clinical applications of HFNC technology, providing a reference for decision making regarding oxygen therapy strategies.
Physiological Advantages of HFNC
The physiological benefits of HFNC are primarily mediated by two core mechanisms: the continuous flushing effect of high-flow gas and the generation of positive end-expiratory pressure (PEEP) (Figure 1). The high-flow gas delivered by HFNC continuously flushes the nasopharyngeal space, reducing the rebreathing of exhaled gas, stabilizing the FiO2, and diminishing anatomical dead space.13 This flushing action exhibits flow-dependent efficacy, with airway dead space clearance increasing by approximately 1.8 mL/s for every 1 L/min rise in flow rate.14 The reduction in anatomical dead space enhances alveolar effective ventilation, improves ventilation–perfusion matching, and increases respiratory efficiency. Furthermore, the flushing effect of high-flow gas reduces airway resistance, enhances lung dynamic compliance, and decreases the breathing work.13,15 In patients with acute hypoxic respiratory failure, those treated with HFNC exhibited a lower respiratory rate compared with mask oxygen therapy, at equivalent levels of arterial carbon dioxide pressure (PaCO2) and pH.15
 |
Figure 1 Physiological benefits of high-flow nasal cannula oxygen therapy. (A) Warmed and humidified gas enhances mucociliary clearance, facilitates the removal of respiratory secretions, and improves patient comfort. (B) Reduction of anatomical dead space and increase of inspired oxygen fraction through continuous flushing of the nasopharyngeal space. (C) Generation of positive end-expiratory pressure by constant high-flow gas. In (B), the box outlines the alveolar region. The black arrows indicate the direction of gas exchange (oxygen, carbon dioxide). White arrows represent the direction of blood flow. Capillary color denotes blood oxygen content (dark blue: low; red: high). Blue areas in the alveoli and upper airway represent alveolar air and the fresh gas delivered by HFNC, respectively. The blue-covered area in the upper airway indicates regions of CO2 washout by HFNC fresh gas. Abbreviations: COT, conventional oxygen therapy; HFNC, high-flow nasal cannula. |
The constant high-flow gas delivered by HFNC generates PEEP, which attenuates the pressure gradient between capillary hydrostatic pressure and alveolar pressure,16,17 thereby promoting alveolar recruitment, increasing end-expiratory lung volume, and mitigating atelectasis and hypoxemia.13 The magnitude of PEEP produced by HFNC is influenced by several factors, including the patients’ age and gender, and the mouth being closed or open during therapy.17 Measurements in healthy volunteers indicated that for every 10 L/min increase in flow rate, the generated PEEP rose by approximately 1.16 cmH2O.16 However, some studies have noted that while PEEP increased in a flow-dependent manner, this relationship was not strictly linear, with higher flow rates producing disproportionately greater increases in airway pressure.17
Moreover, the adequately warmed and humidified oxygen supplied by HFNC enhances mucociliary clearance function, and facilitates the removal of respiratory secretions.18 At the same time, it helps to improve patient comfort and decrease airway resistance.
Application of HFNC During Procedural Sedation
In recent years, more than 50% of gastrointestinal endoscopic procedures have been performed under sedation.19 Sedatives are administered to alleviate patient discomfort and intolerance, improving patients’ satisfaction and facilitating operational conditions. However, these agents carry risks of respiratory depression and subsequent hypoxemia,20 which represent the most frequent adverse events during procedural sedation, with reported incidence rates ranging from 1.8% to 69%.20–22 Severe hypoxemia may lead to arrhythmias, myocardial ischemia,21 permanent neurological injury, and death.23 Therefore, hypoxemia during procedural sedation often requires immediate airway interventions, including mask ventilation, jaw thrust, and endotracheal intubation, which often interrupt the procedure. Conventional oxygen therapy (COT) employed during gastrointestinal endoscopy uses standard nasal cannulas, which are limited by poor sealing and low maximum flow rates, resulting in entrainment of room air and reduced inspiratory oxygen fraction. HFNC overcomes these limitations and provides gas with a constant oxygen fraction, which helps to maintain pulse oximetry during gastrointestinal endoscopy (Table 1). Clinical studies have demonstrated that compared with COT, the application of HFNC significantly reduces the overall incidence of hypoxemia and the need for airway interventions during gastroscopy under sedation.9,10,24 This efficacy had also been validated in obese patients, with HFNC markedly reducing the incidence of hypoxia, subclinical respiratory depression, and severe hypoxemia, thereby minimizing procedural interruptions and airway interventions.9 The beneficial effects of HFNC during procedural sedation can be primarily attributed to the high-flow gas, which facilitates continuous flushing of dead space and generates PEEP, improving oxygenation efficiency. A multicenter randomized controlled trial (RCT) confirmed that, even at comparable FiO2, HFNC during procedural sedation for gastroscopy significantly reduced episodes of desaturation by 20% compared with standard oxygen therapy.10 Nevertheless, it is appropriate to moderately increase the FiO2 for high-risk populations. A small-sample trial applied HFNC with FiO2 of 36–40% in morbidly obese patients and observed no differences in desaturation compared with the COT group.25 During esophagogastroduodenoscopy, mouth opening was often required. Studies indicated that nasal breathing decreased to approximately 47%, and patients would switch to oral breathing during gastrointestinal endoscopy.26 This may lead to leakage of high-flow gas, potentially attenuating the oxygenation efficacy of HFNC. Nevertheless, subgroup analyses from current RCTs have not identified a statistically significant influence of endoscopic type on the overall effectiveness of HFNC oxygen therapy.10
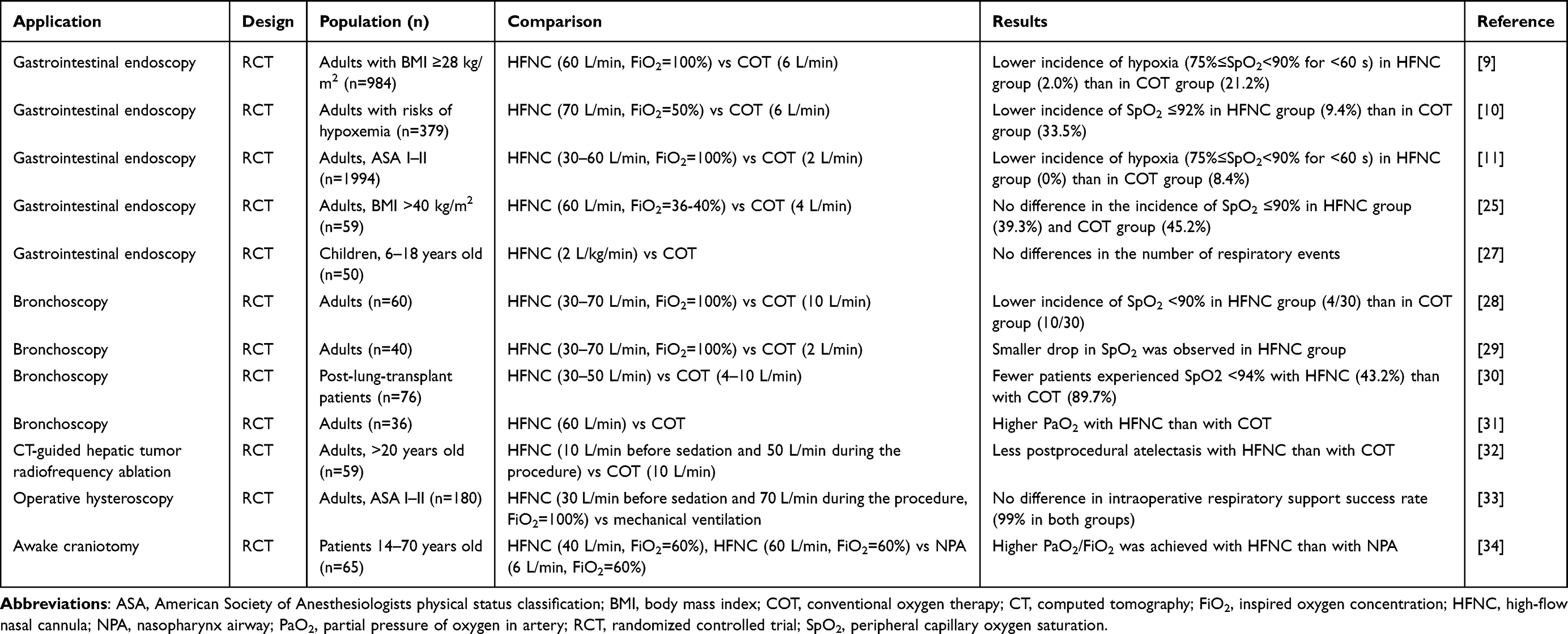 |
Table 1 Summary of Current Trials Evaluating HFNC in Procedural Sedation |
Owing to the characteristic of “shared airway”, airway management in fiberoptic bronchoscopy or endobronchial ultrasound is very difficult. Hypoxemia is a common complication during fiberoptic bronchoscopy examination.35 If desaturation occurs, immediate airway interventions are necessary, which often involve interruption of the procedure and rescue ventilation. Prospective observational studies indicate that HFNC is an effective and safe therapy that can perform effective oxygenation during bronchoscopy.36 Multiple RCTs have demonstrated that HFNC can reduce the incidence of desaturation and hypoxemia,28–30 decrease the need for airway interventions,29 improve post-oxygenation saturation levels, and elevate the minimum intraoperative peripheral oxygen saturation (SpO2).28
HFNC technology can mitigate the loss of end-expiratory lung volume and improve the oxygenation effect.31 Compared with standard nasal cannula oxygen therapy, it has demonstrated better oxygenation effects in other clinical scenarios of procedural sedation, such as computed tomography-guided hepatic tumor radiofrequency ablation,32 operative hysteroscopy,33 and awake craniotomy.34 A meta-analysis summarized the practical data from both pediatric and adult patients across various clinical settings (such as digestive endoscopy, fiberoptic bronchoscopy, cardiovascular intervention surgery, and dentistry). It was concluded that HFNC consistently reduced the risk of hypoxemia, irrespective of the oxygen fraction, propofol administration, or baseline hypoxemia risk.5 Compared with COT, HFNC use was associated with fewer hypoxemic events, higher minimum SpO2, and less requirement for airway maneuvers and procedural interruptions.5 Therefore, for patients with high risks for intraoperative hypoxemia (such as those with comorbidities, obesity, or obstructive sleep apnea) or complex procedures, HFNC should be considered as a suitable oxygenation technique.
Applications of HFNC During Anesthesia Induction
Preoxygenation is often performed during anesthesia induction to improve patients’ oxygen reserves and prevent desaturation and hypoxemia during tracheal intubation. A conventional oxygen delivery device cannot ventilate during laryngoscopy and endotracheal intubation, which poses risks of desaturation, especially in patients with difficult airways. Transnasal humidified rapid-insufflation ventilatory exchange (THRIVE), proposed by Patel and Nouraei in 2015, is an upgraded technique of HFNC,37 which aims to facilitate apneic oxygenation through high flow and high FiO2. Figure 2 illustrates the mechanism of apneic oxygenation during THRIVE therapy. Patel and Nouraei conducted preoxygenation using THRIVE with a flow rate of 70 L/min, in the position of 40-degree head-up tilt angle, and observed an average safe apnea time of 17 minutes.37 No patients experienced oxygen saturation below 90% or hypercapnia. In the study, two patients used THRIVE throughout the entire surgical process, with safe apnea times of 32 minutes and 65 minutes. This finding showed that effective apneic oxygenation of THRIVE allowed it to ventilate during laryngoscopy, significantly extending the safe apnea time and providing more operating time for airway management in patients with difficult airways, thus improving the safety of anesthesia induction and airway management. Many studies have confirmed that THRIVE can significantly prolong safe apnea time (Table 2). The additional application of THRIVE during laryngoscopy prolonged the time when oxygen saturation was ≥95% and reduced the minimum pulse oxygen saturation during laryngoscopy.38 A prospective multicenter study independently evaluated the effectiveness of THRIVE technology in apneic oxygenation. Compared with preoxygenation using a facemask alone, patients who received a facemask combined with THRIVE showed a lower incidence of oxygen saturation decreasing to <95%.7 Applying THRIVE to the entire stage of preoxygenation (both spontaneous breathing and apneic oxygenation) significantly improved the safe apnea time and extended the safety margin of airway management. In an RCT published in 2023, THRIVE was proven to effectively reduce the risk of desaturation during anesthesia induction in obese individuals. Fourteen patients (14/39) in the mask group experienced a desaturation within 18 minutes, compared with only five patients (5/41) in the THRIVE group.39 THRIVE has achieved inspiring therapeutic results in various populations, including pediatric patients40 and patients with morbidly obesity,39,41 obstructive sleep apnea,42 critical illness,43,44 and head and neck cancer.45
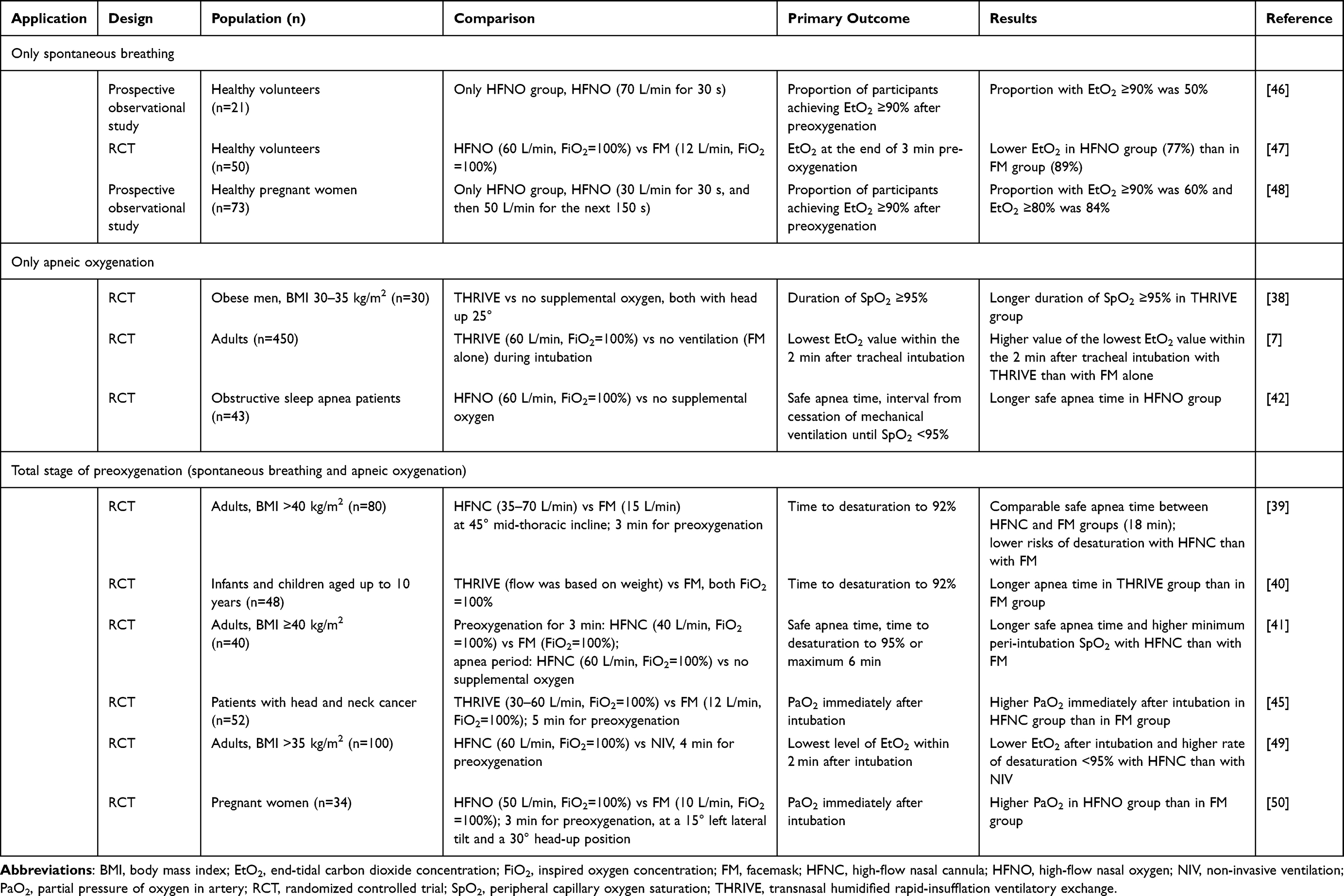 |
Table 2 Summary of Current Trials Evaluating HFNC in Anesthesia Induction |
 |
Figure 2 Mechanism of apneic oxygenation during transnasal humidified rapid-insufflation ventilatory exchange therapy. (A) The turbulent flow formed by high-flow gas in the nasopharyngeal cavity. (B) The interaction between cardiac oscillations and the turbulent flow facilitates the transport of carbon dioxide from the lungs to the nasal or oral cavity. (C) The negative pressure gradient generated by differential gas exchange rates facilitates gas diffusion during apneic oxygenation. In the figure, arrows indicate the direction of gas flow. Curved arrows and vortex symbols represent turbulence within the airway. The box outlines the alveolar region where differential gas exchange occurs. The thickness of the arrows represents the volume of gas participating in exchange process. Abbreviations: COT, conventional oxygen therapy; HFNC, high-flow nasal cannula. |
Nevertheless, the superiority of THRIVE over conventional facemasks remains contentious. Compared with conventional facemask, THRIVE offers the advantage of effective apneic oxygenation during endotracheal intubation; however, it is less efficient during spontaneous breathing. In an observational study, healthy volunteers received THRIVE treatment at a flow rate of 70 L/min and FiO2 of 100% with the mouth closed for 3 minutes, but only half of them achieved the target end-tidal oxygen concentration (EtO2) of 90%, with the median EtO2 being 86%.46 Similar results were observed in pregnant women.48 THRIVE could not quickly and effectively achieve the target EtO2 of 90% during spontaneous breathing. Besides, while some studies suggest that compared with conventional facemasks, THRIVE reduces the incidence of desaturation and improves the lowest SpO2 during intubation, these benefits are not always evident in other studies. The PREOPTI-DAM RCT, conducted at the University Hospital of Nantes in France, found that compared with NIV, preoxygenation with THRIVE in obese patients provided lower EtO2 after intubation and a higher rate of desaturation <95%.49 A meta-analysis involving 11 RCTs found that THRIVE was more effective than conventional mask therapy, but not as effective as NIV.51 The combination of THRIVE and NIV may be a more suitable choice for critically ill or complex patients. It is important to note that variations in control and intervention protocols – such as flow rates (30–70 L/min), preoxygenation duration (3–5 minutes), and patient positioning (supine to 45° head-up) – may influence outcomes. In addition, the threshold defining desaturation (90–95% SpO2) differs across studies, contributing to heterogeneous findings. Despite these discrepancies, THRIVE remains a promising technique for anesthesia induction. Optimal flow rates and positioning require further investigation. A meta-analysis compared nine different therapies (nine combinations of preoxygenation techniques and positions) and identified THRIVE with head elevation as the top-ranked therapy for prolonging safe apnea time.12 THRIVE remained the top-ranked oxygenation regimen even without the consideration of position. In terms of desaturation, although THRIVE was not superior to NIV it was better than non-pressure facemasks.12
There have been concerns regarding the potential risks of gastric insufflation and aspiration during THRIVE therapy in preoxygenation. However, according to relevant research, the PEEP generated by THRIVE, even at a flow rate of up to 80 L/min with the patient’s mouth closed, was still below 10 cmH2O.17 Given that the lower esophageal sphincter can form a pressure barrier of approximately 15–25 mmHg (20–34 cmH2O) under normal conditions to prevent the reflux of gastric contents,52 the PEEP generated by THRIVE seemed insufficient to induce gastric insufflation or aspiration. In healthy fasting awake adults, THRIVE treatment at a flow rate of up to 70 L/min for 30 minutes did not increase the cross-sectional area of the gastric antrum,53 which is considered as a reliable index for gastric content volume.54 No gastric insufflation was observed among 60 participants.53 However, sedatives and neuromuscular blocking drugs can reduce the tension of the upper and lower esophageal sphincters, altering the barrier pressure between the stomach and esophagus.55 Quantitative computed tomography assessments revealed that the gastric gas volume after THRIVE treatment was approximately 24 cm, which was comparable with that in the conventional oxygenation group (23.8 cm3).54 Moreover, the volumes were insufficient to pose a risk of aspiration. Ultrasound assessments of the cross-sectional area of the gastric antrum did not show any change following preoxygenation and tracheal intubation among elderly patients using THRIVE.56 No sonographic evidence of gastric insufflation, such as the “comet-tail sign”, was observed.56 Compared with a pressure-controlled facemask ventilation group, elderly patients using THRIVE demonstrated smaller cross-sectional areas of the gastric antrum and a lower incidence of gastric insufflation.57
Applications of HFNC During Tubeless Laryngopharyngeal Surgery
Microscopic laryngoscopic surgery is widely used for the examination and treatment of various throat diseases. Traditionally, mechanical ventilation with endotracheal intubation was applied for secure oxygenation in such surgery; however, the endotracheal tube often obstructed the surgical view, affecting operative access. To overcome this limitation, tubeless anesthetic techniques have been adopted, which provide a better view of surgical field for surgeons, but present new challenges for the anesthesiologists: sustaining stable peripheral oxygen saturation throughout the procedure and maintaining adequate depth of anesthesia at the same time. The THRIVE technique has been proven to provide effective apneic oxygenation and prolong the safe apneic time in various populations, including morbidly obese patients39 and pediatric patients.40 In recent years, the application of THRIVE has gradually expanded to tubeless upper airway surgery. Multiple observational studies conducted in adults have shown that the application of THRIVE techniques in micro-laryngoscopy surgery is feasible, achieving a good balance between the view of the surgical field and the patient’s oxygenation requirements, improving patients’ safety, and enabling uninterrupted procedures without surgical field obstruction.8,58,59 It can serve as an alternative to tracheal intubation or high-frequency jet ventilation.59 However, in pediatric patients, evidence from RCTs did not support THRIVE as a better oxygenation therapy than standard nursing.60,61 Younger children and those undergoing longer anesthesia remained at high risk of requiring intraoperative rescue ventilation.61
Furthermore, the high oxygen fraction provided by THRIVE also increases the risk of airway fires, especially in surgery using lasers or electrocautery.62,63 It was observed that even in the absence of combustible materials such as PVC endotracheal tubes or gauze, native tissues may act as a fuel under laser energy.62,63 Continuous laser application, low gas flow rates, and high oxygenation fractions were reported as risk factors. It was advised to reduce oxygenation fractions appropriately prior to laser use to mitigate airway fires.63 Additional protective measures included safety training on lasers, minimizing laser energy, eye protection, covering exposed facial and neck areas with wet gauze, using non-flammable airway equipment, and irrigating the surgical site with 0.9% saline in case of fire.62
Another concern about THRIVE is the accumulation of carbon dioxide (CO2). Although THRIVE facilitates apneic oxygenation, its efficiency in eliminating CO2 during apneic oxygenation remains inadequate to match metabolic CO2 production,64 posing risks of hypercapnia and acidosis, which limit the application of THRIVE for long-term surgery. During 30-minute tubeless surgery with THRIVE, PaCO2 was observed to increase at an average rate of 1.8 mmHg/min – more than twice that observed in spontaneously breathing patients (0.8 mmHg/min).65 In addition, the characteristic of the open breathing circuit created technical challenges for monitoring intraoperative end-tidal CO2 during THRIVE therapy. Transcutaneous CO2 monitoring may offer an alternative solution. A novel THRIVE device equipped with a CO2 sampling tube has been developed to capture exhaled gas from the nose or mouth; however, the measured end-tidal CO2 may underestimate the true values, limiting its reliability for detecting hypercapnia. This device would therefore be primarily reserved for detecting apneic events or airway obstruction.66
Applications of HFNC During Postoperative Recovery
COT, such as the nasal cannula or venturi mask, is the main technique for postoperative respiratory care. However, COT cannot supply gas with a stable inspiratory oxygen fraction or provide ventilatory support. When COT fails, NIV or continuous positive airway pressure (CPAP) is applied. Although NIV and CPAP can effectively improve postoperative oxygenation, reducing the incidence of hypoxemia and reintubation,67,68 the requirements for secure mask fitting often result in poor tolerance, skin injury, communication difficulties, and impaired airway secretion clearance. In contrast, HFNC, as a new oxygen delivery technique, can overcome these limitations.69 With high-flow gases continuously flushing the airway, HFNC helps to reduce the rebreathing of exhaled gas and stabilize the FiO2. Warmed and humidified oxygen supplied by HFNC enhances mucociliary clearance function and facilitates the removal of airway secretions. With its superior patient comfort, HFNC represents a promising approach to postoperative respiratory care in extubated patients.
HFNC has shown efficacy in both general populations and critically ill patients at low to medium risk of extubation failure (Table 3). Compared with COT, HFNC improves post-extubation oxygenation, and reduces the incidence of postoperative hypoxemia and reintubation. Among patients undergoing gynecological surgery, those receiving pre-emptive HFNC within 2 hours after extubation showed a higher oxygenation index and less postoperative atelectasis, assessed by lung ultrasound scores and end-expiratory diaphragmatic thickness.70 Multiple RCTs conducted in various populations, including elderly patients,71 obese patients,72 and esophageal cancer patients,73 have confirmed the benefits of HFNC in promoting postoperative oxygenation and improving patient prognosis.
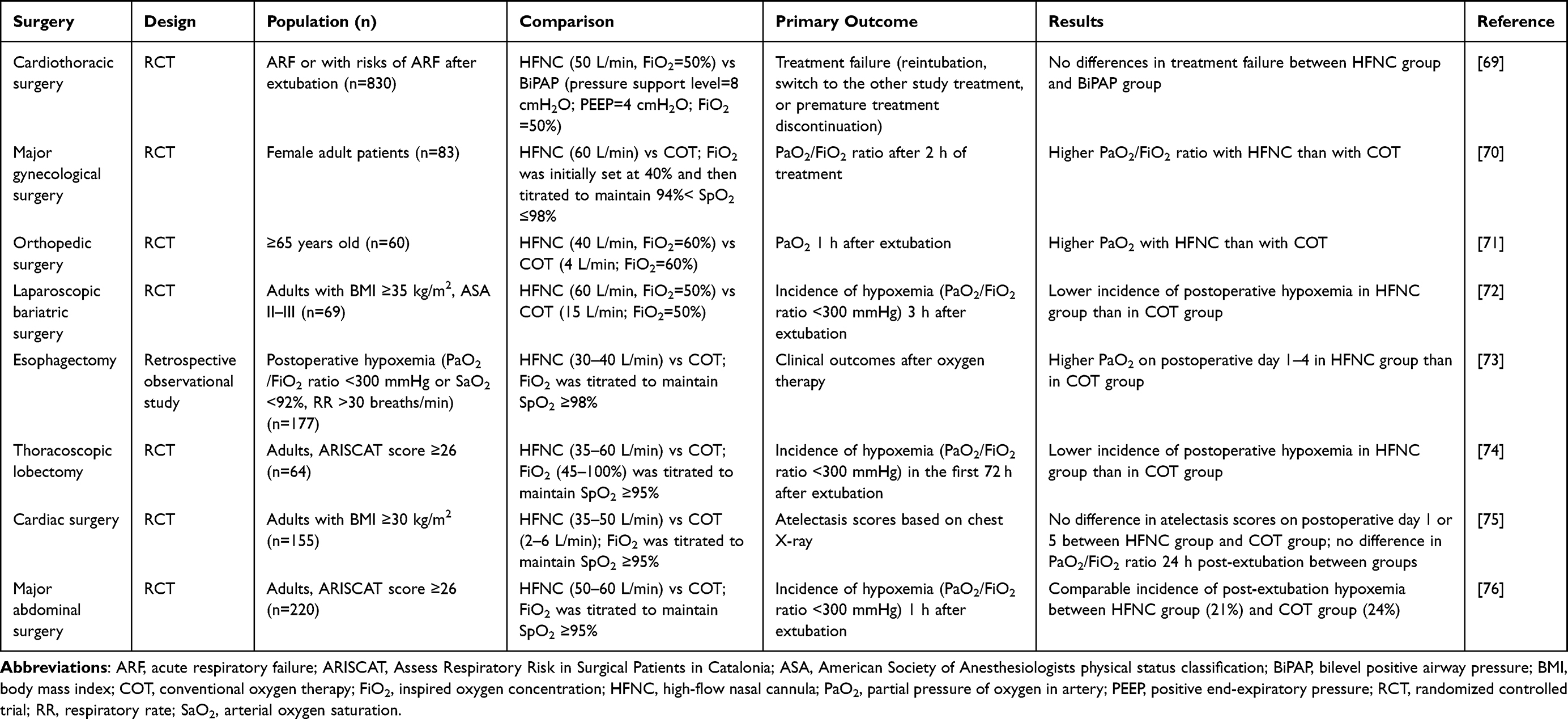 |
Table 3 Summary of Current Trials Evaluating HFNC Oxygenation During Postoperative Recovery |
Among patients with medium to high risks of postoperative pulmonary complications (PPCs), clinical practice data on the efficacy of HFNC are inconsistent. In patients undergoing thoracoscopic lobectomy, HFNC therapy was confirmed to improve post-extubation arterial oxygenation pressure (PaO2), PaO2/FiO2, and arterial oxygen saturation (SaO2)/FiO2, effectively reducing the incidence of postoperative hypoxemia and decreasing the need for salvage NIV and reintubation.74 Besides, prophylactic HFNC therapy after cardiothoracic surgery has been proven to reduce the requirement for escalated respiratory support and reintubation.77 Data from a multicenter, randomized trial in cardiothoracic patients at risk of respiratory failure indicated that HFNC demonstrated comparable therapeutic effects to bilevel positive airway pressure but with a lower incidence of skin rupture.69 Even in patients with hypoxemia, HFNC therapy following extubation has been shown to effectively reduce the need for rescue NIV.78 While multiple studies have reported the advantages of HFNC therapy, there have still been some controversial results. In a study of 155 elective cardiac surgery patients with a body mass index (BMI) ≥30 kg/m2, Corley et al found that postoperative HFNC therapy did not improve PaO2/FiO2 at 24 hours post-extubation or reduce the incidence of early atelectasis.75 Similarly, the OPERA trial, a multicenter RCT conducted across three university hospitals in France, indicated that among patients with a high risk of PPCs, prophylactic HFNC did not prevent postoperative hypoxemia within 24 hours or reduce pulmonary complications.76 It should be noted that the risk of extubation failure increased with the number of risk factors. Studies in critical patients concluded that in patients with four or more risk factors for extubation failure, prophylactic NIV combined with active humidification may be superior to HFNC, leading to better respiratory outcomes.79 Therefore, it is essential to conduct a careful and individualized assessment of a patient’s condition, risk factors for extubation failure and potential PPCs before selecting an oxygen therapy strategy, and to escalate respiratory support in a timely manner, as needed. The guidelines from the European Respiratory Society (ERS) recommend the use of HFNC or COT for patients with a low risk of PPCs, and HFNC or NIV for patients with a high risk of PPCs for postoperative oxygen therapy.80 These recommendations highlight the broad applicability of HFNC for postoperative oxygen therapy across the entire population, with outstanding performance in balancing oxygenation effects and patient comfort.
There remains a challenging clinical problem in the application of HFNC for postoperative oxygen therapy: potential intubation delay following HFNC failure. Such delays may exacerbate respiratory muscle fatigue and induce cardiopulmonary dysfunction, increasing the risks of adverse events. Evidence indicates that delayed intubation following HFNC failure (48 hours after initiating HFNC) is associated with higher intensive care unit (ICU) mortality and longer mechanical ventilation duration.81 These findings highlight the necessity of closely monitoring the efficacy of oxygen therapy and promptly adjusting oxygen therapy interventions. Clinical symptoms such as persistent tachypnea, hypoxemia, and thoracoabdominal asynchrony13 may indicate the need to escalate respiratory therapy, but solely relying on clinical signs may lead to delayed decision making. Reliable predictive tools to evaluate the efficacy of HFNC are urgently required. Roca et al proposed the respiratory rate oxidation index (ROX index, calculated as the ratio of SpO2/FiO2 to respiratory rate) to predict the effectiveness of HFNC therapy.82 A ROX index ≥4.88 was an important predictor of successful HFNC therapy for pneumonia patients.82 Conversely, ROX indices of <2.85 at 2 hours, <3.47 at 6 hours, and <3.85 at 12 hours indicated HFNC failure, with specificities of 99.2%, 99.2%, and 98.4%, respectively.83 Other modified indices, such as the mROX84 (PaO2/FiO2 to respiratory rate ratio) and ROX-HR85 (ROX index to heart rate ratio), have also shown utility in predicting HFNC failure among patients with acute hypoxemia. Machine learning technologies have enabled the integration of multiple clinical indicators to predict HFNC failure and identify more complex and individualized thresholds for escalating respiratory support. For instance, a support vector machine-based model achieved an accuracy of 83%, a sensitivity of 84%, a specificity of 82%, and an area under the curve of 0.82 in external validation.86 Given the differences between perioperative respiratory management and ICU clinical practice, additional studies are needed to validate the predictive performance and refine relative interpretations of these predictive tools in different clinical settings. Decision timepoints should be refined and key clinical parameters such as PaO2 and PaCO2 should also be incorporated to adapt to perioperative clinical practice. Future research should focus on more comprehensive and perioperative-specific models.
Evidence Assessments and Clinical Recommendations for Perioperative Oxygen Therapy
A preliminary evaluation of the available evidence was conducted (Table 4). The application of HFNC for procedural sedation is supported by multiple high-quality RCTs and rigorous meta-analyses, representing the indication with the strongest evidence.5,9–11 Synthesis of these evaluations informed the summarized recommendations for perioperative oxygen therapy across various clinical scenarios (Table 5). For most perioperative scenarios, HFNC was recommended as an alternative or preferred option over COT, with the exception of pediatric tubeless surgery.5,12,60,80 Besides, individualized assessments remained essential. For patients at high risk of PPCs, HFNC or NIV was recommended for oxygen therapy during postoperative recovery, and NIV combined with active humidification may be optimal for critically ill patients.79,81 It should be acknowledged that the assessments of evidence strength in Table 4 were performed via a structured descriptive synthesis based on three key dimensions: study design, methodological rigor, and consistency of findings. As a narrative review, this work carries inherent limitations. A systematic literature analysis and formal evidence grading (for example, the Grading of Recommendations, Assessment, Development, and Evaluation framework)87 were not performed, nor were statistical evaluations of publication bias, imprecision, or heterogeneity feasible. Consequently, the evidence assessments remain descriptive and qualitative. Definitive evidence strengths require confirmation through systematic reviews, and clinical judgment remains paramount.
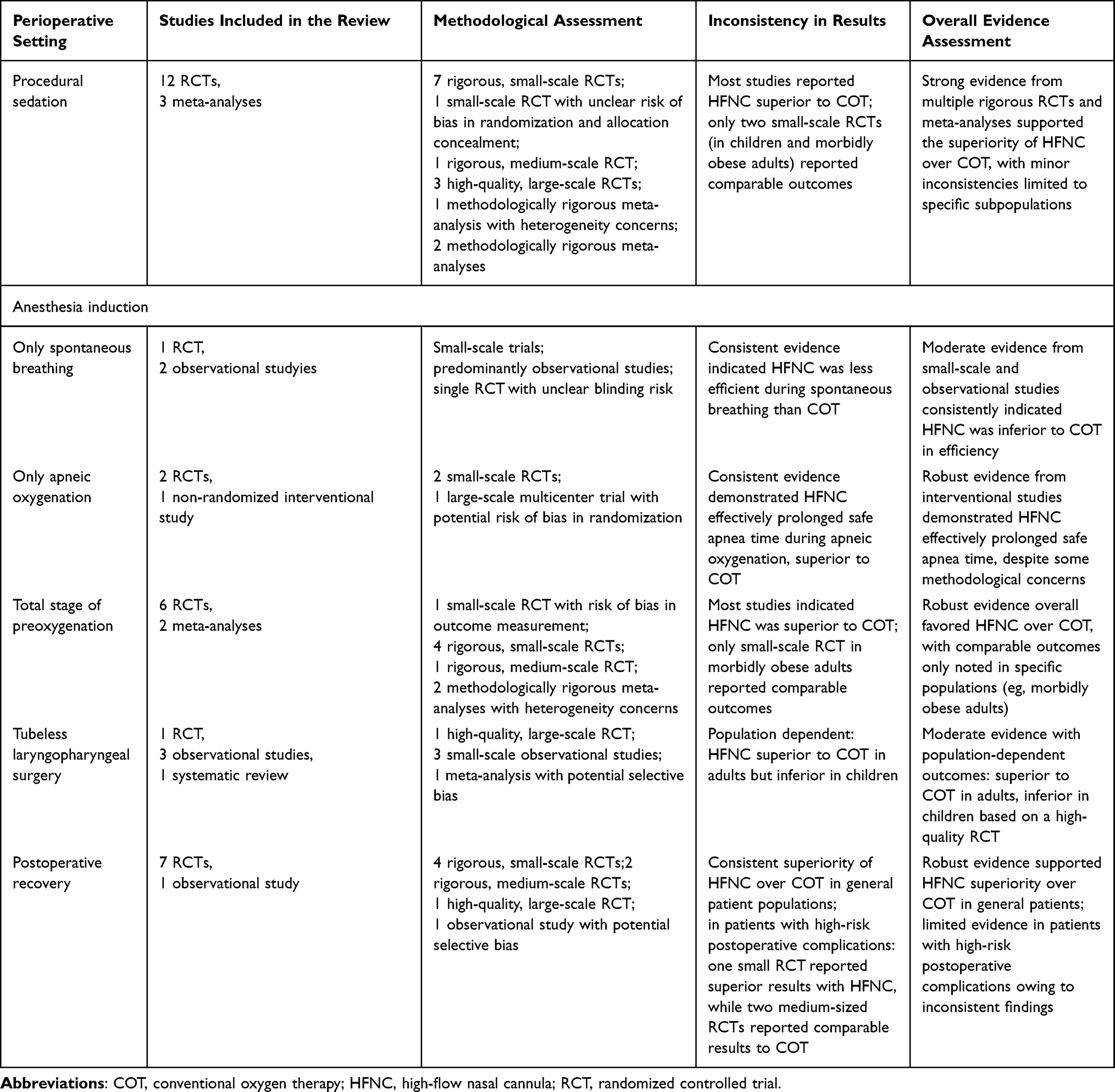 |
Table 4 Summary of Evidence Assessments Across Perioperative Settings |
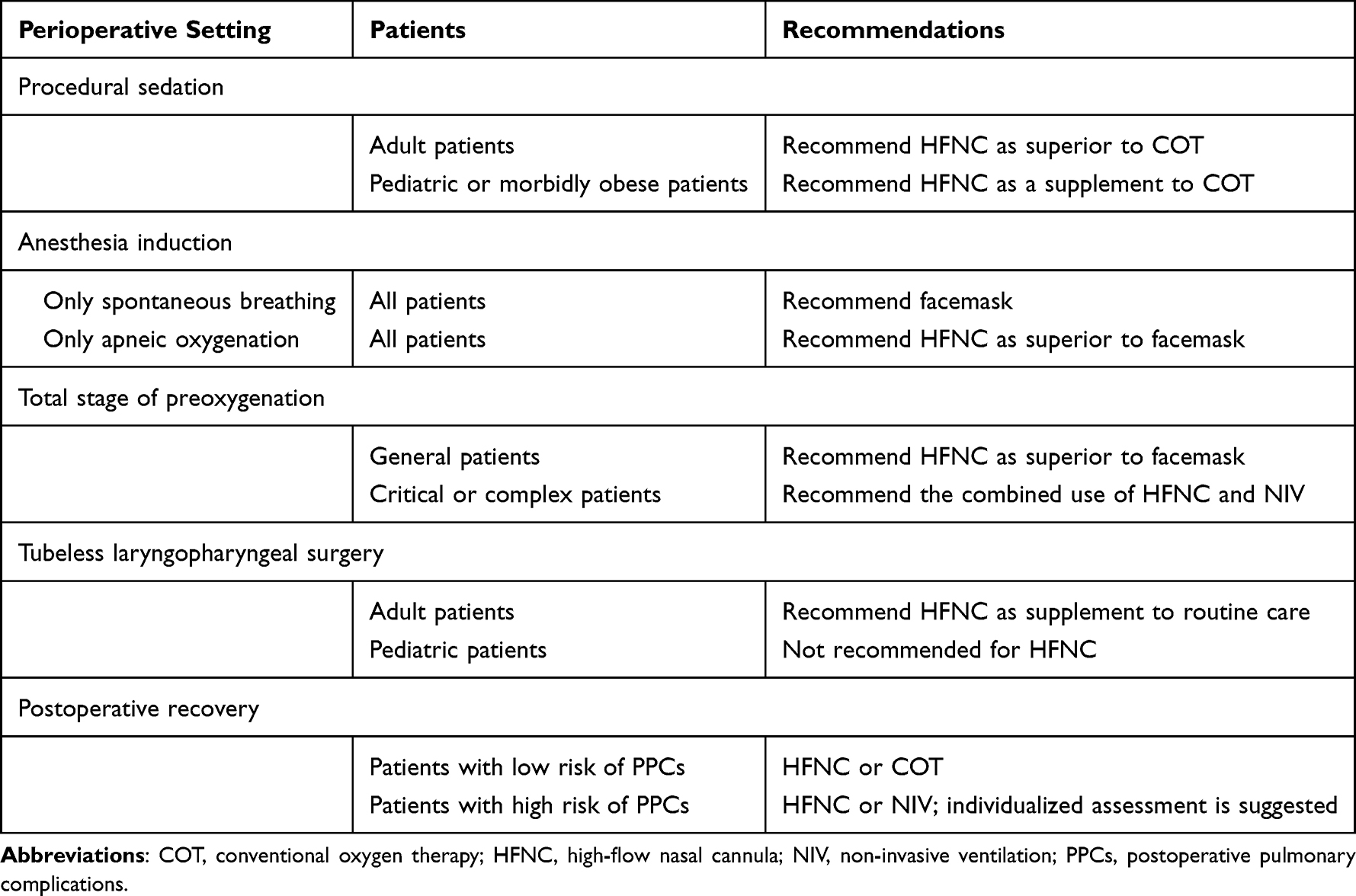 |
Table 5 Evidence-Based Clinical Practice Recommendations for Perioperative HFNC |
Conclusion
As an emerging respiratory support technology, HFNC addresses a key unmet need in perioperative care: providing reliable, non-invasive oxygenation without interfering with procedural access or compromising patient comfort. Multiple studies indicate that HFNC has demonstrated considerable potential across various perioperative settings, with the strongest evidence in applications during procedural sedation. Its unique efficacy during apneic oxygenation offers a valuable alternative for oxygenation during laryngoscopy, tracheal intubation, and brief tubeless surgery. However, heterogeneity in oxygen flow rates, fractions, and treatment durations across studies limits comparability, and the optimal HFNC protocol remains to be established. Challenges include balancing the benefits of high-flow therapy against potential barotrauma risks and weighing oxygenation efficacy against adverse effects associated with high FiO2 exposure. Clinically, HFNC also faces challenges such as risk of CO2 retention during anesthesia, limitations of EtCO2 monitoring, and the potential for delayed intubation in patients at high risk of PPCs. In summary, based on existing evidence, HFNC should be considered as a valuable and recommended technique in perioperative respiratory management. Future research should focus on optimizing clinical protocols, developing reliable predictive models, and validating these through large-scale, multicenter RCTs to advance evidence-based and precise strategies for perioperative respiratory management.
Abbreviations
BMI, body mass index; COT, conventional oxygen therapy; CPAP, continuous positive airway pressure; EtO2, end-tidal oxygen concentration; FiO2, inspired oxygen concentration; HFNC, high-flow nasal cannula oxygen therapy; ICU, intensive care unit; NIV, non-invasive ventilation; PaCO2, arterial carbon dioxide pressure; PaO2, arterial oxygen pressure; PEEP, positive end-expiratory pressure; PPCs, postoperative pulmonary complications; ROX index, respiratory rate oxygenation index; mROX, modified respiratory rate oxygenation index; ROX-HR, respiratory rate oxygenation index to heart rate ratio; SaO2, arterial oxygen saturation; SpO2, peripheral oxygen saturation; THRIVE, transnasal humidified rapid-insufflation ventilatory exchange.
Acknowledgments
Thanks to BioRender for their support in drawing the figures (created in BioRender. Chen J (2026) https://BioRender.com/1p6uuhd; https://BioRender.com/wf6r3jx).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Papazian L, Corley A, Hess D, et al. Use of high-flow nasal cannula oxygenation in ICU adults: a narrative review. Intensive Care Med. 2016;42(9):1336–16. doi:10.1007/s00134-016-4277-8
2. Rochwerg B, Granton D, Wang DX, et al. High flow nasal cannula compared with conventional oxygen therapy for acute hypoxemic respiratory failure: a systematic review and meta-analysis. Intensive Care Med. 2019;45(5):563–572. doi:10.1007/s00134-019-05590-5
3. Beggs S, Wong ZH, Kaul S, Ogden KJ, Walters JA. High-flow nasal cannula therapy for infants with bronchiolitis. Cochrane Database Syst Rev. 2014;2014(1):Cd009609. doi:10.1002/14651858.CD009609.pub2
4. Wang Q, Peng Y, Xu S, Chen L, Lin L, Lin Y. The efficacy of high-flow nasal cannula (HFNC) versus non-invasive ventilation (NIV) in patients at high risk of extubation failure: a systematic review and meta-analysis. Eur J Med Res. 2023;28(1):120. doi:10.1186/s40001-023-01076-9
5. Thiruvenkatarajan V, Sekhar V, Wong DT, Currie J, Van Wijk R, Ludbrook GL. Effect of high-flow nasal oxygen on hypoxaemia during procedural sedation: a systematic review and meta-analysis. Anaesthesia. 2023;78(1):81–92. doi:10.1111/anae.15845
6. Mukherjee D, Mukherjee R. High-flow nasal cannula oxygen therapy in the management of respiratory failure: a review. Cureus. 2023;15(12):e50738. doi:10.7759/cureus.50738
7. Jaber S, De Jong A, Schaefer MS, et al. Preoxygenation with standard facemask combining apnoeic oxygenation using high flow nasal cannula versuss standard facemask alone in patients with and without obesity: the OPTIMASK international study. Ann Intensive Care. 2023;13(1):26. doi:10.1186/s13613-023-01124-x
8. Courbon C. Spontaneous ventilation with high-flow nasal oxygen for elective suspension microlaryngoscopy. OTO Open. 2023;7(2):e54. doi:10.1002/oto2.54
9. Wang L, Zhang Y, Han D, et al. Effect of high flow nasal cannula oxygenation on incidence of hypoxia during sedated gastrointestinal endoscopy in patients with obesity: multicentre randomised controlled trial. BMJ. 2025;388:e080795. doi:10.1136/bmj-2024-080795
10. Nay M-A, Fromont L, Eugene A, et al. High-flow nasal oxygenation or standard oxygenation for gastrointestinal endoscopy with sedation in patients at risk of hypoxaemia: a multicentre randomised controlled trial (ODEPHI trial). Br J Anaesth. 2021;127(1):133–142. doi:10.1016/j.bja.2021.03.020
11. Lin Y, Zhang X, Li L, et al. High-flow nasal cannula oxygen therapy and hypoxia during gastroscopy with propofol sedation: a randomized multicenter clinical trial. Gastrointest Endosc. 2019;90(4):591–601. doi:10.1016/j.gie.2019.06.033
12. Crístian de Carvalho C, Iliff HA, Santos Neto JM, et al. Effectiveness of preoxygenation strategies: a systematic review and network meta-analysis. Br J Anaesth. 2024;133(1):152–163. doi:10.1016/j.bja.2024.02.028
13. Drake MG. High-Flow Nasal Cannula Oxygen in Adults: an Evidence-based Assessment. Ann Am Thorac Soc. 2018;15(2):145–155. doi:10.1513/AnnalsATS.201707-548FR
14. Longhini F, Bruni A, Saraco G, Garofalo E, Conti G. Should high-flow through nasal cannula be used during bronchoscopy in critically ill patients with hypoxemic acute respiratory failure? J Anesthesia Analgesia Critical Care. 2021;1(1):4. doi:10.1186/s44158-021-00001-y
15. Mauri T, Turrini C, Eronia N, et al. Physiologic effects of high-flow nasal cannula in acute hypoxemic respiratory failure. Am J Respir Crit Care Med. 2017;195(9):1207–1215. doi:10.1164/rccm.201605-0916OC
16. Parke RL, Bloch A, McGuinness SP. Effect of very-high-flow nasal therapy on airway pressure and end-expiratory lung impedance in healthy volunteers. Respir Care. 2015;60(10):1397–1403. doi:10.4187/respcare.04028
17. Riva T, Meyer J, Theiler L, et al. Measurement of airway pressure during high-flow nasal therapy in apnoeic oxygenation: a randomised controlled crossover trial. Anaesthesia. 2021;76(1):27–35. doi:10.1111/anae.15224
18. Nishimura M. High-flow nasal cannula oxygen therapy in adults: physiological benefits, indication, clinical benefits, and adverse effects. Respir Care. 2016;61(4):529–541. doi:10.4187/respcare.04577
19. Vargo JJ, Niklewski PJ, Williams JL, Martin JF, Faigel DO. Patient safety during sedation by anesthesia professionals during routine upper endoscopy and colonoscopy: an analysis of 1.38 million procedures. Gastrointest Endosc. 2017;85(1):101–108. doi:10.1016/j.gie.2016.02.007
20. Qadeer MA, Lopez AR, Dumot JA, Vargo JJ. Hypoxemia during moderate sedation for gastrointestinal endoscopy: causes and associations. Digestion. 2011;84(1):37–45. doi:10.1159/000321621
21. Holm C, Christensen M, Rasmussen V, Schulze S, Rosenberg J. Hypoxaemia and myocardial ischaemia during colonoscopy. Scand J Gastroenterol. 1998;33(7):769–772. doi:10.1080/00365529850171747
22. Cai G, Huang Z, Zou T, et al. Clinical application of a novel endoscopic mask: a randomized controlled trial in aged patients undergoing painless gastroscopy. Int J Med Sci. 2017;14(2):167–172. doi:10.7150/ijms.16919
23. Zhang YX, He XX, Chen YP, Yang S. The effectiveness of high-flow nasal cannula during sedated digestive endoscopy: a systematic review and meta-analysis. Eur J Med Res. 2022;27(1):30. doi:10.1186/s40001-022-00661-8
24. Gu WJ, Wang HT, Huang J, et al. High flow nasal oxygen versus conventional oxygen therapy in gastrointestinal endoscopy with conscious sedation: systematic review and meta-analysis with trial sequential analysis. Dig Endosc. 2022;34(6):1136–1146. doi:10.1111/den.14315
25. Riccio CA, Sarmiento S, Minhajuddin A, Nasir D, Fox AA. High-flow versus standard nasal cannula in morbidly obese patients during colonoscopy: a prospective, randomized clinical trial. J Clin Anesth. 2019;54:19–24. doi:10.1016/j.jclinane.2018.10.026
26. Teng WN, Ting CK, Wang YT, et al. Oral capnography is more effective than nasal capnography during sedative upper gastrointestinal endoscopy. J Clin Monit Comput. 2018;32(2):321–326. doi:10.1007/s10877-017-0029-8
27. Klotz D, Seifert V, Baumgartner J, Teufel U, Fuchs H. High-flow nasal cannula vs standard respiratory care in pediatric procedural sedation: a randomized controlled pilot trial. Pediatr Pulmonol. 2020;55(10):2706–2712. doi:10.1002/ppul.24975
28. Douglas N, Ng I, Nazeem F, et al. A randomised controlled trial comparing high-flow nasal oxygen with standard management for conscious sedation during bronchoscopy. Anaesthesia. 2018;73(2):169–176. doi:10.1111/anae.14156
29. Irfan M, Ahmed M, Breen D. Assessment of high flow nasal cannula oxygenation in endobronchial ultrasound bronchoscopy: a randomized controlled trial. J Bronchology Interv Pulmonol. 2021;28(2):130–137. doi:10.1097/lbr.0000000000000719
30. Ben-Menachem E, McKenzie J, O’Sullivan C, Havryk AP. High-flow nasal oxygen versus standard oxygen during flexible bronchoscopy in lung transplant patients: a randomized controlled trial. J Bronchol Interv Pulmonol. 2020;27(4):259–265. doi:10.1097/lbr.0000000000000670
31. Longhini F, Pelaia C, Garofalo E, et al. High-flow nasal cannula oxygen therapy for outpatients undergoing flexible bronchoscopy: a randomised controlled trial. Thorax. 2022;77(1):58–64. doi:10.1136/thoraxjnl-2021-217116
32. Shih CC, Liang PC, Chuang YH, Huang YJ, Lin PJ, Wu CY. Effects of high-flow nasal oxygen during prolonged deep sedation on postprocedural atelectasis: a randomised controlled trial. Eur J Anaesthesiol. 2020;37(11):1025–1031. doi:10.1097/eja.0000000000001324
33. Frassanito L, Grieco DL, Vassalli F, et al. High-flow nasal oxygen versus mechanical ventilation through a laryngeal mask during general anesthesia without muscle paralysis: a randomized clinical trial. Anesth Analg. 2025. doi:10.1213/ane.0000000000007620
34. Yi P, Li Q, Yang Z, Cao L, Hu X, Gu H. High-flow nasal cannula improves clinical efficacy of airway management in patients undergoing awake craniotomy. BMC Anesthesiol. 2020;20(1):156. doi:10.1186/s12871-020-01073-z
35. Albertini RE, Harrell JH 2nd, Kurihara N, Moser KM. Arterial hypoxemia induced by fiberoptic bronchoscopy. JAMA. 1974;230(12):1666–1667.
36. La Combe B, Messika J, Labbé V, et al. High-flow nasal oxygen for bronchoalveolar lavage in acute respiratory failure patients. Eur Respir J. 2016;47(4):1283–1286. doi:10.1183/13993003.01883-2015
37. Patel A, Nouraei SA. Transnasal humidified rapid-insufflation ventilatory exchange (THRIVE): a physiological method of increasing apnoea time in patients with difficult airways. Anaesthesia. 2015;70(3):323–329. doi:10.1111/anae.12923
38. Ramachandran SK, Cosnowski A, Shanks A, Turner CR. Apneic oxygenation during prolonged laryngoscopy in obese patients: a randomized, controlled trial of nasal oxygen administration. J Clin Anesth. 2010;22(3):164–168. doi:10.1016/j.jclinane.2009.05.006
39. Schutzer-Weissmann J, Wojcikiewicz T, Karmali A, et al. Apnoeic oxygenation in morbid obesity: a randomised controlled trial comparing facemask and high-flow nasal oxygen delivery. Br J Anaesth. 2023;130(1):103–110. doi:10.1016/j.bja.2021.12.011
40. Humphreys S, Lee-Archer P, Reyne G, Long D, Williams T, Schibler A. Transnasal humidified rapid-insufflation ventilatory exchange (THRIVE) in children: a randomized controlled trial. Br J Anaesth. 2017;118(2):232–238. doi:10.1093/bja/aew401
41. Wong DT, Dallaire A, Singh KP, et al. High-flow nasal oxygen improves safe apnea time in morbidly obese patients undergoing general anesthesia: a randomized controlled trial. Anesth Analg. 2019;129(4):1130–1136. doi:10.1213/ane.0000000000003966
42. Lei G, Yang S, Wu L, et al. High-flow nasal oxygen prolongs safe apnea time in obstructive sleep apnea patients undergoing general anesthesia: a randomized controlled trial. Risk Manag Healthc Policy. 2025;18:2469–2477. doi:10.2147/rmhp.S518271
43. Jaber S, Monnin M, Girard M, et al. Apnoeic oxygenation via high-flow nasal cannula oxygen combined with non-invasive ventilation preoxygenation for intubation in hypoxaemic patients in the intensive care unit: the single-centre, blinded, randomised controlled OPTINIV trial. Intensive Care Med. 2016;42(12):1877–1887. doi:10.1007/s00134-016-4588-9
44. Miguel-Montanes R, Hajage D, Messika J, et al. Use of high-flow nasal cannula oxygen therapy to prevent desaturation during tracheal intubation of intensive care patients with mild-to-moderate hypoxemia. Crit Care Med. 2015;43(3):574–583. doi:10.1097/ccm.0000000000000743
45. Jo JY, Yoon J, Jang H, Kim WJ, Ku S, Choi SS. Comparison of preoxygenation with a high-flow nasal cannula and a simple face mask before intubation in Korean patients with head and neck cancer. Acute Crit Care. 2024;39(1):61–69. doi:10.4266/acc.2022.01543
46. Ang KS, Green A, Ramaswamy KK, Frerk C. Preoxygenation using the Optiflow™ system. Br J Anaesth. 2017;118(3):463–464. doi:10.1093/bja/aex016
47. Hanouz JL, Lhermitte D, Gérard JL, Fischer MO. Comparison of pre-oxygenation using spontaneous breathing through face mask and high-flow nasal oxygen: a randomised controlled crossover study in healthy volunteers. Eur J Anaesthesiol. 2019;36(5):335–341. doi:10.1097/eja.0000000000000954
48. Tan PCF, Millay OJ, Leeton L, Dennis AT. High-flow humidified nasal preoxygenation in pregnant women: a prospective observational study. Br J Anaesth. 2019;122(1):86–91. doi:10.1016/j.bja.2018.08.015
49. Vourc’h M, Baud G, Feuillet F, et al. High-flow nasal cannulae versus non-invasive ventilation for preoxygenation of obese patients: the PREOPTIPOP randomized trial. EClinicalMedicine. 2019;13:112–119. doi:10.1016/j.eclinm.2019.05.014
50. Zhou S, Zhou Y, Cao X, et al. The efficacy of high flow nasal oxygenation for maintaining maternal oxygenation during rapid sequence induction in pregnancy: a prospective randomised clinical trial. Eur J Anaesthesiol. 2021;38(10):1052–1058. doi:10.1097/eja.0000000000001395
51. Zhong M, Xia R, Zhou J, Zhang J, Yi X, Yang A. The comparison of preoxygenation methods before endotracheal intubation: a network meta-analysis of randomized trials. Front Med. 2024;11:1379369. doi:10.3389/fmed.2024.1379369
52. Allen ML, Denuna-Rivera S, DiMarino AJ Jr. End expiration is more accurate than mid respiration in measuring lower esophageal sphincter pressure. Digestion. 2000;62(1):22–25. doi:10.1159/000007773
53. McLellan E, Lam K, Behringer E, et al. High-flow nasal oxygen does not increase the volume of gastric secretions during spontaneous ventilation. Br J Anaesth. 2020;125(1):e75–e80. doi:10.1016/j.bja.2020.02.023
54. Sud A, Athanassoglou V, Anderson EM, Scott S. A comparison of gastric gas volumes measured by computed tomography after high-flow nasal oxygen therapy or conventional facemask ventilation(). Anaesthesia. 2021;76(9):1184–1189. doi:10.1111/anae.15433
55. de Leon A, Thörn SE, Wattwil M. High-resolution solid-state manometry of the upper and lower esophageal sphincters during anesthesia induction: a comparison between obese and non-obese patients. Anesth Analg. 2010;111(1):149–153. doi:10.1213/ANE.0b013e3181e1a71f
56. Cai Q, Ma W, Wu C, Liu H, Wang S, Zhang G. Is pre-oxygenation with high-flow nasal oxygen safe? randomized control trial of 56 cases of elderly patients during induction of general anesthesia with endotracheal intubation. Nan Fang Yi Ke Da Xue Xue Bao. 2022;42(7):1069–1074. doi:10.12122/j.issn.1673-4254.2022.07.16
57. Huang X, Zhou X, Zhou Z, et al. Effect of transnasal humidified rapid-insufflation ventilatory exchange on gastric insufflation during anaesthesia induction: a randomised controlled trial and multivariate analysis. Eur J Anaesthesiol. 2023;40(7):521–528. doi:10.1097/eja.0000000000001846
58. Ma B, Liu F, Wang D, et al. High-flow nasal cannula in nonlaser microlaryngoscopic surgery: a prospective study of 19 cases in a Chinese population. BMC Anesthesiol. 2022;22(1):81. doi:10.1186/s12871-022-01627-3
59. Huang L, Dharmawardana N, Badenoch A, Ooi EH. A review of the use of transnasal humidified rapid insufflation ventilatory exchange for patients undergoing surgery in the shared airway setting. J Anesth. 2020;34(1):134–143. doi:10.1007/s00540-019-02697-3
60. Humphreys S, von Ungern-Sternberg BS, Taverner F, et al. High-flow nasal oxygen for children’s airway surgery to reduce hypoxaemic events: a randomised controlled trial. Lancet Respir Med. 2024;12(7):535–543. doi:10.1016/s2213-2600(24)00115-2
61. Kim EH, Ji SH, Lee JH, et al. Use of high-flow nasal oxygen in spontaneously breathing pediatric patients undergoing tubeless airway surgery: a prospective observational study. Medicine. 2022;101(27):e29520. doi:10.1097/md.0000000000029520
62. Shankla S, De Zoysa N, Bird J, Girgis M. Facial fire with use of high-flow nasal oxygen during laser surgery. Anaesth Rep. 2024;12(2):e12329. doi:10.1002/anr3.12329
63. Chang MY, Chen JH, Lin SP, et al. Fire safety study on high-flow nasal oxygen in shared-airway surgeries with diathermy and laser: simulation based on a physical model. J Clin Monit Comput. 2022;36(3):649–655. doi:10.1007/s10877-021-00690-4
64. Hermez LA, Spence CJ, Payton MJ, Nouraei SAR, Patel A, Barnes TH. A physiological study to determine the mechanism of carbon dioxide clearance during apnoea when using transnasal humidified rapid insufflation ventilatory exchange (THRIVE). Anaesthesia. 2019;74(4):441–449. doi:10.1111/anae.14541
65. Booth AWG, Vidhani K, Lee PK, et al. The effect of high-flow nasal oxygen on carbon dioxide accumulation in apneic or spontaneously breathing adults during airway surgery: a randomized-controlled trial. Anesth Analg. 2021;133(1):133–141. doi:10.1213/ane.0000000000005002
66. Nagappa M, Wong DT. Is high-flow safer than low-flow nasal oxygenation for procedural sedation? Can J Anaesth. 2021;68(4):439–444. doi:10.1007/s12630-020-01884-1 Sédation procédurale: l’oxygénation nasale à débit élevé est-elle plus sécuritaire que l’oxygénation nasale à faible débit?.
67. Kindgen-Milles D, Müller E, Buhl R, et al. Nasal-continuous positive airway pressure reduces pulmonary morbidity and length of hospital stay following thoracoabdominal aortic surgery. Chest. 2005;128(2):821–828. doi:10.1378/chest.128.2.821
68. Zarbock A, Mueller E, Netzer S, Gabriel A, Feindt P, Kindgen-Milles D. Prophylactic nasal continuous positive airway pressure following cardiac surgery protects from postoperative pulmonary complications: a prospective, randomized, controlled trial in 500 patients. Chest. 2009;135(5):1252–1259. doi:10.1378/chest.08-1602
69. Stéphan F, Barrucand B, Petit P, et al. High-flow nasal oxygen vs noninvasive positive airway pressure in hypoxemic patients after cardiothoracic surgery: a randomized clinical trial. JAMA. 2015;313(23):2331–2339. doi:10.1001/jama.2015.5213
70. Frassanito L, Grieco DL, Zanfini BA, et al. Effect of a pre-emptive 2-hour session of high-flow nasal oxygen on postoperative oxygenation after major gynaecologic surgery: a randomised clinical trial. Br J Anaesth. 2023;131(4):775–785. doi:10.1016/j.bja.2023.07.002
71. Li XN, Zhou CC, Lin ZQ, et al. High-flow nasal cannula oxygen therapy during anesthesia recovery for older orthopedic surgery patients: a prospective randomized controlled trial. World J Clin Cases. 2022;10(24):8615–8624. doi:10.12998/wjcc.v10.i24.8615
72. Ferrando C, Puig J, Serralta F, et al. High-flow nasal cannula oxygenation reduces postoperative hypoxemia in morbidly obese patients: a randomized controlled trial. Minerva Anestesiol. 2019;85(10):1062–1070. doi:10.23736/s0375-9393.19.13364-0
73. Xia M, Li W, Yao J, et al. A postoperative comparison of high-flow nasal cannula therapy and conventional oxygen therapy for esophageal cancer patients. Ann Palliat Med. 2021;10(3):2530–2539. doi:10.21037/apm-20-1539
74. Yu Y, Qian X, Liu C, Zhu C. Effect of high-flow nasal cannula versus conventional oxygen therapy for patients with thoracoscopic lobectomy after extubation. Can Respir J. 2017;2017:7894631. doi:10.1155/2017/7894631
75. Corley A, Bull T, Spooner AJ, Barnett AG, Fraser JF. Direct extubation onto high-flow nasal cannulae post-cardiac surgery versus standard treatment in patients with a BMI ≥30: a randomised controlled trial. Intensive Care Med. 2015;41(5):887–894. doi:10.1007/s00134-015-3765-6
76. Futier E, Paugam-Burtz C, Godet T, et al. Effect of early postextubation high-flow nasal cannula vs conventional oxygen therapy on hypoxaemia in patients after major abdominal surgery: a French multicentre randomised controlled trial (OPERA). Intensive Care Med. 2016;42(12):1888–1898. doi:10.1007/s00134-016-4594-y
77. Wang Y, Huang D, Ni Y, Liang Z. High-flow nasal cannula vs conventional oxygen therapy for postcardiothoracic surgery. Respir Care. 2020;65(11):1730–1737. doi:10.4187/respcare.07595
78. Maggiore SM, Jaber S, Grieco DL, et al. High-flow versus venturimask oxygen therapy to prevent reintubation in hypoxemic patients after extubation: a multicenter randomized clinical trial. Am J Respir Crit Care Med. 2022;206(12):1452–1462. doi:10.1164/rccm.202201-0065OC
79. Hernández G, Paredes I, Moran F, et al. Effect of postextubation noninvasive ventilation with active humidification vs high-flow nasal cannula on reintubation in patients at very high risk for extubation failure: a randomized trial. Intensive Care Med. 2022;48(12):1751–1759. doi:10.1007/s00134-022-06919-3
80. Oczkowski S, Ergan B, Bos L, et al. ERS clinical practice guidelines: high-flow nasal cannula in acute respiratory failure. Eur Respir J. 2022;59(4). doi:10.1183/13993003.01574-2021
81. Kang BJ, Koh Y, Lim CM, et al. Failure of high-flow nasal cannula therapy may delay intubation and increase mortality. Intensive Care Med. 2015;41(4):623–632. doi:10.1007/s00134-015-3693-5
82. Roca O, Messika J, Caralt B, et al. Predicting success of high-flow nasal cannula in pneumonia patients with hypoxemic respiratory failure: the utility of the ROX index. J Crit Care. 2016;35:200–205. doi:10.1016/j.jcrc.2016.05.022
83. Roca O, Caralt B, Messika J, et al. An index combining respiratory rate and oxygenation to predict outcome of nasal high-flow therapy. Am J Respir Crit Care Med. 2019;199(11):1368–1376. doi:10.1164/rccm.201803-0589OC
84. Karim HMR, Esquinas AM. Success or failure of high-flow nasal oxygen therapy: the ROX index is good, but a modified ROX index may be better. Am J Respir Crit Care Med. 2019;200(1):116–117. doi:10.1164/rccm.201902-0419LE
85. Goh KJ, Chai HZ, Ong TH, Sewa DW, Phua GC, Tan QL. Early prediction of high flow nasal cannula therapy outcomes using a modified ROX index incorporating heart rate. J Intensive Care. 2020;8:41. doi:10.1186/s40560-020-00458-z
86. Yu H, Saffaran S, Tonelli R, et al. Machine learning models compared with current clinical indices to predict the outcome of high flow nasal cannula therapy in acute hypoxemic respiratory failure. Crit Care. 2025;29(1):101. doi:10.1186/s13054-025-05336-4
87. Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–394. doi:10.1016/j.jclinepi.2010.04.026
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.