Back to Journals » Psychology Research and Behavior Management » Volume 12
High carbonated soft drink consumption is associated with externalizing but not internalizing behaviours among university students in five ASEAN states
Received 21 March 2019
Accepted for publication 28 June 2019
Published 29 July 2019 Volume 2019:12 Pages 585—592
DOI https://doi.org/10.2147/PRBM.S209611
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Supa Pengpid,1,2 Karl Peltzer2
1ASEAN Institute for Health Development, Mahidol University, Salaya, Nakhonpathom, Thailand; 2Deputy Vice Chancellor Research and Innovation Office, North West University, Potchefstroom, South Africa
Background: The investigation aimed to estimate the association between carbonated soft drink consumption frequency and externalizing and internalizing behaviour among university students in five ASEAN counties.
Methods: A cross-sectional survey included 3353 university students from Indonesia, Malaysia, Myanmar, Thailand and Vietnam, median age 20 years (interquartile range 3 years).
Results: In all five ASEAN countries, the study found a prevalence no soft drink consumption in the past 30 days of 20.3%, less than one time a day 44.7%, once a day 25.4% and two or more times a day 9.6%. In the adjusted logistic regression analysis, higher frequency of soft drink consumption (one and/or two or more times a day) was associated with externalizing behaviour (in physical fight, injury, current tobacco use, problem drinking, drug use, pathological internet use and gambling behaviour), and higher frequency of soft drink consumption (two or more times a day) was associated with depression in females, but no association was found for the general student population in relation to internalizing behaviour (depression, posttraumatic stress disorder, suicidal ideation, suicide plan, suicide attempt and sleeping problem).
Conclusions: Findings suggest that carbonated soft drink consumption is associated with a number of externalizing but not internalizing health risk behaviours.
Keywords: soft drink consumption, addictive behaviour, substance use, mental distress, university students, ASEAN
Introduction
Soft drink consumption has been associated with increased body weight, oral and medical problems.1 Less is known about soft drink consumption and health risk behaviours. Among adolescents, an association between soft drink consumption and health risk behaviours, including substance use, interpersonal violence, injury and poor mental health was found.2–9 Little is known about the relationship between soft drink consumption and health risk behaviours, including substance use and poor mental health, among emerging adults in Asia.
In a sample of adults in South Australia, Shi et al10 found that high levels of soft drink consumption were positively associated with depression, stress-related problem, suicidal ideation, psychological distress and a current mental health condition.
In a study among young women in Texas, USA, “Posttraumatic Stress Disorder (PTSD) symptoms were associated with increased frequency of soda consumption.”11 Several studies found an association between soft drink consumption and depression, eg among female university students in the UK,12 among adult women in Finland,13 university students in Ethiopia,14 among adults in USA,15 China,16 Indonesia,17 and Brazil.18 A study among adults in Indonesia found an association between soft drink consumption and insomnia).19
To our knowledge we could not find any study investigation soft drink consumption and health risk behaviours in emerging adults in Asia. The aimed at investigating the relationship between soft drink consumption frequency and externalizing and internalizing behaviours among university students in five ASEAN countries.
Methods
Sample and procedure
A cross-sectional survey included 3266 university students from five ASEAN countries (Indonesia: Yogyakarta, Malaysia: Kuala Lumpur, Myanmar: Yangon, Thailand: MahaSarakham and Vietnam: Hanoi), median age 20 years (Interquartile Range 3 years). Details of the sampling and data collection procedures have been described previously.20 Briefly, one university per country was selected by purposeful sampling. In each university, a stratified random sampling procedure was used to randomly select undergraduate students for participating in the survey.20
In a class room setting, external research assistants administered a questionnaire and took anthropometric measurements, after informed consent had been obtained from all participating students.20 Ethics approvals were obtained from all participating universities: “University of Malaya Medical Ethics committee (MECID 201412–905)”, “Research and Ethical Committee of University of Medicine 1”, “Committee for Research Ethics (Social Sciences) of Mahidol University (MU-SSIRB 2015/116(B2)”, “Committee of Research Ethics of Hanoi School of Public Health”, and “Research Ethics Committee, Faculty of Medicine and Health Sciences, Universitas Muhammadiyah Yogyakarta.”
Measures
Outcome variables
Physical fighting was assessed with one item: “During the past 12 months, how many times were you in a physical fight?” Responses were grouped into 0=0 times and 1=1 or more times.21
Injury requiring medical attention was assessed with three questions: 1) “In the past 12 months, have you been involved in a road traffic crash as a driver, passenger, pedestrian, or cyclist?” 2) “Did you have any injuries in this road traffic crash which required medical attention?” 3) “In the past 12 months, were you injured accidentally, other than the road traffic crashes which required medical attention?”22
Tobacco use was assessed with one question: “Do you currently use one or more of the following tobacco products (cigarettes, snuff, chewing tobacco, cigars, etc.)?” (Yes, No).23
Problem drinking was assessed with the “Alcohol Use Disorders Identification Test–Consumption (AUDIT-C)”.24 (Cronbach alpha was 0.89).
Drug use (in the past 12 months) was measured with one question: “How often have you taken drugs in the past 12 months, other than prescribed by the health care provider?” Responses were grouped into 0=0 times and 1=1 or more times.20
Pathological internet use was measured with the “Young Diagnostic Questionnaire for Internet Addiction (YDQ).”25 (Cronbach alpha 0.70).
Gambling behaviour was measured with the “South Oaks Gambling Screen (SOGS),”26 and classified as 0=none and any of nine gambling behaviours=1. (Cronbach alpha 0.87)
Depressive symptoms were measured with the “Center for Epidemiologic Studies Depression Scale (CES-D, 10 items)”, with scores of 15 or more classifying severe depression.27 (Cronbach’s α =0.69).
Posttraumatic stress disorder (PTSD) was assessed with a 7-item questionnaire on past month PTSD symptoms.28 (Cronbach alpha =0.77).
Suicidal behaviours (ever ideation, plan and attempt) were adapted from a study by Osman et al.29
Sleeping problems were defined as “severe or extreme having a problem with sleeping, such as falling asleep, waking up frequently during the night, or waking up too early in the morning in the past 30 days?”30
Exposure variables
“Soft drink consumption” was measured with the question, “During the past 30 days, how many times per day did you usually drink carbonated soft drinks (do not include diet soft drinks)?”21 Responses were grouped into 1=I did not drink carbonated soft drinks during the past 30 days, 2=Less than one time per day, 3= 1 time per day, and 4= 2 times per day, or 3 times per day, or 4 times per day, or 5 or more times per day.21
Confounding variables
Socio-demographic items included country, age, sex, and subjective wealth status.20
Social support was assessed with three questions from the “Social Support Questionnaire.”31 (Cronbach alpha 0.65).
Body mass index (BMI) was assessed with anthropometric measures, and classified following Asian criteria: “underweight (<18.50 kg/m2), normal weight (18.50 to 22.99 kg/m2), overweight (23.00 to 24.99 kg/m2), and 25.00+ kg/m2 as obese.”32
Physical activity was assessed with the “International Physical Activity Questionnaire (IPAQ) short-form questionnaire”, and classified as “low, moderate and high physical activity.”33,34
Data analysis
Descriptive statistics were applied in order to present tabulations. Logistic regression was utilized to estimate the odds ratios (with 95% confidence interval=CI) for each behaviour outcome separately, in model 1 the outcome was adjusted by country and in model 2 the outcome was adjusted for country, sex, age, wealth status, social support, body weight status, and physical activity. Potential multi-collinearity between variables was assessed with variance inflation factors, none of which exceeded a value of 1.5. P<0.05 was considered significant. Missing data were not included in the analysis. All statistical procedures were performed using STATA software version 15.0 (Stata Corporation, College Station, TX, USA).
Results
Sample characteristics
The study sample included 3353 university students (median age 20 years, interquartile range=3) from Indonesia (n=231), Malaysia (n=1023), Myanmar (n=485), Thailand (n=799) and Vietnam (n=815). Majority of the participants (62.9%) were female and had a low wealth status (67.0%). Regarding externalizing behaviour, 6.5% of the students reported having been in a physical fight in the past year, 15.4% had sustained a serious injury in the past year, 3.3% were current tobacco users, 15.8% problem drinkers, 8.4% had used drugs in the past year, 35.5% had engaged in pathological internet use, 3.1% gambled weekly, and 55.0 skipped breakfast. In terms of internalizing behaviour, 10.6% had depression, 24.4% PTSD, 11.6% suicidal ideation, 5.0% had a suicide plan, 2.8% had attempted suicide, and 4.5% had sleep problems. In all five ASEAN countries, the study found a prevalence no soft drink consumption in the past 30 days of 20.3%, less than one time a day 44.7%, once a day 25.4% and two or more times a day 9.6%. (see Table 1).
 |
Table 1 Sample characteristics of Association of Southeast Asian Nations university students |
Associations between soft drink consumption frequency and externalizing behaviours
In the final adjusted logistic regression analysis (model 2), higher frequency of soft drink consumption (one and/or two or more times a day) was associated with in physical fight (Adjusted Odds Ratio-AOR: 1.87, Confidence Interval-CI: 1.23, 2.87), injury (AOR: 1.94, CI: 1.42, 2.65), current tobacco use (AOR: 4.74, CI: 1.93, 11.65), problem drinking (AOR: 4.00, CI: 2.73, 5.86), drug use (AOR: 2.44, CI: 1,45, 4.09), pathological internet use (AOR: 1.88, CI: 1.41, 2.51) and gambling behaviour (AOR: 2.83, CI: 1.30, 6.16) (see Table 2).
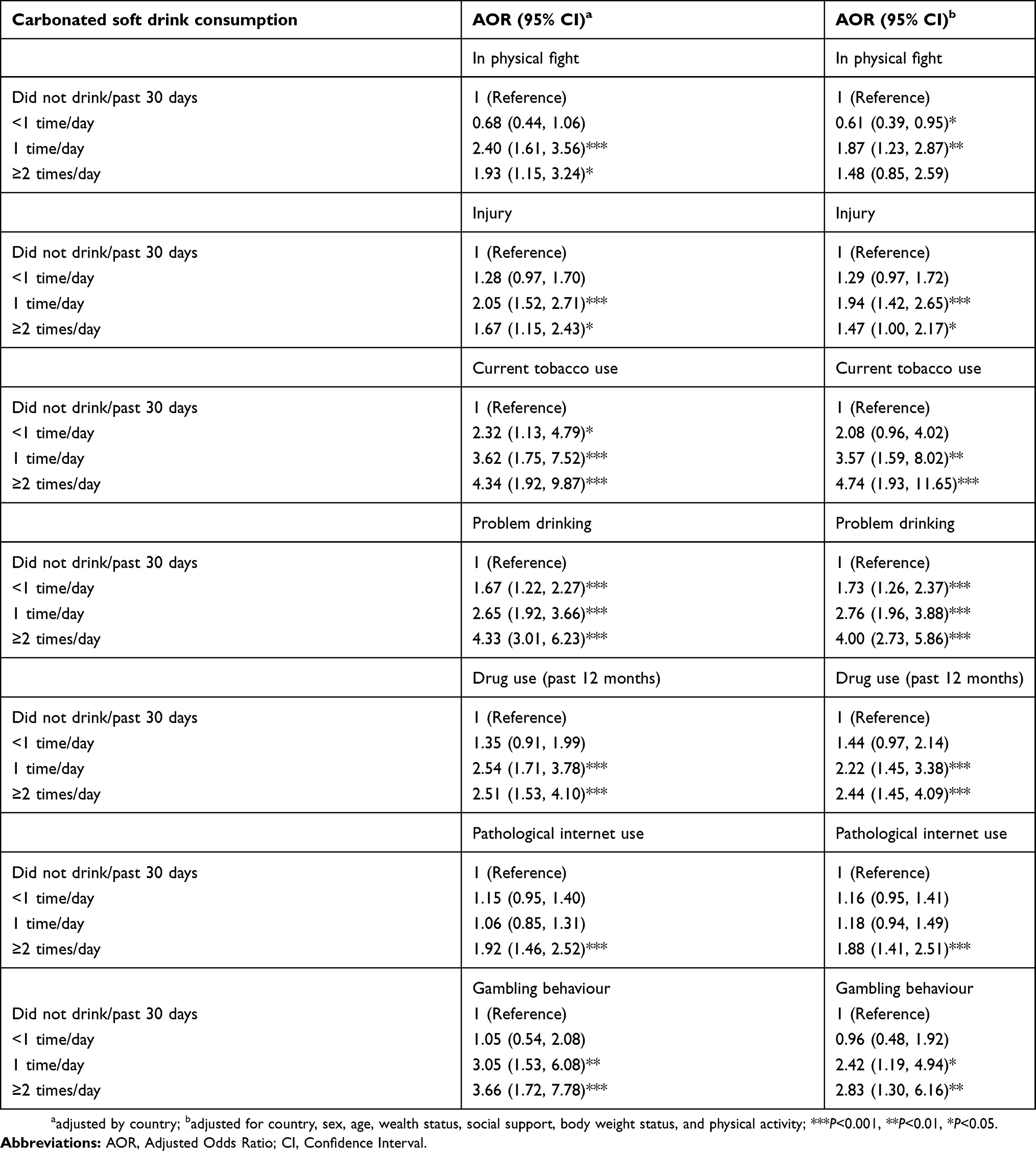 |
Table 2 Associations between soft drink use frequency and externalizing behaviours |
Associations between soft drink consumption frequency and internalizing behaviours
In the final adjusted logistic regression analysis (model 2), higher frequency of soft drink consumption (two or more times a day) was associated with depression in females (AOR: 1.34, CI 1.06, 1.67; analysis not shown), but no association was found for the general student population in relation to depression (AOR: 1.21, CI: 0.79, 1.86), PTSD (AOR: 1.01, CI: 0.73, 1.40), suicidal ideation (AOR: 1.16, CI: 0.77, 1.77) suicide plan (AOR: 1.23, CI: 0.72, 2.11), suicide attempt (AOR: 1.10, CI: 0.56, 2.17) and sleeping problem (AOR: 0.44, CI: 0.19, 1.02) (see Table 3).
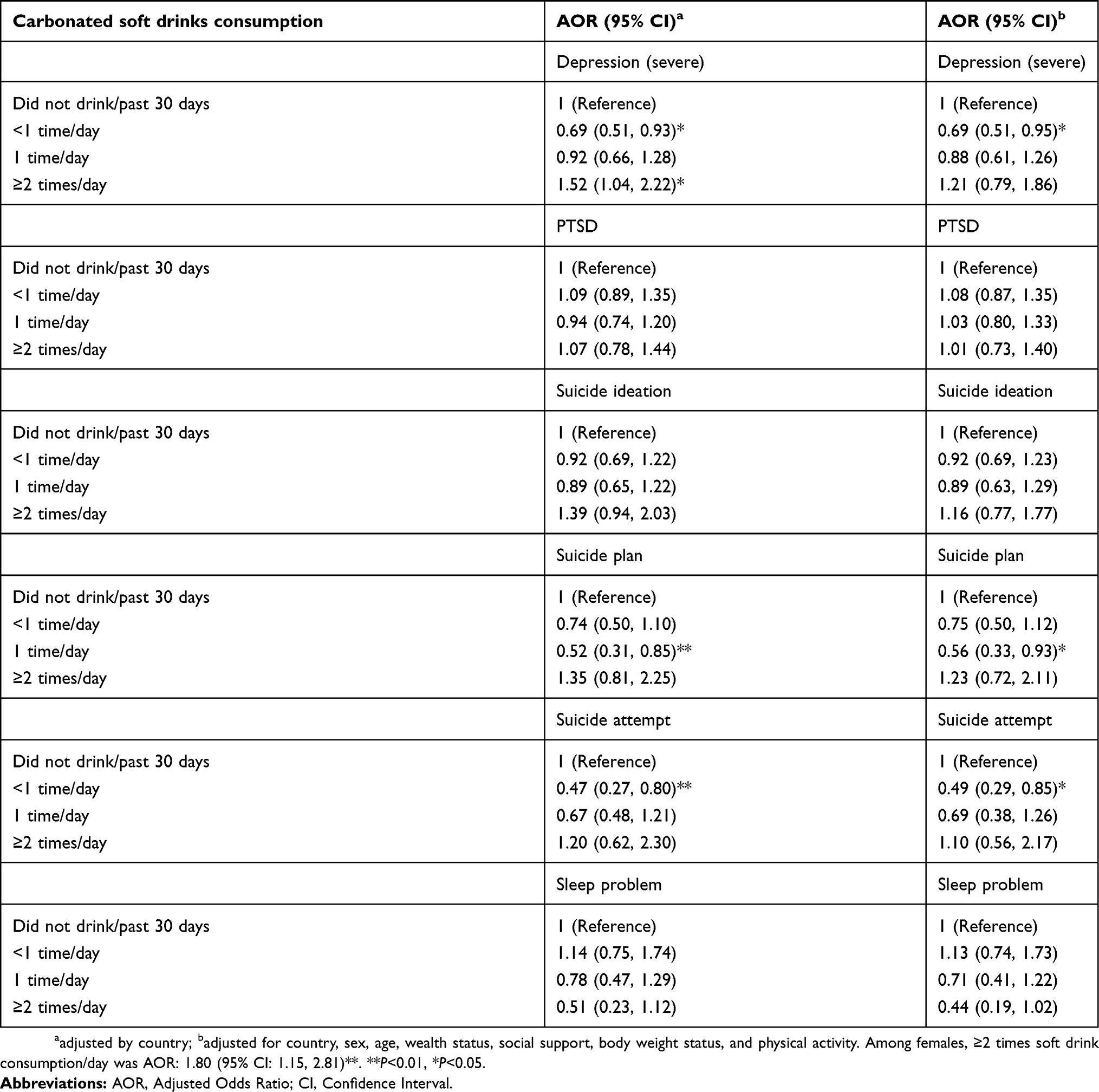 |
Table 3 Associations between soft drink use frequency and internalizing behaviours |
Discussion
This investigation gives new data on the association between soft drink consumption and externalizing and internalizing behaviours among university students in five ASEAN countries. The study found a prevalence of once or more times daily soft drink consumption of 35.0%, which is lower than the prevalence of at least once daily soft drink consumption in 53 low- and middle-income countries among school-going adolescents (54.3%).35
This investigation found a consistent association between higher frequency of soft drink consumption and externalizing behaviours (in physical fight, injury, tobacco use, problem drinking, drug use, pathological internet use and gambling behaviour). These findings are consistent with a number of studies among adolescents2-4,6–9 and novel for emerging adults. In agreement with studies among adolescents,2,8 the strongest associations of soft drink consumption were found for substance use (alcohol, tobacco and drug use) in this study. Soft drinks contain a lot of sugar and other additives, such as caffeine,2 which may be linked to other addictive substances, such as alcohol and nicotine. Therefore, it could be possible that the combined use of these substances increases each other’s addictive effects. Health risk behaviours tend to cluster, and it therefore could be that soft drink consumption is “a marker of other dietary and life-style factors.10
In agreement with two previous studies,12,13 this study found that frequent soft drink consumption among female students increased the odds for depression. The high sugar consumption from soft drinks may affect women differently than men in relation to depression.15 However, no associations were found between soft drink consumption and other internalizing behaviours (PTSD, suicidal behaviour, and sleep problem), contrary to some previous studies.10,11,19
This finding supports addressing the clustering of soft drink consumption with various externalizing behaviours in university health promotion intervention in this population. Further, longitudinal studies are needed to confirm the link between soft drink consumption frequency and externalizing and internalizing behaviours among university students. In addition, more research is needed to investigate the possible mechanisms between soft drink consumption frequency and externalizing and internalizing behaviours in emerging adults.
Study limitations
The study was cross-sectional, which precludes causal inferences. Variables measured was by self-report and may have been underreported. Several study indicators were assessed with single items, and future studies should employ more comprehensive measures.
Conclusion
Study findings concur with previous results that showed an association between higher frequency of soft drink consumption and externalizing behaviours (in physical fight, injury, current tobacco use, problem drinking, drug use, pathological internet use and gambling behaviour), and higher frequency of soft drink consumption (two or more times a day) was associated with depression in females, but no association was found for the general student population in relation to internalizing behaviour (depression, PTSD, suicidal ideation, suicide plan, suicide attempt and sleeping problem).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Vartanian LR, Schwartz MB, Brownell KD. Effects of soft drink consumption on nutrition and health: a systematic review and meta-analysis. Am J Public Health. 2007;97(4):667–675. doi:10.2105/AJPH.2005.083782
2. Bruckauf Z, Walsh SD. Adolescents’ multiple and individual risk behaviors: examining the link with excessive sugar consumption across 26 industrialized countries. Soc Sci Med. 2018;216:133–141. doi:10.1016/j.socscimed.2018.08.029.
3. Pengpid S, Peltzer K. Alcohol use and misuse among school-going adolescents in Thailand: results of a national survey in 2015. Int J Environ Res Public Health. 2019;16(11):
4. Solnick SJ, Hemenway D. Soft drinks, aggression and suicidal behaviour in US high school students. Int J Inj Contr Saf Promot. 2014;21(3):266–273. doi:10.1080/17457300.2013.815631.
5. Jacob L, Stubbs B, Koyanagi A. Consumption of carbonated soft drinks and suicide attempts among 105,061 adolescents aged 12–15 years from 6 high-income, 22 middle-income, and 4 low-income countries. Clin Nutr. 2019. pii: S0261-5614(19)30142-6. doi:10.1016/j.clnu.2019.03.028.
6. Pan X, Zhang C, Shi Z. Soft drink and sweet food consumption and suicidal behaviours among Chinese adolescents. Acta Paediatr. 2011;100(11):e215–22. doi:10.1111/j.1651-2227.2011.02369.x.
7. Terry-McElrath YM, OʼMalley PM, Johnston LD. Energy drinks, soft drinks, and substance use among United States secondary school students. J Addict Med. 2014;8(1):6–13. doi:10.1097/01.ADM.0000435322.07020.53.
8. Ziegler AM, Temple JL. Soda consumption is associated with risk-taking behaviors in adolescents. Am J Health Behav. 2015;39(6):761–771. doi:10.5993/AJHB.39.6.3.
9. Peltzer K, Pengpid S. Unintentional injuries and psychosocial correlates among in-school adolescents in Malaysia. Int J Environ Res Public Health. 2015;12(11):14936–14947. doi:10.3390/ijerph121114936.
10. Shi Z, Taylor AW, Wittert G, Goldney R, Gill TK. Soft drink consumption and mental health problems among adults in Australia. Public Health Nutr. 2010;13(7):1073–1079. doi:10.1017/S1368980009993132.
11. Hirth JM, Rahman M, Berenson AB. The association of posttraumatic stress disorder with fast food and soda consumption and unhealthy weight loss behaviors among young women. J Women’s Health. 2011;20(8):1141–1149. doi:10.1089/jwh.2010.2675.
12. El Ansari W, Adetunji H, Oskrochi R. Food and mental health: relationship between food and perceived stress and depressive symptoms among university students in the United Kingdom. Cent Eur J Public Health. 2014;22(2):90–97. doi:10.21101/cejph.a3941.
13. Rintamäki R, Kaplas N, Männistö S, et al. Difference in diet between a general population national representative sample and individuals with alcohol use disorders, but not individuals with depressive or anxiety disorders. Nordic J Psychiat. 2014;68(6):391–400. doi:10.3109/08039488.2013.851736.
14. Sailaja B, Gezahegn B. Assessment of depressive symptoms related to overconsumption of soft drinks among university students, Hawassa University, Hawassa, Ethiopia. Int J Nurs Educ Res. 2015;3(4):393–399. doi:10.5958/2454-2660.2015.00029.0
15. Burleson C, Anderson K, Copeland Z, Karcs C, Sullivan KL. Consumption of sugar-sweetened beverages associated with increased odds of depression. Epidemiol Open J. 2016;1(2):53–58. Openventio Publishers. doi: 10.17140/EPOJ-1-107 Available from:. doi: https://digitalcommons.georgiasouthern.edu/epid-facpubs/71.
16. Yu B, He H, Zhang Q, et al. Soft drink consumption is associated with depressive symptoms among adults in China. J Affect Dis. 2015;172:422–427. doi:10.1016/j.jad.2014.10.026.
17. Peltzer K, Pengpid S. High prevalence of depressive symptoms in a national sample of adults in Indonesia: childhood adversity, sociodemographic factors and health risk behaviour. Asian J Psychiat. 2018;33:52–59. doi:10.1016/j.ajp.2018.03.017.
18. Barros MBA, Lima MG, Azevedo RCS, et al. Depression and health behaviors in Brazilian adults - PNS 2013. Rev De Saude Publica. 2017;51((suppl 1)):8s. doi:10.1590/S1518-8787.2017051000084.
19. Peltzer K, Pengpid S. Prevalence, social and health correlates of insomnia among persons 15 years and older in Indonesia. Psychol Health Med. 2019;1–12. doi:10.1080/13548506.2019.1566621.
20. Huu TH, Le Viet A, Peltzer K, Pengpid S, Low WY, Win HH. Childhood emotional, physical, and sexual abuse and associations with mental health and health risk behaviours among university students in ASEAN. Child Stud Asia-Pacific Contexts. 2017;7(1):15–26. doi:10.5723/csac.2017.7.1.015
21. World Health Organization (WHO). Global School-based Student Health Survey (GSHS), 2019. Available from: www.who.int/ncds/surveillance/gshs/en/
22. World Health Organization (WHO). Non-Communicable Diseases and their Risk Factors. STEPS Optional Modules, 2019. Available from: https://www.who.int/ncds/surveillance/steps/riskfactor/modules/en/
23. World Health Organization (WHO). Guidelines for Controlling and Monitoring the Tobacco Epidemic. Geneva, Switzerland: WHO; 1998.
24. Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA. The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Ambulatory Care Quality Improvement Project (ACQUIP). Alcohol Use Disorders Identification Test. Arch Inter Med. 1998;158:1789–1795. doi:10.1001/archinte.158.16.1789
25. Young KS. Internet Addiction: Symptoms, Evaluation and Treatment. In: Innovations in Clinical Practice, 1999. A Source Book 17. Sarasota, FL: Professional Resource Press.
26. Lesieur HR, Blume SB. The South Oaks Gambling Screen (SOGS): a new instrument for the identification of pathological gamblers. Am J Psychiat. 1987;144:1184–1188. doi:10.1176/ajp.144.9.1184
27. Andresen EM, Malmgren JA, Carter WB, Patrick DL. Screening for depression in well older adults: evaluation of a short form of the CES-D (Center for Epidemiologic Studies Depression Scale). Am J Prev Med. 1994;10(2):77–84.
28. Kimerling R, Ouimette P, Prins A, et al. Brief report: utility of a short screening scale for DSM-IV PTSD in primary care. J Gen Inter Med. 2006;21:65–67. doi:10.1111/j.1525-1497.2005.00292.x
29. Osman A, Bagge CL, Gutierrez PM, Konick LC, Kopper BA, Barrios FX. The Suicidal Behaviors Questionnaire-Revised (SBQ-R): validation with clinical and nonclinical samples. Assessment. 2001;8:443–454. doi:10.1177/107319110100800409
30. Stranges S, Tigbe W, Gómez-Olivé FX, Thorogood M, Kandala NB. Sleep problems: an emerging global epidemic? Findings from the INDEPTH WHO-SAGE study among more than 40,000 older adults from 8 countries across Africa and Asia. Sleep. 2012;35:1173–1181. doi:10.5665/sleep.2012
31. Brock D, Sarason I, Sarason B, Pierce G. Simultaneous assessment of perceived global and relationship-specific support. J Soc Pers Relat. 1996;13(1):143–152. doi:10.1177/0265407596131008
32. Kanazawa M, Yoshiike N, Osaka T, Numba Y, Zimmet P, Inoue S. Criteria and classification of obesity in Japan and Asia-Oceania. World Rev Nutr Diet. 2005;94:1–12.
33. Craig CL, Marshall AL, Sjöström M, et al. International physical activity questionnaire: 12-Country reliability and validity. Med Sci Sports Exerc. 2003;35:1381–1395. doi:10.1249/01.MSS.0000078924.61453.FB
34. International Physical Activity Questionnaire (IPAQ) Research Committee. International Physical Activity Questionnaire. 2016. Available from: https://sites.google.com/site/theipaq/scoring-protocol.
35. Yang L, Bovet P, Liu Y, et al. Consumption of carbonated soft drinks among young adolescents aged 12 to 15 years in 53 low- and middle-income countries. Am J Public Health. 2017;107(7):1095–1100. doi:10.2105/AJPH.2017.303762.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.