")
Back to Journals » Patient Preference and Adherence » Volume 16
Hierarchical Analysis of Contraceptive Compliance Among Rural Reproductive Age Group Women in Awi Zone, Northwest Ethiopia
Authors Mitiku HD , Lemma MW, Chekole YB, Chekole YT
Received 12 March 2022
Accepted for publication 13 May 2022
Published 24 May 2022 Volume 2022:16 Pages 1279—1293
DOI https://doi.org/10.2147/PPA.S366097
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Habtamu Dessie Mitiku,1 Muluken Wondemnew Lemma,2 Yenework Belayneh Chekole,2 Yonatal Tarkegn Chekole3
1Department of Statistics, College of Natural and Computational Science, Injibara University, Injibara, Ethiopia; 2Department of Computer Science, College of Natural and Computational Science, Injibara University, Injibara, Ethiopia; 3General Practitioner, Injibara General Hospital, Injibara, Ethiopia
Correspondence: Habtamu Dessie Mitiku, Email [email protected]
Background: Contraceptive compliance has become a major health concern around the globe, particularly in rural parts of Ethiopia. Therefore, this study aimed to assess contraceptive compliance among rural women of the reproductive age group in the Awi zone, Northwest Ethiopia.
Methods: A community-based cross-sectional study was conducted on 2341sampled rural women’s reproductive age group from Jan to April 30; 2021G.C. Multistage random sampling was employed. A multilevel logistic regression model was used to identify the predictors of contraceptive compliance, which allows us to account for the random component. Intra-cluster correlation coefficient (ICC) statistics were also computed to measure the variation between clusters.
Results: Results showed that prevalence of contraceptive compliance in the selected districts of Awi zone was 17.1%. At individual level, women’s aged 35– 49 (AOR = 0.50, 95% CI 0.28, 0.90), married women’s (AOR = 8.81, 95% CI 4.62, 16.66), had 1 to 2 living children (AOR = 1.15, 95% CI 1.06, 1.40), women’s work status hard (AOR = 5.80, 95% CI 2.85, 11.82) and moderate (AOR = 4.71, 95% CI 2.39, 9.28), long-acting (AOR = 1.84, 95% CI1.28, 2.64) and positive attitude (AOR = 2.71, 95% CI1.16, 6.33) and at hierarchical level (group level), mass media exposure (AOR = 1.78, 95% CI 1.32, 2.41) and enforcement exposure (AOR = 1.77, 95% CI 1.19, 2.65) were significant factors of contraceptive compliance. Moreover, results for the intra-class correlation coefficient show that variation exists between clusters.
Conclusion: Individual-level (women’s age, married women’s, number of living children, women’s work status, type of contraceptive method and attitude) and community-level (mass media exposure and enforcement exposure) were found to be significant factors associated with compliance in Awi zone.
Keywords: rural women, compliance, Awi zone, multilevel analysis, adherence, contraception
Introduction
Contraception (birth control) is a mechanism for preventing pregnancy by interfering with the normal process of ovulation, fertilization, and implantation. The prevalence of particular methods has changed slowly at the global and regional levels. Globally in 2019, among 1.9 billion women of reproductive age (15–49 years), 1.1 billion require family planning.1 Among these contraceptives, the prevalence of married or in-union women aged 15 to 49 years in the world is 922 million, while 47 m clients withdraw due to different reasons, and contraceptive methods most commonly used vary widely by region.1
In particular, Africa also experiences different contraceptive methods aimed at reducing maternal mortality and morbidity. Besides this effort, contraceptive prevalence among women married or in-union women aged 15 to 49 years is 36%, which is the lowest compared to other parts of the world.2 According to the3 study, the average number of unpracticed women from any contraceptive methods to avoid pregnancy, while they had an interest is 40.9%. Evidence from the previous studies shows that the reasons for the nonuse of contraceptives were “health concerns” and “infrequent sex,” but the prevalence of each reason varied substantially across countries.3
Sub-Saharan Africa also experienced only 17%4 and injectable were the most practiced method of contraception with a prevalence of 9.6% among women of reproductive age1 and close to 214 million women are currently not using a modern contraceptive method.5 Indeed, there were wide variations in the method used across countries.
Contraceptive in Ethiopia setting looks, evidence from EMDHS 2019 survey indicated that the contraceptive prevalence among women married or in-union women aged 15 to 49 years from 2016 to 2019 is increased from 36% to 41%.6 The country Ethiopia tried to design a strategy to succeed in the 2030 millennium development goal for reducing women’s burden in this regard. To succeed in this effort, Ethiopia established the first family planning program in the 1960s.7 According to Ethiopian demographic and health survey 2016 report, modern methods of birth control use among married women were different across regional states, and it ranges from a low of 1% in Somali to a high of 50% in Addis Ababa. The survey also shows that around 47% of the wealthiest households used modern family planning, while 20% use the poorest households. There are several studies conducted on issues related to contraceptive preference and unmet need in different countries. For example, the report by1,6,8–11 indicates that long-acting method of family planning is better for clients concerning safety and efficacy. Similarly, other studies on users who had hard workload,12 married,3,13 women’s job category,10,12 number of living children6,12,14, attitude,15–18 the accessibility of mass media17,19,20, and enforcement by others other than women approval2–4,21,22 were significantly associated with clients preferred choice of methods. This is a clue for further investigation of the method of preference due to the above-mentioned difference. Besides, the increments of trend of using any method of family planning by married women from 8% in 2000 to 36% in 2016 and modern method use from 6% to 35%,21 the health center (group level) factor effects about rural clients were not researched yet. Moreover, countries like Ethiopian people had different cultures with limited income consequently, birth control methods play a significant role in the reduction of maternal health problems and prevention of maternal mortality.12,23 Therefore, providing preferred methods of contraceptive for women reproductive age group is important to preventing mother morbidity and mortality and avoiding unwanted pregnancy as well.24
Accordingly, addressing contraceptive compliance can improve the lives of rural clients. In support of the present study, the Awi Zonal Health Bureau report showed that a large number of users had raised compliance. Health care providers at health center level also had an effect on client’s choice. Therefore, this study is aimed to assess compliance and its associated factors among rural reproductive age group women in Awi zone, Northwest Ethiopia.
Methods and Materials
Study Area and Setting
Awi zone has an estimated total population of 982,942 of whom 491,865 are men and 491,077 women; 970,333 or 92.97% are rural inhabitants.21 Indeed, its 2017 population estimated to 1,077,144. Awi zone is one of the ever green places of Ethiopia, and it has a variety of tourist attraction sites like Zengena Lake and a lot of rivers. Furthermore, the zone is known by horses. It has five governmental hospitals, 46 health centers, and 125 private clinics in the zone.25 In addition, the zonal health bureau report showed that the estimated number of reproductive-age women is 60,860.
Study Design and Period
A community-based cross-sectional study was conducted on women in reproductive age groups from Jan to April 30, 2021, in Awi zone, Northwest Ethiopia.
Target Population
All reproductive age 15 to 49 women who used any birth control method for the last 1 year before the survey in the Awi zone.
Inclusion and Exclusion Criteria
All women of the reproductive age group residing in the Awi zone for at least the last six months were included. However, clients who were mentally ill had a problem with hearing, and non-user mothers were excluded.
Sampling and Sampling Procedure
Multistage sampling was performed. At the first stage, among the nine districts as a rule of thumb (25%), three districts, namely, Ankwsha Guagusa, Chagnie and Zigem, were selected using simple random sampling. Likewise, in the second stage, from each district, 20 subunits of administration (Kebeles) were selected randomly, and based on probability of proportion to size was applied to fix the number of selected participants from each kebele households. Lastly, a total of 2341 (857,690 and 794) participants were selected by systematic random sampling and 2341 eligible women were interviewed.
Study Variables
Outcome Variable
The main outcome of the study was women’s compliance with any of family planning practices, which is measured as the response variable for the ith women which was represented by a random variable Yi, with two possible values coded as “1” and “0”. Therefore, the response variable of the ith women Yi was measured as a dichotomous variable with possible values Yi = 1, if the ith women had compliance experienced on any of family planning and Yi = 0 if the women had not compliance.
Independent Variables
Since the family planning data were a hierarchical structure where women were nested within the cluster/kebele health center, two levels of independent variables were considered. In Level 1 contained individual socio-demographic and women reproductive history variables-related characteristics (women’s age, marital status, religion, women’s job, women’s literacy, number of living children, family size, wealth index, women working status, plurality, abortion, death birth, birth interval, age at first pregnancy, age at first marriage, client method of contraceptive use, method of preference, frequency of sex, the nutritional self-assessment, knowledge of FP and women attitude) and in the Level 2 (health center level) community media exposure, enforcement exposure by a care provider or others and visited by family planning workers within the last 12 months were considered. Therefore, individual-level variables were aggregated at the cluster level to generate community-level variables, to see whether cluster-level variables affected compliance, and to see whether individual-level variables affected compliance.
Measurement of Knowledge and Attitude Related Variables
Knowledge Status of Clients Related Variables
Ever heard about family planning methods, sources of information were you get about FP (health extension worker, radio, TV, etc., if a woman will have exposure to at least one of the three, we consider it as she has media exposure), regarding perceived side effects of using family planning, a sign of headache (persistent), weight gain, amenorrhea, prolonged or heavy bleeding, lactation effect, fear of fewer side effects, and easily available. Those reproductive-age women who answered ≥77% of knowledge assessing questions were considered as having good knowledge.
Attitude Status of Clients Related Variables
Respondents ever discussed family planning issues with their partners and wanted to use it in the future communication with husband or friends on an FP, believe family planning exposes them to infertility, using family planning contradicts their religion and culture and those women who scored ≥90% from attitude assessing questions were considered as having favorable attitude.
Data Collection Procedure and Data Quality
A primary data source with a structured interview questionnaire method was applied. The quality of the data was maintained through pretest and close monitoring of the data collectors and supervisors, during the study period in a field. Furthermore, incompleteness and inconsistency of the data were checked, edited, and cleaned. The data collection questionnaire was developed after reviewing different relevant literature. The questionnaire was first developed in the English language and then translated to both Amharic and Agewegna (local languages) and retranslate back into English. A pretest was done on 5% of the total sample size at Dangla. After the pretest, necessary modifications and corrections took place to ensure validity. The survey data was collected by trained health professionals and during data collection, for confidentiality, any personal identifier was not used.
Statistical Analysis and Data Management
Since the birth control method data were hierarchical, ie, clients are nested within a cluster and we expect that women within the same cluster were more similar to each other than women within the rest of the kebeles. It violates the standard regression model assumptions, which are the independence of observations and the equal variance across cluster assumptions. This implies the need to take into account between-cluster variability by using an advanced model.26–29 For heterogeneity of proportion test z statistics considering the squared sample size as a weight factor were used. Therefore, a two-level mixed-effect logistic regression model was fitted to estimate the association between individual-level and community-level variables and the likelihood of experiencing compliance. Model comparison was done based on deviance (−2 log-likelihood) since the models were nested. LR test and intra-cluster correlation coefficient (ICC) were computed to measure the variation between clusters. The ICC quantifies the degree of heterogeneity of compliances between clusters (the proportion of the total observed variation in compliances that is attributable to between-cluster variations). Four models were constructed for the multilevel logistic regression analysis. The first model (a multilevel random intercept logistic regression model without covariates) was the null model without any explanatory variables, to determine the extent of cluster variations in compliances. The second model (a multilevel model with level 1 independent variables) was adjusted with individual-level variables. The third model (a multilevel model with level 2 variables) was adjusted for community-level variables, while the fourth model was fitted with both individual-level and community-level variables simultaneously. The final model was the best-fitted model since it had the lowest deviance value. Variables with a p value ≤0.25 in the bivariate analysis for both individual-level and community-level factors were fitted to the multivariable model. Adjusted OR (AOR) with 95% CI and a p value was reported, and the analysis was done using SAS version 9.2.
Operational Definition
Kebele is the smallest administrative unit in Ethiopia and which is a part of Woreda.
Compliance: According to the World Health Organization (WHO) definition compliance is the extent to which a person’s behavior coincides with medical or health advice and thus both continuation and correct use are required.
Results and Discussions
Results
Socio-Demographic and Maternal History Variables-Related Characteristics
In this study, 2341 reproductive age group women have participated. All distributed questionnaires were filled out completely and consistently. This made the response rate 100%. Out of the total study subjects, (52.6%) were aged 35–49 years, (43.1%) were aged 20–34, whereas (4.3%) were found to be aged 15–19 years. Nearly 97.6% were married (lived with their husband). Regarding religion (99.6%) of respondents was orthodox. About two-thirds (67.1%) of participants were illiterate. The majority (83.9%) were Agriculture workers, while (12.1%) were non-agricultural and (48.7%), had a medium wealth index. Similarly, (59.9%) of the study participants have a hard workload. The age at first marriage was less than eighteen years (66.6%) and the age at first pregnancy was less than eighteen years (68.9%). Indeed, (95.4%) of participants have a poor diet and almost all (99.1%) were given at single birth (Table 1). Preference for contraceptive method use.
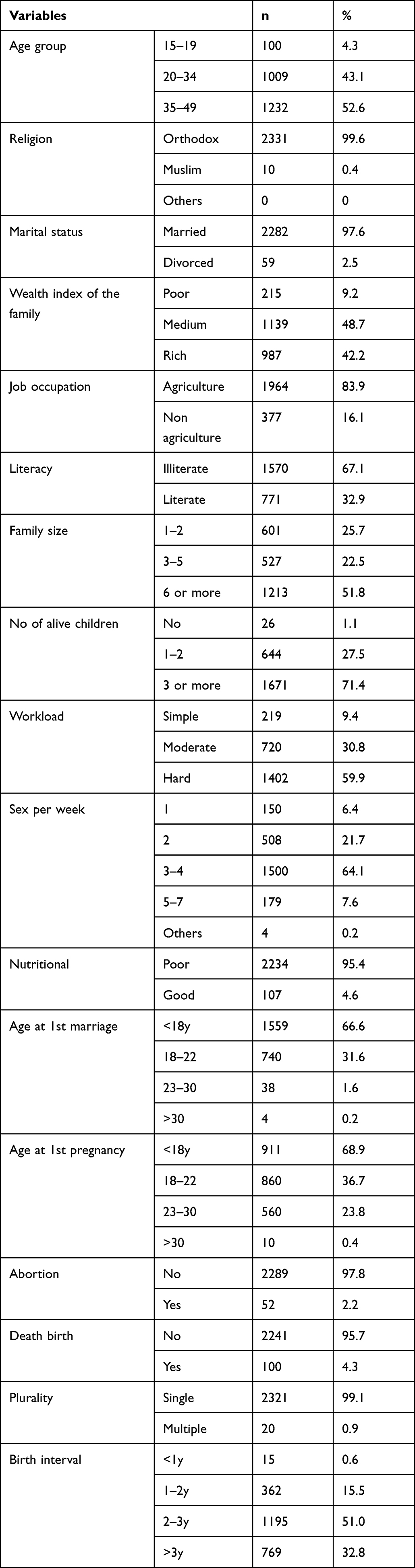 |
Table 1 Socio-Demographic, and Maternal History-Related Variable Characteristics of Study Participants (n = 2341) |
In this study, the most commonly preferred modern contraceptive method was short-acting birth control methods (74.6%), the second (17.1%) was long-acting, and (8.3%) were traditional. Furthermore, in this study, the most commonly preferred modern contraceptive method was injectable (68.8%), the second (12.4%) was pills, implants and IUDs contributed to 8.9% of the total percentage, and other contraceptive methods contributed less than 11.94%. About (91.5%) of respondents had got contraceptive methods according to their choice and only (8.5%) of the clients were enforced to take other than their choice of contraceptive methods (Table 2). Source of information, Knowledge, and Attitude toward contraceptive methods related characteristics.
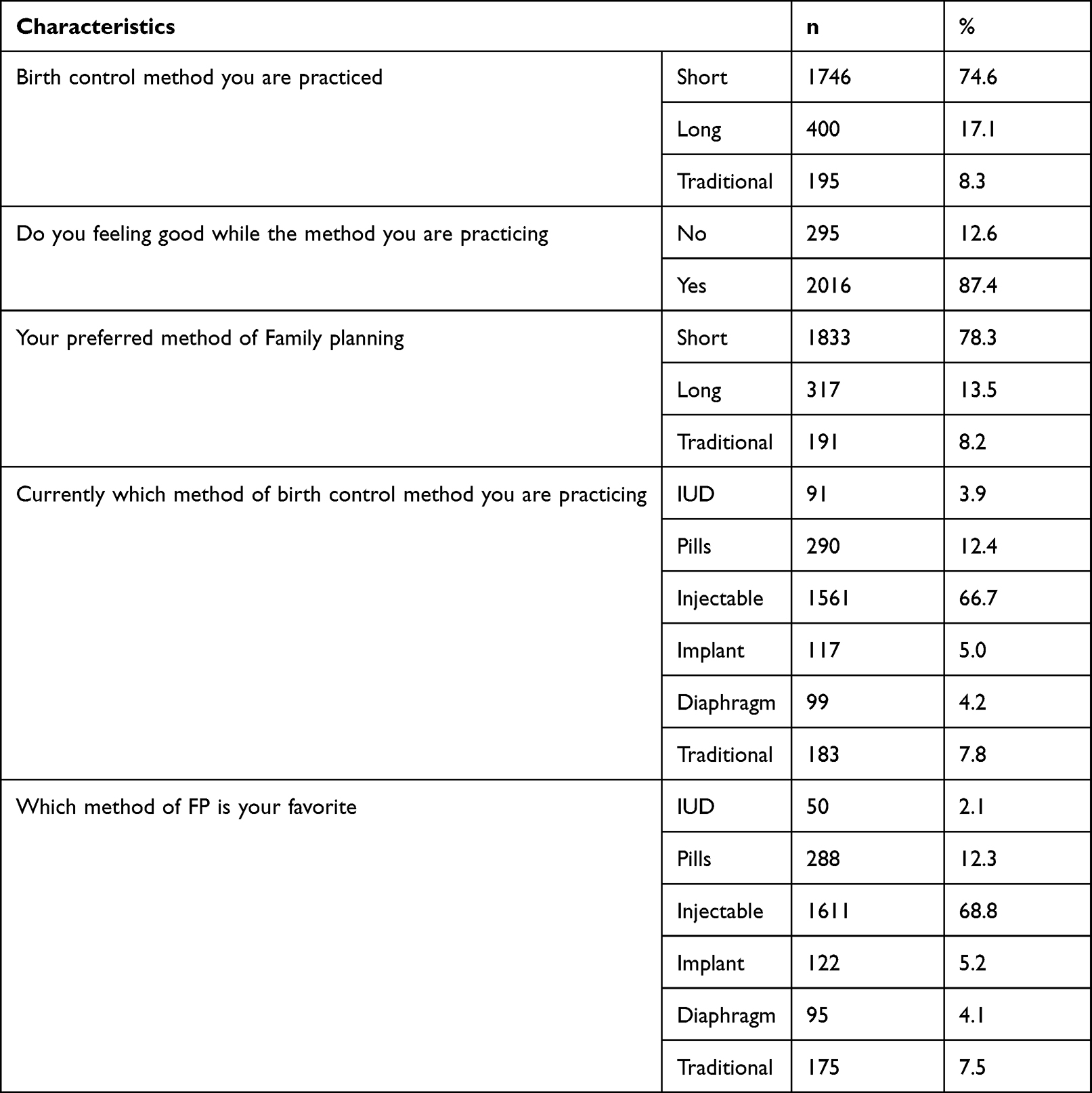 |
Table 2 Preference of Contraceptive Method Use-Related Characteristics of Study Participants (n = 2341) |
In this study, the respondents were also asked about their knowledge of contraceptive methods. Then, a composite index was produced by adding the six responses and a mean score was determined, and it was 3. Accordingly, (80.9%) of the respondents knew contraceptive methods and were labeled as having good knowledge, while (19.1%) were not had the knowledge and were labeled as not knowing. About 86.7% of the study participants obtained information about contraceptive methods from health extension workers. Likewise, the composite index of attitude indicated in Table 3 that (97.8%) of the clients had a positive attitude toward contraceptive methods (Table 3). Health center (Group level) variables related characteristics.
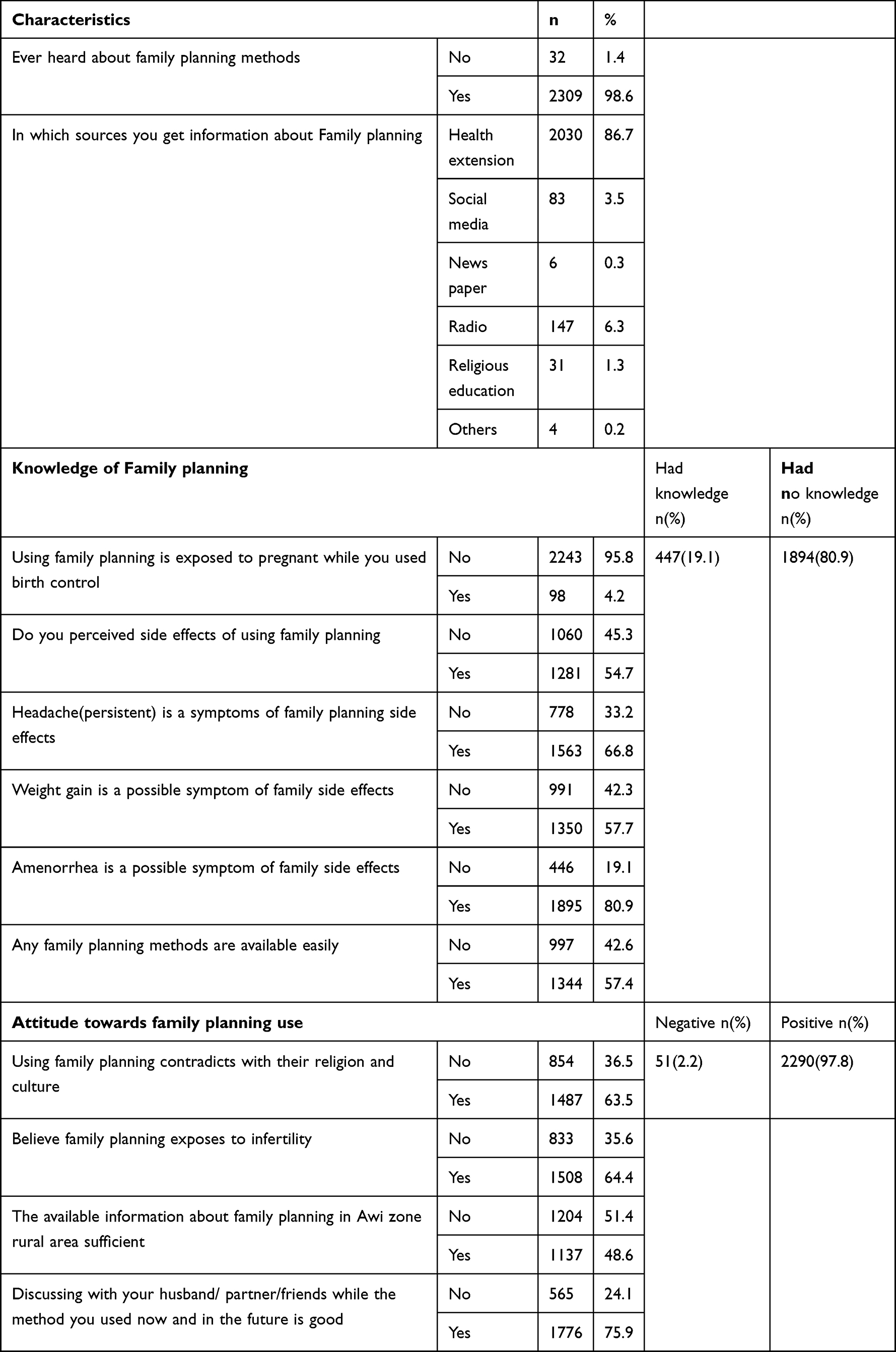 |
Table 3 Source of Information Knowledge, and Attitude Towards Contraceptive Methods Related Characteristics |
Exposure to mass media including radio, television, magazines/newspaper, at least for one of the media, remains below half of the study population. Only 34.4% of the women had exposure to media for 12 months preceding the survey. Media exposure for family planning was also low with (65.6%) of mothers do not hear through radio or TV or newspaper in the last few months before the survey at kebele level. Media exposure about family planning was poor even at group-level. About (8.5%) of the women had exposure to enforced to take other than their choice of contraceptive methods by health care providers (Table 4). Prevalence of contraceptives while used in family planning.
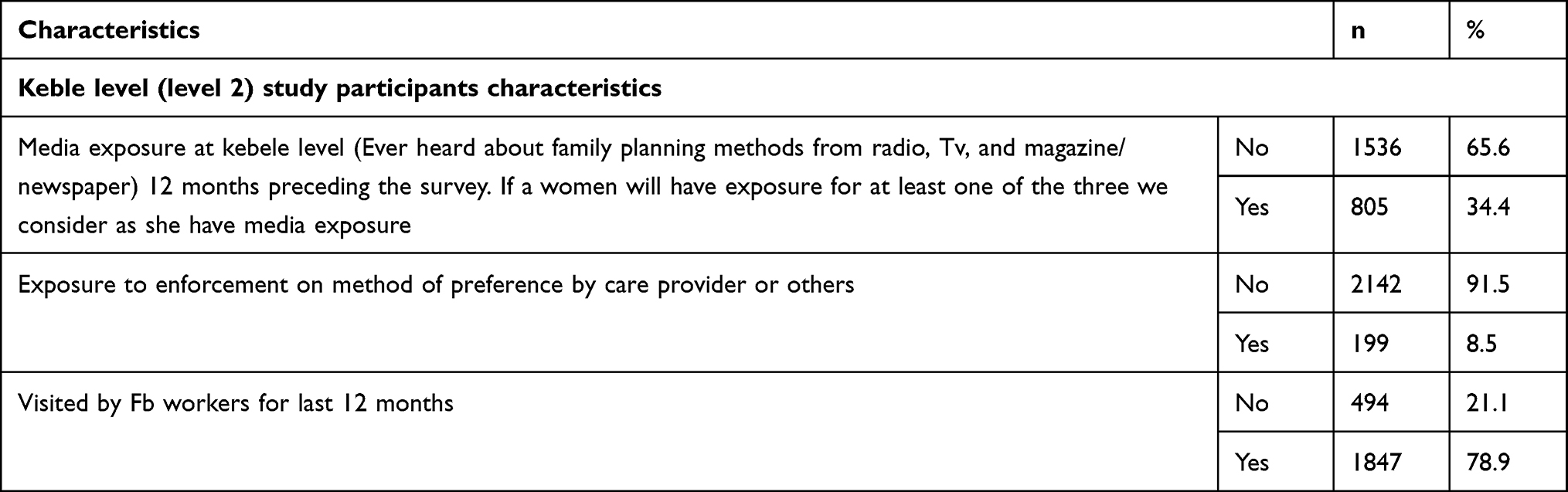 |
Table 4 Description of Cluster Background Characteristics Among Reproductive Age Women in Selected Awi Zone Health Posts (n = 2341) |
Results of this study showed that the prevalence of contraceptive compliance in selected districts of the Awi zone was 17.1%. The compliance varied significantly with different settings. For instance, the compliance was higher among those who had a hard workload (18.8%) and higher among women who had simple workload (9.6%). Similarly, compliance by method of contraceptive was IUD (78%), Implant (34.4%), injectable (17.0%), traditional (13.7%), and pills (7.6%) (Table 5). Factors associated with contraceptive compliance.
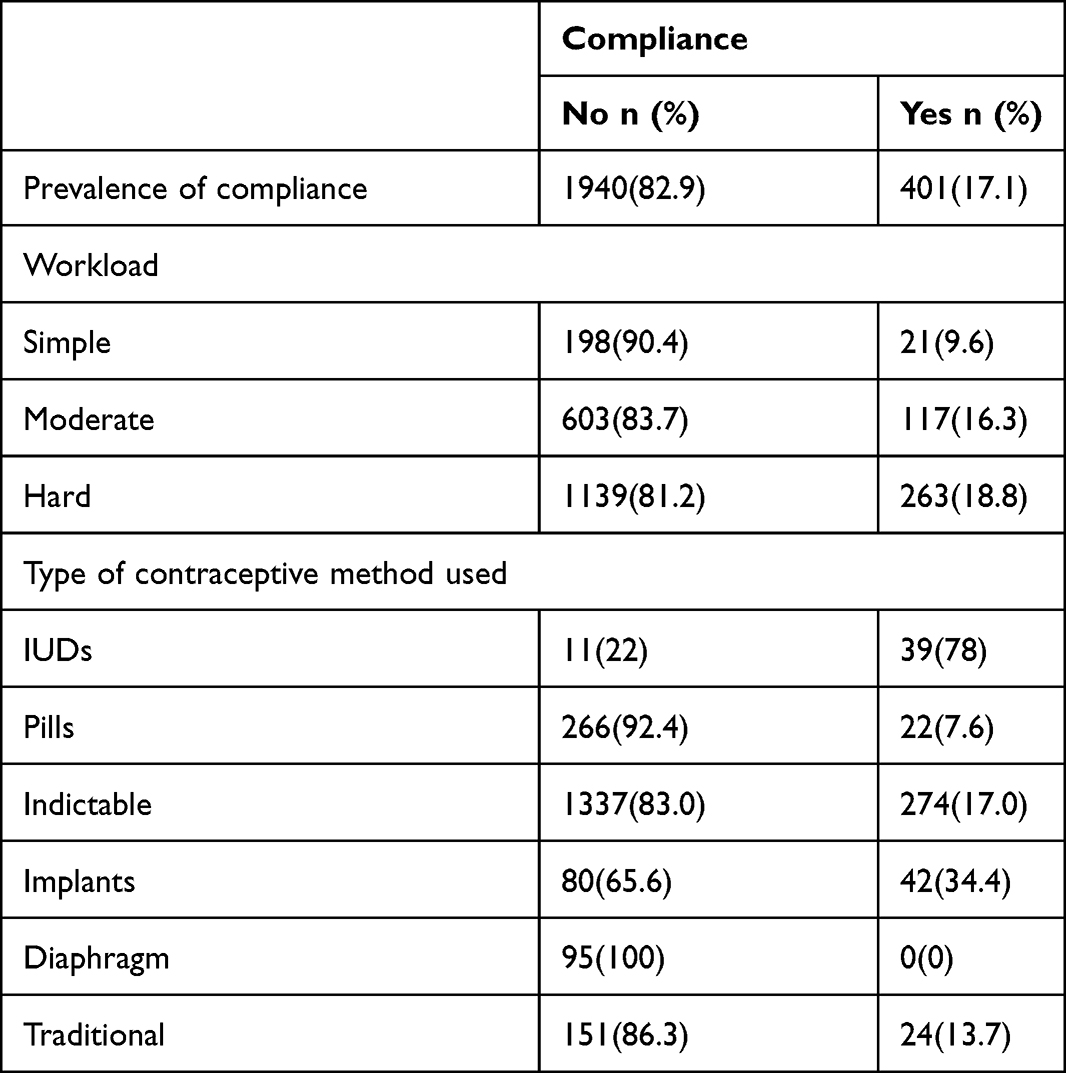 |
Table 5 Prevalence of Contraceptive Compliance by Clients Work Load and Type of Contraceptive Use |
A multilevel logistic regression model was used to identify the effect of contraceptive compliance on both individual and group-level factors. As presented in the empty model, 46% of the total variance in the odds of compliance was accounted for by between cluster variations of characteristics. The between cluster variability declined over successive models from 46% in the empty model to 42.8% in individual-level only model, 43.7% in the group-level factors only model, and 39.7% in the combined model. Thus, the combined model of individual-level and group-level factors were preferred for predicting women’s compliance while using contraceptives. Individual-level determinants in the model I with only individual-level variables were added. The result indicated that women’s age, marital status, women’s job occupation, number of living children, workload, type of contraceptive method used, and attitude towards contraceptive use were significantly associated variables with compliance. The ICC in model I indicated that 42.8% of the variation in compliance, while the use of contraceptives was attributable to difference across the health centers (group-level). From PCV in Table 6, 12.3% of the variance in compliance, while the use of contraceptives across group-level was explained by individual-level factors.
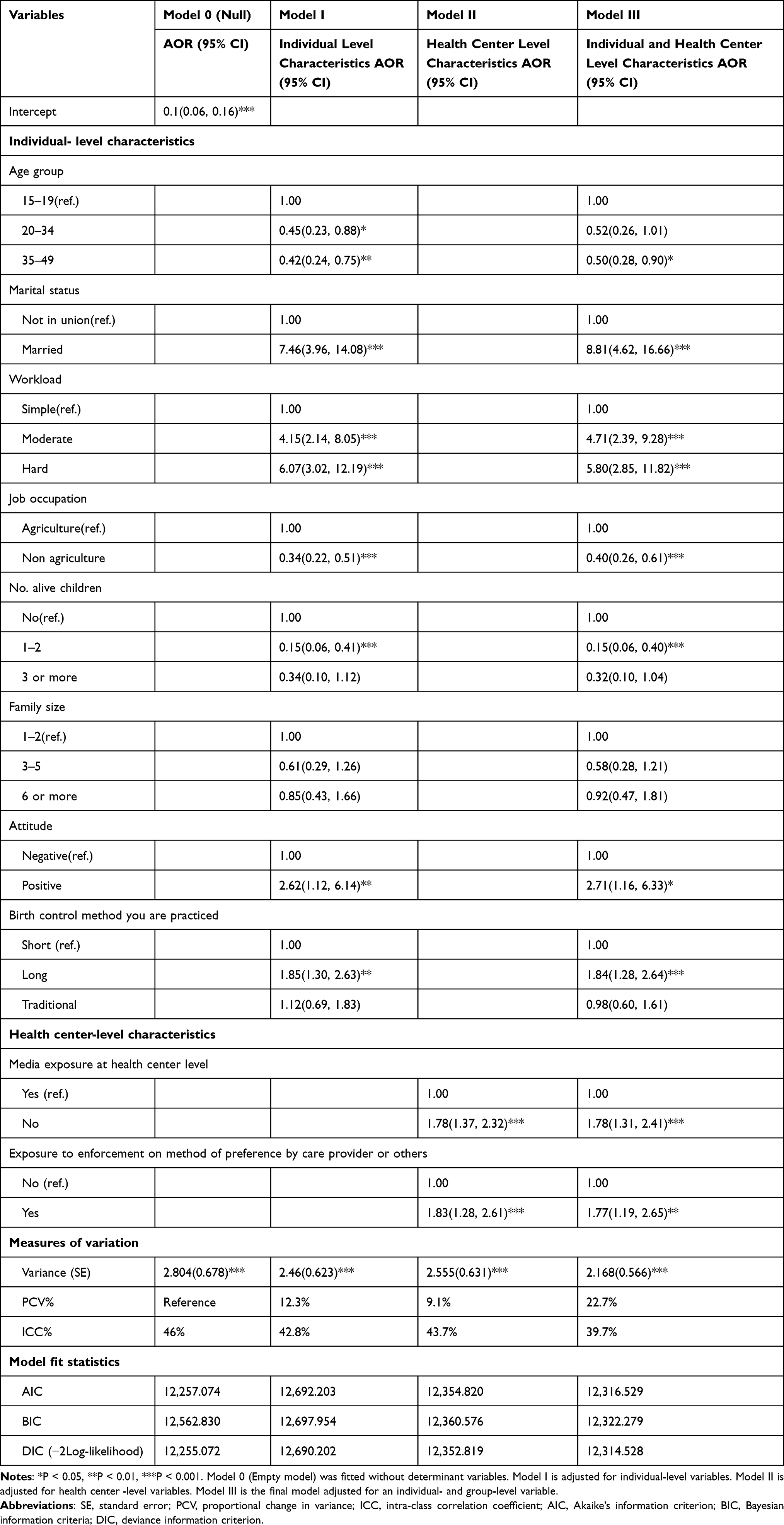 |
Table 6 Multilevel Logistic Regression Output for Predictor of Contraceptive Compliance Among Rural Reproductive Age Group in Awi Zone, Northwest Ethiopia (n = 2341) |
Respondents aged 35–49 years were 0.50 (AOR = 0.50, 95% CI 0.28, 0.90) times less likely to report compliance compared to 15–19 years old and married respondents were 8.81 (AOR = 8.81, 95% CI 4.62, 16.66) times more likely to report compliance to compare to not in union respondents. Respondents with one to two living children were 1.15 (AOR = 1.15, 95% CI 1.06, 1.40) times less likely to report compliance compared to respondents who had no living children. Surprisingly, respondents who had three or more living children did not affect compliance. Likewise, the workload was another factor that women’s respond compliance while using contraceptives. The odds of compliance for those women who have hard work was 5.80 (AOR = 5.80, 95% CI 2.85, 11.82) times higher than its counterpart. In other words, as workload increases from simple to hard, the odds of compliance also increases by 5.80 times. Compared to the simple, the odds of responding compliance by women for those who have moderate workload was 4.71 (AOR = 4.71, 95% CI 2.39, 9.28) times higher and the odds of compliance for non-agricultural in occupation was decreased by 0.4 compared to agriculture. Type of contraceptive method used was also another factor that brings compliance by users. As women’ use contraceptives method from short to long-acting the odds of compliance were increased by 1.84 (AOR = 1.84, 95% CI1.28, 2.64) and the odds of compliance for those who have a positive attitude was 2.71 (AOR = 2.71, 95% CI1.16, 6.33) times higher than its counterpart (Table 6).
Health Center Level (Group-Level) Factors
To examine if the characteristics of the cluster affect women’s compliance, while the use of contraceptives, regardless of women’s characteristics, we analyze group-level attributes. In Model II only group-level variables were added. Cluster characteristics like media exposure and enforcement exposure other than their choice were the factors associated with compliance. The ICC in this model implied that differences between health centers (group-level) account for about 43.7% of the variation in women’s compliance while using contraceptives. The PCV also showed that 9.1% of the variation in compliance between health centers was explained by group-level characteristics. As a clustering factor, media exposure was a strong predictor of compliance. Controlling other individual and community-level factors, hearing information about family planning on mass media information sources in the last 12 months contributed to compliance. Considering, health centers that had no media exposure as a reference, those health centers that had media exposure regardless of family planning had the highest odds of 1.78 (AOR = 1.78, 95% CI 1.32, 2.41) of compliance and health center-level enforcement exposure other than their choice increased odds 1.77 (AOR = 1.77, 95% CI 1.19, 2.65) (Table 6).
Random Effect Measures of Variation
The results of random effects indicated that there was a statistically significant variation in the compliance across the clusters. In other words, compliance was not similarly distributed across the clusters. The intra-cluster correlation coefficients (ICC) revealed that 43.7% of the variation in compliance could be attributed to health center-level factors. After adjusting for individual-level and group-level factors, there is a significant variation in compliance across clusters. About 22.7% of compliance, while the use of contraceptives in clusters was explained in the full model. Moreover, the ICC became decreased from 46% to 42.8%, 43.7% and 39.7%, this indicated that there was variation between clustering. Further, this indicated that when all factors are considered, the effects of clustering are still statistically significant in the full models. The model fit statistics also showed that the full model is better at predicting the compliance since the smaller the better (AIC = 12316.859, BIC = 12322.279, DIC (−2log likelihood) = 12314.528) (Table 6). Also, random slopes for the type of contraceptive model were fitted and the results showed that individual compliances were significantly varied within kebeles with regard to the type of contraceptive use P = 0.014 (Table 7).
 |
Table 7 Random Slope Coefficients of Clients by Type of Contraceptive Use Across Health Centers |
Discussion
This study was conducted to assess the determinants of contraceptive compliance among rural reproductive age group women at individual and health center (group level) in the Awi zone. We found that contraceptives compliance in selected districts of the Awi zone was clustered and affected by different individual and community-level variables and the prevalence was 17.1%.
At the individual level, variables such as women’s age, marital status, women’s job occupation, number of living children, workload, type of contraceptive method used, and attitude towards contraceptive use were significantly associated with compliance. Similarly, community-level access to media exposure and enforcement exposure other than their choice by health care providers or others was found to be a significant factor.
Results from intra-class correlation (ICC) found decreased from 46% to 42.8%, 43.7% and 39.7%. Thus, there is clustering variability in compliance at 5%. So that the current hierarchical analysis at each stage allows us to account for the random variations.26–29 The study also indicated that the standard error of (SE) outcomes, a measure of unexplained cluster heterogeneity, were 0.678, 0.623, 0.631, and 0.566 in null model, model 2, model 3, and model 4, respectively. The unexplained group-level variation in contraceptive compliance decreased to a SE of 0.566 when all variables were added to the empty model. The model fit statistics result also showed that the full model was better for predicting the compliance since the smaller the better (AIC = 12316.859, BIC = 12322.279, DIC (−2log likelihood)=12314.528).
Accordingly, the present study result also shows that short-acting (74.6%) was the most common type of preferred modern contraceptive method. Furthermore, among the short-acting method used inject able (68.8%), was the most common type of modern contraceptive used.7,21,24 A contraceptive method is an unindespansible tool for preventing and reducing maternal mortality and morbidity, as well for children.1,6,23
Women's age had effects on compliance, during the use of contraceptives, where older women had lower odds than young women in compliance. This effect is mainly associated with older aged women might be more experienced and adopted the vaccine contraceptives and most probably they have more desire to limit family size, which in turn variations. Evidence from the previous work showed that age1,4,6 affected contraceptive compliance. On the other hand, this study is not confirmed by studies conducted on age with birth control by9 indicating age is not associated with contraceptive compliance. A possible reason might be that the present study uses multilevel analysis approach so that it shows its effect well.
The marital status is also significantly associated with client’s compliance. Married women were more likely to report compliance than those not in the union. Even though there is no sufficient previous study supporting the present study, the problem might be due to a lack of regular discussion with her spouse regarding the contraceptive method used.3,13 Similarly, women job occupation is a fundamental concern in proceeding use of contraceptives, and it has a strong positive effect on user’s compliance. Indeed, users work from agriculture had more odds of compliance reports. Since, the country Ethiopia, particularly in the study area of the Awi zone, agriculture work through labor intensively, and this difficulty is somehow easy for others. Family feeding responsibility assignment is more tends to mothers in addition to agriculture and they prepare food with charcoal and fetching water from far places. This burden might be more serious than those who work with others. On the other hand, most contraceptive methods by nature require easy work and being a nutritionist and this finding is similar to the previous work by.12,14 On the contrarily studies3,19,22 showed that working status is not a contributing factor to compliance. The possible reason that makes the current study different might be that in the current study participants were rural women alone and a hierarchical multilevel model effect. Likewise, participants’ workload has a positive relationship with compliance,12,14 and having living children between 1 and 2 had lower odds of compliance than those who had no living children. In nulliparous women, the desired number of children is unmet and the intention to bear a child is high and more likely to report compliance. As the number of children increased, women tended to report compliance decreased as their desired number of children would be met.6,12,14
Most importantly, the type of contraceptives had a significant contribution to compliance. This study result indicates that women under long-acting were more likely to report compliance than short-term methods. Odds of users reporting compliance among those who used long-acting method of contraceptives were more likely than short-term methods. Since this study focuses on the rural part of users, it might be due to their life style. Results from previous study1,6,8–11,20 indicate that long acting method of contraceptive vaccines is better than short acting, while in the present study, it contradicts possibly, since this study focused on rural women and they have labor intensive work status may cause to this difference.
Individual-level attitudes toward contraceptive use were a contributing factor to compliance in the Awi zone. A possible reason could be that the clients’ compliance was concerns regarding the attitude in religion, culture, myth, safety, discussion with husband/partner and a lack of trust and insufficient information availability. The proportion of compliance for those participants who had a negative (bad) attitude towards the contraceptives was more likely to report compliance than those who had a positive (good) attitude. This might be due to the lack of sufficient information about contraceptives in the zone Awi regard to contraceptives. In addition to this, participants were believed to contradict religion and culture. More specifically, the more participant’s likelihood report compliance among those they were reported yes regards to the contraceptives contradicts with their religion and culture, exposes to infertility, lack of sufficient information, and spousal discussion and the woman’s approval of family planning were more likely to report compliance than its counterpart. Evidence from the previous study conducted in many countries, participants were reported vaccine hesitancy and refusal about its side effect.15–18
Community-level women's access to media and enforcement exposure were also significant group-level factors in compliance. These factors were significant in different studies.17,19,20 The change in the variance of the random intercept in that model suggests that the community-level factors did contribute to the variance between kebeles. The likelihood of reported compliance among those users nested under kebeles who had mass media campaigns and community mobilization activities as a community level were less likely to report compliance than users from kebeles who had no mass media exposure.12 In addition, women’s approval had less likely to report contraceptive compliance while in use.2–4,21,22
Conclusions
The prevalence of contraceptive compliance in the rural Awi zone was 17.1%. In Awi Zone, contraceptive compliance had significant variations across the kebeles or health centers. Women’s age, married women, number of living children, women's work status, type of contraceptive method, attitude, mass media exposure, and enforcement exposure were a significant factor for compliance. Therefore, public health interventions on family planning that enhance the client’s healthcare and contraceptive education in rural areas are crucial. Moreover, family planning therapeutic company shall consider those burdens for rural clients especially those who had a hard workload.
Data Sharing Statement
Data are available on reasonable requests. The dataset of the study findings is available from the corresponding author on reasonable request at [email protected].
Ethics Approval and Consent to Participate
The study was carried out after receiving an ethical clearance endorsement from Injibara University College of Natural and Computational Science Research Technical and Ethical Review Committee (Ref and all methods were carried out in accordance with relevant guidelines and regulations. All study participants had written informed consent to confirm willingness to participate after explaining the objective of the study. In addition, informed written consent was also obtained from the guardians of study participants and witnessed by the Injibara University Research Ethics Committee. Confidentiality of the information was maintained throughout by excluding names and keeping their privacy. Participants have the right to withdraw at any time from the interview.
and all methods were carried out in accordance with relevant guidelines and regulations. All study participants had written informed consent to confirm willingness to participate after explaining the objective of the study. In addition, informed written consent was also obtained from the guardians of study participants and witnessed by the Injibara University Research Ethics Committee. Confidentiality of the information was maintained throughout by excluding names and keeping their privacy. Participants have the right to withdraw at any time from the interview.
Acknowledgments
This study is financially supported by Injibara University, which does not participate in the design and formal analysis.
Author Contributions
The study was carried out in collaboration with all authors. HDM and MWL conceived the study, and carried out the study design and acquisition of data. YBC and YTC took the analysis of the data and wrote the draft manuscript. All authors critically read, revised and gave the final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding
This work was financed by the Injibara University of Research and Community Services, Ethiopia. It is not involved at any stage of the study.
Disclosure
The authors declare no conflicts of interest relevant to this work.
References
1. United Nations. Population Division Contraceptive Use by Method 2019: Data Booklet. Population Studies. United Nations; 2019:1–28.
2. United Nations. Department of economic and social affairs, population division. World Family Planning 2017 - Highlights (ST/ESA/SER.A/414). 2017.
3. Moreira LR, Ewerling F, Barros AJD, et al. Reasons for nonuse of contraceptive methods by women with demand for contraception not satisfied: an assessment of low and middle-income countries using demographic and health surveys. Reprod Health. 2019;16(1):148. doi:10.1186/s12978-019-0805-7
4. Ba DM, Ssentongo P, Agbese E, et al. Prevalence and predictors of contraceptive use among women of reproductive age in 17 sub-Saharan African countries: a large population-based study. Sex Reprod Healthc. 2019;21:26–32. doi:10.1016/j.srhc.2019.06.002
5. Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia and Rockville, Maryland, USA: CSA and ICF; 2016.
6. EPHI and ICF. Ethiopian Mini Demographic Health Survey. Key Indicators. Rockville, Maryland, USA: EPHI and ICF; 2019.
7. Scholl E, Gashaw SJ, Wagaw A, Wolde Micheal L. Assessment of youth reproductive health programs in Ethiopia. 2014.
8. Mohanan P, Sajjan KA. Fertility pattern and family planning practices in rural area in Dakshina Kannada. Indian J Com Med. 2003;28:15–18.
9. Aslami AN, Aansari MO, Khalique N, Kapil U. (NFHS-III), NFHS, India, International Institute for Population Sciences (IIPS) and Macro International. Indian J Physiol Pharmacol. 2007;1:192–222.
10. Johns Hopkins Bloomberg School of Public Health. Family Planning: A Global Handbook for Providers. Baltimore: Johns Hopkins Bloomberg School of Public Health; 2007.
11. RamaRao S, Liambila IS, Mane B, Mane B. Enhancing contraceptive choice for postpartum women in sub-Saharan Africa with the progesterone vaginal ring: a review of the evidence. Open Access J Contracept. 2015;6(117):117–123. doi:10.2147/OAJC.S55033
12. Tareke A, Tareke AA. Individual and community level associates of contraceptive use in Ethiopia: a multilevel mixed effects analysis. Archiv Public Health. 2019;77(46). doi:10.1186/s13690-019-0371-z
13. Gaetano M, Zaake LA, Annika J. Predictors of contraceptive use among female adolescents in Ghana. Afr J Reprod Health. 2014;18(1):102.
14. Haddis AH. Factors affecting unmet need for family planning in southern nations, nationalities and Peoples Region, Ethiopia. Ethiop J Health Sci. 2011;21(2):77–90.
15. ET Stock Report. Analysis of the 2000 and 2005 Demographic and Health Survey. Calverton, Maryland, USA: Macro International Inc.; 2007.
16. UNFPA, PATH-UNFPA. Outlook 25th anniversary. 2008:25.
17. Westoff CF. Unmet Need for Modern Contraceptive Methods. DHS Analytical Studies No. 28. Calverton, Maryland, USA: ICF International; 2012.
18. Korra A. Attitudes Toward Family Planning, and Reasons for Nonuse Among Women with Unmet Need for Family Planning in Ethiopia. Calverton, MD, USA: ORC Macro; 2002.
19. Eliason S, Quansah-Asare G, Graham-Hayfron Y, Bonsu D, Phillips J, AwusaboAsare K. Factors influencing the intention of women in rural Ghana to adopt postpartum family planning. Reprod Health. 2013;10. doi:10.1186/1742-4755-10-34
20. Mekonnen G, Enquselassie F, Tesfaye G, et al. Prevalence and factors affecting use of long acting and permanent contraceptive methods in Jinka town, Southern Ethiopia: a cross sectional study. Pan Afr Med J. 2014;18. doi10.11604/pamj.2014.18.98.3421
21. EDHS. Ethiopia Demographic and Health Survey (EDHS) 2016 Central Statistical Agency (CSA) [Ethiopia] and ICF. Addis Ababa, Ethiopia and Rockville, Maryland, USA: CSA and ICF; 2016.
22. Sonalkar S, Gaffield ME. Introducing the World Health Organization postpartum family planning compendium 2017. Int J Gynecol Obstetr. 2017;136(1):2–5. doi:10.1002/ijgo.12003
23. Say L, Chou D, Gemmill A. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2(6):323–333. doi:10.1016/S2214-109X(14)70227-X
24. Tsehaye WT, Mengistu D, Birhanu E, Berhe KK. Assessment of preference and its determinant factors to ward modern contraceptive methods among women of reproductive age group in Shire Indaselassie Town, Northern Ethiopia. Hindawi Publish Corporat Int J Fam Med. 2011;2013:8.
25. Central Statistical Agency. Population and housing cencus. 2007.
26. Breslow NE. Approximate inference in generalized linear mixed models. J Am Statist Assoc. 1993;88:9–25.
27. Snijders TAB, Bosker RJ. Multilevel Analysis: An Introduction to Basic and Advanced Multilevel Modeling. London, Thousand Oaks and New Delhi: SAGE Publications Ltd; 1999.
28. Goldstein H. Multilevel Statistical Models.
29. Commenges D, Jacqmin H. The intra-class correlation coefficient distribution frees definition and test. Biometrics. 1994;50(p):517–526. doi:10.2307/2533395
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.