")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 14
High Fibroblast Growth Factor 23 as a Biomarker for Severe Cardiac Impairment in Children with Chronic Kidney Disease: A Single Tertiary Center Study
Authors Palupi-Baroto R, Hermawan K , Murni IK, Nurlitasari T, Prihastuti Y, Sekali DRK, Ambarsari CG
Received 5 February 2021
Accepted for publication 29 April 2021
Published 8 June 2021 Volume 2021:14 Pages 165—171
DOI https://doi.org/10.2147/IJNRD.S304143
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Pravin Singhal
Retno Palupi-Baroto,1 Kristia Hermawan,1 Indah Kartika Murni,1 Tiara Nurlitasari,1 Yuli Prihastuti,1 Debora Roselita Karo Sekali,2 Cahyani Gita Ambarsari2
1Department of Child Health, Faculty of Medicine, Public Health and Nursing Universitas Gadjah Mada/Dr. Sardjito General Hospital, Yogyakarta, Indonesia; 2Department of Child Health, Faculty of Medicine Universitas Indonesia – Cipto Mangunkusumo Hospital, Jakarta, Indonesia
Correspondence: Retno Palupi-Baroto Jl. Farmako Sekip Utara, Yogyakarta, 55281 Tel +6281284934038
Fax +62274 581 876
Email [email protected]
Introduction: Left ventricular hypertrophy (LVH) is the most common cardiac abnormality in chronic kidney disease (CKD). Changes in cardiac geometry and functions may occur in an early stage and worsen as CKD progresses. Recently, the role of fibroblast growth factor 23 (FGF23) is being highlighted and investigated in CKD-related cardiomyopathy. However, only a few studies have reviewed the utilization of FGF23 as a diagnostic biomarker in the pediatric CKD population.
Purpose: This study aimed to identify the role of FGF23 as a biomarker in assessing cardiac changes in children with CKD.
Patients and Methods: We conducted a cross-sectional study that involved children aged 2 to 18 years old with CKD stages 2 to 5D in Dr. Sardjito General Hospital, Yogyakarta, Indonesia. The level of FGF23 was measured using an immunometric enzyme-linked immunosorbent assay. LVMI, RWT, and left ventricular ejection fraction (LVEF) were assessed with echocardiography. Receiver-operating characteristic (ROC) analyses were conducted to assess the diagnostic performance of FGF23 in detecting LVH with impaired contractility.
Results: A total of 43 children with CKD stages 2 to 5D were included, among whom the prevalence of LVH diagnosis was 95.35%. The area under the curve (AUC) of FGF23 to assess LVH and systolic dysfunction was 0.82 (95% CI 0.62– 1.0), and the optimal cutoff point was 1413 RU/mL (sensitivity 80%, specificity 78.95%). The median concentration of FGF23 increased with the decreasing eGFR and the increasing LVMI although the systolic and diastolic functions were preserved.
Conclusion: FGF23 might be used as an early biomarker to detect cardiac changes in pediatric CKD patients, particularly for LVH and impaired systolic function among children with CKD stage 2 and higher.
Keywords: FGF23, left ventricular hypertrophy, ventricular ejection fraction, end-stage kidney disease, dialysis
Introduction
Cardiovascular disease (CVD) is the leading cause of death in children with chronic kidney disease (CKD). Studies reported that 40–50% of all deaths were due to cardiovascular causes, and especially high among those receiving hemodialysis or peritoneal dialysis.1 Cardiac-related death in the dialysis population was caused by cardiac arrest, congestive heart failure, cardiomyopathy, acute myocardial infarction, and pericarditis.1
Changes in cardiac geometry and functions may occur in an early stage and worsen as CKD progresses. Left ventricular hypertrophy (LVH) is the most prevalent cardiac abnormality in CKD-related cardiomyopathy.1 As many as 17–50% of pediatric patients with CKD stages 2–4 developed LVH, and the number was greater in the pediatric dialysis population (30–92%).1,2 Impaired systolic and diastolic functions have also been observed in pediatric CKD.3,4
Fibroblast growth factor 23 (FGF23) is a glycoprotein produced by osteocytes and osteoblasts.5 Under physiological circumstances, it functions as a mineral metabolism regulator in the kidneys and bones. Studies have revealed that the FGF23 level increased as the glomerular filtration rate (GFR) declined6 and elevated before the levels of parathyroid hormone (PTH) and phosphate started to rise.7 Recently, the role of FGF23 in the development of CVD is being highlighted and investigated. However, only a few studies have reviewed the utilization of FGF23 as a parameter in the pediatric CKD population. Mitsnefes et al8 showed that plasma concentration of FGF23 above 170 RU/mL was an independent LVH predictor in children with estimated GFR (eGFR) ≥45 mL/min per 1.73 m2. A recent prospective cohort study found that high FGF23 was borderline associated with high left ventricular mass index (LVMI) (β = 1.8, p = 0.06) in children with CKD and strongly associated with impaired diastolic function over time (β = −0.43, p = 0.01).9 Limited studies on FGF23 in pediatric CKD and its role as a biomarker of CVD warrant further investigation.
The objective of this study was to investigate FGF23 as a biomarker to assess CVD in pediatric CKD. To the best of our knowledge, this is among the first study using FGF23 as a diagnostic marker to assess CVD in children with CKD.
Materials and Methods
Participants
This cross-sectional study involved children with CKD stages 2 to 5D in Dr. Sardjito General Hospital, Yogyakarta, Indonesia, a regional referral hospital for Yogyakarta and southern Central Java, from November 2018 to March 2019. Eligible subjects aged 2 to 18 years were diagnosed with CKD based on Kidney Disease Improving Global Outcomes (KDIGO) 2012.10 Subjects with congenital heart diseases, acquired heart diseases (eg, rheumatic heart disease, Kawasaki disease, and myocarditis), or malignancy of the kidneys were excluded.
The research was conducted in ethical accordance with the World Medical Association Declaration of Helsinki. The study was approved by the Dr. Sardjito General Hospital Institutional Review Board and the Medical and Health Research Ethics Committee Faculty of Medicine, Public Health and Nursing Universitas Gadjah Mada (KE/FK/251/EC/2018). All patients’ caregivers were provided with written informed consent. Complete demographic and clinical data were obtained by the doctors during an outpatient visit or hospital admission.
Echocardiographic Assessment
Echocardiography was done by a pediatric cardiologist who was masked to any patient-specific clinical information. Echocardiography was done using USG Phillips Affiniti 70®. Criteria for LVH in this study was determined based on an increase of LVMI and relative wall thickness (RWT). Left ventricular mass index (LVMI) was determined by the following formula: left ventricle mass (LVM)/body surface area (g/m2). Left ventricular mass (LVM) was calculated by 0.8 ×(1.04 ([left ventricular end-diastolic (LVED) + posterior wall thickness (PW) + interventricular septum (IVS)]3 − LVED) + 0.6 g. Relative wall thickness (RWT) was calculated by 2 × PW/LVED.11 Systolic function was measured by deriving left ventricular ejection fraction (LVEF) as calculated by ((end diastolic diameter-end systolic diameter)/end diastolic diameter) x 100.12 Diastolic function was described by transmitral flow velocity ratio (MV E/A).3
LVMI, RWT, and LVEF were defined based on age and sex-specific reference percentiles by Diaz et al12. High LVMI was defined as LVMI ≥95th percentiles according to age and sex. High RWT was defined as RWT ≥95th percentiles according to age and sex.12 Reduced LVEF was defined as LVEF <5th percentiles. Left ventricular geometry was classified as normal (normal LVMI, normal RWT), concentric remodeling (normal LVMI, high RWT), eccentric LVH (high LVMI, normal RWT), and concentric LVH (high LVMI, high RWT).13 Severe cardiac impairment was defined with LVH and reduced systolic function.
Assays
Venous blood samples were collected in ethylene diamine tetra-acetic (EDTA)-containing vacutainers. Enzyme-linked immunosorbent assay (ELISA), quantitative sandwich enzyme immunoassay, was done to measure the level of FGF23. A specific FGF23 carboxyl-terminal (C-terminal), from Immutopics Inc., San Clemente, CA 92673, USA, was determined using immunometric enzyme assay with the measurement instruments Microplate Reader Biorad 680 (Bio-rad Laboratories Inc, CA, USA) and software Microplate Manager version 5.2.1 (Bio-rad Laboratories Inc., CA, USA). The final values of FGF23 were derived from the average of two replicates from each sample.
Clinical and Laboratory Parameters
The etiologies of CKD were categorized as glomerular disease (nephrotic syndrome, glomerulonephritis, lupus nephritis, and diabetic nephropathy), structural (obstructive uropathy, kidney aplasia/hypoplasia/dysplasia, and reflux nephropathy), and others (polycystic kidney disease [PKD] and nephrocalcinosis). eGFR was calculated with the revised Schwartz Formula 36.5 × L/Cr; GFR was expressed in mL/min per 1.73 m2 body surface area. L represents body length in centimeters, and Cr represents serum creatinine concentration in µmol/L. We recruited children with CKD stages 2 to 5D based on KDIGO staging recommendation as follows: stage 2 (eGFR = 60–89 mL/min per 1.73 m2), stage 3a (eGFR = 45–59 mL/min per 1.73 m2), stage 3b (eGFR = 30–44 mL/min per 1.73 m2), stage 4 (eGFR = 15–29 mL/min per 1.73 m2), stage 5 (eGFR <15 mL/min per 1.73 m2), and stage 5D (eGFR <15 mL/min per 1.73 m2 who underwent long-term hemodialysis or peritoneal dialysis).10 Hemoglobin, uric acid, calcium, phosphate, PTHlevels were taken from medical records at the same time when FGF23 and echocardiography was performed.
Statistical Analysis
Data were presented as a percentage for categorical variables, mean ± standard deviation (SD) for normally distributed data, and median (interquartile range) for non-normally distributed data. Univariate comparisons were analyzed by univariate logistic regression. Log transformation was performed in the case of abnormality distributed variables. P-values less than 0.05 (p <0.05) were considered statistically significant.
The receiver operating characteristic (ROC) curve was used to determine the area under curve (AUC) for identifying the presence of LVH with impaired contractility. The ROC was also used to review the presence of impaired systolic function. The optimal cutoff value of FGF23 was defined as the cutoff obtaining the highest total of sensitivity and specificity. All statistical analyses were performed using the STATA version 14.0 software.
Results
Forty-three children with CKD stages 2 to 5D were included in the study. The median age when FGF23 was tested was 12.89 (IQR 9.26–15.63) years. Almost 90% of the subjects were in advanced CKD.
Table 1 summarizes the baseline characteristics of patients in the study. The primary diagnoses of CKD were glomerular diseases (22/43, 51.16%), congenital anomalies of the kidney and urinary tract (CAKUT) (17/43, 39.53%), and others (4/43, 9.3%). The glomerular diseases included nephrotic syndrome (13/43, 27.91%), lupus nephritis (2/43, 4.65%), diabetic nephropathy (1/43, 2.33%), and other glomerulonephritis (7/43, 16.28%). CAKUT disorders included kidney aplasia/hypoplasia/dysplasia (9/43, 20.93%), obstructive uropathy (7/43, 16.28%), and reflux nephropathy (1/43, 2.33%). Others consisted of PKD (3/43, 6.98%) and bilateral nephrocalcinosis (1/43, 2.33%).
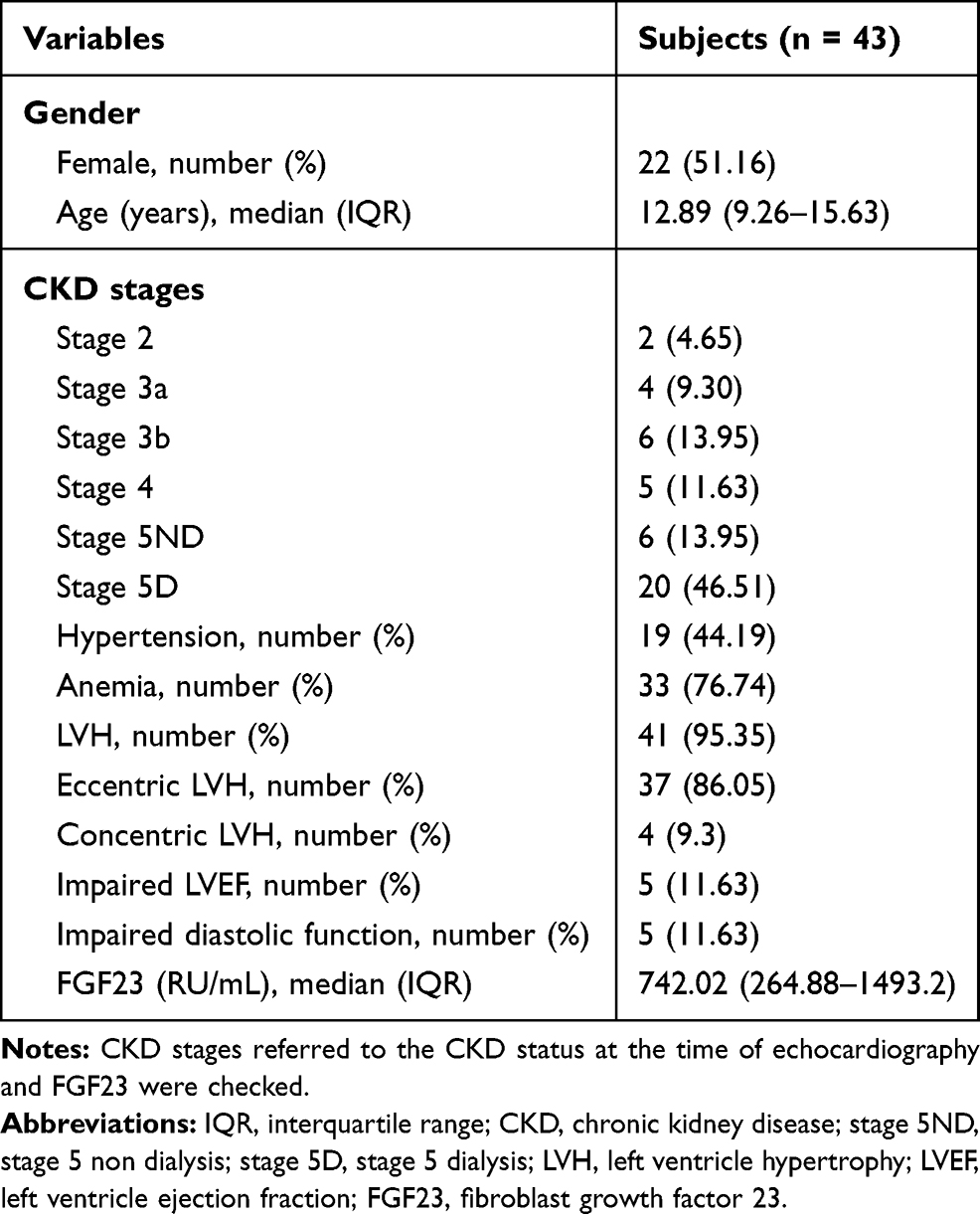 |
Table 1 Baseline Characteristics of Subjects |
Plasma FGF23, LVH, Systolic and Diastolic Functions, and CKD Progression
Table 2 shows the median values of LVMI, RWT, LVEF, and MV E/A in children with CKD stages 2 to 5D. The median concentration of FGF23 substantially increased in the higher stage of CKD. As kidney functions deteriorated, the median values of LVMI increased, but systolic and diastolic functions remained preserved. Figure 1 shows that the median values of FGF23 increased significantly in patients with LVH and impaired systolic function (p = 0.03).
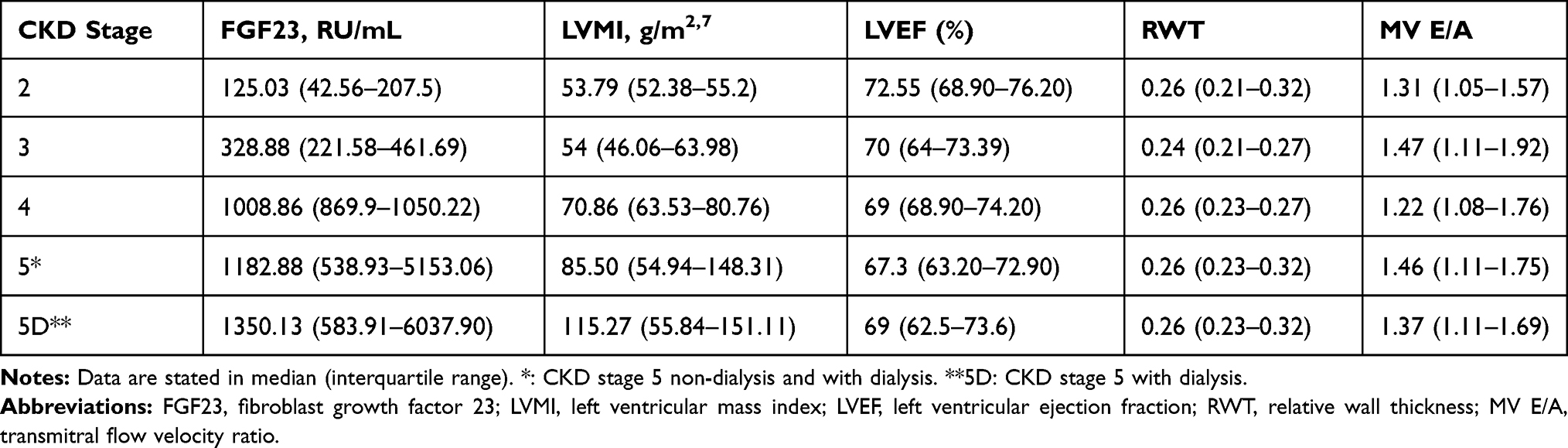 |
Table 2 FGF23, LVMI, RWT, and Systolic and Diastolic Function by CKD Stage |
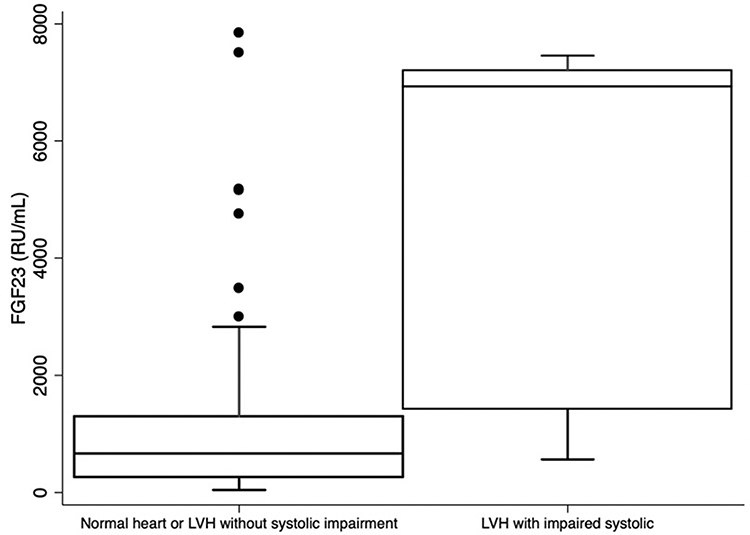 |
Figure 1 Plasma FGF23 and cardiac changes. Abbreviations: FGF23, fibroblast growth factor 23; LVH, left ventricular hypertrophy. Note: data are presented in median (interquartile range) |
Plasma FGF23 as a Biomarker for CVD in Pediatric CKD
The associations of FGF23, eGFR, hypertension, hemoglobin level, bone mineral biomarkers, and severe cardiac impairment are shown in Table 3. Univariate logistic regression showed that FGF23 was associated with LVH and systolic dysfunction (OR 2.82 (95% CI 1.11–7.15), p-value 0.03), whereas other variables did not show any association. The ROC for plasma FGF23 as a biomarker for LVH with impaired systolic is displayed in Figure 2. The AUC of FGF23 as a biomarker for low LVEF was 0.82 (95% CI 0.62–1.00). The optimal cutoff point was 1413 RU/mL. When this was used as a cutoff to define reduced ejection fraction, sensitivity and specificity were 80% and 78.95%, respectively.
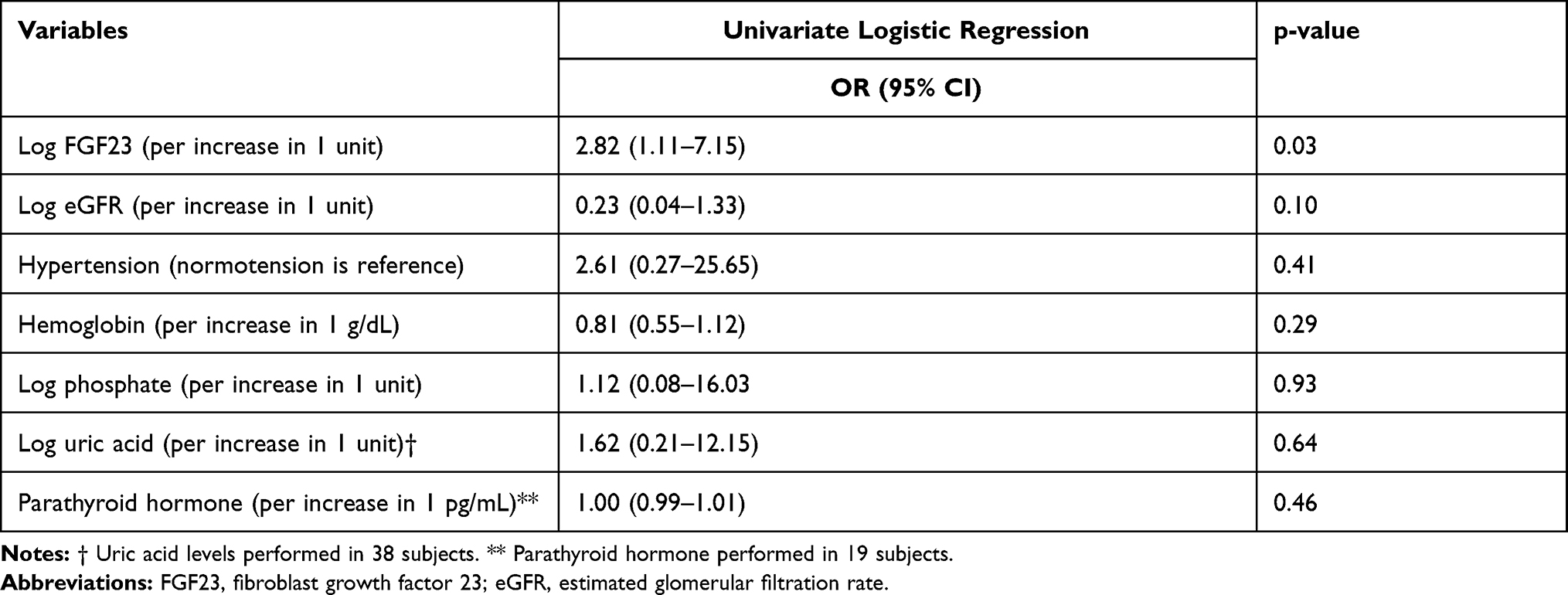 |
Table 3 Severe Cardiac Impairment Associated with FGF23, eGFR, Hypertension, Hemoglobin and Bone-Mineral Disease Markers |
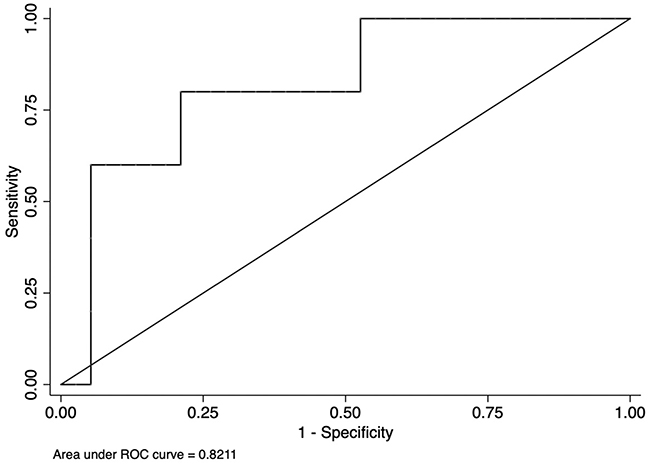 |
Figure 2 Receiver operating curve (ROC) plasma FGF23 for assessing LVH and impaired systolic function. |
Discussion
Cardiovascular disease is one of the most common complications occurring in children with CKD. The incidence and severity of CVD become more significant in patients who receive long-term dialysis. A recently published study from the pediatric kidney transplantation centers in Indonesia reported that all patients had hypertension and 42% of patients had cardiomyopathy before the kidney transplantation and the longest dialysis duration before the transplantation was 72 months.14 About 86.05% of patients in our study had LVH with eccentric type. The eccentric LVH shows the addition of serial cardiac sarcomere and is associated with volume overload, causing thickening of the cardiac wall and enlargement of the left ventricular space.15,16 Compared to previous studies reporting the number of patients with LVH in the pediatric CKD population, our current study displays a greater prevalence. Two significant CKD-related comorbidities that occurred in our study subjects, namely hypertension (44.19%) and anemia (76.74%), likely contributed to this. The Chronic Kidney Disease in Children (CKiD) study 2012 reported the prevalence of hypertension was 54% and the prevalence of anemia was 45% in children with CKD.17 Studies involving the pediatric CKD population show that most of the patients suffered from anemia and hypertension.15,18 Furthermore, the majority of the pediatric CKD cases received multiple blood transfusions before hemodialysis initiation, implying that severe anemia is commonly found in children with severe CKD in Indonesia.19 Another important point to consider is that 55.81% of our study population were at CKD stage 5D which has greater risks for having long-term hypertension and anemia, and thus, this also resulted in a significant number of severe cardiac impairments.1
The role of FGF23 as an early biomarker for LVH has been proposed by prior publications both in children8 and adults.20,21 Mitsnefes et al8 suggested the upper tertile of FGF23 level in children with CKD was 170 RU/mL, while our study displayed remarkably high FGF23 values that have started to increase as early as CKD stage 2. Compared to the study by Mitsnefes et al8 which suggested that LVH occurred in pediatric CKD patients with FGF23 level ≥100 RU/mL, our study identified one LVH case with an FGF23 level as low as 42 RU/mL who had CKD for 30 months without hypertension and anemia as comorbidities. The remarkably high values of FGF23 were also observed in an Indonesian study comprised of adult patients with CKD on hemodialysis (median 6737 rU/mL; range 958–10723).23 The level of FGF23 might be associated with dietary phosphate intake and fractional excretion of phosphate depending on areas in a given population.24 Our results raised a question as to whether the level of FGF23 in children with CKD could be influenced by local dietary habits containing high phosphate.
As far as we are aware, this is one of the first studies using FGF23 to assess LVH with impaired contractility in children with CKD. Our findings indicated FGF23 is a good biomarker to determine the presence of LVH with systolic dysfunction (AUC 0.82; 95% CI 0.62–1.00). One cross-sectional study by Nielsen et al21 in adults with end-stage kidney disease also concluded that higher FGF23 levels were associated with lower cardiac function. LVH can evolve into a maladaptive form and show a continuous process of cardiac remodeling resulting in myocyte death, decreased capillary density, and increased myocardial fibrosis. In this phase, the patients present with arrhythmias, diastolic dysfunction, and systolic dysfunction, which ultimately leads to congestive heart disease. The exact pathological mechanism of how FGF23 correlates with reduced LVEF has not been elucidated. Our study suggests that FGF23 could be used as an early biomarker to detect changes in patients with severe cardiac impairment. Mitsnefes et al8 and Seeherunvong et al22 reported strong correlations between FGF23 and LVMI. The large cohort by Mitsnefes et al8 included 587 children in CKD stages 2 to 4 with a longer CKD duration of 5 to 13 years. A retrospective study by Seeherunvong et al22 involved 26 pediatric patients on long-term hemodialysis, and thus, hypertension contributed to the increased LVMI as a common comorbidity in CKD.
The present study found the median concentration of FGF23 increased with the deterioration of kidney function, together with an increase in the LVMI, while the systolic and diastolic functions were preserved (Table 2). This holds a significant point because most children with CKD do not have multiple comorbidities that may affect the cardiac function as adults do, namely pre-existing vascular diseases, cardiac diseases, or diabetes.
This study has some strengths. Both acquisition and interpretation of the echocardiography were done blinded by one cardiologist. This is also the first study that assessed the role of FGF23 in LVH with impaired contractility in children with CKD. This study has some limitations. Firstly, although we acknowledge that cFGF23 has high intra-individual variation thereby lowering its sensitivity for diagnostic purpose,24 we used cFGF23 rather than intact FGF23 as a parameter due to the unavailability of intact FGF23 assay in our country. Secondly, the number of subjects was small, being completed in a single tertiary center. In addition, the pediatric dialysis unit has not been extensively accessible in Indonesia. Indonesia is the world’s largest island country with a large population, and its referral system is complex; thus, many patients either had deteriorated before admission25 or had not been documented. We believe the magnitude of CKD progression toward FGF23 can be more significant if the sample size was greater.
Conclusion
FGF23 might be used as an early biomarker to detect cardiac changes in pediatric CKD patients, particularly for LVH and impaired systolic function among children with CKD stage 2 and higher.
Acknowledgments
The authors would like to thank to Sri Mardilah for her assistance in organizing the patients for echocardiography as well as Cambridge Proofreading for the careful reading and editing of this manuscript. Our study was funded by research grant Dana Masyarakat (DAMAS) 2018 Faculty of Medicine, Public Health and Nursing Universitas Gadjah Mada. We declare that the funding support did not influence its outcome.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mitsnefes MM. Cardiovascular disease in children with chronic kidney disease. J Am Soc Nephrol. 2012;23(4):578–585. doi:10.1681/ASN.2011111115
2. Mitsnefes M, Flynn J, Cohn S, et al. Masked hypertension associates with left ventricular hypertrophy in children with CKD. J Am Soc Nephrol. 2010;21(1):137–144. doi:10.1681/ASN.2009060609
3. Doyon A, Haas P, Erdem S, et al. Impaired systolic and diastolic left ventricular function in children with chronic kidney disease—results from the 4C Study. Sci Rep. 2019;9(1):11462. doi:10.1038/s41598-019-46653-3
4. Scavarda VT, Pinheiro AC, Costa SD, et al. Children with chronic renal disease undergoing dialysis or conservative treatment—differences in structural and functional echocardiographic parameters. Echocardiography. 2014;31(9):1131–1137. doi:10.1111/echo.12525
5. Erben RG. Physiological actions of fibroblast growth factor-23. Front Endocrinol (Lausanne). 2018;9:267. doi:10.3389/fendo.2018.00267
6. Portale AA, Wolf M, Juppner H, et al. Disordered FGF23 and mineral metabolism in children with CKD. Clin J Am Soc Nephrol. 2014;9(2):344–353. doi:10.2215/CJN.05840513
7. Isakova T, Wahl P, Vargas GS, et al. Fibroblast growth factor 23 is elevated before parathyroid hormone and phosphate in chronic kidney disease. Kidney Int. 2011;79(12):1370–1378. doi:10.1038/ki.2011.47
8. Mitsnefes MM, Betoko A, Schneider MF, et al. FGF23 and left ventricular hypertrophy in children with CKD. Clin J Am Soc Nephrol. 2018;13(1):45–52. doi:10.2215/CJN.02110217
9. Tranaeus Lindblad Y, Olauson H, Vavilis G, et al. The FGF23-Klotho axis and cardiac tissue Doppler imaging in pediatric chronic kidney disease—a prospective cohort study. Pediatr Nephrol. 2018;33(1):147–157. doi:10.1007/s00467-017-3766-5
10. KDIGO CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int (Suppl). 2013;3:1–150.
11. Park MK. Park: Pediatric Cardiology for Practitioners.
12. Diaz A, Zocalo Y, Bia D. Reference intervals and percentile curves of echocardiographic left ventricular mass, relative wall thickness and ejection fraction in healthy children and adolescents. Pediatr Cardiol. 2019;40(2):283–301. doi:10.1007/s00246-018-2000-y
13. Faul C, Amaral AP, Oskouei B, et al. FGF23 induces left ventricular hypertrophy. J Clin Invest. 2011;121(11):4393–4408. doi:10.1172/JCI46122
14. Ambarsari CG, Hidayati EL, Trihono PP, et al. Experience of the first 6 years of pediatric kidney transplantation in Indonesia: a multicenter retrospective study. Pediatr Transplant. 2020;24(8):e13812. doi:10.1111/petr.13812
15. Shroff R, Weaver DJ
16. Wong CJ, Moxey-Mims M, Jerry-Fulker J, Warady BA, Furth SL. CKiD (CKD in children) prospective cohort study: a review of current findings. Am J Kidney Dis. 2012;60(6):1002–1011. doi:10.1053/j.ajkd.2012.07.018
17. Ambarsari CG, Trihono PP, Kadaristiana A, et al. Five-year experience of continuous ambulatory peritoneal dialysis in children: a single center experience in a developing country. Med J Indones. 2019;28(4):329–337. doi:10.13181/mji.v28i4.3807
18. Ambarsari CG, Trihono PP, Kadaristiana A, et al. Low-dose maintenance intravenous iron therapy can prevent anemia in children with end-stage renal disease undergoing chronic hemodialysis. Int J Nephrol. 2020;2020:1–8. doi:10.1155/2020/3067453
19. Rahman M, Xie D, Feldman HI, et al. Association between chronic kidney disease progression and cardiovascular disease: results from the CRIC Study. Am J Nephrol. 2014;40(5):399–407. doi:10.1159/000368915
20. Nielsen TL, Plesner LL, Warming PE, et al. FGF23 in hemodialysis patients is associated with left ventricular hypertrophy and reduced ejection fraction. Nefrologia. 2019;39(3):258–268. doi:10.1016/j.nefro.2018.10.007
21. Seeherunvong W, Abitbol CL, Chandar J, et al. Fibroblast Growth Factor 23 and left ventricular hypertrophy in children on dialysis. Pediatr Nephrol. 2012;27(11):2129–2136. doi:10.1007/s00467-012-2224-7
22. Rudiansyah M, Lubis L, Bandiara R, et al. The correlation of fibroblast growth factor 23 (FGF23) and iron profile in chronic kidney disease patients on dialysis with anemia. Sys Rev Pharm. 2020;11(6):780–784. doi:10.31838/srp.2020.6.114
23. Yuen SN, Kramer H, Luke A, et al. Fibroblast growth factor-23 (FGF-23) levels differ across populations by degree of industrialization. J Clin Endocrinol Metab. 2016;101(5):2246–2253. doi:10.1210/jc.2015-3558
24. Smith ER, Cai MM, McMahon LP, Holt SG. Biological Variability of Plasma Intact and C-Terminal FGF23 Measurements. J Clin Endocrinol Metab. 2012;97(9):3357–3365. doi:10.1210/jc.2012-1811
25. Ambarsari CG, Sindih RM, Saraswati M, Trihono PP. Delayed admission and management of pediatric acute kidney injury and multiple organ dysfunction syndrome in children with multiple wasp stings: a case series. Case Rep Nephrol Dial. 2019;9(3):137–148. doi:10.1159/000504043
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.